polytetrafluoroethylene patch grafting for closure of stomach defects in the rat
TRANSCRIPT
Short note
Br. J. Surg. 1993, Vol. 80, August, 1013-1014
Polytetrafluoroethylene patch grafting for closure of stomach defects in the rat
T. Gaga and F. Gurer*
Departments of General Surgery and *Histology, Faculty of Medicine, Anatolian University, Eskiqehir, Turkey Correspondence to: Dr T. Gaga
Definitive surgical management of large lacerations of the second and third parts of the duodenum and of chronic duodenal fistula and perforation resulting from malignant infiltration of the stomach and duodenum is diff ic~l t l -~.
'To solve these problems, the serosal patch techniq~e ' .~ , pedicle patches of ileum, and lyophilized bovine tendon-like heterologous structures have been employed'. However, use of an expanded polytetrafluoroethylene (PTFE ) patch (GORE- TEX; W. L. Gore, Elkton, Arizona, USA) for this purpose has not been cited in the literature. In the present study, the healing process of experimental stomach defects closed by a PTFE patch was followed.
Materials and methods Fourteen 8-week-old male rats (Rattus norvegicus albus) weighing 200 g were used. Each was given standard feed and water, and starved for 8 h before the experiments.
Under ether anaesthesia a midline laparotomy was made and a defect 1 cm in diameter in the fundus area of the stomach created by removing the full thickness of the gastric wall. This defect was then closed with a PTFE patch, secured with a continuous 3/0 polypropylene suture taken from the seromuscular layer and placed within l m m of the edge of the graft. After haemostasis had been achieved, the abdomen was closed without drainage using 2/0 nylon.
Rats were allowed water within the first 24 h after operation; standard feeding was resumed after this. No antibiotics were given. The animals were killed at 3 , 5 , 8, 14, 20 and 30 days.
The grafted area with surrounding healthy tissue was excised from the dead rats and fixed in 10 per cent neutral formaldehyde. The excised tissue was placed in paraffin blocks and 6-pm sections taken for routine histological examination following staining with haematoxylin and eosin.
Results Two rats died within 48 h. At autopsy, none of the animals showed any evidence of leakage or peritonitis. There were no adhesions in the area of the patch or elsewhere in the abdominal cavity.
Histological examination showed progressive covering of the graft with cellular material, starting from the edges and eventually covering the whole area of the graft with keratinized squamous epithelium (Figures 1-6).
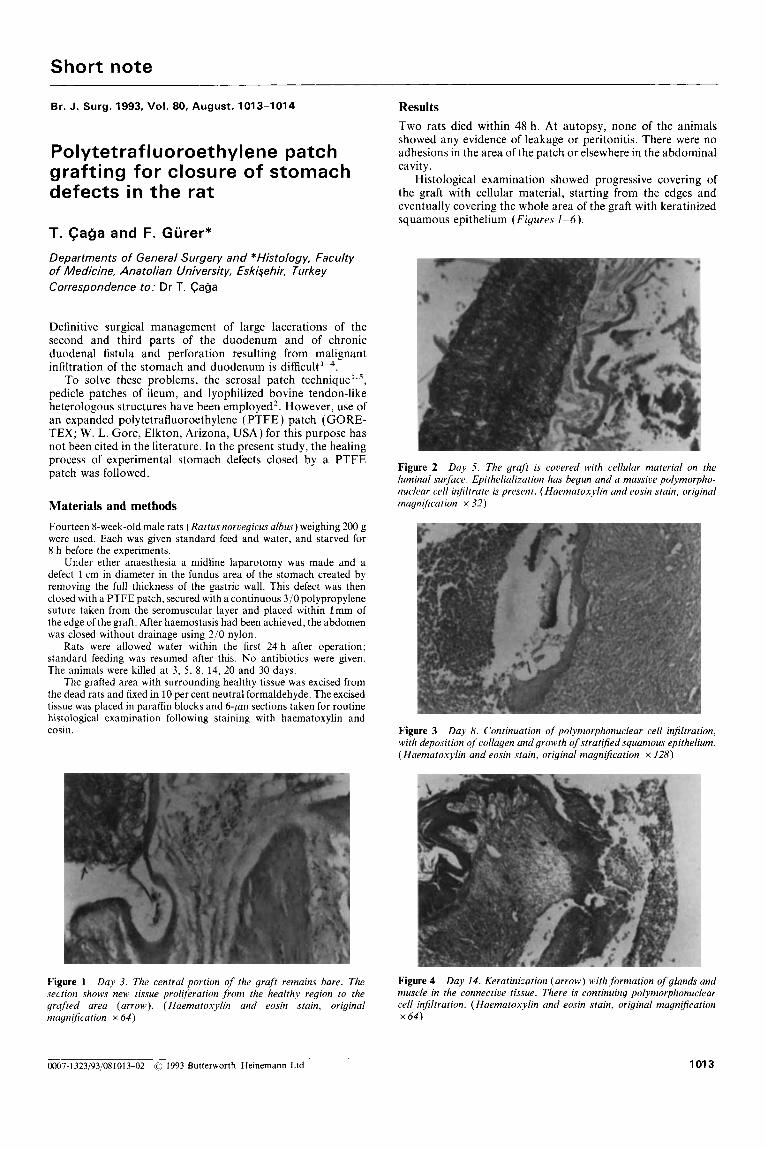
Figure 2 Day 5. The graft is covered with cellular material on the luminal surface. Epithelializution has begun and a massive polymorpho- nuclear cell infiltrate is present. ( Haematoxylin and eosin stain, original magnification x 32)
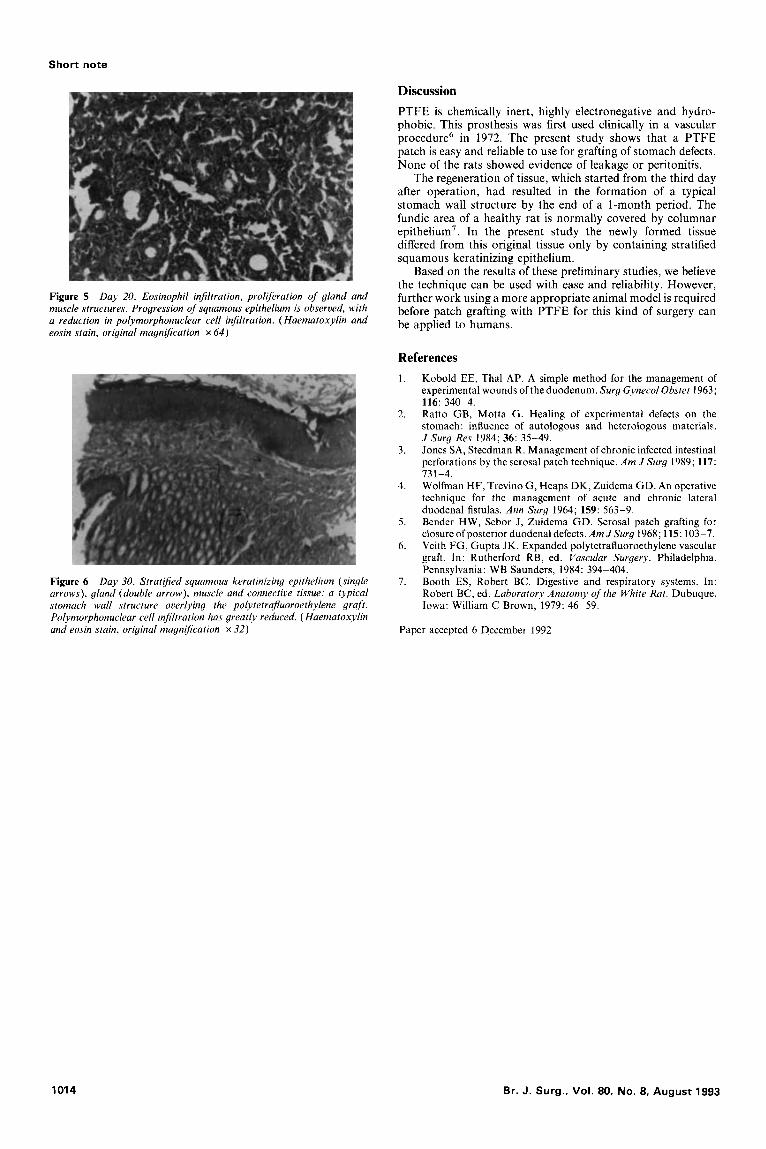
Figure 3 Day 8. Continuation of polyrnorphonuclear cell infiltration, with deposition of collagen and growth of stratified sguamous epithelium. (Haematoxylin and eosin stain, original magnijication x 128)
Figure 1 Day 3. The central portion of the graft remains bare. The Figure 4 Day 14. Keratinization (arrow) with formation of glands and section shows new tissue proliferation from the healthy region to the muscle in the connective tissue. There is continuing polymorphonuclear grafted area (arrow). (Haematoxylin and eosin stain, original cell infiltration. ( Haematoxylin and eosin stain, original magnijication magnification x 64) x 6 4 )
0007-1 323/93/081013-02 0 1993 Butterworth-Heinemann Ltd 1013
Short note
Discussion PTFE is chemically inert, highly electronegative and hydro- phobic. This prosthesis was first used clinically in a vascular procedure6 in 1972. The present study shows that a PTFE patch is easy and reliable to use for grafting of stomach defects. None of the rats showed evidence of leakage or peritonitis.
The regeneration of tissue, which started from the third day after operation, had resulted in the formation of a typical stomach wall structure by the end of a 1-month period. The fundic area of a healthy rat is normally covered by columnar epithelium’. In the present study the newly formed tissue differed from this original tissue only by containing stratified squamous keratinizing epithelium.
Based on the results of these preliminary studies, we believe the technique can be used with ease and reliability. However, further work using a more appropriate animal model is required before patch grafting with PTFE for this kind of surgery can be applied to humans.
Figure 5 Day 20. Eosinophil injiltration, proliferation of gland and muscle structures. Progression of squamous epithelium is observed, with a reduction in polymorphonuclear cell injiltration. ( Haematoxylin and eosin stain, original magnification x 64)
Figure 6 Day 30. Stratified squamous keratinizing epithelium (single arrows), gland (double arrow), muscle and connective tissue: a typical stomach wall structure overlying the polytetrajuoroethylene graft. Polymorphonuclear cell injiltration has greatly reduced. ( Haematoxylin and eosin stain, original magniJication x 32)
References 1. Kobold EE, Thal AP. A simple method for the management of
experimental wounds of the duodenum. Surg Gynecol Obstet 1963; 116: 340-4. Ratto GB, Motta G. Healing of experimental defects on the stomach: influence of autologous and heterologous materials,. J Surg Res 1984; 36: 35-49. Jones SA, Steedman R. Management of chronic infected intestinal perforations by the serosal patch technique. Am J Surg 1989; 117:
Wolfman HF, Trevino G, Heaps DK, Zuidema GD. An operative technique for the management of acute and chronic lateral duodenal fistulas. Ann Surg 1964; 159: 563-9. Bender HW, Sebor J, Zuidema GD. Serosal patch grafting for closure ofposterior duodenal defects. Am JSurg 1968; 115: 103-7. Veith FG, Gupta JK. Expanded polytetrafluoroethylene vascular graft. In: Rutherford RB, ed. Vascular Surgery. Philadelphia, Pennsylvania: WB Saunders, 1984: 394-404. Booth ES, Robert BC. Digestive and respiratory systems. In: Robert BC, ed. Laboratory Anatomy of the White Rat. Dubuque, Iowa: William C Brown, 1979: 46-59.
2.
3 .
731-4. 4.
5.
6.
7.
Paper accepted 6 December 1992
1014 Br. J. Surg.. Vol. 80, No. 8, August 1993