polymorphisms, hypertension and thiazide diuretics
TRANSCRIPT
1587
Review
ISSN 1462-241610.2217/PGS.11.110 © 2011 Future Medicine Ltd Pharmacogenomics (2011) 12(11), 1587–1604
Polymorphisms, hypertension and thiazide diuretics
For many years, it has been predicted that the pharmacogenomic approach, the study of the influence of genetic variations on drug effect, would have revolutionized drug prescribing. However, despite major advances in this field, pharmacogenomics (PGX) has so far failed to create a major impact on day-to-day prescription practices. Hypertension is an attractive disease process for pharmacogenetic research. In fact, cardiovascular (CV) diseases are the major cause of health burden and cost worldwide, with arterial hypertension accounting for approximately 50% of them [1]. In 2001, 7.6 million deaths worldwide, approximately 54% of all strokes and 47% of all ischemic heart diseases were attributable to ele-vated systolic blood pressure (SBP) [2]. More than one half of these events occurred among people of working age (45–69 years). It has been estimated that the total number of adults with hypertension is set to increase by over 60% by 2025, rising from 972 million to 1.56 billion worldwide [3]. In clini-cal trials, the current antihypertensive therapy, compared with placebo, is able to reduce the associated CV diseases by 20 and 30% (in heart diseases and stroke, respectively) [4]. However, in the general hypertensive population, approxi-mately only one third of patients can control their blood pressure (BP) by a therapy similar to that used in clinical trials [5]. Therefore, the efficiency of the current therapeutic strategy in preventing CV diseases is further reduced in this general population [6,7]. Furthermore, it is well known that the individual BP variability to the main class of antihypertensive drugs (diuretic hydro-chlorothiazide [HCTZ], angiotensin-converting
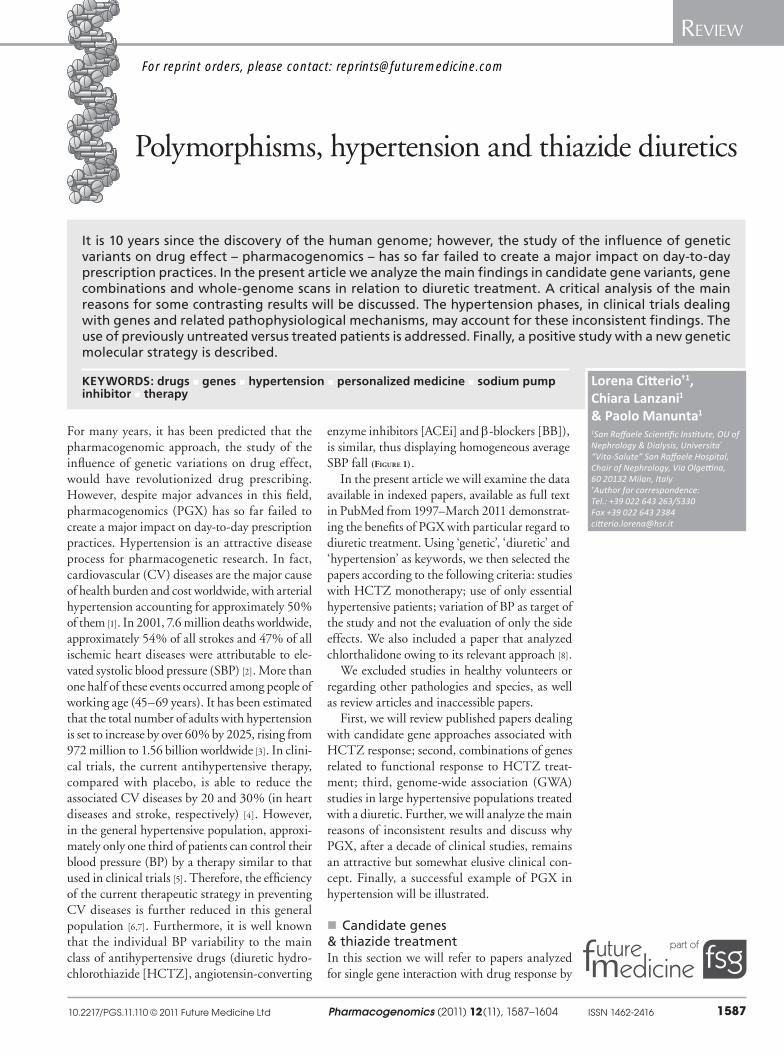
enzyme inhibitors [ACEi] and b-blockers [BB]), is similar, thus displaying homogeneous average SBP fall (Figure 1).
In the present article we will examine the data available in indexed papers, available as full text in PubMed from 1997–March 2011 demonstrat-ing the benefits of PGX with particular regard to diuretic treatment. Using ‘genetic’, ‘diuretic’ and ‘hypertension’ as keywords, we then selected the papers according to the following criteria: studies with HCTZ monotherapy; use of only essential hypertensive patients; variation of BP as target of the study and not the evaluation of only the side effects. We also included a paper that analyzed chlorthalidone owing to its relevant approach [8].
We excluded studies in healthy volunteers or regarding other pathologies and species, as well as review articles and inaccessible papers.
First, we will review published papers dealing with candidate gene approaches associated with HCTZ response; second, combinations of genes related to functional response to HCTZ treat-ment; third, genome-wide association (GWA) studies in large hypertensive populations treated with a diuretic. Further, we will analyze the main reasons of inconsistent results and discuss why PGX, after a decade of clinical studies, remains an attractive but somewhat elusive clinical con-cept. Finally, a successful example of PGX in hypertension will be illustrated.
� Candidate genes & thiazide treatmentIn this section we will refer to papers analyzed for single gene interaction with drug response by
It is 10 years since the discovery of the human genome; however, the study of the influence of genetic variants on drug effect – pharmacogenomics – has so far failed to create a major impact on day-to-day prescription practices. In the present article we analyze the main findings in candidate gene variants, gene combinations and whole-genome scans in relation to diuretic treatment. A critical ana lysis of the main reasons for some contrasting results will be discussed. The hypertension phases, in clinical trials dealing with genes and related pathophysiological mechanisms, may account for these inconsistent findings. The use of previously untreated versus treated patients is addressed. Finally, a positive study with a new genetic molecular strategy is described.
KEYWORDS: drugs � genes � hypertension � personalized medicine � sodium pump inhibitor � therapy
Lorena Citterio†1, Chiara Lanzani1 & Paolo Manunta1
1San Raffaele Scientific Institute, OU of Nephrology & Dialysis, Universita “Vita-Salute” San Raffaele Hospital, Chair of Nephrology, Via Olgettina, 60 20132 Milan, Italy †Author for correspondence:Tel.: +39 022 643 263/5330 Fax +39 022 643 2384 [email protected]
For reprint orders, please contact: [email protected]
Pharmacogenomics (2011) 12(11)1588 future science group
Review Citterio, Lanzani & Manunta
selecting studies with HCTZ monotherapy. With the aim of analyzing the antihypertensive effect of HCTZ, we only included studies of essential hypertensive patients and did not select studies performed on healthy volunteers.
In the early PGX studies, a candidate gene approach has been applied with regard to genes of major hormonal systems involved in BP regulation. In 2001 Turner et al. investigated the C825T polymorphism of the gene encod-ing the G-protein b3-subunit (GNB3) in asso-ciation with BP response to diuretic therapy in 197 black subjects (134 men and 63 women) and 190 non-Hispanic white subjects (76 men and 114 women) with essential hypertension who underwent monotherapy with HCTZ for
4 weeks [9]. Mean declines in SBP and diastolic BP (DBP) were 6 ± 2 mmHg (p < 0.001) and 5 ± 1 mmHg (p < 0.001) greater, respectively, in TT than in CC homozygotes.
In 2002 Schwartz et al. demonstrated that the relationship between the ACE insertion/deletion (I/D) polymorphism and antihypertensive response to a standard dose of HCTZ differed significantly between women and men [10]. In a regression model that considered the effects of baseline BP, race, gender, age and waist-to-hip ratio, there was a significant interaction between the effects of the ACE genotype and gender on the responses of both SBP and DBP to HCTZ. Among women, mean declines in SBP and DBP were greater in II than in DD
ACEi
-60
-50
-40
-30
-20
-10
0
10
20
30
∆SBP(mmHg)
-60
-50
-40
-30
-20
-10
0
10
20
30HCTZ
BB
-60
-50
-40
-30
-20
-10
0
10
20
30
-6.7
-7.3
-9.7
∆SBP(mmHg)
∆SBP(mmHg)
Figure 1. Individual systolic blood pressure fall after 1 month of treatment with an ACE inhibitor ([A] black), diuretic hydrochlorothiazide ([B] green), and b-blocker ([C] yellow). With all three antihypertensive treatments, the average SBP falls are similar. However, a great SBP variability is present: 80 mmHg with ACEi (from -60 to +20 [A]), 60 mmHg with HCTZ (from -45 to +15 [B]) and 57 mmHg with BB (from -37 to +20 [C]). The gray bars in (A) and the dark green bars in (B) represent subjects having the average variation in SBP after ACEi and HCTZ treatment, respectively. In (C) the average value is displayed by an orange bar.ACEi: Angiotensin-converting enzyme inhibitor; BB: b-blockers; HCTZ: Hydrochlorothiazide; SBP: Systolic blood pressure.

www.futuremedicine.com 1589future science group
Polymorphisms, hypertension & thiazide diuretics Review
homozygotes whereas among men, they were greater in DD than in II homozygotes.
After these initial findings, the authors started to analyze groups of candidate genes involved in related mechanisms of action. However, all of these papers considered the genes one by one.
In two unrelated cohorts from different eth-nicities (African–Americans and white subjects), BP response to HCTZ was examined in relation to a set of candidate gene polymorphisms that have been previously associated with interin-dividual differences in BP: a-adducin (ADD1) Gly460Trp, the endothelial nitric oxide syn-thase (NOS3) Glu298Asp, the b1-adrenoceptor (ADRB1) Arg389Gly, the b2-adrenoceptor (ADRB2) Arg16Gly and the lipoprotein lipase (LPL) Ser447Stop. NOS3 encodes the endothe-lial nitric oxide synthase, implicated in vascular smooth muscle relaxation through a cGMP-mediated signal transduction pathway. ADRB1 and ADRB2 are members of the adrenergic recep-tor group of G-protein-coupled receptors. They are located primarily in the brain, heart, coro-nary artery, kidney and muscle and are involved in cardiac stimulation, coronary vasodilation and relaxation of the colon and esophagus. LPL encodes lipoprotein lipase, which is expressed in the heart, muscle and adipose tissue and is linked to many disorders of lipoprotein metabo-lism. After adjustment for covariates (e.g., eth-nicity, gender, age and waist-to-hip ratio), the evidence of association was limited to an effect of the Glu298Asp polymorphism of NOS3 (GG: -8.6 ± 0.4 vs GT+TT: -7.1 ± 0.6 DBP fall in response to HCTZ), which explained 1% of interindividual variation in the adjusted DBP response to HCTZ [11].
A Japanese cohort of 76 outpatients with essential hypertension who had been newly pre-scribed thiazides as monotherapy or in addition to other antihypertensive drugs were retro spectively assessed [12]. The thiazides were a combination of indapamide (64.5%), trichlormethiazide (26.3%), mefruside (7.9%) and HCTZ (1.3%). Mean BP (MBP) response <5 mmHg defined par-ticipants as responders. A total of 48 SNPs in 17 candidate genes (codifying factors related to renin (REN)–angiotensin–aldosterone system [RAAS] and sympathetic nervous system), including ADD1 Gly460Trp were genotyped. The com-parison of polymorphism prevalence between responders and nonresponders demonstrated sig-nificant differences in the thiazide-sensitive NaCl cotransporter (NCC): SLC12A3 C1784T (C allele vs T allele, odds ratio [OR]: 3.81, p = 0.016, CI: 1.25–11.63) and b3-adrenoreceptor: ADRB3
T727C (Trp64Arg); (T allele vs C allele, OR: 4.59, p = 0.005, CI: 1.54–13.68). No poly-morphisms were s ignificantly related to the effect of the thiazides for the other genes, based on the comparison of each allele frequency between responders and nonresponders.
In 2005 Turner et al. investigated the role of SNPs in genes encoding or influencing renal sodium transport systems in a sample of 585 adults with essential hypertension (50% black individuals; 47% women) treated with HCTZ for 4 weeks [13]. After adjustment for ethnicity, sex, age, and waist-to-hip ratio, three SNPs in WNK lysine deficient protein kinase 1 (WNK1), encoding a lysine-deficient protein kinase that regulates thiazide-sensitive NaCl cotransport, made statistically significant contributions to predict ambulatory BP responses, accounting for 2–4% of variation in SBP and DBP responses (p < 0.05). SNPs in the ADRB2 and the epithelial sodium channel g-subunit (SCNN1G) genes were associated with a similar magnitude of variation in ambulatory SBP response (p = 0.028) or office DBP response (p < 0.05), respectively. However, SNPs evaluated in the other genes were not asso-ciated with significant variation in ambulatory or office BP responses.
In 2007 Schelleman et al. investigated whether the interaction between diuretics and ADD1 Gly460Trp or GNB3 rs2301339 polymorphism modified the risk of myocardial infarction (MI) or stroke from the Rotterdam Study [14]. The risk of MI in current users of low-ceiling diuret-ics with one or two copies of the ADD1 Trp allele (hazard ratio [HR]: 0.92) was similar to the expected joint effect of the Trp allele and low-ceiling diuretics on a multiplicative scale (1.04 × 0.90 = 0.94) (synergy index: 0.99; 95% CI: 0.43–2.27). No drug–gene interaction was found on the risk of stroke. Conversely, a trend towards an interaction was found between cur-rent use and the GNB3 rs230119 G/A polymor-phism on the risk of MI (synergy index: 0.51; 95% CI: 0.23–1.15). The main limitation of this study was the relatively small number of events.
More recently, the association of common polymorphisms in RAS genes and ADD1 Gly460Trp with BP responses to four differ-ent antihypertensive drugs (amlodipine, biso-prolol, HCTZ and losartan) was analyzed in a controlled study including 208 hypertensive Finnish men from the GENRES study. All par-ticipants used the four drugs, each for 4 weeks as a monotherapy, separated by 4-week placebo periods. Common polymorphisms of these genes do not significantly predict BP responses to the

Pharmacogenomics (2011) 12(11)1590 future science group
Review Citterio, Lanzani & Manunta
different compounds, at least in white hyperten-sive men, even if ADD1 460Trp and angioten-sinogen (AGT ) 235Thr alleles were associated with higher systolic white coat effect during the placebo periods (p-values of 0.03 and 0.01, re spectively) [15].
Neural precursor cell-expressed, developmen-tally downregulated 4-like (NEDD4L) is involved in the regulation of plasma volume and BP by controlling cell surface expression of the kidney
epithelial sodium channel. In 2009 Luo et al. performed a case–control study of hypertension (n = 1686), a 4-week clinical trial (n = 311), and a case–control study of orthostatic hypotension (n = 793) in Chinese subjects [16]. NEDD4L A allele was significantly associated with hyper-tension after appropriate adjustment (OR: 1.39; 95% CI: 1.13–1.72; p = 0.002). The BP reduc-tion in A carriers after HCTZ treatment was greater than that in GG carriers, with differences of 6.1 mmHg (p = 0.009) in SBP and 2.7 mmHg (p = 0.027) in DBP.
In 2010 Duarte et al. analyzed 100 SNPs in the serine threonine kinase 39 (STK39) gene in 195 ‘good’ and 194 ‘poor’ responders to HCTZ and found an association with DBP not replicated in Epidemiology of Responses to Antihypertensives (GERA) and Pharmacogenomic Evaluation of Antihypertensive Responses (PEAR) populations [17]. STK39 is a gene that regulates NCC activity that has been recently implicated as a hyperten-sion susceptibility gene in an Amish population in a GWA study [18]. Two SNPs (rs6749447 and 3754777) were initially associated with BP, and these associations were also found in three other Caucasian replication cohorts.
Han et al. examined the influence of organic anion transporters 1 and 3 (OAT1 and OAT3) polymorphisms on high BP and the response to thiazide diuretics in a Chinese population [19]. The association with hypertension was investi-gated in two independent case–control studies (n = 1592 and 602, respectively) with adjust-ment for geographic location. Two clinical tri-als (n = 542 and 274, respectively) were con-ducted in untreated hypertensive patients. The intergenic polymorphism rs10792367, located between OAT1 and OAT3, was not found to be associated with hypertension; however, it appeared to be involved in variations in anti-hypertensive responses to HCTZ. This paper underlines two important points: first, to get significant results, it is important to study the untreated hypertensives; second, a polymor-phism not associated to hypertension per se may be relevant for response to therapy.
In 2011 Huang et al. investigated the response to initial treatment of HCTZ in nondiabetic hypertensive patients who were either previously untreated or unsatisfactorily treated according to REN SNPs and levels [20]. After dividing into three groups according to the HCTZ SBP response, the upper one third of responders had older age, higher SBP, higher pulse pressure and lower plasma REN activity (PRA) when compared with the lower one third responders. REN rs11240688 CC polymorphism and base-line PRA were two independent predictors for the BP-lowering response. Both genetic and hor-monal variables were included in a synergic score that resulted in association with BP response to thiazide. This article underlines the possibility to combine hormonal and genetic information to predict response to therapy, even if the effect size (mmHg of SBP response to thiazide) of this interaction is similar to that of single effects (b = 9.9 vs 7.4 vs 8.2 for SNP, hormone level and synergic score, respectively).
In the PEAR population Lobmeyer et al. studied 15 SNPs in the GRK2 gene (ADRBK1) and one GRK5 polymorphism (Gln41Leu) according to response to atenolol or HCTZ [21,22] and discovered that G-protein-coupled receptor kinases (GRK2 and GRK5) are impor-tant regulators of b-adrenergic signaling. The objective of the PEAR study was to identify the genetic determinants of the antihypertensive and adverse metabolic responses to a thiazide diuretic (HCTZ), a BB (atenolol), and their drug combination. This will be accomplished through candidate genes (2200 CV and met-abolic-related genes) and GWA approaches. In this study, GRK5 Leu41 was found not to be associated with BP response to antihyper-tensive medication. On the contrary, a SNP in ADRBK1 (rs1894111 G>A) demonstrated a signal for association with SBP and DBP response to HCTZ in white subjects (DBP: -11.29 ± 3.74 [G/A] vs -4.26 ± 4.79 mmHg [G/G], p = 0.0034 and SBP: -18.37 ± 14.90 [G/A], -8.11 ± 7.55 mmHg [G/G], p = 0.0191). In black hypertensive patients a different SNP in ADRBK1 (rs4930416, A>C) was found to be associated with a greater BP reduction following treatment with HCTZ.
� Combinations of genes related to functional response to HCTZ Beside the single-gene analyses reported above, other studies have also displayed various combi-nations of gene–gene interactions in response to HCTZ treatment.

www.futuremedicine.com 1591future science group
Polymorphisms, hypertension & thiazide diuretics Review
In 2004 Frazier et al. evaluated the relation-ship between variations in genes of the RAAS system and BP response to a thiazide diuretic in African–Americans (125 men and 130 women) and non-Hispanic white subjects (133 men and 113 women) [23]. The performed analyses were race and gender specific. The angiotensin II recep-tor type 1 (AGTR1) A1166C and AGT G-6A polymorphisms displayed a significant effect on SBP response to the diuretic in African–American women. Multilocus analyses indicated that the effects of these genes c ombined additively to influence response.
Schelleman et al. published data on two dif-ferent population-based prospective studies in 2006 [24,25]: the first study investigated the partici-pation of the RAAS genes, ADD1 and GNB3 in modifying the mean difference in BP levels among diuretic, BB or ACEi users. The study was con-ducted in the 625 Dutch hypertensive individuals (Doetinchem Cohort Study). Only the interaction between diuretic use and the GNB3 825C/T poly-morphism was significant (C allele vs TT geno-type SBP: 4.33 mmHg [95% CI: 0.14–8.54]). To assess gene–gene–drug interactions, the mean difference in BP was compared between combi-nations of two out of the five genes. The ADD1 Trp allele, the AGT T allele versus GG and MM, respectively, and diuretic use were associated with a significant difference in DBP (3.09 mmHg [95% CI: 0.16–2.93], 169 vs 149 measurements) [24]. In the second study, the ADD1 Gly460Trp (GW) and AGT M235T polymorphisms were examined in relation to the mean difference in BP using antihypertensive drugs (i.e., diuretic, BB, calcium antagonist or ACEi) in 3025 hyperten-sive subjects of the Rotterdam Study. In diuretic users no relationship between drug–gene interac-tion and BP levels was found after adjustment for potential confounders, with the GW or WW gen-otype having a 1.25 mmHg (95% CI: -2.86–5.35) higher mean SBP and a 0.39 mmHg (95% CI: -1.95–2.74) higher mean DBP compared with diuretic users with the GG genotype. In addi-tion, they assessed the effect of gene–gene inter-actions of the ACE I/D, AGT M235T and ADD1 Gly460Trp polymorphisms on BP variation in patients treated with antihypertensive drugs. None of the gene–gene combinations (AGT–ADD1 or AGT–ACE or ADD1–ACE) modified the mean difference in SBP or DBP level [25].
Recently (2011) Li et al. studied whether the ACE I/D polymorphism and the aldosterone synthase (CYP11B2) gene -344T/C polymor-phism were associated with individual response to HCTZ in a Han Chinese population (816
mild/moderate hypertensive patients) with essential hypertension [26]. The results dem-onstrated that the ACE I/D polymorphism was a ssociated with SBP response to HCTZ (p = 0.009). Neither the CYP11B2 -344T/C polymorphism, nor the two-SNP i nteraction ana lysis reported a s ignificant association with BP response to HCTZ.
� GWA studies of HCTZThe GWA approach has also been pursued in the PGX of HCTZ to identify novel genes influ-encing antihypertensive drug response. In 2008 Turner et al. performed a GWA study suggesting that the chromosome 12 locus may influence the DBP response to HCTZ in 194 non-Hispanic black subjects and 195 non-Hispanic white subjects with essential hypertension selected from opposite tertiles of response to HCTZ (25 mg/day, per os, for 4 weeks) [27]. Haplotype trend regression identified a region of chromo-some in proximity to lysozyme (LYZ), YEATS domain-containing 4 (YEATS4) and fibroblast growth receptor substrate 2 (FRS2), which was significantly associated with DBP response. This result was also confirmed in an independent data set of 291 black subjects and in the sample of 294 white subjects.
� Main reasons for inconsistent resultsThe numerous data we reported above and sum-marized in Table 1 demonstrated the possible rela-tionship between polymorphic variant(s), mostly in candidate genes, and response to thiazides and their effect on BP level or MI risk and stroke event. Some inconsistencies have been found among the association responses of certain SNP variants in different studies, primarily for ADD1 Gly460Trp and ACE I/D. What could the causes be of these controversial results?
There are two main reasons for such incon-sistent findings: first, the phase of hypertension considered (i.e., never-treated patients, naive vs previously treated patients), and second p henotype bias.
� Phase of hypertensionThe meaning of phase of hypertension is well evidenced in a study by Capasso et al., [28] which uses an animal model to demonstrate that Na entry is increased during the induction phase of hypertension in young Milan Hypertensive animals, paralleled by an upregulation of the NaK
2Cl cotransporter at the level of the
thick ascending limb. On the contrary, dur-ing the maintenance phase of hypertension,
Pharmacogenomics (2011) 12(11)1592 future science group
Review Citterio, Lanzani & Manunta
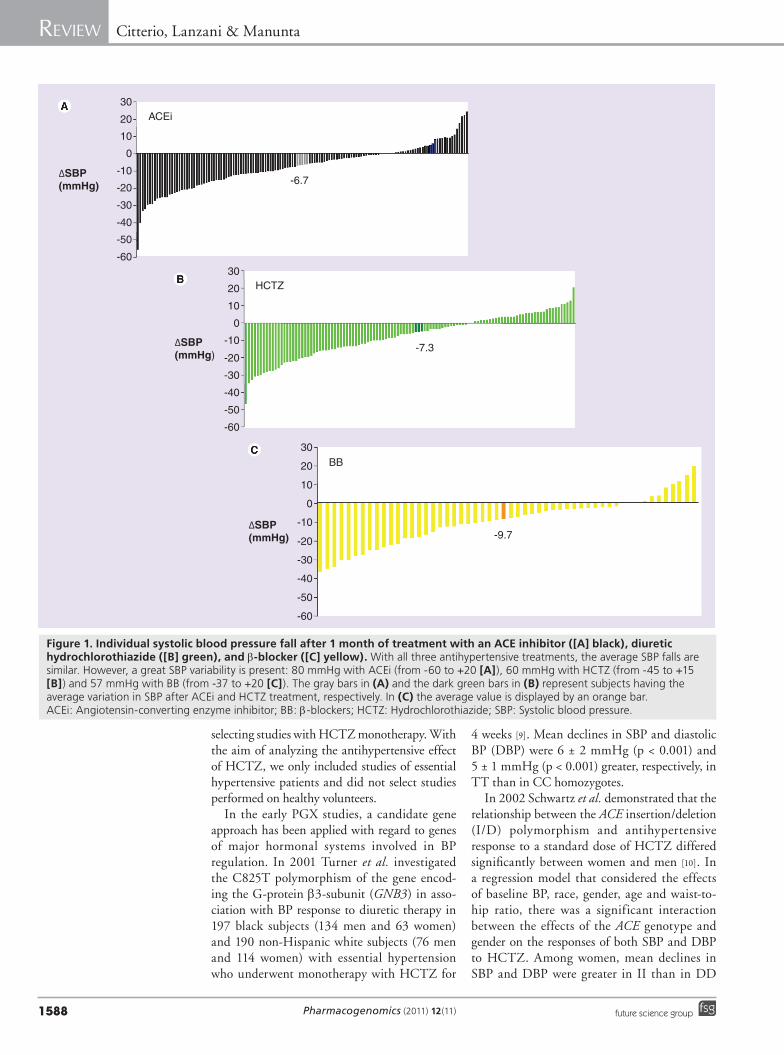
Table 1. Studies reporting the influence of gene polymorphisms on the effect of thiazide antihypertensive drugs.
Gene Previous treat-ment
Therapy Association with HT
Association to response
Treatment result p-value Population descent
Sample size Ref.
Effect size† OR
Single genes
GNB3 PTP+ HCTZ Yes Yes, also gender and race specific
SBP: -16.3 DBP: -10.9
<0.001<0.001
EA
190197
[9]
ACE I/D PTP+ HCTZ Not tested Yes, gender specific
Women II: SBP: -20, DBP: -10; men DD: SBP: -14; DBP: -11
0.003
0.001
EA
184192
[10]
ADD1 NOS3ADRB1ADRB2LPL
PTP+ HCTZ NRNRNRNRNR
NoYesNoNoNo
DBP: -8.6b: 2.29
0.034EA
294291
[11]
ADD1 Naive HCTZ Yes Yes MBP: -14.7 0.002 E 58 [37] ADD1 Naive HCTZ No in SS
Yes in MIYes MBP: -16.5 (SS)
MBP: -12.5 (MI)0.0040.01
E 143 [38]
ADD1 Naive HCTZ No Yes SBP: -23.5DBP: -16.5
<0.022<0.0001
E 268 [50]
ADD1 PTP- HCTZ+ other
No Yes, in relation to MI or stroke event
NR 0.49 0.002 E 471 [51]
ADD1 ACE I/D
Naive HCTZ No Yes MBP: -12MBP: -10
0.0020.049
E 86 [39]
17 genesTSCADRB3
PTP‡ THZTHZ+
Not testedYes, for TSC ADRB3
MBP: -6.7MBP: -6.8
3.84.6
0.0160.005
J 76 [12]
AGTRENACE I/DAGTR1CYP11B2
PTP+ HCTZ Not tested Yes, for AGT + AGTR1 in black females
AGT SBP: -22.2 AGTR1 SBP: -22.5
0.0320.038
EA
246255
[23]
WNK1ADRB2SCNN1GSLC12A1KCNJ1CLCNKBSLC12A3WNK4SCNN1BCYP11B2CYP17A1NR3C2AGTRENACE I/DADD1
PTP+ HCTZ Not tested Yes, for WNK1 (rs2107614, rs1159744 and rs2277869)
ADRB2 (rs2400707)
SCNN1G (rs5723,rs5729)
Ambulatory
SBP: -11.1SBP: -11.5SBP: -18.9DBP: -6DBP: -6.3DBP: -18.9
SBP: -12.4
OfficeSBP: -7.4SBP: -9
0.0390.00070.0570.060.0440.034
0.028
0.0180.014
EA
294291
[13]
Effect size: decrease in blood pressure after thiazide treatment. Studies are listed in chronological order and divided into single genes, gene interactions and genome-wide association studies.†Expressed as.‡Not explicitly mentioned in the paper.A: African; C: Chinese; CHD: Coronary heart disease; DBP: Diastolic blood pressure; E: European; GWAS: Genome-wide association studies; HCTZ: Hydrochlorothiazide; HT: Hypertension; I/D: Insertion/deletion; J: Japanese; MBP: Mean blood pressure; MI: Myocardial Infarction; NR: Not reported; ns: Nonsignificant; OR: Odds ratio; PTP-: Previously treated patients without washout; PTP+: Previously treated patients with washout; SBP: Systolic blood pressure; SS: Sassari; THZ: Thiazide; TSC: Thiazide-sensitive NaCl cotransporter.

www.futuremedicine.com 1593future science group
Polymorphisms, hypertension & thiazide diuretics Review
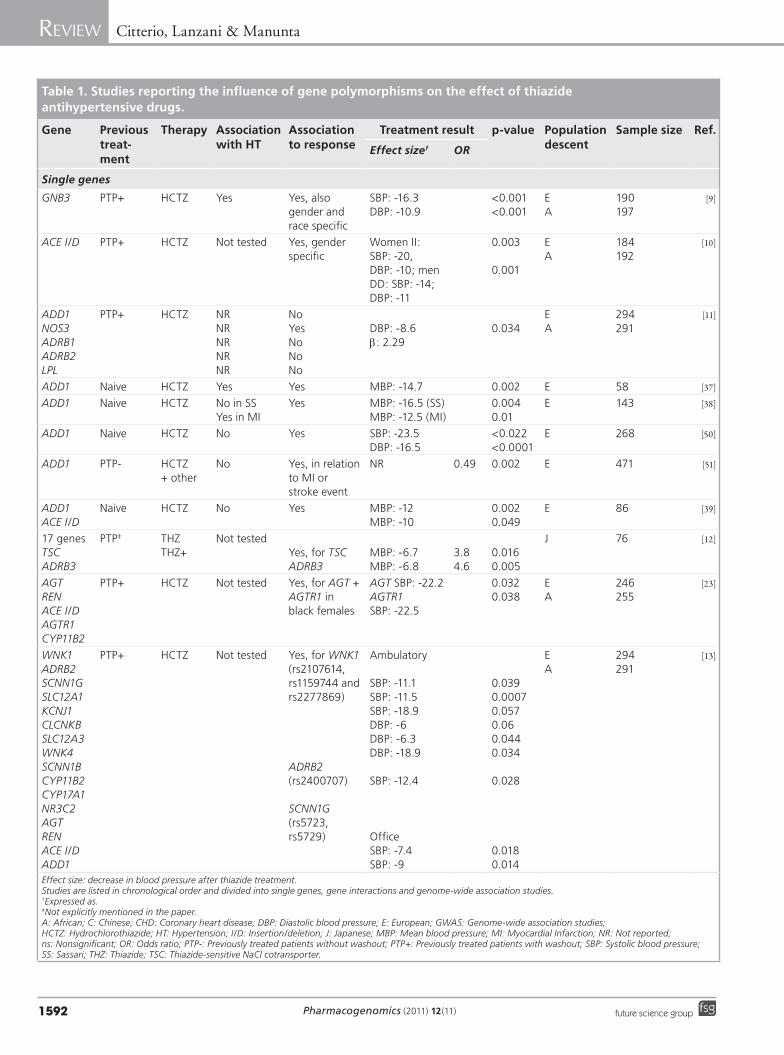
Table 1. Studies reporting the influence of gene polymorphisms on the effect of thiazide antihypertensive drugs (cont.).
Gene Previous treat-ment
Therapy Association with HT
Association to response
Treatment result p-value Population descent
Sample size Ref.
Effect size† OR
Single genes (cont.)
ADD1ACE I/DAGTR1GNB3AGT
Naive and PTP-
THZ (diuretics)
No NoNoNoYes (adjusted)No
SBP: -4.33 all; -4.74 naive
‡
E 106 [24]
ADD1AGT
Naive and PTP+
THZ (diuretics)
Yes, ADD1 associated with SBP at baseline in treated patients only
No nsns
E 212 [25]
ADD1GNB3
Naive and PTP+
THZ (diuretics)
No No, in relation to MI or stroke event
ns E 701 [14]
ADD1 PTP- THZ Yes No, in relation to BP or CHD event
ns EA
12,362mixed(34.4% A)
[8]
ADD1ACE I/DAGTAGTR1
Naive and PTP+ 4 weeks
HCTZ No Yes Gly Gly
Gly: -5.5 ns E 208 [15]
ADD1WNK1NEDD4L
Naive HCTZ YesNoNo
YesYesNo
SBP: -11.4SBP: -11.8
<0.05<0.01ns
E 193 [52]
NEDD4L PTP+ 4 weeks
HCTZ Yes Yes SBP: -23.3 DBP: -10.6 R2: 35.4% SBP37.0% DBP
0.0090.027
C 542 (2 weeks)311 (4 weeks)
[16]
ADD1 PTP- THZ (diuretics)+ other
Not tested Relation to MI:Yes, for Gly460 carriersNo, for Trp460 carriers
NR
NR
0.62
0.88
0.005
ns
E 1203 [53]
STK39 Naive and PTP+ (GERA and PEAR) PTP+ (validation)
HCTZ
HCTZ
Not tested Yes, in Caucasians
No
DBP: -7.8
NR
DBP: 1.83
0.0160.009
ns
EA
195194
GERA (201 E + 274 A)PEAR (113 E + 81 A)
[17]
OAT1
OAT3
Naive PTP+ (8 weeks)
HCTZ
HCTZ+
No Yes, after correction for pretreatment
SBP: 4.84 weeks – I trial
SBP: 6.18 weeks – II trial
0.006
0.003
C I trial:524 (2 weeks) → 311 (4 weeks)II trial: 274 (4 weeks) → 245 (8 weeks)
[19]
Effect size: decrease in blood pressure after thiazide treatment. Studies are listed in chronological order and divided into single genes, gene interactions and genome-wide association studies.†Expressed as.‡Not explicitly mentioned in the paper.A: African; C: Chinese; CHD: Coronary heart disease; DBP: Diastolic blood pressure; E: European; GWAS: Genome-wide association studies; HCTZ: Hydrochlorothiazide; HT: Hypertension; I/D: Insertion/deletion; J: Japanese; MBP: Mean blood pressure; MI: Myocardial Infarction; NR: Not reported; ns: Nonsignificant; OR: Odds ratio; PTP-: Previously treated patients without washout; PTP+: Previously treated patients with washout; SBP: Systolic blood pressure; SS: Sassari; THZ: Thiazide; TSC: Thiazide-sensitive NaCl cotransporter.
Pharmacogenomics (2011) 12(11)1594 future science group
Review Citterio, Lanzani & Manunta
Table 1. Studies reporting the influence of gene polymorphisms on the effect of thiazide antihypertensive drugs (cont.).
Gene Previous treat-ment
Therapy Association with HT
Association to response
Treatment result p-value Population descent
Sample size Ref.
Effect size† OR
Single genes (cont.)
RENAGTACE I/D
PTP-? HCTZ
HCTZ+ other
Not tested Yes, REN Mono SBP: -18
Add on
0.007
ns
C 30 (mono-therapy)60 (add on therapy)
[20]
GRK5 ADRBK1
NaivePTP+ 4–6 weeks (PEAR)
HCTZ Not tested No, GRK5Yes, ADRBK1
Black:SBP: -13DBP: -9;White: SBP: -9DBP: -5
0.04
0.0034
EA
237167
[22]
ACE I/DCYP11B2
PTP+ 2 weeksplacebo
HCTZ Not tested Yes, ACE SBP: DD: -9.4, ID: -4.8, II: -5.1
0.009 C (Han) 816 [26]
Gene interactions
ADD1 ACE I/D
Naive HCTZ No Yes, additive MBP: 12.7 15.75 E 86 [39]
AGTRENACE I/DAGTR1CYP11B2
PTP+ HCTZ Not tested Yes, AGT + AGTR1 in black femalesInteraction: additive effect
Add -24 ‡ EA
246255
[23]
ADD1AGT
Naive andPTP-
THZ (diuretics)
No Yes, in two-SNP ana lysisADD1–AGT
DBP: -3.09 ‡ E 106 [24]
ADD1AGTACE I/D
Naive andPTP+
THZ (diuretics)
Not tested No ns E 212 [25]
ADD1WNK1NEDD4L
Naive HCTZ Yes, in two-SNP ana lysis with ADD1 +NEDD4L
Yes, in two-SNP ana lysis with ADD1 +WNK1Yes, in three-SNP ana lysis among ADD1 Trp–WNK1 GG–NEDD4L GG
SBP: -15.2
SBP: -23.2
p trend0.008
p trend0.008
E 193 [52]
ACE I/DCYP11B2
PTP+ 2 weeks placebo
HCTZ No interaction ns C (Han) 776 [26]
Effect size: decrease in blood pressure after thiazide treatment. Studies are listed in chronological order and divided into single genes, gene interactions and genome-wide association studies.†Expressed as.‡Not explicitly mentioned in the paper.A: African; C: Chinese; CHD: Coronary heart disease; DBP: Diastolic blood pressure; E: European; GWAS: Genome-wide association studies; HCTZ: Hydrochlorothiazide; HT: Hypertension; I/D: Insertion/deletion; J: Japanese; MBP: Mean blood pressure; MI: Myocardial Infarction; NR: Not reported; ns: Nonsignificant; OR: Odds ratio; PTP-: Previously treated patients without washout; PTP+: Previously treated patients with washout; SBP: Systolic blood pressure; SS: Sassari; THZ: Thiazide; TSC: Thiazide-sensitive NaCl cotransporter.

www.futuremedicine.com 1595future science group
Polymorphisms, hypertension & thiazide diuretics Review
the expression and activity of both the apical (NCC) transporters and basolateral (kidney-specific chloride channels) channels expressed in distal convolute tubule of Milan Hypertensive animals are upregulated [29]. These data clearly indicate that different mechanisms could be involved in the triggering and maintenance phase. For instance, BP increase in response to diuretic or BB treatment, as reported in Figure 1, suggests that the triggering mechanisms may be opposite: volume, Na-related or increased sympathetic activity, respectively, for the two antihypertensive treatments.
In agreement with this concept is the result obtained at the clinical level in a population-based study by Kuznetsova et al. who studied certain cardiac parameters (e.g., lateral mitral annular early peak diastolic mitral annular velocities [Ea], late peak diastolic mitral annular velocities [Aa] and the ratio at the four acquisition sites [Ea/Aa]) in relation to age group and ADD1 Gly460Trp genotype [30]. For lateral Ea and Ea/Aa, there was a significant interaction between the ADD1 geno-type and age, – analyzed as a continuous variable – indicating that the genetic effects of ADD1 were significantly more prominent in younger subjects in whom longstanding environmental factors and aging are less likely to mask genetic effects.
Renovascular hypertension (RVH) is an exam-ple of a hypertension phase, in which increased BP is triggered by the reduction of renal blood flow (i.e, renal artery constriction). RVH is sustained by a sequence of mechanisms that start with renal secretion of REN, followed by renal sodium retention, and ending with peripheral vascular autoregulation or vascular remodeling. At this phase, structural vascular or organ changes may take over the initial functional changes [31–33].
Regardless of this variety of mechanisms, hyper-tension may be reverted by removing the renal artery stenosis [34]. However, if this maneuver is performed when the vascular structural changes or renal damage reach a critical level that confers to them the ability to maintain hypertension, its effect on BP is negligible [35].
The time (or phase)-dependent changes of the various mechanisms supporting hyperten-sion occur in spite of the fact that a ‘trigger-ing’ mechanism – the renal artery clip – main-tains the same degree of artery constriction. In humans with primary hypertension, RVH or monogenic forms of hypertension, there are data to support the phase-dependent variations of the mechanisms underlying hypertension or organ damage [15]. Therefore, in order to correctly evaluate the genotype–intermediate phenotype relationship, the phase-dependent changes illus-trated above must take into consideration the natural history of hypertension (both the initial triggering mechanism and its secondary ones).
According to international guidelines, all newly diagnosed hypertensives, before starting any antihypertensive medication, must imple-ment lifestyle chances and dietary modifica-tions [36]. After this period, we may call them ‘naive patients’. Naive hypertensive patients may present no underlying target-organ damage and should be considered as being in the first hyper-tensive phase. The earliest symptoms include increased renal sodium reabsorption – owing to genetic variants – glomerular hyperfiltration and night urine output – which reflects isch-emic changes to tubules and a decline in the concentration function. In the second and third hypertensive phase, the next symptom is micro-albuminuria which suggests glomerular damage.
Table 1. Studies reporting the influence of gene polymorphisms on the effect of thiazide antihypertensive drugs (cont.).
Gene Previous treat-ment
Therapy Association with HT
Association to response
Treatment result p-value Population descent
Sample size Ref.
Effect size† OR
Genome-wide association studies
100K Affymetrix array
PTP+ HCTZ Not tested Yes, three-SNP haplotype in black sample:LYZ, YEATS4,FRS2
DBP‡ 2.39 × 10-7
EA
195194
[27]
Effect size: decrease in blood pressure after thiazide treatment. Studies are listed in chronological order and divided into single genes, gene interactions and genome-wide association studies.†Expressed as.‡Not explicitly mentioned in the paper.A: African; C: Chinese; CHD: Coronary heart disease; DBP: Diastolic blood pressure; E: European; GWAS: Genome-wide association studies; HCTZ: Hydrochlorothiazide; HT: Hypertension; I/D: Insertion/deletion; J: Japanese; MBP: Mean blood pressure; MI: Myocardial Infarction; NR: Not reported; ns: Nonsignificant; OR: Odds ratio; PTP-: Previously treated patients without washout; PTP+: Previously treated patients with washout; SBP: Systolic blood pressure; SS: Sassari; THZ: Thiazide; TSC: Thiazide-sensitive NaCl cotransporter.

Pharmacogenomics (2011) 12(11)1596 future science group
Review Citterio, Lanzani & Manunta
The degree of urine protein ranges from trace to moderate. A 24-h urine protein is less than 1 g. However, naive hypertensives with altera-tion in diastolic function, microalbuminuria, or increased vascular intima-media thickness should be considered in the second hyperten-sive phase. Moreover, hypertensive patients with more pronounced target-organ damage such as the presence of left ventricular hypertrophy or stage II chronic kidney disease should be consid-ered in the third hypertensive phase. The phase affects which genetic mechanisms are at work.
Therefore, in PGX studies in which naive patients are recruited, the relationship between gene variants and diuretic response can be addressed with positive consistent results [19,37–40]. This is the unique condition in which PGX studies should be conducted. In fact, negative results have been obtained in previ-ously treated patients after a washout period of 30 days [11,15]. The rate of returning BP to pretreatment levels after withdrawal from ther-apy may vary between 1 month–1 year and is affected by the type of previous therapy. There are many publications demonstrating that 1 month of washout is not enough to remove the effect of the previous therapy. Indeed, the same patient could demonstrate an increased plasma REN after 1 month of diuretic washout compared with time before starting any treat-ment [41]. As a consequence, withdrawal effects should be avoided in order to elucidate the rela-tionship between genetic variants and response to drugs, especially for relatively short periods of therapy (1–2 months).
On the other hand, in previously treated patients, we may address the role of genetic mechanisms involved in major cardiac, renal and CNS events. For example, longlasting hyperten-sion is critical in the case of CV outcomes result-ing from many years of multifactorial arterial modifications. An average of a 3-year duration in the majority of clinical trials using different antihypertensive agents may identify a decrease of approximately 20–30% of CV events [4].
Our research group recently demonstrated that data obtained in naive patients cannot be replicated in those who are previously treated [40]. These findings are owing to CV structural changes associated with longlasting hypertension which superimpose and mask the characteristic genotype–phenotype relationship causing the initial development of hypertension [42,43]. The same type of results were obtained by Han et al. and demonstrate that the association between BP fall and the OAT1 and OAT3 gene pair is
involved in the transport of thiazide diuretics in naive patients, but not in previously treated patients [19].
All of the points discussed above support the need of naive patients in PGX studies lasting only a few weeks. The disregard of this require-ment by most PGX studies on primary hyper-tensive patients may account for inconsistent results published to date [44,45].
� Biased phenotypesStudying the relationship between DNA vari-ants and cellular- or whole-organism pheno-types in experimental settings for the estima-tion of the clinical impact of specific molecular mechanisms in complex human diseases represents a difficult task. The search for the missing heritability involves the structural and architectural variation in the genome, in the environment, and in unknown interactions and networks [46]. Despite numerous impre-cisions regarding current estimates, it may still be possible to discover ‘all the heritabil-ity’ by first improving phenotyping with the expansion to quantitative or more precise phe-notypes as required to reduce heterogeneity. Phenotype definition is the starting point for unbiased association designs. The main fac-tors that may potentially affect it at different levels are summarized here: mixed population relative to ethnicity of the study subjects [11]; small sample size leading to an underpowered study [12]; data collection in population-based studies by self-reported questionnaires for drug-use records; and uncertainties regarding the other antihypertensive agents used in the weeks preceeding BP measurements [24,25]. This last point is clearly linked to the already men-tioned problem of inclusion of patients not only receiving monotherapy with thiazides, but also combined therapy with other antihypertensive drugs [12,20] or inclusion of previously treated patients with a period of washout too short to avoid the effect of the previous drug (30 days) [15]. The extreme condition for BP basal values taken when the patients were switched from the previous therapy to diuretics, without a washout period or lack of any information of the dura-tion of hypertension or other confounders may influence phenotype definition [24]. Another crucial issue regards the lack of environmen-tal and gene–gene interaction ana lysis in the majority of papers [16]. In Table 1 we reported only six papers dealing with genetic epistasis, generally a two-SNP approach. Large sample sizes are now required to investigate multigenic

www.futuremedicine.com 1597future science group
Polymorphisms, hypertension & thiazide diuretics Review
analyses both in candidate genes and in new loci identified in GWA studies. In addition, appro-priate statistical tools will be required to cope with this complexity.
� Adducin-endogenous ouabain gene networkGly460Trp a-adducin polymorphism & HCTZOur research group was initially interested in the pharmacogenetic evaluation of BP response to diuretics according to a SNP ana lysis, and partic-ularly in ADD1 Gly460Trp (rs4961). Adducin is a heterodimeric cytoskeleton protein and consists of an a-subunit (ADD1) and either a b-subunit (ADD2) or g-subunit (ADD3), according to the tissue. This structural protein is involved in many cellular processes such as the promo-tion of the organization of the spectrin–actin lattice by favoring spectrin–actin binding, and by controlling the rate of actin polymerization as an end capping actin protein. Other adducin activities concern signal transduction, cell-to-cell contact formation and cell migration [47]. Most interestingly, the ADD1 minor Trp460 variant stimulates renal sodium transport by activation of NaK ATPase at the basolateral membrane with resulting enhanced tubular sodium transport and BP compared with carriers of the major Gly460 variant [47]. However, also a concurrent greater activation of Src-dependent signal transduction can be activated favoring both vascular remodel-ing and cardiac diastolic relaxation [42,48]. Owing to the increase in tubular sodium reabsorption, diuretics should trigger less counter-regulatory mechanisms, thus producing a more beneficial therapeutic effect in patients carrying the Trp allele. A recent basic study described the identi-fication of g-adducin as a novel auxiliary factor interacting with NCC in mouse kidney lysates. It was discovered that g-adducin dynamically regulated NCC, likely by amending the phos-phorylation state, and consequently the activity of the tr ansporter [49].
In the first study in 1997, the effect of a-addu-cin polymorphisms on the long-term response to diuretic treatment was tested in a small set of hypertensive patients. After 2 months of HCTZ therapy, the decrease in the MBP was greater in Gly/Trp heterozygotes than in Gly/Gly major homozygotes (mean decrease: 14.7 ± 2.2 vs 6.8 ± 1.4 mmHg, respectively; p = 0·002) [37]. The likelihood of such a response to chronic HCTZ treatment was greater in heterozygote patients than in major homozygotes: 11 (58%) out of 21 heterozygotes and eight (22%) out
of 37 major homozygotes demonstrated such a response (relative risk: 4.8). Moreover, PRA was lower in the Gly/Trp heterozygotes than in the major homozygotes; however, the difference did not reach significance [37].
In a subsequent study, two hypertensive popu-lations, the Sassari and Milano populations were treated for 2 months; the first with 12.5 mg/d HCTZ and the second with a double dose. A total of 30 patients out of 143 had been taking antihypertensive medications and had discontin-ued them for at least 4 months. Average MBP decreased after diuretic treatment significantly more in hypertensives carrying at least one 460Trp allele than in the 460Gly homozygotes (p < 0.001, pooled populations), despite a slight difference in frequency of the 460Trp allele between the two populations. This allele also significantly influenced basal PRA; it was lower after diuretic therapy irrespective of their being in the Sassari or Milano cohort [38]. The greater DBP, MBP varia-tion and lower pretreatment PRA after HCTZ treatment in individuals carrying at least one 460Trp allele were confirmed in a further study on another Sassari cohort comprised of 268 mild-to-severe primary hypertensive patients after 8 weeks of diuretic treatment [50]. In this study authors also reported erythrocyte abnormalities of sodium transport systems (e.g., the NaK pump, NaK
2Cl
cotransporter and LiNa counter-transporter), and intraerythrocyte sodium concentration accord-ing to ADD1 Gly460Trp genotype: this polymor-phism accelerated Na transport thereby affecting renal Na handling and BP regulation by an altera-tion in ion transport across the cell membrane through changes in the actin cytoskeleton [50].
This ADD1 genetic variant was used in an ele-gant population-based case–control study to verify whether it modified the effect of diuretic therapy on the incidence of MI and stroke. Among the carriers of the adducin major genotype, diuretic therapy was not associated with the risk of MI or stroke. Conversely, in carriers of the adducin variant, diuretic therapy was associated with a lower risk of combined MI or stroke than other antihypertensive therapies (OR: 0.49; 95% CI: 0.32–0.77; p = 0.002). The case–control synergy index was 0.45 (95% CI: 0.26–0.79) for the com-bined outcome of MI and stroke. The point esti-mates of this drug–gene interaction were similar in separate analyses of MI (synergy index: 0.41; 95% CI: 0.21–0.80) and stroke (synergy index: 0.53; 95% CI: 0.24–1.19). The data in this study suggest that among carriers of the ADD1 major genotype, diuretics are comparable with other antihypertensive medications; however, among
Pharmacogenomics (2011) 12(11)1598 future science group
Review Citterio, Lanzani & Manunta
All patients
Study number 2 Study number 1
HCTZ
Profile No NoYes
238
(a) (b) (c)
98 100
Yes YesNo
Losartan Rostafuroxin
Number of patients% of patients
Number of patients-50
-40
-30
-20
-10
10
20
30
0
346-50
-40
-30
-20
-10
0
SB
P d
ecre
ase
afte
r 5
wee
ks (
mm
Hg
)S
BP
dec
reas
e (m
mH
g)
10
20
30
Rostafuroxin
Placebo
(a) (b) (c) (d) (e)
196 7421%
4523%
2919%
ProfileADD1 rs4961 Trp and ADD3 rs3731566 GG
orLSS rs2254524 AA and ADD1 rs4961 Trp
orLSS rs2254524 CA+AA and MDR1 rs1045642 CC
orMDR1 rs1045642 TT and HSD3B1 rs10923835 AT+TT
No previous treatment
No previous treatment
Previous treatment
All patients
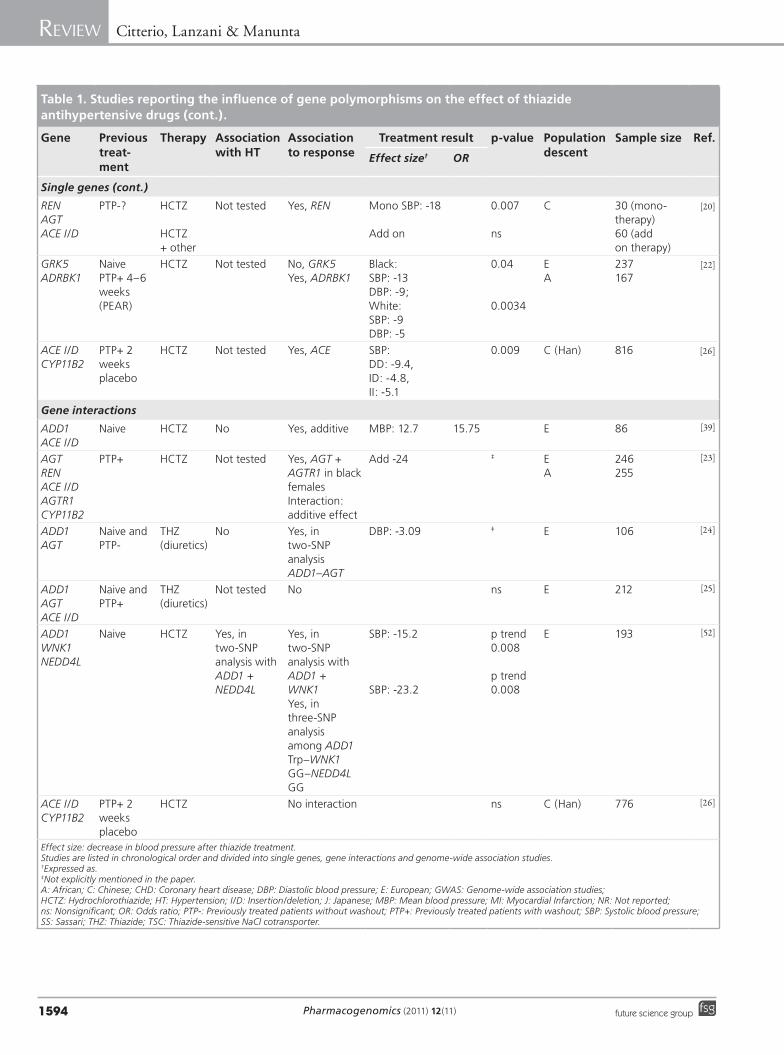
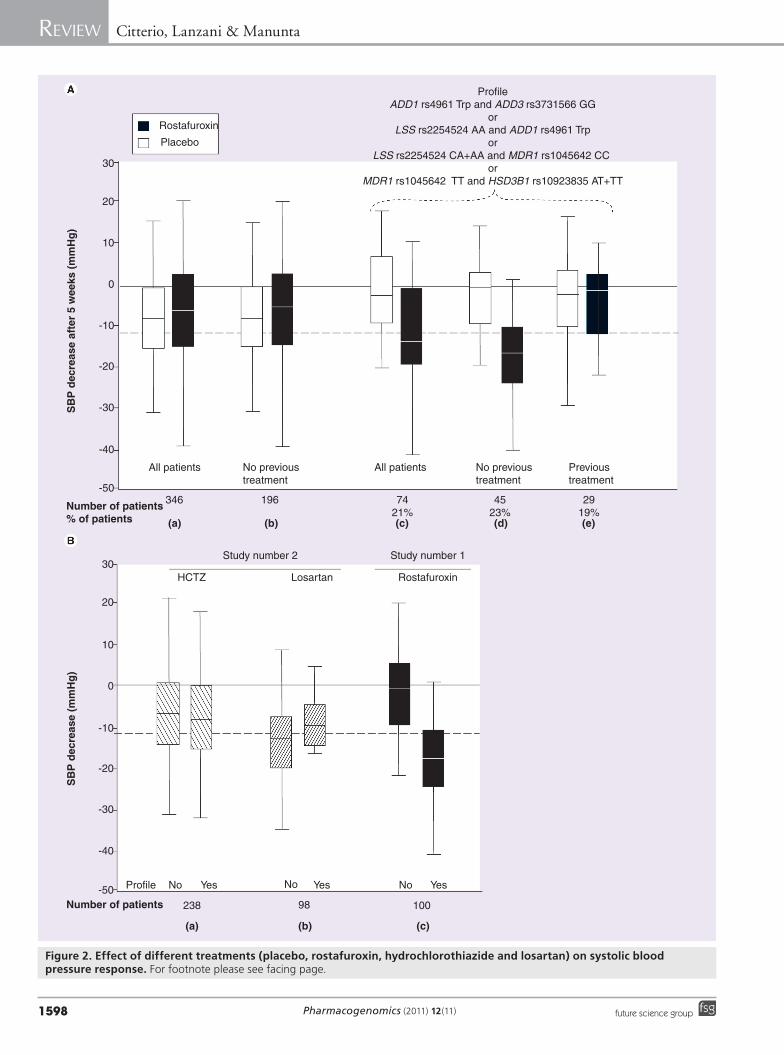
Figure 2. Effect of different treatments (placebo, rostafuroxin, hydrochlorothiazide and losartan) on systolic blood pressure response. For footnote please see facing page.

www.futuremedicine.com 1599future science group
Polymorphisms, hypertension & thiazide diuretics Review
carriers of the ADD1 460Trp variant, diuretics are associated with a lower risk of MI and stroke than other antihypertensive agents; a clear example of a drug–Gly460Trp genetic variant interaction in relation to the outcome of an event [51].
The study presented by Sciarrone [39] et al. rep-resented an improvement of pharmacogenetics in terms of both phenotyping and genetic contribu-tion: to avoid the interference of previous therapy and of the stage of the disease, only naive patients with mild hypertension were included, and two-SNP ana lysis was performed for two candidate genes (ADD1 and ACE). A significant decrease in MBP occurred after 2 months of treatment with HCTZ in the presence of both the inser-tion (I) allele of ACE and the 460Trp allele of ADD1 compared with the opposite combina-tion (-12.7 ± 1.9 mmHg vs -3.43 ± 1.7 mmHg, respectively). Considering an arbitrary definition of responders at MBP decrease >15 mmHg, an OR equal to 15.75 of being a responder to HCTZ was obtained for carriers of these two genotypic groups. Therefore, this last study represents a tentative attempt to cope with genetic com-plexity of drug response, based on a candidate gene approach.
In the GenHAT study, 36,913 hypertensive patients of white and black (34.4%) ethnicities were randomized to different drugs (e.g., thiazide, calcium channel blocker, ACEi and a-blocker) and genotyped for ADD1 Gly460Trp. A 6-month BP change according to genotype and treatment assignment revealed an identical SBP response to chlorthalidone in Trp allele carriers (-7.42 mmHg) and noncarriers (-7.44 mmHg), whereas DBP reduction was very slightly smaller in Trp allele carriers (-3.23 and -3.57 mmHg, respectively) with p-value of 0.116. Definitively, there were no clinically relevant genotype–treatment interac-tions for 6-month changes in SBP nor DBP [8]. Primary outcome coronary heart disease did not differ among treatments or genotypes nor was there any interaction between treatment and the
ADD1 Gly460Trp genotype. However, subgroup analyses indicated a potentially greater risk of treatment with thiazide compared with ACEi plus calcium channel blocker for the primary and several related secondary outcomes in Trp allele carriers compared with GlyGly homozygous women [8]. In this study, baseline characteristics were biased because GlyGly homozygotes were significantly (p < 0.0001) more frequent than the Trp allele carriers in black participants than in non-black participants. Furthermore, the BP basal values were taken when the patients were switched from the previous therapy to diuretics, without a washout period.
A different combination of common variants in the WNK1 and NEDD4L genes and again in the ADD1 Gly460Trp were chosen for associa-tion relative to two maneuvers changing body sodium: an acute saline infusion and chronic diuretic treatment [52]. In the distal tubule WNK1 affects sodium homeostasis through its effect on the NCC and sodium channel, while NEDD4L encodes ubiquitin ligase that con-trols cell-surface expression of epithelial sodium channels. To avoid the confounding influence of previous therapy or the duration of hyperten-sion on the genetic effect, enrolled patients were naive and consequently never treated. In this study the authors demonstrated the importance of taking into account the physiological inter-actions between the systems in identifying and understanding genetic effects. In fact, when indi-viduals carried specific alleles of the three genes in combination, the effects on renal-sodium handling and BP homeostasis could be marked and of potential clinical relevance (carriers: -23.2 mmHg vs a verage response -8.5 mmHg, p = 0.008) [52].
Van Wieren-de Wijer et al. reported a nested case–control study to determine whether the ADD1 460Trp variant allele modified the risk-lowering effect of diuretics on MI [53]. They concluded that the ADD1 gene does not play an
Figure 2. Effect of different treatments (placebo, rostafuroxin, hydrochlorothiazide and losartan) on systolic blood pressure response (please see facing page). (A) Effect on SBP response after 5 weeks of rostafuroxin (all doses; black) or placebo (white) in patients enrolled according to the presence or absence of the genetic profile. A genetic profile is a linear combination of genotypes at single SNPs or at their interactions. It combines at least one of the four interactions that demonstrated the greatest difference in variation of SBP within therapy, as indicated. (a) All patients; (b) no previously treated patients; (c) all patients carrying the genetic profile (general linear model: model, p = 2.38 × 10-5; profile × therapy interaction, p = 3.23 × 10-6); (d) no previously treated patients carrying the genetic profile (general linear model: model, p = 3.1 × 10-8; profile × therapy interaction, p = 1.84 × 10-8); (e) previously treated patients carrying the genetic profile. Percentages refer to relative group of patients. (B) Effect on SBP response according to the presence or absence of the genetic profile in different studies: 4 weeks of HCTZ (left, black striped) (a) or losartan (right, white striped) (b) (study 2), and 5 weeks of rostafuroxin (all doses, black) (c) (study 1; p = 7.84 × 10-8, one-way ANOVA). The box plot graph summarizes the statistical measures (median, the 75th and 25th percentiles and minimum and maximum data values) of the distribution of the SBP decreases (mmHg). The continuous line indicates 0 mmHg, whereas the dotted line represents the first tertile value of SBP decrease after treatment in study 1. HCTZ: Hydrochlorothiazide; SBP: Systolic blood pressure. Reproduced with permission from [40].

Pharmacogenomics (2011) 12(11)1600 future science group
Review Citterio, Lanzani & Manunta
important role in modifying the risk of nonfatal MI associated with the use of thiazide diuretics, despite among carriers of only major genotype the risk was significantly lower among thiazide users as compared with users of other antihypertensives (OR: 0.88; 95% CI: 0.58–1.33).
From all of these positive data it is clear that Trp allele carriers may benefit more strongly from thiazides than carriers of the Gly allele. It is well known that thiazide diuretics – in contrast to loop and potassium-sparing diuretics – induce a net retention of calcium [54]. A passive basolat-eral NaCa antiport driven by low intracellular sodium concentrations results in luminal calcium influx [55]. Both thiazides and the ADD1 Trp allele cause low intracellular sodium concentra-tion, predisposing Trp allele carriers to higher calcium reabsorption [50]. This may explain why thiazide-induced calcium retention, is faster and stronger in carriers of the ADD1 Trp allele.
Rostafuroxin pharmacogenomic trial A recent challenge in the post-genome era is taking advantage of the recent discoveries of individual gene susceptibility to disease, deci-phering biological function of these variants and identifying gene networks that in turn regulate the outcome of the disease. This rep-resents an improved procedure in comparison to using single-gene information usually devoid of context [56]. Conversely, the concept of reg-ulatory genetic network properly handles the genetic complexity, and most importantly, is a new opportunity to detect the molecular target for developing tailored therapeutic interven-tions [42]. Furthermore, the pharmacogenomic approach with naive hypertensives, may be use-ful to strengthen the ‘causation’ of genetic mech-anism, the so-called ‘triggering mechanism’. In this way it is possible to select subsets of patients relatively more homogenous for the respective core genetic network, clinical characteristics (type of organ damage) and in turn longlasting response to a selective drug.
To date there are not many examples of rational drug design projects started with more attention to these features than the traditionally targeted receptors. An example is reported by our group in two companion papers describing the effect of a very selective inhibitor of endog-enous ouabain and the Trp ADD1 allele, both performed in rodents and in humans [40,57]. Rostafuroxin normalized BP in the subset of naive patients carrying specific genotypes, alone or in combination, or clustered in a profile com-posed of least one of the combinations of gene
variants. This approach takes into account the genetic heterogeneity controlling the endogenous ouabain tissue concentrations, the interaction between ouabain and adducin with Src–Na, K-ATPase and rostafuroxin effects. By group-ing all of the patients carrying the profile, we obtained a mean placebo-corrected SBP fall of 14 mmHg [40]. This study also reported a con-trolled study in which naive patients received two reference antihypertensive drugs; losartan and HCTZ. The values for the SBP fall after 4 weeks of treatment in carriers of the profile mentioned above did not vary compared with noncarriers (-10.6 ± 3.3 vs -13.1 ± 1.04 mmHg or -8.5 ± 1.5 vs -7.8 ± 0.96 mmHg, respectively, Figure 2) [40].
ConclusionThe success of tailored medicine depends on having accurate diagnostic tests capable of iden-tifying patients who can respond to t argeted th erapies or who are susceptible to adverse effects. The increase in rate of many promising drug candidates failing the late-stage clinical phases concerns different level of inadequacy: a poor understanding of the pathways involved in the mechanism of action; the use of selective ligands acting on individual target design, fol-lowing the rational of the ‘one gene, one drug, one disease’ paradigm. The former weakness could depend on an inappropriate choice of ani-mal models that fail to target effects in humans, while the latter could be overcome by the novel concept of polypharmacology, which is built on the fundamental concept that drugs modulate multiple targets [58]. Consequently, advances in this field should boost research on allosteric inhibitors, or molecules that might target alter-et alter-ter-native sites, many of which are sites of protein–protein interactions (targeting interactions). Finding drug-like molecules capable of disrupt-ing an interaction remains a major challenge for successful clinical translation, and new techno-logical developments in basic science will likely make this standard practice in the future [59].
A pharmacogenomic procedure may not only optimize the development of targeted drugs and dose and treatment duration, but may also facili-tate the identification of subgroups of patients likely to benefit from current drugs such as diuret-ics. In this case, an ideal study should respect general principles of including naive hypertensive individuals with phenotypic specificity, and the genetic prediction markers should be components of a system targeted by the drug or of the counter-regulatory systems opposing the drug effect in BP fall. As thiazide acts on a precise target, the
www.futuremedicine.com 1601future science group
Polymorphisms, hypertension & thiazide diuretics Review
NaCl symporter on the distal convolute tubule, but influences several physiological mechanisms, its effect is spread along different pathways not central to the targeted disease. This implies that genetic profiling for the identification of patients who will respond will not presumably reach cer-tain levels of sensitivity compared with those rela-tive to specific molecular targets, as in the case of rostafuroxin.
Future perspectiveAccording to the hypertension phase, we could be on a brink of a new era in pharmacogenomic studies:
� Early phase, in which the triggering mecha-nism (i.e., increased Na reabsorption, renal artery stenosis and hyperaldosteronism) pro-motes the transition from normotension to hypertension [42]. This early phase corresponds to precise renal phenotypes as a right shift of
the pressure natriuresis relationship [60], renal glomerular hyper filtration and cardiac pheno-types as diastolic cardiac dysfunctions (lateral mitral annular Ea, Aa and Ea/Aa) [61,62].
� Maintenance phase in which BP rise is sus-tained by hormonal modifications (e.g., RAAS and endogenous ouabain) or increased activity of sympathetic nervous system. As a conse-quence, vascular remodeling occurs with a fur-ther increase in BP [63,64]. Left-ventricular car-diac hypertrophy and initial kidney damage as microalbuminuria leaking become evident [65].
� Late phase which leads to target-organ damage as a result of years of uncontrolled hyperten-sion [3]. Despite the great amount of resources spent, only 20–30% of hypertensive popula-tions have BP values at target, lower than 135/85 mmHg [1–3,66], resulting in an increased
Executive summary
State-of-the-art of blood pressure control � Cardiovascular diseases are the major causes of health burdens and costs worldwide, and arterial hypertension may account for
approximately 50% of them. � In the general hypertensive population, approximately only one third of patients have a control of their blood pressure by way of
therapy. The efficiency of the current therapeutic strategy in preventing cardiovascular diseases is further reduced in this population. � Despite major advances in this field, pharmacogenomics has so far failed to create a major impact on day-to-day prescription practices.
Types of pharmacogenomic studies in thiazide treatment � A review of indexed papers, available as full text on PubMed from 1997–March 2011 showing a pharmacogenomic approach with
regard to thiazide treatment were included. Analysis of studies with hydrochlorothiazide (HCTZ) monotherapy was performed. � First, published papers dealing with candidate-gene approaches for single-gene interactions with drug response were analyzed. Second,
combinations of candidate genes involved in related mechanism of actions for functional response to HCTZ treatment. Third, genome-wide association studies in large hypertensive population treated with diuretic were examined.
Main reasons for inconsistent results � Two main reasons account for some inconsistent findings among the association responses of certain SNP variants in different studies:
the phase of hypertension considered and biased phenotypes. � Phase of hypertension: to study the relationship between the genotypes of the patients and their response to drugs, all of the
confounder effects of previous therapy need to be got rid of. When naive patients were recruited, positive consistent results were obtained.
� Biased phenotype: the aim is to discover ‘all the heritability’ by improving phenotyping. This can be achieved by avoiding mixed populations relative to ethnicity, small sample sizes leading to an unpowered study, by removing uncertainties about the other antihypertensive agent use in weeks before, and by improving environmental and gene–gene interaction analysis.
Adducin-endogenous ouabain gene network: a special case of pharmacogenomic risk modeling � Pharmacogenetic studies on Adducin 1 gene are an example of analysis of both single and combination of genes using
naive hypertensives. � Improvement of procedure, using the concept of regulatory genetic network, properly handled the genetic complexity and is a new
technique for the detection of the molecular target to allow for the development of tailored therapeutic intervention: the Adducin-endogenous ouabain gene network.
� Genetic profile selection for the effect of a very selective inhibitor takes into account the genetic heterogeneity controlling the ouabain tissue concentrations and the interaction between ouabain and adducin with Src–Na, K-ATPase. This genetic profile is highly specific as not effective for two reference antihypertensive drug response, losartan and HCTZ.
Advances in the pharmacogenomics of thiazides � Identification of subgroups of patients likely to benefit to current drugs such as diuretics. � According to the hypertension phase, inclusion of untreated hypertensive individuals with phenotypic specificity. � In previously treated patients, the role of genetic mechanisms involved in major cardiac, renal and cardiovascular events may
be addressed. � Detection of the regulatory genetic network where genetic variant(s) operate with all the interacting environmental and biological
factors and the respective hierarchical organization.

Pharmacogenomics (2011) 12(11)1602 future science group
Review Citterio, Lanzani & Manunta
BibliographyPapers of special note have been highlighted as:� of interest�� of considerable interest
1 Abegunde DO, Mathers CD, Adam T, Ortegon M, Strong K. The burden and costs of chronic diseases in low-income and middle-income countries. Lancet 370, 1929–1938 (2007).
2 Williams B. The year in hypertension. J. Am. Coll. Cardiol. 55, 65–73 (2009).
3 Kearney PM, Whelton M, Reynolds K et al. Global burden of hypertension: ana lysis of worldwide data. Lancet 365, 217–223 (2005).
4 Turnbull F. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trials. Lancet 362, 1527–1535 (2003).
5 Chobanian AV. Shattuck lecture. The hypertension paradox--more uncontrolled
disease despite improved therapy. N. Engl. J. Med. 361, 878–887 (2009).
6 Levy D, Larson MG, Vasan RS, Kannel WB, Ho KK. The progression from hypertension to congestive heart failure. JAMA 275, 1557–1562 (1996).
7 Raman SV. The hypertensive heart. An integrated understanding informed by imaging. J. Am. Coll. Cardiol. 55, 91–96 (2010).
8 Davis BR, Arnett DK, Boerwinkle E et al. Antihypertensive therapy, the a-adducin polymorphism, and cardiovascular disease in high-risk hypertensive persons: the Genetics of Hypertension-Associated Treatment Study. Pharmacogenomics J. 7, 112–122 (2007).
9 Turner ST, Schwartz GL, Chapman AB, Boerwinkle E. C825T polymorphism of the G-protein b(3)-subunit and antihypertensive response to a thiazide diuretic. Hypertension 37, 739–743 (2001).
10 Schwartz GL, Turner ST, Chapman AB, Boerwinkle E. Interacting effects of gender and genotype on blood pressure response to hydrochlorothiazide. Kidney Int. 62, 1718–1723 (2002).
11 Turner ST, Chapman AB, Schwartz GL, Boerwinkle E. Effects of endothelial nitric oxide synthase, a-adducin, and other candidate gene polymorphisms on blood pressure response to hydrochlorothiazide. Am. J. Hypertens. 16, 834–839 (2003).
12 Matayoshi T, Kamide K, Takiuchi S et al. The thiazide-sensitive Na(+)-Cl(-) cotransporter gene, C1784T, and adrenergic receptor-b3 gene, T727C, may be gene polymorphisms susceptible to the antihypertensive effect of thiazide diuretics. Hypertens. Res. 27, 821–833 (2004).
13 Turner ST, Schwartz GL, Chapman AB, Boerwinkle E. WNK1 kinase polymorphism
number of CV events such as acute MI, chronic kidney disease and stroke.
Therefore, in PGX studies two types of patients can be recruited: naive patients and previous-treated patients.
In naive patients it is possible to address: the functional effect of the gene variants of inter-est in humans; the regulatory genetic network where the gene is operating with all the inter-acting environmental and biological factors and the respective hierarchical organization; the consistency between the natural history of the established pathophysiological mecha-nisms underlying hypertension; and the new molecular mechanism detected with genetics. Furthermore, naive patients may be appropri-ate for studying the genotype–BP relationships without the confounders owing to the influ-ence of previous treatments that cannot be removed by a washout period of 1 month, or the various phases of hypertension that involve a variety of additional molecular mechanisms that superimpose the triggering one.
However, in previously treated patients, the rate of returning to pretreatment BP lev-els after withdrawal from therapy may vary from 1 month–1 year, and the type of previ-ous therapy affects such a rate. There are many publications demonstrating that 1 month of washout is not enough to remove the effect of the previous therapy.
On the other hand, withdrawal, per se, may trigger a variety of pressor mechanisms
(e.g., increasing REN–angiotensin system activity after removal of their inhibitors), which are unrelated to the mechanisms triggered by the genetic architecture underlying the initial development of hypertension. Therefore, to study the relationship between the genotypes of the patients and their response to drugs, we need to get rid of all the confounder effects of previous therapy.
Furthermore, large studies in previously treated patients coming from a long history of previous therapies, population stratification and other confounders must also be taken into con-sideration. In all of these studies there are long-term follow-up data, with a number of discreet events or continuous phenotypes that are cer-tainly suitable for pharmacogenomic ana lysis. Of course, we expect to find different genetic mechanisms related to environmental, pharma-cological or organ-damage m odifications that could be relevant for CV events.
Financial & competing interests disclosureResearch at the authors’ laboratories is financed by Italian Ministry of Health grant RF-FSR-2008-1141719 (P Manunta) and Italian Ministry of University and Scientif ic Research grant 2008W5AZEC_ 001 (P Manunta). The authors have no other relevant affilia-tions or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
www.futuremedicine.com 1603future science group
Polymorphisms, hypertension & thiazide diuretics Review
www.futuremedicine.com
and blood pressure response to a thiazide diuretic. Hypertension 46, 758–765 (2005).
� A positive pharmacogenetic response for the WNK1 gene, predicting interindividual differences in antihypertensive treatment to hydrochlorothiazide.
14 Schelleman H, Klungel OH, Witteman JC et al. Diuretic–gene interaction and the risk of myocardial infarction and stroke. Pharmacogenomics J. 7, 346–352 (2007).
15 Suonsyrja T, Hannila-Handelberg T, Fodstad H et al. Renin-angiotensin system and a-adducin gene polymorphisms and their relation to responses to antihypertensive drugs: results from the GENRES study. Am. J. Hypertens. 22, 169–175 (2009).
16 Luo F, Wang Y, Wang X et al. A functional variant of NEDD4L is associated with hypertension, antihypertensive response, and orthostatic hypotension. Hypertension 54, 796–801 (2009).
17 Duarte JD, Lobmeyer MT, Wang Z et al. Lack of association between polymorphisms in STK39, a putative thiazide response gene, and blood pressure response to hydrochlorothiazide. Pharmacogenet. Genom. 20, 516–519 (2010).
18 Wang Y, O’Connell JR, McArdle PF et al. From the cover: whole-genome association study identifies STK39 as a hypertension susceptibility gene. Proc. Natl Acad. Sci. USA 106, 226–231 (2009).
19 Han YF, Fan XH, Wang XJ et al. Association of intergenic polymorphism of organic anion transporter 1 and 3 genes with hypertension and blood pressure response to hydrochlorothiazide. Am. J. Hypertens. 24, 340–346 (2010).
�� Underlines two important points: to get significant results it is important to study the untreated hypertensives, and a polymorphism not associated with hypertension per se may be relevant for response to therapy.
20 Huang CC, Chung CM, Hung SI et al. Genetic variation in renin predicts the effects of thiazide diuretics. Eur. J. Clin. Invest. 41(8), 828–835 (2011).
21 Johnson JA, Boerwinkle E, Zineh I et al. Pharmacogenomics of antihypertensive drugs: rationale and design of the Pharmacogenomic Evaluation of Antihypertensive Responses (PEAR) study. Am. Heart J. 157, 442–449 (2009).
22 Lobmeyer MT, Wang L, Zineh I et al. Polymorphisms in genes coding for GRK2 and GRK5 and response differences in antihypertensive-treated patients. Pharmacogenet. Genom. 21, 42–49 (2011).
23 Frazier L, Turner ST, Schwartz GL, Chapman AB, Boerwinkle E. Multilocus effects of the renin-angiotensin-aldosterone system genes on blood pressure response to a thiazide diuretic. Pharmacogenomics J. 4, 17–23 (2004).
24 Schelleman H, Stricker BH, Verschuren WM et al. Interactions between five candidate genes and antihypertensive drug therapy on blood pressure. Pharmacogenomics J. 6, 22–26 (2006).
25 Schelleman H, Klungel OH, Witteman JC et al. The influence of the a-adducin G460W polymorphism and angiotensinogen M235T polymorphism on antihypertensive medication and blood pressure. Eur. J. Hum. Genet. 14, 860–866 (2006).
26 Li Y, Zhou Y, Yang P et al. Interaction of ACE and CYP11B2 genes on blood pressure response to hydrochlorothiazide in Han Chinese hypertensive patients. Clin. Exp. Hypertens. 33(3), 141–146 (2011).
27 Turner ST, Bailey KR, Fridley BL et al. Genomic association ana lysis suggests chromosome 12 locus influencing antihypertensive response to thiazide diuretic. Hypertension 52, 359–365 (2008).
28 Capasso G, Rizzo M, Evangelista C et al. Altered expression of renal apical plasma membrane Na+ transporters in the early phase of genetic hypertension. Am. J. Physiol. Renal. Physiol. 288, F1173–F1182 (2005).
29 Capasso G, Rizzo M, Garavaglia ML et al. Upregulation of apical sodium-chloride cotransporter and basolateral chloride channels is responsible for the maintenance of salt-sensitive hypertension. Am. J. Physiol. Renal. Physiol. 295, F556–F567 (2008).
�� Evidence from animal models of different physiological mechanisms involved in distinct phases of salt-sensitive hypertension.
30 Kuznetsova T, Citterio L, Herbots L et al. Effects of genetic variation in adducin on left ventricular diastolic function as assessed by tissue Doppler imaging in a Flemish population. J. Hypertens. 26, 1229–1236 (2008).
31 Bianchi G, Tenconi LT, Lucca R. Effect in the conscious dog of constriction of the renal artery to a sole remaining kidney on haemodynamics, sodium balance, body fluid volumes, plasma renin concentration and pressor responsiveness to angiotensin. Clin. Sci. 38, 741–766 (1970).
32 Guyton AC, Coleman TG, Cowley AV Jr et al. Arterial pressure regulation. Overriding dominance of the kidneys in long-term regulation and in hypertension. Am. J. Med. 52, 584–594 (1972).
33 Davis JO. The pathogenesis of chronic renovascular hypertension. Circ. Res. 40, 439–444 (1977).
34 Funder JW, Blair-West JR, Cain MC et al. Circulatory and humoral changes in the reversal of renovascular hypertension in sheep by unclipping the renal artery. Circ. Res. 27, 249–258 (1970).
35 Edmunds ME, Russell GI, Bing RF. Reversal of experimental renovascular hypertension. J. Hypertens. 9, 289–301 (1991).
36 Mancia G, de Backer G, Dominiczak A et al. 2007 ESH-ESC practice guidelines for the management of arterial hypertension: ESH-ESC task force on the management of arterial hypertension. J. Hypertens. 25, 1751–1762 (2007).
37 Cusi D, Barlassina C, Azzani T et al. Polymorphisms of a-adducin and salt sensitivity in patients with essential hypertension. Lancet 349, 1353–1357 (1997).
38 Glorioso N, Manunta P, Filigheddu F et al. The role of a-adducin polymorphism in blood pressure and sodium handling regulation may not be excluded by a negative association study. Hypertension 34, 649–654 (1999).
39 Sciarrone MT, Stella P, Barlassina C et al. ACE and a-adducin polymorphism as markers of individual response to diuretic therapy. Hypertension 41, 398–403 (2003).
� Good example of a possible genetic interaction analysis in a pharmacogenetic treatment with hydrochlorothiazide.
40 Lanzani C, Citterio L, Glorioso N et al. Adducin- and ouabain-related gene variants predict the antihypertensive activity of rostafuroxin, part 2: clinical studies. Sci. Transl. Med. 2, 59ra87 (2010).
�� Successful translation from animals to humans of a novel drug targeting hypertensive genetic abnormalities in adducin- and ouabain-related genes.
41 Swart S, Bing RF, Swales JD, Thurston H. Plasma renin in long-term diuretic treatment of hypertension: effect of discontinuation and restarting therapy. Clin. Sci. (Lond.). 63, 121–125 (1982).
42 Citterio L, Lanzani C, Manunta P, Bianchi G. Genetics of primary hypertension: the clinical impact of adducin polymorphisms. Biochim. Biophys. Acta 1802, 1285–1298 (2010).
43 Guyton AC, Coleman TG, Granger HJ. Circulation: overall regulation. Ann. Rev. Physiol. 34, 13–46 (1972).
44 Arnett DK, Claas SA, Lynch AI. Has pharmacogenetics brought us closer to ‘personalized medicine’ for initial drug treatment of hypertension? Curr. Opin. Cardiol. 24, 333–339 (2009).
45 Johnson JA. Pharmacogenomics of antihypertensive drugs: past, present and future. Pharmacogenomics 11, 487–491 (2010).
Pharmacogenomics (2011) 12(11)1604 future science group
Review Citterio, Lanzani & Manunta
46 Manolio TA, Collins FS, Cox NJ et al. Finding the missing heritability of complex diseases. Nature 461, 747–753 (2009).
47 Bianchi G. Genetic variations of tubular sodium reabsorption leading to “primary” hypertension: from gene polymorphism to clinical symptoms. Am. J. Physiol. Regul. Integr. Comp. Physiol. 289, R1536–R1549 (2005).
48 Ferrandi MLC, Citterio L, Glorioso N et al. Also on behalf of OASIS-HT Investigators: probing the genetics of hypertension with rostafuroxin: from rats to patients. Sci. Transl. Med. 2, ra86 (2010).
49 Dimke H, San-Cristobal P, de Graaf M et al. g-Adducin stimulates the thiazide-sensitive NaCl cotransporter. J. Am. Soc. Nephrol. 22, 508–517 (2011).
50 Glorioso N, Filigheddu F, Cusi D et al. a-adducin 460Trp allele is associated with erythrocyte Na transport rate in North Sardinian primary hypertensives. Hypertension 39, 357–362 (2002).
51 Psaty BM, Smith NL, Heckbert SR et al. Diuretic therapy, the a-adducin gene variant, and the risk of myocardial infarction or stroke in persons with treated hypertension. JAMA 287, 1680–1689 (2002).
� A clear example of drug–ADD1 Gly460Trp genetic variant interaction in relation to the outcome of myocardial infarction or stroke.
52 Manunta P, Lavery G, Lanzani C et al. Physiological interaction between a-adducin and WNK1-NEDD4L pathways on sodium-related blood pressure regulation. Hypertension 52, 366–372 (2008).
�� Genetic epistatic interaction of different genes influencing renal sodium transport systems in response to acute sodium load and response to hydrochlorothiazide.
53 van Wieren-de Wijer DB, Maitland-van der Zee AH, de Boer A et al. Interaction between the Gly460Trp a-adducin gene variant and diuretics on the risk of myocardial infarction. J. Hypertens. 27, 61–68 (2009).
54 Rejnmark L, Vestergaard P, Pedersen AR et al. Dose-effect relations of loop- and thiazide-diuretics on calcium homeostasis: a randomized, double-blinded Latin-square multiple cross-over study in postmenopausal osteopenic women. Eur. J. Clin. Invest. 33, 41–50 (2003).
55 Vormfelde SV, Sehrt D, Bolte D et al. Hydrochlorothiazide efficacy and polymorphisms in ACE, ADD1 and GNB3 in healthy, male volunteers. Eur. J. Clin. Pharmacol. 62, 195–201 (2006).
56 Chen Y, Zhu J, Lum PY et al. Variations in DNA elucidate molecular networks that cause disease. Nature 452, 429–435 (2008).
57 Ferrandi M, Molinari I, Torielli L et al. Adducin- and ouabain-related gene variants predict the antihypertensive activity of rostafuroxin, part 1: experimental studies. Sci. Transl. Med. 2, 59ra86 (2010).
58 Hopkins AL. Network pharmacology: the next paradigm in drug discovery. Nat. Chem. Biol. 4, 682–690 (2008).
�� Advances in systems biology introduces the novel concept of polypharmacology both for efficacy and toxicity.
59 Russell RB, Aloy P. Targeting and tinkering with interaction networks. Nat. Chem. Biol. 4, 666–673 (2008).
60 Manunta P, Cusi D, Barlassina C et al. a-adducin polymorphisms and renal sodium handling in essential hypertensive patients. Kidney Int. 53, 1471–1478 (1998).
61 Manunta P, Ferrandi M, Bianchi G, Hamlyn JM. Endogenous ouabain in cardiovascular function and disease. J. Hypertens. 27, 9–18 (2009).
62 Kuznetsova T, Manunta P, Casamassima N et al. Left ventricular geometry and endogenous ouabain in a Flemish population. J. Hypertens. 27, 1884–1891 (2009).
63 Manunta P, Hamlyn JM, Simonini M et al. Endogenous ouabain and the renin-angiotensin-aldosterone system: distinct effects on Na handling and blood pressure in human hypertension. J. Hypertens. 29(2), 349–356 (2011).
64 Pulina MV, Zulian A, Berra-Romani R et al. Upregulation of Na+ and Ca2+ transporters in arterial smooth muscle from ouabain-induced hypertensive rats. Am. J. Physiol. Heart Circ. Physiol. 298, H263–H274 (2010).
65 Viazzi F, Leoncini G, Conti N et al. Microalbuminuria is a predictor of chronic renal insufficiency in patients without diabetes and with hypertension: the MAGIC study. Clin. J. Am. Soc. Nephrol. 5, 1099–1106 (2010).
66 Mancia G, Parodi A, Merlino L, Corrao G. Heterogeneity in antihypertensive treatment discontinuation between drugs belonging to the same class. J. Hypertens. 29, 1012–1018 (2011).