placental abruption liu wei department of ob & gy ren ji hospital
TRANSCRIPT

Placental Abruption
Liu Wei
Department of Ob & Gy
Ren Ji hospital
General Consideration• Definition The separation of the placenta from its site of
implantation after 20 weeks of gestation or during the course of delivery.
• Frequency 0.51%-2.33% (our country) 1% (other countries) • Incidence of fetal death 200‰-350‰

Etiology• Uncertain (primary cause)• Risk factors1. Increased age and parity2. Vascular diseases: preeclampsia, chronic
hypertension, renal disease.3. Mechanical factors: trauma, intercourse,
polyhydramnios, 4. Supine hypotensive syndrome5. Smoking, cocaine use, uterine myoma

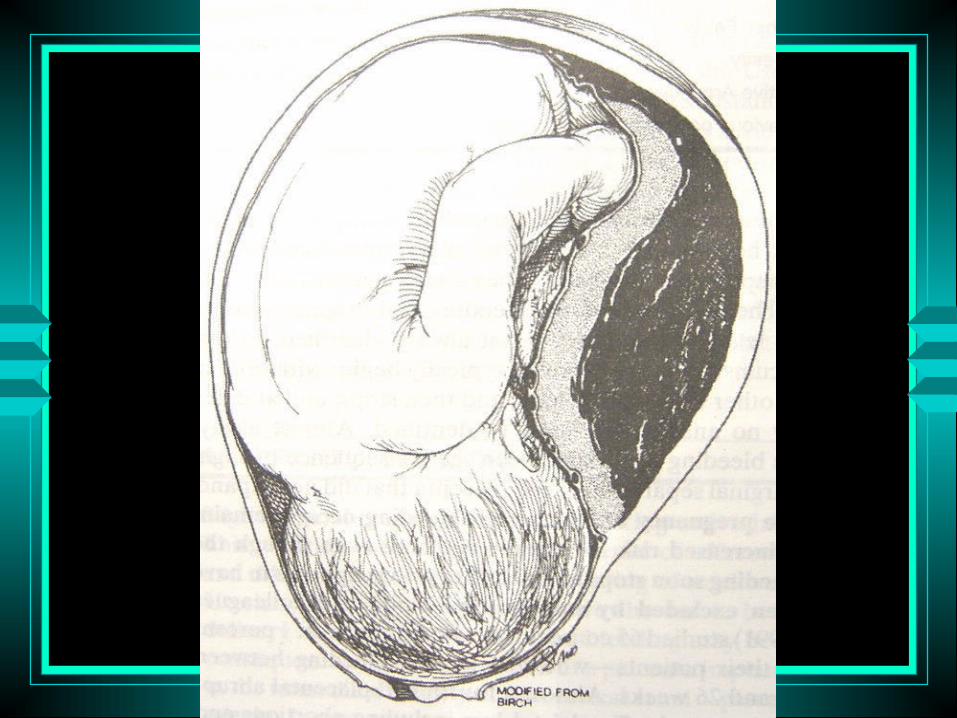
Pathology• Main change hemorrhage into the decidua basalis → decidua
splits → decidural hematoma → separation, compression, destruction of the placenta adjacent to it
• Types revealed abruption, concealed abruption,
mixed type• Uteroplacental apoplexy 子宫胎盘卒中

Pathology

Manifestation• Vaginal bleeding companied with abdominal
pain• Mild type abruption≤ 1/3, apparent vaginal bleeding• Severe type abruption > 1/3, large retroplacental hematoma,
vaginal bleeding companied by persistent abdominal pain, tenderness on the uterus, change of fetal heart rate. shock and renal failure.

Adjunctive Examination• Ultrasonography1. Position of placenta, severity of abruption,
survival of fetus2. Signs: retroplacental hematoma3. Negative findings do not exclude placental
abruption• Laboratory examination1. consumptive coagulopathy: Rt, DIC2. Function of liver and kidney.

Diagnosis• sign and symptom
1. Vaginal bleeding
2. Uterine tenderness or back pain
3. Fetal distress
4. High frequency contractions
5. Hypertonus
6. Idiopathic preterm labor
7. Dead fetus
Diagnosis• Ultrasonography• Differential diagnosis
1. Placenta previa
Painless bleeding
2. Pre-rupture of uterus
dystocia
Complication• DIC• Hypovolemic shock• Amnionic fluid embolism• Acute renal failure
Treatment• Treatment will vary depending upon
gestational age and the status of mother and fetus
• Treatment of hypovolemic shock: intensive transfusion with blood
• Assessment of fetus• Termination of pregnancy: CS or Vaginal
delivery

Treatment• Treatment of consumptive coagulopathy
1. Supplement of coagulation factors: fresh blood, frozen blood plasma, fibrinogen, blood platelet.
2. Heparin: high coagulation
3. Anti-fibrinolysis• Prevention of renal failure

END