phototoxicity testing—in vivo and in vitro
TRANSCRIPT
Fd Chew. Toxic. Vol. 25, No. 5, pp. 407414, 1987 Printed in Great Britain. All rights reserved
0278-6915/87 $3.00 + 0.00 Copyright 0 1987 Pergamon Journals Ltd
Review Section
PHOTOTOXICITY TESTING--IN VW0 AND IN VITRO*
TH. MAURER Ciba-Geigy Ltd, CH-4002 Basel, Switzerland
(Received 21 November 1985; revisions received 4 September 1986)
Introduction
Phototoxic reactions to psoralens, to products from coal tar or plants and to drugs are well known, and both animal tests and in oitro methods exist for their assessment. Nevertheless, new agents may be devel- oped, such as the non-steroidal anti-inflammatory agents, in which such activity is unexpected.
The question then arises as to whether the available methods are sensitive enough. Phototoxicity testing has changed markedly in the last 10 years. Methods have been improved, and new compounds have been involved in clinical studies.
This review is divided into four major parts, deal- ing with adverse human reactions and with predictive testing in man, in animals and in vitro. The limi- tations of animal and in vitro methods, as well as the various influences on testing, including the emission spectrum of the radiation source, the light dose, the animal strain and the vehicle, are considered and the different testing procedures are discussed with regard to predictions of effects in man.
Following the convention defined by Cronin (1980), the term ‘photosensitivity’ is used in this paper to describe any eruption caused by light; it does not, therefore, necessarily imply an allergic mech- anism but covers both phototoxic and photoallergic reactions.
Adverse human reactions
Marzulli & Maibach (1985) defined phototoxicity as a non-immunological light-induced skin response (dermatitis) to a photoactive chemical, the response being likened to an exaggerated sunburn. The photo- active chemical may reach the target tissues either by direct application or indirectly via the blood system following ingestion or parenteral administration.
*Based on a paper presented at an International Sym- posium on Skin Care and Function, Environmental/ Occupational Influences, Oslo, 29-31 Auaust 1985.
Abbreviohons: CSM = Committee on Safety >f Medicines (UK): CPZ = chlornromazine: DMCT = demethvl- ehlorretraeycline (d~meclocyclme); MED = mini&l erythematogenic dose; S-MOP = 8-methoxypsoralen; PUVA = psoralen plus UV-A; UV = ultraviolet irra- diation.
Phototoxic reactions are comparable with primary irritation reactions in that they may be elicited after a single exposure, no induction period is required, neither flare-up reactions nor cross reactions occur and a high incidence of reactors is possible in an exposed population.
Among the known topical photosensitizers are anthracene, fluoranthene, phenanthrene, benzo- pyrene and acridine from pitch and coal tar, furo- coumarins, including 8-methoxypsoralen (8-MOP, xanthotoxin), 5-methoxypsoralen (bergapten) and trimethoxypsoralen, and various dyes, notably eosin, methylene blue, toluidine blue, acridine orange, acriflavine, rose bengal, Disperse Blue 35, neutral red and trypoflavin (Cronin, 1980; Haudenschild & Krebs, 1982). The incidence of phototoxicity follow- ing accidental exposure to one of these topical photo- sensitizers and simultaneous exposure to sunlight may be high, as is the case with psoralens present in plants. In contrast, the incidence of phototoxic reac- tions to ingested drugs is normally very low.
Table 1 summarizes a long list of drugs collected by Magnus (1976) from reports of the UK Committee on Safety of Medicines (CSM). During the 7-year period from 1964 to 1971, more than 100 million packages of drugs were prescribed in the UK by general practitioners and only 454 reports on photo- sensitization reactions were collected. It is clear that the effective incidence will be higher than that shown in Table 1, but never very much higher, in view of the definition of phototoxic reactions.
The whole list compiled by Magnus (1976) in- cluded 69 compounds, so most of the individual compounds were reported to have induced only a few reactions. However, for a few compounds (pro- triptyline, demethylchlortetracycline (DMCT) and nalidixic acid), the incidence of phototoxic reactions was significantly above average. Ten years later, the same compounds are still the major cause of photo- toxic reactions. The photosensitizing agents have been classified by Hawk (1984) on the same basis as the list compiled by Magnus (1976). Hawk (1984) listed analgesics (including azapropazone), anti- bacterial agents (nalidixic acid, sulphonamides and DMCT), antidepressants, (protriptyline), anti- diabetics, antiepileptics, antifungals, antihistamines, antihypertensives and antiarrhythmics, cytotoxins, diuretics (hydrochlorothiazide), oral contraceptives
407

408 TH. MAURER
Table 1. Data from Committee on Safety of Medicines, 1964-1971, on the incidence of phototoxic reactions to drugs prescribed in the UK in 1970’
Type of drug No. of Total prescriptions
reactions (x 106)
Hypnotics Miscellaneous anticonvulsants,
hypnotics and sedatives Tranquillizers
Protriptyline Stimulants Analgesics Autonomic drugs Antihistamines Oral contraceptives Antibiotics
Demethylchlortetracycline Antibacterials 55
Nalidixic acid 43
^ L
13 83 52
10
13 44 75 55
14.0
6.4 17.56 0.2 2.0 8.0 6.0
13.8
24.5 0.8 2.9 0.4
*Data from Magnus (1976).
and oestrogens, specific photosensitizers (meth- oxsalen, trioxsalen) and tranquillizers (chlor- promazine). Of the individual examples given in parenthesis, sulphonamides and chlorpromazine fea- tured in more than 20 reports to the CSM between 1964 and 1981 and the others in more than 50 such reports in the same period.
Since 1981, the distribution of phototoxic reactions has changed, with benoxaprofen and a few other non-steroidal anti-inflammatory drugs causing the majority of phototoxic side-effects. Consequently phototoxicity screening tests have become in- creasingly important in the development of new non-steroidal anti-inflammatory drugs. However, phototoxicity testing is not a routine procedure for all new chemicals and therefore much less experience has been gained in this than, for example, in irritation testing. It is therefore necessary to ascertain what screening tests are available and how sensitive they are, as well as to identify the reference compounds that should be used to determine the specificity of a phototoxicity test.
Human testing
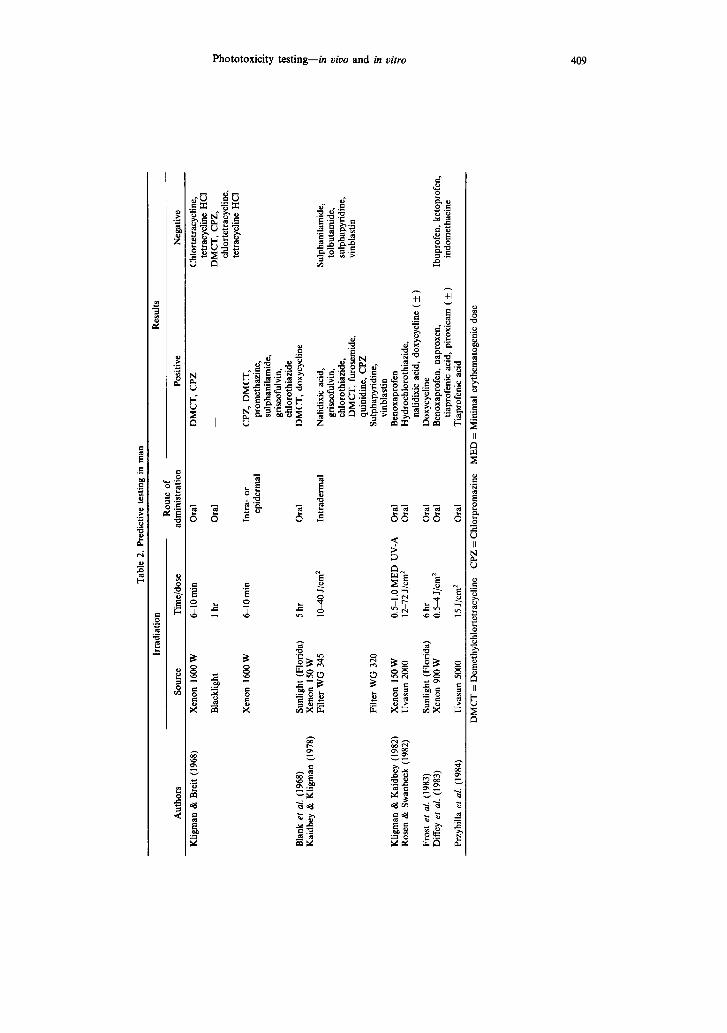
Table 2 summarizes published results of photo- toxicity studies in human volunteers. The variables in the different reports are not the reference compounds, which were the same as the main causative agents identified in clinical practice, but the light source and the doses.
Kligman & Breit (1968) evaluated the usefulness of various light sources (xenon, fluorescent sunlight and blacklight) and of various routes of administration (oral, intradermal or epidermal). After oral adminis- tration, only DMCT and chlorpromazine induced phototoxic reactions. More compounds were positive after intradermal or epidermal application.
Kaidbey & Kligman (1978) improved the method involving intradermal administration of the com- pounds by using a xenon solar simulator (Berger, 1969 & 1976) for local UV-A irradiations, and ob- served positive reactions to nalidixic acid, griseoful- vin, chlorothiazide, DMCT, furosemide, quinidine and chlorpromazine. The minimal elicitation dose was 10 J/cm2 for quinidine and 40 J/cm’ for griseoful- vin, demonstrating the range of phototoxic potential among the compounds tested. Positive reactions to
sulphanilamide, sulphapyridine and vinblastin were only elicited when the emission spectrum contained UV-B. New light sources and new reference com- pounds have since been introduced, but the light dose has still not been standardized.
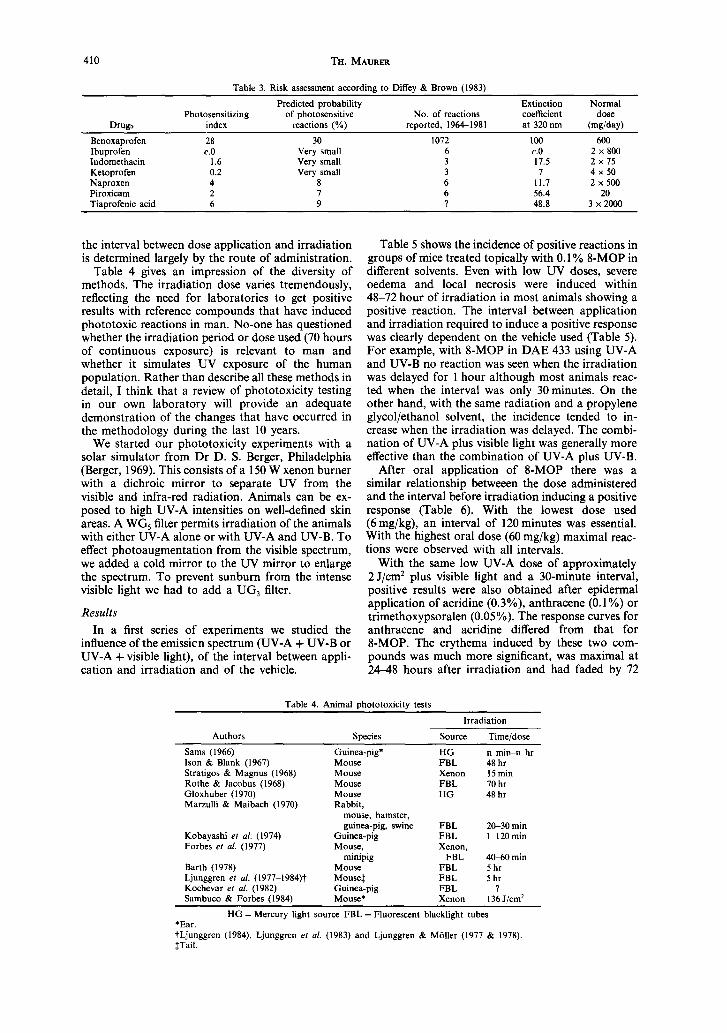
A new method for predicting phototoxic potential was introduced by Diffey & Brown (1983). On the basis of the normal daily dose, the extinction coefficient at 320 nm and the radiant exposure, a photosensitizing index is calculated for each drug. With an extended formula, individual risks may be evaluated by considering the individual’s outdoor activities and exposure to sunlight.
Examples of the estimated risk, calculated for a l-hour midsummer exposure in the UK, are shown in Table 3. There is a reasonable correlation between the calculated risks and the number of clinical reports.
The high risk with benoxaprofen is based on the combination of a relatively high daily dose and a large extinction coefficient at 320 nm. The risk with piroxicam is much smaller because the compound is pharmacologically more active and, therefore, the daily dose requirement is correspondingly lower.
Animal studies
In vivo procedures
Before human studies are performed to evaluate the effective risk of drugs in man, animal screening studies are essential. There are no regulatory guide- lines on methods of testing new compounds for their phototoxic potential, so it is not surprising that no standardized method is available. Furthermore, it is very difficult to compare the different published methods because so many variables are involved. These include the species, the light source, the light dose, the route of administration and the interval between chemical treatment and irradiation. The guinea-pig and the mouse are the main species used, while xenon and fluorescent blacklight tubes are the light sources that have been used more frequently. Light doses including UV-B are limited by the ery- thematogenic action; a large variation (0.5100 J/ cm*) has been observed using UV-A lamps. The choice of a local or systemic route of administration depends on the possible type of human exposure, and
Tab
le
2. P
redi
ctiv
e te
stin
g in
m
an
Aut
hors
Irra
diat
ion
Res
ults
R
oute
of
S
ourc
e T
ime/
dose
ad
min
istr
atio
n Po
sitiv
e N
egat
ive
Klig
man
&
B
reit
(196
8)
Bla
nk
et a
l. (1
968)
K
aidb
ey
& K
ligm
an
(197
8)
Klig
man
&
Kai
dbey
(1
982)
X
enon
15
0 W
R
osen
&
S
wan
beck
(1
982)
U
vasu
n 20
00
Fros
t el
al
. (1
983)
D
iffe
y et
al
. (1
983)
Su
nlig
ht
(Flo
rida
) X
enon
90
0 W
Przy
billa
ef
al.
(198
4)
Uva
sun
5000
Xen
on
16
00 W
Bla
cklig
ht
Xen
on
1600
W
Sunl
ight
(F
lori
da)
Xen
on
150
W
Filte
r W
G
345
Filte
r W
G
320
&lO
min
1 hr
6lO
min
5hr
l&40
J/
cm*
0.5-
1.0
ME
D
UV
-A
12-7
2 J/
cm*
6hr
0.5-
4 J/
cm*
15 J
/cm
*
Ora
l
Ora
l
Intr
a-
or
epid
enna
l
Ora
l
Intr
aden
nal
Ora
l O
ral
Ora
l O
ral
Ora
l
DM
CT
, C
PZ
CPZ
, D
MC
T,
prom
etha
zine
, su
lpha
nila
mid
e,
gris
eofu
lvin
, ch
loro
thia
zide
D
MC
T,
doxy
cycl
ine
Chl
orte
trac
yclin
e,
tetr
acyc
line
HC
I D
MC
T,
CPZ
, ch
lort
etra
cycl
ine,
te
trac
yclin
e H
CI
Sulp
hani
lam
ide,
to
lbut
amid
e,
sulp
hapy
ridi
ne,
vinb
last
in
Ibup
rofe
n,
keto
prof
en,
indo
met
haci
ne
Nal
idix
ic
acid
, gr
iseo
fidv
in,
chlo
roth
iazi
de,
DM
CT
, fu
rose
mid
e,
quin
idin
e,
CPZ
Su
lpha
pyri
dine
, vi
nbla
stin
B
enox
apro
fen
Hyd
roch
loro
thia
zide
, na
lidix
ic
acid
, do
xycy
clin
e (
f )
Dox
ycyc
line
Ben
oxap
rofe
n,
napr
oxen
, tia
prof
enic
ac
id,
piro
xica
m
( +
)
Tia
prof
enic
ac
id
DM
CT
=
Dem
ethy
lchl
orte
trac
yclin
e C
PZ
= C
hlor
prom
azin
e M
ED
=
Min
imal
er
ythe
mat
ogen
ic
dose
410 Tn. MAURER
Table 3. Risk assessment according to Diffey & Brown (1983)
Drugs Photosensitizing
index
Predicted probability of photosensitive
reactions (%) No. of reactions
reported, 19641981
Extinction Normal coefficient dose at 320 nm (mg/day)
Benoxaprofen 28 30 1072 100 600 Ibuprofen C.0 Very small 6 C.0 2 x 800 Indomethacin 1.6 Very small 3 17.5 2 x 75 Ketoprofen 0.2 Very small 3 7 4 x 50 Naproxen 4 8 6 11.7 2 x 500 Piroxicam 2 7 6 56.4 20 Tiaorofenic acid 6 9 ? 48.8 3x2000
Table 4. Animal ohototoxicitv tests
the interval between dose application and irradiation is determined largely by the route of administration.
Table 4 gives an impression of the diversity of methods. The irradiation dose varies tremendously, reflecting the need for laboratories to get positive results with reference compounds that have induced phototoxic reactions in man. No-one has questioned whether the irradiation period or dose used (70 hours of continuous exposure) is relevant to man and whether it simulates UV exposure of the human population. Rather than describe all these methods in detail, I think that a review of phototoxicity testing in our own laboratory will provide an adequate demonstration of the changes that have occurred in the methodology during the last 10 years.
We started our phototoxicity experiments with a solar simulator from Dr D. S. Berger, Philadelphia (Berger, 1969). This consists of a 150 W xenon burner with a dichroic mirror to separate UV from the visible and infra-red radiation. Animals can be ex- posed to high UV-A intensities on well-defined skin areas. A WGS filter permits irradiation of the animals with either UV-A alone or with W-A and UV-B. To effect photoaugmentation from the visible spectrum, we added a cold mirror to the UV mirror to enlarge the spectrum. To prevent sunburn from the intense visible light we had to add a UG3 filter.
Results
In a first series of experiments we studied the influence of the emissicn spectrum (UV-A + UV-B or UV-A + visible light), of the interval between appli- cation and irradiation and of the vehicle.
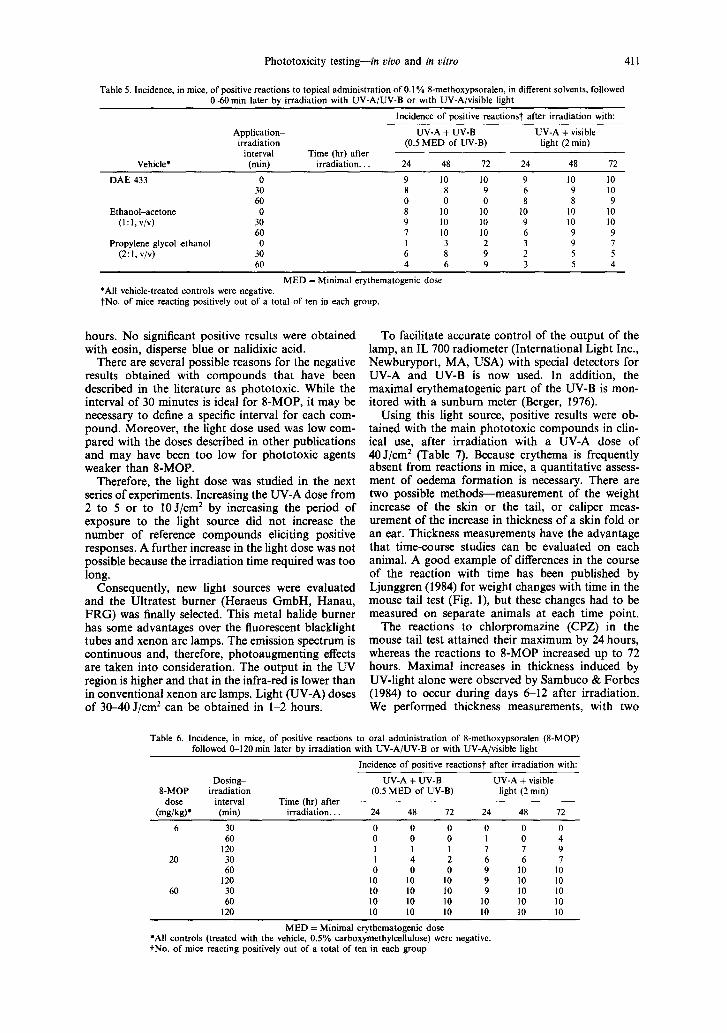
Table 5 shows the incidence of positive reactions in groups of mice treated topically with 0.1% 8-MOP in different solvents. Even with low UV doses, severe oedema and local necrosis were induced within 48-72 hour of irradiation in most animals showing a positive reaction. The interval between application and irradiation required to induce a positive response was clearly dependent on the vehicle used (Table 5). For example, with 8-MOP in DAE 433 using UV-A and UV-B no reaction was seen when the irradiation was delayed for 1 hour although most animals reac- ted when the interval was only 30minutes. On the other hand, with the same radiation and a propylene glycol/ethanol solvent, the incidence tended to in- crease when the irradiation was delayed. The combi- nation of UV-A plus visible light was generally more effective than the combination of UV-A plus UV-B.
After oral application of 8-MOP there was a similar relationship betweeen the dose administered and the interval before irradiation inducing a positive response (Table 6). With the lowest dose used (6 mg/kg), an interval of 120 minutes was essential. With the highest oral dose (60 mg/kg) maximal reac- tions were observed with all intervals.
With the same low UV-A dose of approximately 2 J/cm2 plus visible light and a 30-minute interval, positive results were also obtained after epidermal application of acridine (0.3%), anthracene (0.1%) or trimethoxypsoralen (0.05%). The response curves for anthracene and acridine differed from that for 8-MOP. The erythema induced by these two com- pounds was much more significant, was maximal at 24-48 hours after irradiation and had faded by 72
Irradiation
Authors Species Source Time/dose
Sams (1966) Guinea-pig* HG n min-n hr Ison & Blank (1967) Mouse FBL 48 br Stratigos & Magnus (1968) Mouse Xenon 15min Rotbe & Jacobus (1968) Mouse FBL 70 hr Gloxhuber (1970) Mouse HG 48 hr Marzulli & Maibach (1970) Rabbit,
mouse, hamster, guinea-pig, swine FBL 2&30 min
Kobayashi er al. (1974) Guinea-pig FBL I-120 min Forbes er al. (1977) Mouse, Xenon,
minipig FBL 40-60 min Barth (1978) Mouse FBL 5 hr Ljunggren ef al. (1977-1984)t Mouse1 FBL 5 hr Kochevar er al. (1982) Guinea-pig FBL ? Sambuco & Forbes (1984) Mouse* Xenon 136 J/cm2
HG = Mercury light source FBL = Fluorescent blacklight tubes *Ear. tLjunggren (1984), Ljunggren ef al. (1983) and Ljunggren & Miiller (1977 & 1978). fTail.
Phototoxicity testing-in vivo and in vitro 411
Table 5. Incidence, in mice, of positive reactions to topical administration of 0. I % 8-methoxypsoralen, in different solvents, followed O-60 min later by irradiation with WV-A/W-B or with UV-A/visible light
Incidence of positive reactionst after irradiation with:
Vehicle*
Application- irradiation
interval (min)
Time (hr) after irradiation.
UV-A + UV-B UV-A + visible (0.5 MED of UV-B) light (2 min)
24 48 12 24 48 12
DAE 433
Ethanol-acetone (I:l,v/v)
Propylene glycolkthanol (2:l, v/v)
0 9 IO IO 9 30 8 8 9 6 60 0 0 0 8 0 8 IO IO IO
30 9 10 10 9 60 7 IO IO 6 0 I 3 2 3
30 6 8 9 2 60 4 6 9 3
IO IO 9 IO 8 9
IO IO 10 10 9 9 9 7 5 5 5 4
MED = Minimal erythematogenic dose *All vehicle-treated controls were negative. tNo. of mice reacting positively out of a total of ten in each group.
hours. No significant positive results were obtained with eosin, disperse blue or nalidixic acid.
There are several possible reasons for the negative results obtained with compounds that have been described in the literature as phototoxic. While the interval of 30 minutes is ideal for 8-MOP, it may be necessary to define a specific interval for each com- pound. Moreover, the light dose used was low com- pared with the doses described in other publications and may have been too low for phototoxic agents weaker than g-MOP.
Therefore, the light dose was studied in the next series of experiments. Increasing the UV-A dose from 2 to 5 or to 10 J/cm* by increasing the period of exposure to the light source did not increase the number of reference compounds eliciting positive responses. A further increase in the light dose was not possible because the irradiation time required was too long.
Consequently, new light sources were evaluated and the Ultratest burner (Heraeus GmbH, Hanau, FRG) was finally selected. This metal halide burner has some advantages over the fluorescent blacklight tubes and xenon arc lamps. The emission spectrum is continuous and, therefore, photoaugmenting effects are taken into consideration. The output in the UV region is higher and that in the infra-red is lower than in conventional xenon arc lamps. Light (UV-A) doses of 30-40 J/cm2 can be obtained in l-2 hours.
To facilitate accurate control of the output of the lamp, an IL 700 radiometer (International Light Inc., Newburyport, MA, USA) with special detectors for UV-A and UV-B is now used. In addition, the maximal erythematogenic part of the UV-B is mon- itored with a sunburn meter (Berger, 1976).
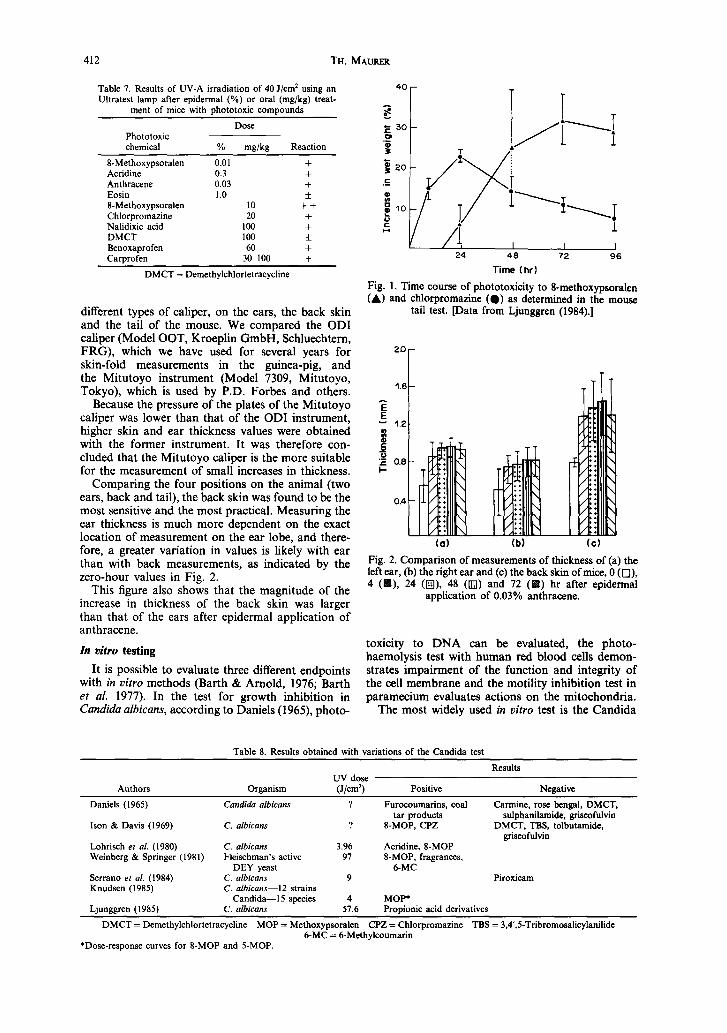
Using this light source, positive results were ob- tained with the main phototoxic compounds in clin- ical use, after irradiation with a UV-A dose of 40 J/cm2 (Table 7). Because erythema is frequently absent from reactions in mice, a quantitative assess- ment of oedema formation is necessary. There are two possible methods-measurement of the weight increase of the skin or the tail, or caliper meas- urement of the increase in thickness of a skin fold or an ear. Thickness measurements have the advantage that time-course studies can be evaluated on each animal. A good example of differences in the course of the reaction with time has been published by Ljunggren (1984) for weight changes with time in the mouse tail test (Fig. l), but these changes had to be measured on separate animals at each time point.
The reactions to chlorpromazine (CPZ) in the mouse tail test attained their maximum by 24 hours, whereas the reactions to g-MOP increased up to 72 hours. Maximal increases in thickness induced by UV-light alone were observed by Sambuco & Forbes (1984) to occur during days 612 after irradiation. We performed thickness measurements, with two
Table 6. Incidence, in mice, of positive reactions to oral administration of 8methoxypsoralen (S-MOP) followed O-120 min later by irradiation with UV-A/UV-B or with UV-A/visible light
Incidence of positive reactionst after irradiation with:
Dosing- UV-A + UV-B UV-A + visible g-MOP irradiation (0.5 MED of W-B) light (2 min)
dose interval Time (hr) after
(mg/kg)* (min) irradlatlon. 24 48 72 24 48 72
6 30 0 0 0 0 0 0 60 0 0 0 I 0 4
120 I I 1 1 I 9 20 30 I 4 2 6 6 7
60 0 0 0 9 IO 10 120 10 10 IO 9 IO IO
60 30 IO IO IO 9 IO 10 60 IO IO 10 10 10 IO
120 IO IO IO IO 10 10
MED = Minimal erythematogenic dose *All controls (treated with the vehicle, 0.5% carboxymethylcellulose) were negative. tNo. of mice reacting positively out of a total of ten in each group.
412 TH. MAURER
Table 7. Results of UV-A irradiation of 40 J/cm* using an Ultratest lamp after epidermal (%) or oral (mg/kg) treat-
ment of mice with phototoxic compounds
Dose Phototoxic chemical % mg/kg Reaction
8-Methoxypsoralen 0.01 + Acridine 0.3 + Anthracene 0.03 + Eosin 1.0 f 8-Methoxypsoralen IO ++ Chlorpromazine 20 + Nalidixic acid I00 + DMCT 100 f Benoxaprofen 60 + Carprofen 3&lOO +
DMCT = Demethylchlortetracycline
different types of caliper, on the ears, the back skin and the tail of the mouse. We compared the ODI caliper (Model OOT, Kroeplin GmbH, Schluechtern, FRG), which we have used for several years for skin-fold measurements in the guinea-pig, and the Mitutoyo instrument (Model 7309, Mitutoyo, Tokyo), which is used by P.D. Forbes and others.
Because the pressure of the plates of the Mitutoyo caliper was lower than that of the ODI instrument, higher skin and ear thickness values were obtained with the former instrument. It was therefore con- cluded that the Mitutoyo caliper is the more suitable for the measurement of small increases in thickness.
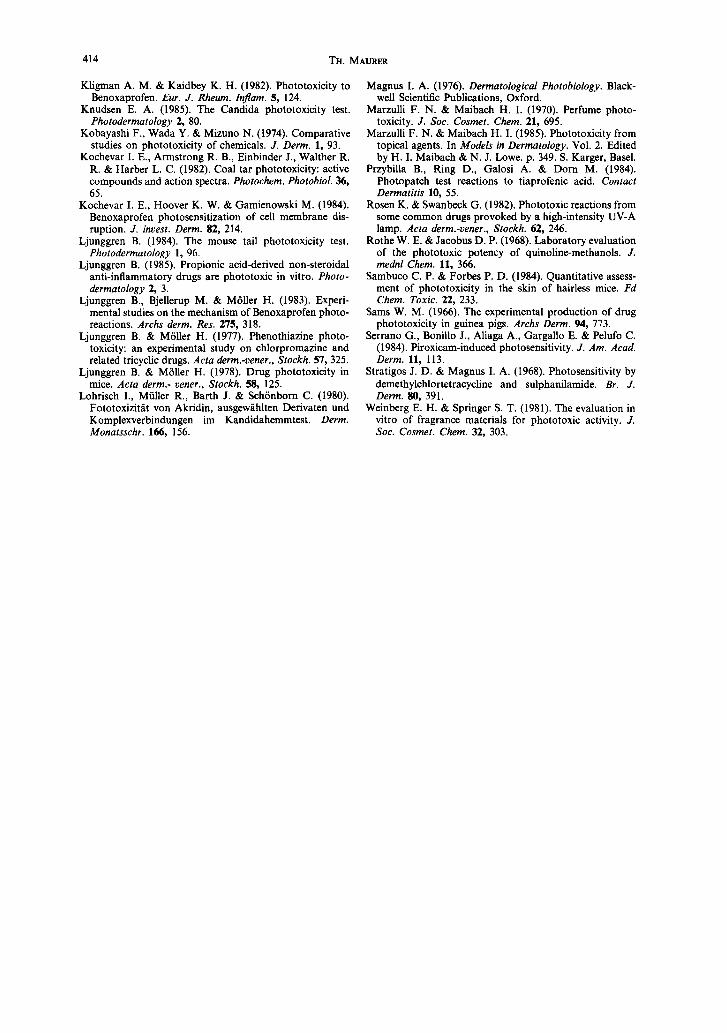
Comparing the four positions on the animal (two ears, back and tail), the back skin was found to be the most sensitive and the most practical. Measuring the ear thickness is much more dependent on the exact location of measurement on the ear lobe, and there- fore, a greater variation in values is likely with ear than with back measurements, as indicated by the zero-hour values in Fig. 2.
This figure also shows that the magnitude of the increase in thickness of the back skin was larger than that of the ears after epidermal application of anthracene.
In aitro testing
It is possible to evaluate three different endpoints with in vitro methods (Barth & Arnold, 1976; Barth et al. 1977). In the test for growth inhibition in Cundidu albicuns, according to Daniels (1965), photo-
40 -
24 48 72 96
Time (hrl
Fig. 1. Time course of phototoxicity to Smethoxypsoralen (A) and chlorpromazine (a) as determined in the mouse
tail test. [Data from Ljunggren (1984).]
2.0
r
0.4 -
(a) (b) (cl
Fig. 2. Comparison of measurements of thickness of (a) the left ear, (h) the right ear and (c) the back skin of mice, 0 (o),
), 24 (I), 48 (IJJJ) and 12 (H) hr after epidemal application of 0.03% anthracene.
toxicity to DNA can be evaluated, the photo- haemolysis test with human red blood cells demon- strates impairment of the function and integrity of the cell membrane and the motility inhibition test in paramecium evaluates actions on the mitochondria.
The most widely used in vitro test is the Candida
Table 8. Results obtained with variations of the Candida test
Authors Organism UV dose
(J/cm? Positive
Results
Negative
Daniels (I 965) Candida albicam ? Furocoumarins, coal Carmine, rose bengal, DMCT, tar products sulphanilamide, griseofulvin
Ison & Davis (1969) C. albicans ? S-MOP, CPZ DMCT, TBS, tolbutamide, griseofulvin
Lohrisch ef al. (1980) C. albicans 3.96 Acridine, S-MOP Weinberg & Springer (1981) Fleischman’s active 97 S-MOP, fragrances,
DEY yeast 6-MC Serrano ef al. (1984) C. albicans 9 Piroxicam Knudsen (I 985) C. nlbicans-12 strains
Candida- species 4 MOP* Ljunggren (1985) C. albicam 57.6 Propionic acid derivatives
DMCT = Demethylchlortetracycline MOP = Methoxypsoralen CPZ = Chlorpromazine TBS = 3,4’,5-Tribromosalicylanilide 6-MC = 6-Methylcoumarin
*Dose-response curves for S-MOP and 5-MOP.

Phototoxicity testing--in uiuo and in vitro 413
Table 9. Compounds giving positive results in the photohaemolysis test
Authors W dose Postive results
Barth ef al. (1977) Ljunggren et al. (1983) Bjellerup & Ljunggren (1984) Kochevar et al. (1984) Ljunggren (1985)
10 min4 hr 10.8 J/cm’ 3&144 J ? W-A 43.2 J/cm2
UV-B 0.035-16 J/cm*
Acridine, anthracene, CPZ, sulphanilamide Benoxaprofen DMCT, CPZ Benoxaprofen Propionic acid derivatives,
3/6 nonpropionic acid derivatives Prooionic acid derivatives
CPZ = Chlorpromazine DMCT = Demethylchlortetracycline
test (Daniels, 1965), but several variations on the method have been published (Table 8) and a stan- dardized method does not exist.
Differences in the sensitivity of various Cundidu albicans strains and Candida species were observed by Knudsen (1985) in an assessment of sensitivity to PUVA (psoralen plus UV-A), but there were no essential differences between the various strains. Not all known phototoxic agents have induced reactions in this test system. DMCT, for example, has given negative results (Daniels, 1965; Ison & Davis 1969). Kavli & Volden (1984) recommended the Candida test as an in vitro method, but with the reservation that false-negative and false-positive results are possi- ble.
A test based upon the haemolysis of human red blood cells by UV light and chemicals was developed later than the Candida test. This has been used by a number of workers (Table 9) but the range of data is, at present, too small for a complete evaluation of the usefulness of the test.
An interesting paper on propionic acid derivatives and other non-steroidal anti-inflammatory agents, recently published by Ljunggren (1985), raised several important points. First, it was recommended that photohaemolysis tests with UV-A and UV-B light should be performed separately, depending on the absorption characteristics of the compound. Negative results obtained with piroxicam demonstrated that UV absorption did not equate with photoreactivity in this system. Despite the negative result, piroxicam had a higher absorption in the UV region than the other compounds tested. Ljunggren concluded that in vitro models are not sufficient for predictive purposes and for correlation with clinical photoxicity, but must be supplemented with in uivo tests.
Other test systems have been proposed but have not attained as much importance as the tests described.
Conclusion
In this review I have attempted to indicate the complexity of in vitro and in vioo phototoxicity testing and the various factors that may influence each system. We have seen that there are different ways of screening for the phototoxic potential of chemicals, and to facilitate the sound comparison of results it is essential that reports of phototoxicity tests include an exact description of the methodology used. Such tests should be performed, with the aim of preventing phototoxic reactions in the general population. How- ever, it is important to realize the limitations of the tests available at present. They are capable of de- tecting chemicals with phototoxic potential but it is not possible to predict the exact incidence of photo-
toxic reactions that may result from the use of any single compound.
REFERENCES
Barth J. (1978). Mouse screening test for evaluating protec- tion to longwave ultraviolet radiation. Br. J. Derm. 99, 357.
Barth J. & Arnold T. (1976). Zur Aussagekraft des Para- mlzientestes fiir die Erfassung von Fotosensibilisatoren. Derm. Monatsschr. 162, 900.
Barth J., Hofmann C. & Fickweiler E. (1977). Unter- suchungen zur fotohlmolytischen Potenz von Pharmaka und Industriesubstanzen. Derm. Monatsschr. 163, 613.
Berger D. S. (1969). Specification and design of solar ultraviolet simulator. .I. invest. Derm. 53, 192.
Berger D. S. (1976). The sunburning ultraviolet meter: design and performance. Photochem. Photobiol. 24, 587.
Bjellerup M. & Ljunggren B. (1984). Studies on photo- hemolysis with special reference to demethyl- chlortetracycline. Acta derm.-vener., Stockh. 64, 378.
Blank H., Cullen St. I. & Catalan0 P. M. (1968). Photo- sensitivity studies with demethylchlortetracycline and doxycycline. Archs Derm. 97, 1.
Cronin E. (1980). Contact Dermatitis. p. 414. Churchill Livingstone, Edinburgh.
Daniels F. (1965). A simple microbiological method for demonstrating phototoxic compounds. J. inoest. Derm. 44, 259.
Diffey B. L. & Brown S. (1983). A method for predicting the phototoxicity of non-steroidal anti-inflammatory drugs. Br. J. clin. Pharm. 16, 633.
Diffey B. L.. Daymond T. J. & Fairgreaves H. (1983). Phototoxic reactions to piroxicam, naproxen and tiaprofenic acid. Br. J. Rheumatol. 22, 239.
Forbes P. D., Urbach F. & Davies R. E. (1977). Photo- toxicity testing of fragrance raw materials. Fd Cosmet. Toxicol. 15, 55.
Frost P., Weinstein G. D. & Gomez E. C. (1983). Phototoxic potential of minocycline and doxycycline. Archs Derm. 105, 681.
Gloxhuber C. (1970). Priifung von Kosmetik-Grundstoffen auf fototoxische Wirkung. J. Sot. Cosmet. Chem. 21,825.
Haudenschild E. & Krebs A. (1982). Exogene Photo- dermatosen. Ther. Umsch. 39, 178.
Hawk J. L. M. (1984). Photosensitizing agents in the United Kingdom. Clin. exp. Derm. 9, 300.
Ison A. E. & Blank H. (1967). Testing drug phototoxicity in mice. J. invest. Derm. 49, 508.
Ison A. E. & Davis C. M. (1969). Phototoxicity of quinoline methanols and other drugs in mice and yeast. 1. invest. Derm. 52, 193.
Kaidbey K. H. & Kligman A. M. (1978). Identification of systemic phototoxic drugs by human intradermal assay. J. invest. Derm. 70, 272.
Kavli G. & Volden G. (1984). The Candida test for photo- toxicity. Photodermatology 1, 204.
Kligman A. M. & Breit R. (1968). The identification of phototoxic drugs by human assay. J. invest. Derm. 51,90.
414 TH. MAURER
Kligman A. M. & Kaidbey K. H. (1982). Phototoxicity to Magnus I. A. (1976). Dermatological Photobiology. Black- Benoxaprofen. Eur. J. Rheum. Iflam. 5, 124. well Scientific Publications, Oxford.
Knudsen E. A. (1985). The Candida phototoxicity test. Marzulli F. N. & Maibach H. I. (1970). Perfume nhoto- Photodermatology 2,’ 80.
Kobavashi F.. Wada Y. & Mizuno N. (1974). Comnarative studies on phototoxicity of chemicals. J. ‘Derm. i, 93.
Kochevar I. E., Armstrong R. B., Einbinder J., Walther R. R. & Harber L. C. (1982). Coal tar phototoxicity: active compounds and action spectra. Photochem. Photobiol. 36, 65.
Kochevar I. E., Hoover K. W. & Gamienowski M. (1984). Benoxaprofen photosensitization of cell membrane dis- ruption. J. invest. Derm. 82, 214.
Ljunggren B. (1984). The mouse tail phototoxicity test. Photodermatology 1, 96.
Ljunggren B. (1985). Propionic acid-derived non-steroidal anti-inflammatory drugs are phototoxic in vitro. Photo- dermatology 2, 3.
Ljunggren B., Bjellerup M. & Miiller H. (1983). Experi- mental studies on the mechanism of Benoxaprofen photo- reactions. Archs derm. Res. 275, 318.
Ljunggren B. & Miiller H. (1977). Phenothiazine photo- _ toxicity: an experimental study on chlorpromazine and related tricyclic drugs. Acta derm.-vener., Stockh. 57,325.
Ljunggren B. & Miiller H. (1978). Drug phototoxicity in
toxicity. J. Sot. Cosmet. Chem. il, 645. _ Marzulli F. N. & Maibach H. I. (1985). Phototoxicitv from
topical agents. In Models in D;rma;ology. Vol. 2. ‘Edited by H. I. Maibach & N. J. Lowe. p. 349. S. Karger, Basel.
Przybilla B., Ring D., Galosi A. & Dom M. (1984). Photopatch test reactions to tiaprofenic acid. Contact Dermatitis 10, 55.
Rosen K. & Swanbeck G. (1982). Phototoxic reactions from some common drugs provoked by a high-intensity UV-A lamp. Acta a&m.-ie&r., Stockh.-62, 246. _
Rothe W. E. & Jacobus D. P. (1968). Laboratorv evaluation of the phototoxic potency of &inoline-methanols. J. mednl Chem. 11, 366.
Sambuco C. P. & Forbes P. D. (1984). Quantitative assess- ment of phototoxicity in the skin of hairless mice. Fd Chem. Toxic. 22, 233.
Sams W. M. (1966). The experimental production of drug phototoxicity in guinea pigs. Archs Derm. 94, 773.
Serrano G., Bonillo J., Aliaga A., Gargallo E. & Pelufo C. (1984). Piroxicam-induced photosensitivity. J. Am. Acad. Derm. 11, 113.
Stratigos J. D. & Magnus I. A. (1968). Photosensitivity by -mice. Acta derm.- vener., Stockh. 58, 125. demethylchlortetracycline and sulphanilamide. Br. J.
Lohrisch I.. Miiller R., Barth J. & Schonbom C. (1980). Derm. 80. 391. Fototoxizitat von Al&din, ausgewahlten Derivatdn und Weinberg E; H. & Springer S. T. (1981). The evaluation in Komplexverbindungen im Kandidahemmtest. Derm. vitro of fragrance materials for phototoxic activity. J. Monatsschr. 166, 156. Sot. Cosmet. Chem. 32, 303.