photorefractive keratectomy with mitomycin-c after corneal transplantation for keratoconus
TRANSCRIPT

ARTICLE
Photorefractive keratec
tomy with mitomycin-Cafter corneal transplantation for keratoconusChris Hodge, BAppSc, Gerard Sutton, MB BS, MD, FRANZCO, FRACS,Michael Lawless, MB BS, FRANZCO, FRACS, FRCOphth, Chris Rogers, MB BS, FRANZCO, FRACS
Q
P
1884
2011 Aublished
PURPOSE: To evaluate the efficacy of photorefractive keratectomy (PRK) for residual refractiveerror after penetrating keratoplasty (PKP) for keratoconus.
SETTING: Private ophthalmic clinic.
DESIGN: Case series.
METHOD: Consecutive patients who had PRK augmented with topical mitomycin-C (MMC) afterPKP for keratoconus were retrospectively reviewed. Patients were divided into a a low cylindergroup (refractive cylinder %6.00 D) and a high cylinder group (refractive cylinder >6.00 D).Visual acuity, refraction, and keratometry were analyzed preoperatively and 1, 3, 6, and 12months postoperatively.
RESULTS: The study comprised 47 eyes (41 patients). The spherical equivalent (SE) decreasedfrom �4.24 D G 3.23 (SD) preoperatively to �0.71 G 1.03 D 12 months postoperatively in thelow cylinder group and from�4.19G 3.54 D to�2.45G 3.42 D, respectively, in the high cylindergroup. The refractive cylinder decreased from �4.27G 1.4 D to �1.71G 1.55 D, respectively, inthe low cylinder group and from �7.78 G 1.21 D to �4.6 G 2.54 D, respectively, in the high cyl-inder group. By the last follow-up, 8.3% of patients had lost 2 lines of corrected distance visualacuity. There were no cases of corneal haze greater than 2C or of graft rejection.
CONCLUSIONS: Penetrating keratoplasty with adjunctive MMC decreased several refractivevariables in patients with previous PKP. These results compare well with those in the publishedliterature and suggest PRK is as effective as, and probably safer than, laser in situ keratomileusisin treating refractive error in these cases.
Financial Disclosure: No author has financial or proprietary interests in any material or methodmentioned.
J Cataract Refract Surg 2011; 37:1884–1894 Q 2011 ASCRS and ESCRS
The primary measure of success of penetrating kerato-plasty (PKP) has generally been defined in terms of vi-sual acuity, graft clarity, and survival. These measuresreflect the 2 major problems with the surgery; that is,debilitating astigmatism and graft rejection.1–5
Secondary measures of success in PKP for keratoco-nus include astigmatism and the mean sphericalequivalent (SE). Olson et al.6 report the lowest meanastigmatism (2.76 diopters [D]) after PKP for keratoco-nus, with only 15% of eyes having astigmatism greaterthan 5.00 D. They also found that 77% of eyesachieved a corrected distance visual acuity (CDVA)of 6/7.5 or better. In a study by Javadi et al.3 of 164eyes that had PKP for keratoconus, the mean astigma-tismwas 3.4G 1.8 D and the mean spherical error was�0.61G 2.6 D. They found no correlation between the
SCRS and ESCRS
by Elsevier Inc.
results and trephination or suturing technique, sup-porting the later findings in a 2006 metaanalysis byFrost et al.7
Astigmatism as a measure of success appears to berelatively constant, with a reported mean value be-tween 2.75 D and 4.00 D.3,5–11 The management of sig-nificant postoperative astigmatism and anisometropiahas been most commonly treated with gas-permeablecontact lenses.12–15 Although lens designs have im-proved, many keratoconic patients have corneal trans-plantation because of their initial intolerance to contactlens wear.16 Refractive surgical procedures, such asarcuate incisions, resuturing, retrephination, wedgeexcisions, and Ruiz-type techniques, have been usedto treat post-graft astigmatism.17–24 In general, theycorrect various amounts of astigmatism but with
0886-3350/$ - see front matter
doi:10.1016/j.jcrs.2011.05.029

1885PRK WITH MMC AFTER PKP FOR KERATOCONUS
limited predictability and without allowing treatmentof anisometropia.
After the advent of photorefractive keratectomy(PRK), the technique was used to treat post-PKP re-fractive errors.25,26 The early results were variableand restricted by the development of the haze and re-gression commonly associated with significant correc-tions with all surface excimer laser procedures.27–29 Itis possible that the effect of haze was accentuated inthese cases because of the presence of already acti-vated keratocytes.30 This problem, however, can beameliorated, at least to some degree, by the use of post-operative mitomycin-C (MMC).30
Laser in situ keratomileusis (LASIK) has also beenused to treat post-PKP refractive errors again; how-ever, the results have been variable.31–39 The creationof the LASIK flap further weakens the wound andhas been suggested as a cause of unusual refractiveoutcomes and loss of CDVA.40 Intraoperative compli-cations leading to reduced visual outcomes have alsobeen reported.37,40,41
In this study, we evaluated the effects and overallsafety of PRKwithMMC 0.02% to treat residual refrac-tive errors in patients who had previous PKP for kera-toconus. We believe this is the largest published seriesto date of PRK after PKP.
PATIENTS AND METHODS
Eyes of consecutive patients who had PRK for refractive er-ror after previous PKP to treat keratoconus between 2006and 2008 were assessed in a retrospective chart analysis.Data collected included age, sex, manifest refraction, SErefraction, topographic cylinder, pachymetry, CDVA, anduncorrected distance visual acuity (UDVA) preoperativelyand 1, 3, 6, and 12 months postoperatively. The CDVA wasobtained through the phoropter or with the patient's glasses.Vector analysis was calculated at 12 months.
Inclusion criteria included a clear corneal graft for kerato-conus with no current signs of allograft rejection, suture re-moval before surgery, and a stable refraction for 3 months.Exclusion criteria were similar to those in all patients havingPRK and included pregnancy and ocular comorbidities thatmay affect vision or the healing process (eg, cataract or sig-nificant dry eye).
Submitted: January 9, 2011.Final revision submitted: April 6, 2011.Accepted: May 2, 2011.
From Vision Eye Institute (Hodge, Sutton, Lawless, Rogers),Chatswood, Sydney Medical School (Hodge, Sutton), Universityof Sydney, and Save Sight Institute (Sutton), Sydney MedicalSchool Foundation, Sydney University, Sydney, Australia.
Corresponding author: Chris Hodge, Vision Eye InstituteChatswood, NSW, Australia 2067. E-mail: [email protected].
J CATARACT REFRACT SURG -
The minimum gap between surgeries was 6 weeks. Theupper limit of treatment for the 2 laser units used in the studywas 6.00 D of cylinder; therefore, patients were divided into2 groups for data analysis. The low cylinder group com-prised patients with a refractive cylinder of 6.00 D or lowerand the high cylinder group, patientswith refractive cylinderabove 6.00 D. The patients were grouped to compartmental-ize the effect on the overall statistics of the expected under-correction and planned undercorrection in patients withpreoperative refractive cylinder above 6.00 D.
All refractive errors were reduced by 10% when pro-grammed for ablation because patients with PRK proceduresin conjunction with MMC have shown a tendency towardovercorrection and consecutive hyperopia. This is presum-ably due to MMC's attenuation of the wound-healingresponse.
The PRKwas performed using a LadarVision laser (AlconLaboratories, Inc.) or an Allegretto laser (Wavelight AG). Allsurgeries were performed by 1 of 3 surgeons (G.S., M.L.,C.R.). The protocol for treating astigmatism was to markthe patient's sclera before surgery with the patient seated.Marks were made with a medium Codman marker pen(Johnson & Johnson) at 0 degree and 180 degrees. Immedi-ately before the ablation with the LadarVision laser, the hor-izontal axis line on the unit was rotated to align with the 2limbal markings to ensure proper registration and ablationonto the cornea. The marking procedure before ablationwas the same in eyes having PRK with the Allegretto laser;at the ablation, the surgeon manipulated the patient's headto ensure the marks were located across the horizontalmedium. No additional procedures, for example arcuate T,were performed in eyes with a refractive cylinder above6.00 D. Immediately after the laser treatment, a sponge(Corneal Light Shield, BD Visitec, Beaver-Visitec Interna-tional) impregnated with MMC 0.02% was applied to alleyes for between 15 seconds and 60 seconds. The titrationof MMC application was dependent primarily on the levelof correction treated.
After surgery, a bandage contact lens (Focus Night &Day,Ciba Vision) was placed on the operated eye for 4 days.Patients received ciprofloxacin 0.3% (Ciloxan) 4 times dailyfor 1 week after surgery. Diclofenac sodium (VoltarenOphthalmic) was instilled the morning after surgery. Fluoro-metholone (FML) was started after contact lens removal andcontinued for 1 week 4 times per day.
Statistical analysis was performed using SPSS software(version 16.0, SPSS, Inc.). Student t tests were used to analyzeresults.
RESULTS
The study comprised 47 eyes of 41 consecutive pa-tients (25 in low cylinder group; 16 in high cylindergroup). The mean age of the 16 women and 25 menwas 40 years G 12 (SD) (range 22 to 67 years).Thirty-two eyes were treated with the LadarVisionlaser and 15 eyes with the Allegretto laser. The meanlength of MMC application was 40.1 G 14.8 seconds(median 30 seconds).
Refraction
Table 1 shows the preoperative and postoperativerefractive data by group. Although a final
VOL 37, OCTOBER 2011
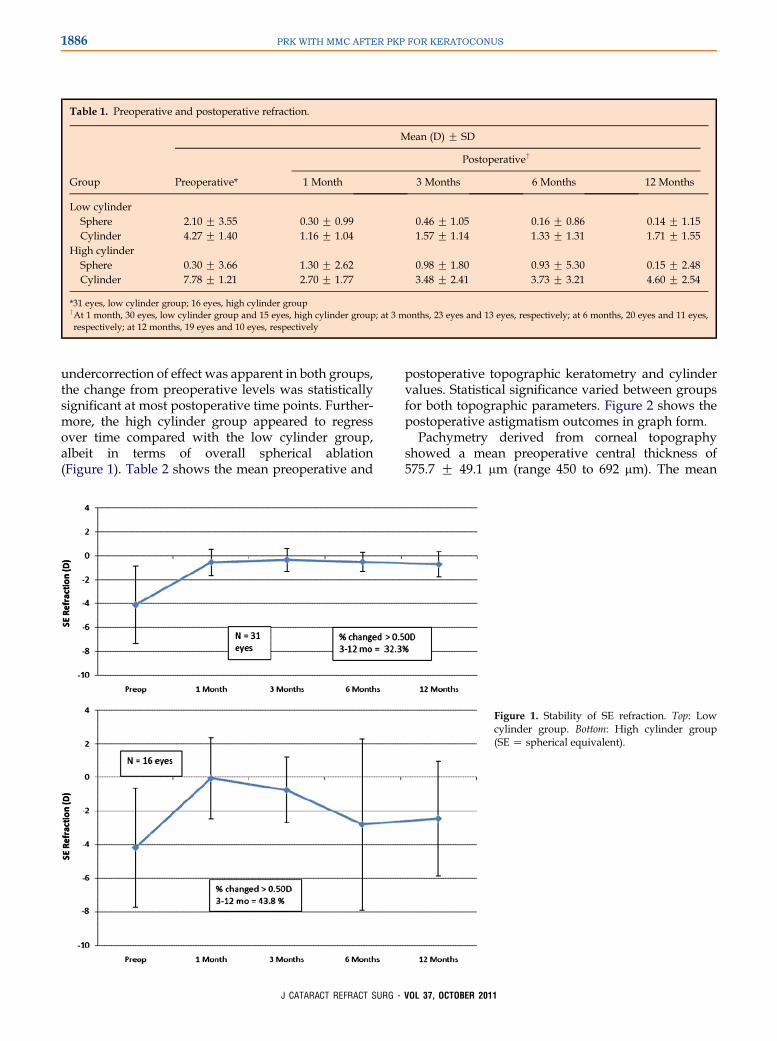
Table 1. Preoperative and postoperative refraction.
Group
Mean (D) G SD
Preoperative*
Postoperative†
1 Month 3 Months 6 Months 12 Months
Low cylinderSphere �2.10 G 3.55 0.30 G 0.99 0.46 G 1.05 0.16 G 0.86 0.14 G 1.15Cylinder �4.27 G 1.40 �1.16 G 1.04 �1.57 G 1.14 �1.33 G 1.31 �1.71 G 1.55
High cylinderSphere �0.30 G 3.66 1.30 G 2.62 0.98 G 1.80 �0.93 G 5.30 �0.15 G 2.48Cylinder �7.78 G 1.21 �2.70 G 1.77 �3.48 G 2.41 �3.73 G 3.21 �4.60 G 2.54
*31 eyes, low cylinder group; 16 eyes, high cylinder group†At 1 month, 30 eyes, low cylinder group and 15 eyes, high cylinder group; at 3 months, 23 eyes and 13 eyes, respectively; at 6 months, 20 eyes and 11 eyes,respectively; at 12 months, 19 eyes and 10 eyes, respectively
1886 PRK WITH MMC AFTER PKP FOR KERATOCONUS
undercorrection of effect was apparent in both groups,the change from preoperative levels was statisticallysignificant at most postoperative time points. Further-more, the high cylinder group appeared to regressover time compared with the low cylinder group,albeit in terms of overall spherical ablation(Figure 1). Table 2 shows the mean preoperative and
J CATARACT REFRACT SURG -
postoperative topographic keratometry and cylindervalues. Statistical significance varied between groupsfor both topographic parameters. Figure 2 shows thepostoperative astigmatism outcomes in graph form.
Pachymetry derived from corneal topographyshowed a mean preoperative central thickness of575.7 G 49.1 mm (range 450 to 692 mm). The mean
Figure 1. Stability of SE refraction. Top: Lowcylinder group. Bottom: High cylinder group(SE Z spherical equivalent).
VOL 37, OCTOBER 2011
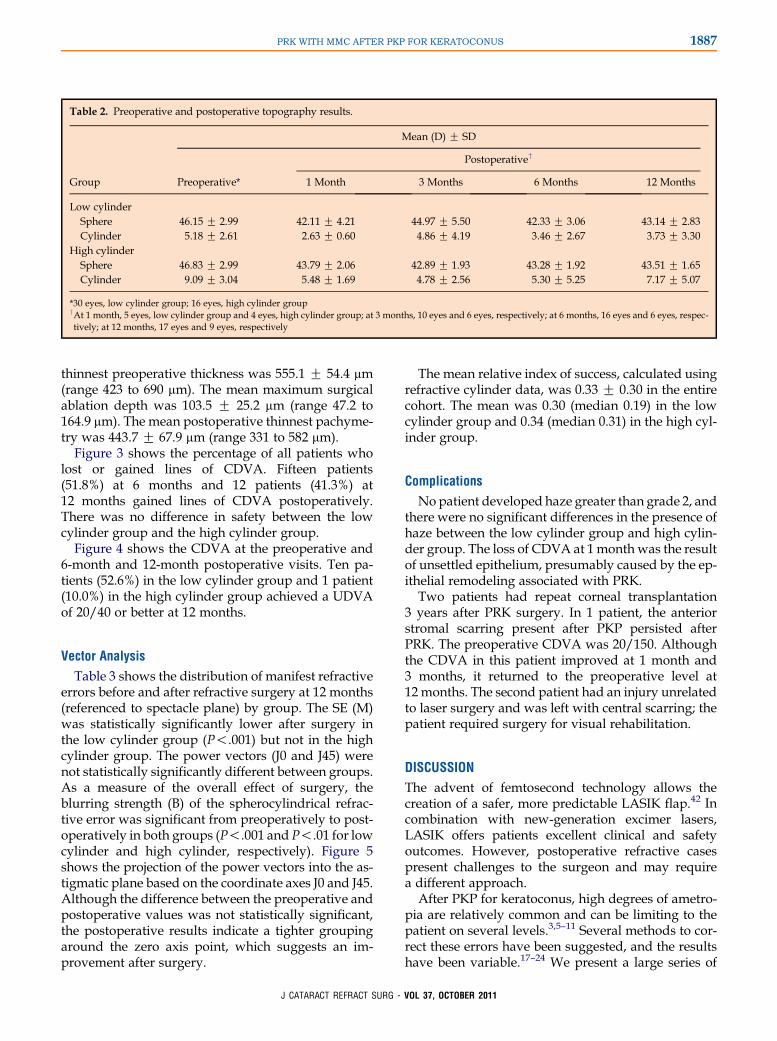
Table 2. Preoperative and postoperative topography results.
Group
Mean (D) G SD
Preoperative*
Postoperative†
1 Month 3 Months 6 Months 12 Months
Low cylinderSphere 46.15 G 2.99 42.11 G 4.21 44.97 G 5.50 42.33 G 3.06 43.14 G 2.83Cylinder 5.18 G 2.61 2.63 G 0.60 4.86 G 4.19 3.46 G 2.67 3.73 G 3.30
High cylinderSphere 46.83 G 2.99 43.79 G 2.06 42.89 G 1.93 43.28 G 1.92 43.51 G 1.65Cylinder 9.09 G 3.04 5.48 G 1.69 4.78 G 2.56 5.30 G 5.25 7.17 G 5.07
*30 eyes, low cylinder group; 16 eyes, high cylinder group†At 1 month, 5 eyes, low cylinder group and 4 eyes, high cylinder group; at 3 months, 10 eyes and 6 eyes, respectively; at 6 months, 16 eyes and 6 eyes, respec-tively; at 12 months, 17 eyes and 9 eyes, respectively
1887PRK WITH MMC AFTER PKP FOR KERATOCONUS
thinnest preoperative thickness was 555.1 G 54.4 mm(range 423 to 690 mm). The mean maximum surgicalablation depth was 103.5 G 25.2 mm (range 47.2 to164.9 mm). The mean postoperative thinnest pachyme-try was 443.7 G 67.9 mm (range 331 to 582 mm).Figure 3 shows the percentage of all patients who
lost or gained lines of CDVA. Fifteen patients(51.8%) at 6 months and 12 patients (41.3%) at12 months gained lines of CDVA postoperatively.There was no difference in safety between the lowcylinder group and the high cylinder group.
Figure 4 shows the CDVA at the preoperative and6-month and 12-month postoperative visits. Ten pa-tients (52.6%) in the low cylinder group and 1 patient(10.0%) in the high cylinder group achieved a UDVAof 20/40 or better at 12 months.
Vector Analysis
Table 3 shows the distribution of manifest refractiveerrors before and after refractive surgery at 12 months(referenced to spectacle plane) by group. The SE (M)was statistically significantly lower after surgery inthe low cylinder group (P!.001) but not in the highcylinder group. The power vectors (J0 and J45) werenot statistically significantly different between groups.As a measure of the overall effect of surgery, theblurring strength (B) of the spherocylindrical refrac-tive error was significant from preoperatively to post-operatively in both groups (P!.001 and P!.01 for lowcylinder and high cylinder, respectively). Figure 5shows the projection of the power vectors into the as-tigmatic plane based on the coordinate axes J0 and J45.Although the difference between the preoperative andpostoperative values was not statistically significant,the postoperative results indicate a tighter groupingaround the zero axis point, which suggests an im-provement after surgery.
J CATARACT REFRACT SURG -
The mean relative index of success, calculated usingrefractive cylinder data, was 0.33 G 0.30 in the entirecohort. The mean was 0.30 (median 0.19) in the lowcylinder group and 0.34 (median 0.31) in the high cyl-inder group.
Complications
Nopatient developed haze greater than grade 2, andthere were no significant differences in the presence ofhaze between the low cylinder group and high cylin-der group. The loss of CDVA at 1month was the resultof unsettled epithelium, presumably caused by the ep-ithelial remodeling associated with PRK.
Two patients had repeat corneal transplantation3 years after PRK surgery. In 1 patient, the anteriorstromal scarring present after PKP persisted afterPRK. The preoperative CDVA was 20/150. Althoughthe CDVA in this patient improved at 1 month and3 months, it returned to the preoperative level at12 months. The second patient had an injury unrelatedto laser surgery and was left with central scarring; thepatient required surgery for visual rehabilitation.
DISCUSSION
The advent of femtosecond technology allows thecreation of a safer, more predictable LASIK flap.42 Incombination with new-generation excimer lasers,LASIK offers patients excellent clinical and safetyoutcomes. However, postoperative refractive casespresent challenges to the surgeon and may requirea different approach.
After PKP for keratoconus, high degrees of ametro-pia are relatively common and can be limiting to thepatient on several levels.3,5–11 Several methods to cor-rect these errors have been suggested, and the resultshave been variable.17–24 We present a large series of
VOL 37, OCTOBER 2011
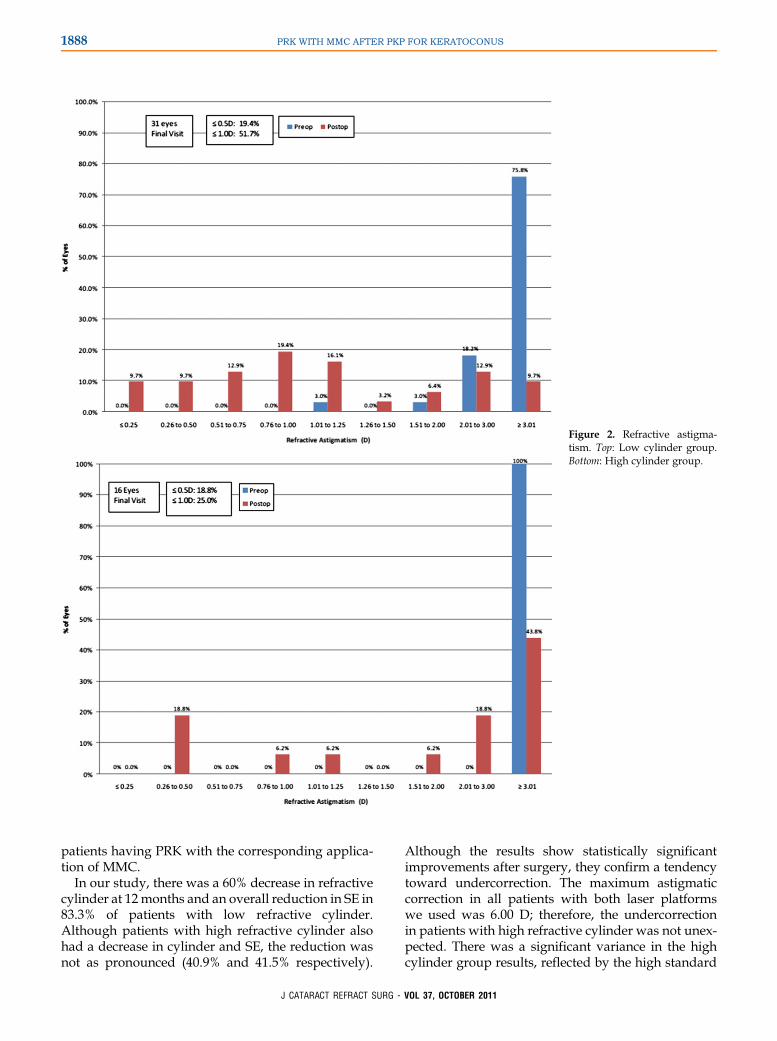
Figure 2. Refractive astigma-tism. Top: Low cylinder group.Bottom: High cylinder group.
1888 PRK WITH MMC AFTER PKP FOR KERATOCONUS
patients having PRK with the corresponding applica-tion of MMC.
In our study, there was a 60% decrease in refractivecylinder at 12months and an overall reduction in SE in83.3% of patients with low refractive cylinder.Although patients with high refractive cylinder alsohad a decrease in cylinder and SE, the reduction wasnot as pronounced (40.9% and 41.5% respectively).
J CATARACT REFRACT SURG -
Although the results show statistically significantimprovements after surgery, they confirm a tendencytoward undercorrection. The maximum astigmaticcorrection in all patients with both laser platformswe used was 6.00 D; therefore, the undercorrectionin patients with high refractive cylinder was not unex-pected. There was a significant variance in the highcylinder group results, reflected by the high standard
VOL 37, OCTOBER 2011
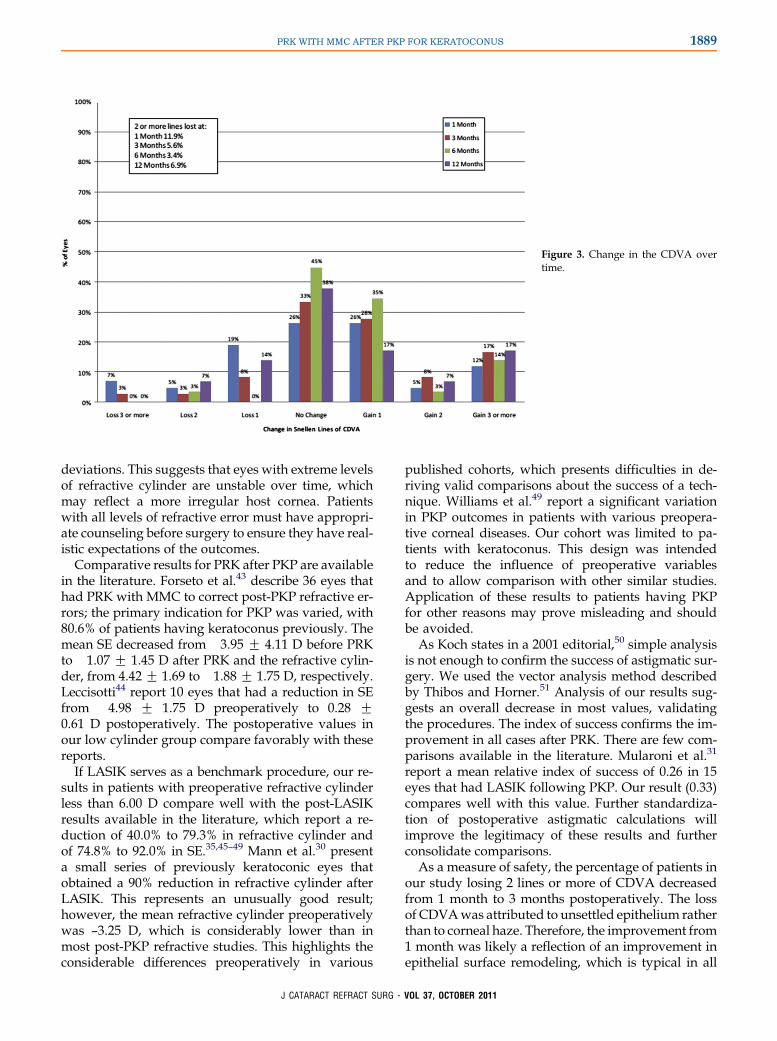
Figure 3. Change in the CDVA overtime.
1889PRK WITH MMC AFTER PKP FOR KERATOCONUS
deviations. This suggests that eyes with extreme levelsof refractive cylinder are unstable over time, whichmay reflect a more irregular host cornea. Patientswith all levels of refractive error must have appropri-ate counseling before surgery to ensure they have real-istic expectations of the outcomes.
Comparative results for PRK after PKP are availablein the literature. Forseto et al.43 describe 36 eyes thathad PRK with MMC to correct post-PKP refractive er-rors; the primary indication for PKP was varied, with80.6% of patients having keratoconus previously. Themean SE decreased from �3.95 G 4.11 D before PRKto �1.07 G 1.45 D after PRK and the refractive cylin-der, from 4.42 G 1.69 to �1.88 G 1.75 D, respectively.Leccisotti44 report 10 eyes that had a reduction in SEfrom �4.98 G 1.75 D preoperatively to 0.28 G0.61 D postoperatively. The postoperative values inour low cylinder group compare favorably with thesereports.
If LASIK serves as a benchmark procedure, our re-sults in patients with preoperative refractive cylinderless than 6.00 D compare well with the post-LASIKresults available in the literature, which report a re-duction of 40.0% to 79.3% in refractive cylinder andof 74.8% to 92.0% in SE.35,45–49 Mann et al.30 presenta small series of previously keratoconic eyes thatobtained a 90% reduction in refractive cylinder afterLASIK. This represents an unusually good result;however, the mean refractive cylinder preoperativelywas –3.25 D, which is considerably lower than inmost post-PKP refractive studies. This highlights theconsiderable differences preoperatively in various
J CATARACT REFRACT SURG -
published cohorts, which presents difficulties in de-riving valid comparisons about the success of a tech-nique. Williams et al.49 report a significant variationin PKP outcomes in patients with various preopera-tive corneal diseases. Our cohort was limited to pa-tients with keratoconus. This design was intendedto reduce the influence of preoperative variablesand to allow comparison with other similar studies.Application of these results to patients having PKPfor other reasons may prove misleading and shouldbe avoided.
As Koch states in a 2001 editorial,50 simple analysisis not enough to confirm the success of astigmatic sur-gery. We used the vector analysis method describedby Thibos and Horner.51 Analysis of our results sug-gests an overall decrease in most values, validatingthe procedures. The index of success confirms the im-provement in all cases after PRK. There are few com-parisons available in the literature. Mularoni et al.31
report a mean relative index of success of 0.26 in 15eyes that had LASIK following PKP. Our result (0.33)compares well with this value. Further standardiza-tion of postoperative astigmatic calculations willimprove the legitimacy of these results and furtherconsolidate comparisons.
As a measure of safety, the percentage of patients inour study losing 2 lines or more of CDVA decreasedfrom 1 month to 3 months postoperatively. The lossof CDVAwas attributed to unsettled epithelium ratherthan to corneal haze. Therefore, the improvement from1 month was likely a reflection of an improvement inepithelial surface remodeling, which is typical in all
VOL 37, OCTOBER 2011
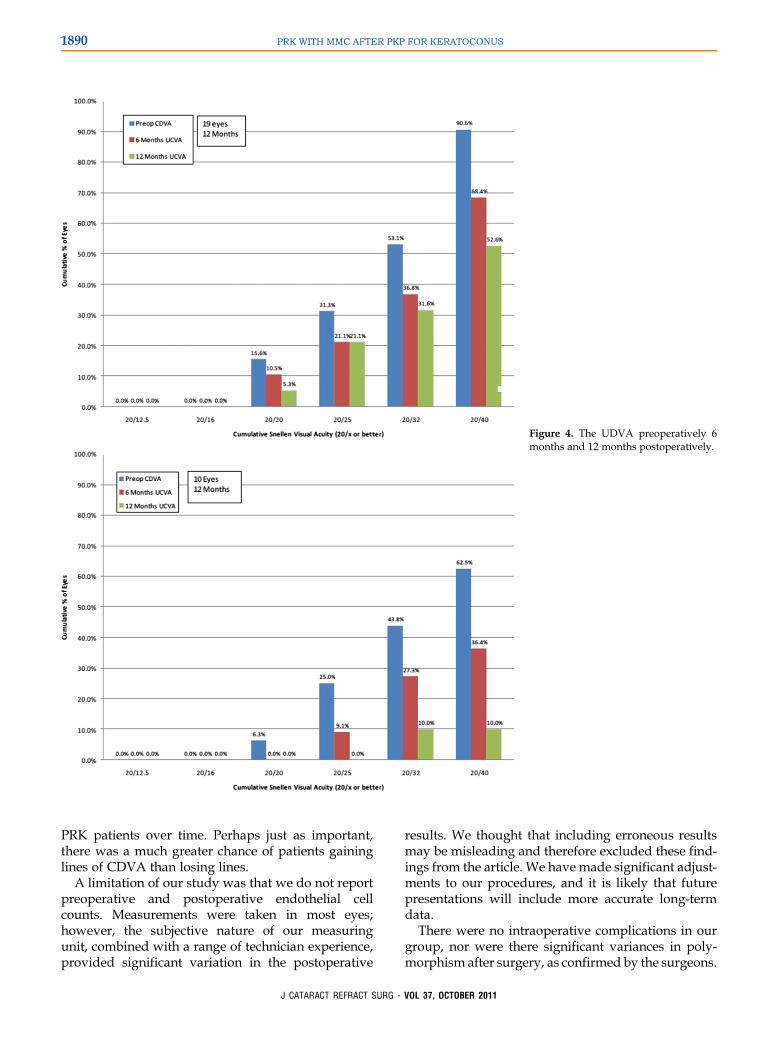
Figure 4. The UDVA preoperatively 6months and 12 months postoperatively.
1890 PRK WITH MMC AFTER PKP FOR KERATOCONUS
PRK patients over time. Perhaps just as important,there was a much greater chance of patients gaininglines of CDVA than losing lines.
A limitation of our study was that we do not reportpreoperative and postoperative endothelial cellcounts. Measurements were taken in most eyes;however, the subjective nature of our measuringunit, combined with a range of technician experience,provided significant variation in the postoperative
J CATARACT REFRACT SURG -
results. We thought that including erroneous resultsmay be misleading and therefore excluded these find-ings from the article. We have made significant adjust-ments to our procedures, and it is likely that futurepresentations will include more accurate long-termdata.
There were no intraoperative complications in ourgroup, nor were there significant variances in poly-morphism after surgery, as confirmed by the surgeons.
VOL 37, OCTOBER 2011
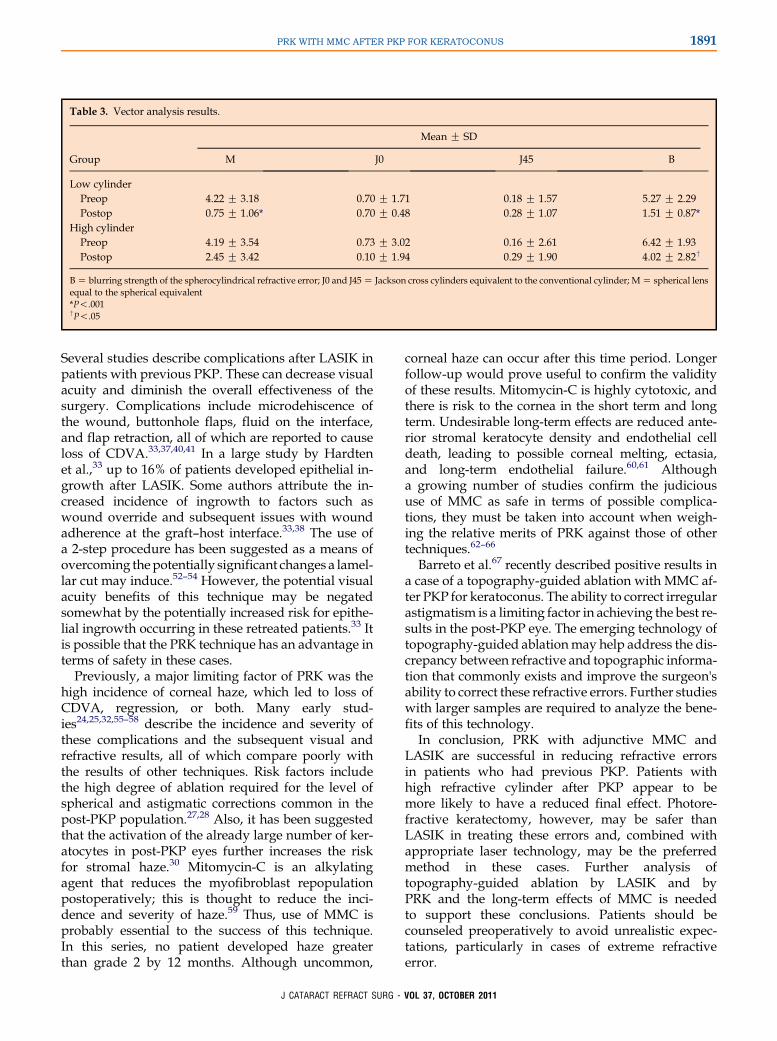
Table 3. Vector analysis results.
Group
Mean G SD
M J0 J45 B
Low cylinderPreop �4.22 G 3.18 �0.70 G 1.71 �0.18 G 1.57 5.27 G 2.29Postop �0.75 G 1.06* �0.70 G 0.48 �0.28 G 1.07 1.51 G 0.87*
High cylinderPreop �4.19 G 3.54 �0.73 G 3.02 0.16 G 2.61 6.42 G 1.93Postop �2.45 G 3.42 �0.10 G 1.94 0.29 G 1.90 4.02 G 2.82†
BZ blurring strength of the spherocylindrical refractive error; J0 and J45Z Jackson cross cylinders equivalent to the conventional cylinder; MZ spherical lensequal to the spherical equivalent*P!.001†P!.05
1891PRK WITH MMC AFTER PKP FOR KERATOCONUS
Several studies describe complications after LASIK inpatients with previous PKP. These can decrease visualacuity and diminish the overall effectiveness of thesurgery. Complications include microdehiscence ofthe wound, buttonhole flaps, fluid on the interface,and flap retraction, all of which are reported to causeloss of CDVA.33,37,40,41 In a large study by Hardtenet al.,33 up to 16% of patients developed epithelial in-growth after LASIK. Some authors attribute the in-creased incidence of ingrowth to factors such aswound override and subsequent issues with woundadherence at the graft–host interface.33,38 The use ofa 2-step procedure has been suggested as a means ofovercoming thepotentially significant changes a lamel-lar cut may induce.52–54 However, the potential visualacuity benefits of this technique may be negatedsomewhat by the potentially increased risk for epithe-lial ingrowth occurring in these retreated patients.33 Itis possible that the PRK technique has an advantage interms of safety in these cases.
Previously, a major limiting factor of PRK was thehigh incidence of corneal haze, which led to loss ofCDVA, regression, or both. Many early stud-ies24,25,32,55–58 describe the incidence and severity ofthese complications and the subsequent visual andrefractive results, all of which compare poorly withthe results of other techniques. Risk factors includethe high degree of ablation required for the level ofspherical and astigmatic corrections common in thepost-PKP population.27,28 Also, it has been suggestedthat the activation of the already large number of ker-atocytes in post-PKP eyes further increases the riskfor stromal haze.30 Mitomycin-C is an alkylatingagent that reduces the myofibroblast repopulationpostoperatively; this is thought to reduce the inci-dence and severity of haze.59 Thus, use of MMC isprobably essential to the success of this technique.In this series, no patient developed haze greaterthan grade 2 by 12 months. Although uncommon,
J CATARACT REFRACT SURG -
corneal haze can occur after this time period. Longerfollow-up would prove useful to confirm the validityof these results. Mitomycin-C is highly cytotoxic, andthere is risk to the cornea in the short term and longterm. Undesirable long-term effects are reduced ante-rior stromal keratocyte density and endothelial celldeath, leading to possible corneal melting, ectasia,and long-term endothelial failure.60,61 Althougha growing number of studies confirm the judicioususe of MMC as safe in terms of possible complica-tions, they must be taken into account when weigh-ing the relative merits of PRK against those of othertechniques.62–66
Barreto et al.67 recently described positive results ina case of a topography-guided ablation with MMC af-ter PKP for keratoconus. The ability to correct irregularastigmatism is a limiting factor in achieving the best re-sults in the post-PKP eye. The emerging technology oftopography-guided ablationmay help address the dis-crepancy between refractive and topographic informa-tion that commonly exists and improve the surgeon'sability to correct these refractive errors. Further studieswith larger samples are required to analyze the bene-fits of this technology.
In conclusion, PRK with adjunctive MMC andLASIK are successful in reducing refractive errorsin patients who had previous PKP. Patients withhigh refractive cylinder after PKP appear to bemore likely to have a reduced final effect. Photore-fractive keratectomy, however, may be safer thanLASIK in treating these errors and, combined withappropriate laser technology, may be the preferredmethod in these cases. Further analysis oftopography-guided ablation by LASIK and byPRK and the long-term effects of MMC is neededto support these conclusions. Patients should becounseled preoperatively to avoid unrealistic expec-tations, particularly in cases of extreme refractiveerror.
VOL 37, OCTOBER 2011
Figure 5. Projections of the vectors into theastigmatic plane based on the coordinateaxes J0 and J45 for the low refractive cylinderand high refractive cylinder groups Top:Low cylinder group. Bottom: High cylindergroup.
1892 PRK WITH MMC AFTER PKP FOR KERATOCONUS
REFERENCES1. Pramanik S, Musch DC, Sutphin JE, Farjo AA. Extended long-
term outcomes of penetrating keratoplasty for keratoconus.
Ophthalmology 2006; 113:1633–1638
2. Zadok D, Schwarts S, Marcovich A, Barkana Y, Morad Y,
Eting E, Avni I. Penetrating keratoplasty for keratoconus; long-
term results. Cornea 2005; 24:959–961
3. Javadi MA, Motlagh BF, Jafarinasab MR, Rabbanikhah Z,
Anissian A, Souri H, Yazdani S. Outcomes of penetrating kera-
toplasty in keratoconus. Cornea 2005; 24:941–946
4. Alvarez de Toledo J, de la Paz MF, Barraquer RI, Barraquer J.
Long-term progression of astigmatism after penetrating
J CATARACT REFRACT SURG -
keratoplasty for keratoconus; evidence of late recurrence. Cor-
nea 2003; 22:317–323
5. Lim L, Pesudovs K, Coster DJ. Penetrating keratoplasty for ker-
atoconus: visual outcome and success. Ophthalmology 2000;
107:1125–1131
6. Olson RJ, Pingree M, Ridges R, Lundergan ML, Alldredge C Jr,
Clinch TE. Penetrating keratoplasty for keratoconus: a long--
term review of results and complications. J Cataract Refract
Surg 2000; 26:987–991
7. Frost NA, Wu J, Lai TF, Coster DJ. A review of randomized
controlled trials of penetrating keratoplasty techniques.Ophthal-
mology 2006; 113:942–949
VOL 37, OCTOBER 2011
1893PRK WITH MMC AFTER PKP FOR KERATOCONUS
8. Jacobsen N, Højgaard-Olsen K. Promising results using the
Hanna Corneal Trephine System in penetrating keratoplasty.
Cornea 2006; 25:371–376
9. Lim L, Pesudovs K, Goggin M, Coster DJ. Late onset post-
keratoplasty astigmatism in patients with keratoconus. Br JOph-
thalmol 2004; 88:371–376. Available at: http://www.ncbi.nlm.
nih.gov/pmc/articles/PMC1772053/pdf/bjo08800371.pdf. Ac-
cessed June 11, 2011
10. Seitz B, Langenbucher A, Kus MM, K€uchle M, Naumann GOH.
Nonmechanical corneal trephination with the excimer laser im-
proves outcome after penetrating keratoplasty. Ophthalmology
1999; 106:1156–1164; ; discussion by WJ Stark 1164–1165
11. Doyle SJ, Harper C, Marcyniuk B, Ridgway AEA. Prediction of
refractive outcome in penetrating keratoplasty for keratoconus.
Cornea 1996; 15:441–445
12. Geerards AJM, Vreugdenhil W, Khazen A. Incidence of rigid
gas-permeable contact lens wear after keratoplasty for kerato-
conus. Eye Contact Lens 2006; 32:207–210
13. Gruenauer-Kloevekorn C, Kloevekorn-Fischer U, Duncker GI.
Contact lenses and special back surface design after penetrat-
ing keratoplasty to improve contact lens fit and visual outcome.
Br J Ophthalmol 2005; 89:1601–1608. Available at: http://www.
ncbi.nlm.nih.gov/pmc/articles/PMC1772965/pdf/bjo08901601.
pdf. Accessed June 11, 2011
14. Eggink FAGJ, Nuijts RMMA. A new technique for rigid gas per-
meable contact lens fitting following penetrating keratoplasty.
Acta Ophthalmol Scand 2001; 79:245–250. Available at: http://
onlinelibrary.wiley.com/doi/10.1034/j.1600-0420.2001.790307.
x/pdf. Accessed June 11, 2011
15. Mannis MJ, Zadnik K, Deutch D. Rigid contact lens wear in the
corneal transplant patient. CLAO J 1986; 12:39–42
16. Dana MR, Putz JL, Viana MAG, Sugar J, McMahon TT. Contact
lens failure in keratoconus management. Ophthalmology 1992;
99:1187–1192
17. Zuberbuhler B, Agrawal A, Gale R, Kipioti T, Gauba V, Noble B.
Modified Ruiz procedure for reducing high astigmatism after
penetrating keratoplasty. Cornea 2007; 26:1171–1177
18. Ezra DG, Hay-Smith G, Mearza A, Falcon MG. Corneal wedge
excision in the treatment of high astigmatism after penetrating
keratoplasty. Cornea 2007; 26:819–825
19. GhanemRC,AzarDT.Femtosecond-laserarcuatewedge-shaped
resection to correct high residual astigmatismafter penetrating ker-
atoplasty. J Cataract Refract Surg 2006; 32:1415–1419
20. Ilari L, Daya SM. Corneal wedge resection to treat progressive
keratoconus in the host cornea after penetrating keratoplasty.
J Cataract Refract Surg 2003; 29:395–401
21. Belmont SC, Lazzaro DR, Muller JW, Troutman RC. Combined
wedge resection and relaxing incisions for astigmatism after
penetrating keratoplasty. J Refract Surg 1995; 11:472–476
22. Lugo M, Donnenfeld ED, Arentsen JJ. Corneal wedge resection
for high astigmatism following penetrating keratoplasty.
Ophthalmic Surg 1987; 18:650–653
23. WhitehouseG,SuttonG, LawlessMA,RogersC.Refractive ker-
atoplasty for post-graft astigmatism. Aust N Z J Ophthalmol
1994; 22:243–247
24. Nordan LT, Binder PS, Kassar BS, Heitzmann J. Photorefractive
keratectomy to treat myopia and astigmatism after radial kera-
totomy and penetrating keratoplasty. J Cataract Refract Surg
1995; 21:268–273
25. JohnME,Martines E, Cvintal T, Mellor Filho A, Soter F, Barbosa
de Sousa MC, Boleyn KL, Ballew C. Photorefractive keratec-
tomy following penetrating keratoplasty. J Refract Corneal
Surg 1994; 10:S206–S210
26. Ali�o JL, Muftuoglu O, Ortiz D, Artola A, P�erez-Santonja JJ,
Castro de Luna G, Abu-Mustafa SK, Garcia MJ. Ten-year
J CATARACT REFRACT SURG -
follow-up of photorefractive keratectomy for myopia of more
than �6 diopters. Am J Ophthalmol 2008; 145:37–45
27. Kalski RS, SuttonG, Bin Y, LawlessMA, Rogers C. Comparison
of 5-mm and 6-mm ablation zones in photorefractive keratec-
tomy for myopia. J Refract Surg 1996; 12:61–67
28. Sutton G, Kalski RS, Lawless MA, Rogers C. Excimer retreat-
ment for scarring and regression after photorefractive keratec-
tomy for myopia. Br J Ophthalmol 1995; 79:756–759. Available
at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC505242/pdf/
brjopthal00020-0044.pdf. Accessed June 11, 2011
29. Solomon R, Donnenfeld ED, Thimons J, Stein J, Perry HD.
Hyperopic photorefractive keratectomy with adjunctive topical
mitomycin-C for refractive error after penetrating keratoplasty
for keratoconus. Eye Contact Lens 2004; 30:156–158
30. Mann E, Zaidman GW, Shukla S. Efficacy of nonsimultaneous
bilateral LASIK after nonsimultaneous bilateral penetrating ker-
atoplasty. Cornea 2006; 25:1053–1056
31. Mularoni A, Laffi GL, Bassein L, Tassinari G. Two-step LASIK
with topography-guided ablation to correct astigmatism after
penetrating keratoplasty. J Refract Surg 2006; 22:67–74
32. SchraepenP,VandorselaerT,TrauR,TassignonMJ.LASIKand
arcuate incisions for the treatment of post-penetrating kerato-
plasty anisometropia and/or astigmatism. Bull SocBelgeOphtal-
mol 2004; 292:19–25. Available at: http://www.ophthalmologia.
be/download.php?dof_idZ218. Accessed June 11, 2011
33. Hardten DR, Chittcharus A, LindstromRL. Long term analysis of
LASIK for the correction of refractive errors after penetrating ker-
atoplasty. Cornea 2004; 23:479–489
34. Preschel N, Hardten DR, LindstromRL. LASIK after penetrating
keratoplasty. Int Ophthalmol Clin 2000; 40(3):111–123
35. Webber SK, Lawless MA, Sutton GL, Rogers CM. LASIK for
post penetrating keratoplasty astigmatism and myopia. Br J
Ophthalmol 1999; 83:1013–1018. Available at: http://www.
ncbi.nlm.nih.gov/pmc/articles/PMC1723178/pdf/v083p01013.
pdf. Accessed June 11, 2011
36. Zaldivar R, Davidorf J, OscherowS. LASIK formyopia and astig-
matism after penetrating keratoplasty [letter]. J Refract Surg
1997; 13:501–502
37. HardtenDR, ChittcharusA, LindstromRL. Long-term analysis of
LASIK for the correction of refractive errors after penetrating ker-
atoplasty. Trans Am Ophthalmol Soc 2002; 100:143–150. dis-
cussion 150–152. Available at: http://www.aosonline.org/
xactions/2002/1545-6110_v100_p143.pdf. Accessed June
11, 2011
38. Chan CC, Rootman DS. Corneal lamellar flap retraction after
LASIK following penetrating keratoplasty. Cornea 2004; 23:
643–646
39. McGhee CNJ, Bryce IG. Natural history of central topographic
islands following excimer laser photorefractive keratectomy.
J Cataract Refract Surg 1996; 22:1151–1158
40. Sharma N, Sinha R, Vajpayee RB. Corneal lamellar flap retrac-
tion after LASIK following penetrating keratoplasty [letter].
Cornea 2006; 25:496
41. Solomon R, Donnenfeld ED, Perry HD, Nirankari VS. Post-
LASIK corneal flap displacement following penetrating kerato-
plasty for bullous keratopathy. Cornea 2005; 24:874–878
42. Sutton G, Hodge C. Accuracy and precision of LASIK flap thick-
ness using the IntraLase Femtosecond laser in 1000 consecu-
tive cases. J Refract Surg 2008; 24:802–806
43. Forseto AS, Marques JC, Nos�eW. Photorefractive keratectomy
with mitomycin C after penetrating and lamellar keratoplasty.
Cornea 2010; 29:1103–1108
44. Leccisotti A. Photorefractive keratectomy with mitomycin C after
deep anterior lamellar keratoplasty for keratoconus. Cornea
2008; 27:417–420
VOL 37, OCTOBER 2011
1894 PRK WITH MMC AFTER PKP FOR KERATOCONUS
45. Forseto AS, Francesconi CM, Nos�e RAM, Nos�eW. Laser in situ
keratomileusis to correct refractive errors after keratoplasty.
J Cataract Refract Surg 1999; 25:479–485
46. Koay PYP, McGhee CNJ, Weed KH, Craig JP. Laser in situ ker-
atomileusis for ametropia after penetrating keratoplasty.
J Refract Surg 2000; 16:140–147
47. Parisi A, Salchow DJ, Zirm ME, Stieldorf C. Laser in situ kerato-
mileusis after automated lamellar keratoplasty and penetrating
keratoplasty. J Cataract Refract Surg 1997; 23:1114–1118
48. Donnenfeld ED, KornsteinHS, AminA, SpeakerMD,Seedor JA,
Sforza PD, Landrio LM, Perry HD. Laser in situ keratomileusis
for correction of myopia and astigmatism after penetrating kera-
toplasty. Ophthalmology 1999; 106:1966–1974; discussion JH
Talamo, 1974–1975
49. Williams KA, Lowe MT, Bartlett CM, Kelly L, Coster DJ. The
Australian Corneal Graft Registry: 2007 Report Available at:
Adelaide, Australia, Flinders University Press, 2007. http://
dspace.flinders.edu.au/dspace/bitstream/2328/1723/3/FINAL%
20COMPILED%20REPORT%202007.pdf. Accessed June
11, 2011
50. Koch DD. How should we analyze data? [editorial] J Cataract
Refract Surg 2001; 27:1–3
51. Thibos LN, Horner D. Power vector analysis of the optical out-
come of refractive surgery. J Cataract Refract Surg 2001;
27:80–85
52. Cheng ACK, Lam DSC, Rao SK. Long-term analysis of LASIK
for the correction of refractive errors after penetrating kerato-
plasty [letter]. Cornea 2005; 24:891; reply by DR Hardten, A
Chittcharus, RL Lindstrom, 891–892
53. Busin M, Zambianchi L, Garzione F, Maucione V, Rossi S.
Two-stage laser in situ keratomileusis to correct refractive er-
rors after penetrating keratoplasty. J Refract Surg 2003;
19:301–308
54. Walker NJ, Apel AJG. Effect of hinged lamellar keratotomy on
post-keratoplasty astigmatism and vision. Clin Exp Ophthalmol
2004; 32:147–153
55. Amm M, Duncker GIW, Schr€oder E. Excimer laser correction of
high astigmatism after keratoplasty. J Cataract Refract Surg
1996; 22:313–317
56. ChanW-K, Hunt KE, GlasgowBJ,Mondino BJ. Corneal scarring
after photorefractive keratectomy in a penetrating keratoplasty.
Am J Ophthalmol 1996; 121:570–571
57. Lazzaro DR, Haight DH, Belmont SC, Gibralter RP,
Aslanides IM, Odrich MG. Excimer laser keratectomy for astig-
matism occurring after penetrating keratoplasty. Ophthalmology
1996; 103:458–464
58. Tuunanen TH, Ruusuvaara PJ, Uusitalo RJ, Tervo TM. Photo-
astigmatic keratectomy for correction of astigmatism in corneal
grafts. Cornea 1997; 16:48–53
J CATARACT REFRACT SURG -
59. Teus MA, de Benito-Llopis L, Ali�o JL. Mitomycin C in corneal re-
fractive surgery. Surv Ophthalmol 2009; 54:487–502
60. Nassiri N, Farahangiz S, Rahnavardi M, Rahmani L, Nassiri N.
Corneal endothelial cell injury induced by mitomycin-C in photo-
refractive keratectomy: nonrandomized controlled trial.
J Cataract Refract Surg 2008; 34:902–908
61. Roh DS, Cook AL, Rhee SS, Joshi A, Kowalski R, Dhaliwal DK,
Funderburgh JL. DNA cross-linking, double strand breaks, and
apoptosis in corneal endothelial cells after a single exposure to
mitomycin C. Invest Ophthalmol Vis Sci 2008; 49:4837–4843.
Available at: http://www.iovs.org/content/49/11/4837.full.pdf.
Accessed June 11, 2011
62. Panda A, Pe’er J, Aggarwal A, Das H, Kumar A, Mohan S. Effect
of topicalmitomycinCon corneal endothelium.AmJOphthalmol
2008; 145:635–638
63. Midena E, Gambato C, Miotto S, Cortese M, Salvi R,
Ghirlando A. Long-term effects on corneal keratocytes of
mitomycin C during photorefractive keratectomy: a randomized
contralateral eye confocal microscopy study. J Refract Surg
2007; 23:S1011–S1014
64. Goldsberry DH, Epstein RJ, Majmudar PA, Epstein RH,
Dennis RF, Holley G, Edelhauser HF. Effect of mitomycin C on
the corneal endothelium when used for corneal subepithelial
haze prophylaxis following photorefractive keratectomy.
J Refract Surg 2007; 23:724–727
65. de Beneto-Llopis L, Teus MA, Ortega M. Effect of mitomycin-C
on the corneal endothelium during excimer laser surface abla-
tion. J Cataract Refract Surg 2007; 33:1009–1013
66. Zhao LQ, Wei RL, Ma XY, Zhu H. Effect of intraoperative
mitomycin-C on healthy corneal endothelium after laser-
assisted subepithelial keratectomy. J Cataract Refract Surg
2008; 34:1715–1719
67. Barreto J Jr, Netto MV, Reis A, Nakano M, Alves MR,
Bechara SJ. Topography-guided (NIDEK customized aspheric
treatent zone) photorefractive keratectomy with mitomycin C
after penetrating keratoplasty for keratoconus: case report.
J Refract Surg 2009; 25:S131–S135
VOL
37, OCTOBER 2011First author:Chris Hodge, BAppSc
Vision Eye Institute, Chatswood,Sydney, Australia