physician assistant reimbursement: hot topicsc.ymcdn.com/sites/ · physician assistant...
TRANSCRIPT

Physician Assistant
Reimbursement: Hot Topics

2

Physician Assistant
reimbursement: Hot Topics
James A. Kilmark, PA-C• Physician Assistant in Emergency Medicine
• Emergency Physicians Medical Group: PA/NP Collaborative Team
• Co-Lead PA – St. Joseph Mercy Hospital Emergency Department, Ann Arbor MI
• Past President – Michigan Academy of Physician Assistants
• Michigan Academy of Physician Assistants Chairperson – Reimbursement Committee
• Governor Appointed Member – Michigan Board of Osteopathic Medicine and Surgery
Disclaimer: This Presentation is provided for informational purposes only and does not constitute legal or payment advice. The ultimate responsibility for statutory and regulatory compliance, as well as the proper submission of claims, rests entirely upon the provider of services.
3

Learning Objectives
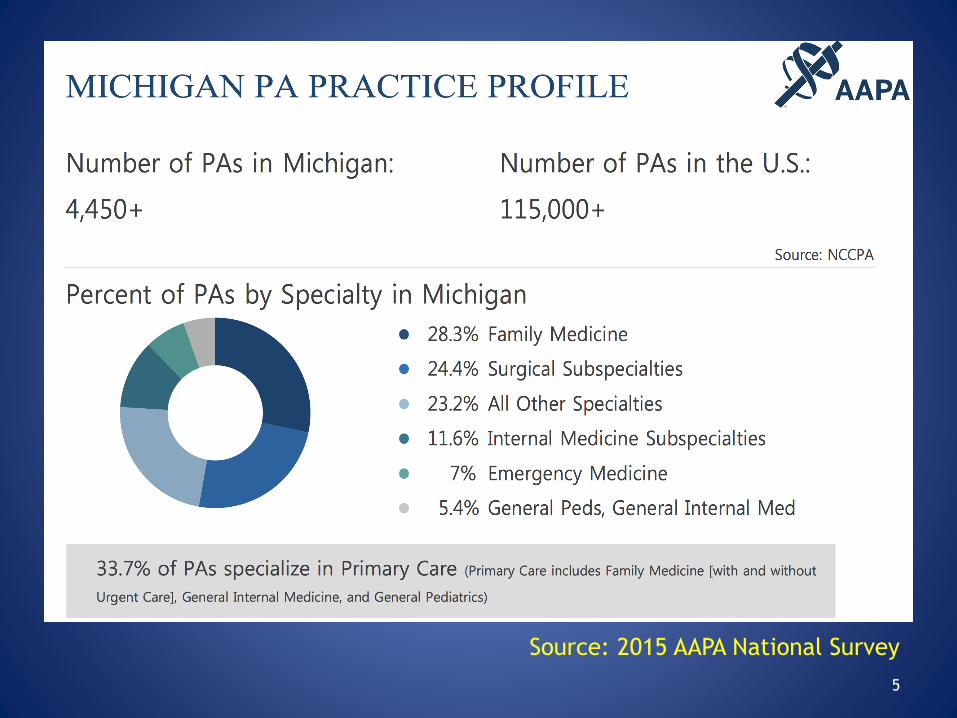
• Statistics – Michigan PAs
• Review of Michigan Law regarding PA scope of practice– Public Act 379
• Blue Cross Blue Shield of Michigan and BCN– August 2017 The Record credentialing /
recredentialing
– MAPA Meeting with BCBSM / BCN officials Oct 2017
– BCN Refusal of payment for PA services as a primary care provider?
• Refusal of payment for services provided by a Physician Assistant
• CMS Appeal process for denial of claims4
5
Source: 2015 AAPA National Survey

6
Source: 2015 AAPA National Survey

7
Source: 2017 AAPA Salary Report
Data collected Feb-March 2017
N=302 (Michigan)

Scope of Practice for PAs &
Physician / PA relationship in practice
The boundaries of a PAs scope of practice are
determined by four parameters:
1. Historically - ***Delegation by a Supervising
Physician (and the physicians scope of
practice)***well…..sort of……ENTER Legislation
Public Act 379 ***
2. PAs Education and Experience
3. State Law
4. Facility Policy
8

Michigan Public Health Code
“Practice as a Physician Assistant” means the practice of medicine, osteopathic medicine and surgery, and podiatric medicine and surgery and is defined as a health profession subfield (MCL 333.17001, 333.17008).
"Practice of medicine" means the diagnosis, treatment, prevention, cure, or relieving of a human disease, ailment, defect, complaint, or other physical or mental condition, by attendance, advice, device, diagnostic test, or other means, or offering, undertaking, attempting to do, or holding oneself out as able to do, any of these acts (MCL333.17001).
9

PA Scope of Practice
Historically PAs practice medicine in MI under legislation that defined Physicians in a supervisory role.
The MI Public Health code also used terms related to Physicians delegating abilities to the PA
Public Act 379 – Enacted March 22nd 2017
• PAs now practice medicine as part of a practice agreement within a healthcare team
• PAs also have full prescribing rights including schedule 2-5 controlled substances without restriction as long as it is authorized within a defined practice agreement.
10
Public Act 379 Summary
• PAs will work within a Practice Agreement with a “participating physician”
• PAs will continue to practice medicine and remain a sub-field of Medicine, Osteopathic Medicine and Podiatry boards
• PAs will continue to be held to the standards of competency and training
• The terms “supervision” and “delegation“ were removed in law in favor of a practice agreement with a physician
• Removes arbitrary PA/physician ratios in the statute
• PAs are now fully independent prescribers
– MUST HAVE A DEA # AND MICHIGAN CONTROLLED SUBSTANCE LICENSE
• PAs will continue to practice with a participating physician as a member of a practice team
11

Public Act 379 Summary
What is a“participating physician”
“a physician designated by a group of
physicians under section 333.17049 to
represent that group, or a physician designated
by a health facility or agency under section
333.20174 to represent that health facility or
agency.”
12

Public Act 379 Summary
What is a Practice Agreement? • A Practice Agreement is a written agreement between
a PA and a participating physician.
• It generally defines the communication and decision making process by which the PA and the participating physician provide medical care to their patients.
• It may also place conditions on specific duties, procedures or drugs, if the parties of the agreement choose to do so.
• It is not intended to be a burdensome or lengthy document, but rather, provide a general understanding of each professional’s knowledge and skills utilized in each unique practice setting.
13

Public Act 379 SummaryWhat is required in a practice agreement?
a. A process between the physician assistant
and participating physician for communication, availability and decision
making when providing medical treatment to a patient. The process
must utilize the knowledge and skills of the physician assistant and
participating physician based on their education, training and
experience.
b. A protocol for designating an alternative physician for consultation in
situations in which the participating physician is not available for
consultation.
c. The signature of the physician assistant and the participating physician.
d. A termination provision that allows the physician assistant or
participating physician to terminate the practice agreement by providing
written notice at least 30 days before the date of termination.
Go to www.MichiganPA.org for a sample practice agreement and to learn
more about PA practice in MI14

Does the state of Michigan and the
Public act define what PAs Can’t do:
• PAs cannot perform refraction/optometry
• PAs cannot perform abortions or prescribe medications
or a device that will lead to miscarriage or fetal death
• PAs CAN “pronounce death” but Cannot sign a death
certificate
• PAs performing flex sig / colonoscopy in and outpatient
facility **does not pertain to hospital based
settings**Michigan Rule 325.3802 specifies that
endoscopic procedures performed in a surgical
outpatient facility are defined as "surgery" and can only
be performed by a "physician."
15

Blue Cross Blue Shield of Michigan and Blue Care
Network: What’s new? MAPA recently met with
officials

Blue Cross Blue Shield Of Michigan
• Register with BCBSM and obtain an individual PA PIN or add a PA to a group.
• Call BCBSM’s Provider Enrollment and Data Management department at 800-822-2761
• bcbsm.com/provider/enrollment*
http://www.bcbsm.com/providers/join-the-blues-network/enrollment.html
Blue Cross Blue Shield Of Michigan
a quick refresher
• Allows Direct or Indirect Billing for services provided by a PA
• **This is not CMS – ”incident to” or “shared service”**
• Direct Billing refers to the billing of services
under the provider identification number of the
PA practitioner who performed the service
Source: BCBSM The Record April 2008

Blue Cross Blue Shield Of Michigan
Direct Billing:
• If the PA provides any level of service that is provided without fulfilling one of the three “indirect billing” scenarios the bill is submitted using the PAs license number and 85% of the Physician’s Fee schedule will be paid to the practice.
• Bill services performed by the physician assistant by reporting the billing physician's or group's PIN in field 33b and the physician assistant's license number in field 24J on the CMS-1500.
Source: BCBSM The Record April 2008 - page 21

Blue Cross Blue Shield Of Michigan
• Indirect Billing describes billing for services rendered by the PA under the PIN of the supervising physician
Source: BCBSM The Record April 2008 - page 21
Blue Cross Blue Shield Of Michigan
“Indirect Criteria”
• Any service where the physician delivers any component of
the service
• Services for which the physician has provided specific clinical direction to the Non physician Practitioner prior to or during the service
• Services for which the PA has presented pertinent clinical
findings and obtained approval of evaluation and
management by the physician prior to the end of the day
following the service
Source: BCBSM The Record April 2008 - page 21

Blue Cross Blue Shield Of Michigan
• Report the PIN of the billing physician in field 24J, Rendering Provider ID #, on the CMS-1500 claim.
• Do not include the physician assistant's license number on these claims.
Source: BCBSM The Record April 2008 - page 21

BCBSM Update on Reimbursement for
Hospital Employed PAs
• BCBSM has indicated that a hospital will not
be reimbursed for services provided by
hospital employed PAs if the PAs salary is
part of the negotiated hospital payments.
• THE QUESTION! ARE HOSPITALS INCLUDING
PAS IN THE FINANCIAL REPORTS SUPPLIED TO
BCBSM IN THE PAYMENT NEGOTIATIONS?

BCBSM and BCN announce requirement
for enrollment / re-enrollment for PAs
August 2017 – The Record
• Physician assistants must re-enroll to be reimbursed for services within their scope of
• license for dates of service on or after Feb. 1, 2018.
• Beginning Oct. 1, 2017, physician assistants must: Re-enroll and be credentialed with
Blue Cross Blue Shield of Michigan and Blue Care Network, including our Medicare
Advantage programs.
• Complete our attestation form, indicating that they have a legally required practice
• agreement with a physician, along with other required documents.
• For participation with BCN, PAs must enroll as part of an existing contracted group or
• request participation via a new group practice.
• Complete a CAQH ProView credentialing application within 14 calendar days of
• submitting enrollment requests.
• Current reimbursement arrangements will be terminated for dates of service after Jan.
• 31, 2018
BCBSM – The Record August 2017
http://www.bcbsm.com/newsletter/therecord/2017/record_0817/the_record_0817.html

BCBSM and BCN announce requirement
for enrollment / re-enrollment for PAs• Regarding dates of service on or after Feb. 1: PAs who have re-enrolled by Jan. 31 will be
eligible for reimbursement for services within their scope of license either directly or under a group for all lines of business. PAs who have not will have their claims denied.
• PAs may choose to continue to be affiliated with physician groups and bill under the groups. If so, PAs should ensure they indicate the groups’ information when they contract and re-enroll.
• PAs will continue to be reimbursed at 85 percent of the physician fee schedule.
• Current BCN authorization and referral requirements will continue to apply.
• Why are Blue Cross and BCN making this change?
• We’re making this change because the state of Michigan allows PAs to work within their full scope of practice without direct or general supervision by a participating physician.
• The state also requires that PAs initiate and maintain a practice agreement with
• participating physicians.
• How to contract and re-enroll
• Starting Oct. 1, PAs can find and use the Blue Cross and BCN practitioner agreements
• and enrollment forms on bcbsm.com.
• We’ll also provide additional information in upcoming editions of The Record and BCN Provider News.
• If you have questions, contact Provider Inquiry or your provider consultant.
http://www.bcbsm.com/newsletter/therecord/2017/record_0817/the_record_0817.html

BCBSM and BCN meeting with MAPA
Oct. 17, 2017
• Discussion of intent for re-enrollment / enrollment under BCN
• Discussion of indirect v direct billing parameters for BCBSM and how it compares to “incident to” and “shared service” under CMS
• Discussed PQRS and how to communicate with BC on those who are already enrolled
• Discussed Tiered incentives like physicians under Physician Group Incentive Payments (PGIP)
• Discussed reimbursement for psychiatric services

BCBSM and BCN meeting with MAPA
Oct. 17, 2017
• Discussed direct payment of services
provided to PA
– Considering direct payment in 2018 for
certain plans
– Credentialing of PAs include BCBSM, BCN,
BCNA, MAPPO, they will not require
credentialing for PPO….yet?

BCN and payment for primary care
services
• MAPA has received inquiries from practices that they are receiving rejection for payment of PA services– Cited cause is that PAs cannot be designated as
primary care providers
– Suspicion is that practices are not submitting claims under the collaborating physician
– Request claims rejections be passed along to MAPA who will intern communicate with officials at BCN

Private Payers
Private payers cover services delivered by PAs/NPs
Individual payers may require billing for NPPs to be submitted under the physician’s name and/or provider number or the hospital’s tax ID
Not necessarily the same as Medicare’s “incident to” policy

Private Payers
It is not fraud to bill under the physician/hospital if authorized by the payer
It is a mistake to assume that all payers follow the same billing rules
Must have specific policies from payers in your region


32
Medicare Payment
Covered Services Coverage is limited to the services a PA is legally authorized to perform in accordance with State law (or State regulatory mechanism provided by State law).
Generally the services of a PA may be covered under Medicare Part B, if all of the following requirements are met:
• They are the type that are considered physician’s services if furnished by a doctor of medicine or osteopathy (MD/DO);
• They are performed by a person who meets all the PA qualifications,
• They are performed under the general supervision of an MD/DO;
• The PA is legally authorized to perform the services in the state in which they are performed; and
• They are not otherwise precluded from coverage because of one of the statutory exclusions.
Excerpt from Medicare Policy Manual: Chapter 15 §190
Recent CMS/WPS refusal of
payment• Group practices have had refusals for payment
when PAs within different specialties perform services on the same patient on the same day– CMS Taxonomy for PAs….only 1 = 97
• What to do?
Recently MAPA was made aware of WPS refusing payment for procedures performed by PAs
Radiology setting – percutaneous renal biopsy
Trauma setting – bedside bronchoscopy in trauma patient
PLEASE FORWARD SIMILAR REFUSALS TO MAPA

Recent CMS/WPS refusal of
payment for procedures
MAPA / AAPA encourage these cases be appealed through the defined CMS 5 level appeal process.
1st level appeal does not address “scope of practice”
2nd level appeal should include explanation of inclusion of scope of practice
3rd level of appeal by an Administrative law judge should include
State law scope of practice (inclusive or without exclusion)
Evidence of education and training of the service
Hospital privledging for providing the service

Questions?
35

Medicare
Medicare will reimburse for services
provided to Medicare beneficiaries
provided by PAs in all areas / settings:
At 85% of the physician fee schedule
Why is this important?
36

Medicare “Incident to”
“Incident to” is a Medicare billing provision that allows PAs to bill Medicare
under the physician’s NPI number, if Medicare’s strict criteria for “incident-
to” billing are met:
• Services are provided in a physician’s office or physician’s clinic;
• Physician sees Medicare patient on initial visit, establishes a diagnosis and
treatment plan. PA sees patient on follow up visit;
• For established Medicare patients with a new problem, the physician sees
the patient first for the new problem, establishes a diagnosis and
treatment plan, PA sees patient on follow up visit;
• a Physician is on site, within the suite of offices, when the patient is seen
by the PA;
• Services are within the PA’s state law scope of practice; and
• the PA represents a direct financial expense to the physician billing (W-2
or leased employee, or independent contractor).37

Medicare “Incident to”
The physician must continue to see the patient at a
frequency that reflects ongoing management of the
patient’s care. If all of the above criteria (previous slide)
are met, you may bill Medicare under the physician’s NPI
with reimbursement at 100%.
If any of the first 4 bulleted criteria are not met, bill
Medicare under the PA’s NPI with reimbursement at 85%.
38

Medicare “Incident to”
PAs may see new Medicare patients, see established
Medicare patients with new problems, and may see
Medicare patients under state law guidelines for
supervision; the claim must then be submitted under the
PA’s NPI.
Reimbursement at will be at 85% of the Physician Fee
Schedule.
39

Medicare “Incident to”
Remember!
“Incident to” is a Medicare Provision this provision
DOES NOT necessarily apply to Private Payers
“Incident to” applies to the outpatient physician
office only! There are separate provisions for
hospital based PA practice.
Should your office use “incident to”?
40

Medicare “Shared Service”
Shared Visit billing is a Medicare provision that applies to anevaluation and management (E/M) service in which both the physicianand the PA participate, allowing the combined service to be billedunder the physician’s NPI, with reimbursement at 100% of thePhysician Fee Schedule.
• The shared visit concept does not apply to procedures or critical care services or nursing home visits.
• The PA and physician must be employed by the same entity.
• Shared visits can be applied to initial and subsequent hospital visits, as well as visits in the Emergency Dept.
• The patient must be seen by the PA and the physician on the same calendar day. However, this does not mean at the same time.
41

Medicare “Shared Service”
“Shared Services” apply to Hospital
Inpatient / Hospital Outpatient and
Emergency Department Settings.
“Incident to” does not apply in these
settings
42

Medicare “Shared Service”
To properly document a “Shared Service” the Physician must have a face to face encounter with the patient on the same calendar day as the PA
The Physician must document a portion of the evaluation and management (E&M) encounter.
“Seen and Agree”, “I agree with the PAs plan” does not meet the level for “shared service” billing.
43

Medicare Shared Visit – Key Points
• Hospital inpt/outpt or ED
• Services performed on same calendar day
• Common employment
• E/M services, but not critical care or procedures
• Physician delivers face-to-face portion of E/M service
• Clear documentation on medical record of physician’s professional service