prediction of survival in patients with head and neck cancer
TRANSCRIPT
PREDICTION OF SURVIVAL IN PATIENTS WITH HEADAND NECK CANCER
Robert Jan Baatenburg de Jong, PhD 1, Jo Hermans, PhD 2, Jan Molenaar 3,Jeroen Johannes Briaire 1, Saska le Cessie, PhD 2
1 Department of Otolaryngology and Head and Neck Surgery, Leiden University Medical Center, P. O. Box 9600,2300RC Leiden, Holland. E-mail: [email protected] Department of Medical Statistics, Leiden University Medical Center, P. O. Box 9600, 2300RC Leiden, Holland3 Datamanager ONCDOC (Oncology Documentation), Leiden University Medical Center, P. O. Box 9600, 2300RCLeiden, Holland
Accepted 22 January 2001
Abstract: Background. In patients with head and neck squa-mous cell carcinoma (HNSCC) the estimated prognosis is usuallybased on the TNM classification. The relative weight of the threecontributing parameters is often not completely clear. Moreover,the impact of other important clinical variables such as age, gen-der, prior malignancies, etc is very difficult to substantiate in dailyclinical practice. The Cox-regression model allows us to estimatethe effect of different variables simultaneously. The purpose ofthis study was to design a model for application in new HNSCCpatients. In our historical data-base of patients with HNSCC, pa-tient, treatment, and follow-up data are stored by trained onco-logical data managers. With these hospital-based data, we de-veloped a statistical model for risk assessment and prediction ofoverall survival. This model serves in clinical decision making andappropriate counseling of patients with HNSCC.
Patients and Methods. All patients with HNSCC of the oralcavity, the pharynx, and the larynx diagnosed in our hospitalbetween 1981 and 1998 were included. In these 1396 patients,the prognostic value of site of the primary tumor, age at diagno-sis, gender, T-, N-, and M-stage, and prior malignancies werestudied univariately by Kaplan-Meier curves and the log-ranktest. The Cox-regression model was used to investigate the effect
of these variables simultaneously on overall survival and to de-velop a prediction model for individual patients.
Results. In the univariate analyses, all variables except gen-der contributed significantly to overall survival. Their contributionremained significant in the multivariate Cox model. Based on therelative risks and the baseline survival curve, the expected sur-vival for a new HNSCC patient can be calculated.
Conclusions. It is possible to predict survival probabilities in anew patient with HNSCC based on historical results from a data-set analyzed with the Cox-regression model. The model is sup-plied with hospital-based data. Our model can be extended byother prognostic factors such as co-morbidity, histological data,molecular biology markers, etc. The results of the Cox-regressionmay be used in patient counseling, clinical decision making, andquality maintenance. © 2001 John Wiley & Sons, Inc. Head Neck23: 718–724, 2001.
Keywords: prognostic model; survival; head and neck squa-mous cell carcinoma; univariate analysis; multivariate analysis;Cox-regression; TNM-classification
The TNM grading system has been the mainstayof cancer outcome prediction in patients withhead and neck squamous cell carcinoma(HNSCC) for many years. The TNM consists of (1)the size of the primary tumor (Tis, T1, T2, T3, T4),
Correspondence to: R. J. Baatenburg de Jong
© 2001 John Wiley & Sons, Inc.
718 Survival Prediction for Head and Neck Cancer Patients HEAD & NECK September 2001

(2) description of regional (N0, N1, N2a, N2b,N2c, N3), and (3) distant metastasis (M0, M1).Each combination of these three variables can beseen as a bin into which patients with these char-acteristics are placed. This is called the TNM-binmodel1 and consists of 60 bins (5X6X2). One of thecharacteristics of a bin model is that the numberof bins increases rapidly with the number of vari-ables. For example, when we add the variable “pri-mary tumor site” (lip, oral cavity, nasopharynx,oropharynx, hypopharynx, glottic larynx, supra-glottic larynx, and esophagus), the result is 480bins. In fact we should also add relevant param-eters like age, gender, race, and histological grade.This would result in thousands of bins with veryfew patients in most of the bins even in large co-horts.
The clustering of various subsets of TNM cat-egories into four stages was undertaken in an at-tempt to stratify according to prognosis and tosimplify communication. This clustering will ofcourse result in a loss of accuracy because, forexample, a patient with a T4N0M0 carcinomamay biologically be very different from a patientwith a T1N2M0 carcinoma, whereas both tumorsare stage IV diseases. Furthermore, the stagegroupings were created based on presumed prog-nosis: no prospective, multivariate analysis wasperformed to create the four stage groupings fromthe various combinations of T, N, and M.2 In ad-dition, the stage grouping does not take otherprognostic parameters, such as age, gender, andprior malignancies, into account.
It is clear that, although the TNM classifica-tion harbors very important clinical information,it is not as useful in daily clinical practice as wewant it to be. Most importantly, it is not veryuseful for prediction of outcome in an individualcancer patient at initial presentation.
Multivariable techniques such as Cox regres-sion have provided methods to predict survivaltime from diagnosis until an endpoint (usuallydeath) for decades. However, complexity and un-familiarity with these methods at the level of phy-sicians and lack of sufficient clinically relevantdata prevented use in daily otolaryngeal practiceuntil now. The SOKAL score,3 which is used in
Table 1. Baseline demographic and tumor data of thestudy population.
(Sub)sites Number of PatientsLip 139Oral cavity 292Oropharynx 153Nasopharynx 41Hypopharynx 141Esophagus 218Glottic carcinoma 480Supraglottic carcinoma 198Total number of patients 1981–1998 1662
Excluding Tis and esophagusLip 138Oral cavity 286Oropharynx 152Nasopharynx 41Hypopharynx 141Glottic carcinoma 442Supraglottic carcinoma 196Total number of patients in this study 1396
GenderMale 1105Female 291Total 1396
Age categories<50 yr. 18850–59 37160–69 436$70 401Total 1396
T-stageT1 516T2 369T3 208T4 279Tx 24Total 1396
N-stageN0 985N1 148N2 180N3 82Nx 1Total 1396
Distant metastasisM0 1378M1 17Mx 1Total 1396
TreatmentIrradiation only 802Surgery only 223Surgery and postop irradiation 251Otherwise 120Total 1396
Year of diagnosis1981–85 3081986–90 3651991–95 4181996–98 305Total 1396
Table 1. (continued)
Prior malignanciesNone 1257Single prior malignancy 111Multiple prior malignancies 28Total 1396
Survival Prediction for Head and Neck Cancer Patients HEAD & NECK September 2001 719
haemato-oncology, is an example of an existingprognostic score. However, this system uses riskcategories as do most other prognostic systems.Although superior to, eg, the TNM staging (be-cause they are usually based on survival analy-sis), such systems lose information due to simpli-fication as well.
The purpose of this study was to design amodel in which the prognostic value of age, gen-der, site of the primary tumor, and T-, N-, andM-stage and prior malignancies is integrated topredict survival probabilities. This would allowfor a more precise and individual prediction ofoutcome in HNSCC patients. Therefore, thismodel may help in clinical decision making andappropriate counseling of patients with HNSCC.
PATIENTS AND METHODS
Between January 1981 and December 1998, 1662patients with primary HNSCC were diagnosed in
our hospital (Table 1). Patients with esophagealcancer (n 4 218) were excluded because (1) thenumber of patients with incomplete TNM stagingwas relatively large and (2) because prognosis isextremely poor. Patients with carcinoma in situ(n 4 51; including 3 patients with carcinoma insitu of the esophagus) were excluded as well be-cause the prognosis of these patients is very goodand because these patients did not contribute tosubclasses other than N0 and M0. The studysample contained 1396 patients with SCC of thelip, oral cavity, pharynx, and larynx.
Study Design. Data were collected from our hos-pital-based cancer registry system (ONCDOC),which was established in 1981. In this registrysystem, patient, treatment, and follow-up data ofeach cancer patient in our hospital are stored bytrained oncological data-managers. These dataare retrieved from the patients file and the hos-
Table 2. Multivariate analysis (FU limited to 120 months).
ParametersRegression
coefficient B p valueRelative risk
(exp (B))95% Confidence interval
for relative risk
(Sub)site .000Nasopharynx .000 1.000Lip .008 1.008 .545 1.865Oral cavity .695 2.003 1.169 3.432Oropharynx .429 1.535 .884 2.667Hypopharynx .625 1.868 1.079 3.236Glottic carcinoma .119 1.127 .647 1.961Supraglottic ca .250 1.284 .744 2.217
Gender .67Female .000 1.000Male .040 1.041 .865 1.252
Age .000<50 yr. .000 1.00050–59 .312 1.366 1.024 1.82460–69 .594 1.812 1.370 2.396$70 yr. .997 2.710 2.057 3.568
T-stage .000T1 .000 1.000T2 .391 1.478 1.189 1.839T3 .657 1.930 1.505 2.475T4 .860 2.363 1.853 3.014Tx .804 2.236 1.316 3.797
N-Stage .000N0 .000 1.000N1 .401 1.493 1.178 1.894N2 .725 2.065 1.639 2.601N3 1.044 2.841 2.143 3.766
Distant metastasis .000M0 .000 1.000M1 1.821 6.178 3.579 10.662
Prior malignancy7 .000No .000 1.000Yes .640 1.897 1.515 2.375
720 Survival Prediction for Head and Neck Cancer Patients HEAD & NECK September 2001
pital-based data-system1. ONCDOC also per-forms an independent and active follow-up. Pri-marily, the patients file is used for this purpose.When patients are lost to follow up, ONCDOCwill contact the family’s doctor and/or the DutchRegistry of Births, Deaths, and Marriages. In thisway follow-up is as complete as possible.
One of the other tasks of ONCDOC is qualitycontrol: the TNM stage, which is applied to a par-ticular patient, is checked retrospectively byONCDOC. When discrepancies exist, ONCDOCand the physician will discuss the TNM stage un-til agreement is reached. Patients were staged ac-cording the UICC manual. In 1981 the second edi-tion was used; from 1982–1988 the third editionwas used; from 1989–1992 the fourth edition wasused; from 1993–1998 the revised fourth editionwas used.
Choice of Factors. We included only simple andbasic variables (age, gender, site of the primary
tumor, T-, N-, and M-stage, and prior malignan-cies) available for all patients and available be-fore treatment. Prior malignancies were definedas all preceding malignant tumors except forbasal cell and squamous cell carcinoma of theskin.
Based on the therapeutic nil hypothesis,4–8
treatment was not considered as a prognostic fac-tor in this study (see Discussion).
Statistical Analysis. The only endpoint in thisstudy was overall survival. Follow-up of patientswas limited to 10 years after diagnosis becausethe number of patients with longer follow-up wassmall and these low numbers may theoreticallycause unjust differences in survival. The prognos-tic value of site of the primary tumor, age atdiagnosis, gender, prior malignancies, and T-, N-,and M-stage on survival were studied univari-ately by Kaplan-Meier curves and the log-ranktest. The Cox-regression model was used to inves-tigate the effect of these variables simultaneouslyon overall survival and to develop a predictionmodel for individual patients.1 ZIS by HISCOM, The Netherlands
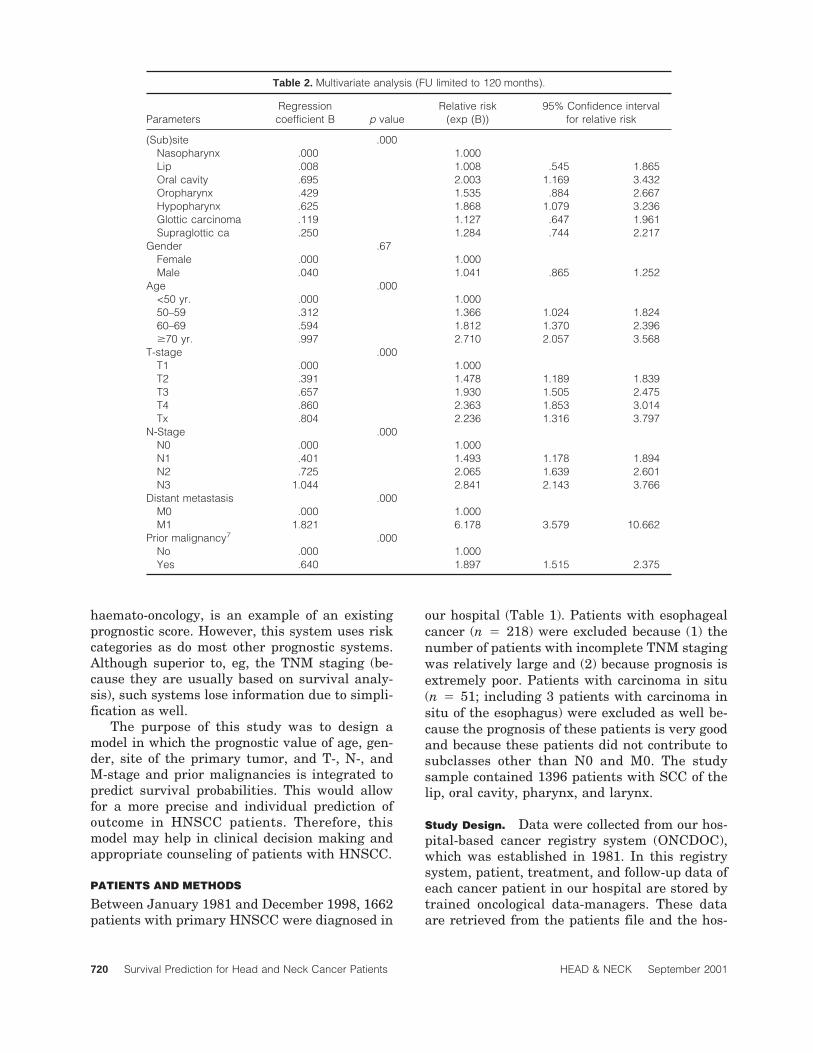
FIGURE 1. Expected survival for a 55-year-old male patient with a T1N2M0 carcinoma of the oral cavity (stage IV) and without a historyof prior malignancies. The expected 2- and 5-year overall survival rates are 67% and 45%, respectively.
Survival Prediction for Head and Neck Cancer Patients HEAD & NECK September 2001 721
Validation. The Cox model was validated in twoways: (1) for each patient a prognostic index iscalculated by adding the regression coefficients(Table 2) of the risk factors. A high prognosticindex indicates a poor prognosis. Based on thisprognostic index the patients were divided intofive groups (varying from patients with a favor-able prognosis to patients with a poor prognosis),and in each of the five groups the average ex-pected survival curve was compared with the ob-served Kaplan-Meier curve. (2) To judge the sta-bility of the prognostic index derived from the Coxregression, we applied a split-sample technique.9
For this purpose the total cohort was randomlysplit into two groups: two-thirds of the patientswas used to develop the prognostic index; theother one-third was used to check the predictivevalue of the index. The results in the latter groupconfirmed the predictions based on the formergroup (data not shown). Hence, only data for theentire data set are presented.
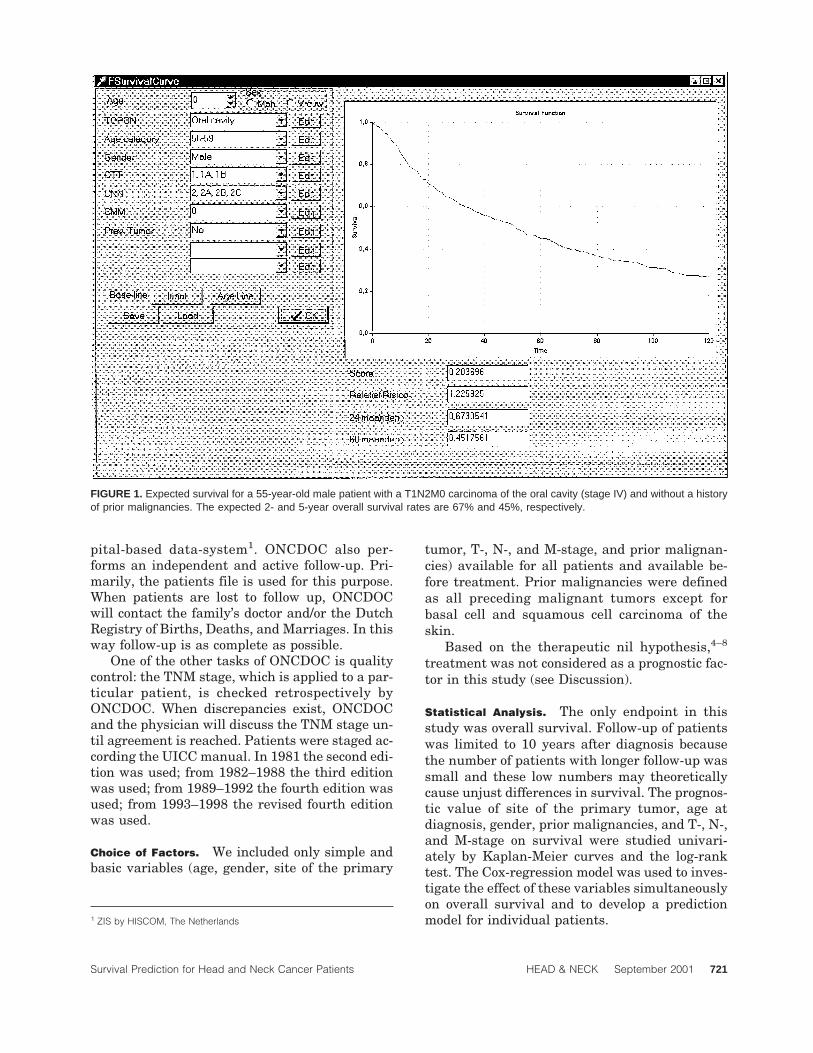
Software. Data were analyzed in SPSSt (version10.0). Dedicated software was designed in Bor-
land Delphit to allow for easy input of a new pa-tient for whom a prediction is needed. The calcu-lated survival curve for that individual is thendisplayed onscreen (Figures 1 and 2).
RESULTS
Follow-Up. The median follow-up time was 5.2years (range 0–120 months). Only 6% of the pa-tients were lost to follow-up.
Univariate Analysis. In the univariate analyses,all variables except gender contributed signifi-cantly to overall survival (Table 3).
Multivariate Analysis. Having established theunivariate relationship between age, gender, siteof the primary tumor, T-, N-, and M-stage, priormalignancies, and survival, the next step was toexamine how these variables perform in a mul-tiple Cox regression analysis. Patients with Nx (n4 1) or Mx (n 4 1) were excluded from this analy-sis. All variables (except gender) remained sig-nificant in the multivariate Cox model. Whereas
FIGURE 2. Expected survival for a 55-year-old male patient with a T4N3M0 carcinoma of the oral cavity (stage IV) without a history ofprior malignancies. The expected 2- and 5-year survival rates are 27% and 7%, respectively.
722 Survival Prediction for Head and Neck Cancer Patients HEAD & NECK September 2001
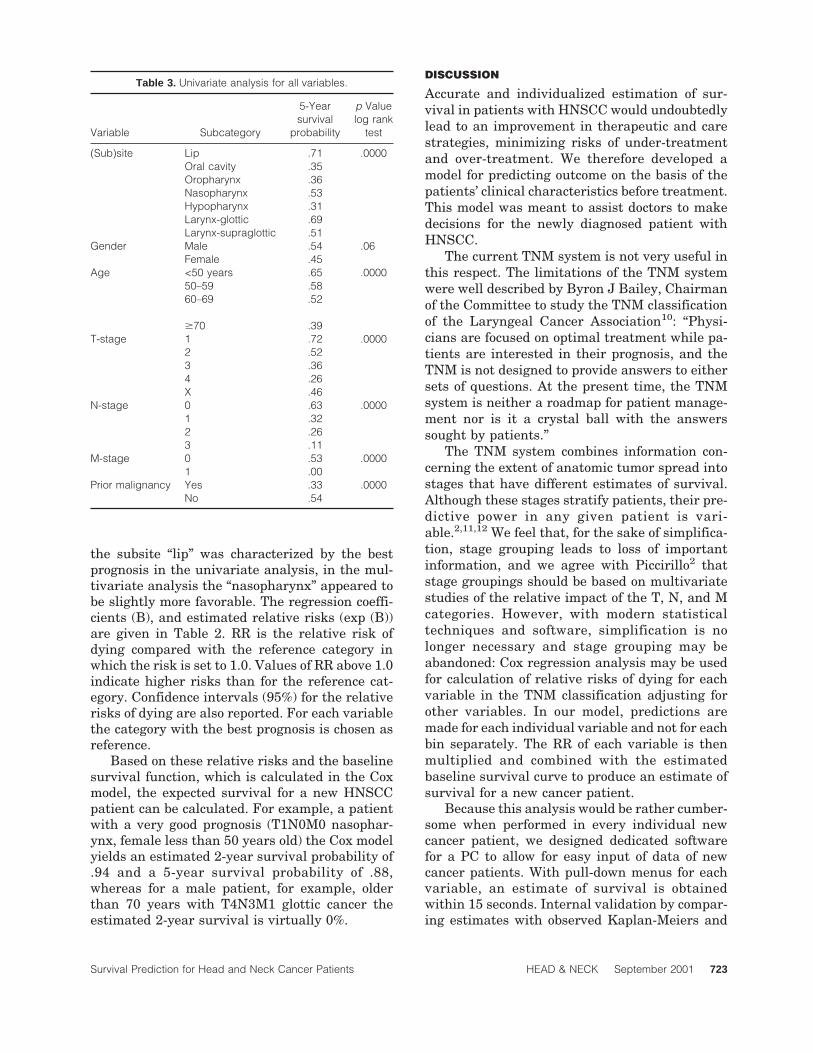
the subsite “lip” was characterized by the bestprognosis in the univariate analysis, in the mul-tivariate analysis the “nasopharynx” appeared tobe slightly more favorable. The regression coeffi-cients (B), and estimated relative risks (exp (B))are given in Table 2. RR is the relative risk ofdying compared with the reference category inwhich the risk is set to 1.0. Values of RR above 1.0indicate higher risks than for the reference cat-egory. Confidence intervals (95%) for the relativerisks of dying are also reported. For each variablethe category with the best prognosis is chosen asreference.
Based on these relative risks and the baselinesurvival function, which is calculated in the Coxmodel, the expected survival for a new HNSCCpatient can be calculated. For example, a patientwith a very good prognosis (T1N0M0 nasophar-ynx, female less than 50 years old) the Cox modelyields an estimated 2-year survival probability of.94 and a 5-year survival probability of .88,whereas for a male patient, for example, olderthan 70 years with T4N3M1 glottic cancer theestimated 2-year survival is virtually 0%.
DISCUSSION
Accurate and individualized estimation of sur-vival in patients with HNSCC would undoubtedlylead to an improvement in therapeutic and carestrategies, minimizing risks of under-treatmentand over-treatment. We therefore developed amodel for predicting outcome on the basis of thepatients’ clinical characteristics before treatment.This model was meant to assist doctors to makedecisions for the newly diagnosed patient withHNSCC.
The current TNM system is not very useful inthis respect. The limitations of the TNM systemwere well described by Byron J Bailey, Chairmanof the Committee to study the TNM classificationof the Laryngeal Cancer Association10: “Physi-cians are focused on optimal treatment while pa-tients are interested in their prognosis, and theTNM is not designed to provide answers to eithersets of questions. At the present time, the TNMsystem is neither a roadmap for patient manage-ment nor is it a crystal ball with the answerssought by patients.”
The TNM system combines information con-cerning the extent of anatomic tumor spread intostages that have different estimates of survival.Although these stages stratify patients, their pre-dictive power in any given patient is vari-able.2,11,12 We feel that, for the sake of simplifica-tion, stage grouping leads to loss of importantinformation, and we agree with Piccirillo2 thatstage groupings should be based on multivariatestudies of the relative impact of the T, N, and Mcategories. However, with modern statisticaltechniques and software, simplification is nolonger necessary and stage grouping may beabandoned: Cox regression analysis may be usedfor calculation of relative risks of dying for eachvariable in the TNM classification adjusting forother variables. In our model, predictions aremade for each individual variable and not for eachbin separately. The RR of each variable is thenmultiplied and combined with the estimatedbaseline survival curve to produce an estimate ofsurvival for a new cancer patient.
Because this analysis would be rather cumber-some when performed in every individual newcancer patient, we designed dedicated softwarefor a PC to allow for easy input of data of newcancer patients. With pull-down menus for eachvariable, an estimate of survival is obtainedwithin 15 seconds. Internal validation by compar-ing estimates with observed Kaplan-Meiers and
Table 3. Univariate analysis for all variables.
Variable Subcategory
5-Yearsurvival
probability
p Valuelog rank
test
(Sub)site Lip .71 .0000Oral cavity .35Oropharynx .36Nasopharynx .53Hypopharynx .31Larynx-glottic .69Larynx-supraglottic .51
Gender Male .54 .06Female .45
Age <50 years .65 .000050–59 .5860–69 .52
$70 .39T-stage 1 .72 .0000
2 .523 .364 .26X .46
N-stage 0 .63 .00001 .322 .263 .11
M-stage 0 .53 .00001 .00
Prior malignancy Yes .33 .0000No .54
Survival Prediction for Head and Neck Cancer Patients HEAD & NECK September 2001 723

by the split-sample technique was very satisfac-tory. In the near future our predictions will bevalidated in a different population.
Our data as collected by ONCDOC were spe-cifically intended for research according to a pro-tocol and therefore characterized by consistency,accuracy, availability, and completeness. Hoever,this is an observational study with a potential forbias and systematic errors in treatment assign-ment. The goal of this study was however not tocompare treatment options but to integrate diag-nostic data to improve our prognostic accuracy. Inany index for prognostic stratification, choices be-tween treatment options, which are not undercontrol of the investigator, will influence outcome.This systematic error cannot be eliminated and isthe reason why this study is based on the thera-peutic nil hypothesis.
The data presented here show that the out-come for a given patient can be presented by asimple score that makes use of known risk fac-tors. The risk of death increased cumulatively inproportion to the number and weight of risk fac-tors present.
In 1993 Burke and Henson1 formulated 12 cri-teria for selecting a prognostic system. Our modelfulfills most of these criteria. However, we did notstudy relapse predictions even though our modelis suitable for that purpose also. In addition, thisstudy was based on the nil hypothesis, and there-fore our model does not allow for grouping bytreatment. Evaluation of different treatmentstrategies can only be done by randomized trials.Results of such trials may only be included in aprognostic index under strict conditions. The onlyassumption we made is that the RR of the vari-ables studied are multiplicative. Interactions be-tween variables may play a role and will be sub-ject of further research. With these possibleshortcomings in mind, we feel that our model mayserve as the enhanced prognostic system Burkeand Henson1 proposed.
Finally, it is important to realize that the clini-
cal variables incorporated in this model aresimple variables that do not reflect the biologicalheterogeneity of HNSCC. Our goal is to identifyother prognostic markers and to study their inde-pendence in our model. When such a variable re-mains significant in the multivariate Cox analy-sis it may be added to the model.
CONCLUSIONS
It is possible to predict survival probabilities in anew patient with HNSCC based on historical re-sults from a data-set analyzed with the Cox-regression model. The results of the Cox-regression may be used in patient counseling,clinical decision making, and quality mainte-nance.
REFERENCES1. Burke HB, Henson DE. Criteria for prognostic factors and
for an enhanced prognostic system. Cancer 1993;72(10):3131–3135.
2. Piccarillo JF. Purposes, problems and proposals for prog-ress in cancer staging. Arch Otolaryngol Head Neck Surg1995;121:145–149.
3. The Italian Co-Operative CML Study Group. Prognosticdiscrimination in “good-risk” chronic granulocytic leuke-mia. Blood 1984;63:789–799.
4. Feinstein AR. Clinical biostatistics XIV. Clin PharmacolTher 1972;13:285–297.
5. Feinstein AR. Clinical biostatistics XV. Clin PharmacolTher 1972;13:442–457.
6. Feinstein AR. Clinical biostatistics XVI. Clin PharmacolTher 1972;13:609–624.
7. Feinstein AR. Clinical biostatistics XVII. Clin PharmacolTher 1972;13:755–768.
8. Picarillo JF, Wells CK, Sasaki CT, Feinstein AR. Newclinical severity staging system for cancer of the larynx.Ann Otol Rhinol Laryngol 1994;103:83–92.
9. The Chronic Leukemia Working Party of the EuropeanGroup for Blood and Marrow Transplantation. Lancet1998;352:1087–1092.
10. Bailey BJ. Beyond the ‘new’ TNM classification. Arch Oto-laryngol Head Neck Surg 1991;117:369–370.
11. Ahmad K, Kim YH, Fayos JV. Reliability of the AJCC’sstaging system as a prognostic indicator. Acta Oncol1987;26(3):173–174.
12. Fielding LP, Henson DE. Multiple prognostic factors andoutcome analysis in patients with cancer. Cancer1993;71(7):2426–2429.
724 Survival Prediction for Head and Neck Cancer Patients HEAD & NECK September 2001