precision cancer medicine - eiseverywhere.com · precision cancer medicine and big data with a...
TRANSCRIPT

Precision Cancer Medicineand Big Data
with a focus on children with cancer
Gilles Vassal
3
Each human being is unique
Desoxyribonucleic acid, DNA
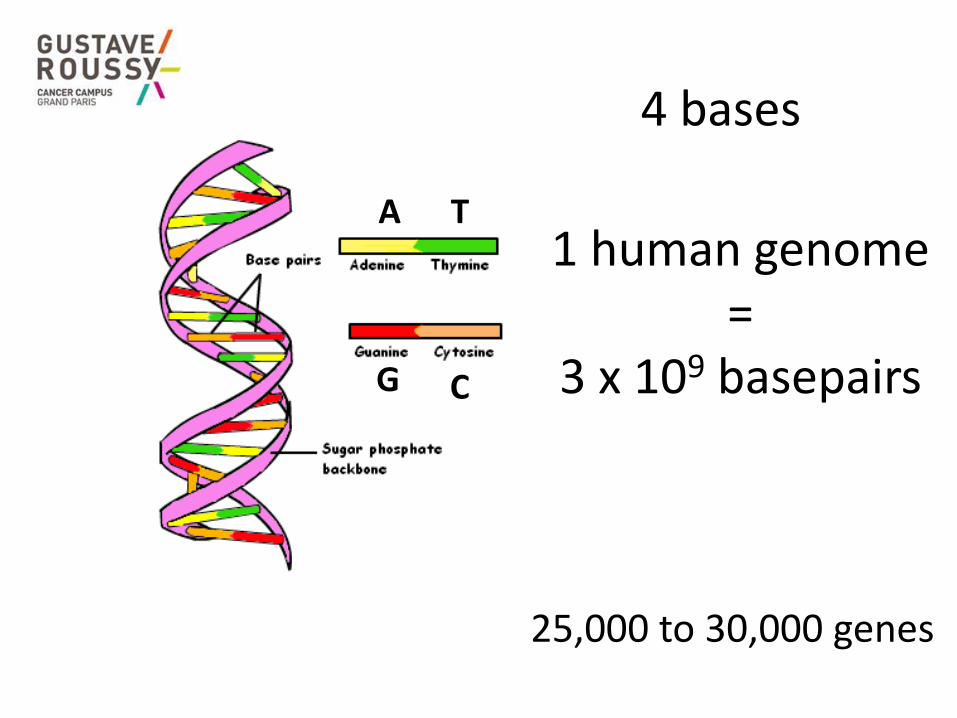
A T
G C
4 bases
1 human genome=
3 x 109 basepairs
25,000 to 30,000 genes
DNA sequencing of the First Human GenomeStarted 199013 years, $2.7 bnCompleted on April 14, 2013
Cancer
• Interaction between Genome and Environment
– Eg, Tobacco, UV, virus,…….
– Somatic alterations
• Genetic predisposition
– Eg Breast cancer (BRCA)
– Constitutional DNA
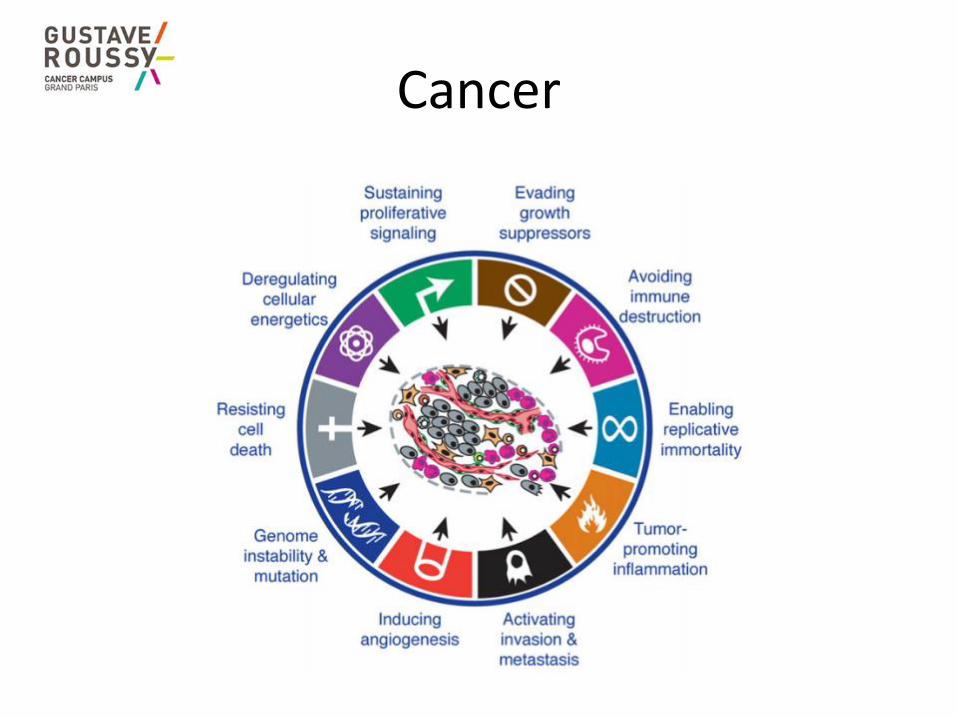
Cancer
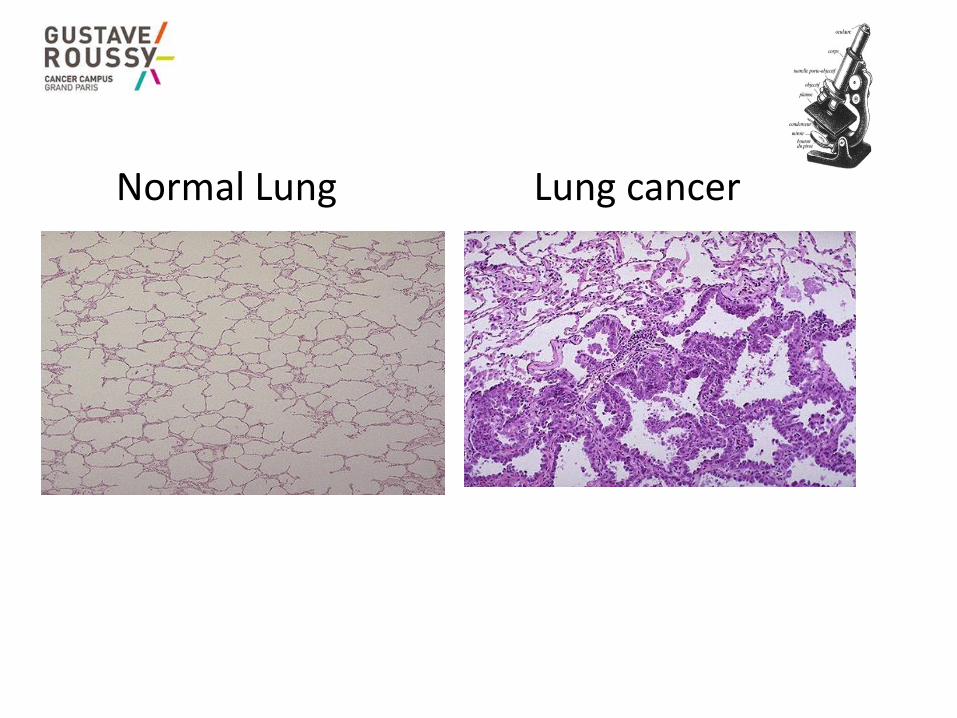
Normal Lung Lung cancer
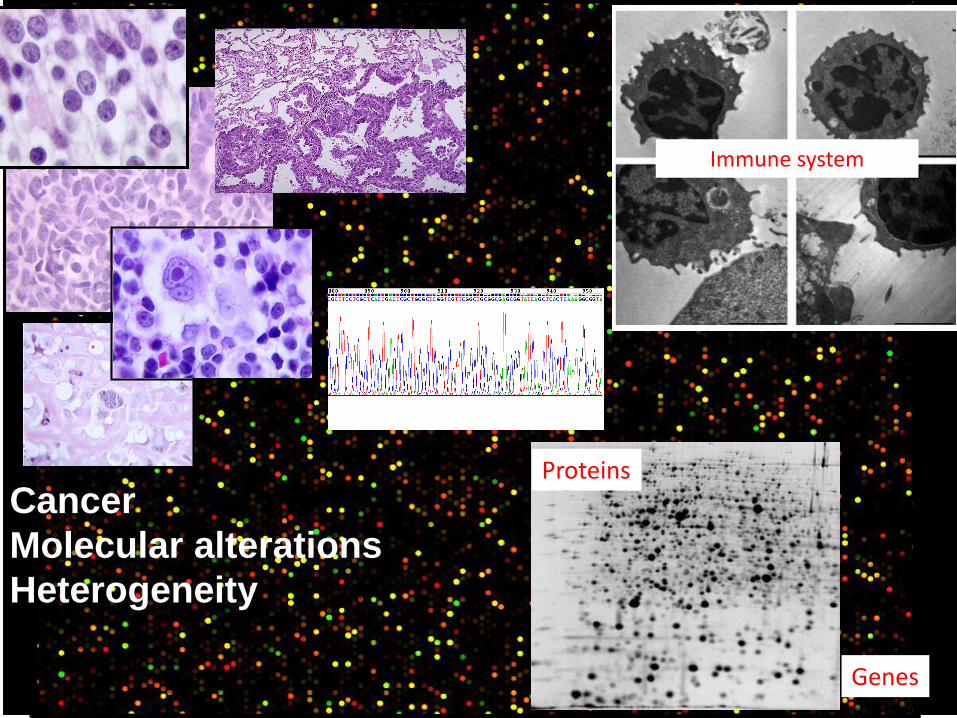
Genes
Cancer
Molecular alterations
Heterogeneity
Immune system
Proteins
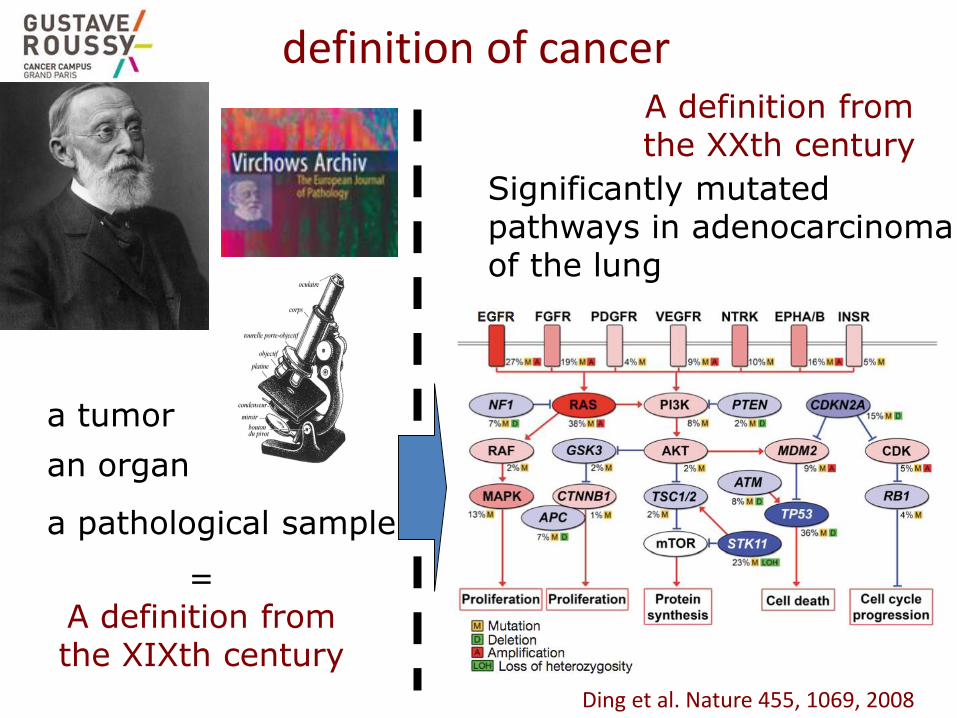
definition of cancer
a tumor
an organ
a pathological sample
= A definition from the XIXth century
Significantly mutated pathways in adenocarcinoma of the lung
Ding et al. Nature 455, 1069, 2008
A definition from the XXth century
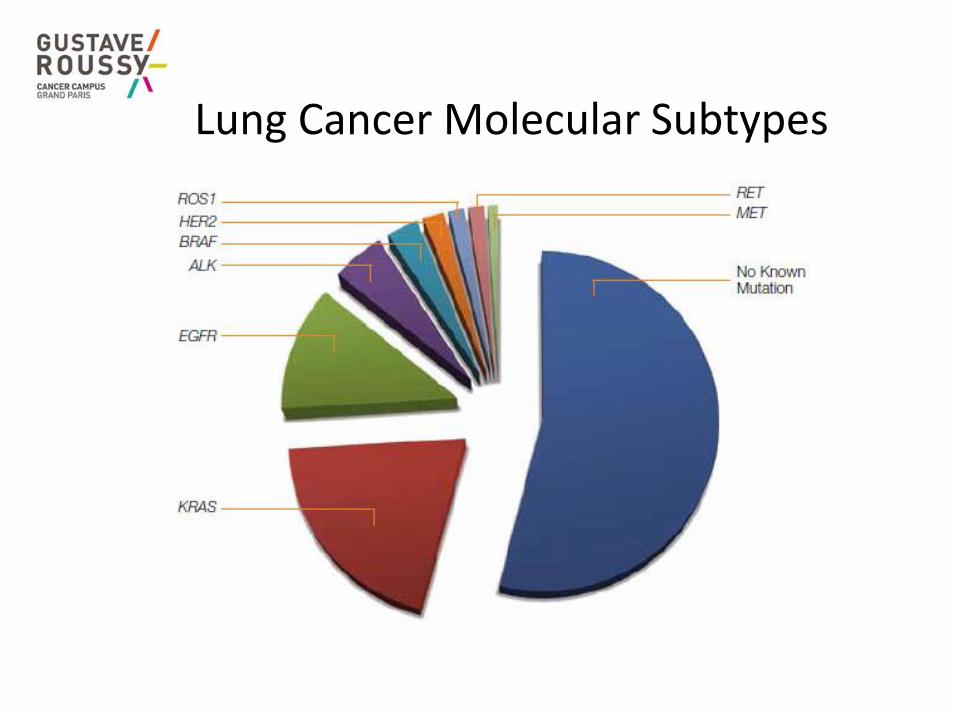
Lung Cancer Molecular Subtypes
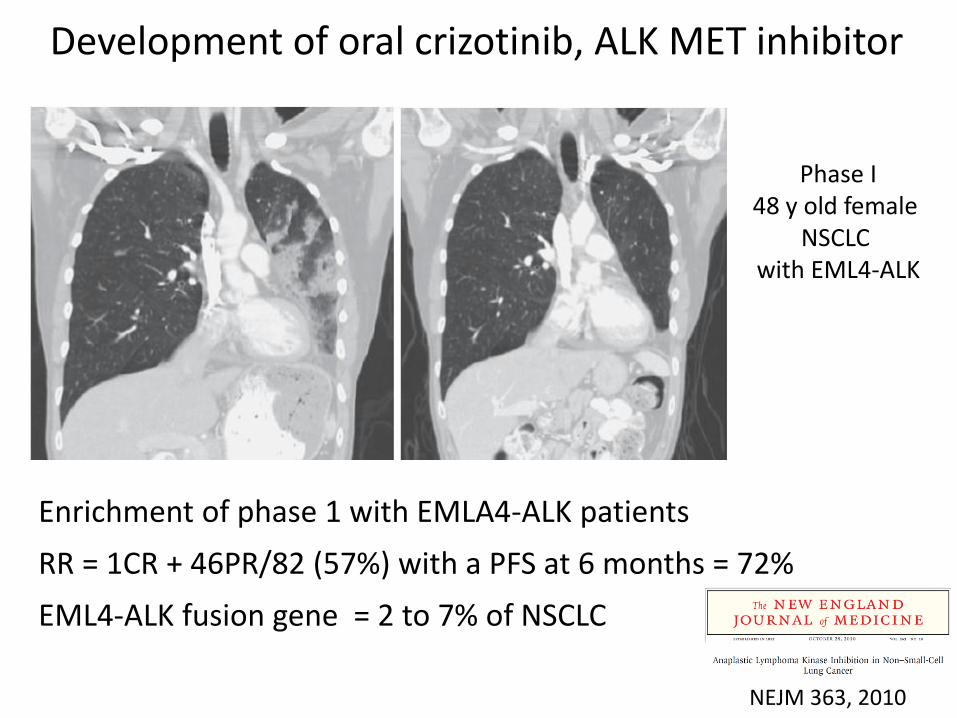
Enrichment of phase 1 with EMLA4-ALK patients
RR = 1CR + 46PR/82 (57%) with a PFS at 6 months = 72%
EML4-ALK fusion gene = 2 to 7% of NSCLC
Phase I48 y old female
NSCLC with EML4-ALK
NEJM 363, 2010
Development of oral crizotinib, ALK MET inhibitor
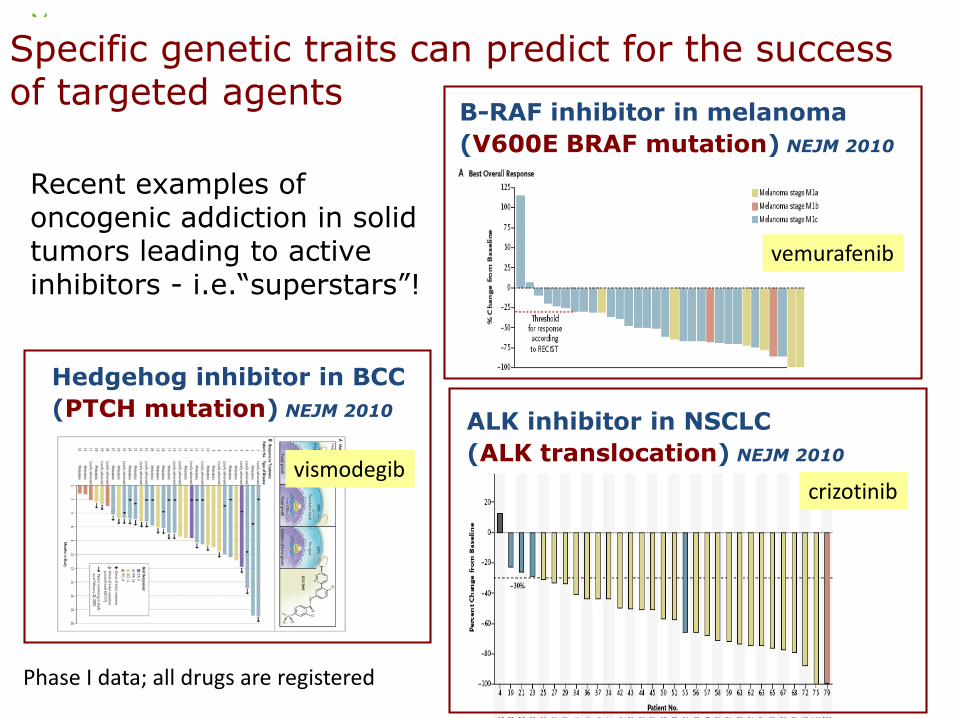
Specific genetic traits can predict for the success of targeted agents
Recent examples of oncogenic addiction in solid tumors leading to active inhibitors - i.e.“superstars”!
B-RAF inhibitor in melanoma
(V600E BRAF mutation) NEJM 2010
ALK inhibitor in NSCLC
(ALK translocation) NEJM 2010
Hedgehog inhibitor in BCC
(PTCH mutation) NEJM 2010
Phase I data; all drugs are registered
vemurafenib
crizotinibvismodegib
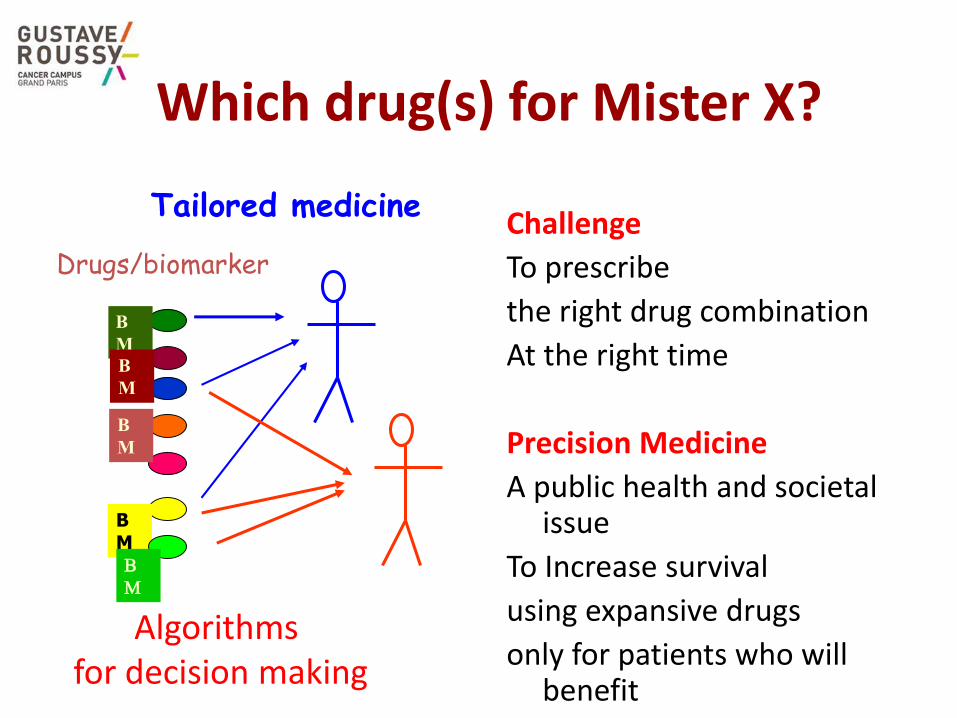
Which drug(s) for Mister X?
Challenge
To prescribe
the right drug combination
At the right time
Precision Medicine
A public health and societalissue
To Increase survival
using expansive drugs
only for patients who willbenefit
Drugs/biomarker
Tailored medicine
B
M
B
M
B
M
BMB
M
Algorithms for decision making
19
Precision cancer medecine
At least for a first step : Stratified Medicine
1. Moving away from empirism and serendipityto a biology-based therapy
2. Matching the right drug with the right cancer type
3. Defining the right response biomarker on each patient’s tumor
4. Organizing molecular follow up of patients under therapy
The Ultimate goal
individual biology-guided treatment decision
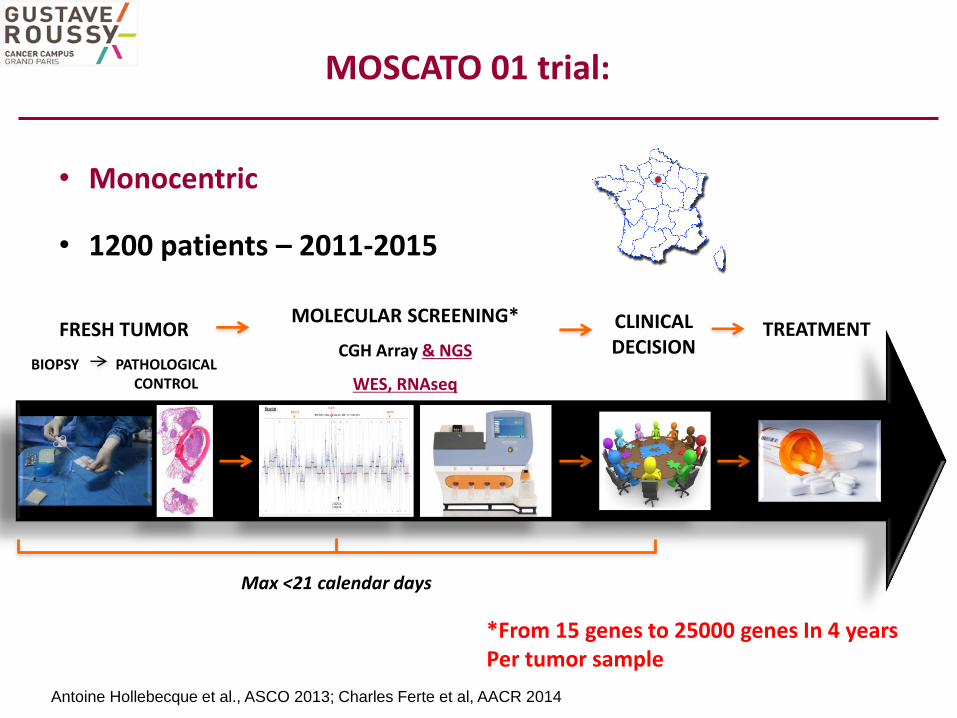
MOLECULAR SCREENING*
CGH Array & NGS
WES, RNAseq
CLINICAL DECISION
Max <21 calendar days
FRESH TUMOR
BIOPSY PATHOLOGICAL CONTROL
TREATMENT
• Monocentric
• 1200 patients – 2011-2015
Antoine Hollebecque et al., ASCO 2013; Charles Ferte et al, AACR 2014
MOSCATO 01 trial:
*From 15 genes to 25000 genes In 4 yearsPer tumor sample

0
5
10
15
20
25
30
35
40
45
50
Mut
atio
n PI
K3C
AA
mp
lific
atio
n FG
F4A
mp
lific
atio
n FG
F3M
uta
tion
KRA
SA
mp
lific
atio
n FG
FR1
Am
plif
icat
ion
PIK3
CAA
mp
lific
atio
n ER
BB
2Po
siti
ve IH
C P-
MET
Am
plif
icat
ion
MD
M2
Am
plif
icat
ion
EGFR
Tran
slo
cati
on N
OTC
H2
Am
plif
icat
ion
FGF1
9M
uta
tion
BRA
FA
mp
lific
atio
n N
OT
CH2
Mut
atio
n ER
BB2
Mut
atio
n EG
FRA
mp
lific
atio
n M
ET
Mut
atio
n PT
ENLo
ss P
TEN
Gai
n PI
K3C
AA
mp
lific
atio
n AR
Mut
atio
n N
RA
SM
uta
tion
FBXW
7M
uta
tion
AKT
1A
mp
lific
atio
n CC
ND
1Lo
ss N
OTC
H1
Tran
slo
cati
on A
LKA
mp
lific
atio
n KI
TG
ain
FGFR
1D
elet
ion
PTEN
Mut
atio
n ER
BB3
Am
plif
icat
ion
AKT2
Am
plif
icat
ion
CCN
E1A
mp
lific
atio
n FG
FR2
Am
plif
icat
ion
IGF
1RA
mp
lific
atio
n N
OT
CH1
Am
plif
icat
ion
PIK3
CBD
elet
ion
CDK
N2A
Del
etio
n CD
KN
2BM
uta
tion
FGFR
3M
uta
tion
HR
AS
Mut
atio
n ID
H1
Mut
atio
n IN
PP4B
Mut
atio
n M
ETM
uta
tion
TSC
1Lo
ss R
B1A
mp
lific
atio
n CC
NE2
Am
plif
icat
ion
CDK
4G
ain
FGF3
Mut
atio
n N
OTC
H4
Mut
atio
n TS
C2
Am
plif
icat
ion
EIF4
EBP1
Am
plif
icat
ion
PIK3
R5A
mp
lific
atio
n RI
CTO
RD
elet
ion
CHE
K1D
elet
ion
NF1
Del
etio
n TS
C1G
ain
AKT
1G
ain
AR
Mut
atio
n A
PCM
uta
tion
BRC
A2
Mut
atio
n FG
FR1
Mut
atio
n LK
B1
Mut
atio
n M
AP2K
4M
uta
tion
RB1
Mut
atio
n TP
53M
uta
tion
VH
LLo
ss C
DKN
2A
Loss
CD
KN2
BTr
ansl
oca
tion
ER
GTr
ansl
oca
tion
PTE
NTr
ansl
oca
tion
RO
S1A
mp
lific
atio
n AK
T1A
mp
lific
atio
n AL
KA
mp
lific
atio
n BR
AF
Am
plif
icat
ion
BRD
4A
mp
lific
atio
n CD
K2
Am
plif
icat
ion
CDK
6A
mp
lific
atio
n CD
K8
Am
plif
icat
ion
FGFR
Am
plif
icat
ion
FGFR
4A
mp
lific
atio
n ID
H2
Am
plif
icat
ion
IGF
1A
mp
lific
atio
n KD
RA
mp
lific
atio
n M
YCC
Am
plif
icat
ion
NO
TCH
3A
mp
lific
atio
n PD
GFR
AA
mp
lific
atio
n VE
GFA
Del
etio
n ST
K11
Del
etio
n TP
53
Gai
n FG
F4Po
siti
ve IH
C To
tal-M
ETM
uta
tion
CDKN
2A
Mut
atio
n FG
F19
Mut
atio
n FG
F3M
uta
tion
FGFR
Mut
atio
n FG
FR4
Mut
atio
n H
ER3
Mut
atio
n KI
TM
uta
tion
MTO
RM
uta
tion
PDG
FRA
Mut
atio
n ST
K11
Tran
slo
cati
on R
ET
105 actionable aberrations used to choose the targeted treatment
Fre
qu
en
cy (N
)
27 most frequent abormalitiesrepresent 78% of the actionable aberrations
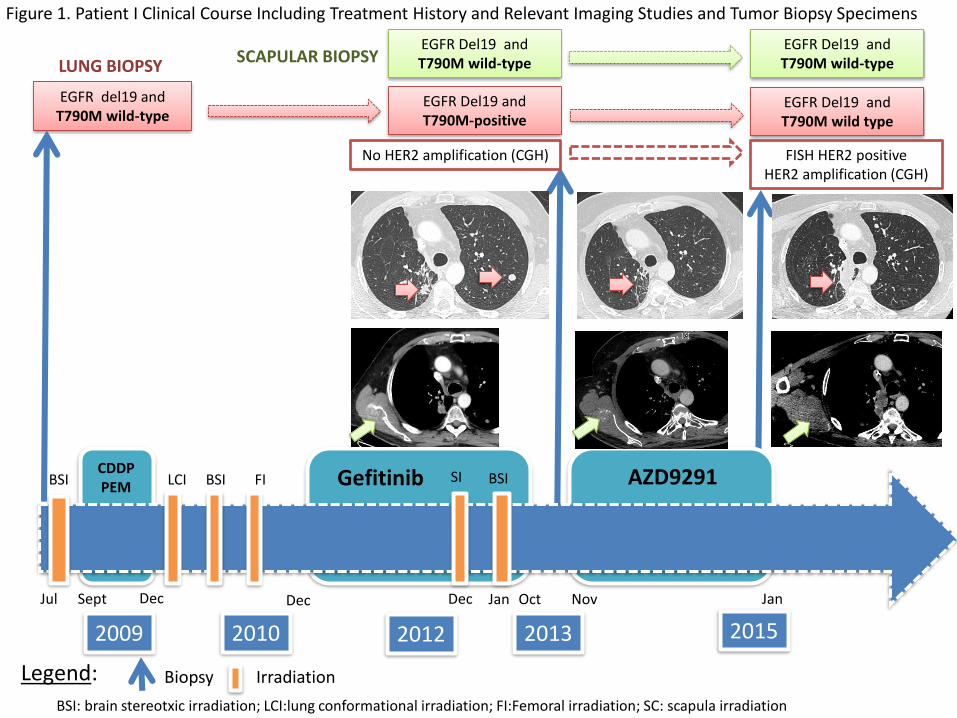
BSI LCI
LUNG BIOPSYSCAPULAR BIOPSY
FI
Biopsy IrradiationLegend:
BSI
BSI: brain stereotxic irradiation; LCI:lung conformational irradiation; FI:Femoral irradiation; SC: scapula irradiation
2012
Dec
SI BSI
JanDecSeptJul Dec Oct Nov Jan
2009 2010 2013 2015
EGFR Del19 and T790M-positive
Gefitinib AZD9291
EGFR del19 and T790M wild-type
CDDPPEM
EGFR Del19 and T790M wild-type
EGFR Del19 and T790M wild-type
EGFR Del19 and T790M wild type
Figure 1. Patient I Clinical Course Including Treatment History and Relevant Imaging Studies and Tumor Biopsy Specimens
FISH HER2 positiveHER2 amplification (CGH)
No HER2 amplification (CGH)
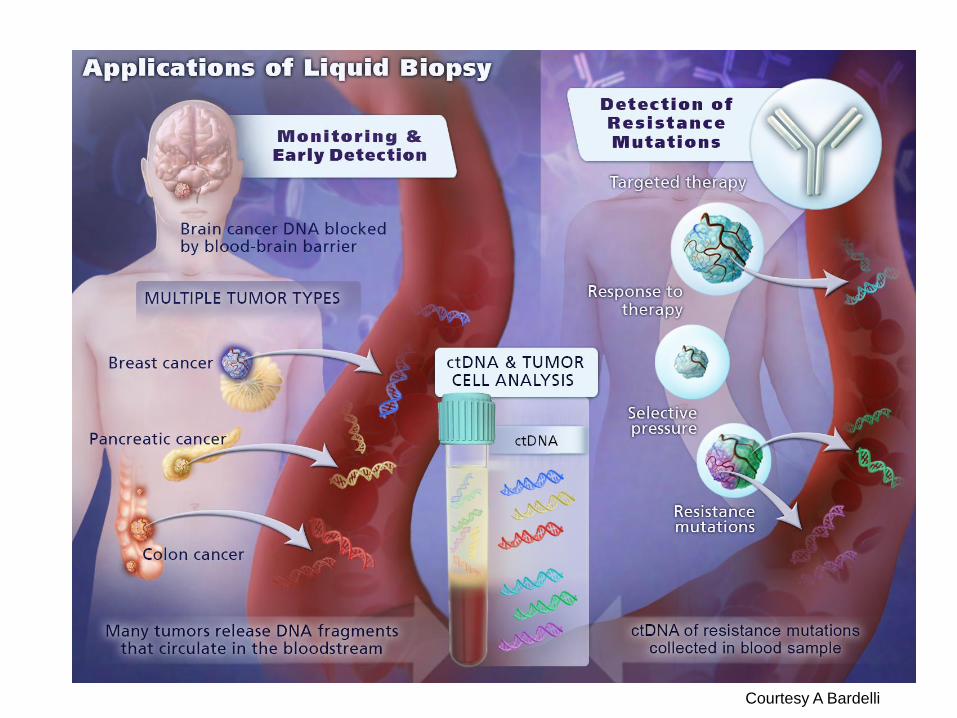
Courtesy A Bardelli
Cancer in Young People in Europe
Each year: 35 000 new cases 15,000 <15 years and 20,000 15 -24 years
80% are disease-free at 5 years with multidisciplinary treatments 300,000 EU citizens are childhood cancer survivors
2/3 have long-term side-effcets
6,000 young people die each year
Cancer: first cause of death by disease beyond one year in EU
STILL A PUBLIC HEALTH ISSUE
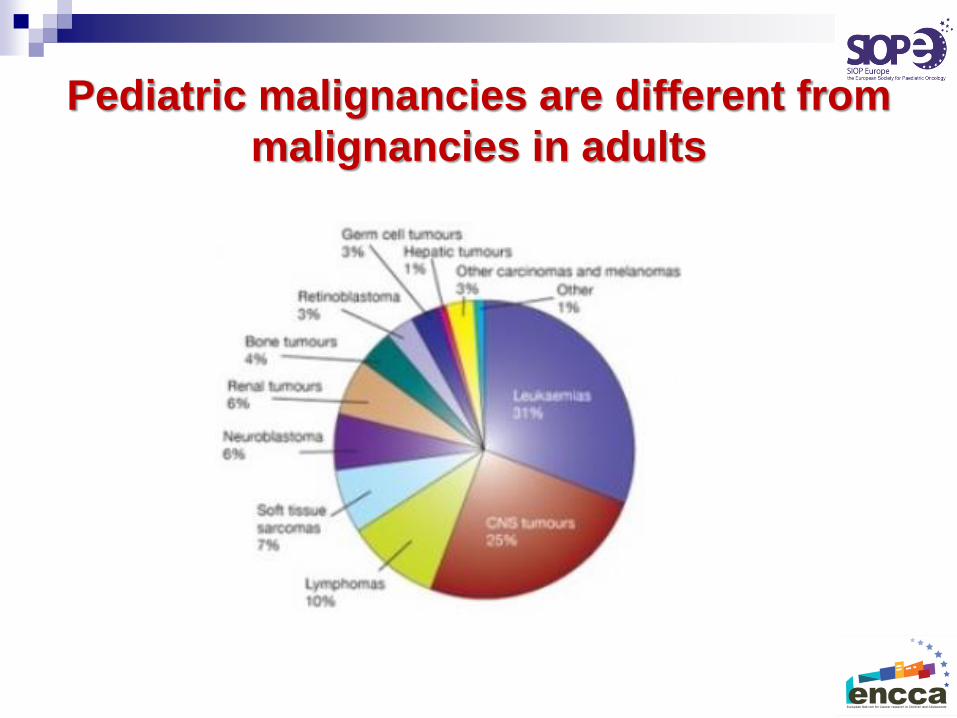
Pediatric malignancies are different from
malignancies in adults
http://www.siope.eu/SIOPE_StrategicPlan2015/
By 2025:
To increase cure rate in patients with poor
prognosis malignancies
To increase quality of life (cure) in survivors
To tackle inequalities
SIOPE Strategic Plan
A long term sustainable strategy
Designed within the FP7
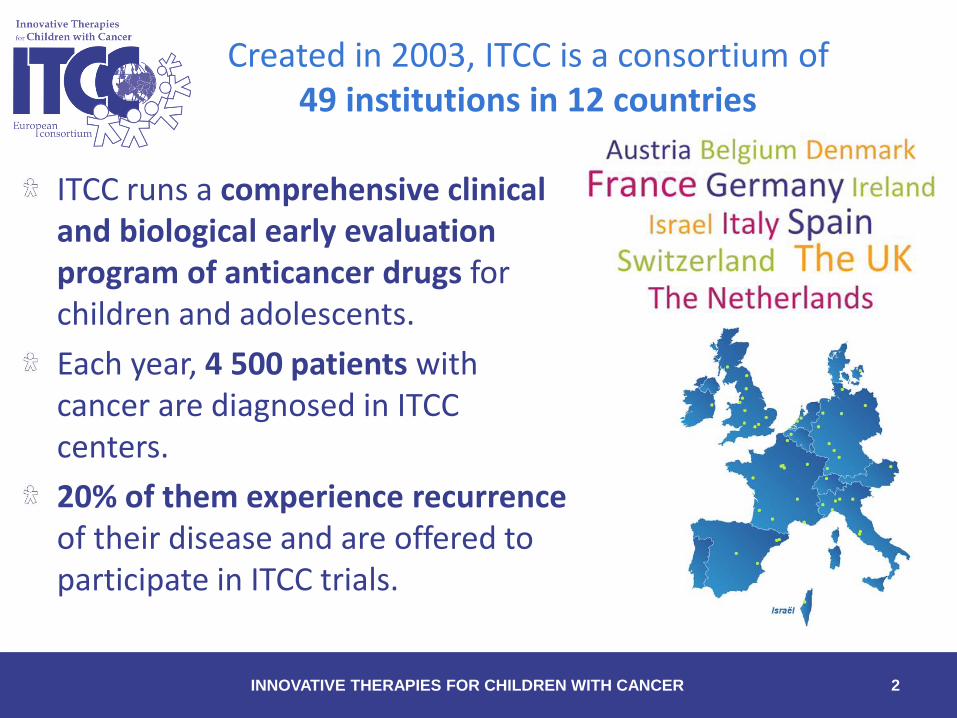
Created in 2003, ITCC is a consortium of 49 institutions in 12 countries
INNOVATIVE THERAPIES FOR CHILDREN WITH CANCER 2
ITCC runs a comprehensive clinical and biological early evaluation program of anticancer drugs for children and adolescents.
Each year, 4 500 patients with cancer are diagnosed in ITCC centers.
20% of them experience recurrenceof their disease and are offered to participate in ITCC trials.
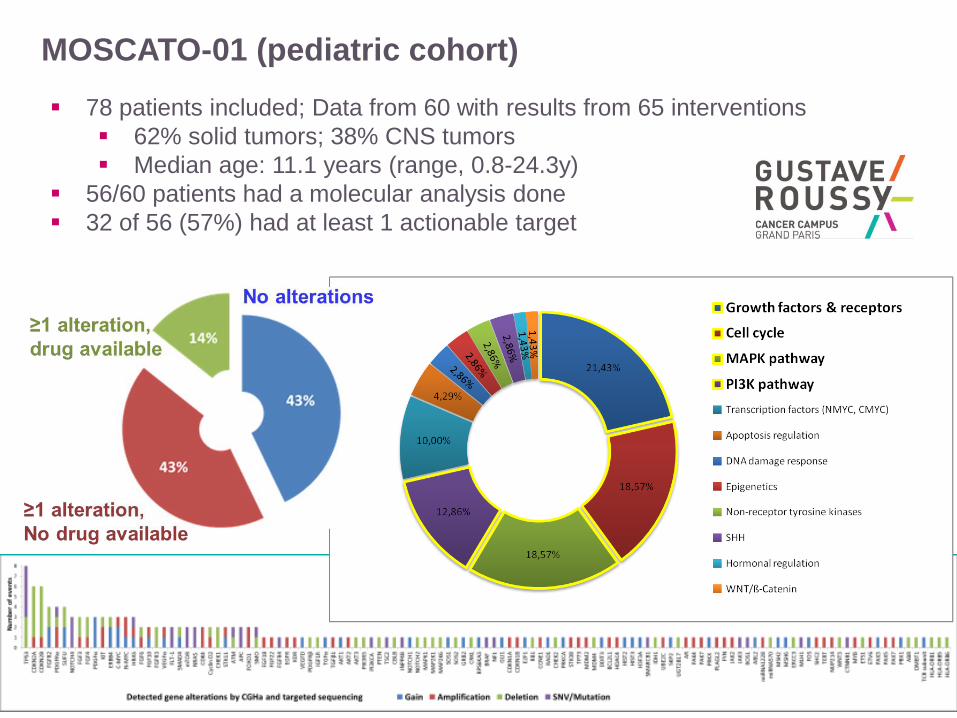
78 patients included; Data from 60 with results from 65 interventions
62% solid tumors; 38% CNS tumors
Median age: 11.1 years (range, 0.8-24.3y)
56/60 patients had a molecular analysis done
32 of 56 (57%) had at least 1 actionable target
MOSCATO-01 (pediatric cohort)
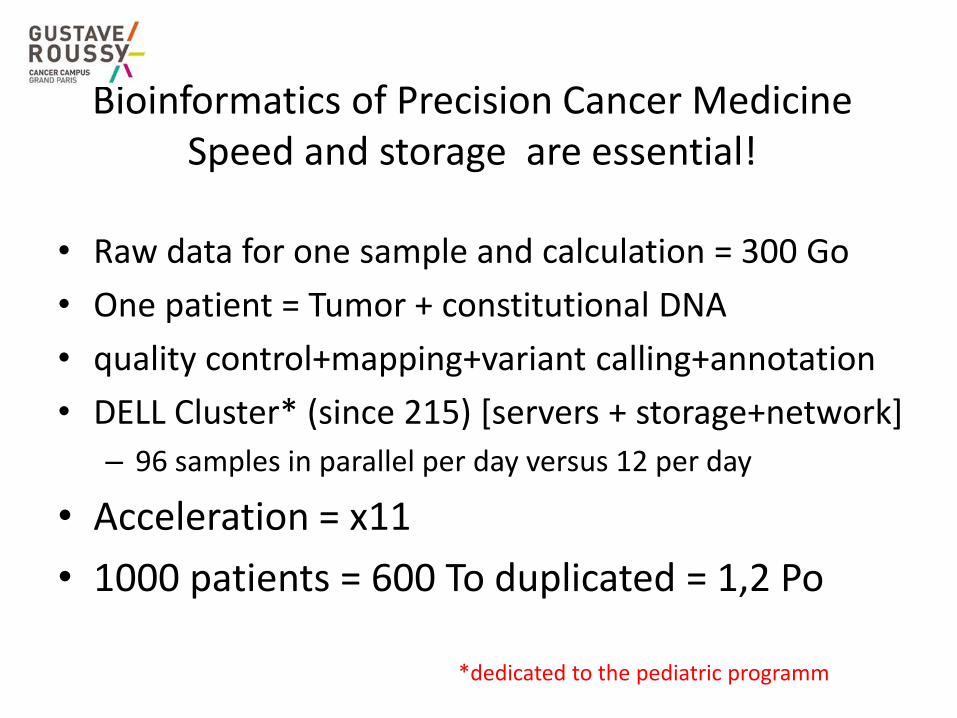
Bioinformatics of Precision Cancer MedicineSpeed and storage are essential!
• Raw data for one sample and calculation = 300 Go
• One patient = Tumor + constitutional DNA
• quality control+mapping+variant calling+annotation
• DELL Cluster* (since 215) [servers + storage+network]
– 96 samples in parallel per day versus 12 per day
• Acceleration = x11
• 1000 patients = 600 To duplicated = 1,2 Po
*dedicated to the pediatric programm
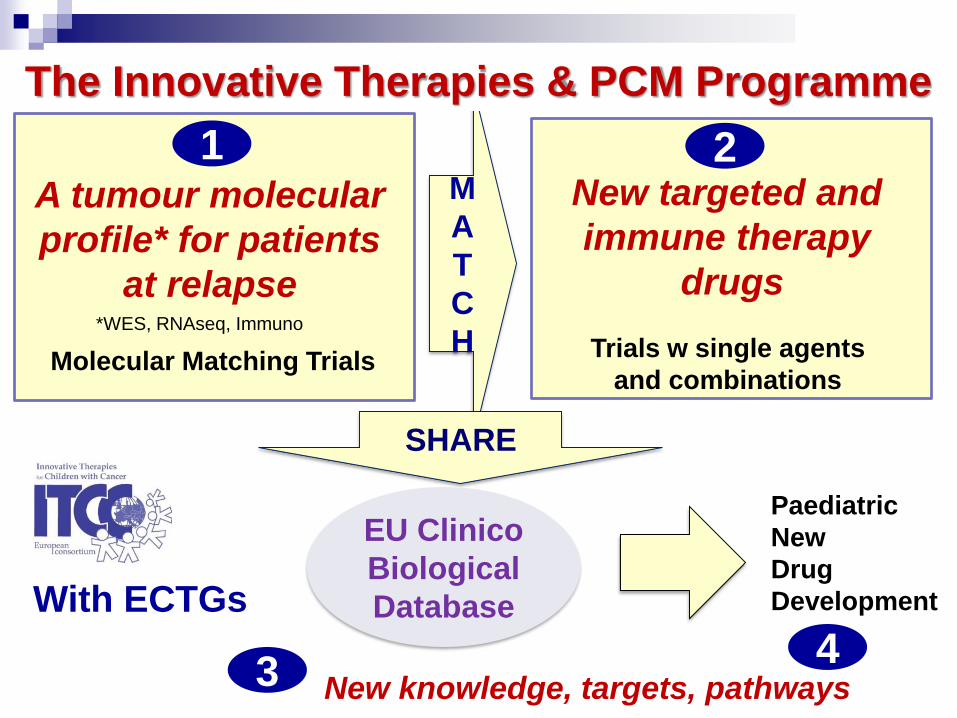
M
A
T
C
H
SHARE
With ECTGs
The Innovative Therapies & PCM Programme
EU Clinico
Biological
Database
New knowledge, targets, pathways 3
Paediatric
New
Drug
Development
4
New targeted and
immune therapy
drugs
2
Trials w single agents
and combinations
A tumour molecular
profile* for patients
at relapse
Molecular Matching Trials
1
*WES, RNAseq, Immuno
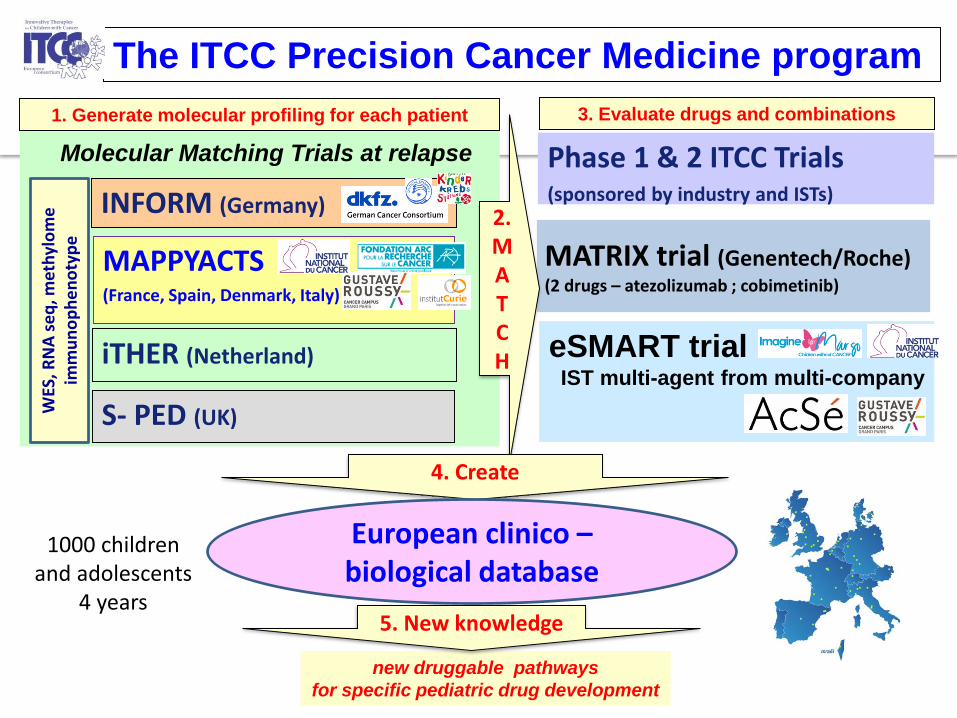
MATRIX trial (Genentech/Roche)(2 drugs – atezolizumab ; cobimetinib)
MAPPYACTS (France, Spain, Denmark, Italy)
1. Generate molecular profiling for each patient
2.MATCH
4. Create
new druggable pathways
for specific pediatric drug development
INFORM (Germany)
iTHER (Netherland)
S- PED (UK)
The ITCC Precision Cancer Medicine program
Molecular Matching Trials at relapse
eSMART trialIST multi-agent from multi-company
Phase 1 & 2 ITCC Trials(sponsored by industry and ISTs)
3. Evaluate drugs and combinations
European clinico –biological database
5. New knowledge
WES
, RN
A s
eq
, met
hyl
om
eim
mu
no
ph
en
oty
pe
1000 childrenand adolescents
4 years

Projet National MAPPYACTS
ON-PURPOSE FRESH TUMOR BIOPSY/SURGERY & PATHOLOGY CONTROL
MOLECULAR PROFILING(CGH & NGS)
MOLECULARTUMOR BOARD
TREATMENTBiopsie à la
rechutePortrait Moléculaire
Tumoral (WES/RNAseq)
RCP moléculaire Traitement
RCP
moléculaire
Enfant et adolescent, en rechute, tumeur solide et leucémie
MoleculAr Profiling for Pediatric and Young Adult Cancer Treatment Stratification
300 enfants en 3 ans
PHRC 2015
Fondation ARC
Ouverture décembre 2015
PI B Geoerger
RCP
Nationale
Children and their parentsneed to travel to investigating centersto access early innovation

A multistakehoder platform(Academia, Parents, Industry, Regulatory)
Vassal, Eur J Cancer, 2015, 51, 218

Precision Cancer Medicine Programm
Thanks to the patients and their family
Thanks to: