practical aspects of managing diabetes in adolescents
TRANSCRIPT

Practical aspects of managing diabetes in adolescentsHB Mortensen
Department of Paediatrics, Glostrup University Hospital, Denmark
Mortensen HB. Practical aspects of managing diabetes in adolescents. Acta Pædiatr 1998; Suppl 425: 72–6.Stockholm. ISSN 0803-5326
In 1988 and 1990 screening for HbA1c and albumin excretion rate in diabetic children was carried outthroughout Denmark. Each study included approximately 1000 diabetic patients. Raised levels of HbA1c
(9.5–10%) were found despite 60% of these young people receiving three or more insulin injections daily.The prevalence of persistent microalbuminuria was 4.3%, which was associated only with age and diastolicblood pressure. A recent international survey of HbA1c and insulin treatment involving 2873 children foundan average HbA1c of 8.6%6 1.7%, which varied significantly (p , 0. 0001) between centres. Severehypoglycaemia was related to a young age (0–8 y) and low HbA1c. There were no significant differences inglycaemic control between adolescents treated with two, three, four or more insulin injections daily.Adolescents on four or more injections received significantly (p , 0:001) more insulin. Girls receivingfour or more injections had a significantly (p , 0:01) higher body mass index than girls on twice-dailyinsulin. Preadolescent children on premixed insulin showed similar HbA1c levels to those on a combinationof short- and long-acting insulin, whereas in adolescents, significantly better HbA1c values were achievedwith individual combinations. Despite intensive diabetes management, particularly in adolescence, nearnormoglycaemia is achieved only in a few individuals.` Adolescence, blood glucose, child, diabetescontrol, glycosylated, haemoglobin A, insulin treatment
HB Mortensen, Department of Paediatrics, Glostrup University Hospital, DK-2600 Glostrup, Denmark
Despite initiatives to formulate consensus guidelines for themanagement of type 1 diabetes in childhood and adoles-cence (1–3), relatively little information is available on theoutcome of current diabetes therapy. Danish investigations(4, 5) and a recent international survey (6) demonstrated thatblood glucose control in unselected young diabetic patientswas not satisfactory, even though a large proportion of thesepatients was on intensive insulin treatment regimens.The Diabetes Control and Complications Trial (DCCT)Research Group (7) showed that a group of highly selected,motivated and closely supported adolescents in the 13–17-y-old age group can achieve excellent glycaemic controland a reduction in microvascular complications. However,the results from the DCCT also showed that intensivediabetes management with greater emphasis on glycaemiccontrol increased the risk of severe hypoglycaemia 2–4-foldand a significant proportion of these patients gained weight.The practicalities of applying the DCCT recommendationsto a wider group of adolescents remain difficult.
The aim of this paper was to describe practical aspects ofmanaging diabetes in adolescents. Data were drawn fromblood-glucose control and some types of microvascularcomplications in diabetic children in two Danish studiesand in the international survey performed by the Hvidørestudy group on childhood diabetes.
Metabolic control in Danish children andadolescentsThe two Danish studies were conducted in 1988 and 1990
(4, 5). Each study included approximately 1000 young type1 diabetes patients, 350 children below 12 y and 700adolescents aged 12–19 y. These patients were treated at22 paediatric departments, representing approximately80% of all children and adolescents with type 1 diabetesin Denmark. HbA1c (centrally determined). Insulin doseincreased during maturation of both genders and blood-glucose control in this period was not satisfactory eventhough a large percentage (60%) was on three or moreinsulin injections daily (Table 1). No differences in HbA1c
were observed in children treated with two, three, four ormore insulin injections daily (8).
Elevated overnight albumin excretion rate
During the 1990 study, persistent microalbuminuria wasfound in 4.3% of 957 Danish children and adolescents(aged 2–19 y) with type 1 diabetes and mean diabetesduration of 6 y (5). Based on recent literature, the preva-lence of microalbuminuria in paediatric populations variesfrom 4.3 to 20% (9–12). The discrepancies in the preva-lence of persistent microalbuminuria found in these studiesmay partly be explained by differences in age, blood-glucose control, the populations investigated and thescreening procedure used in these studies. However,during the past decade, a declining incidence of nephro-pathy in type 1 diabetes has been observed (13). Micro-albuminuria is seldom seen before puberty. Thus, screeningfor microalbuminuria need only be recommended in pae-diatric care after 12 y of age. It still remains controversial
Acta Pædiatr Suppl 425: 72–6. 1998
q Scandinavian University Press 1998. ISSN 0803-5326
whether diabetes duration per se is associated with raisedurinary albumin. Some studies have shown a possibleassociation (5, 14), while others dispute this finding (15).This may indicate that young people should be screenedfor microalbuminuria regardless of diabetes duration,beginning at the first stage of puberty.
Among the adolescents with microalbuminuria, 60%had diastolic blood pressure (DBP) in the upper quartilefor DBP among adolescents with normoalbuminuria. Theonly variables associated with a significant effect onelevated urine albumin excretion were age and DBP (16).
International survey on HbA1c and insulintreatmentThis investigation (6) involved 22 paediatric departments
from 18 countries in Europe, Japan and North America, andaimed to evaluate insulin regimens and metabolic control(centrally determined HbA1c) in children and adolescentswith type 1 diabetes. The study included a total of 2873children (1443M, 1430F), with a median age of 13 y (range1–18 y), representing approximately 70% of all childrenand adolescents treated at the centres.
Blood-glucose control
The survey found a mean HbA1c of 8.6% (equivalent to8.3% in the DCCT) in these young people (6). This com-pared with the DCCT results in adolescents, in which theintensive treatment group had a mean HbA1c of 8.1% vs9.8% in the conventional treatment group (7). Among thechildren in the study (age 0–11 y), 41% had HbA1c valuesbelow 8.0%. By contrast, among adolescents (aged 12–18y) only 29% had HbA1c values below 8%, despite the factthat 38% of this group were on three or more insulininjections daily, i.e. a similar proportion to the wholestudy population.
Centre differences
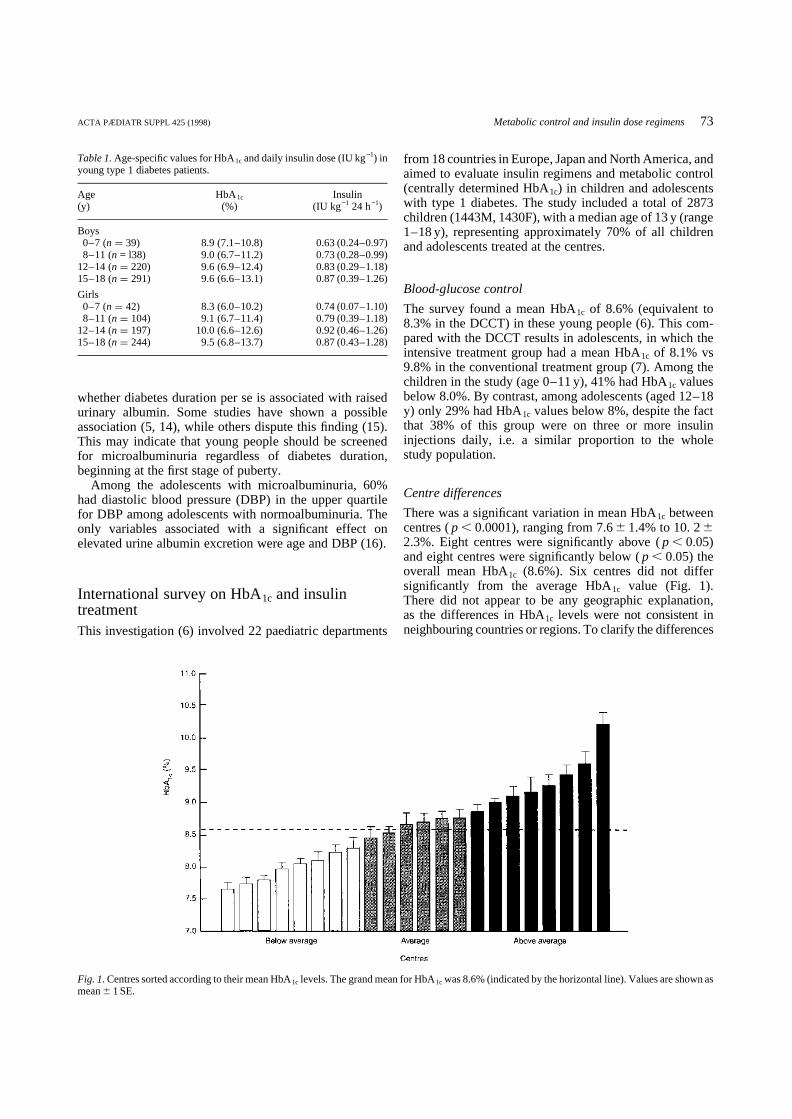
There was a significant variation in mean HbA1c betweencentres (p , 0:0001), ranging from 7.66 1.4% to 10. 262.3%. Eight centres were significantly above (p , 0:05)and eight centres were significantly below (p , 0:05) theoverall mean HbA1c (8.6%). Six centres did not differsignificantly from the average HbA1c value (Fig. 1).There did not appear to be any geographic explanation,as the differences in HbA1c levels were not consistent inneighbouring countries or regions. To clarify the differences
ACTA PÆDIATR SUPPL 425 (1998) Metabolic control and insulin dose regimens73
Table 1.Age-specific values for HbA1c and daily insulin dose (IU kg−1) inyoung type 1 diabetes patients.
Age HbA1c Insulin(y) (%) (IU kg−1 24 h−1)
Boys0–7 (n ¼ 39) 8.9 (7.1–10.8) 0.63 (0.24–0.97)8–11 (n = l38) 9.0 (6.7–11.2) 0.73 (0.28–0.99)
12–14 (n ¼ 220) 9.6 (6.9–12.4) 0.83 (0.29–1.18)15–18 (n ¼ 291) 9.6 (6.6–13.1) 0.87 (0.39–1.26)
Girls0–7 (n ¼ 42) 8.3 (6.0–10.2) 0.74 (0.07–1.10)8–11 (n ¼ 104) 9.1 (6.7–11.4) 0.79 (0.39–1.18)
12–14 (n ¼ 197) 10.0 (6.6–12.6) 0.92 (0.46–1.26)15–18 (n ¼ 244) 9.5 (6.8–13.7) 0.87 (0.43–1.28)
Fig. 1.Centres sorted according to their mean HbA1c levels. The grand mean for HbA1c was 8.6% (indicated by the horizontal line). Values are shown asmean6 1 SE.

among centres, further work is needed to compare interna-tional childhood data prospectively and to investigatewhether there are cultural or socioeconomic differencesin the choice of treatment regimen in the countries withsignificantly different mean HbA1c levels.
Hypoglycaemic events
The frequency of severe hypoglycaemia (loss of conscious-ness/seizures) of 22 events per 100 patient-years is similarto that reported in the DCCT for adolescents on conven-tional treatment (7). The risk of development of severehypoglycaemia was associated with a decrease in HbA1c
levels. The increased incidence of severe hypoglycaemicepisodes observed in the younger children (60 events per100 patient-years) indicates that tight control in this agegroup should be undertaken with extreme caution, ashypoglycaemia may impair normal brain development(17). In children below 8 y of age it may be safer to aimfor less tight blood-glucose control. No significant differ-ences in the incidence of hypoglycaemia could be shownfor centres (discussed above) with a mean HbA1c signifi-cantly below or equal to the grand mean for the study(Table 2). This finding may reflect the ability of thesecentres to improve HbA1c levels in their poorly controlledpatients rather than lowering the HbA1c in all patients.
The glycaemic targetThe DCCT and other studies have shown an associationbetween better metabolic control and a significant reduc-tion in the risk of developing microvascular complications(18). The European insulin-dependent diabetes mellitus(IDDM) policy group (19) has recommended that HbA1c
should be below 6.5% for adults, but whether such a lowlevel should be the aim in children is debatable in view ofthe increased risk of hypoglycaemia with low HbA1c levels(6). Most importantly, HbA1c values cannot be readilytranslated from laboratory to laboratory, so quoting abso-lute values is futile and potentially dangerous. However,until further studies are able to establish a suitable targetHbA1c level for children, the value (8.1%) obtained by theintensive treatment group of adolescents in the DCCTwould seem to be a good starting point.
Insulin regimens and insulin types
A mixture of short- and intermediate-acting insulin is themost commonly used combination in children on two, threeor more insulin injections daily (Fig. 2). The next mostpopular combination (short-acting and premixed insulin) ismainly used in children on a three-times daily regimen.When premixed or intermediate insulin is given alone, thisis almost exclusively to children on one or two injectionsper day. In this study, 60% of the patients were on twice-daily insulin, most of which was premixed insulin. Pre-mixed insulin is commonly used in the prepubertal years,presumably because of its ease of use and the fact that manystudies have failed to show significant differences betweenfixed insulin mixtures and variable mixtures (20). In addi-tion, premixed insulin might avoid the risk of error whenparents or patients mix the insulins themselves. The gly-caemic control in preadolescent children on premixedinsulin appeared to be comparable to that in those on avariable combination of short- and long-acting insulin.However, the potential benefit of individual self-adjust-ment of the ratio of short- and intermediate/long-actinginsulin became apparent in the adolescent subgroup, wherepremixed insulin was associated with significantly poorercontrol.
Infants, toddlers and young diabetic patients were trea-ted with significantly less short-acting insulin than olderchildren, possibly because of residualb-cell function (21)or for fear of inducing severe hypoglycaemic attacks.Adolescent boys treated with more daily units of short-acting insulin had significantly lower HbA1c levels thanthose on more units of long-acting insulin. In a follow-upstudy of former DCCT participants (22), a higher bolus:-basal insulin ratio was correlated with lower HbA1c values.
Quality of lifeIn a recent Danish study of attitude and behaviour in
74 HB Mortensen ACTA PÆDIATR SUPPL 425 (1998)
Table 2.Incidence of hypoglycaemia (unconsciousness or seizures) duringthe 3-month observation in the 8 centres with HbAlc levels below andabove average, and the 6 centres with HbAlc levels around the grand mean(8.6%).
Incidence ofFrequency hypoglycaemiaof events Number of (number per 100
Centre class (3 months) patients patient-years)
Below average 50 916 21.8Average 48 667 28.8Above average 58 1224 19.0
Fig. 2.Relationship between insulin types and injection frequency in 2857children and adolescents with type 1 diabetes. Six patients were notreceiving insulin and 10 used an infusion pump.

adolescent type 1 diabetes patients (23), it was demon-strated that poor metabolic control (as assessed by HbA1c)affected the psychosocial well-being of an individual,which may lead to problems with daily diabetes manage-ment. Improvements in metabolic control can be achievedby the use of intensive diabetes management (18), althoughit is important to select patients for such regimens carefully.These regimens are difficult to learn, involve multipleinjections and frequent blood-glucose measurements andrequire considerably increased resources. Such manage-ment also resulted in more hypoglycaemic events andincreases in body weight. This weight gain, an undesirableby-product of a strict regimen, might influence the typicalteenager’s compliance or adherence (24). Girls, in parti-cular, may omit insulin doses in attempts to control weight.Selected candidates for intensive diabetes management,therefore, are highly motivated and have no phobiaabout needles, with good support from family and friends(25) and an excellent diabetes education. By contrast,adolescents with significant family dysfunction, poor com-pliance, recurrent diabetic ketoacidosis and severe eatingdisorders should not be considered suitable candidates forintensive regimens. Most of these patients are not moti-vated to achieve tight metabolic control and are unwillingor unable to participate actively in their glucose manage-ment, which is a major factor in the multiple daily insulinregimen. Alternatively, in cases of long-term poor glycae-mic control due to poor adherence to insulin treatment (26),these children will often benefit from twice-daily insulin,which in many situations will improve their HbA1c valuesconsiderably. Thus, poor metabolic control per se is notnecessarily an indication for a more intensive insulin ther-apy regimen. Further analysis of the DCCT results inadolescents (27) suggested that supportive behaviouraltherapy over a long period in compliant patients was themain factor in obtaining good control.
ConclusionsChildren and adolescents should be treated in collaborationwith a team of health-care professionals including educa-tors, nurses, dieticians, mental health professionals, socialworkers and diabetologists. To prevent microvascularcomplications, it is necessary to develop managementguidelines and quality-assessment programmes for child-hood and adolescence with a view to reaching optimalmetabolic control in a greater proportion of young peoplewith diabetes.
References1. Krans HMJ, Porta M, Keen H, editors. Diabetes care and research in
Europe: the St Vincent Declaration action programme. WHO Regio-nal Office for Europe, 1992 (unpublished document EUR/ICP/CLR055/3. Available on request from the WHO Regional Office forEurope, Geneva)
2. International Society of Pediatric and Adolescent Diabetes (ISPAD).Declaration of Kos. Diabetes Young 1994; 30: 14
3. Consensus Guidelines for the Management of Insulin-dependent(Type 1) Diabetes Mellitus (IDDM) in Childhood and Adolescence.International Society of Pediatric and Adolescent Diabetes (ISPAD)and International Diabetes Federation (European Region, 1995).London: Freund Publishing House, 1995
4. Mortensen HB, Hartling S, Petersen KE and the Danish Study Groupof Diabetes in Childhood. A nationwide cross-sectional study ofglycosylated haemoglobin in Danish children with Type 1 diabetes.Diabetic Med 1988; 5: 871–6
5. Mortensen HB, Marinelli K, Nørgaard K, Main K, Kastrup KW, IbsenKK, et al. and the Danish Study Group of Diabetes in Childhood. Anationwide cross-sectional study of urinary albumin excretion rate,arterial blood pressure and blood glucose control in Danish childrenwith Type 1 diabetes mellitus. Diabetic Med 1990; 7: 887–97
6. Mortensen HB, Hougaard P for the Hvidøre Study Group on Child-hood Diabetes. Comparison of metabolic control in a cross-sectionalstudy of 2,873 children and adolescents with IDDM from 18 coun-tries. Diabetes Care 1997; 20: 714–20
7. The Diabetes Control and Complications Trial Research Group.Effect of intensive diabetes treatment on the development and pro-gression of long-term complications in adolescents with insulin-dependent diabetes mellitus. J Paediatr 1994; 125: 177–88
8. Mortensen HB, Villumsen J, Vølund Aa, Petersen KE, Nerup J andthe Danish Study Group of Diabetes in Childhood. Relationshipbetween insulin injection regimen and metabolic control in youngDanish Type 1 diabetic patients. Diabetic Med 1992; 9: 834–9
9. Mathiesen ER, Saurbrey N, Hommel E, Parving H-H. Prevalence ofmicroalbuminuria in children with Type 1 (insulin-dependent) dia-betes mellitus. Diabetologia 1986; 29: 640–3
10. Nørgaard K, Storm B, Graa M, Feldt-Rasmussen B. Elevated albuminexcretion and retinal changes in children with Type 1 diabetes arerelated to long-term poor blood glucose control. Diabetic Med 1989;6: 325–8
11. D’Antonio JA, Ellis D, Doft BH, Becker DJ, Drash AL, Kuller LH,et al. Diabetic complications and glycemic control. The Pittsburghprospective insulin-dependent diabetes cohort study status report after5 yr of IDDM. Diabetes Care 1989; 12: 694–700
12. Joner G, Brinchmann-Hansen 0, Torres CG, Hansen KF. A nation-wide cross-sectional study of retinopathy and microalbuminuria inyoung Norwegian type 1 (insulin-dependent) diabetic patients. Dia-betologia 1992; 35: 1049–54
13. Bojestig M, Arnqvist HJ, Hermansson G, Karlberg BE, Ludvigsson J.Declining incidence of nephropathy in insulin-dependent diabetesmellitus. N Engl J Med 1994; 330: 15–8
14. Rudberg S, Ullman E, Dahlquist G. Relationship between earlymetabolic control and the development of microalbuminuria – alongitudinal study in children with Type 1 (insulin-dependent) dia-betes mellitus. Diabetologia 1993; 36: 1309–14
15. Stephenson JM, Fuller JH, the EURODIAB IDDM ComplicationsStudy Group and the WHO Multinational Study of Vascular Diseasein Diabetes Study Group. Microalbuminuria is not rare before 5 yearsof IDDM. J Diabetes Complications 1994; 8: 166–73
16. Mortensen HB, Hougaard P, Ibsen KK, Parving H-H and the DanishStudy Group of Diabetes in Childhood. Relationship between bloodpressure and urinary albumin excretion rate in young Danish Type 1diabetic patients: comparison to non-diabetic children. Diabetic Med1994; 11: 155–61
17. Rovet JF, Ehrlich RM, Czuchta D, Akler M. Psychoeducationalcharacteristics of children and adolescents with insulin-dependentdiabetes mellitus. J Learn Disabil 1993; 26: 7–22
18. The Diabetes Control and Complications Trial Research Group. Theeffect of intensive treatment of diabetes on the development andprogression of long term complications in insulin-dependent diabetesmellitus. N Engl J Med 1993; 329: 977–86
19. JE Asvall, W Mayes, HMJ Krans, editors. Consensus guidelines forthe management of insulin-dependent (Type 1) diabetes. EuropeanIDDM Policy Group. Bussum, The Netherlands: Medicom EuropeBV, 1993
ACTA PÆDIATR SUPPL 425 (1998) Metabolic control and insulin dose regimens75

20. McEvilly EA, Eccles L, Rayner PHW. An assessment of the benefitsof premixed insulins in childhood diabetes. Practical Diabetes 1990;7: 122–4
21. Couper JJ, Hudson L, Werther GA, Warne GL, Court JM, HarrisonLC. Factors predicting residualb-cell function in the first year afterdiagnosis of childhood type 1 diabetes. Diabetes Res Clin Pract 1991;11: 9–16
22. Bergenstal R, Callahan P, Johnson M, Upham P, Hollander P, SpencerM, et al. Management principles that most influence glycemic control:a follow-up study of former DCCT participants. Diabetes 1996; 45(Suppl 2): 124 (Abstract)
23. Olsen B, Sander S, Nellemann D, Mortensen HB and the DanishStudy Group of Diabetes in Childhood. Treatment of young peoplewith diabetes. An attitude and behaviour study. J Pediatr EndocrinolMetab 1996; 9 (Suppl 2): 64 (Abstract)
24. Daneman D. Can eating disorders in adolescence be prevented? HormRes 1998; in press
25. La Greca AM, Auslander WF, Greco P, Spetter D, Fisher BE Jr,Santiago JV. I get by with a little help from my family and friends:adolescents’ support for diabetes care. J Ped Psychol 1995; 20: 449–76
26. Morris AD, Boyle DIR, McMahon AD, Greene SA, MacDonald TM,Newton RW for the DARTS/MEMO Collaboration. Adherence toinsulin treatment, glycaemic control, and ketoacidosis in insulin-dependent diabetes mellitus. Lancet 1997; 350: 1505–10
27. Greene SA. Diabetes in the young; current challenges in their man-agement. In: Shield JPH, Baum JD, editors. Ballie`re’s clinical pae-diatrics. London: Ballie`re Tindall, 1996; 4: 563–74
76 HB Mortensen ACTA PÆDIATR SUPPL 425 (1998)