polio and its eradication initiatives - sapraa eradication - prof... · polio and its eradication...
TRANSCRIPT
POLIO AND ITS ERADICATION INITIATIVES
Presentation made to the South African Pharmaceutical Regulatory Affairs Association (SPRAA)
26th August 2016Presentation by Prof (Emeritus) MJ Matjila,
Chairman: National Polio Expert Committee (NPEC - South African)
Outline of the presentation
1. Historical events on polio disease2. Epidemiology3. Foundation for disease eradication4. Global polio eradication initiative5. Activities undertaken thus far & planned – at global, regional &
national levels6. Roles of health care workers and of members of the civil society, 7. Key take home messages
1400-1380 BCE
A VERY BRIEF HISTORY OF POLIOMYELITIS
Barry D. Schoub
Polio Eradication Stakeholder’s Symposium
Johannesburg. 10th Sept 2015

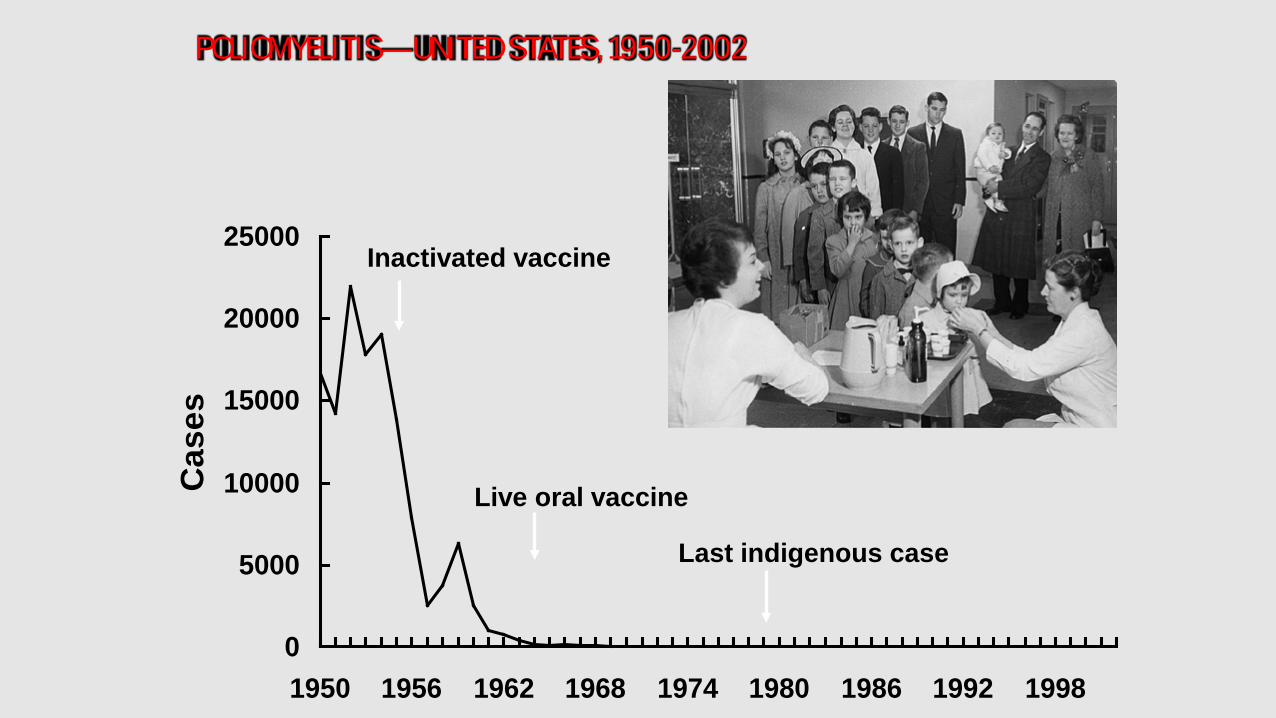
POLIOMYELITIS—UNITED STATES, 1950-2002
0
5000
10000
15000
20000
25000
1950 1956 1962 1968 1974 1980 1986 1992 1998
Cas
es
Inactivated vaccine
Live oral vaccine
Last indigenous case
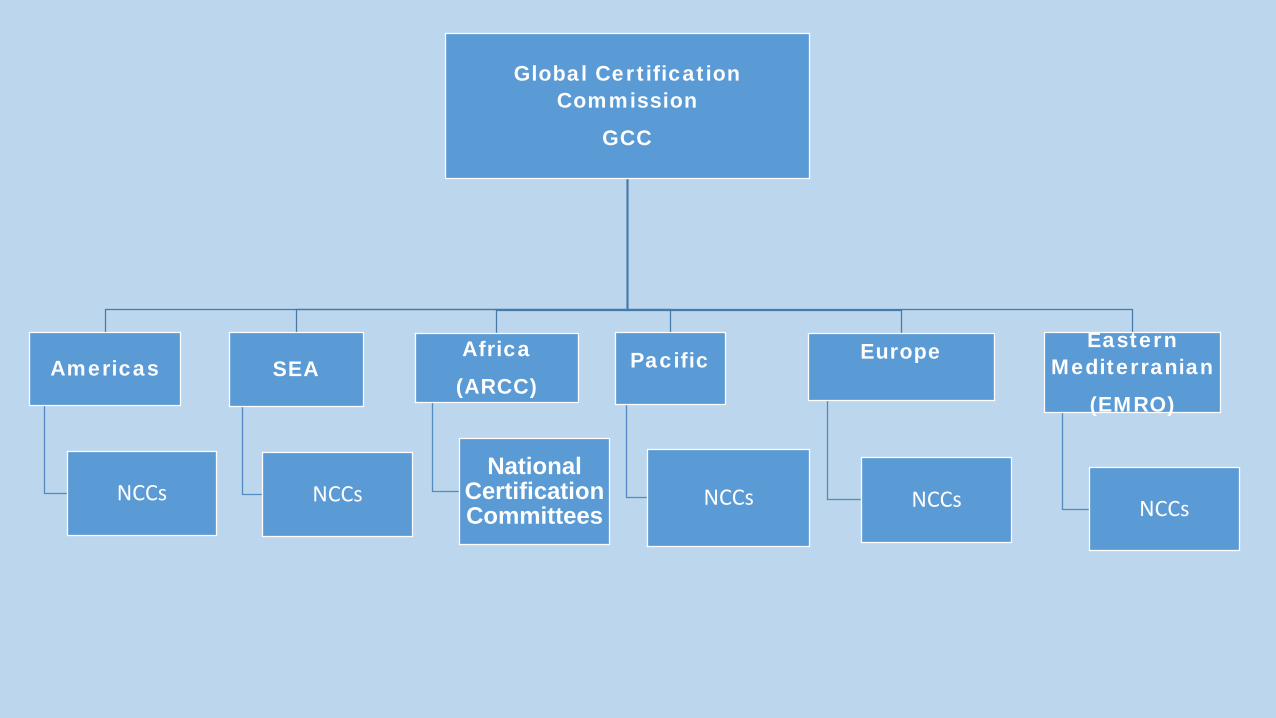
Global Certification Commission
GCC
Americas
NCCs
SEA
NCCs
Africa
(ARCC)
National Certification Committees
Pacific
NCCs
Europe
NCCs
Eastern Mediterranian
(EMRO)
NCCs
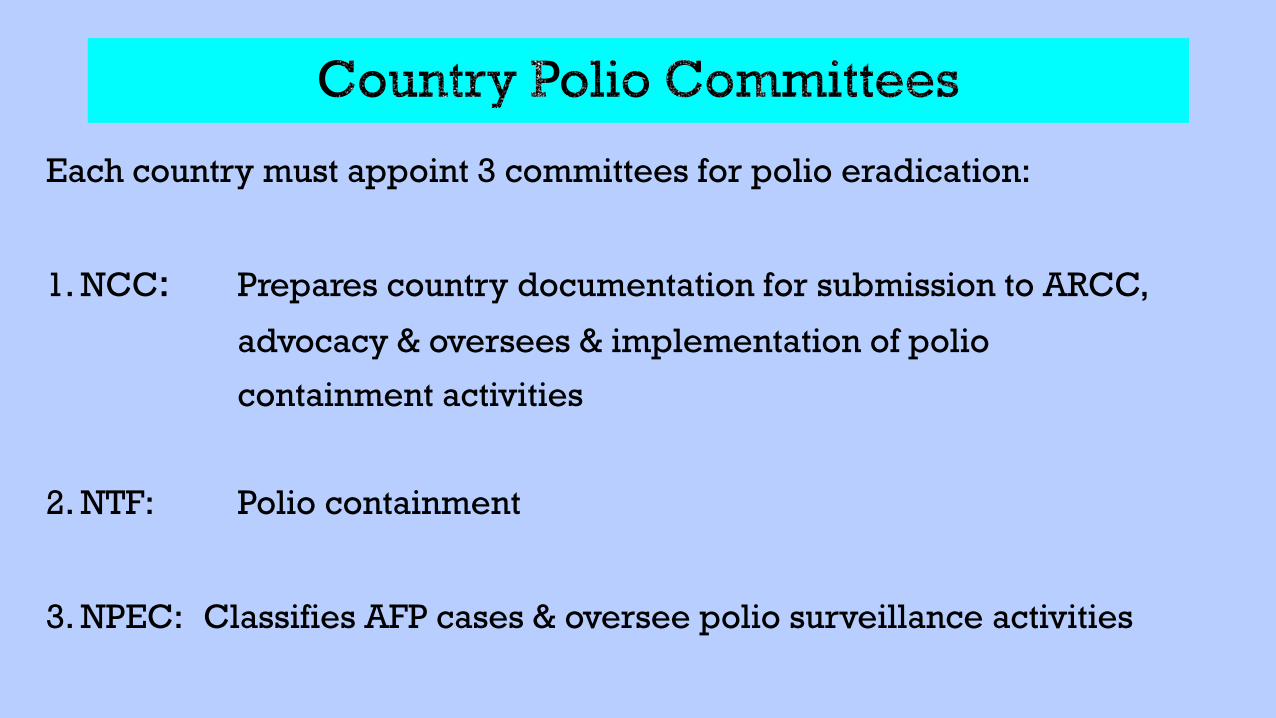
Each country must appoint 3 committees for polio eradication:
1. NCC: Prepares country documentation for submission to ARCC,
advocacy & oversees & implementation of polio
containment activities
2. NTF: Polio containment
3. NPEC: Classifies AFP cases & oversee polio surveillance activities
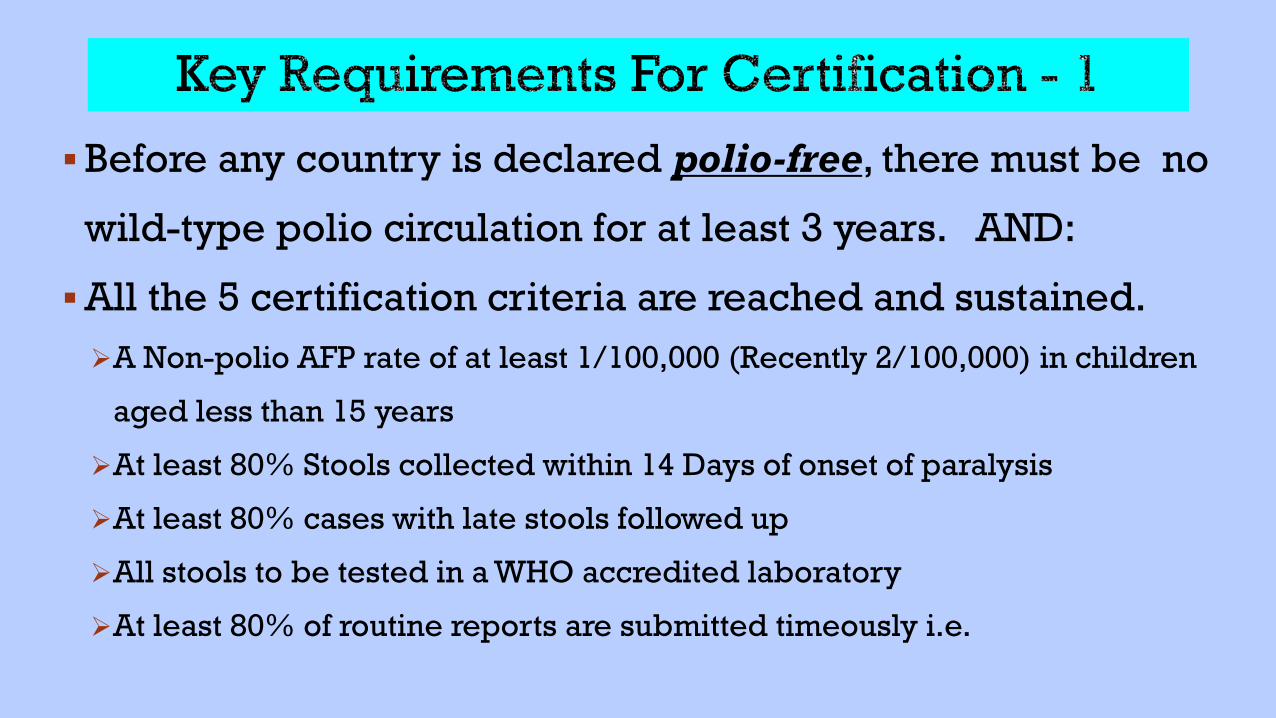
Before any country is declared polio-free, there must be no
wild-type polio circulation for at least 3 years. AND:
All the 5 certification criteria are reached and sustained. A Non-polio AFP rate of at least 1/100,000 (Recently 2/100,000) in children
aged less than 15 years
At least 80% Stools collected within 14 Days of onset of paralysis
At least 80% cases with late stools followed up
All stools to be tested in a WHO accredited laboratory
At least 80% of routine reports are submitted timeously i.e.
Poliomyelitis:Clinical Manifestations
• Most of infections occur in children <5 years of age
• Most of infections are in-apparent (Reservoir of infection especially in children)
• About 5% of infections – minor nonspecific illness:
Fever, malaise, headache, nausea & vomiting.
• +2% of infections - nervous system involvement
About 1% Flaccid paralysis &
About 1% Aseptic meningitis
• Flaccid paralysis occur in <1% of infections
Extent of paralysis reaches its maximum development within 3-4 days - hence AFP
Residual paralysis tends to be permanent after 60 days of clinical onset
Clinical aspects of Poliomyelitis infection
Most cases are asymptomatic infections
Clinical illness, flu like symptoms & no paralysis
Paralytic poliomyelitis only 1 in 200 infections
Paralysis is an unusual manifestation of infection
Poliovirus Transmission
Poliovirus infects only human beings, no animal reservoir. Primarily person-to-person via the faecal-oral route The time between infection and onset of paralysis is 10-21 days. Virus intermittently excreted for ≥ 1 month post- infection. Most viral shedding occurs just prior to the onset of paralysis and
during the first two weeks after paralysis occurs.
Pathogenesis
Virus enters oral cavity Local replication in tissues expressing receptor (e.g.
tonsils, Peyers patches of ileum, and lymph nodes) Viremia with hematologic spread to CNS Retrograde spread along neurons to spinal cordMotor neurons destroyed by viral replication Paralysis extent depends on proportion of motor neurons
lost
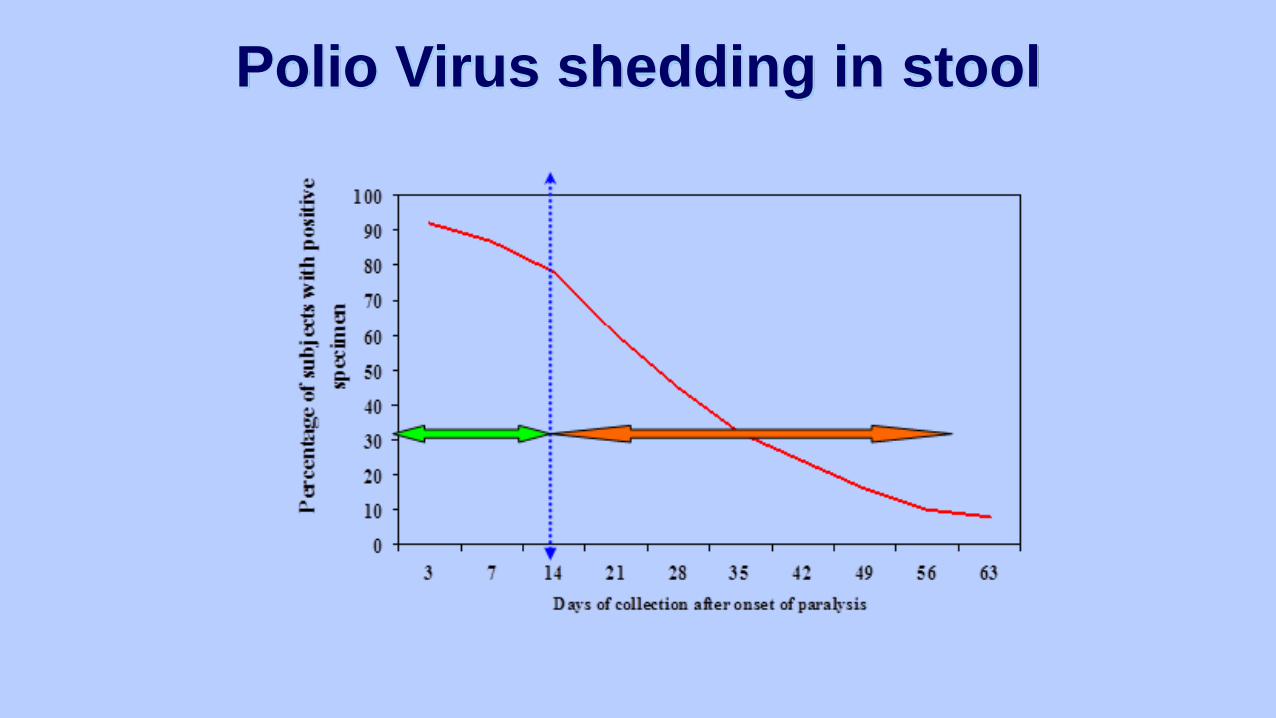
Polio Virus shedding in stool
Poliomyelitis :Clinical Manifestations
• Other causes of Acute Flaccid Paralysis:
• GBS
• Other Entero-viruses, Coxsackie & Echo viruses
• Others illnesses that affect the nervous system (including toxins
Most of infections are in-apparent (Reservoir of infection
especially in children)
Not A Specific Disease, Not Polio,
But A SYNDROME
Acute Flaccid Paralysis Surveillance
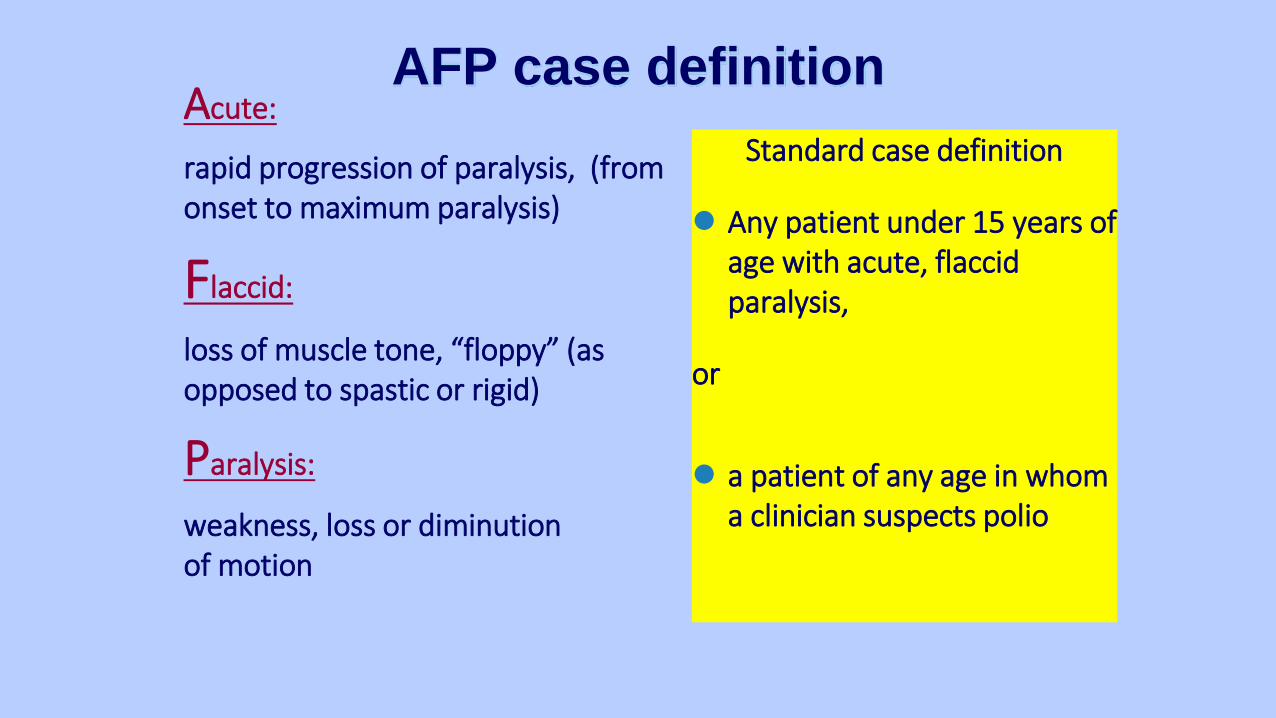
Acute:
rapid progression of paralysis, (from onset to maximum paralysis)
Flaccid:
loss of muscle tone, “floppy” (as opposed to spastic or rigid)
Paralysis:
weakness, loss or diminutionof motion
Standard case definition
Any patient under 15 years of age with acute, flaccid paralysis,
or
a patient of any age in whom a clinician suspects polio
AFP case definition
AFP surveillance steps
Collect 2 stool specimens 24 to 48 hrs apart, within
14 days of onset of paralysis
Put and seal in appropriate container
Ship to NICD in reverse cold chain, arrive < 72 hrs.
Copy of Case Investigation Form goes with the
specimen
If not adequately investigated: clinical notes, other
diagnostic information/ results & 60 Day Follow Up
AFP Performance Indicators
1 % of all expected AFP monthly reports that were receivedTarget: 90%
2 Non-polio AFP rate in children < 15 years of ageTarget: 4 / 100 000
3 Investigation ≤ 48 hours of report Target: ≥ 80%
4 2 stools collected at least 24 – 48 hours apart & within 14 days of paralysis onset – Target: ≥ 80%
5 Stool specimens arriving at the lab < 3 days of being sentTarget: ≥ 80%
6 Stool specimens arriving at the laboratory in "good condition"Target: ≥ 80%
AFP Stool Adequacy Rate
This is the second most important indicator for assessing the performance of AFP surveillance
A sensitive AFP surveillance system MUST be Capable of collecting 2 stool specimens within 14 days of onset of
paralysis 24 to 48 hours apart From at least 80% of all reported AFP cases.
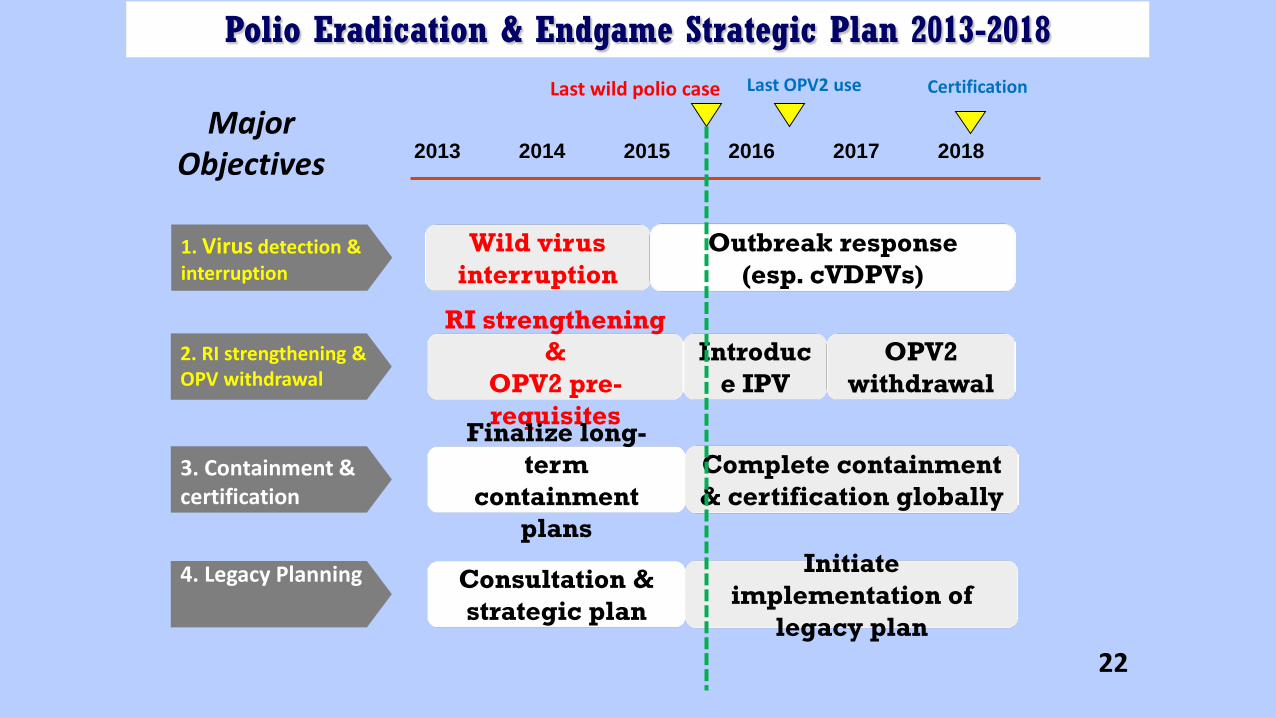
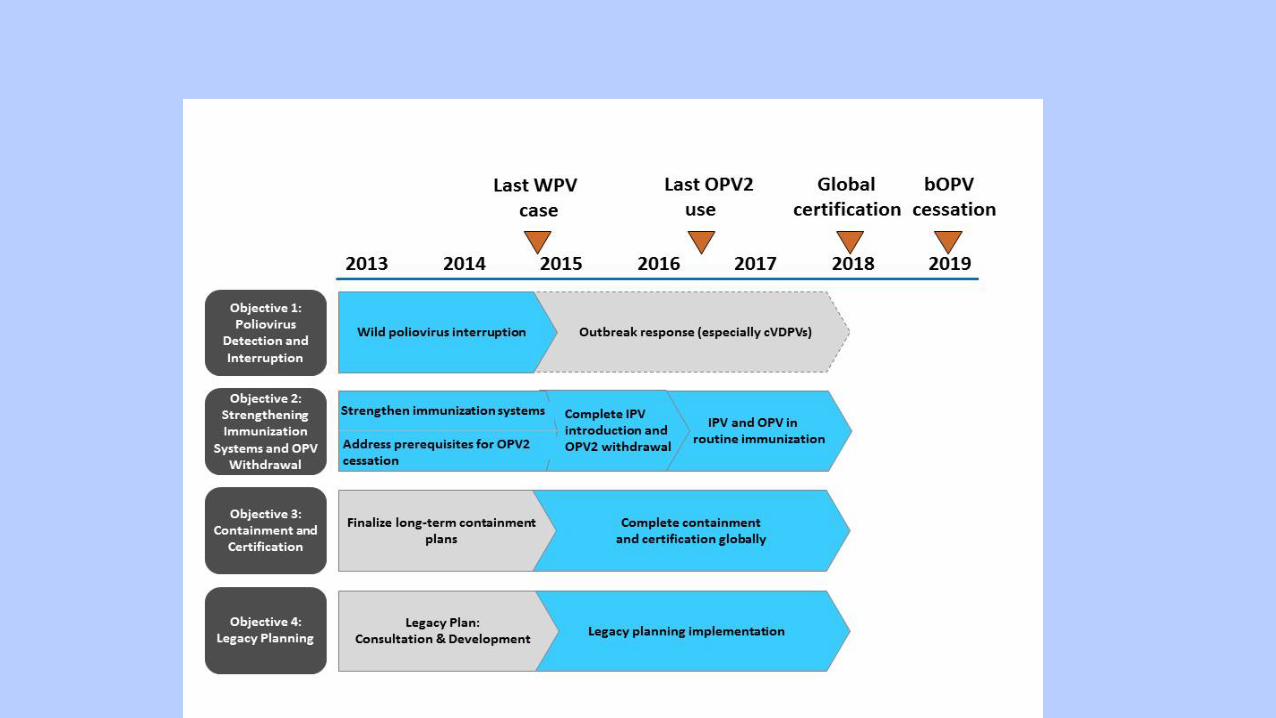
2013 2014 2015 2016 2017 2018
1. Virus detection & interruption
Last wild polio case Certification
2. RI strengthening & OPV withdrawal
3. Containment & certification
Introduce IPV
Wild virus interruption
Outbreak response (esp. cVDPVs)
RI strengthening &
OPV2 pre-requisites
OPV2withdrawal
4. Legacy Planning
Finalize long-term
containment plans
Complete containment & certification globally
Consultation & strategic plan
Initiate implementation of
legacy plan
Last OPV2 use
Major Objectives
Polio Eradication & Endgame Strategic Plan 2013-2018
22
Within 3 months of the switch, each country is required to have in place full containment of all wild type 2 as well as Sabin type 2 containing material, and any material which may be potentially infectious but not yet tested for wild or Sabin polio virus type 2 .
Global Action Plan for Polio containment
http://www.polioeradication.org/Portals/0/Document/Resources/PostEradication/GAPIII_2014.pdf
23
What samples need to be destroyed• Samples that have been confirmed as containing wild-type polioviruses
• Samples that have been confirmed as containing VDPV type 2 viruses
• Samples that have been confirmed as containing Sabin (Vaccine) strain of poliovirus type 2
24
What samples need to be destroyed
• Samples that may potentially contain wild type polio viruses, VDPV2 or Sabin 2 virus (even if they have not been tested for polio viruses)
• stool samples• rectal swabs• environmental samples• Respiratory samples (throat swabs)• Polio permissive cells or animals that have had virus introduced to
them• RNA and cDNA that may contain full genome or capsid sequences
In the near future type 1 and type 3 viruses of the mentioned strains will need to be destroyed as well25
Destruction of infectious materials• Polioviruses
• small non-enveloped viruses (hardy)• Destroyed by prolonged exposure to bleach, or elevated
temperatures above 56°C
26
Destruction of infectious materials – before April 2016
• Samples should be inventoried
• Any samples containing or potentially containing wild type viruses or VDPVs – needs to be autoclaved, autoclaved remains tracked and placed into a biohazardous container, incinerated as for destruction of biohazardous materials (usually controlled by a private 3rd party company), data trail of the destruction procedure should be kept on hand as proof of destruction
• Any samples containing or potentially containing Sabin type 2 polio virus – needs to be discarded as per biological waste (red bin, collected and incinerated by 3rd party company)
27
Destruction of infectious materials – After July 2016
• Samples should be inventoried
• Any samples containing or potentially containing wild type viruses or VDPVs or Sabin type 2 virus – needs to be autoclaved, autoclaved remains tracked and placed into a biohazardous container, incinerated as for destruction of biohazardous materials (usually controlled by a private 3rd party company), data trail of the destruction procedure should be kept on hand as proof of destruction
28
If samples cannot be destroyed• Research projects still ongoing may require samples that may contain
polio
• The laboratory will need to comply with the requirements set in the Global Action Plan (3rd edition) http://www.polioeradication.org/Portals/0/Document/Resources/PostEradication/GAPIII_2014.pdf
• Otherwise laboratories will need to be in contact with the WHO & NICD to discuss suitable storage until the completion of the project, at which time the samples will need to be destroyed
29
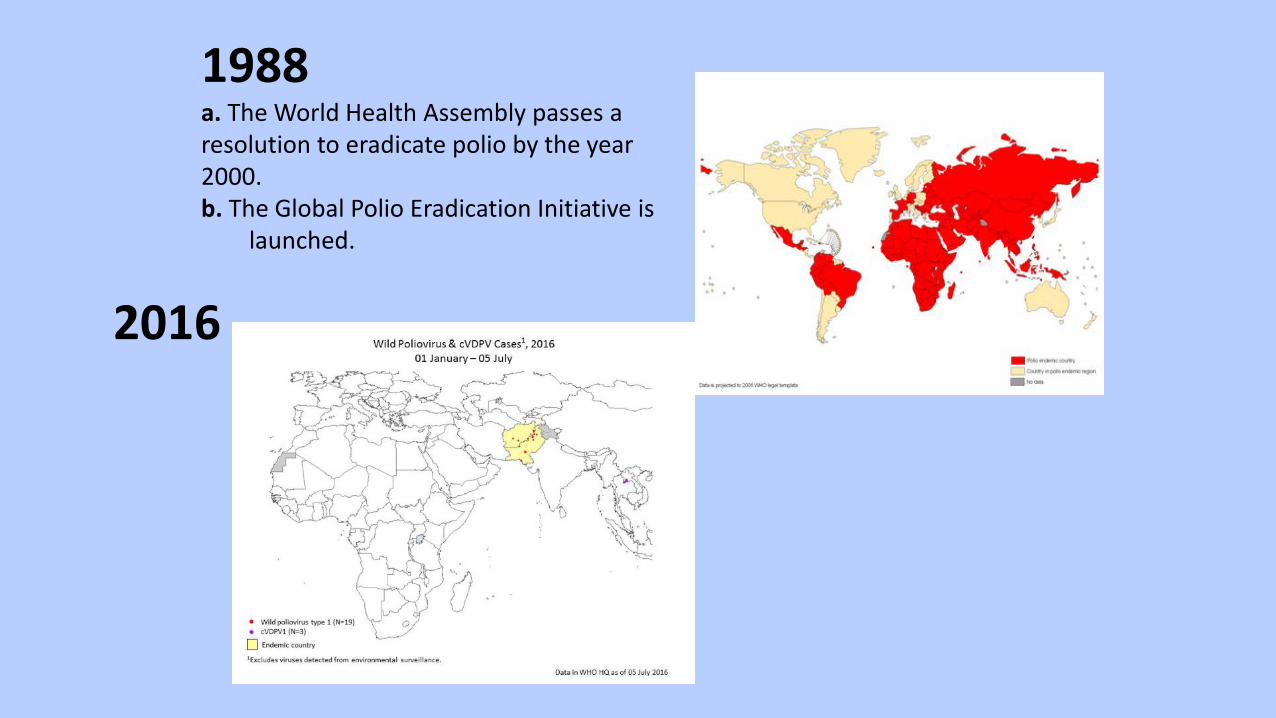
1988a. The World Health Assembly passes a resolution to eradicate polio by the year 2000.b. The Global Polio Eradication Initiative is
launched.
2016

1991Luis Fermin Tenorio, a 3 years old boy living in Junin, Northern Peru was the last case of wild polio in the WHO Region of the Americas
1994The WHO Region of the Americas was certified polio-free
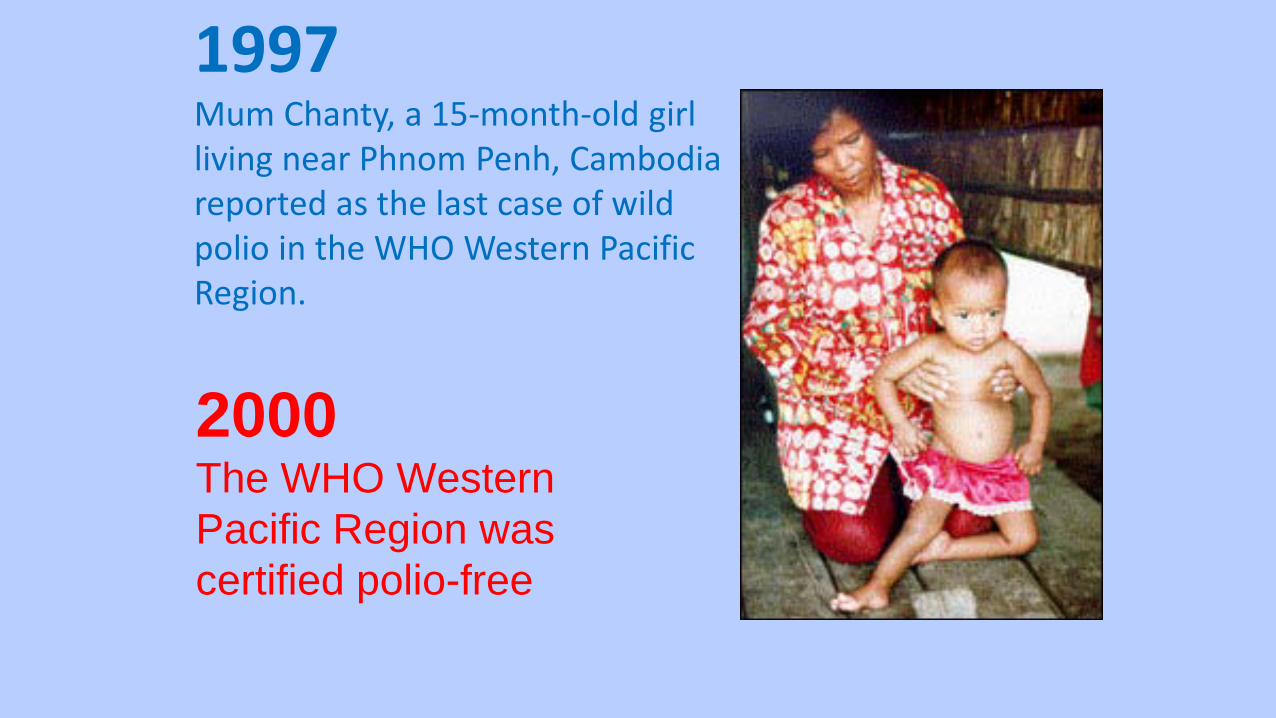
1997Mum Chanty, a 15-month-old girl living near Phnom Penh, Cambodia reported as the last case of wild polio in the WHO Western Pacific Region.
2000The WHO Western Pacific Region was certified polio-free

1998In Turkey on 26 November, 1998, Melik Minas, a 33-month-old unvaccinated child, is the last child paralysed by indigenous wild poliovirus in the European Region.
2002The WHO European Region was certified polio-free

Towards a polio-free India2011Rukhsar Khatun, a 18 months old girl from West Bengal of India, remains the last polio crippled child in the South East Asia Region
2014The WHO South East Asia Region was certified polio-free
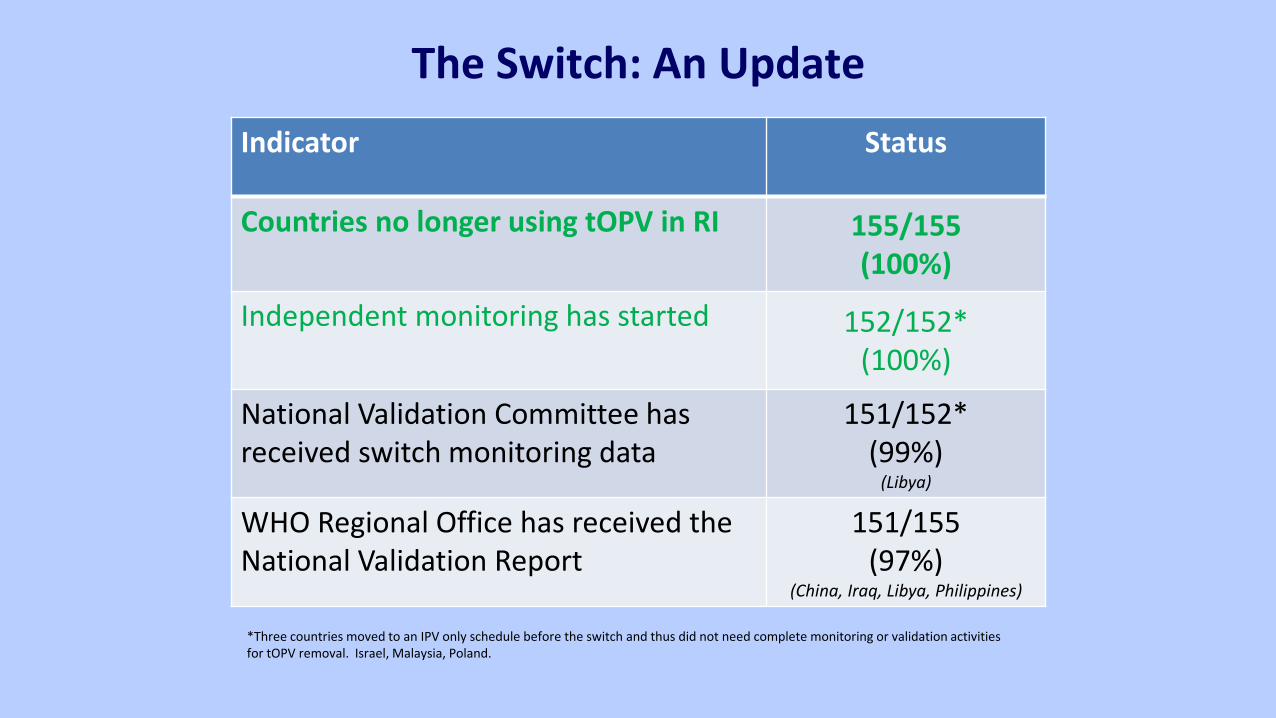
Indicator Status
Countries no longer using tOPV in RI 155/155 (100%)
Independent monitoring has started 152/152* (100%)
National Validation Committee has received switch monitoring data
151/152*(99%)
(Libya)
WHO Regional Office has received the National Validation Report
151/155(97%)
(China, Iraq, Libya, Philippines)
*Three countries moved to an IPV only schedule before the switch and thus did not need complete monitoring or validation activities for tOPV removal. Israel, Malaysia, Poland.
The Switch: An Update
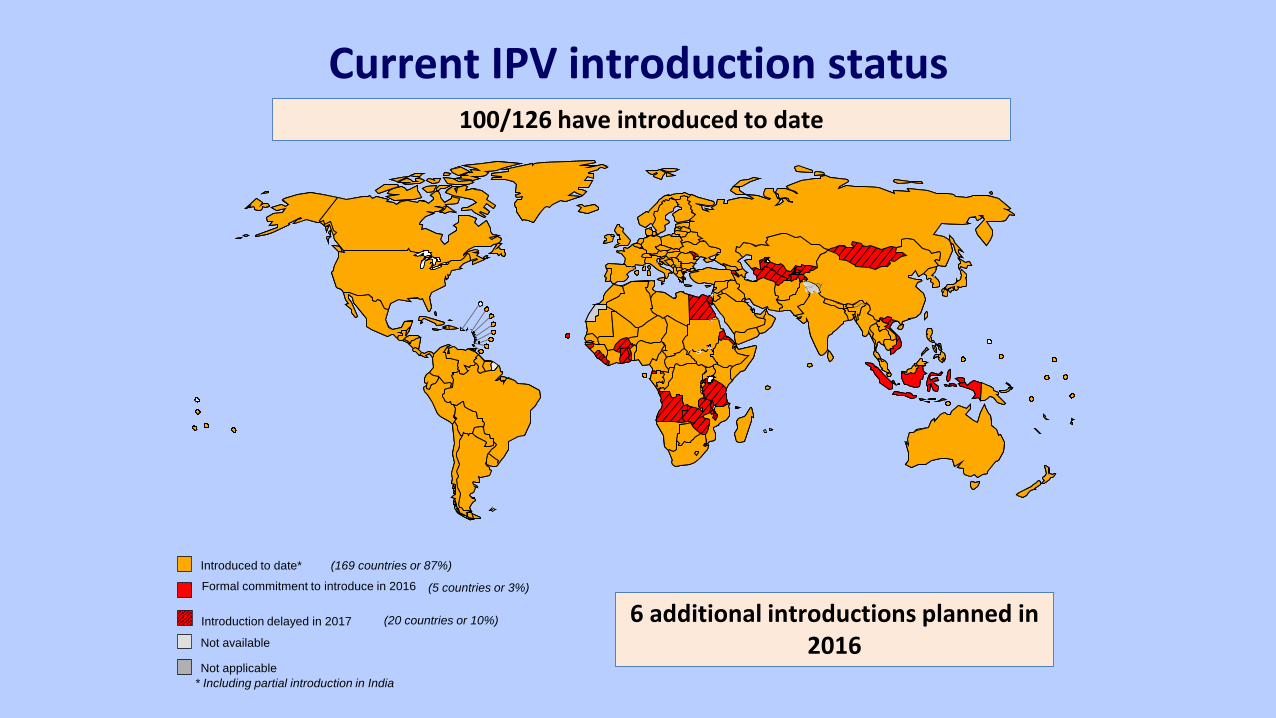
Current IPV introduction status100/126 have introduced to date
(5 countries or 3%)
Introduced to date* (169 countries or 87%)
(20 countries or 10%)
Not available
Not applicable
Introduction delayed in 2017
Formal commitment to introduce in 2016
* Including partial introduction in India
6 additional introductions planned in 2016
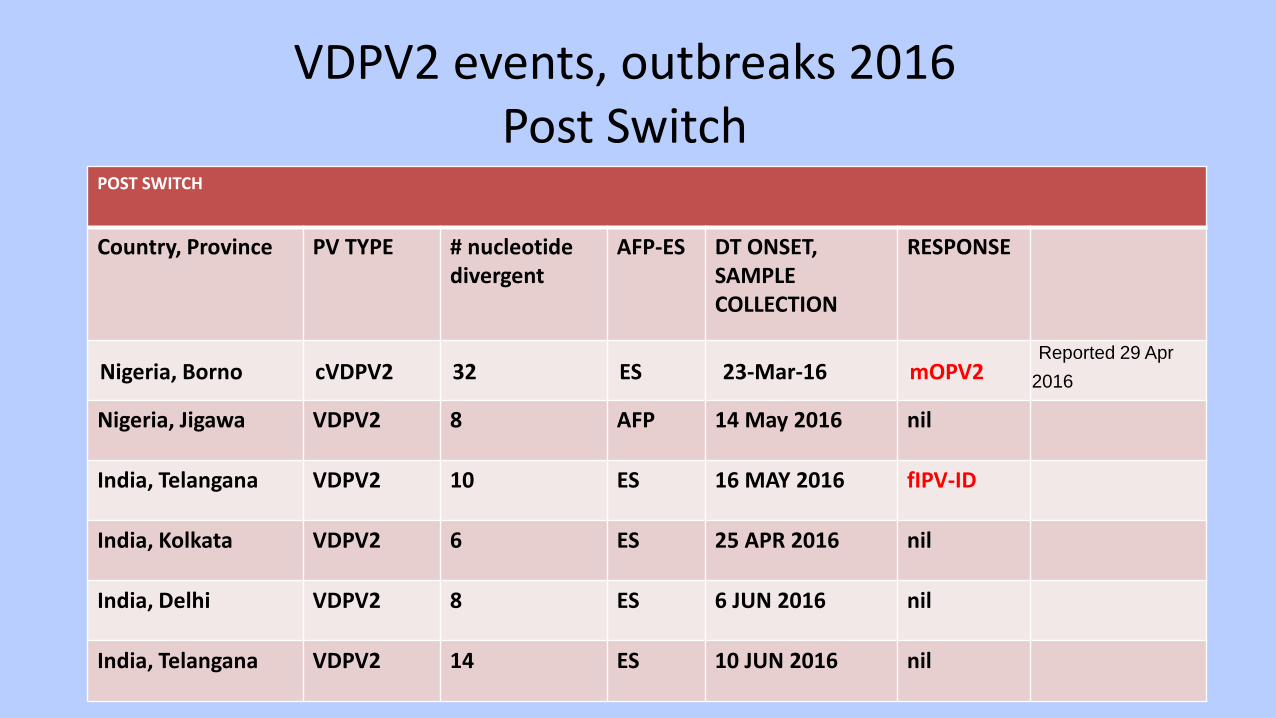
VDPV2 events, outbreaks 2016Post Switch
POST SWITCH
Country, Province PV TYPE # nucleotide divergent
AFP-ES DT ONSET, SAMPLE COLLECTION
RESPONSE
Nigeria, Borno cVDPV2 32 ES 23-Mar-16 mOPV2Reported 29 Apr
2016
Nigeria, Jigawa VDPV2 8 AFP 14 May 2016 nil
India, Telangana VDPV2 10 ES 16 MAY 2016 fIPV-ID
India, Kolkata VDPV2 6 ES 25 APR 2016 nil
India, Delhi VDPV2 8 ES 6 JUN 2016 nil
India, Telangana VDPV2 14 ES 10 JUN 2016 nil
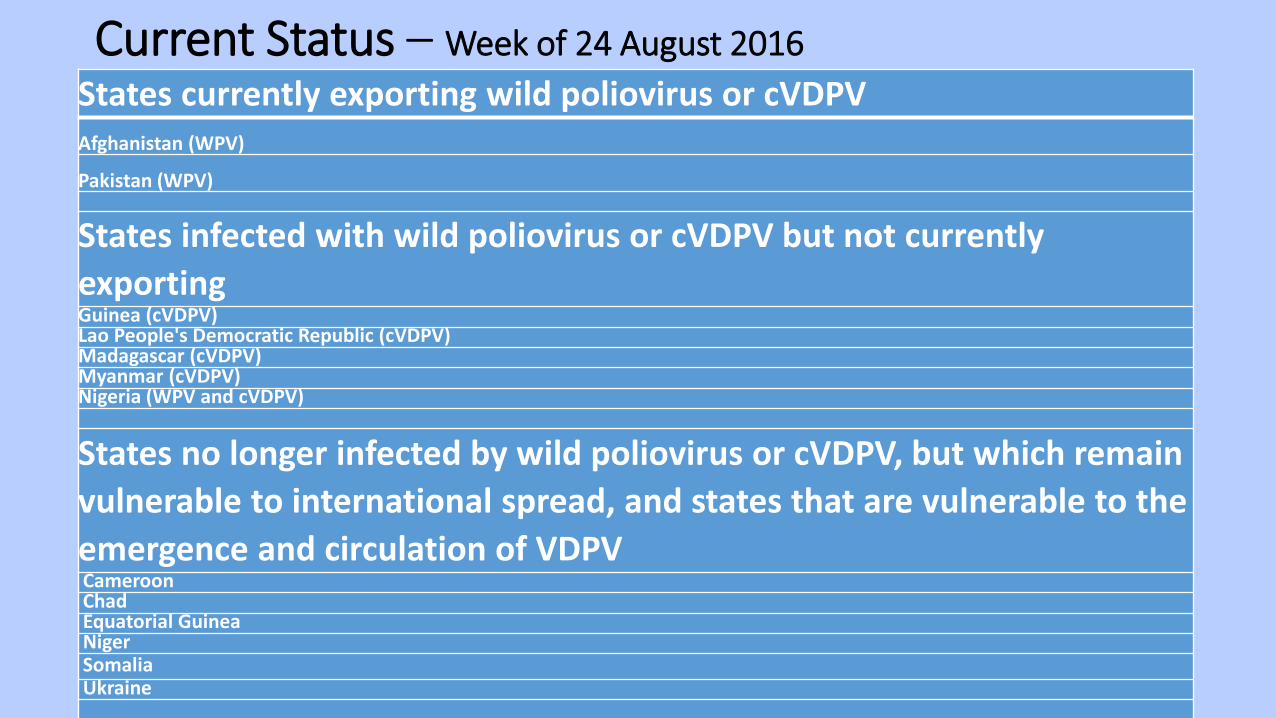
Current Status – Week of 24 August 2016States currently exporting wild poliovirus or cVDPVAfghanistan (WPV)
Pakistan (WPV)
States infected with wild poliovirus or cVDPV but not currently exportingGuinea (cVDPV)Lao People's Democratic Republic (cVDPV)Madagascar (cVDPV)Myanmar (cVDPV)Nigeria (WPV and cVDPV)
States no longer infected by wild poliovirus or cVDPV, but which remain vulnerable to international spread, and states that are vulnerable to the emergence and circulation of VDPVCameroonChadEquatorial GuineaNigerSomaliaUkraine
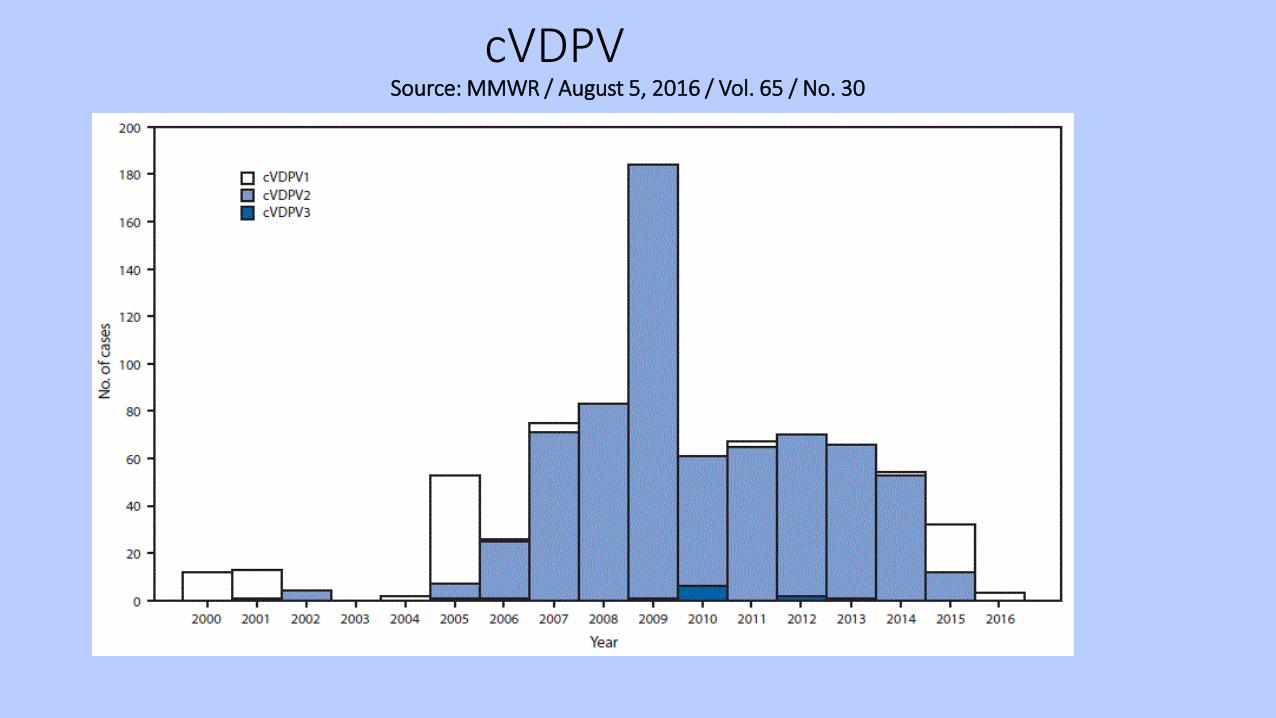
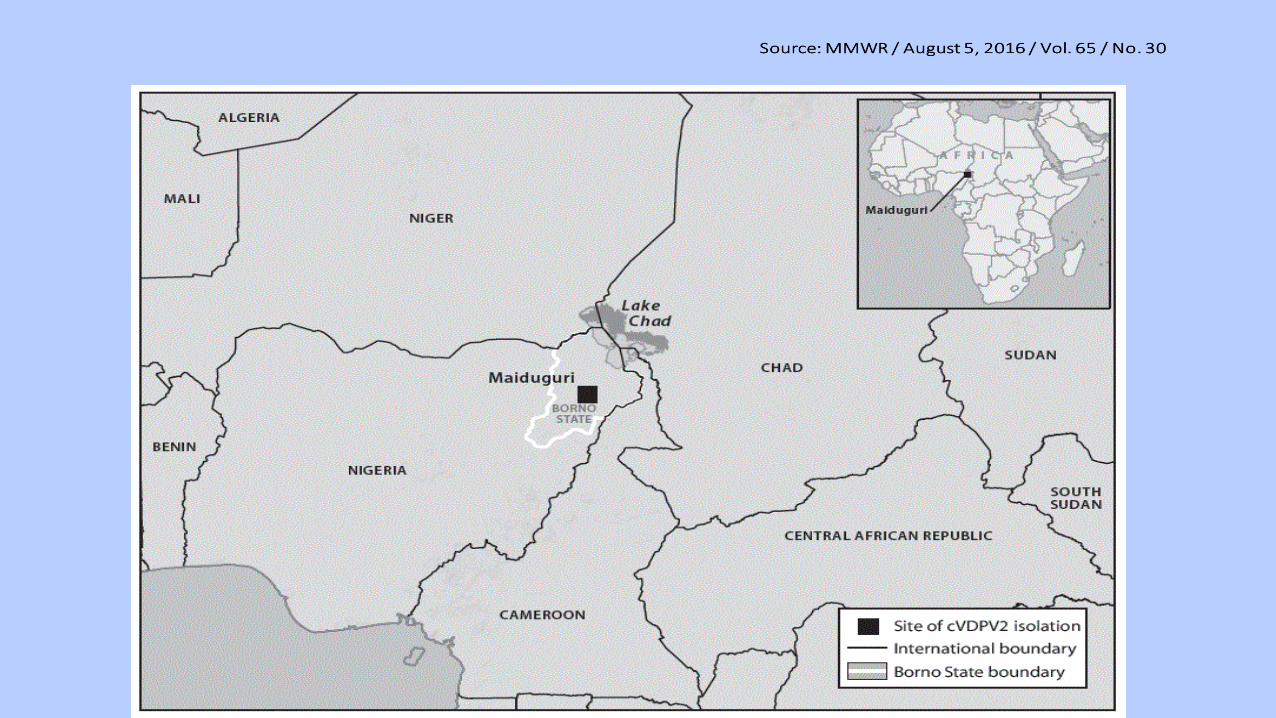
cVDPVSource: MMWR / August 5, 2016 / Vol. 65 / No. 30
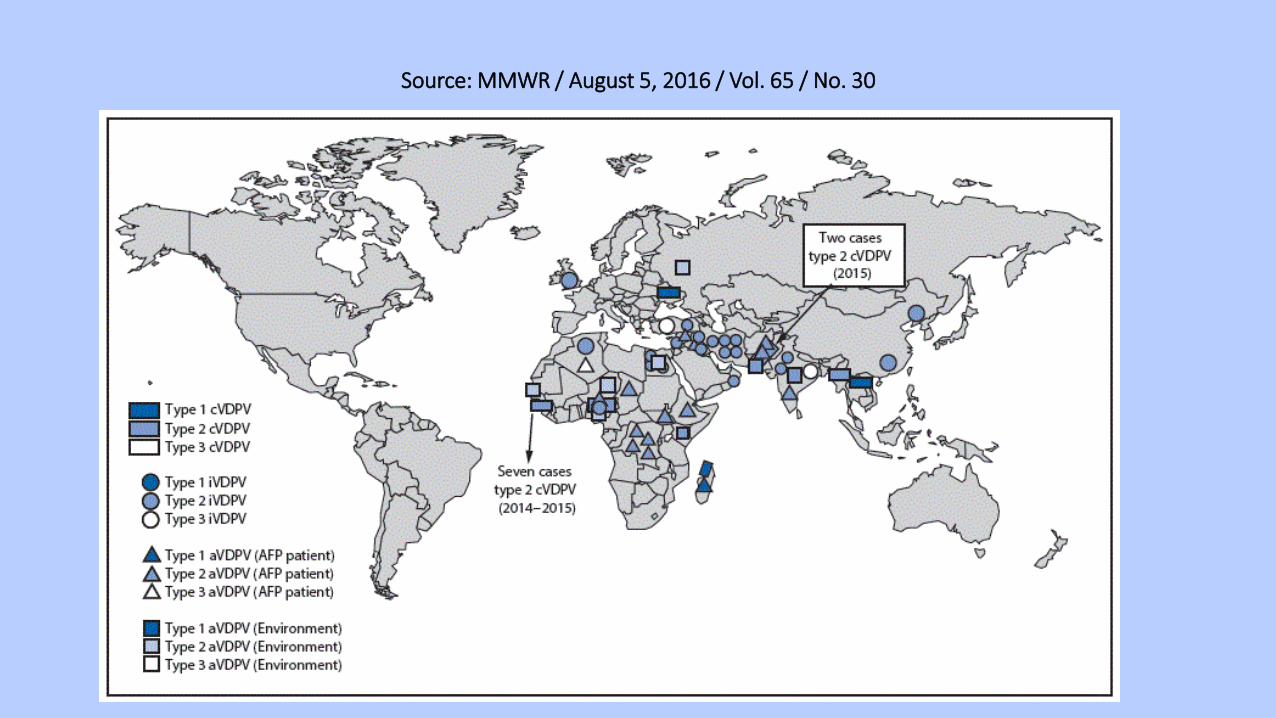
Source: MMWR / August 5, 2016 / Vol. 65 / No. 30
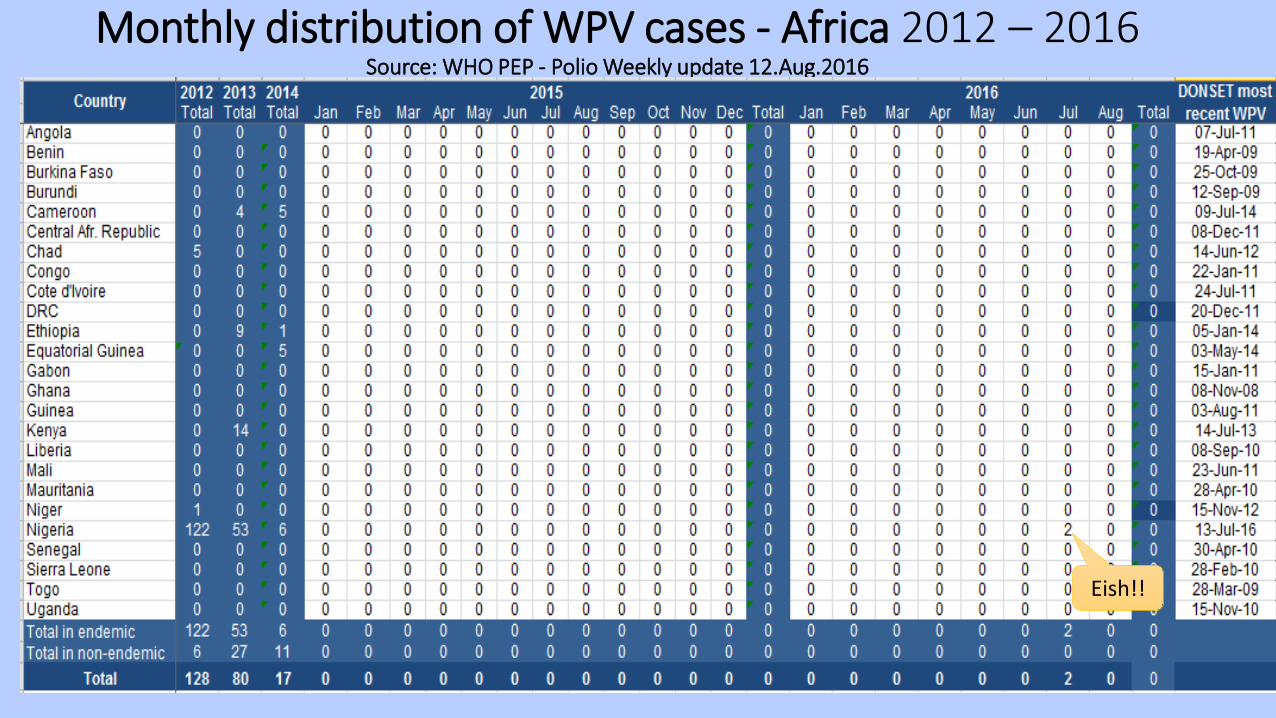
Monthly distribution of WPV cases - Africa 2012 – 2016Source: WHO PEP - Polio Weekly update 12.Aug.2016
Eish!!
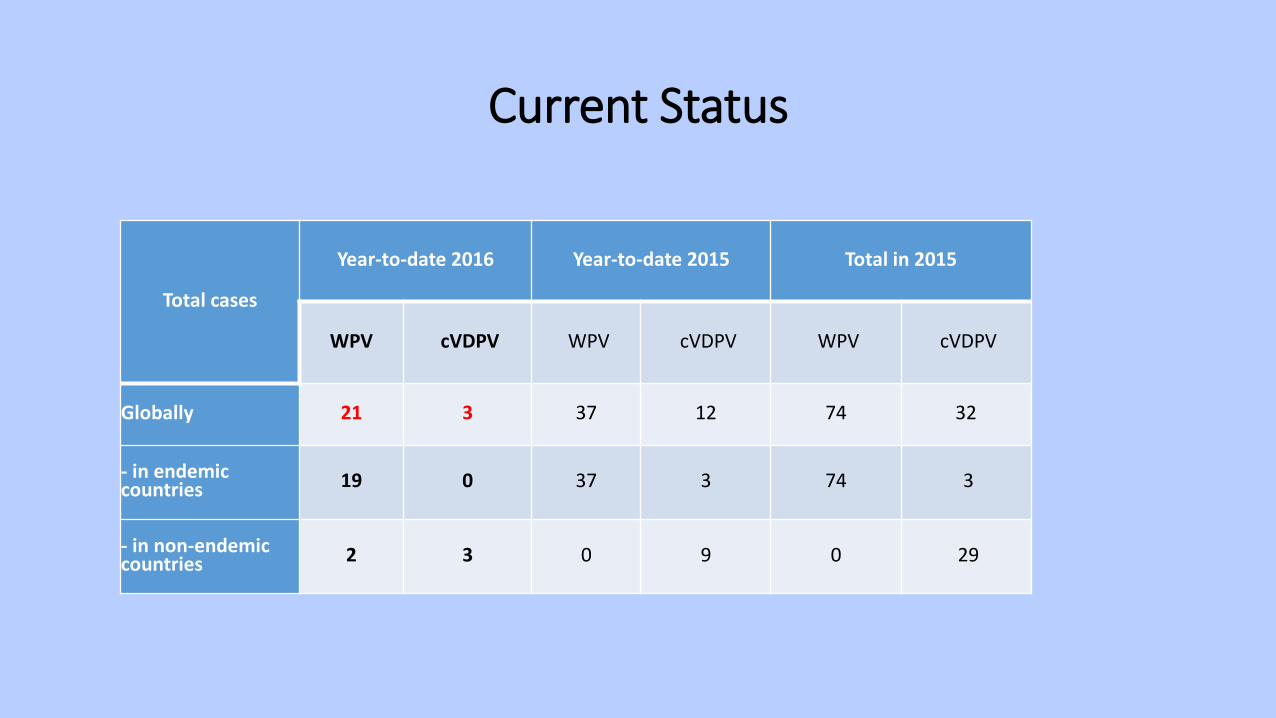
Current Status
Total cases
Year-to-date 2016 Year-to-date 2015 Total in 2015
WPV cVDPV WPV cVDPV WPV cVDPV
Globally 21 3 37 12 74 32
- in endemic countries 19 0 37 3 74 3
- in non-endemic countries 2 3 0 9 0 29
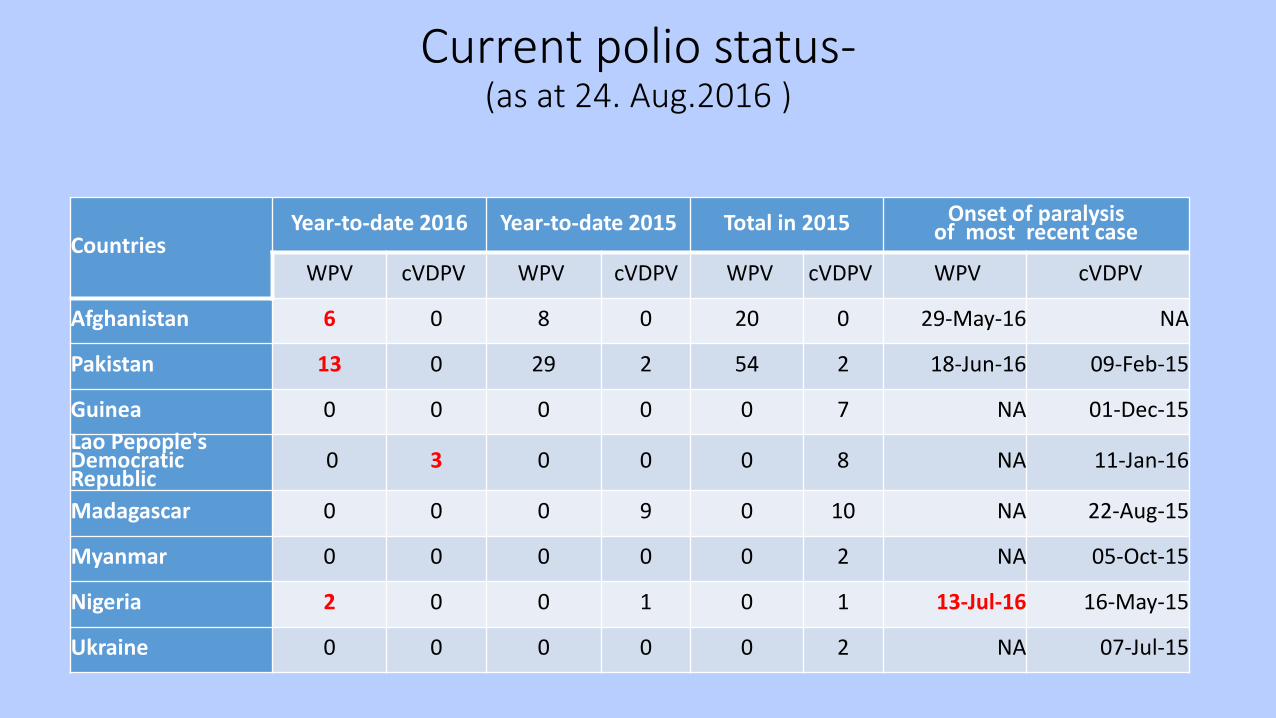
Current polio status-(as at 24. Aug.2016 )
CountriesYear-to-date 2016 Year-to-date 2015 Total in 2015 Onset of paralysis
of most recent case
WPV cVDPV WPV cVDPV WPV cVDPV WPV cVDPV
Afghanistan 6 0 8 0 20 0 29-May-16 NA
Pakistan 13 0 29 2 54 2 18-Jun-16 09-Feb-15
Guinea 0 0 0 0 0 7 NA 01-Dec-15Lao Pepople's Democratic Republic
0 3 0 0 0 8 NA 11-Jan-16
Madagascar 0 0 0 9 0 10 NA 22-Aug-15
Myanmar 0 0 0 0 0 2 NA 05-Oct-15
Nigeria 2 0 0 1 0 1 13-Jul-16 16-May-15
Ukraine 0 0 0 0 0 2 NA 07-Jul-15

Source: MMWR / August 5, 2016 / Vol. 65 / No. 30
2 new WPV cases from Nigeria
• Two new WPV type 1 cases were reported
• WPV type1 from Borno State in: – Jere LGA from a contact (onset of paralysis of index case: 4 July 2016)
(the index case had a negative test result)
– Gwoza LGA (onset of paralysis: 13 July 2016)
2 new WPV cases in Nigeria- 1st Case reported on 4th July 2016 -
• Genetic sequencing suggests these isolates are most closely linked to WPV1 last detected in Borno in 2011.
• Genetic analysis can therefore be interpreted to mean that the virus detected had circulated undetected for several years
• These isolates are the first WPV1s detected in Nigeria since July 2014
• Significant surveillance gaps and area generally inaccessible
2 new WPV cases from NigeriaWhat are the implications for countries?
• Until global polio eradication is achieved, there is a risk that any country can be affected by those countries with continued polio transmission.
• Important that countries remain vigilant by strengthening AFP surveillance
• Important that routine immunization activities be strengthened to ensure adequate population immunity.
WHO – ARCC’s RESPONSE
The World Health Organization Regional Committee for the African Region met on the 21 August and declared the recent polio outbreak a public health emergency for the countries of the Lake Chad Basin, calling for a coordinated outbreak response across the region.
2 new WPV cases from NigeriaWhat is Nigeria doing now?
• Conducting several rounds of outbreak response activities / campaigns that will be synchronized with neighbouringcountries in the Lake Chad Basin that have been affected by insecurity and inaccessibility: Chad, Cameroun, Niger and Central African Republic.
• Additionally, surveillance is being further strengthened in these countries to avoid missing any circulation.
2 new WPV cases from NigeriaWhat are the implications for the AFRO regions?
• Since a WHO region needs to be polio free for at least 3 years, to be certified to have eradicated polio, with the new cases, the earliest the region can be certified is 2019.
• It’s Important that all countries maintain high immunization coverage especially in the hard-to-reach sub-populations populations.– Through strengthened routine immunization activities– Hightened Supplementary Immunization Activities (SIA)
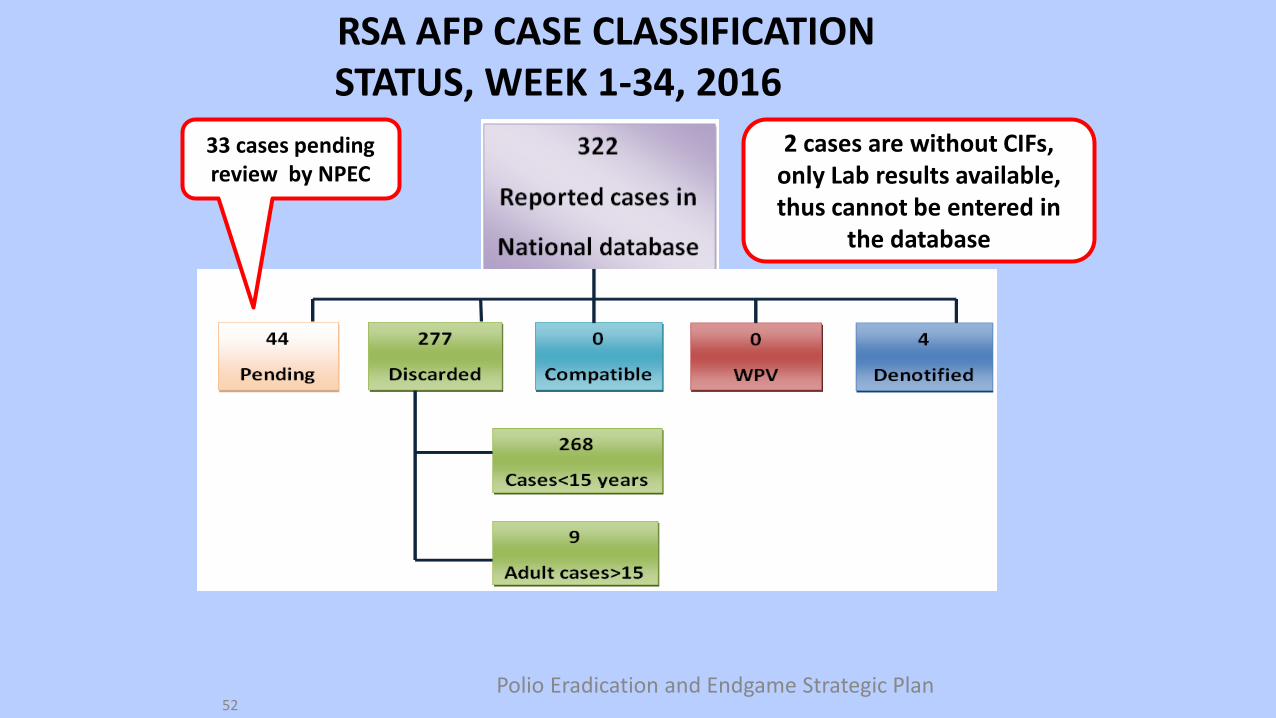
RSA AFP CASE CLASSIFICATION STATUS, WEEK 1-34, 2016
Polio Eradication and Endgame Strategic Plan52
2 cases are without CIFs, only Lab results available, thus cannot be entered in
the database
33 cases pending review by NPEC
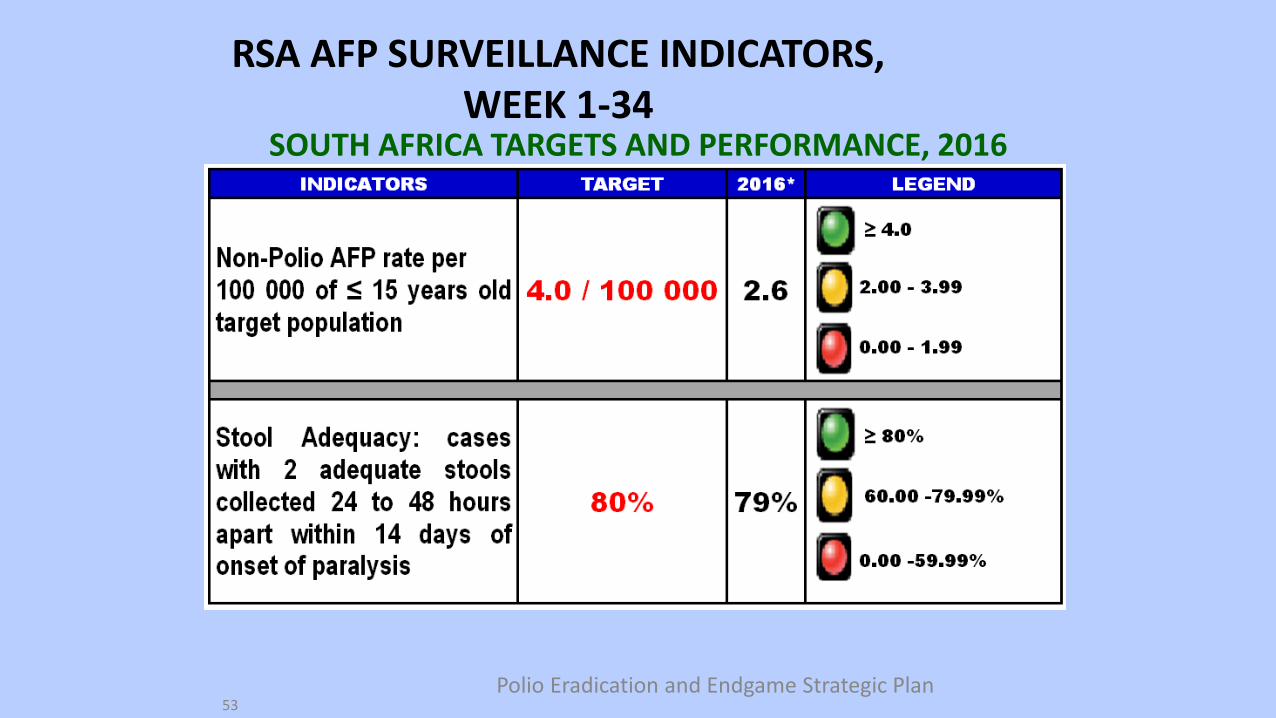
RSA AFP SURVEILLANCE INDICATORS, WEEK 1-34
Polio Eradication and Endgame Strategic Plan53
SOUTH AFRICA TARGETS AND PERFORMANCE, 2016
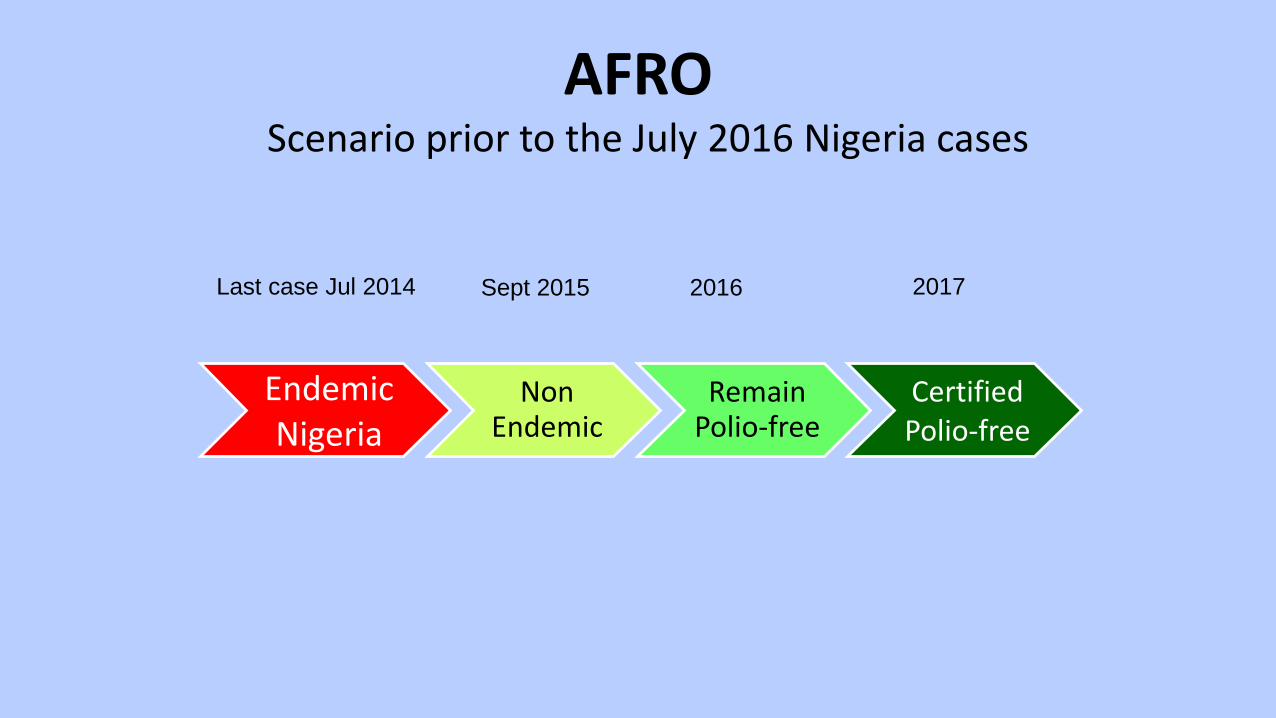
AFRO Scenario prior to the July 2016 Nigeria cases
EndemicNigeria
Non Endemic
Remain Polio-free
Certified Polio-free
Sept 2015 2016 2017Last case Jul 2014
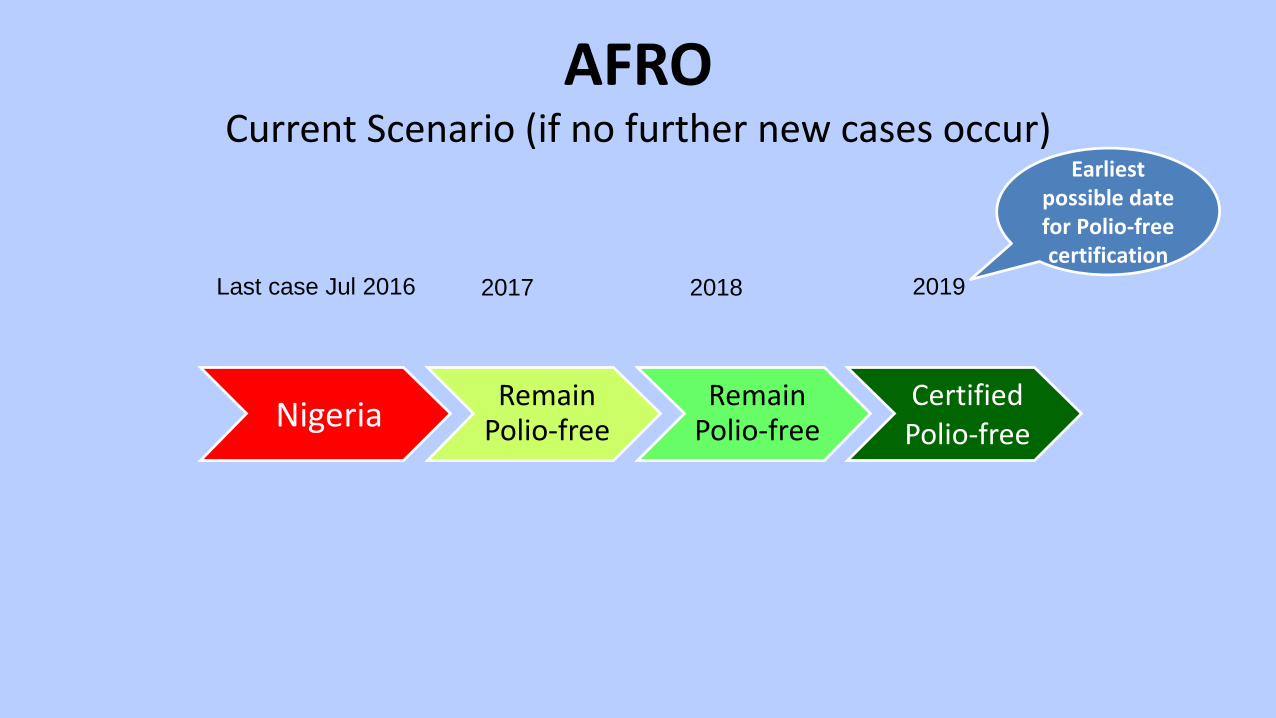
AFRO Current Scenario (if no further new cases occur)
Nigeria Remain Polio-free
Remain Polio-free
Certified Polio-free
2017 2018 2019Last case Jul 2016
Earliest possible date for Polio-free certification

Mitigation of Risks
International importation
Gaps in AFP surveillance or
delays in detection of WPV
Delayed and/or inadequate response
to importation
Areas with low population immunity
Emergence of VDPVs
Complacency/ Lack of focus
Current priorities for polio eradication
1. Maintaining high population immunity through polio vaccination campaigns and RI coverage
2. Sustaining sensitive surveillance for detection of poliovirus
3. Mitigating risk of importation – cross border vaccination/vaccination of international travellers
4. Emergency preparedness & response planning
5. Polio end game strategy
THANK YOU