pragmatic communication deficits in children with epilepsy
TRANSCRIPT
Research Report
Pragmatic communication deficits in children with epilepsy
Mark Broeders†, Hilde Geurts† and Aag Jennekens-Schinkel‡§
†Psychonomics, University of Amsterdam, Amsterdam, the Netherlands‡Child Neurology, University Medical Centre, Utrecht, the Netherlands§Rudolf Magnus Institute of Neuroscience, Utrecht, the Netherlands
(Received January 2009; accepted September 2009)
Abstract
Background: Various psychiatric and neurological disorders including epilepsy have been associated with languagedeficits. Pragmatic language deficits, however, have seldom been the focus of earlier studies in children with epilepsy.Moreover, it is unknown whether these pragmatic deficits are related to general intellectual functioning. Both issueswill be addressed in this study.Aims: 1) Explore pragmatic language deficits in children with epilepsy while controlling for having a neurologicalillness and having to visit a tertiary paediatric hospital regularly, and 2) Determine whether pragmatic difficulties, ifpresent, are discrete or associated with general intellectual functioning.Methods & Procedures: The Children’s Communication Checklist (CCC), a pragmatic language questionnaire,created by D. V. M. Bishop in 1998, was filled out by parents of 30 children with epilepsy (mean age ¼ 10 years),30 age-matched children with various neurological disorders other than epilepsy, and 30 age-matched typicallydeveloping controls. The full-scale intelligence quotient (FSIQ) was individually measured to estimate the children’slevel of overall intelligence. The clinical groups were assessed in a tertiary paediatric hospital.Outcomes & Results: The pragmatic composite score distinguished between the two neurologically impaired groups,even after controlling for FSIQ. Of children with epilepsy, 23% had pragmatic deficits, whereas only 3% of thechildren with various other neurological disorders and none of the typically developing children had these deficits.When compared scale by scale with typically developing children, children in both clinical groups showed morestructural language problems and problems of language use, but these differences disappeared when FSIQ wascontrolled for.Conclusions & Implications: Pragmatic deficits in communication are present in children treated for variousneurological impairments, but more so in children whose seizures necessitate referral to a tertiary hospital. Cliniciansshould be sensitive to and inquire after pragmatic aspects of communication. Additional research is needed toelucidate mechanisms underlying these deficits.
Keywords: children, epilepsy, language, pragmatics, communication.
What this paper addsWhat we already known on the subjectPragmatic deficits in communication are a feature of a wide range of neurodevelopmental and psychiatric disorders.The Children’s Communication Checklist (CCC) is particularly suitable to screen children for communicationproblems in general and for pragmatic deficits in particular. Thus far, only two studies applied the CCC in studiesof children with epilepsy, but the results are inconclusive.
What the paper addsChildren with various neurological disorders have a pragmatic deficit, as shown by the easily applicable CCC. Thesedeficits are more frequent and more pronounced in children with epilepsy. Intelligence level is related to problemsof communication rather than pragmatics per se.
International Journal of Language & Communication DisordersISSN 1368-2822 print/ISSN 1460-6984 online q 2010 Royal College of Speech & Language Therapists
http://www.informahealthcare.com
DOI: 10.3109/13682820903374246
Address correspondence to: Mark Broeders, Psychonomics, University of Amsterdam, Roetersstraat 15, 1018WB, Amsterdam, the Netherlands;e-mail: [email protected]
INT. J. LANG. COMM. DIS., SEPTEMBER–OCTOBER 2010,VOL. 45, NO. 5, 608–616

Introduction
Communication disorders encompass a wide range ofdeficits such as limited vocabulary, shortened utter-ances, simplified grammatical structures, limitedvarieties of grammatical structures, impaired narrativeskills, and stereotyped language (American PsychiatricAssociation 2000). Language disorders typically consistof deficits in the structural components of language,that is, syntax, semantics, phonology, and morphology.Communication disorders, affecting the speech acts orthe interaction between speaker and listener, transcenddeficits in these structural components (Bara et al.1999, Martin and McDonald 2003). Crucial foreffective communication is, among others, the ability toadapt language utterances to the listener, the context,and the situation (Bishop and Baird 2001). The notionof pragmatic language refers to these intricatecommunicative adaptations.
Deficits in pragmatic language are present in a widerange of psychiatric disorders such as autism andattention deficit hyperactivity disorder (for example,Bishop and Baird 2001, Geurts et al. 2004, and Peppeet al. 2006). Neurological disorders such as right-hemisphere damage have also been associated withdeficits in pragmatics (Cheang and Pell 2006).Abnormalities of language structure and, more recently,deficits of pragmatics have been suggested to be featuresof many children with epilepsy (Caplan et al. 2002,Cohen and Le Normand 1998, Parkinson 2006, Rejno-Habte Selassie et al. 2008, Schoenfeld et al. 1999).Nonetheless, the findings on pragmatics in languageuse of children with epilepsy have been inconsistent.This may be explained by at least four methodologicaldifferences between the studies.
A first issue involves the confounding effect of co-morbidity. For instance, in a study addressingpragmatic functioning in children with varioussubtypes of epilepsy by Parkinson (2006), all childrenshowed autistic traits, autism or autistic regression.Since one of the key characteristics of autism is thepragmatic deficits (for example, Bishop and Baird2001, and Geurts et al. 2004), it is conceivable thatpragmatic abnormalities as reported in this study can beaccounted for by autism or autistic features. Hence, it isimportant that in studies of children with epilepsy,either those children with an additional diagnosis ofautism are excluded or that autism is controlled for.As reported in a letter to the editor, the exploratorystudy by Lew et al. (2006) suggested that children withfocal probably symptomatic epilepsy have deficits invarious aspects of communication, including prag-matics. Since none of the children in this samplesuffered from co-morbid disorders such as autism, thepragmatic difficulties as described by Parkinson (2006)
in children with epilepsy cannot be fully explained byautism, which implies that other explanations areneeded to account for the inconsistent findings.
A second issue is that general intellectual function-ing might be a confounding variable in previous studies.The pragmatic deficits described by Parkinson (2006)were found in children with epilepsy who besides thepresence of autistic features also had low non-verbalintelligence levels (below 70). Unfortunately, the studyby Lew et al. (2006) does not report intelligencequotients (IQ). In the most recent and largest study todate, Rejno-Habte Selassie et al. (2008) did not find anypragmatic language difficulties in pre-schoolers withvarious types of epilepsy but without neuro-impair-ments. Importantly, all the participants in this studyhad normal to high IQ (above 70). Hence, anotherpossible explanation for the inconsistent results is thatIQ might be related to pragmatic language use. Earlierstudies of children have suggested an associationbetween lower IQ and more difficulties in bothlanguage structure and pragmatics (for example,Conrad 1972, and Hatton 1998). Therefore, IQshould be taken into account when studying pragmaticlanguage use in children with epilepsy, preferably anindex such as full-scale (FS) IQ that covers both fluidand crystallized aspects of cognition. Moreover, FSIQincludes verbal intelligence and therefore it automati-cally corrects for poor verbal functioning.
A third methodological issue is that the researchtools adopted do not always measure pragmaticlanguage. Caplan et al. (2002) for instance, basedtheir finding of communication deficits in children withvarious types of epilepsy on the application of aninstrument that measured formal thought disorder.As the problems inventoried with that instrumentresembled pragmatic language problems, they inter-preted their findings in terms of communication.Nonetheless, even when more suitable instruments wereused, results with respect to the presence or absence ofpragmatic language deficits remained (for example, Lewet al. 2006, Parkinson 2006, and Rejno-Habte Selassieet al. 2008). Most tests of pragmatic languagefunctioning in children have been developed to assessthe child itself (for example, Adams and Lloyd 2005,Hyter 2007, and Russell and Grizzle 2008). Suchprocedures yield detailed knowledge, but are timeconsuming and often exceed situational facilities. Incase of disease they, moreover, might easily exceed thechild’s performance potential. For these reasons,instruments have been developed that allow one toinventory indirectly pragmatic skills quickly andreliably. One such instrument, to be filled out byparents or clinicians, is the Children’s CommunicationChecklist (CCC; Bishop 1998). This questionnaireenables one to differentiate between children who
Pragmatic deficits in children with epilepsy 609

encounter difficulties with pragmatic language use andthose who encounter difficulties with languagestructure. Studies applying the CCC have shown thatthis is a valid instrument to measure both languagestructure and pragmatic language use (for example,Bishop 1998, Bishop and Baird 2001, Geurts et al.2004, Gilmour et al. 2004, and Norbury et al. 2004).The CCC is widely used in clinical practice. To ourknowledge, only two studies previously applied theCCC or the more recent CCC-2 (Bishop 2003) inchildren with epilepsy (Lew et al. 2006, Rejno-HabteSelassie et al. 2008). However, while Lew et al. (2006)did report deficits in children with epilepsy, Rejno-Habte Selassie et al. (2008) could not confirm thesedeficits in their selection of non-autistic children withepilepsy who had IQ greater than 70. Hence, even instudies that used the same tool to measure pragmaticlanguage inconsistent findings emerged.
A fourth methodological issue pertains to age.Rejno-Habte Selassie et al. (2008) studied pre-schoolersin the narrow age range of 6–7 years while age rangedbetween 4 and 16 years in the study of Lew et al.(2006). Since pre-schoolers show structural languagedeficits (Rejno-Habte Selassie et al. 2008), it could wellbe that in children with a younger age structural deficitsare more noticeable than pragmatics, while at an olderage the pragmatics deficits are easier to observe forparents. This idea was recently put forward by Geurtsand Embrechts (2008) as a similar pattern of findingswas obtained in individuals with autism. Pre-schoolersand schoolchildren with autism were challenged onboth language structure and pragmatic language use,but parents reported relatively more structural languagedeficits (on the CCC-2) in pre-schoolers, while inschoolchildren the pragmatic language deficits weremore prominent. Thus, the presence of associateddisorders, general intelligence levels of the participants,differences in research tools, and the age of theparticipants might each have contributed to thedifferent findings regarding pragmatic language inindividuals with epilepsy.
In the current study we examine language structureand language use of non-autistic children with epilepsy,and compare this to the language structure andlanguage use of age-matched typically developingchildren and children with various neurologicaldisorders but without epilepsy. Our major aim is toexplore pragmatic language deficits in children withepilepsy. If pragmatic deficits are indeed present inchildren older than six years of age with epilepsy (Lewet al. 2006), we would expect lower CCC ratings, thatis, poorer pragmatics, for children with epilepsy thanfor typically developing controls. As inconsistencies inearlier pragmatics-related findings in children withepilepsy might be due to IQ, we will study whether
pragmatic difficulties, if present, are discrete orassociated with general intellectual functioning asassessed by FSIQ. Finally, by comparing the epilepsygroup with a group of children with variousneurological disorders but no epilepsy, we aim tocontrol for having a neurological illness and having tovisit a paediatric ward of a tertiary paediatric hospitalregularly. This latter control group is relevant as onemight argue that the stress associated with this, and alsothe exceptional position these children are in, mighthave an effect on their social–emotional development(Boekaerts and Roder 1999) and perhaps even on theircommunicative skills.
Methods
The study was approved by the Ethical committee ofthe Psychology Department of the University ofAmsterdam. The Medical Ethics Committee of theUniversity Medical Centre Utrecht (UMCU) ruled thatthe protocol did not require examination within theframework of the Medical Research Act.
Patients and typically developing peers
All data with respect to patients were obtained in theSector of Neuropsychology of the WilhelminaChildren’s Hospital (UMCU), a tertiary hospitalwhere children with pharmacologically intractableepilepsies are referred to, because of its affiliation tothe Dutch Collaborative Epilepsy Surgery Programme.The children underwent a comprehensive assessment togather functional status information, which wasrequested by the child neurologists. Between 2002and 2006, parents of 207 consecutive patients filled outthe CCC as a regular part of the neuropsychologicalassessment. Information obtained from their medicalcharts enabled the authors to form two clinical groups:an epilepsy group and a non-epilepsy neurologicalcomparison group.
Inclusion criteria for the epilepsy group were: (1)unambiguous diagnosis of non-symptomatic epilepsy,(2) no prior brain surgery and (3) no additionalbehavioural (including autism spectrum) disorders.This resulted in an epilepsy group (EPI) of 30 children(mean age ¼ 10 years, 0 months, SD ¼ 2.38; 18 boys,twelve girls). Epilepsy types were simple partial epilepsy(n ¼ 4), complex partial epilepsy (n ¼ 20), andgeneralized epilepsy (n ¼ 6). The mean age of onsetof epilepsy was 5 years, 6 months (SD ¼ 3.64).
The non-epilepsy neurological comparison group(non-EPI) consisted of 92 children with variousneurological conditions. We selected 30 childrenwhose age matched with that of the EPI children(mean age ¼ 9 years, 5 months, SD ¼ 2.27; 22 boys,
610 Mark Broeders et al.

eight girls). This non-EPI group consisted of childrensuffering from a broad spectrum of acquired anddevelopmental neurological disorders: cerebral tumour(n ¼ 7), closed head injury (n ¼ 5), neurofibromatosistype 1 (n ¼ 3), hydrocephalus (n ¼ 2), metabolicdisorder (n ¼ 2), and various other neurologicaldisorders, ranging from encephalitis to sinovenousthrombosis (n ¼ 11).
A typically developing (TD) control group wascomposed of a selection of 30 (mean age ¼ 9 years,7 months, SD ¼ 1.51; 18 boys, twelve girls) Dutchchildren who had participated in a previous study, inwhich CCC parent reports had been gathered for 90 TDchildren across the Netherlands and Belgium (Geurtset al. 2004). None of the TD children ever hadproblems at school or suffered from neurodevelop-mental disorders.
Materials and procedures
Parents or caretakers of the children completed theCCC (Bishop 1998). This questionnaire had beentranslated from English to Dutch in a two-waytranslation procedure (Hartman et al. 1998). TheDutch CCC consists of 70 questions, divided into ninescales. Two scales refer to language structure, that is,Speech production (A) and complexity of Syntax (B).Five scales (C–G) inventory pragmatic use of language.The remaining two scales, Social relationships (H) andSpecific Interests (I), are intended to gather informationon autistic features that are not directly related tocommunication. Answers are given on a three-pointscale (does not apply ¼ 0, applies somewhat ¼ 1,definitely applies ¼ 2, and unable to judge ¼ missingvalue). Table 1 shows the CCC scales with exampleitems, the ranges of possible scale scores and thenumber of items per scale. The scores are summated for
each scale. A pragmatic composite score can becalculated by adding the scores of the scales C–G.Bishop (1998) suggested a cut-off score of 132 for thepragmatic composite score1, as this cut-off provided thebest discrimination between children with languagestructure difficulties and those with pragmatic languagedifficulties. For each scale and the pragmatic compositea lower score implies more difficulties. Reliabilitymeasures (Cronbach’s a) for the Dutch CCC varybetween 0.55 (Interests) and 0.86 (Coherence) in aclinical sample, with an internal consistency of 0.83 forthe pragmatic composite score. The reliability measuresfor Dutch TD children vary between 0.02 (Syntax) and0.68 (Stereotyped Conversation and InappropriateConversation) with an internal consistency score of0.76 for the overall pragmatic score (Geurts et al. 2005,2008).
An intelligence test was administered to all childrenat the time when the parents filled out the CCC. Inboth clinical groups, test selection depended on the ageand clinical condition of the child, for example,Wechsler Pre-school and Primary Scale of Intelli-gence—Revized (WPPSI-R), Snijders–Oomen Non-Verbal Intelligence Test (SON), McCarthy Develop-mental Scales (MOS), and Wechsler Intelligence Scalefor Children—Revized (WISC-R). The FSIQ of thechildren in the TD control group was estimated on thebasis of a short version of the WISC-R (for details, seeGeurts et al. 2004).
Statistical analyses
The statistical analyses were performed in SPSS 12.0.All analyses were performed with a significance level ofa ¼ 0.05 (two-tailed). We compared the groups withrespect to age and IQ with a one-way analysis ofvariance (ANOVA). Differences between groups with
Table 1. Children’s Communication Checklist (CCC) scales with ranges of possible scale scores, number of items, and example itemof each scale
CCC scale RangeNumberof items Example item
(A) Speech Output 16–38 11 People can understand virtually everything he/she says(B) Syntax 24–32 4 Speech is mostly two- to three-word phrases such as ‘me got ball’ or ‘give dolly’(C) Inappropriate Initiation 18–30 6 Talks to anyone and everyone(D) Coherence 20–36 8 Can give an easy-to-follow account of a past event such as a birthday party or a
holiday(E) Stereotyped Conversation 14–30 8 Pronounces words in an over-precise manner: accent may sound rather affected
or ‘put on’, as if the child is mimicking a television personality rather thantalking like those around him/her
(F) Use of Conversational Context 16–32 8 Tends to repeat back what others have just said(G) Conversational Rapport 18–34 8 Ignores conversational overtures from others (for example, if asked ‘What are
you making?’ just continues working as if nothing had happened)(H) Social Relationships 14–34 10 Is popular with other children(I) Interests 20–34 7 Uses sophisticated or unusual words; for example, if asked for animal names
might say ‘aardvark’ or ‘tapir’
Pragmatic deficits in children with epilepsy 611
respect to gender were analysed using a Chi-square (x 2)test. When significant differences were found betweenthe groups, these variables were entered as covariates inthe next analyses.
To identify pragmatic deficits in children withepilepsy, we focused on pragmatics by conducting anANOVA with the pragmatic composite score asdependent measure and group (EPI, non-EPI, andTD) as a between subject factor. This analysis wasrepeated with the exclusion of the Coherence scale fromthe pragmatic composite score as this scale mightmeasure language structure.1 Bonferroni-correctedpost-hoc analyses were carried out to investigate thenature of the potential main effect of group. Toestimate the occurrence of pragmatic difficulties, wecalculated the number of children who scored below thecut-off of 132 points on the pragmatic composite score(including the Coherence scale as this scale wasoriginally included in the pragmatic composite score) ineach group. A x 2-test determined whether thesenumbers differed significantly in the three groups.
We also explored the broader range of languageaspects in children with epilepsy and screened forpossible structural difficulties. To do so, a multivariateanalysis of variance (MANOVA) was performed withgroup as between-subjects factor (EPI, non-EPI, andTD) and the nine CCC scale scores as dependentvariables. A significant main effect of group wasfollowed up by Bonferroni-corrected post-hoc analysesto distinguish between the three groups.
Results
As expected, the groups differed neither with respectto age, F , 1, p . 0.05, nor to gender, x 2(2, n ¼90) ¼ 1.55, p . 0.05. Differences were found, how-ever, between the three groups in mean IQ, F (2, 89) ¼
19.22, p , 0.001. Post-hoc analyses showed that theEPI group had the lowest IQ (mean IQ ¼ 79.9,SD ¼ 19.77). The mean IQ of the non-EPI group( ¼ 91.8, SD ¼ 17.48) was lower than of the TDgroup ( ¼ 108.3, SD ¼ 16.07) but significantly higherthan of the EPI group. In the EPI group, 71% of thechildren used multiple anti-epilepsy drugs (AED), 25%were on monotherapy and 4% were medication free.
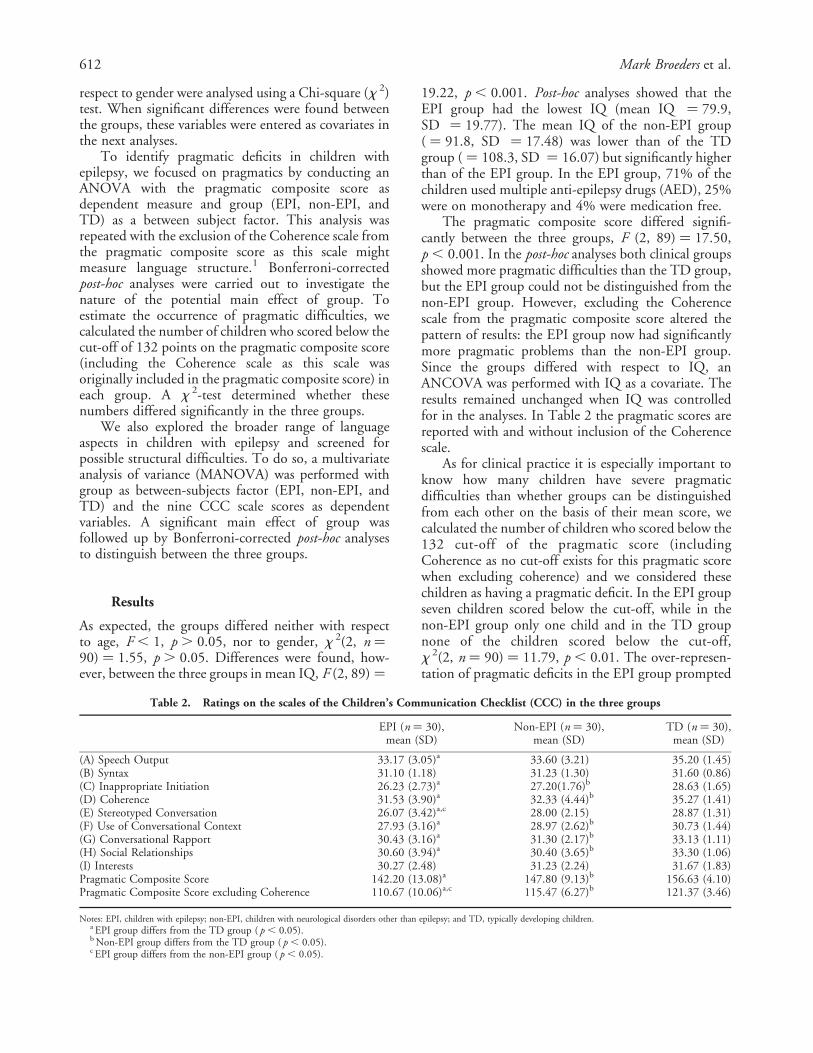
The pragmatic composite score differed signifi-cantly between the three groups, F (2, 89) ¼ 17.50,p , 0.001. In the post-hoc analyses both clinical groupsshowed more pragmatic difficulties than the TD group,but the EPI group could not be distinguished from thenon-EPI group. However, excluding the Coherencescale from the pragmatic composite score altered thepattern of results: the EPI group now had significantlymore pragmatic problems than the non-EPI group.Since the groups differed with respect to IQ, anANCOVA was performed with IQ as a covariate. Theresults remained unchanged when IQ was controlledfor in the analyses. In Table 2 the pragmatic scores arereported with and without inclusion of the Coherencescale.
As for clinical practice it is especially important toknow how many children have severe pragmaticdifficulties than whether groups can be distinguishedfrom each other on the basis of their mean score, wecalculated the number of children who scored below the132 cut-off of the pragmatic score (includingCoherence as no cut-off exists for this pragmatic scorewhen excluding coherence) and we considered thesechildren as having a pragmatic deficit. In the EPI groupseven children scored below the cut-off, while in thenon-EPI group only one child and in the TD groupnone of the children scored below the cut-off,x 2(2, n ¼ 90) ¼ 11.79, p , 0.01. The over-represen-tation of pragmatic deficits in the EPI group prompted
Table 2. Ratings on the scales of the Children’s Communication Checklist (CCC) in the three groups
EPI (n ¼ 30),mean (SD)
Non-EPI (n ¼ 30),mean (SD)
TD (n ¼ 30),mean (SD)
(A) Speech Output 33.17 (3.05)a 33.60 (3.21) 35.20 (1.45)(B) Syntax 31.10 (1.18) 31.23 (1.30) 31.60 (0.86)(C) Inappropriate Initiation 26.23 (2.73)a 27.20(1.76)b 28.63 (1.65)(D) Coherence 31.53 (3.90)a 32.33 (4.44)b 35.27 (1.41)(E) Stereotyped Conversation 26.07 (3.42)a,c 28.00 (2.15) 28.87 (1.31)(F) Use of Conversational Context 27.93 (3.16)a 28.97 (2.62)b 30.73 (1.44)(G) Conversational Rapport 30.43 (3.16)a 31.30 (2.17)b 33.13 (1.11)(H) Social Relationships 30.60 (3.94)a 30.40 (3.65)b 33.30 (1.06)(I) Interests 30.27 (2.48) 31.23 (2.24) 31.67 (1.83)Pragmatic Composite Score 142.20 (13.08)a 147.80 (9.13)b 156.63 (4.10)Pragmatic Composite Score excluding Coherence 110.67 (10.06)a,c 115.47 (6.27)b 121.37 (3.46)
Notes: EPI, children with epilepsy; non-EPI, children with neurological disorders other than epilepsy; and TD, typically developing children.a EPI group differs from the TD group ( p , 0.05).b Non-EPI group differs from the TD group ( p , 0.05).c EPI group differs from the non-EPI group ( p , 0.05).
612 Mark Broeders et al.
additional analyses to better describe the profile of thesechildren. First, separate t-tests with each CCCpragmatic scale as dependent variable and group(above the cut-off and below the cut-off) asindependent variable, show that children with a scorebelow the cut-off obtained significantly lower scores onall separate CCC pragmatic scales when compared tochildren with a score above the cut-off (all p’s , 0.05).Further, in the EPI group, children with a pragmaticdeficit had lower IQ’s than those with a pragmaticcomposite score above the cut-off, t (28) ¼ 2.102,p , 0.05. Due to the explorative nature of theseadditional analyses, we did not apply Bonferronicorrections (Rothman 1990). Moreover, all sevenchildren with a pragmatic deficit suffered from complexpartial seizures. The groups with a pragmatic compositescore above and below the cut-off did not differ withrespect to age and age of epilepsy onset. Exclusion of theseven low scoring children from the analyses did notalter the finding of more pragmatic difficulties in theEPI group. To explore a possible confounding effect ofAED, we divided the group of children with epilepsy intwo, mono- versus poly-therapy. Children who were onpoly-therapy obtained lower pragmatic compositescores than the children who were on mono-therapy,although this difference was marginally significant,t (25) ¼ 1.974, p ¼ 0.05. Moreover, all children with ascore below the cut-off were on multiple AEDs.
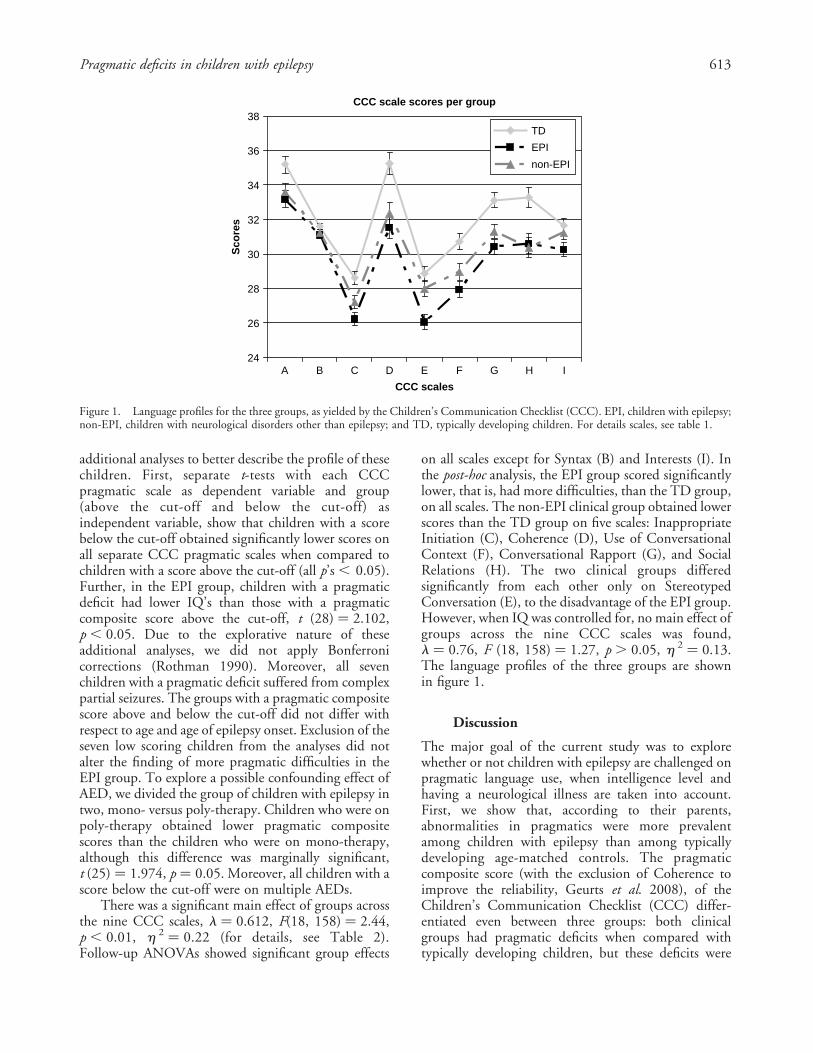
There was a significant main effect of groups acrossthe nine CCC scales, l ¼ 0.612, F(18, 158) ¼ 2.44,p , 0.01, h 2 ¼ 0.22 (for details, see Table 2).Follow-up ANOVAs showed significant group effects
on all scales except for Syntax (B) and Interests (I). Inthe post-hoc analysis, the EPI group scored significantlylower, that is, had more difficulties, than the TD group,on all scales. The non-EPI clinical group obtained lowerscores than the TD group on five scales: InappropriateInitiation (C), Coherence (D), Use of ConversationalContext (F), Conversational Rapport (G), and SocialRelations (H). The two clinical groups differedsignificantly from each other only on StereotypedConversation (E), to the disadvantage of the EPI group.However, when IQ was controlled for, no main effect ofgroups across the nine CCC scales was found,l ¼ 0.76, F (18, 158) ¼ 1.27, p . 0.05, h 2 ¼ 0.13.The language profiles of the three groups are shownin figure 1.
Discussion
The major goal of the current study was to explorewhether or not children with epilepsy are challenged onpragmatic language use, when intelligence level andhaving a neurological illness are taken into account.First, we show that, according to their parents,abnormalities in pragmatics were more prevalentamong children with epilepsy than among typicallydeveloping age-matched controls. The pragmaticcomposite score (with the exclusion of Coherence toimprove the reliability, Geurts et al. 2008), of theChildren’s Communication Checklist (CCC) differ-entiated even between three groups: both clinicalgroups had pragmatic deficits when compared withtypically developing children, but these deficits were
CCC scale scores per group
24
26
28
30
32
34
36
38
A B C D E F G H I
CCC scales
Sco
res
TD
EPI
non-EPI
Figure 1. Language profiles for the three groups, as yielded by the Children’s Communication Checklist (CCC). EPI, children with epilepsy;non-EPI, children with neurological disorders other than epilepsy; and TD, typically developing children. For details scales, see table 1.
Pragmatic deficits in children with epilepsy 613

slightly, but significantly, more profound in childrenwith epilepsy than in children with various otherneurological disorders. Second, when examining thescales separately, the CCC also differentiated betweenchildren with epilepsy and typically developing childrenon all scales except for Syntax and Interests. However,although the CCC revealed more stereotyped languageproblems in children with epilepsy than in childrenwith various other neurological disorders but withoutepilepsy, differences between the groups disappearedwhen we controlled for IQ. This shows that the deficitsof children with epilepsy on separate CCC scales asreported by Lew et al. (2006) might be confounded byIQ. Third, the pattern of language scores was highlysimilar in both clinical groups. However, the fact that23% of children with epilepsy showed pragmaticdeficits, as against 3% of the clinical group with variousneurological diseases but no epilepsy, suggests thatpragmatic language deficits are not rare in children withepilepsy, and also that the deficit is not solely due tohaving a chronic neurological disease and its associatedaversive effects (Boekaerts and Roder 1999).
As we hypothesized that pragmatic difficulties couldbe related to intelligence and since differences in IQwere found between the groups, we co-varied for IQ inour analyses. In keeping with a generally known trend,the IQ distribution of the present epilepsy group wasshifted to lower values (BjØrnaes et al. 2001, Dodrill2004). One might argue that the pragmatic deficitswere due to lower intelligence and indeed, when IQ wascontrolled for in the analyses, each separate scale nolonger reached statistical significance. Hence, thefindings on the separate scales, Stereotyped languagein particular (see above), might reflect the cognitivedisadvantage of the group with epilepsy. Clearly, thepresently reported effect of IQ may put into perspectivethe disadvantage in every CCC sub-scale, as reported byLew et al. (2006): intelligence affected communicativeefficiency or vice versa. Some of the previousinconsistent findings (for example, Lew et al. 2006,Parkinson 2006, and Rejno-Habte Selassie et al. 2008)might indeed be due to the differences in intelligencelevels of the participants across the studies.
In contrast to the individual scales, on thepragmatic composite score (both with and withoutthe Coherence scale), which is in general more reliablethan the scores on sub-scales (Bishop 1998, Geurts et al.2008), controlling for IQ did not alter the disadvantageof children with epilepsy and children with otherneurological disorders. It has to be noted that adifference on the pragmatic composite score betweenthe two clinical groups arose only when Coherence wasexcluded. Therefore, in children with a neurologicaldisorder, be it epilepsy or otherwise, communicationmay be hampered by a variable that is not covered by
IQ as an index of general intellectual functioning.Identification of this variable requires a comprehensiveassessment that is beyond the scope of the present study.It might have been worthwhile to compare the effects ofIQ components (for example, verbal versus non-verbalIQ), but by using the full-scale IQ score weautomatically correct for poor verbal functioning.Furthermore, the clinical setting of the study requiredthe use of tests that were adapted to the child’sperformance potential, resulting in IQ data from avariable set of intelligence tests of which thecomponents were not identical.
The results are greatly in line with those reported byLew et al. (2006), but not with those reported by Rejno-Habte Selassie et al. (2008). One possible explanationfor this difference might be that the majority of childrenwho participated in the latter study were younger thanthose who participated in the study by Lew et al. (2006)and our study. Geurts and Embrechts (2008) comparedlanguage profiles in pre-school children with autism andschool-aged children with autism using the CCC-2, andshowed these language profiles to be dissimilar. Besidespragmatic language deficiencies, all children withautism showed deficiencies in structural language aswell. However, while the structural language problemswere more prominent in the pre-schoolers (similar tothe study of Rejno-Habte Selassie et al. 2008), thepragmatic language problems were more prominent inthe older children. As a possible explanation for thisfinding, the authors hypothesized that parents of pre-schoolers might be more focused on structural languagedifficulties than on pragmatic problems. When childrengrow older, the focus may change and parents may bemore worried by pragmatic language difficulties. Thismay explain the different outcomes in the current studyand the study by Lew et al. (2006), and Rejno-HabteSelassie et al. (2008). However, to determine whetherthis is indeed the case a longitudinal study is needed toexplore whether the parents’ perspective is changing orwhether the language problems presented in thechildren are changing across development.
Having found that pragmatic abnormalities areunduly, but not generally, present in children with non-symptomatic, but difficult to treat epilepsy, the nextquestion is whether specific epilepsy variables identifythe subset of children with pragmatic languageabnormalities. Lew et al. (2006) found the differencesfrom non-clinical norms to be significant in the sub-group of children with focal epilepsies, whereas thegeneralized epilepsy subgroup varied from poor tosuperior, which may have concealed differences fromnon-clinical norms. We found only (but not all)children with complex partial epilepsy to score belowthe cut-off. These children had lower intelligence scoresthan the children with epilepsy who scored above the
614 Mark Broeders et al.

cut-off. All seven children with scores below the cut-offwere taking multiple AEDs. As children who encounterclear pragmatic language deficits may need additionalcare, the present findings can only highlight thenecessity to disentangle the complex of illness,treatment and environmental determinants of prag-matic competence in larger study. children.
There are limitations to our study. First, epilepsyfactors such as seizure frequency, seizure type,lateralization, and localization of epilepsy have notbeen taken into account. These factors may benegatively related to language and psychosocialfunctioning (Caplan et al. 2002, Hermann et al.2002). Secondly, our group of children was biasedtowards the more severe types of epilepsy as manychildren with pharmacologically intractable epilepsies,who are known to frequently have lower IQ and usemore AED, were referred to our centre, which isaffiliated to the Dutch Collaborative Epilepsy SurgeryProgramme. The use of anti-epilepsy drugs was notcontrolled for. Three-quarters of the sample of childrenwith epilepsy were on various combinations of AED. Inaddition, in the non-epilepsy neurological controlgroup various drugs were used. The number of childrenwas far too small for analysis of a treatment effect.
Notwithstanding these caveats, the present study isthe first to show a relationship between communicationand intelligence in children with epilepsy, but it alsodemonstrates that pragmatic deficits in children withepilepsy cannot be fully explained by intelligence.Because of their importance for social functioning,clinicians should be sensitive to and inquire after thesepragmatic aspects of communication.
Acknowledgements
The authors would like to thank Monique van Schooneveld forproviding a workspace and the necessary facilities to conduct theresearch. They also thank the two anonymous reviewers for theirvaluable comments and criticisms. Declaration of interest: Allauthors declare no conflict of interest in conducting or reporting ourresearch.
Note
1. Recent findings suggest that the Coherence scale measuresstructural rather than pragmatic language difficulties (Bishop,2003, Geurts et al. 2008). In the newer CCC, the CCC-2,Coherence is, therefore, no longer included in the pragmaticcomposite score.
References
ADAMS, C. and LLOYD, J., 2005, Elicited and spontaneouscommunicative functions and stability of conversationalmeasures with children who have pragmatic languageimpairments. International Journal of Language and Com-munication Disorders, 40, 333–347.
AMERICAN PSYCHIATRIC ASSOCIATION, 2000, Diagnostic andStatistical Manual of Mental Disorders, 4th-TR (Washington,DC: American Psychiatric Association).
BARA, B. G., BOSCO, F. M. and BUCCIARELLI, M., 1999,Developmental pragmatics in normal and abnormalchildren. Brain and Language, 68, 507–528.
BISHOP, D. V. M., 1998, Development of the Children’sCommunication Checklist (CCC): a method for assessingqualitative aspects of communicative impairment in children.Journal of Child Psychology and Psychiatry, 39, 879–891.
BISHOP, D. V. M., 2003, The Children’s Communication Checklist—2(London: Psychological Corporation).
BISHOP, D. V. M. and BAIRD, G., 2001, Parent and teacher reportof pragmatic aspects of communication: use of the Children’sCommunication Checklist in a clinical setting. Develop-mental Medicine and Child Neurology, 43, 809–818.
BJØRNAES, H., STABELL, K., HENRIKSEN, O. and LOYNING, Y.,2001, The effects of refractory epilepsy on intellectualfunctioning in children and adults: a longitudinal study.Seizure, 10, 250–259.
BOEKAERTS, M. and RODER, I., 1999, Stress, coping, andadjustment in children with a chronic disease: a review ofthe literature. Disability and Rehabilitation, 21, 311–337.
CAPLAN, R., GUTHRIE, D., KOMO, S., SIDDARTH, P.,CHAYASIRISOBHON, S., KORNBLUM, H., SANKAR, R., HANSEN,R., MITCHELL, W. and SHIELDS, W. D., 2002, Socialcommunication in children with epilepsy. Journal of ChildPsychology and Psychiatry, 43, 245–253.
CHEANG, H. S. and PELL, M. D., 2006, A study of humour andcommunicative intention following right hemisphere stroke.Clinical Linguistics and Phonetics, 20, 447–462.
COHEN, H. and LE NORMAND, M. T., 1998, Language acquisitionin children with partial epilepsy. Brain and Cognition, 37,182–186.
CONRAD, R., 1972, The developmental role of vocalizing in short-term memory. Journal of Verbal Learning and VerbalBehavior, 11, 521–533.
DODRILL, C. B., 2004, Neuropsychological effects of seizures.Epilepsy and Behavior, 5 (Suppl. 1), S21–S24.
GEURTS, H. M. and EMBRECHTS, M., 2008, Language profiles inASD, SLI, and ADHD. Journal of Autism and DevelopmentalDisorders, 38, 1931–1943.
GEURTS, H. M., HARTMAN, C., VERTE, S., OOSTERLAAN, J.,ROEYERS, H. and SERGEANT, J. A., 2005, Psychometrischekwaliteiten en normering van de Nederlandse Children’sCommunication Checklist. Diagnostiekwijzer, 3, 102–119.
GEURTS, H. M., HARTMAN, C., VERTE, S., OOSTERLAAN, J.,ROEYERS, H. and SERGEANT, J. A., 2008, Pragmaticsfragmented: the factor structure of the Dutch Children’sCommunication Checklist (CCC). International Journal ofLanguage and Communication Disorders, iFirst article, 1–26.
GEURTS, H. M., VERTE, S., OOSTERLAAN, J., ROEYERS, H.,HARTMAN, C. A., MULDER, E. J., VAN BERCKELAER-ONNES,I. A. and SERGEANT, J. A., 2004, Can the Children’sCommunication Checklist differentiate between childrenwith autism, children with ADHD, and normal controls?Journal of Child Psychology and Psychiatry, 45, 1437–1453.
GILMOUR, J., HILL, B., PLACE, M. and SKUSE, D. H., 2004, Socialcommunication deficits in conduct disorder: a clinical andcommunity survey. Journal of Child Psychology andPsychiatry, 45, 967–978.
HARTMAN, C. A., GEURTS, H. M., VERTE, S., ROEYERS, H.,SERGEANT, J. A. and BISHOP, D. V. M., 1998, De Drie C’s:Children’s Communication Checklist, [The Three C’s:Children’s Communication Checklist]. Unpublished manu-script, Vrije Universiteit, Amsterdam).
Pragmatic deficits in children with epilepsy 615

HATTON, C., 1998, Pragmatic language skills in people withintellectual disabilities: a review. Journal of Intellectual andDevelopmental Disability, 23, 79–100.
HERMANN, B., SEIDENBERG, M., BELL, B., RUTECKI, P., SHETH, R.,RUGGLES, K., WENDT, G., O’LEARY, D. and MAGNOTTA, V.,2002, The neurodevelopmental impact of childhood-onsettemporal lobe epilepsy on brain structure and function.Epilepsia, 43, 1062–1071.
HYTER, Y. D., 2007, Pragmatic language assessment: a pragmatics-as-social practice model. Topics in Language Disorders, 27,128–145.
LEW, A. R., LEWIS, C., OWEN, L., WEST, S., TOMLIN, P., ROACH, J.and VASSALLO, G., 2006, Psychosocial problems and seizure-related factors in children with epilepsy. DevelopmentalMedicine and Child Neurology, 48, 702–704.
MARTIN, I. and MCDONALD, S., 2003, Weak coherence, no theoryof mind, or executive dysfunction? Solving the puzzle ofpragmatic language disorders. Brain and Language, 85,451–466.
NORBURY, C. F., NASH, M., BAIRD, G. and BISHOP, D. V. M.,2004, Using a parental checklist to identify diagnostic groupsin children with communication impairment: a validation ofthe Children’s Communication Checklist—2. International
Journal of Language and Communication Disorders, 39,345–364.
PARKINSON, G. M., 2006, Pragmatic difficulties in children withautism associated with childhood epilepsy. PediatricRehabilitation, 9, 229–246.
PEPPE, S., MCCANN, J., GIBBON, F., O’HARE, A. and RUTHERFORD,M., 2006, Assessing prosodic and pragmatic ability inchildren with high-functioning autism. Journal of Pragmatics,38, 1776–1791.
REJNO-HABTE SELASSIE, G. R., VIGGEDAL, G., OLSSON, I. andJENNISCHE, M., 2008, Speech, language, and cognition inpreschool children with epilepsy. Developmental Medicineand Child Neurology, 50, 432–438.
ROTHMAN, K. J., 1990, No adjustments are needed for multiplecomparisons. Epidemiology, 1, 43–46.
RUSSELL, R. L. and GRIZZLE, K. L., 2008, Assessing child andadolescent pragmatic language competencies: toward evidence-based assessments.Clinical Child and Family psychology Review,11, 59–73.
SCHOENFELD, J., SEIDENBERG, M., WOODARD, A., HECOX, K.,INGLESE, C., MACK, K. and HERMANN, B., 1999,Neuropsychological and behavioral status of children withcomplex partial seizures. Developmental Medicine and ChildNeurology, 41, 724–731.
616 Mark Broeders et al.