practice transformation research informing the future ... · pdf filepractice transformation...
TRANSCRIPT
Practice Transformation Research Informing the Future Delivery of Healthcare:
Insights from IHARP
William T. Lee, BSPharm, MPA, FASCPPharmacy System Director, Carilion Medical Center
Gary R. Matzke, BS Pharm, PharmD, FCP, FCCPProfessor VCU School of Pharmacy
Medical College of Wisconsin School of PharmacySymposium: Emerging Pharmacy Practice Models in
Healthcare DeliveryJune 24, 2016
OBJECTIVES
• Describe the clinical processes that comprise the IHARP care delivery model.
• State the key lessons learned during the implementation of the IHARP care delivery model.
• Characterize how the clinical care and health utilization outcome evaluation metrics were impacted by the IHARP program.
• Describe the IHARP program’s influence on the cost of health care services delivery.
• Assess the relative contribution of improvements in clinical outcomes, patient and provider satisfaction and economic measures on the sustainability of clinical pharmacy services.

CMMI Medication Management (MM) Health Care Innovation Awardees
• University of Southern California (USC)• University of Pennsylvania’s HeartStrong program
(HeartStrong)• Pharmacy Society of Wisconsin (PSW)• University of Tennessee’s SafeMed program (SafeMed) • University of Hawaii at Hilo’s Pharm2Pharm program
(Pharm2Pharm) and • Carilion New River Valley Medical Center in partnership
with Virginia Commonwealth University’s Improving Health for At-risk Rural Patients (IHARP)
Status of MM Innovation Projects
• Quantitative analysis for three of the six programs: IHARP, USC, and Pharm2Pharm was conducted by an external consultant group.
• They did not conduct a quantitative analysis for the HeartStrong or SafeMed programs, because they did not have sufficient participant-level program data to conduct an analysis.
• Additionally, due to clarity concerns regarding PSW’s targeting criteria a quantitative analysis of PSW was not conducted.
PROJECT GOALS
• Create a sustainable patient centered continuity of care health care delivery model within a rural health system comprised of multiple hospitals, primary care practices, and community pharmacies;
• Achieve better patient health outcomes• Smarter spending by optimizing medication-related health
outcomes • Implement and evaluate a new model of pharmacist
workforce development; and • Evaluate the clinical, humanistic and economic outcomes
associated with this new health care delivery model
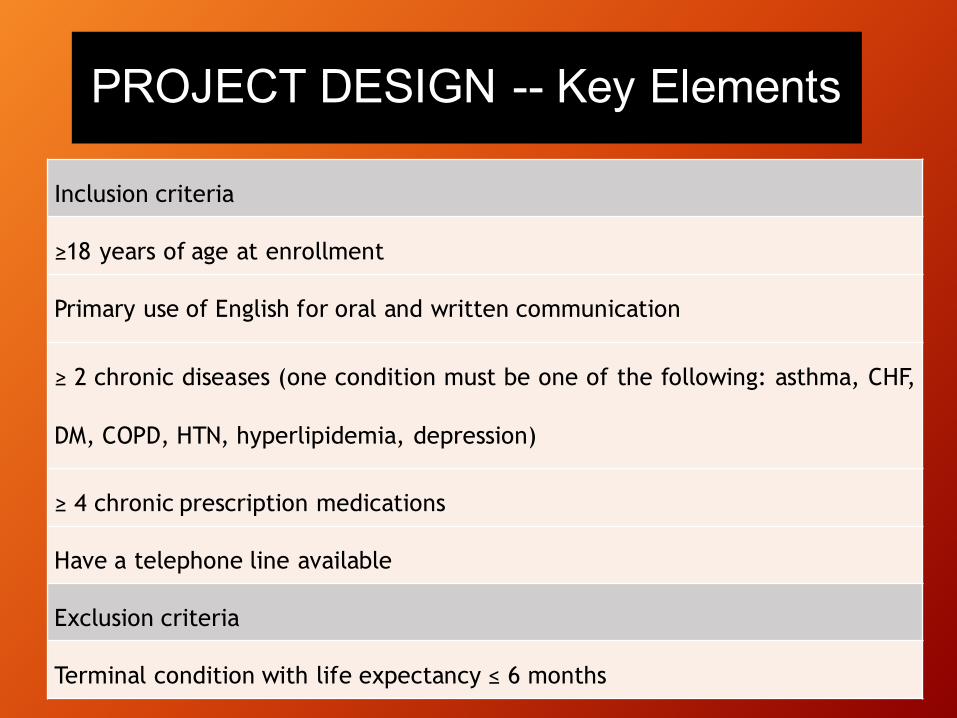
Inclusion criteria
≥18 years of age at enrollment
Primary use of English for oral and written communication
≥ 2 chronic diseases (one condition must be one of the following: asthma, CHF,
DM, COPD, HTN, hyperlipidemia, depression)
≥ 4 chronic prescription medications
Have a telephone line available
Exclusion criteria
Terminal condition with life expectancy ≤ 6 months
PROJECT DESIGN -- Key Elements
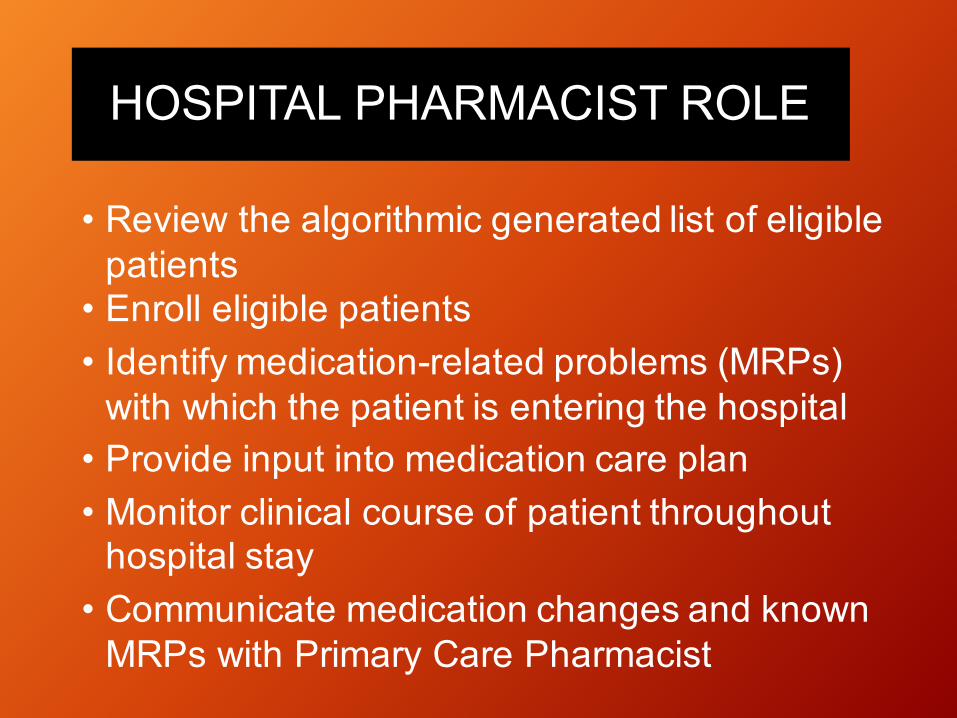
HOSPITAL PHARMACIST ROLE
• Review the algorithmic generated list of eligible patients
• Enroll eligible patients• Identify medication-related problems (MRPs)
with which the patient is entering the hospital• Provide input into medication care plan• Monitor clinical course of patient throughout
hospital stay• Communicate medication changes and known
MRPs with Primary Care Pharmacist
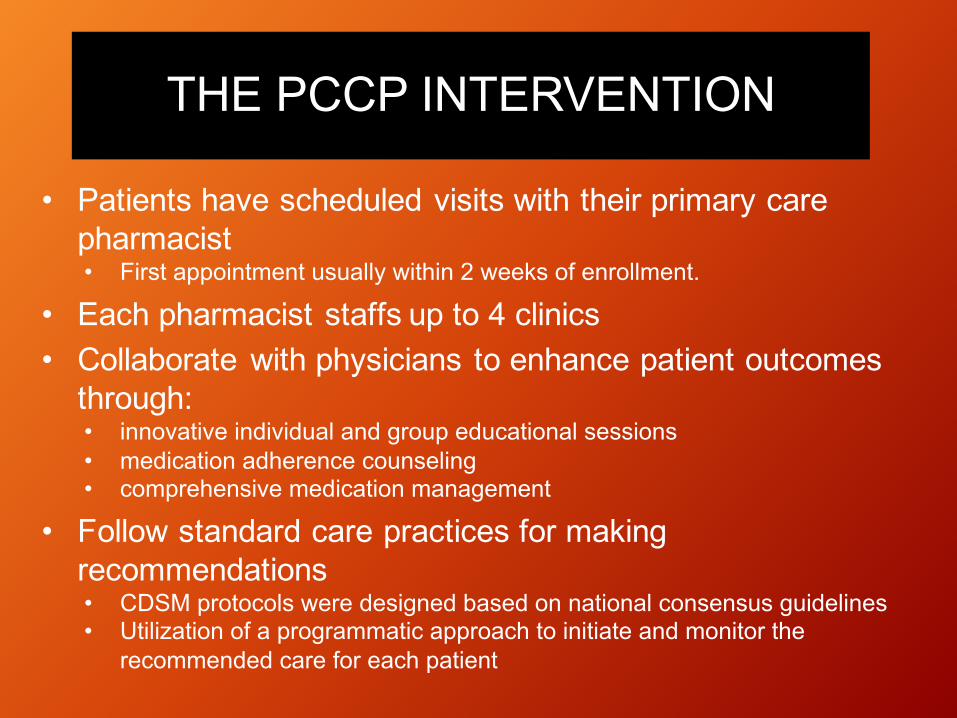
THE PCCP INTERVENTION
• Patients have scheduled visits with their primary care pharmacist• First appointment usually within 2 weeks of enrollment.
• Each pharmacist staffs up to 4 clinics• Collaborate with physicians to enhance patient outcomes
through:• innovative individual and group educational sessions• medication adherence counseling• comprehensive medication management
• Follow standard care practices for making recommendations• CDSM protocols were designed based on national consensus guidelines• Utilization of a programmatic approach to initiate and monitor the
recommended care for each patient
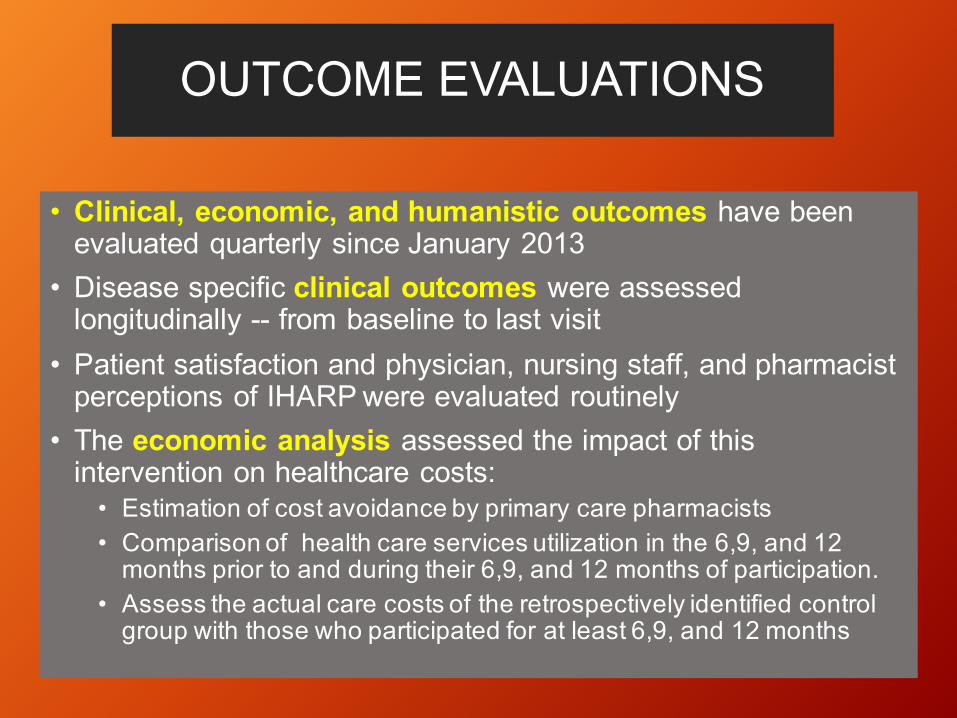
OUTCOME EVALUATIONS
• Clinical, economic, and humanistic outcomes have been evaluated quarterly since January 2013
• Disease specific clinical outcomes were assessed longitudinally -- from baseline to last visit
• Patient satisfaction and physician, nursing staff, and pharmacist perceptions of IHARP were evaluated routinely
• The economic analysis assessed the impact of this intervention on healthcare costs:
• Estimation of cost avoidance by primary care pharmacists• Comparison of health care services utilization in the 6,9, and 12
months prior to and during their 6,9, and 12 months of participation. • Assess the actual care costs of the retrospectively identified control
group with those who participated for at least 6,9, and 12 months

Humanistic Outcomes
Measure Baseline 6 12 18 24
Humanistic outcomes
Physician and Staff Satisfaction X X X X Email survey
Patient satisfaction X X X X Mailed Survey
Pharmacist and Provider
Experience
X X Interviews
CareModelDocumentation:CustomizationofElectronicMedicalRecords
DocumentationToolSelection• Capturesrequireddata• InteroperabilitywithEMR• Communicationfeatures• Customizationpotential• Reporting• Security• Sustainability
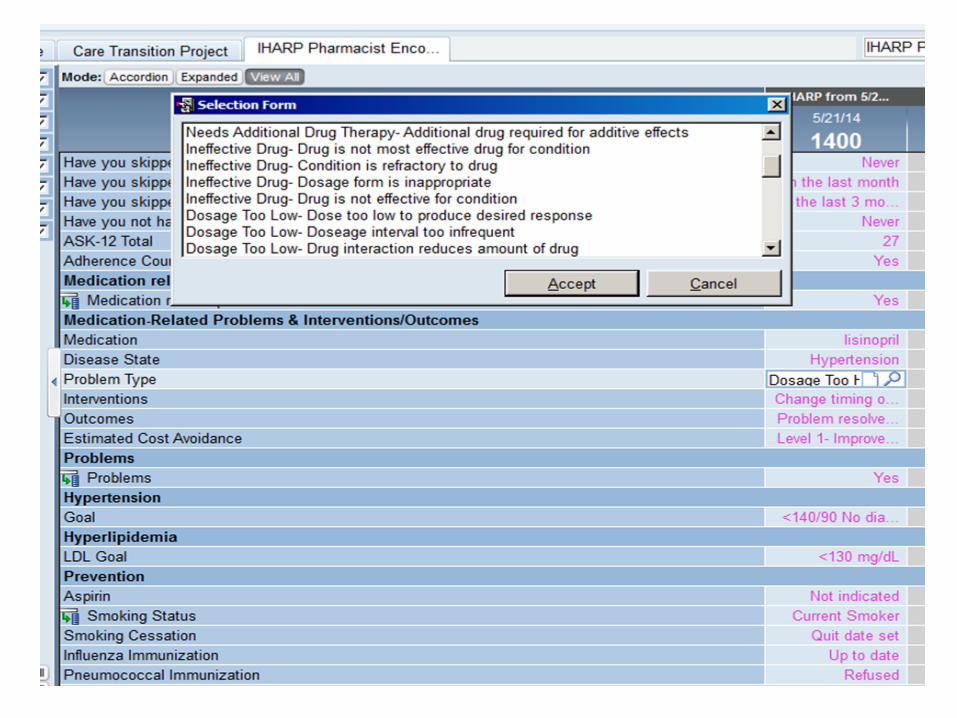

MedicationRelatedProblemDocumentation
ProblemTypeExamplesUnnecessaryDrugTherapy
NovalidindicationTherapeuticduplicationNondrugtherapyneeded
NeedsAdditionalDrugTherapy
InitiationofdrugtherapyrequiredAdditionaldrugrequiredforadditiveeffects
InterventionExamplesAdddrugChangedrugtoanotherRxDiscontinuedrugIncreasedoseDecreasedoseEducation-PrescriptionMed
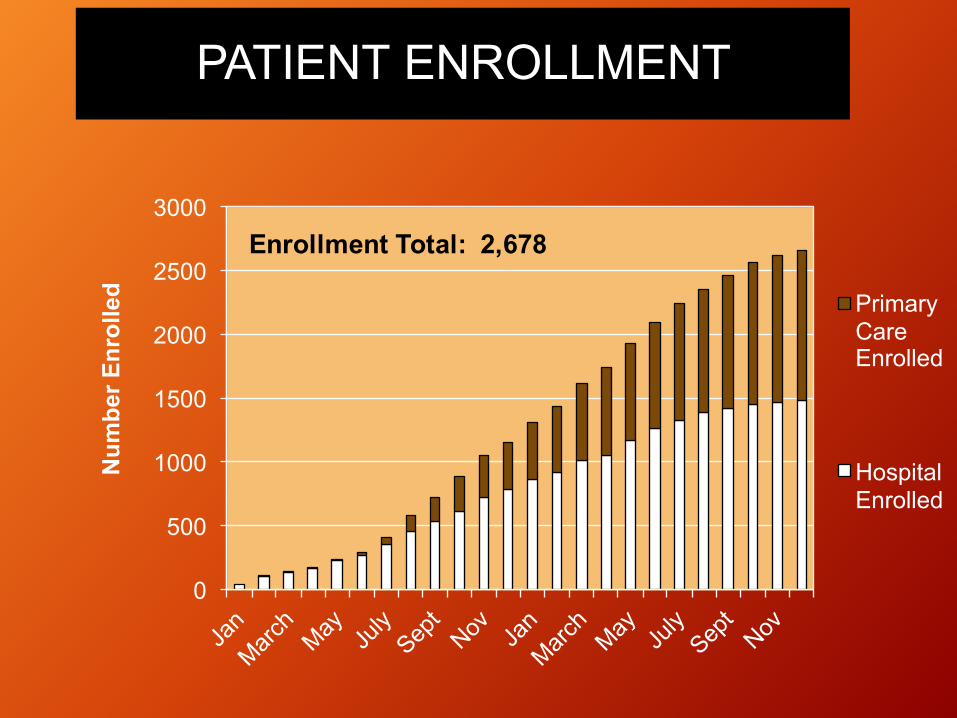
PATIENT ENROLLMENT
0
500
1000
1500
2000
2500
3000
Num
ber E
nrol
led Primary
Care Enrolled
Hospital Enrolled
Enrollment Total: 2,678
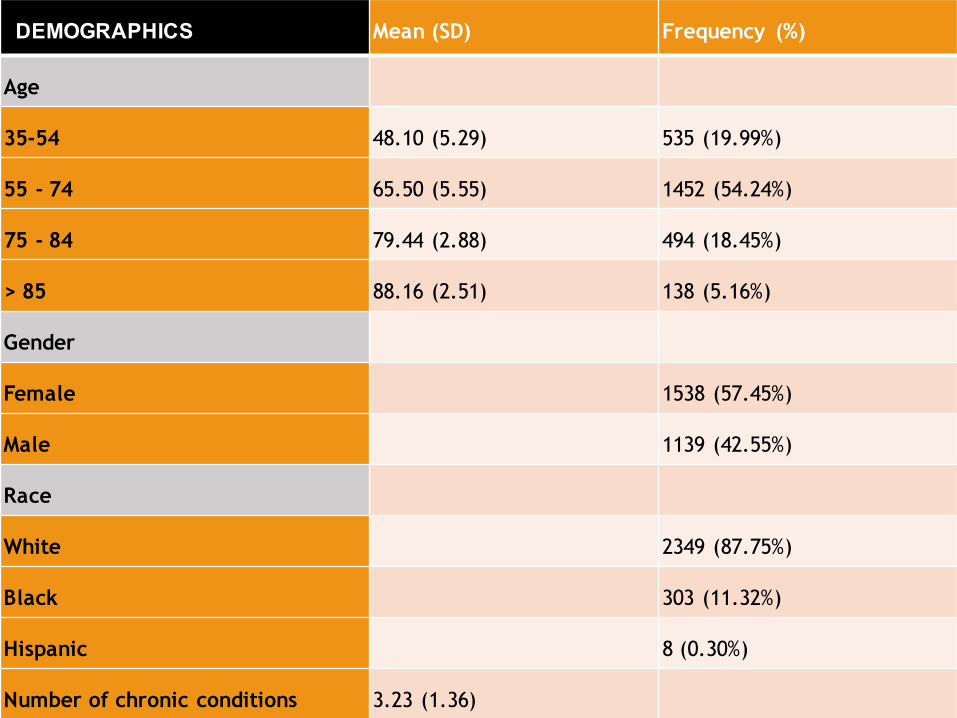
DEMOGRAPHICS Mean (SD) Frequency (%)
Age
35-54 48.10 (5.29) 535 (19.99%)
55 - 74 65.50 (5.55) 1452 (54.24%)
75 - 84 79.44 (2.88) 494 (18.45%)
> 85 88.16 (2.51) 138 (5.16%)
Gender
Female 1538 (57.45%)
Male 1139 (42.55%)
Race
White 2349 (87.75%)
Black 303 (11.32%)
Hispanic 8 (0.30%)
Number of chronic conditions 3.23 (1.36)

Chronic Conditions at time of Enrollment
Disease State (N=18427) n (%)
Hypertension 2164 80.8
Hyperlipidemia 2012 75.2
Diabetes 1500 56.3
Anxiety 658 24.6
COPD 608 22.7
Thyroid 548 20.5
Chronic kidney disease 388 14.5
Gout 200 7.5
Chronic heart failure 186 7.0
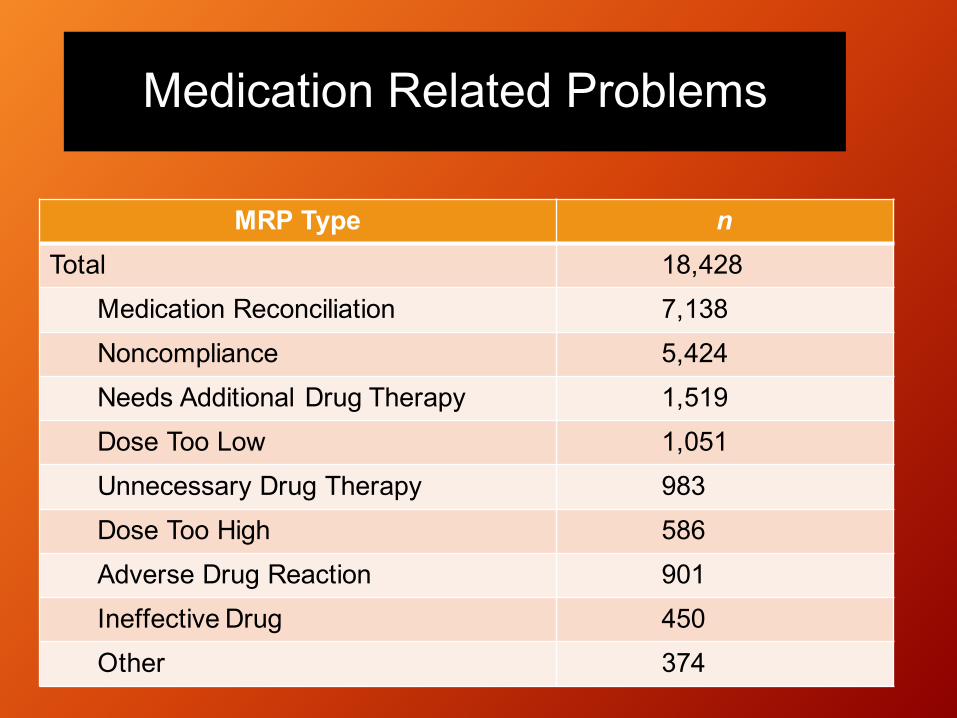
Medication Related Problems
MRP Type nTotal 18,428
Medication Reconciliation 7,138Noncompliance 5,424Needs Additional Drug Therapy 1,519Dose Too Low 1,051Unnecessary Drug Therapy 983Dose Too High 586Adverse Drug Reaction 901Ineffective Drug 450Other 374
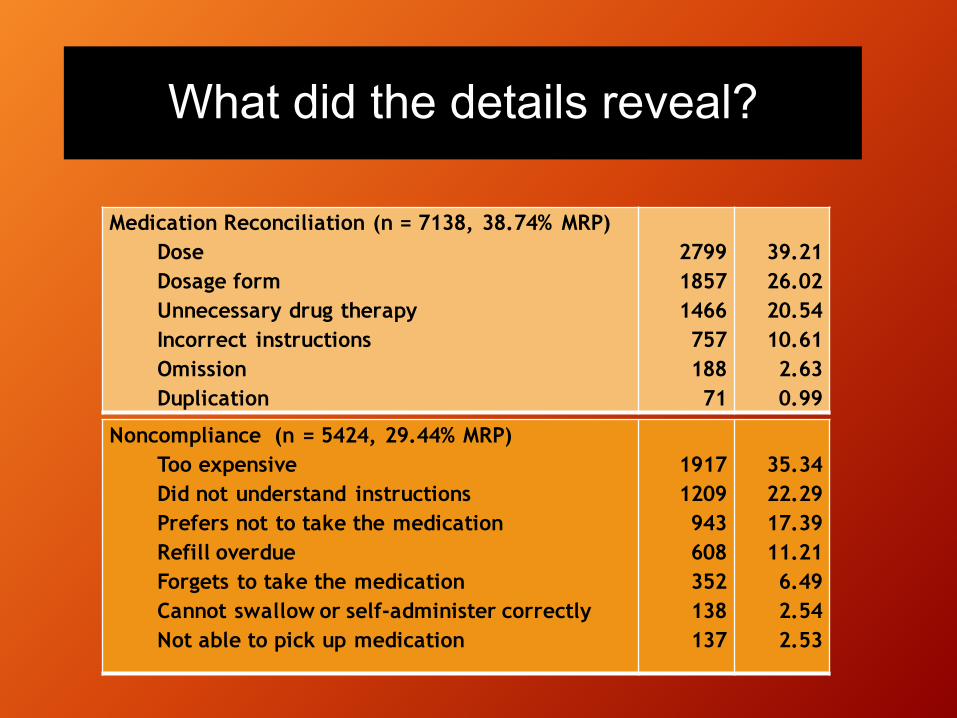
What did the details reveal?
Medication Reconciliation (n = 7138, 38.74% MRP)DoseDosage form Unnecessary drug therapyIncorrect instructionsOmissionDuplication
27991857146675718871
39.2126.0220.5410.612.630.99
Noncompliance (n = 5424, 29.44% MRP)Too expensiveDid not understand instructions Prefers not to take the medication Refill overdueForgets to take the medicationCannot swallow or self-administer correctly Not able to pick up medication
19171209943608352138137
35.3422.2917.3911.216.492.542.53

Pharmacist Interventions
Interventions (n = 19,677) (n) (%)
Discontinue Drug 5756 29.25
Add Drug 3059 15.55
Increase Dose 1571 7.98
Change Drug to Another Rx 1128 5.73
Education Adherence 1115 5.67
Decrease Dose 1020 5.18
Education Prescribed Med 1001 5.09
Cost Switch 876 4.45
Refill Drug 747 3.80
Initiation of Monitoring 515 2.62
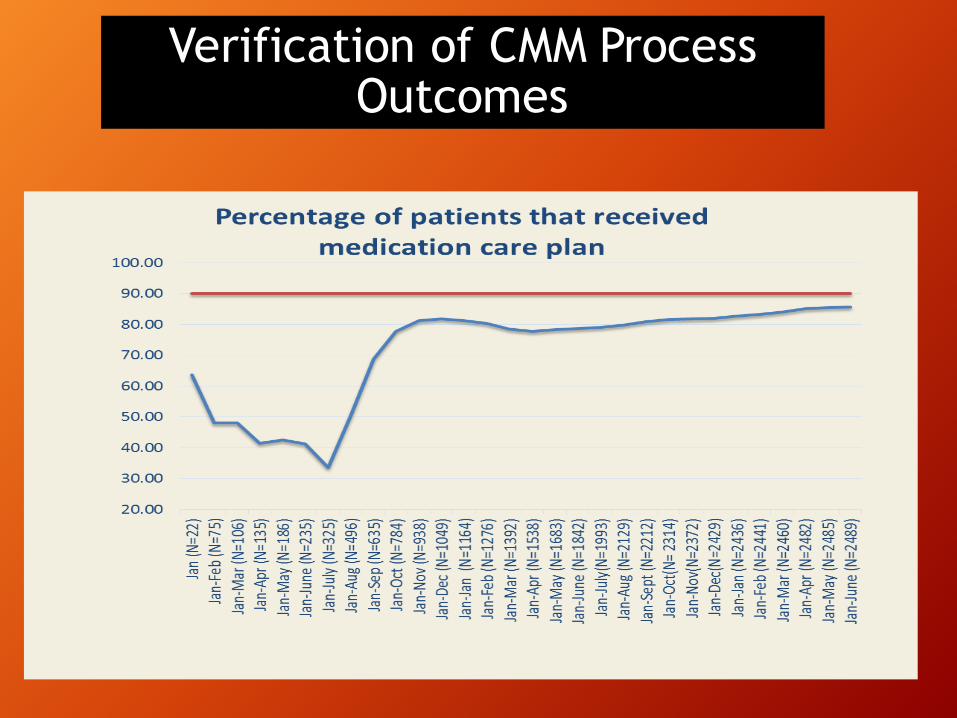
Verification of CMM Process Outcomes
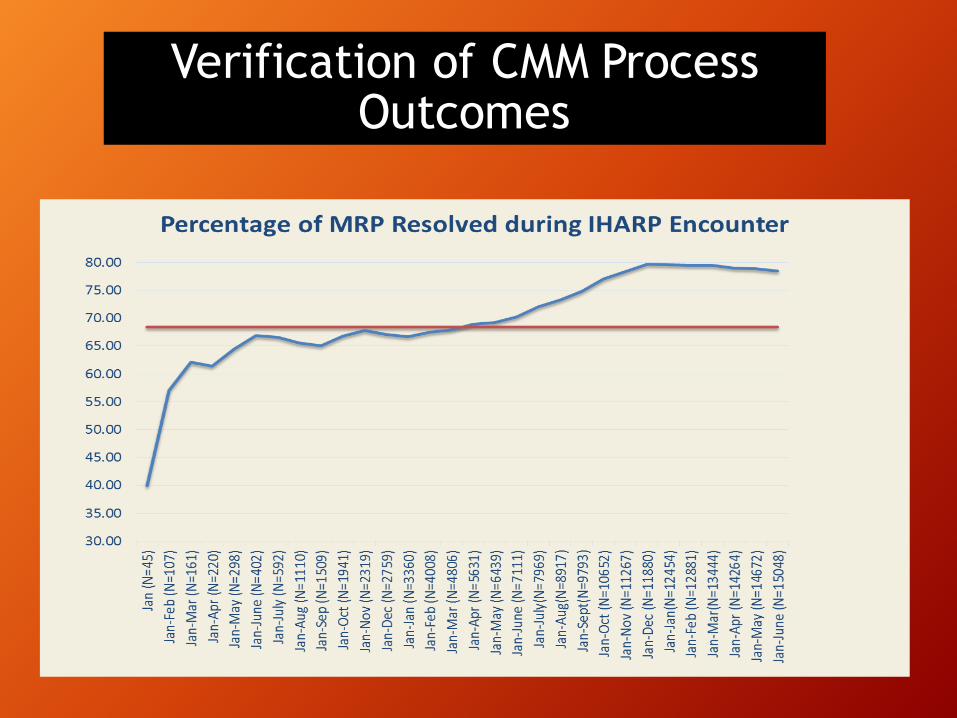
Verification of CMM Process Outcomes

CLINICAL OUTCOMES
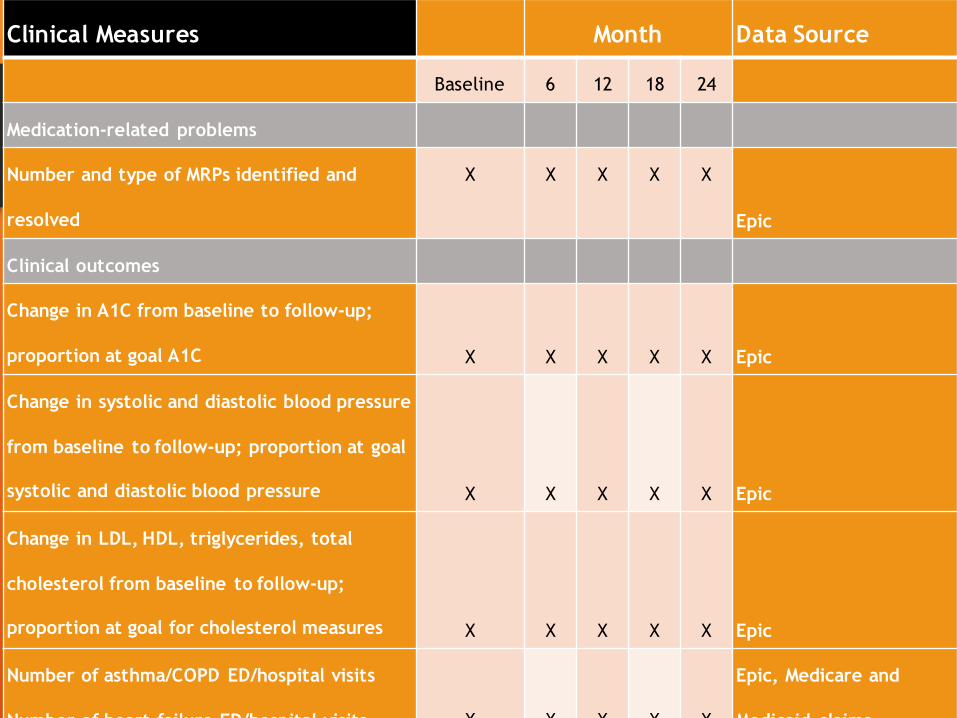
Clinical Measures Month Data Source
Baseline 6 12 18 24
Medication-related problems
Number and type of MRPs identified and
resolved
X X X X X
Epic
Clinical outcomes
Change in A1C from baseline to follow-up;
proportion at goal A1C X X X X X Epic
Change in systolic and diastolic blood pressure
from baseline to follow-up; proportion at goal
systolic and diastolic blood pressure X X X X X Epic
Change in LDL, HDL, triglycerides, total
cholesterol from baseline to follow-up;
proportion at goal for cholesterol measures X X X X X Epic
Number of asthma/COPD ED/hospital visits
Number of heart failure ED/hospital visits X X X X X
Epic, Medicare and
Medicaid claims
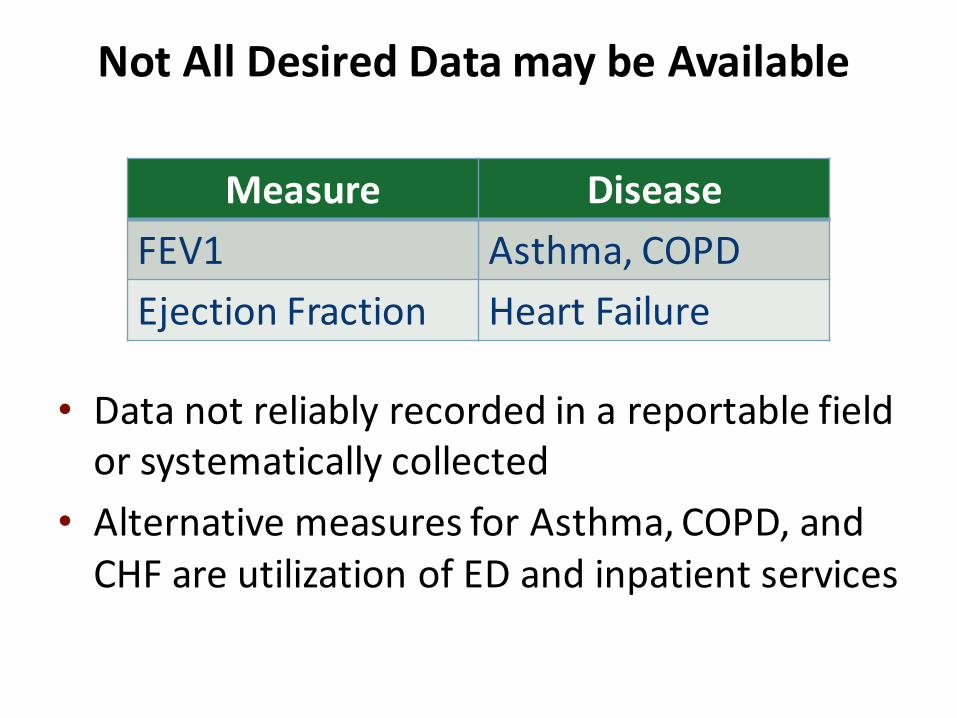
NotAllDesiredDatamaybeAvailable
• Datanotreliablyrecordedinareportablefieldorsystematicallycollected
• AlternativemeasuresforAsthma,COPD,andCHFareutilizationofEDandinpatientservices
Measure DiseaseFEV1 Asthma,COPDEjectionFraction HeartFailure
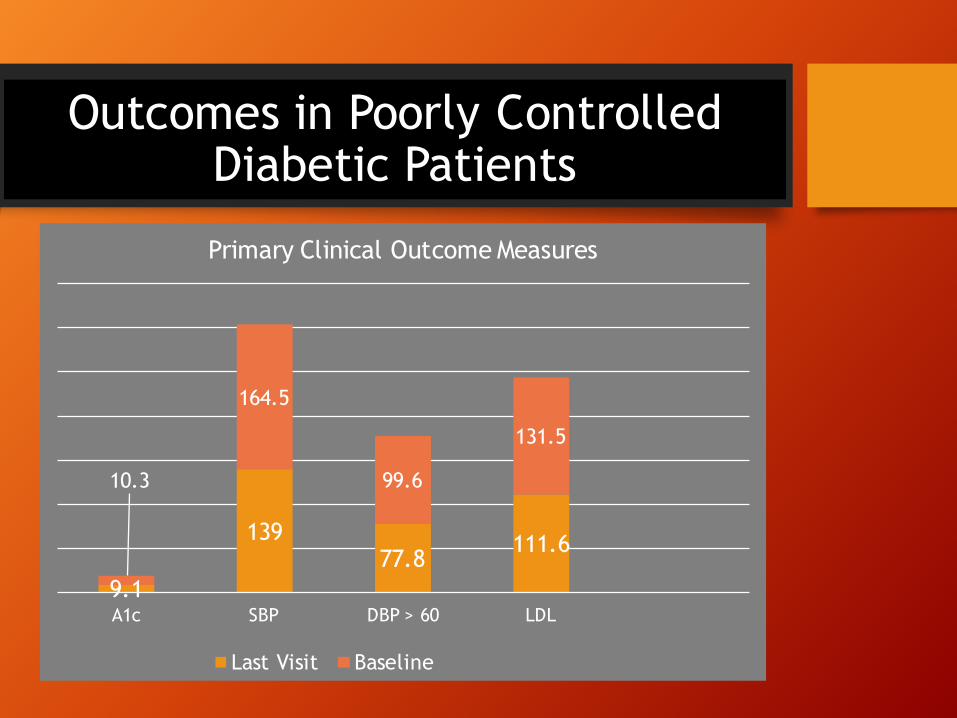
Outcomes in Poorly Controlled Diabetic Patients
9.1
13977.8
111.6
10.3
164.5
99.6
131.5
A1c SBP DBP > 60 LDL
Primary Clinical Outcome Measures
Last Visit Baseline
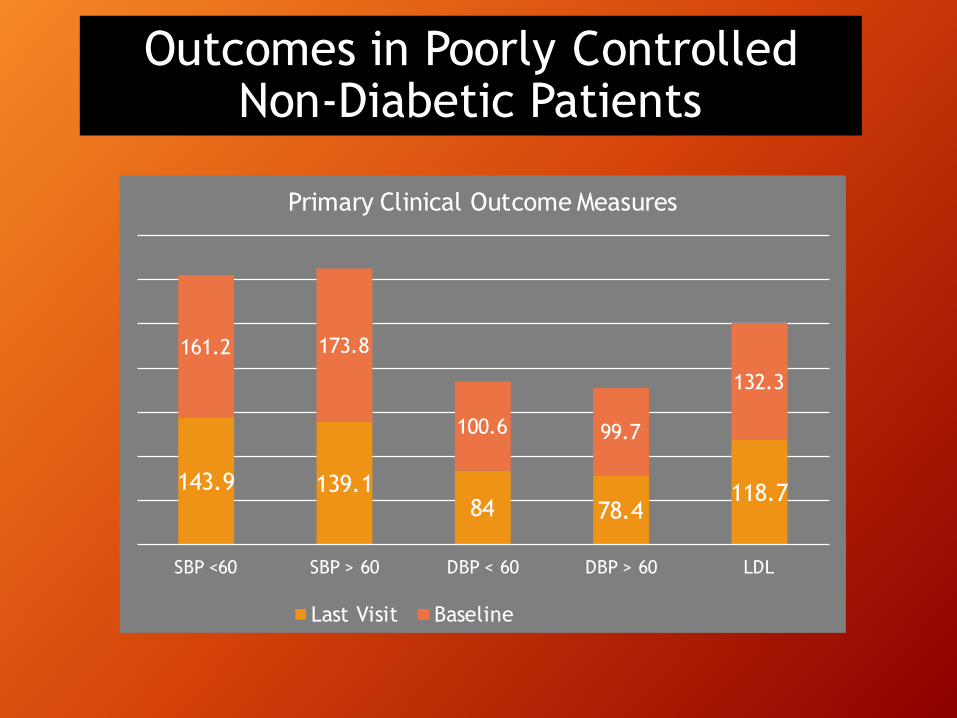
Outcomes in Poorly Controlled Non-Diabetic Patients
143.9 139.184 78.4
118.7
161.2 173.8
100.6 99.7
132.3
SBP <60 SBP > 60 DBP < 60 DBP > 60 LDL
Primary Clinical Outcome Measures
Last Visit Baseline
PATIENT AND PROVIDER SATISFACTION
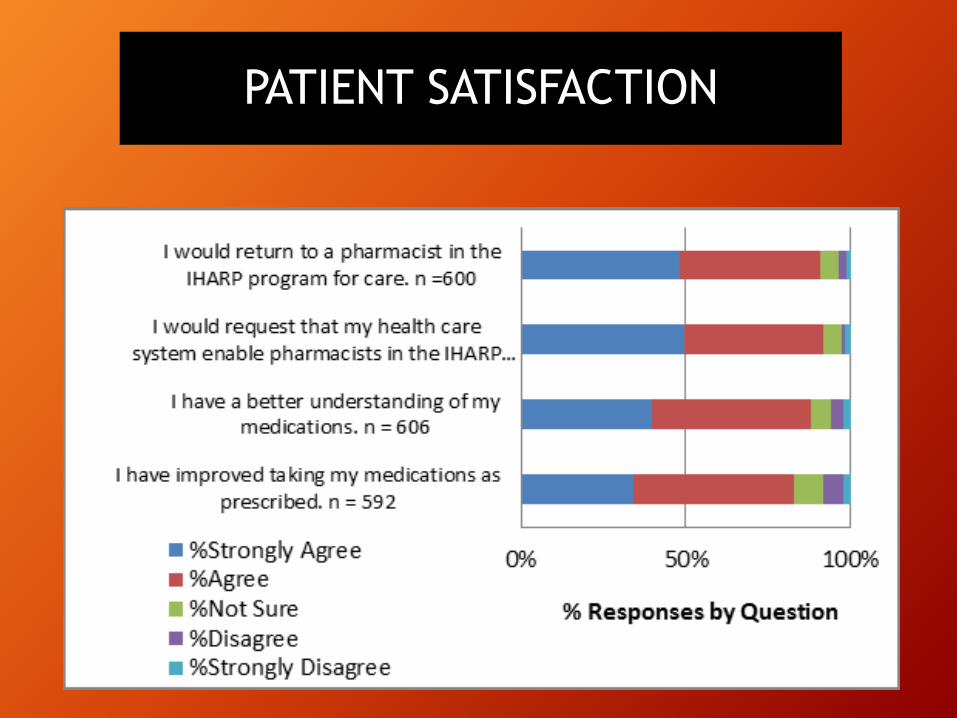
PATIENT SATISFACTION
• “I was sad I hadn't known of this sooner, but ecstatic that I do now. She helped me save substantially on expenses. She also explained the importance of taking meds as directed – e.g. twice a day means exactly that, not combining both doses into one. Obviously my experience with IHARP has been great!”
• “This is a great program. It has helped me a lot to understand my medications. It is great to know what I am taking and what it is for. Everyone needs to be in this program and it would be great for the older people (that's me). It is really great the pharmacist calls to make sure I am doing O.K.”
Patient Comments
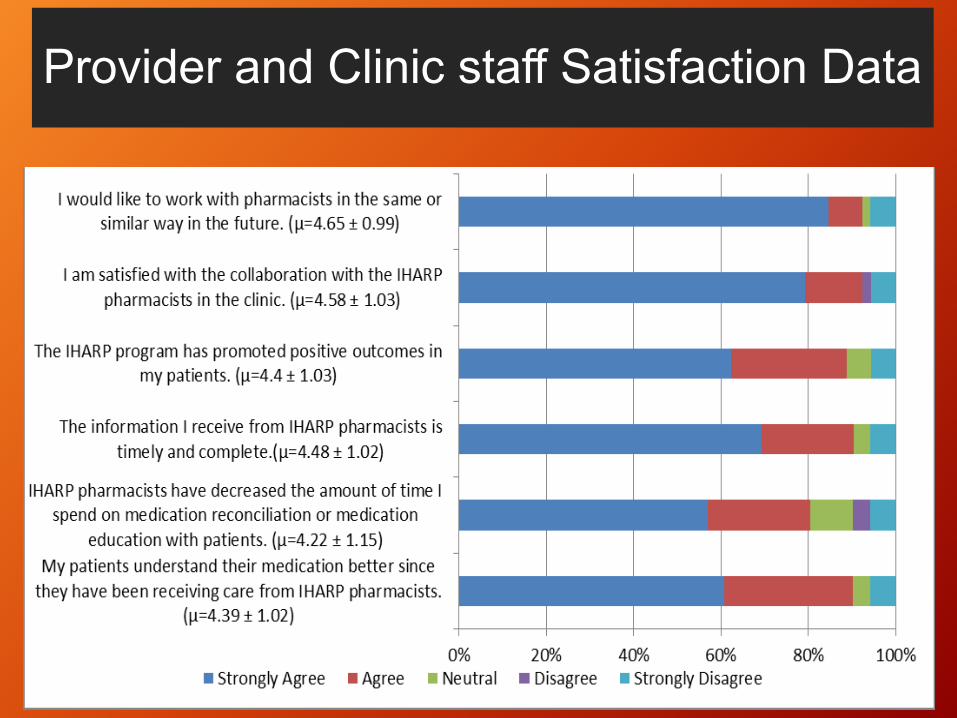
Provider and Clinic staff Satisfaction Data

Physician Comments“This is hands down the most helpful program that has ever been offered in our primary care clinic. It has been enormously useful to me as a provider--- it saves tremendous time and the pharmacists are a great resource for medication related questions.
It has likewise been tremendously helpful to patients-- it has improved their understanding of their medications and disease process, has saved them money and has likely improved outcomes and decreased risk by ensuring compliance with prescribed therapies. The best thing since sliced bread, in my humble opinion.”
ESTIMATED COST AVOIDANCE, AND HEALTH CARE SERVICES
UTILIZATION

Estimated Cost Avoidance associated with resolution of Medication Related Problems
Avoidance Value n Total
Reduced drug product costs $ 64 1602 $ 102,496
Additional physician visit $ 369 410 $ 151,114
Additional prescription order $ 454 1640 $ 744,462
Emergency room visit $ 1,010 213 $ 215,130
Hospital admission $ 28,263 78 $ 2,204,526
Project Total $3,417,728
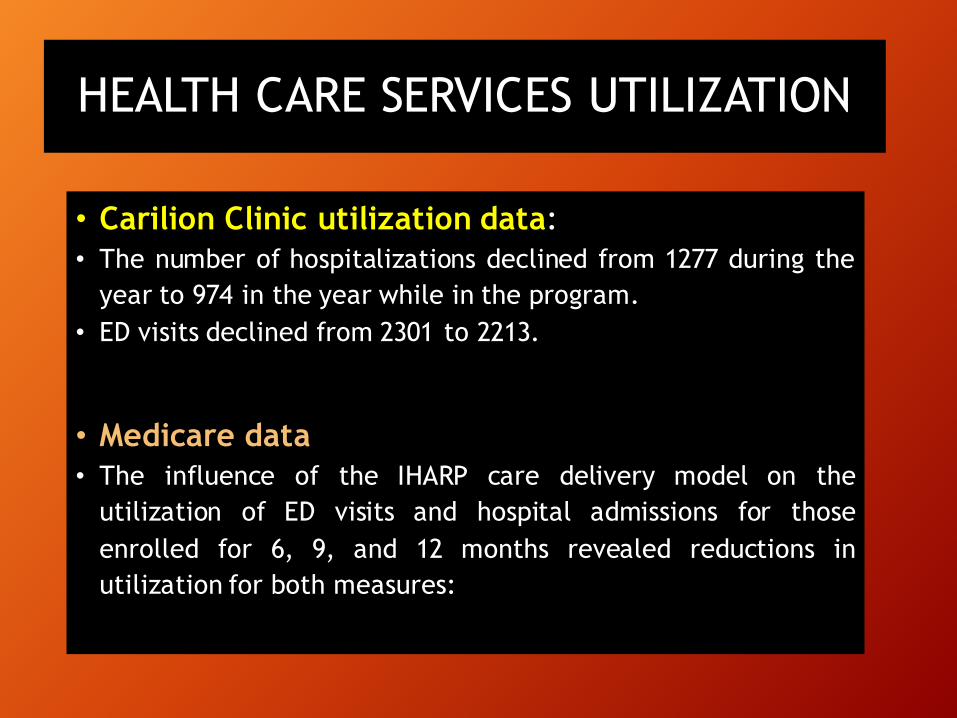
HEALTH CARE SERVICES UTILIZATION
• Carilion Clinic utilization data:• The number of hospitalizations declined from 1277 during the
year to 974 in the year while in the program.• ED visits declined from 2301 to 2213.
• Medicare data:• The influence of the IHARP care delivery model on the
utilization of ED visits and hospital admissions for thoseenrolled for 6, 9, and 12 months revealed reductions inutilization for both measures:
SUSTAINABILITY PLANNING
Generate Revenue
Enhance Quality
Reduced Costs
LESSONS LEARNED
• Data collection and archiving were challenging but essential• Continual monitoring of data (CQI) allowed for adjustment of
procedures to facilitate achievement of desired outcomes• Access to EMR data greatly facilitates continuity of care• The role for a pharmacist on a primary care team is not
apparent to everyone• Building relationships with staff is as important as building
relationships with patients• Adherence is sometimes all about money• Role for pharmacy technician ?
Institutional Implications
• “Transitions of Care” model-- implications for pharmacy staffing patterns
• Collaboration with community pharmacies and Carilion owned retail pharmacies—a challenge
• Medication reconciliation process –system wide and pharmacy coordinated
• Increased MAP needs recognized- required changes in staffing and communication

Institutional Implications
• IHARP Analysis of institutional data – provides a basis for sound ROI for expansion
• Changing Role of Inpatient Pharmacist. Pre-admission understanding, post-discharge continuity
• Impact -- Patient Satisfaction / patient Engagement initiatives
• Contribution to improvements in HCAHPS and CG-HCAHPS implications for sustainability
Professional Implications
• Medicare Provider status –is this the “holy grail”• Refine training and curriculum of pharmacists
(initial training and updating skills)• New expanded roles for technicians• New practice paradigm shift - continuum of care• Standardization of clinical pharmacy care • Telepharmacy and template for standard of care
Conclusions
• The addition of comprehensive medication and disease state management into team based PCMH is scalable and can be delivered to high risk patients
• PCMH staff, physicians, and pharmacists have a high degree of satisfaction with the skills pharmacists bring to a patient care team
• Early data strongly suggest that there is a positive return on investment associated with the IHARP care model
IHARP PROJECT TEAM• Leadership
• William Lee, DPh, MPA, FASCP• Michael J. Czar, RPh, PhD• Anthony R. Stavola, MD• Gary R. Matzke, PharmD FCP,
FCCP• Leticia R. Moczygemba, PharmD,
PhD
• Carilion Partners• Michael Jeremiah, MD• Charles Tarasidis, PharmD• Chad Alvarez, PharmD
• Clinical Pharmacists• Karen J. Williams, PharmD, BCPS• Heidi D. Wengerd, PharmD• Kelley D. Mills, PharmD• Courtney P. Dickerson, PharmD• Tanvi Patil, PharmD• Nikisa Blevins, PharmD• Ann Lucktong, PharmD• Randi Carpenter, PharmD
• IHARP Staff• Kristy Crigger• Christine Riddell• Andrea Pierce, PharmD• Della Varghese• Bhavini Kaneria, MS• Samantha Marks, PharmD
DISCUSSION
PHARMACY