povezanost posttraumatskog stresa i kvaliteta … · 2009-09-07 · vise; kronbah alfa koeficijent...
TRANSCRIPT
PSlhijai. dan./2005/J7/2/289-295/Jm/ko"ic GmnlOVJC J. POI·e:alJasl postlraumalskog S{r('$111 halite/a !i;·ota...
289
/slrativatki rad
UDK: 616. 89·008. 44{: 355.48(497.Jlj"1999··
POVEZANOST POSTTRAUMATSKOG STRESAI KVALITETA ZIVOTA KOD GRADANA
POSLE VAZDUSNlH NAPADA
Jclcna Jankovic Gavrilovic1.2, Dusica Lccic Tosevski,Olga Colo"ie, Sara Dimie, Veselinka Susie3
,
Milica Pejovic Milovaoi:evie,Smiljka Popo"ic Deusie2
, Stefan Priebe'
I Odeljenje za socijalnu i komunalnu psihijatriju Barts i Medicinski fakultetQueen Mary u Londonu, London, Velika Britanija
2 Inslitut za rnentalno zdravlje, Beograd, Srbija i Cma Gora3 Srpska Akademija nauka i umetnosti, Srbija i Crna Gora
Apstrakt: lako su halilet zivota i posnraumatski sITes detaljno prou~avani, njih(J\'mcdusobni odnos je retko ispitivan. Ovo istrtlhvilnje prouCava odnos izmedu posttfilumatskog~lrcsa i kvalitcta zivota u rclativno homogenoj i neselektivnoj g.rupi gradana koji su bili izlozeni vazdu~nim napadima. K\"alitel fivola (MANSA), posttraumatski SlTes (IES) i depresija/anskio/J10Sl (SCL-90-R) ispitivani su kod d\"e grupe studenata medicine (N1=139. N2=475)posle jednc. odnosno. d\'e godinc v37.du~njh n3pada u Srbiji i Cmoj Gori. RC7.ultati pokazujuSl;lbu do srednjc lzrazenu \·czu izmedu posltraumatskog stresa i subjektivnog d07jvljaja kvalilela :"(ivma. Nakon ispilivanja sleptna tleprcsivnosli i anksiozllosti, jcdino jc veza izmcdu postlraumatskog siresa i zadovoljstva memalnim zdravljem statisli~ki zna~ajna u obema grupama.(:ini se da anksioznOSI i dcprcsij<l imaju ulicaja - u vclikuj mcri, ali nc potpuno, na vezu izmcdu p0S11raumalskog stresa i Jj~nog do:bvljaj3 kvaliteta .tivota.
KJju~ne reci: pOSllraumulski sIres. kvafirel i;vota. vazduIni napadi. gradcmi
290 PSlhI)QI. dan./100JJj7/1/}1I9·195/JunACJ\"lc GO\'ril<:wii: J. PO"UOIIOll posftraumalJkog s{rcsa i kvuiJlel<t ;:1\'<110...
UvodKancept kvaliteta zivotaje 5ve popularniji u psihijatrijskim istraziva
njima 1I poslednje dye decenije [lJ i postoji dasHl literature koja se odnosi nakvalite! iivota razlicitih grupa psihijatrijskih pacijenata [2]. lako ne postoji definicija kvaliteta fivota koja je univerzalno prihvacena [31. vetina strucnjaka scslaie da postoje subjektivni i objektivni pokazatclji kvaliteta fivota i da su subjcktivni ani koji Sll kljucni. Koncept subjcktivnog kvaliteta fivota - dalje utekstu sK1 (subjective quality of life - SQOL) fokusira sc oa individualnu percepciju i procenu kvaliteta njegovog iii njcnog kvaliteta iivota [4,5]. U procenikvaliteta zivota koristi se veliki broj skala - od ouill koje se odnose na zdravlje,preko onih koje su speciticne za bolest, do opstih. U psihijatrijskim istraiivanjima,u skladll sa opstim konceptom, kao indikatori SK.Z ustanovljcni su proccna zadovoljstva iivotom II cehni i procena zadovoljstva spccificnim aspcktima iivota [6].
U opstoj populaciji, kao i u uzorku pacijenata, simptomi raspolo:l.cnjaoznaceni su kao najznacajniji i stalni cinioci koji uticu na sKl. Razlicita istrazivanja pokazuj~ niie rezultate SKl kod ispitanika sa viSim stepenom dcpresivnih simptoma [7,8,9]. Zbog toga treba kontrolisati uticaj simptoma raspolozcnja prilikom. procene SK2:. Pa ipak, opsta varijansa izmectu simptomaraspoloienja i SKZ rctko prelazi 25% i sKl se ne moze smatrati pratecompojavom dcpresivnih simptoma [5].
lako postoji obimna literatura 0 posttraumatskom stresu i kvalitctuzivota, mali broj istraiivanja proucava vezu izmcdu ova dva pojma [4,10].Ovo je u sllprotnosti sa definicijom posttraumatskog stresnog porcmccaja II
DSM IV koja navodi uticaj dnlstvenog funkcionisanja kao kriterijum dijagnoze. Koncept drustvenog funkcionisanja razlicitje od kvaliteta iivota, ali scprcklapa sa njim i u vezi je sa njim. Osim loga, pokazalo se da kod generalizovanog anksioznog poremecaja i nakon utvrdivanja postojanja psihapatolo~kih fenomena, postoji visok stepen astecenja. Rezultati Nacionalne vijctnamske studije 0 ponovnom prilagodavanju veterana muskog i icnskog pala,pokazuje ua su ispitanici sa PTSP imali znacajno povisen rizik od smanjenogfunkcionisanja u razlicitim aspektima i.ivota [12,13 J. Najveci broj retkih istrazivanja koja se bave kvalitetom zivota i mentalnim zdravljem posle steesnag dogadaja posmatrala su iIi psihijatrijske pacijente iIi veterane. ZdraviIjudi retko su bili sistemalski ispilivani.
U ovom istrazivanju posttraumatski sires ispitivan je u dye relativnohomogene i neseleklivne grupe studenata medicine, nakon jedne i nakon dyegod inc ad vazdusnih napada na Beograd.
Napadi su trajali od 24. marta do 9.juna 1999. godine, izvodili su seskoro svakc noci i uzrokovali su civilne ;lrtve sirom Srbijc i erne Gore. Proccnjujc sc jc dajc broj civilnih irtava iznosio ako 1,200 [14].
avo istrazivanjc postavlja sledeca pitanja:1. Kakva jc povezanost posttraumatskog stresa i kvaliteta fivota?2. Oa Ii u ovoj povezanosti posreduju silllptomi anksioznosti i depre
sivnosti?
f$iltijOI, ria" 110051J71212S9-}951Jankol"c Gavnlol'lc J. l'ovcomllr posrlrolilltOlskog srresa I halUtta tll'o/a...
291
MetodUzorakGrupa A sastoji se od 139 ad ukupno 141 studenta cetvrte godine
Medicinskog fakulteta koji prate nastavu u jednoj psihijatrijskoj ustanovi uBeogradu (95 iena, 44 muskaraca), starosti izmedu 21 i 28 godina (srednjavrcdnost 23.8 god.; SO= J.3). U vreme izvodenja istraiivanja, u prolece 2000.godine, oko godinu dana oakon vazdusnih napada, cetvoro studenata zivelojc sa partnerom i niko od njih nije imao decu. Nivo posttraumatskog stresa,naCini za prevazilaienje stn:sa i licoe osobine ove grupe prikazanc su oa drugom mes[U [14,15,16].
Grupa B sastoji se od 475 od oko 600 studenata druge godine medicine koji slusaju nastavu na Institutu za fIziologiju Medicinskog fakulteta uBeogradu (334 zene i 141 muskarac), starosti izmedu 20 i 29 godina (srednjavrednost 21.1 god.; SD;;=Q.7). U vreme izvodenja istraiivanja, u prolece 2001.godine, ako dye godine nakon vazdusnih napada, sest studenata zivelo je sapartnerom, i cetvoro od njih imalo je decu.
Svi ispitanici bili su izlozeni vazdusnim napadima, tokom proleca1999, kao civili. Posto je nezavisni istrazivac predstavio ciljeve istrazivanjastudentima, dobijen je pristanak za istraiivanje.
InstrumentiKvalitet zivota ocenjivan je pomocu Kratke Mancesterske skale za
procenu kvaliteta Zivota (Manchester Short Assessment of Quality of Life MANSA) [18]. MANSA je kratka skala za procenu opsteg nivoa kvalitetazivota koja se koristi u mnogim ispitivanjima mentalnog zdravlja. Ova skalaima slienosti sa lntervjuom 0 kvaliteru zivota [19,20] i Lankasirskim profi10m kvaliteta iivota (Lancashire Quality of Life Profile - LQLP), ali je iI1mogo prcciznija od njih [21]. Sve ove skale imaju isti koncept i veoma slicoa pitanja koja se tieu zadovoljstva, llkljueujuci i skalu od I do 7, na kojoj Ioznaeava nepovoljni pol, a 7 povoljni pol. Nezavisno od prikupljanja podataka ° licnim detaljima i abjektivnim okolnostima iivota, MANSA sadrii sesnacst pitanja od kojih se ~etiri smatraju "objektivnim", a ostalih dvanaest suprocena zadovoljstva zivotom II celini i u speeificnim podrucjima iivota. Korelacije izmedll sKi zbira na upitnicima MANSA i LQLP bile su 0.83 iiivise; Kronbah alfa koeficijent za Dcenu zadovoljstva bio je 0.74, a udruienost sa psihopatologijom je bila u skladu sa rezultatima dobijenim na LQLP,bo sto se i navodi u literaturi [18].
Primenjena je Skala uticaja dogadaja (The Impact of Event Scale IES) [21], upitnik od petnaest stavki, koji meri simptome posttraumatskogstresa, nametanje i izbegavanje.
Anksiozni i depresivni simptomi proccnjivani su Preglednom listomsimptoma (Symptom Checklist 90-R ~ SCL-90-R9) - instrumentom od devedesct stavki za samoproccnu opstc psihopatologije oa deset subskala [22].
292 1'~ihijQ/. dall./200j/J7/211lJ9-295/Janko\-;c Gtn"rdOI";c.J PrJYe:anosl posllraumu{slwg Slre.fa I h'uiJlI:l<I :ivota.. ,.
StalisTicka analizaT-teSl i Pirsonov koeficijent korclacijc kori~ccl1j su da bi sc ispitala
veza izmedu SKZ i posttraumatskog stresa. U slcdcccm karaku, bivarijantnekorelacije koje su dosligle stalisticku znacajnost proveravane su Uodnosu oaanksioznost i simptome depresivnosti taka sto su izracunavani parcijalni koeficijenti korelacije, eliminisuci uticaj anksioznosti i depresivnosli oa rczultateIES i SQOL. Kako bi se smanjila greska I lipa a priori izracunavali smo parcijalne koeticijente sarno kada je bivarijanlna korelacija bila znacajna.
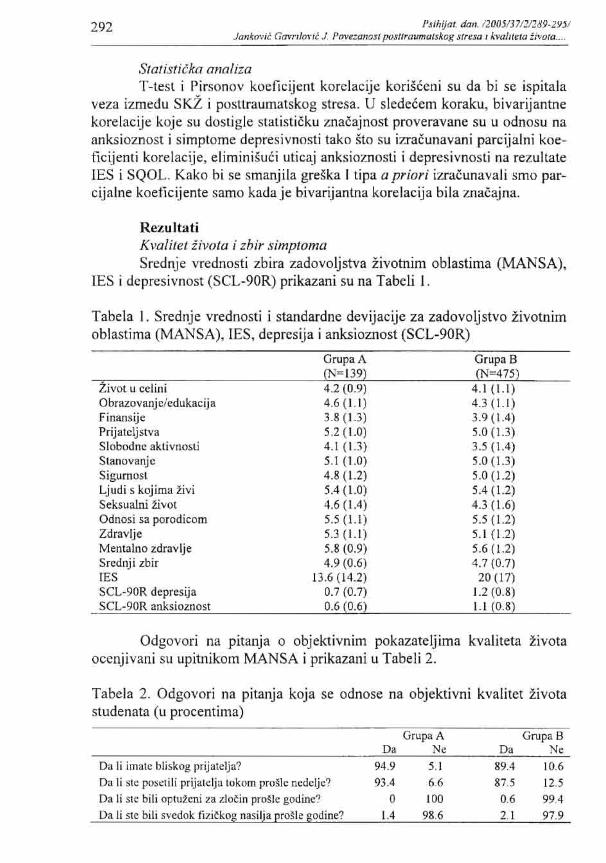
RezultatiKvalitet iivo/a i zbir simplomaSrednje vrednosti zbira zadovoljstva zivotnim oblastima (MANSA),
JES i depresivnost (SCL-90R) prikazani su na Tabeli I.
Tabela I. Srcdnje vrcdnosti i standardnc dcvijacije za zadovoljstvo fivotnimoblastima (MANSA), lESt dcprcsija i anksioznost (SCL-90R)
fivot u ccliniObrazovanj c/cdukacij aFinansijcPrijalcljsrvaSlobodnc aktivnostiStanovanjcSigunJoslLjudi 5 kojima ZiviSeksualni fivotOdnosi sa porodicomZdravljeMentalno zdravljeSrednji zbirIESSCL·90R depresijaSCL-90R anksioznost
GrupaA(N=139)4.2 (0.9)4.6(1.1)3.8 (1.3)5.2 (1.0)4.1(1.3)5.1(1.0)4.8 (1.2)5.4(1.0)4.6 (1.4)5.5 (1.1)5.3(1.1)5.8 (0.9)4.9 (0.6)
13.6 (14.2)0.7 (0.7)0.6 (0.6)
Grupa B(N=475)
4.1 (1.1)4.3 (1.1)3.9 (1.4)5.0 (1.3)3.5 (1.4)5.0 (1.3)5.0 (1.2)5.4 (1.2)4.3 (1.6)5.5(1.2)5.1 (1.2)5.6 (1.2)4.7 (0.7)
20 (17)1.2 (0.8)L.I (0.8)
Odgovori na pitanja 0 objektivnim pokazatcljima kvalitcta fivotaocenjivani su upitnikom MANSA i prikazani u Tabeli 2.
Tabela 2. Odgovori na pitanja koja se odnose na objektivni kvalitet zivotastudcnata (li procentima)
Oa Ii imale bliskog prijalclja?
Oa Ii SIC poseliJi prijalclj:l tokom proSlc ncdc1jc?
Da Ii SIC bili optuicni za zlotin prostc godinc?
Oa Ii SIC bili svcdok fizi~kog nasilja pro~tc godine?
GrupaAOa Nc
94.9 5.1
93.4 6.6
o 1001.4 98.6
Grupa BOa Ne
89.4 10.687.5 12.5
0.6 99.4
2.1 97.9
PJ/hijat. da". /2IJIJj/J7/2/289-29J1Jankovic G"",ilOl,jC J. PO"e:onos/ posllrrmmal.Jlwg JlreJa i halueta :wota...
293
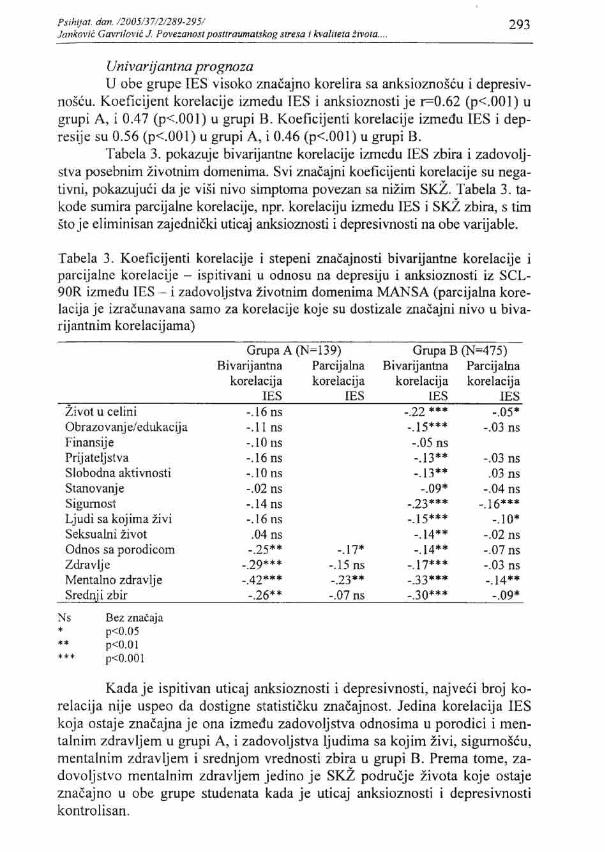
Univarijanlna prognozaU obe grupe IES visoko znacajno korelira sa anksioznoscu i depresiv
noseu. Koefieijent korelacije izmedu IES i anksiomosti je r=O.62 (p<.OO I) ugrupi A, i 0.47 (p<.OOI) u grupi B. Koeficijenti korelacije izmedu IES i depresijc su 0.56 (p<.OO I) u grupi A, i 0.46 (p<.OO I) u grupi B.
Tabela 3. pokazuje bivarijantne korelaeije izmedu I£S zbira i zadovoljstva posebnim iivotoim domenima. Svi znacajni koeficijenti korelacije su negativni, pokazujuCi da je visi nivo simptoma pove-/..an sa niiirn SKZ. Tabela 3. takode sumira parcijalne korelacije, opr. korelaciju izmedu IES i SKZ zbira, s timsto jc cIiminisan zajcdnicki uticaj anksiozilosti i deprcsivnosti na abe varijable.
Tabela 3. Koeficijenti korelacije i stepeni zna~ajnosti bivarijantne korelacije iparcijalne korclacije - ispitivani U odnosu ua depresiju i anksioZllosti iz SCL90R izmedu IES - i zadovoljstva fivotnim domenima MANSA (parcijalna korelacija jc izracuoavana samo za korelaclje koje su dostizale znacajni nivo u bivarijaotnim korclacijama)
Grupa A (N 139) Grupa B (N 475)
Zivot u celiniObrazovanjeledukacijaFinansijePrijateljstvaSiobodna aktivnostiStanov<lnjeSigumoslLjudi sa kojima tiviScksualni iivotOdnos sa porodicomZdravljeMentalno zdravljeSrednj i zbir
Bivarijantnakorelacija
lES-.16 ns-.1 [ os-.10 ns-.16 ns-.10 ns-.02 os-.14 ns-.16 ns.04 ns
·.25**-.29***-.42*·*
·.26**
Parcijalnakorelacija
IES
-.17*-.15 os-.23**-.07 ns
Bivarijantnakorelacija
rES-.22 ***-.15***-.05 ns-.13**-.13"**~.09*
-.23***-.15***-.14**·.14**
-.17***-.33***-.30***
Parcijamakorelacija
IES
~.03 ns.03 ns
-.04 ns-.16***
-.10*-.02 os-.07 os-.03 ns-.14**
-.09*
~,,.,..,
Bez znat:ljap<O.05p<O.OIp<O.OOI
Kadaje ispitivan uticaj anksioznosti i depresivnosti, najvcCi broj korclacija nije uspeo da dostigne statisticku znacajnost. Jedina korelacija JESkoja ostaje znacajna jc ona izmedu zadovoljstva odnosima u porodici i mentalnim zdravljem u grupi A, i zadovoljstva Ijudima sa kojim zivi, sigumo~cu,mentalnim zdravljem i srcdnjam vrednasti zbira u grupi B. Prema tome, zadovoljstvo mentalnim zdravljem jedino je sKi podrucje zivota koje oslajeznacajno u abe grupe studenata karla je uticaj anksioznosti i depresivnostikontrolisan.

294 PSlhyal. dun,/200S/37/1/189-29JIJallkm'ic Gg.,"n/m'''' J. PUl'f;a/W3I pt1Slfrtrumarskog Jlr<,sa i halltela ;1\'0111....
Sto se lite pokazatelja objektivnog kvaliteta zivota prikazanih u Tabcli 2, test za vezu sa IES pokazuje sarno jedan statisticki znacajan rczultat: ugrupi Bt studenti koji su bili zrtve fizickog nasilja, imali su visi IES zbir(t=2.44, df=471, p<.05).
DiskusijaVeza izmedu posttraumatskog strcsa i kvaliteta zivota ispitivana je II
dye grupe studenata. Uzorci su bili rclativno veliki, neselektivni i homogeni,liZ llvazavanje razlicitih cinilaca kao sto su uzrasl. obrazQvanje, i zaposlenost. Stoga nije bila potrebe da se kontrolisc uticaj lib cinilaca. Metodoloskasnaga istrazivanja je u tome sto su svi ispitanici bili izloicni istim stresogenim dogadajima, i vremenski interval izmedu dogadaja i ispitivanja u okvirusvake grupe bio je isti.
Nivo pottraumatskog stresa varira u okviru obc grupe i srcdnji SKZ.ie bio slican onome nadenom kod drugih neklinickih llzoraka [24]. Odslikavajuci njihovu homogenost u odnosu na zivotne okolnosti, uzroci pokazujuvrlo ograniceno ncslaganjc u odnosu na objektivne pokazatelje kvaliteta zivota. Varijablc sa tako malim niYoom neslaganja najverovatnije nlsu U znacajnoj korclaciji sa dnlgim parametrirna. Jedina statisticki znacajna veza kojusmo identifikovali jc visi lES zbir kod ispitanika koji su bili zrtve nasilja uposlednjih godinu dana. Iskustvo dozivljenog nasilja maze samostalno dauzrokuje posttraumatski stres, iii u kombinaciji sa delovanjem stresogenogdogadaja lokom vazdusnih napada. Neka istrazivanja ukazuju da izlaganjeveeem broju traumatskih iskustava povecava mogucnost odgovora II skladusa simptomima posttraumatskog strcsa [25].
U obe grupc postojala je korelacija slabe do srednje jacinc izmeduIES zbira i SKi: oecne. Zbog vceeg uzorka u grupi B, Yeci broj koefieijcnatakorelaeije dostigao jc statisticku znacajnost. Srcdnja vrednost zbira oecnezadovoljstva moze sc posmatrati kao najpouzdanija vrednost SKi; skora 1"121.Postojalajc sugeslija da se, osim 1I slucaju kada postoji speeificna hipoteza uodnosu na pojedinacno podrucje zivota, prvo testira srednja vrednost zbira.Sarno kada postoji znacajan rezultat u pogledu srednje vrednosti zbira trebaanalizirati i intcrpretirati rezultate za pojedina podrucja zivota. U obc grupcsrcdnja vrednost zbira zaista znacajno korclira sa lES i koefieijenti su slicneveJicinc. Veze su postojane, iako se srednjc vrednosti nivoa posttraumatskogstresa razlikuju izmedu dye grupc zbog razloga koje nismo u stanju da i.stra:limo na osnovu podataka sakupljenih prilikom iSlraiivanja.
Razlicit vrcmenski period izmedu stresogenog dogadaja i ispitivanja,tj. jedna godina nasuprot dye god inc, izgleda da nema kljucni uticaj na povezanost posttraumatskog stresa i SKi:. M~dutim, izgleda da je ova jasna povczanost - uglavnom, ali ne potpuno - pod uticajem simptoma anksioznosti idcpresivnosti. Posttraumatski stres moze biti povezan sa simptomima raspo·lozenja i anksioznosti za koje se zna da irnaju uticaj na oecnu sKi. Povezanost posttraumatskog stresa sa zadovoljslvom ispitanika sopstvenim mental·
PS11Jijul. dUrl./JOOJ/J7/2/289-29J/}lmko\';c GlJ\'Ti/o"ji;} Po,'e:mWSI pomTaum(llskog Slreso ; haliteta !i.'OIO...
295
nim zdravljem najjaca je u bivarijantnim testovima, i jedina jc koja ostajestatisticki znacajna u obe grupe nakon ispitivanja simptoma raspolo'ienja ianksiozllosti. Ova povezanost, takode, moze biti kvalitativno razlicita, tako daje prateci simptomi raspolozenja i anksioznosti ne mogu potpuno objasniti.
Nedostatak ovog istra:l:ivanjaje u prislupu poprecnog preseka, koji nedozvoljava da se izvedu zakljucci na osnovu uzrocne veze. Visi nivoi post~
traumatskog stresa, uglavnom posredovani depresivnoscu i anksioznoseu,uticu oa SKi: i, obrnulo, nizi sKi moze imati negativan uticaj na simptome.Buduee prospektivno longitudinalno istrazivanje trebalo bi da se bavi UZTOCnoseu.
ZakljucakRezultati ukazuju daje posttraumatski stres pavezan sa sKi u relativ
no homagenim i neselektivnim grupama gradana koji su doiiveli stresogen ipotencijalno traumatican dogadaj. Rezultati se slaz.u u dva nezavisna, ali slic~
na uzorka. S drugc stranc, trcbala bi ih ponoviti u drugim grupama iii kon~
tckstima.U budueim istrazivanjima bila bi korisnc ispitati pokazatclje kvalile~
ta iivota u uzorcima u kojima ispitanici imaju posttraumatski stres. Takvoispitivanje moze pokazati da sKi utice na pasttraumatski stres, iii je njegovarelcvantna poslcdica, iii i jedno i drugo, i identifikovati ulogu simptoma ras~
polozcnja u ovoj povczanosti. U svakom slucaju, simptomi anksiaznasti idcpresivnosti moraju sc smatrati ciniocima posredovanja. Priroda ove povezanosti jos llvek nijc jasna, i dalje sistematicno ispitivanjc, primenom kvanti~
tativnih i kvalitativnih metoda, ncophodno je za razumcvanje procesa koji suII korenu ovih povezanosti. Istrazivanja intervcncija nebala bi da ispitaju daIi terapijske intervencije primamo za cilj treba da imaju pobo.ijsanjc pasHra·umatskog stresa iii simptoma raspolozenja da bi uticali na sKZ, iii bi pobolj~
sani SKZ naknadno vodio do smanjenja nivoa anksioznosti, depresivnosti iposuraumatskog stresa.

P!1lhIJUI. dan.I2QOj!J712J297-JOjlJanKo,';" GQ\',"'Q\:ic. J. Auximion ofpoSllraumul,c JlreJJ l:md qual;ty aflife ...
297
Research article
UDK: 616. 89-008. 441 : 355.48f497. /1)"1999"
ASSOCIATION OF POSTTRAUMATIC STRESS ANDQUALITY OF LIFE IN CIVILIANS AFTER AIR ATTACKS
Jclena .Jankovic Gavrilovic1J, Dusiea Lecic Tosevski2
,
Olga Colovicz, Sara Dimicz, Veselinka SusieJ,
Milica Pejovic Milovancevic2,
Smiljka Popovic Deusic2, Stefan Priebe'
Unit for Social and Community Psychiatry, Barts and the London School ofMedicine, Queen Mary, University of London, United Kingdom
2The Institute of Mental Health, University ofBc1grade, Belgrade,Serbia and Montenegro
J Serbian Academy of Science and Art, Serbia and Montenegro
Abstract: Although qualit)· of life and poslIraumatic stress have been cxtensivelystudied, their relationship has rarely been investigated. This study explored the relationshipbetwecn posttmumatic stress and quality of life in - relatively homogeneous and nonselective - groups of ch'ilians who had been exposed 10 air attacks. Quality of life (MANSA),posttraumatic stress (IES), and depression and anxicty (SCL9Q-R) were assessed in twogroups of medical students (NI""139, N2"'415), onc and two years respectively after air attacks in Yugoslavia. Results show weak to moderatc associations between posttr<lumaticSlIess and subjective quality of life scores. After controlling for depression and anxiety, onlythe association between posttraumatic stress and satisfaction wilh mental health remains statistically significant in both groups. Anxicty and dcpression appear to mediate -largely, butnot fully. the association between posttraumatic stress and subjective quality of life.
Kc)' words: posttraumatic stress, quality oflife, air auocles. civilians
29K Psrhrjal. dan. 11005137111297-J051Jank(/~Ic GUm/OI'ie, J. Associarion ofposllraumulic stress ond qllaMy oflift!_.
IntroductionThe concept of quality of life has become increasingly popular in
psychiatric research over the last two dccndes [I], and there is a wide rangeof literature on quality of life findings in different groups of psychiatric patients 12"1. Although no single definition of quality of life has been univer·sally accepted [3], most experts agree that there are subjective and objectiveindicators of quality of life and that the subjective ones an: central. The concept of subjective quality of life (SQOL) centres on the individual's perception and appraisal of the quality of his or her own life [4,5]. Numerous scaleshave been used to assess quality of life and the constructs range from healthrelated and disease sped lie ones, to more generic ones. In psychiatric re·search, ratings of satisfaction with life as a whole and with different life do·mains have been established as indicators of SQOL in line with a genericconcept [6].
In the general population, as well as in patient samples. mood symptoms have been identified as the most significant and consistent factor intlu·encing SQOL. Various studies indicate lower SQOL scores in subjects withhigher degrees of depressive symptoms 17,8,9]. Thus, the influence of moodsymptoms should be controlled for in studies on SQOL. Yet, the commonvariance between mood symptoms and SQOL rarely exceeds 25%, andSQOL cannot be just regarded as an epiphenomenon of depressive symptoms[6].
Even though the literature on both posttraumatic stress and quality oflife is vast, there has been relatively little research on the association of thetwo [4,10]. This is despite the definition of Posnraumatic Stress Disorder inDSM IV that mentions impact on social functioning as a criterion for the di·agnosis. Social functioning is a concept different from, but related to andoverlapping with quality of life. In addition, it has been shown that generalanxiety disorder is associated with high impainnent even after controlling forother psychopathology [111. Research from the National Vietnam Readjust.ment Study, both of male and female veterans, showed iliat subjects withPTSD had significantly higher risk of diminished functioning in several aspects of life [12,13]. Most of the few studies on quality of life and mentalhealth after a stressful event were conducted either in psychiatric patients orveterans. Non.paticnt civilian groups have rarely been systematically stud·ied.
In this study, posttraumatic stress was assessed in two - relativelyhomogeneous and non·selective - groups of medical students, one year andtwo years after experiencing air anacks in Belgrade.
The attacks lasted from March 24 to June 9, 1999, occurred almostevery night during that period of time and resulted in casualties among civil·ians throughout Serbia and Montenegro. The number of civilian deaths hasbeen estimated at around 500 p 4].
I'sihijal. dan./2005/37/1/291-J05/J,mAoI'ic G-al'"hmc, J. AssrJ(:iGllon ojposllroumalic slress and quality ojiljl': ..
299
The study addressed the following questions:1. What is the association betv.reen posttraumatic stress and quality
of life?2. Is the association mediated through anxiety and depressive
symptoms?
MethodSampleGroup A consists of 139 out of 141 fourth year medical students in
one psychiatric teaching hospital in Belgrade (95 women, 44 men). The ageranged from 21 to 28 years (mean=23.8; SD 1.3). At the time of the study inspring 2000 approx. 1 year after the air attacks, four students lived with apartner and none had children [15]. The level of posttraumatic stress, copingstrategies and personality characteristics of this group are presented elsewhere [15,16,17].
Group B consists of 475 out of approximately 600 second year medical students taking a course at the Institute of Physiology in Belgrade (334women, 141 men). Their age ranged from 20 to 29 years (mean=21.1; SD0.7). At the time of the study in spring 2001 approx. 2 years after the air attacks, six students lived with a partner and four had children.
All of the subjects were medical students at the University of Belgrade's School of Medicine, and all had been exposed to air attacks as civilians in spring 1999.
After a complete description of the study by an independent researcher to the students, informed consent was obtained.
!nsh·umenfs
Quality of life was assessed on the Manchester Short Assessment ofQuality of Life [18]. The MANSA is a brief instrument for obtaining a ge~
neric construct of quality of life widely used in mental health service research. It is similar lO, but much more concise than the Quality of Life Interview [19,201, and the Lancashire Quality of life Profile (LQLP) [21]. All ofthese tools share the same concept and have very similar satisfaction questions including I to 7 rating scales with 1 being the unfavourable and 7 thefavourable end of the scale. Apart from collecting personal details and objective circumstances of life, the MANSA contains 16 questions of which fourare considered "objective" and 12 are ratings of satisfaction with life as awhole and different life domains. Correlations between SQOL scores onMANSA and LQLP were all 0.83 or higher; Cronbach's alpha for satisfactionratings was 0.74, and association with psychopathology is in line with resultsfor LQLP as reported in the literature [18].
300 PSlhijm. don 1200J/J7IZJZ97.JOj/Ja"lm"i(: Go·.,,/Ul'lc. J. ASSOC;lllum ofpomraumollc SlUSS and qualify oflife.
The Impact or Event Scale [22], a 15·items questionnaire that measures intrusion and avoidance symptoms of posttraumatic stress was administered.
Anxiety and depressive symptoms were self-rated on the SymptomChecklist 90-R [23] - a 90 items instrument for self-rating of general psychological symptoms on 10 sub-scales.
Statistical AnalysisT-tests and rearson's correlation coefficients were used to explore
the association between SQOL and posttraumatic stress. In a next step.bivariate correlations that reached statistical significance were controlled foranxiety and depressive symptoms by calculating partial correlation coerficients. with the influence of anxiety and depression on both IES and SQOLscores eliminated. In order to reduce Type 1 error a priori we calculat~d partial correlations only when the bivariate correlation was significant.
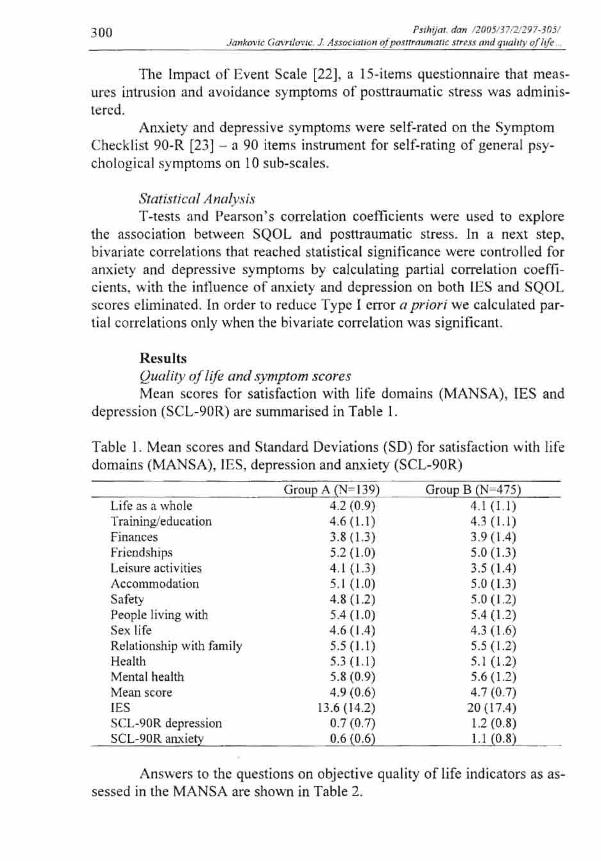
ResultsQuality oflife and symptom scoresMean scores for satisfaction with life domains (MANSA), lES and
depression (SCL-90R) are summarised in Table I.
Table 1. Mean scores and Standard Deviations (SD) for satisfaction with lifedomains (MANSA), IE5, depression and anxiety (SCL-90R)
Life as a wholeTrainingleduc<ltionFinancesFricndshipsLeisure activitiesAccommodationSafetyPeople living withSex lifeRelationship with familyHealthMental healthMean scoreIESSCL-90R depressionSCL-90R anxiety
Group A (N 139)4.2 (0.9)4.6 (L1)3.8 (1.3)5.2 (1.0)4.1 (1.3)5.1 (1.0)4.8 (1.2)5A (1.0)4.6 (1.4)5.5 (1.1)5.3 (1.1)5.8 (0.9)4.9 (0.6)
13.6 (14.2)0.7 (0.7)0.6 (0.6)
Group B (N 475)4.1 (L1)4.3(L1)3.9 (1.4)5.0 (1.3)3.5 (IA)5.0 (1.3)5.0 (12)SA (1.2)4.3 (1.6)5.5 (1.2)5.1 (1.2)5.6 (1.2)4.7 (0.7)20(17.4)1.2 (0.8)LI (0.8)
Ans\'iers to the questions on objective quality of life indicators as assessed in the MANSA arc shown in Table 2.
Psihifm don_/2005JJ7/2/297-305/JankJJ"'c GU'..,.,IO\·iC, J Ass(>t:ioliO" ofpoSllroumouc sIren rmd quality oflift
301
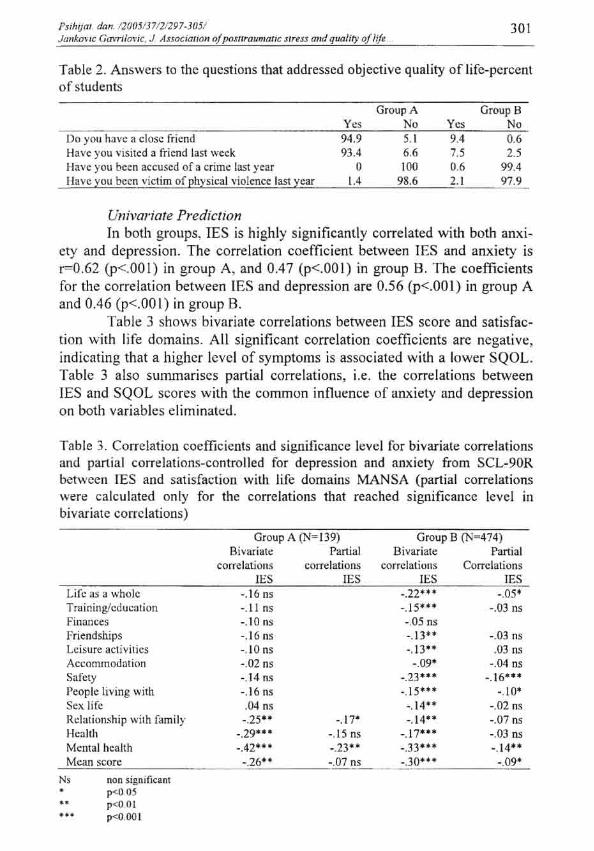
Table 2. Answers to the questions that addressed objective quality of life-percentof students
Do you have a close friendHave )'OU visited a friend last weekHave you been accused of a crime last yearI-lave you been victim of physical violence last year
Group AYes No94.9 5.193.4 6.6
o IOU1.4 98.6
Group BYes No9.4 0.67.5 2.50.6 99.42.1 97.9
Univariate PredictionIn both groups, IES is highly significantly correlated with both anxi
ety and depression. The correlation coefficient between IES and anxiety isr=0.62 (p<.001) in group A, and 0.47 (p<.OOl) in group B. The coefficientsfor the correlation between tES and depression are 0.56 (p<.OOl) in group Aand 0.46 (p<.OOI) in group B.
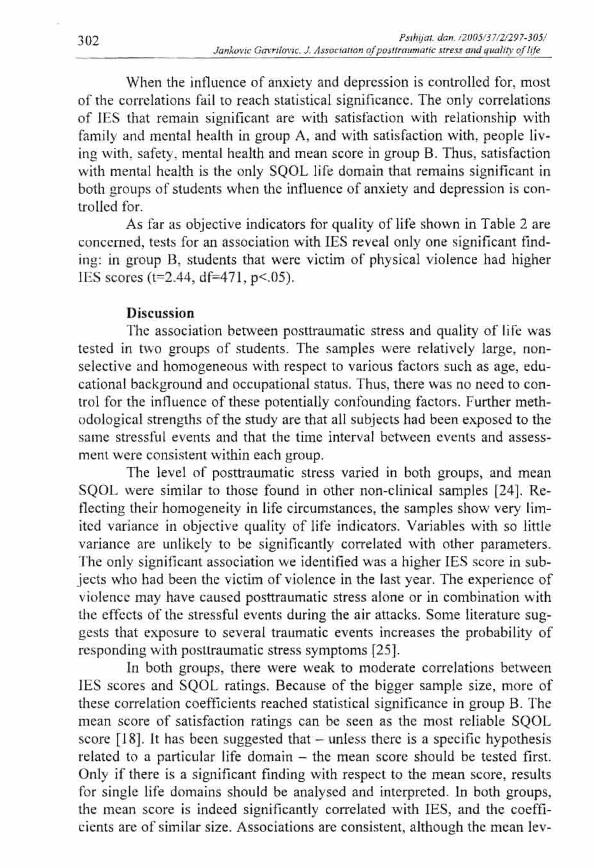
Table 3 shows bivariate correlations between lES score and satisfaction with life domains. All significant correlation coefficients are negative,indicating that a higher level of symptoms is associated with a lower SQOL.Table 3 also summarises partial correlations, i.e. the correlations betweenIES and SQOL scores with the common innuence of anxiety and depressionon both variables eliminated.
Table 3. Correlation coefficients and significance level for bivariate correlationsand partial correlations-controlled for depression and anxiety from SCL-90Rbelv.'cen rES and satisfaction with life domains MANSA (partial correlationswere calculated only for the correlations that rcached significance Icvel inbivariate correlations)
Group A (N'"139)
-.03 ns.03 ns
-.04 liS
-.16"·-.10·
-.02 ns-.07 ns-.03 liS-.14"
-.09'
Life as a wholeTrai Iling/cd uC[llionFinam;esfriendshipsLeisure activitiesAccommod<ltionSafetyPeople living withSex.1ifcRelationship with familyHealthMental healthMean score
Bivariatecorrelation.~
IES-.16 ns-.11 ns-.10 liS-.16 IlS
-.10 ns-.02 liS-.14 liS-.16 ns.04 liS-.25·-
-.29"--.42·"-.26-'
Partialcorrelations
IES
-.17·-.15 ns-.23"-.07 ns
Group B (N"'474)Bivariate Partial
correlations CorrelationsIES JES
-.22'" -.05'-.15'" -.03 ns-,OS ns-.13"-.13"-.09'
-.23'"-.15'"-.t4"-.t4"
-.17'"-.33"--.30" •
N,
.....nnn significant",",OSp<O.OIp<O.OOI
302 hlhlJol. da".I2/}05/37IZI297·J05J)o"l.m'ic Gffrri!m'ic. J. ,Issoc,micln a!JW:>lInmmmit; $Irt,i.l cmd qua"'y a/lift
When the influence of anxiety and depression is controlled for, mostof the correlations fail to reach statistical significance. The only correlationsof IES that remain significant are with satisfaction with relationship withfamily and mental health in group A, and with satisfaction with, people living with, safety, mental health and mean score in group B. Thus, satisfaction\",ith mental health is the only SQOL life domain that remains significant inboth groups of students when the influence of anxiety and depression is controlled for.
As far as objective indicators for quality of life shown in Table 2 areconcerned, tests for an association \vith IES reveal only one significant finding: in group 13, students that were victim of physical violence had higherIES scores (1=2.44, df=471, p<.OS).
DiscussionThe association between posttraumatic stress and quality of life was
tested in two groups of students. The samples were relatively large, nonselective and homogeneous with respecI to various factors such as age, educational background and occupational status. Thus, there was no need to control for the inlluence of these potentially confounding factors. Further methodological strengths of the study are that all subjects had been exposed to thesame stressful events and thaI the time interval between events and assessment wcre consistent within each group.
The level of posttraumatic Slress varied in both groups, and meanSQOL were similar to those found in other non-clinical samples [24]. Reflecting their homogeneity in life circumstances, the samples show very limited variance in objective quality of life indicators. Variables with so littlevariance arc unlikely to be significantly correlated with other parameters.The only significant association we identified was a higher IES score in subjects who had been the victim of violence in the last year. The experience ofviolence may have caused posttraumatic stress atone or in combination withthe effects of the stressful events during the air attacks. Some literature suggests that exposure 10 several traumatic events increases the probability ofresponding with posttraumatic stress symptoms [25].
In both groups, there were weak to moderate correlations betweenIES scores and SQOL ratings. Because of the bigger sample size, more ofthese correlation coefficients reached statistical significance in group B. Themean score of satisfaction ratings can be seen as the most reliable SQOLscore [18]. It has been suggested that - unless there is a specific hypothesisrelated to a particular life domain - the mean score should be tested first.Only if there is a significant finding with respect to the mean score, resultsfor single life domains should be analysed and interpreted. In bOlh groups,the mean score is indeed significantly correlated with lES, and the coefficients are of similar size. Associations are consistent, although the mean lev-

PSt/UJiII. dun. 12005!J71]!Z97-JOJ!Jankol'lc Gm."lo,·ic. J. ASSOCIU/lon ojpoSllfllUmIJ/ic Slrus alld qrmll/Y oflife
303
cis of posttraumatic stress differ bet\veen two groups for reasons that wecannot explore on the basis of data collected in the study.
The different period of time between stressful events and assessment,i.e. one year versus two years, appear not to have had a major impact on theassociation bet\vecn posttraumatic stress and SQOL. This clear association,however. seems to be - mainly though not fully - mediated through symptoms of anxiety and depression. Posttraumatic stress can be associated withmood and anxiety symptoms which are known to impact on SQOL ratings.The association of posttraumatic stress with subjects' satisfaction with theirmental health is the strongest one in bivariate tests, and the only one that remains statistically significant in both groups after controlling for mood andanxiety symptoms. It seems plausible that satisfaction with mental healthmay be more closely linked with posttraumatic stress symptoms than satisfaction with other life domains, and a stronger correlation is less likely to beexplained by the innuence of third factors as in this case mood and anxietysymptoms. Also, this association might be qualitati ...-ely different so that concomitant mood and anxiety symptoms cannot fully explain it.
A shortcoming of the study design is the cross-sectional approachwhich does nOl allow conclusions to be drawn on causal relationships.Higher levels of posttraumatic stress might - mainly mediated through depression and anxiety - impact on SQOL, and, vice versa, lower SQOL mighthave had a negative influence on symptoms. Future prospective longitudinalresearch should address the issue of causality.
ConclusionThe findings suggest that posttraumatic stress is associated with
SQOL in relatively homogeneous and non-selective groups of civilians whoexperienced stressful and potentially traumatic events. The results are relatively consistent in two independent but similar samples. Yet, they should bereplicated in different groups and contexts.
It might be useful to assess quality of life indicators in future studiesof samples suflering from posttraumatic stress. Such assessment may revealthat SQOL influences posttraumatic stress or is a relevant consequence of it,or both, and identify the role of mood symptoms in this association. In anycase, symptoms of anxiety and depression need to be obtained and considered as mediating factors. The nature of the relationship is not clear yet, andfurther systematic research applying quantitative and qualitative methods isrequired to understand the underlying processes. Intervention studies mightexplore whether therapeutic interventions should primarily aim to improveposttraumatic stress or mood symptoms to affect SQOL, or whether an improved SQOL will subsequently lead to reduced level:. of anxiety, depressionand posttraumatic stress.
304 I'sihijal. d"".1200JfJ7121297·JOJIJ(wkovic (;avriIQl"lC. J. ASS<JC;afion o/postrraumQr/(: $fUSS "nd quality a/lift .
Referenc(!sI. Lauer G. Concepts of quality of life in mental health care. In: S. Priebe,
Oliver J, W. Kaiser (cds.) Quality of life and mental health care. Petersfield: Wrightson Oiomedical Publishing Ltd; 1999. pp.l·l8.
2. Priebe S, Oliver J, Kaiser W. Quality of life and mental health care. Petersfield: Wrightson Biomedical Publishing Ltd; 1999.
3. Gill TM, Feinstein AR. A critical appraisal of the quality of life measurements. J Am Med Assoc 1994; 272: 619-626.
4. Mendlowicl M, Stein M. Quality of life in individuals with 3tLxiety disorders. Am J of Psychiatry 2000; 157:669-682.
5. Dimenas ES, Dahlof CG, Jem SC, Wiklund IK. Defining quality of lifein medicine. Scand J Prim Health Care 1990; 1:7-10.
6. Priebe S. Research in quality of life in mental health care: aims andstrategies in quality of life and mental health care. In: Priebe S, OliverJ, Kaiser W (cds.) Quality of life and mental health care. Petersfield:Wrightson Biomedical Publishing Ltd; 1999. pp. lJ9-154.
7. Kaiser W, Priebe S, Hoffmann K, Isennann M, Roder-Wanner UU,Huxley P. Profiles of subjective quality of life in schizophrenic in- andout-patient samples. Psychiatry Res, 1997; 6. 153-166.
8. Pyne 1M, Patterson TL, Kaplan, RM, Gillin, JC, Koch WL, Grant t.Assessment of the quality of life of patients with major depression. Psy·chiatr $erv 1997; 48: 224-230.
9. Kohen 0, Burgess AP, Catalan J, Lant A. The role of anxiety and depression in quality of life and symptom reporting in people with diabetcs mellitus. Qual of Life Res 1998; 7: 197-204.
10. Hansson L. Quality of life in depression and anxiety. Int Rev Psychiatry 2002; 14,3:185-189.
II. Wittchen I-IU, Carter RM, pfiser H, Montgomery SA, Kessler Re. Disabilities and quality of life in pure and comorbid generalized anxietydisorder and major depression in a national survey. Int Clin Psychophannacol2000; 15: 319-328.
12. Zatzick Of, Marrnar CR, Weiss DS, Browner WS, Metzler TJ, Golding1M, Stewart A, Schlenger WE, Wells KB. Posttraumatic stress disorderand functioning and quality of life outcomes in a nationally representative sample of male Vietnam veterans. Am J Psychiatry 1997a:154:1690-1695.
13. Zatzick DF, Weiss DS, Marmar CR, Metzler TJ. Wells K, Golding 1M,Stewart A, Schlenger WE, Browner WS. (1997b). Post-traumatic stressdisorder and functioning and quality of life outcomes in female Vietnam veterans. Mil Merl, 162; 10: 661-665.
14. Amnesty Intemational. Amnesty International Report. London 2000.15. Gavrilovic J, Leck Tosevski 0, Knclcvic G, Priebe S. Predictors of
posttraumatic stress in civilians one year after air attacks - a study ofYugoslavian students. J Nerv Ment Dis 2002; 190: 257-262.
16. Gavrilovic J, Lccic Tosevski D, Dimie S. Pejovic Milovancevie M,Knezevic G, Priebe S. Coping strategies in civilians during air attacks.Sod Psychiatry Psychiatr Epidemiol 2003;38: 128-133.
Psihijflf. da". /}005/371}1297·)O)lJa"ko\·;c Gmnlol"lc. J AssQ{"imion ofpoSllflllImUIiC Slre.fS and qrrahry oflife
305
17. Lecie Tosevski D, G<lvrilovir.: J. Knezevic G, Priebe S. Personality factors and posttraumatic stn:ss: associations in civilians one year after airallacks. J Personal Disord 2003; 17: 537-549.
18. Priebe S, Huxley P, Knight S, Evans S. Application and resulls of theManchester Short Assessment of Quality of Life (MANSA). Int J SocPsychiatry 1999; 45: 7-12.
19. Lehman AC, Ward NC, Linn LC. Chronic mental patients: the qualityof life issues. Am J Psychiatry 1982; 139: 1271·1275.
20. Lehman AC. Possidente S, Hawker F. The quality of life in a state hos·pital and in a community residences. Hasp Community Psychiatry1986; 37: 901-907.
21. Oliver 1PJ. The social care directive development of a quality of lifeprofile for use in community services for the mentally ill. Soc.ial Workand Social Science Review 1991; 3:5-45.
22. Horowitz MJ, Wilner N, Alvarez W. Impact of Event Scale: a measureof subjective stress. Psychosom Med 1979;41: 209-218.
23. Derogatis LR. SCL-90-R: Administration, scoring and procedures man~ua!. II. Towson, MD: Clinical Psychometric Research. 1983.
24. Priebe S, Gnl)'lers T, Heinze M, Hoffmann C, Jackel A. Subjectiveevaluation criteria in psychiatric care - methods of assessment for research and general practice. Psychiatr Prax 1995; 22: 140-144.
25. Follene YM, Polusny MA, Bechtc AE, Naugle AE. Cumulative trauma:the impact of child sexual abuse, adult sexual assault and spouse abuse.J of Trauma Stress 1996; 9:257-262.
ie/ella JANKOVIC GAVRlLOVIC, Odeljenje za soeijalnu i komunalnu psihijatriju Barts i Medieinski fakllitet Queen Mary u Londonu, London, VelikaBritanija
ielell" JANKOVIC GAVRlLOVIC. Unit for Social and Community Psychiatry. Barts and the London School of Medicine, Queen Mary, UniversilYof London. United Kingdom
E-mail: [email protected]