pre pregnancy care
TRANSCRIPT
+
PRE PREGNANCY CARE (PPC)
DR ALIFAH MOHD ZIZI
KAPIT O&G UPDATES
+DEFINITION…
Identify and modify biomedical,
behavioural and social risks to a
woman health or pregnancy through
prevention and management
+GOALS….
1. Help the mother to maintain her well-being
2. Obstetrician & physician have ultimate time to
assess, manage and treat many conditions or
complications before conception
3. Help the mother to achieve a healthy outcome
for herself & also her unborn fetus
4. Reduce maternal or neonatal morbidity and
mortality
+COMPONENTS…
1. Identification of pregnancy related risks
2. Patient’s education and informed choice regarding pregnancy risks, management options and reproductive alternative
3. Identifying couples who are at increased risk of having babies with a genetic malformation.
4. Initiation of interventions, when possible to provide optimum pregnancy outcome
5. Women and their partners being encouraged to prepare actively for pregnancy, and be as healthy as possible
+WHO????
Any women who wish to embark on
pregnancy, especially those who are at
risk
+WHEN??
Anytime… OR
At least 3 months before getting pregnant
+WHAT TO EXPECT ??
1.Complete history- medical, surgical, drug,
family history, social
2.Physical examination
3.Laboratory investigations
+Pre-pregnancy Counselling
Age related risk
Body Weight (BMI)
Chronic diseases
Infections (STIs)
Medication review
Immunisation status (Rubella)
Genetic counselling
Diet
Exercise
Smoking
Alcohol
Elicit drug abuse
Psychosocial –relationship/stress/ financial/mental health
+ AGE- RELATED RISKS
Most pregnancies are uneventful and have a good outcome
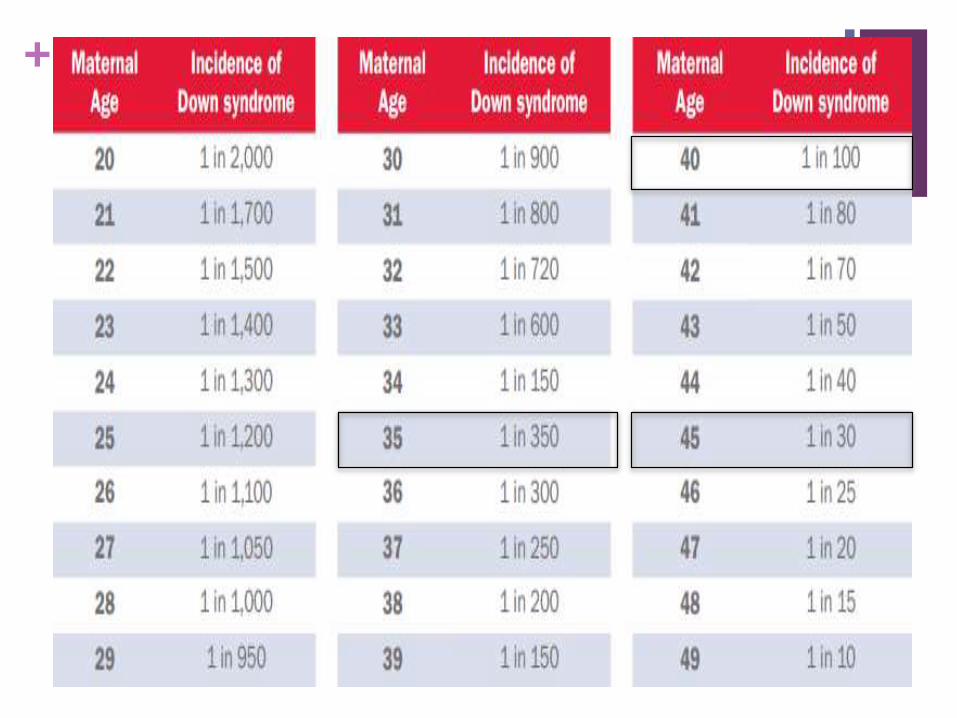
The risk of fetal chromosomal abnormalities, particularly trisomy 21 (Down's syndrome) increases sharply with maternal age
There is also an increased risk of infertility, miscarriage, twins, fibroids, hypertension, gestational diabetes, labour problems, and perinatal mortality with increasing maternal age.
+
+
Teenage pregnancy also associated with
1.Nutritional issue
2.Anaemia / Hypertension
3.Emotional
4.Social issue
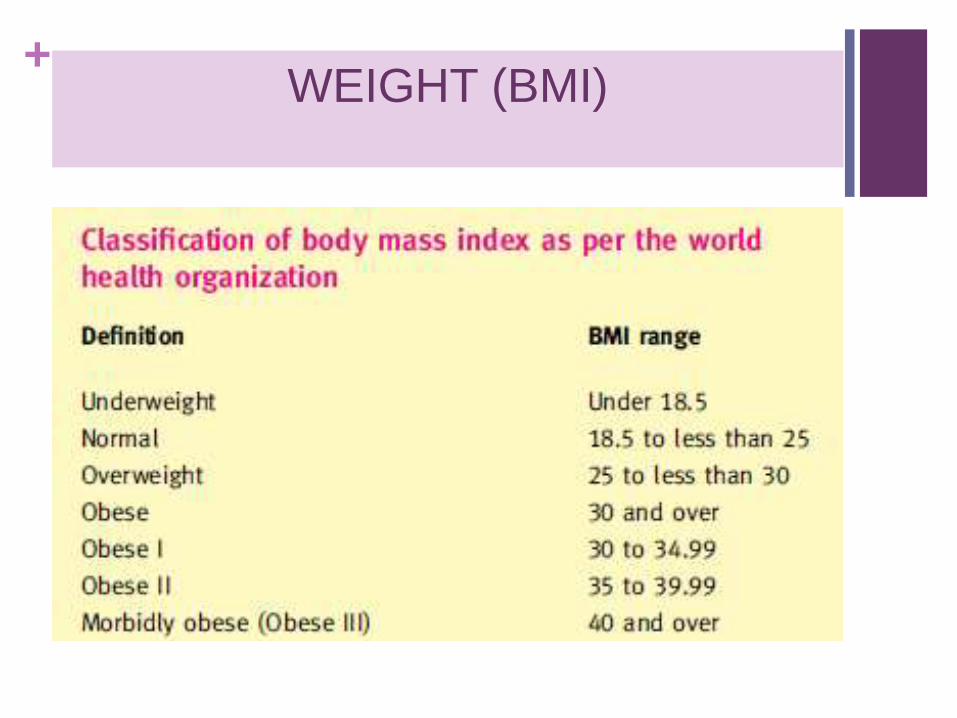
+WEIGHT (BMI)
+ A healthy weight reduces the risk of
Infertility
Neural Tube Defect (NTD)
Miscarriage
Preterm delivery
Gestational diabetes
Hypertension
Thromboembolic disease
Caesarean delivery & intrapartum complication
Consultation with a dietician may be helpful
Aim to reduce weight to normal BMI.
+CHRONIC DISEASES
Many chronic diseases and their
treatments may have implications
for fetal health and development
Similarly pregnancy and labour
may worsen pre-existing maternal
conditions

+
Heart Disease
Chronic HPT
DM
Epilepsy
Thyroid Disease
Connective Tissue Disease
Mental Health Illness
Infection
+1. Chronic Hypertension
Woman with chronic hypertension may have
impact on the pregnancy (eg Pre- eclampsia,
IUGR or worsening of any end organ
damage)
Aims
1.To ensure BP stable
2.To identify if any complication (end organ)
3.To adjust anti-hypertensive to a safer choice
Women should take 75 mg aspirin from 12
weeks' gestation to delivery
+ STOP!!
1) Angiotensin-
converting enzyme
(ACE) inhibitors or
angiotensin-II
receptor blocker
(ARB)
2) Chlorothiazide
-Increased risk of
congenital abnormalities
Drugs of choice
Methyldopa
Labetolol
Nifedipine
+2. Diabetes Mellitus
Aims..
Ensure good control of blood
sugar
HbA1c < 7%
Reduce Weight
Screen for complications
Baseline Renal Function
Opthalmologist referral
+ Impact of Pregnancy to DM
-Worsening retinopathy and nephropathy
-Difficulty in controlling blood sugar
Impact of DM to pregnancy
- MOTHER- PE, Intrapartum complications, Operative morbidity, PPH
- FETUS- Miscarriage, congenital malformations, stillbirth and neonatal death, macrosomia, polyhydramnions, shoulder dystocia,
Convert OHA to insulin
Metformin safe to be used in pregnancy
Folic acid 5mg a day should be started to reduce the risk of child having neural tube defect
+3.Heart Disease
All women with congenital or acquired heart disease
should discuss future pregnancies with a cardiologist
and obstetrician
Need detail assessment of cardiac status (ECHO)
The ability to tolerate pregnancy is related to
1.Presence of pulmonary hypertension
2.Haemodynamic significant of any lession
3.Functional class (NYHA)
4.Presence of cyanosis (Spo2 <80%)
+ Pregnancy is contra-indicated
1) Pulmonary hypertension
2) Marfan's syndrome with a dilated aortic root
3) Severe aortic or mitral valve stenosis
4) Any patient with poor ventricular function
5) Eisenmenger’s syndrome
HIGH MORTALITY
1.Eisenmenger's syndrome or cardiomegaly
- mortality may be as high as 25% to 50%.
2.Primary pulmonary hypertension and cyanotic disease
-maternal mortality of 50%
+ If the woman takes warfarin, this
should be converted LMWH
Those with rheumatic heart
disease should continue their
penicillin
Angiotensin-converting enzyme
(ACE) inhibitors and angiotensin
receptor blocker (ARB) are both
severely teratogenic.
Statins are contra-indicated in
pregnancy .
+4.Epilepsy
Referral for Neuromedical specialist before conception to reduce or
change drug treatment if possible
Assess fit free period (preferably 6 months – 1 year)
More concern on the effect of AED (anti-epileptic drugs to developing
fetus)
Counsel about the balance between the possible harm done by
medication compared with against the risk of developing seizure in
pregnancy
+AEDs (anti-epileptic drugs)
Phenytoin, phenobarbitone, carbamazepine, sodium
valproate, lamotrigine, Keppra (Levetiracetam) all
cross placenta and teratogenic
The risk increases if using sodium valproate and
also with the number of drugs use (polytheraphy)
MAJOR ABNORMALITY MINOR ABNORMALITY
-Neural tube defect
-Orofacial cleft
-Congenital heart defects
-Dysmorphic features
-Hypoplastic nails
+ Use monotheraphy if possible
DO NOT CHANGE the drugs if the epilepsy well controlled
with that particular medication
Recommend folic acid 5 mg per day before conception and
up to 12 weeks following conception
Arrange for detail scan during 2nd trimester
Educate family members regarding care if patient
develop seizure
+5.Thyroid Disease
Check TFTs if not done in the last 6 months
Need to liase with ENDOCRINOLOGIST
Those with subclinical hypothyroidism, should commence
treatment
Those on treatment for hypothyroidism, should be reviewed to
ensure optimum control. The requirement for thyroid
replacement therapy increases in pregnancy.
Hyperthyroid individuals should be reviewed and may wish to
consider treatment with radio-active iodine or surgery prior to
pregnancy.
Need to assess for any complications from the thyroid disease
+
Impact on the disease to pregnancy
-THYROTOXICOSIS- miscarriage, IUGR, thyroid
storm
-HYPOTHYROID- miscarriage, IUGR, neonatal
kernicterus
Carbimazole, PTU and thyroxine are safe in
pregnancy
If underwent RAI (radio-iodine ablation) need to
delay pregnancy at least 1 year
+6.Infections (STIs)
Includes – HIV, Hepatitis B, Herpes, Genital warts,
Syphillis
Any active sexually transmitted illness (STIs) are not
advice for pregnancy
Need to liase with ID physician (infectious disease)
or GUM (genito-urinary medicine) specialist for
treatment before embark on pregnancy
Risk of transmission to the developing fetus if
untreated
+MEDICATION REVIEWS
It is good practice to minimise exposure to all drugs, including those bought over the counter
There is little data on herbal preparations in pregnancy, and they should also be avoided
+IMMUNISATION STATUS
Ensure that the immunisation status (esp Rubella) is
up to date
Those who is never vaccinated is succeptible for
Rubella infection in pregnancy and will put baby at
risk of Congenital Rubella Syndrome (cataract,
deafness, heart, lung, brain anomalies)
Live vaccine should be given more than 1 month
before embark to pregnancy
+GENETIC COUNSELLING
This is recommended for those
1) Who have had a previous child with an inherited disease such as Down's syndrome or cystic fibrosis
2) Have a family history of a genetic disorder.
Couples need to know what the risk of having an affected child is and whether screening, genetic testing, pre-natal or pre-implantation is available.
+NUTRITION
In healthy women on a normal diet, advice on
eating 5 portions of fruit and vegetables per
day and consuming dairy products to raise
stores of vitamins, iron and calcium is
reasonable.
Dietary changes to optimise growth and
development
Vegetarian diets lack adequate amounts of
amino acid, iron, vitamin B12, complex lipids
+SMOKING & ALCOHOL
Smoking in pregnancy :
Intrauterine growth retardation
Miscarriage and stillbirth
Premature delivery
Placental problems
Fetal alcohol syndrome- facial anomalies, mental
retardation, behavioural problems
Smoking & alcohol cessation during pregnancy will improve pregnancy outcome
+ILLICIT DRUGS
Advise to stop using illicit drugs if
a pregnancy is desired
Offer referral where the woman
is planning a pregnancy and is
unable to stop using without
support
Methadone clinic
+CAFFEINE
Limit 300mg/day
Consumption of > 250mg/day can decrease fertility
>500mg/day increase miscarriage, stillbirth, IUGR
+ENVIRONMENTAL EXPOSURE
Avoid organic solvents
Mercury associated with ADHD
Lead miscarriage, stillbirth, IUGR, premature birth
Work place environment
+EXERCISE
Mild to moderate exercise while pregnant is not
harmful if done on a regular basis prior to pregnancy
Do not initiate strenous exercise regime during
pregnancy
Low impact routine
+PSYCHOSOCIAL
Assess marital or relationship status
Any stressor – financial, support (may need social
worker involvement)
Any mental health need to liase with psychiatric
team

THANK YOU
!