pharmacy informatics workgroup 1 a pharmacy technician externship program lezlie cohn-oswald, cpht....
TRANSCRIPT
Pharmacy Informatics Workgroup 1
A PHARMACY TECHNICIAN EXTERNSHIP PROGRAM
Lezlie Cohn-Oswald, CPhT.Clinical Pharmacy Technician
Associate Director,
Pharmacy Technician Externship Program
Salt Lake City VA Health Care Center
Pharmacy Informatics Workgroup
2
PRESENTATION OBJECTIVES
Define what a Pharmacy Technician Externship Program entails.
How a Pharmacy Technician Externship Program can help in training, recruitment and job satisfaction of pharmacy technicians.
Explain what contents should be part of a
Pharmacy Technician Externship Program.

Pharmacy Informatics Workgroup
3
DEFINITIONS
> INTERNSHIP: *Any official or formal program to provide practical experience for beginners in an occupation or profession.
> EXTERNSHIP: *A required period of supervised practice done off campus or away from one's affiliated institution.
*Dictionary.com
Pharmacy Informatics Workgroup
4
TECH EXTERN PROGRAM OBJECTIVES
> To afford pharmacy technician students an opportunity to receive a well-rounded, practical experience in their chosen field.
> To train future technicians for possible positions within the VA.
> To train our current pharmacy technician workforce how to be mentors and educators.
Pharmacy Informatics Workgroup
5
THE “WHY”
> Inpatient/Outpatient settings
> Opportunity to help the profession
> State Pharmacy Technician Licensure
- Utah = 180 hours total practical (extern) hours
> Job opportunities
- contract positions to FTEs
Pharmacy Informatics Workgroup
6
PROGRAM SET-UP
> Contact State Board of Pharmacy
-State laws regulating pharmacy
technicians
- licensure
- registration
- state certification
- permit
Pharmacy Informatics Workgroup
7
PROGRAM SET-UP
> School programs
- Must be accredited program recognized
by U.S. Department of Education or the
Council for Higher Education Accreditation
(CHEA)
- Quantity of students in facility
“limit quantity for quality”
- Keep school contact list
Pharmacy Informatics Workgroup
8
PROGRAM SET-UP (cont’)
> Academics Affiliate Office paperwork
- MOU(Memorandum Of Understanding)
contract (VA Form 10-0094g)
- Trainee Qualifications and Credentials
Verification Letter (TQCVL) (SAMPLE 1)
- Trainee Registration VA Form10-0410
Pharmacy Informatics Workgroup
9
TRAINEE QUALIFICATIONS AND CREDENTIALS (SAMPLE 1) VERIFICATION LETTER (TQCVL)(date)(name of medical center director (station #)(address)___________________________Dear (medical center director):1. I certify that the information identified below has been verified for these trainees who are scheduled to receive all or part of their clinical training at the VA Salt Lake City Health Care System:
Social Security Discipline of Study Degree Level orTrainee Name(s) Number (SSN) or Specialty Post Graduate Year 2. In addition, I certify that these trainees:
a. Are enrolled in the designated training program. b. Have satisfactory physical and mental health necessary to perform the duties of the
proposed assignment, including appropriate tuberculin testing and hepatitis B vaccination (or waiver).
c. Have had verification of educational credentials as required by the admission criteria of the academic program.
d. Have had verification of current license(s) through the appropriate state licensing board(s) as required by the academic program.
e. Have provided letters of reference as appropriate to the admissions criteria of the academic program.
f. Have appropriate citizenship documents (e.g., current, unexpired visa; evidence of naturalization; or a permanent U.S. immigrant status) if non-United States (U.S.) citizens.
g. Have Educational Commission on Foreign Medical Graduates (ECFMG) certificates if graduates of international medical schools.3. I will notify the VASLCHCS within 72 hours of changes in the status of individual trainees (i.e., academic probation, remediation, early withdrawal from the program) or adverse action that impacts on the trainee appointment.4. I certify that all appropriate documents pertaining to the listed trainees are maintained on file and available to the VASLCHCS for review if requested. ____________________________________ (Complete Name, Title, Affiliate/Institution, Training Program w/ signature line)Approve / Disapprove Comments:____________________(name of chief of staff) & (name of medical center director) separate (date) and (signature line) Approve / Disapprove Comments:____________________
Pharmacy Informatics Workgroup
10
PROGRAM SET-UP (cont’)
> Human Resources paperwork - WOC checklist (Appendix 1B)
- Trainee Information Sheet (sample 2)
- OP-306 Declaration for Federal
Employment
- SF-61 Appointment Affidavit
Pharmacy Informatics Workgroup
11
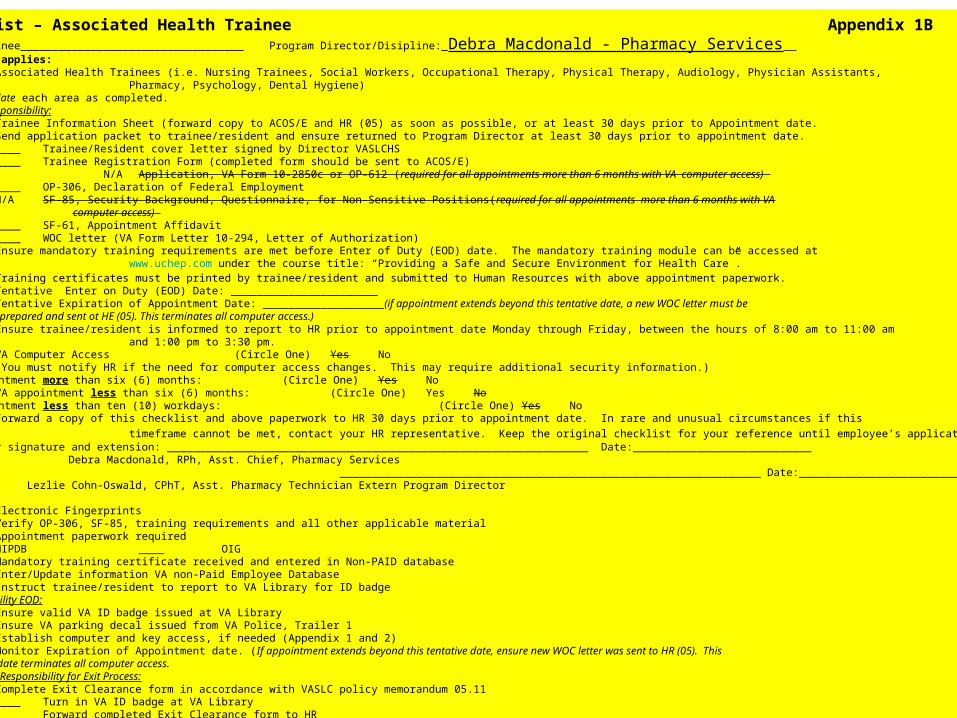
WOC Checklist – Associated Health Trainee Appendix 1BName of WOC Trainee___________________________________ Program Director/Disipline:_Debra Macdonald - Pharmacy Services Check area that applies:
_X__ Associated Health Trainees (i.e. Nursing Trainees, Social Workers, Occupational Therapy, Physical Therapy, Audiology, Physician Assistants, Pharmacy, Psychology, Dental Hygiene)Below, initial and date each area as completed.Program Director Responsibility:
____ Trainee Information Sheet (forward copy to ACOS/E and HR (05) as soon as possible, or at least 30 days prior to Appointment date.____ Send application packet to trainee/resident and ensure returned to Program Director at least 30 days prior to appointment date.
____ Trainee/Resident cover letter signed by Director VASLCHS____ Trainee Registration Form (completed form should be sent to ACOS/E)
N/A Application, VA Form 10-2850c or OP-612 (required for all appointments more than 6 months with VA computer access) ____ OP-306, Declaration of Federal EmploymentN/A SF-85, Security Background, Questionnaire, for Non-Sensitive Positions(required for all appointments more than 6 months with VA
computer access) ____ SF-61, Appointment Affidavit____ WOC letter (VA Form Letter 10-294, Letter of Authorization)
____ Ensure mandatory training requirements are met before Enter of Duty (EOD) date. The mandatory training module can be accessed at www.uchep.com under the course title: “Providing a Safe and Secure Environment for Health Care”.
____ Training certificates must be printed by trainee/resident and submitted to Human Resources with above appointment paperwork.____ Tentative Enter on Duty (EOD) Date: ___________________________ Tentative Expiration of Appointment Date: ___________________(if appointment extends beyond this tentative date, a new WOC letter must be
prepared and sent ot HE (05). This terminates all computer access.)____ Ensure trainee/resident is informed to report to HR prior to appointment date Monday through Friday, between the hours of 8:00 am to 11:00 am
and 1:00 pm to 3:30 pm.N/A VA Computer Access (Circle One) Yes No
(You must notify HR if the need for computer access changes. This may require additional security information.)N/A VA appointment more than six (6) months: (Circle One) Yes No
____ VA appointment less than six (6) months: (Circle One) Yes NoN/A VA appointment less than ten (10) workdays: (Circle One) Yes No
____ Forward a copy of this checklist and above paperwork to HR 30 days prior to appointment date. In rare and unusual circumstances if this
timeframe cannot be met, contact your HR representative. Keep the original checklist for your reference until employee’s application terminates. Program Director signature and extension: __________________________________________________________________ Date:____________________________
Debra Macdonald, RPh, Asst. Chief, Pharmacy Services __________________________________________________________________ Date:_____________________________ Lezlie Cohn-Oswald, CPhT, Asst. Pharmacy Technician Extern Program Director HR Responsibility:
____ Electronic Fingerprints____ Verify OP-306, SF-85, training requirements and all other applicable material____ Appointment paperwork required____ HIPDB ____ OIG____ Mandatory training certificate received and entered in Non-PAID database____ Enter/Update information VA non-Paid Employee Database____ Instruct trainee/resident to report to VA Library for ID badge
Supervisor Responsibility EOD:____ Ensure valid VA ID badge issued at VA Library____ Ensure VA parking decal issued from VA Police, Trailer 1____ Establish computer and key access, if needed (Appendix 1 and 2)____ Monitor Expiration of Appointment date. (If appointment extends beyond this tentative date, ensure new WOC letter was sent to HR (05). This
date terminates all computer access.Supervisor Responsibility for Exit Process:____ Complete Exit Clearance form in accordance with VASLC policy memorandum 05.11
____ Turn in VA ID badge at VA Library____ Forward completed Exit Clearance form to HR
Pharmacy Informatics Workgroup
12
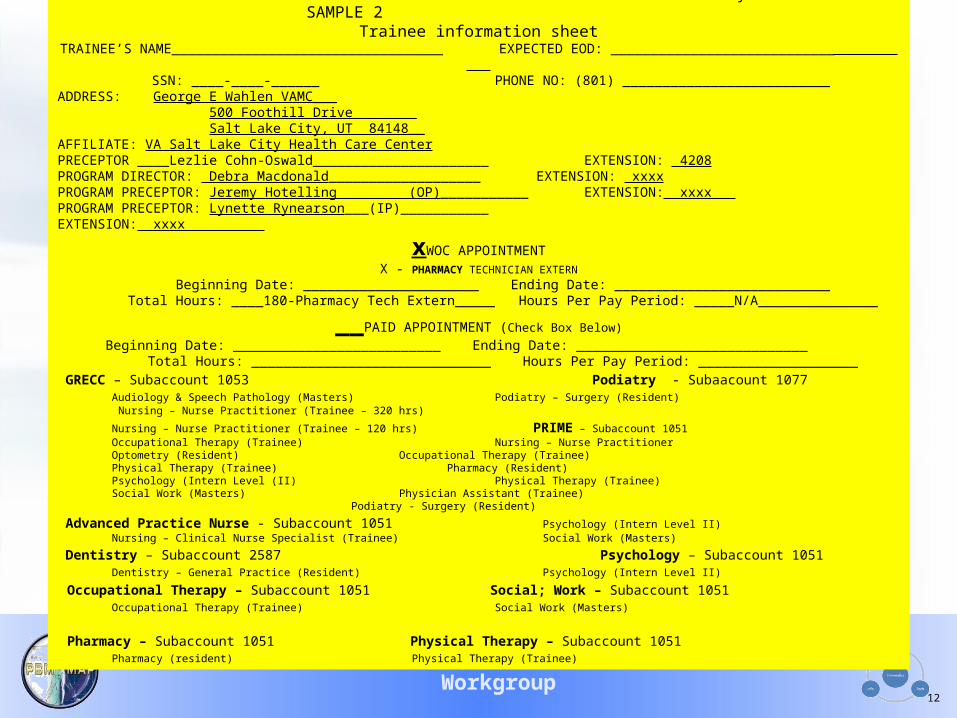
Va salt lake city hcs SAMPLE 2Trainee information sheet
TRAINEE’S NAME__________________________________ EXPECTED EOD: ____________________________ SSN: ____-____-______ PHONE NO: (801) __________________________
ADDRESS: George E Wahlen VAMC___ 500 Foothill Drive________ Salt Lake City, UT 84148__ AFFILIATE: VA Salt Lake City Health Care CenterPRECEPTOR ____Lezlie Cohn-Oswald______________________ EXTENSION: 4208PROGRAM DIRECTOR: Debra Macdonald___________________ EXTENSION: xxxxPROGRAM PRECEPTOR: Jeremy Hotelling (OP)___________ EXTENSION: xxxx PROGRAM PRECEPTOR: Lynette Rynearson___(IP)___________ EXTENSION: xxxx
xWOC APPOINTMENTX - PHARMACY TECHNICIAN EXTERN
Beginning Date: ______________________ Ending Date: ___________________________Total Hours: ____180-Pharmacy Tech Extern_____ Hours Per Pay Period: _____N/A_______________
__PAID APPOINTMENT (Check Box Below)
Beginning Date: __________________________ Ending Date: _____________________________Total Hours: ______________________________ Hours Per Pay Period: ____________________
GRECC – Subaccount 1053 Podiatry - Subaacount 1077 Audiology & Speech Pathology (Masters) Podiatry – Surgery (Resident) Nursing – Nurse Practitioner (Trainee – 320 hrs)
Nursing – Nurse Practitioner (Trainee – 120 hrs) PRIME – Subaccount 1051 Occupational Therapy (Trainee) Nursing – Nurse Practitioner Optometry (Resident) Occupational Therapy (Trainee) Physical Therapy (Trainee) Pharmacy (Resident) Psychology (Intern Level (II) Physical Therapy (Trainee) Social Work (Masters) Physician Assistant (Trainee)
Podiatry - Surgery (Resident)
Advanced Practice Nurse - Subaccount 1051 Psychology (Intern Level II) Nursing – Clinical Nurse Specialist (Trainee) Social Work (Masters)
Dentistry – Subaccount 2587 Psychology – Subaccount 1051 Dentistry – General Practice (Resident) Psychology (Intern Level II)
Occupational Therapy – Subaccount 1051 Social; Work – Subaccount 1051 Occupational Therapy (Trainee) Social Work (Masters)
Pharmacy – Subaccount 1051 Physical Therapy – Subaccount 1051 Pharmacy (resident) Physical Therapy (Trainee)
Pharmacy Informatics Workgroup
13
PROGRAM SET-UP (cont’)
> Human Resources paperwork (cont’)
- VA Form 0711 Request for Personal
Identification Verification Card
- WOC Letter of Agreement
(VA Form Letter 10-294, Letter of
Authorization )
- VA Mandatory Training certificates
Pharmacy Informatics Workgroup
14
PROGRAM SET-UP (cont’)
> VA/Contract technician coordination
- interview staff
- set parameters of shadowing
- preceptors
> Pharmacist coordination
- supervisors
- licensure
Pharmacy Informatics Workgroup
15
STUDENT INTERVIEW
> Contacted by school
> Make contact with student
> Interview student
Pharmacy Informatics Workgroup
16
STUDENT INTERVIEW (cont’)
> Interviewing a prospective student will help to assure you have the right student for your program as well as the right program for the student.
> Interview:
- Why this facility?
- What kind of schedule are you looking for?
- Expectation(s) from this rotation?
- Future goals?
“TREAT YOUR EXTERNSHIP LIKE A JOB INTERVIEW”
> Fill out HR paperwork, give station map & information for online mandatory training to student.
Pharmacy Informatics Workgroup
17
STUDENT INTERVIEW (cont’)
> Set Schedules
- Make calendar for self & student
- Pharmacy Technician Externship
Time Agreement (Sample 3)
- both parties sign agreement with
copy to student & copy to student
file
Pharmacy Informatics Workgroup
18
PHARMACY TECHNICIAN EXTERNSHIP TIME AGREEMENT
180 hours total time needed90 hours Outpatient 90 hours Inpatient
OTHER
__60 days = @ 3hours/day = 180 hours (30 days in each pharmacy)
__45 days = @ 4hours/day = 180 hours (22.5 days in each pharmacy)
__30 days = @ 6hours/day = 180 hours (15 days in each pharmacy)
__22.5 days = @ 8hours/day = 180 hours (11.25 days in each pharmacy)
Student Name (print)
(signature) Date ________________________
Preceptor Name (print)
(signature) Date ________________________
SAMPLE 3
Pharmacy Informatics Workgroup
19
PROGRAM CONTENT
> Orientation to Pharmacy Service - Administration
- Clinical
- Outpatient
- Inpatient
- Customer information
- Medical Center layout
- Physician Order Entry (POE) facility/organization
Pharmacy Informatics Workgroup
20
PROGRAM CONTENT (cont’)
> Concentrated Learning Experience: Outpatient-
- In/Out Window
- Pharmacy automation
- Window & mail fill areas
- Prescription tracking
- Mail-out area*unable to have computer access as WOC = unable to answer phones

Pharmacy Informatics Workgroup
21
PROGRAM CONTENT(cont’)
> Concentrated Learning Experience: Inpatient
- Bar code labeling - Unit Dose fills
- Ward inspections - *IV admixtures
- Crash cart fill (USP Chapter <797> review)
- Pharmacy automation
- Automatic replenishment
*may be unable to receive hands-on training, but able to review ongoing IV process
Pharmacy Informatics Workgroup
22
PROGRAM CONTENT(cont’)
> Concentrated Learning Experience:
Duties occurring in both pharmacies: - Waste disposal - Medication dispensing
- Outdate inspections
Not rotated through area; are given overview:
- Inventory management
- Controlled substances
Pharmacy Informatics Workgroup
23
PROGRAM GOALS
> Documentation/Communication
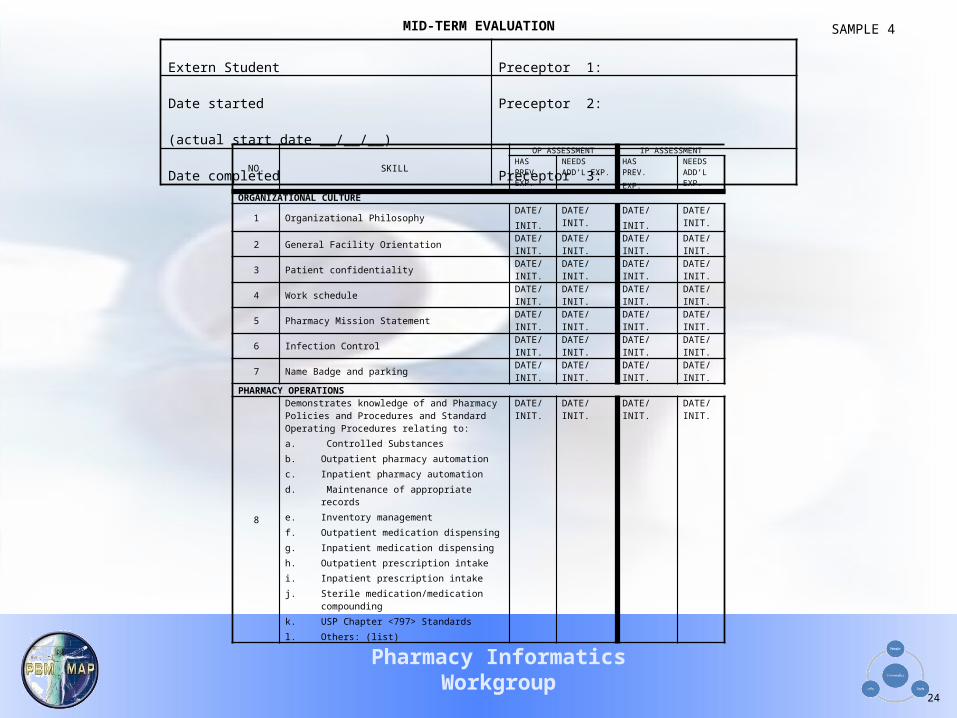
- Mid-term evaluation (sample 4)
(45 hour & 135 hour marks)
> Student Program Director contacted with update of student progress
Pharmacy Informatics Workgroup
24
Extern Student Preceptor 1:
Date started (actual start date __/__/__) Preceptor 2:
Date completed Preceptor 3:
NO. SKILL
OP ASSESSMENT IP ASSESSMENTHASPREV.EXP.
NEEDS ADD’L EXP.
HASPREV.
EXP.
NEEDS ADD’L EXP.
ORGANIZATIONAL CULTURE
1 Organizational PhilosophyDATE/
INIT.
DATE/ INIT. DATE/
INIT.
DATE/ INIT.
2 General Facility OrientationDATE/ INIT.
DATE/ INIT. DATE/ INIT. DATE/ INIT.
3 Patient confidentialityDATE/ INIT.
DATE/ INIT. DATE/ INIT. DATE/ INIT.
4 Work scheduleDATE/ INIT.
DATE/ INIT. DATE/ INIT. DATE/ INIT.
5 Pharmacy Mission StatementDATE/ INIT.
DATE/ INIT. DATE/ INIT. DATE/ INIT.
6 Infection ControlDATE/ INIT.
DATE/ INIT. DATE/ INIT. DATE/ INIT.
7 Name Badge and parkingDATE/ INIT.
DATE/ INIT. DATE/ INIT. DATE/ INIT.
PHARMACY OPERATIONS
8
Demonstrates knowledge of and Pharmacy Policies and Procedures and Standard Operating Procedures relating to:
a. Controlled Substances
b. Outpatient pharmacy automation
c. Inpatient pharmacy automation
d. Maintenance of appropriate records
e. Inventory management
f. Outpatient medication dispensing
g. Inpatient medication dispensing
h. Outpatient prescription intake
i. Inpatient prescription intake
j. Sterile medication/medication compounding
k. USP Chapter <797> Standards
l. Others: (list)
DATE/ INIT.
DATE/ INIT. DATE/ INIT. DATE/ INIT.
MID-TERM EVALUATION SAMPLE 4
Pharmacy Informatics Workgroup
25
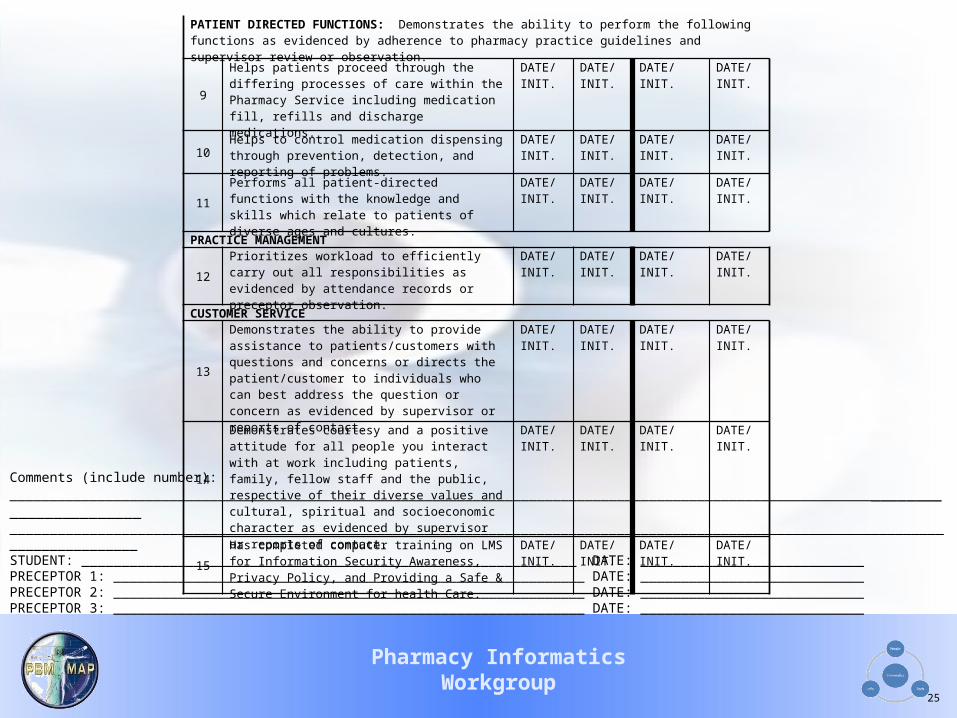
Comments (include number):________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ STUDENT: ______________________________________________________________ DATE: ____________________________PRECEPTOR 1: ___________________________________________________________ DATE: ____________________________PRECEPTOR 2: ___________________________________________________________ DATE: ____________________________PRECEPTOR 3: ___________________________________________________________ DATE: ____________________________
PATIENT DIRECTED FUNCTIONS: Demonstrates the ability to perform the following functions as evidenced by adherence to pharmacy practice guidelines and supervisor review or observation.
9Helps patients proceed through the differing processes of care within the Pharmacy Service including medication fill, refills and discharge medications.
DATE/ INIT.
DATE/ INIT.
DATE/ INIT. DATE/ INIT.
10 Helps to control medication dispensing through prevention, detection, and reporting of problems.
DATE/ INIT.
DATE/ INIT.
DATE/ INIT. DATE/ INIT.
11Performs all patient-directed functions with the knowledge and skills which relate to patients of diverse ages and cultures.
DATE/ INIT.
DATE/ INIT.
DATE/ INIT. DATE/ INIT.
PRACTICE MANAGEMENT
12Prioritizes workload to efficiently carry out all responsibilities as evidenced by attendance records or preceptor observation.
DATE/ INIT.
DATE/ INIT.
DATE/ INIT. DATE/ INIT.
CUSTOMER SERVICE
13
Demonstrates the ability to provide assistance to patients/customers with questions and concerns or directs the patient/customer to individuals who can best address the question or concern as evidenced by supervisor or reports of contact.
DATE/ INIT.
DATE/ INIT.
DATE/ INIT. DATE/ INIT.
14
Demonstrates courtesy and a positive attitude for all people you interact with at work including patients, family, fellow staff and the public, respective of their diverse values and cultural, spiritual and socioeconomic character as evidenced by supervisor or reports of contact.
DATE/INIT.
DATE/ INIT.
DATE/INIT. DATE/ INIT.
15Has completed computer training on LMS for Information Security Awareness, Privacy Policy, and Providing a Safe & Secure Environment for health Care.
DATE/ INIT.
DATE/ INIT.
DATE/ INIT. DATE/ INIT.
Pharmacy Informatics Workgroup
26
PROGRAM GOALS (cont’)
> Student(s) unable to progress through program:
> Review you facility’s policy for dismissal (Medical Center Trainee Orientation, Dismissal and Termination Policy)
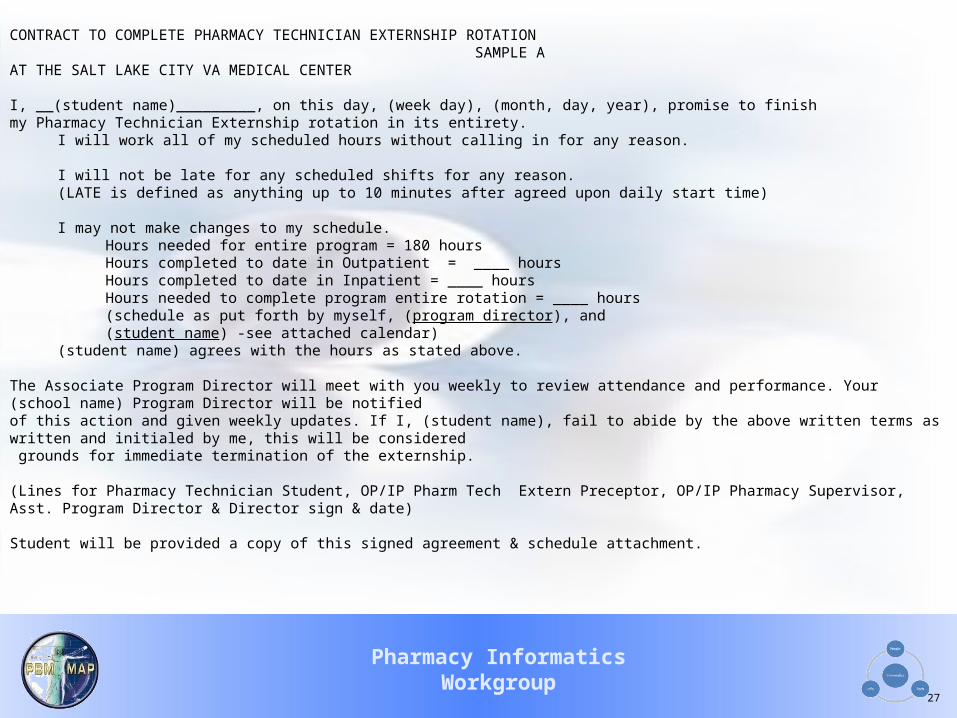
> Contract for program completion (Sample A)
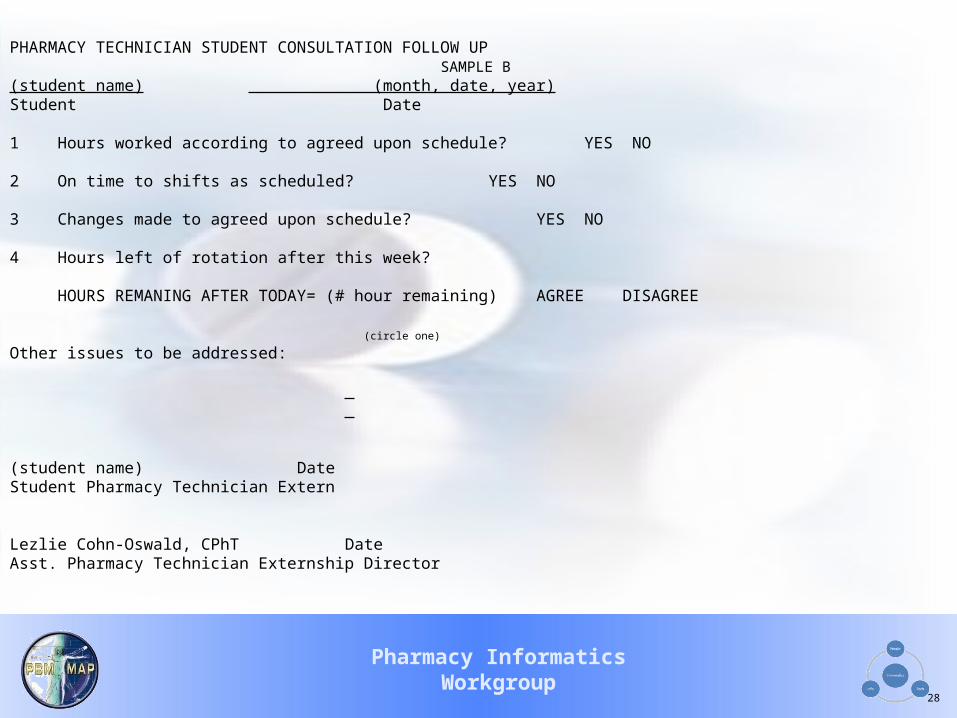
> Student consultation follow-up (Sample B)
Pharmacy Informatics Workgroup
27
CONTRACT TO COMPLETE PHARMACY TECHNICIAN EXTERNSHIP ROTATION SAMPLE AAT THE SALT LAKE CITY VA MEDICAL CENTER
I, __(student name)_________, on this day, (week day), (month, day, year), promise to finishmy Pharmacy Technician Externship rotation in its entirety.
I will work all of my scheduled hours without calling in for any reason.
I will not be late for any scheduled shifts for any reason.
(LATE is defined as anything up to 10 minutes after agreed upon daily start time)
I may not make changes to my schedule.
Hours needed for entire program = 180 hoursHours completed to date in Outpatient = ____ hours
Hours completed to date in Inpatient = ____ hours
Hours needed to complete program entire rotation = ____ hours(schedule as put forth by myself, (program director), and (student name) -see attached calendar)
(student name) agrees with the hours as stated above.
The Associate Program Director will meet with you weekly to review attendance and performance. Your (school name) Program Director will be notified of this action and given weekly updates. If I, (student name), fail to abide by the above written terms as written and initialed by me, this will be considered grounds for immediate termination of the externship.
(Lines for Pharmacy Technician Student, OP/IP Pharm Tech Extern Preceptor, OP/IP Pharmacy Supervisor, Asst. Program Director & Director sign & date)
Student will be provided a copy of this signed agreement & schedule attachment.
Pharmacy Informatics Workgroup
28
PHARMACY TECHNICIAN STUDENT CONSULTATION FOLLOW UP SAMPLE B
(student name) (month, date, year)Student Date
1 Hours worked according to agreed upon schedule? YES NO
2 On time to shifts as scheduled? YES NO
3 Changes made to agreed upon schedule? YES NO
4 Hours left of rotation after this week?
HOURS REMANING AFTER TODAY= (# hour remaining) AGREE DISAGREE (circle one)
Other issues to be addressed:
(student name) DateStudent Pharmacy Technician Extern
Lezlie Cohn-Oswald, CPhT DateAsst. Pharmacy Technician Externship Director
Pharmacy Informatics Workgroup
29
ROTATION END
> Paperwork - School-provided end-of rotation
evaluation (class grade)
- Student evaluation of program
(Sample C)
- Non-Paid Employees Clearance Sheet
(memo 05.11 in lieu of VA Form 3248 B)

Pharmacy Informatics Workgroup
30
Salt Lake City VA Medical Center SAMPLE C Pharmacy Technician Training ProgramPharmacy Technician Externship Program
STUDENT EVALUATION OF EXTERNSHIPName:
Signature: Date:
Directions:At the end of the externship training, each student is required to evaluate their externship experience. Your input allows the program to monitor the externship content and also informs the program of strengths and weaknesses. Please give your honest evaluation and comments below.
Part I: Please rate your externship experience at this site in the following areas. For each response in the POOR column, please give specific information about why you have evaluated the site as POOR.
EXCELLENT GOOD FAIR POOR1 LOCATION of the site: 2 ACCESSIBILITY of the
preceptor at this site:3 ACCESSIBILITY of the
pharmacy staff at this site:4 HELPFULNESS of the staff in guiding you and answering your questions:5 APPROPRIATENESS of your
externship activities:6 COMPLETENESS of your training: 7 PREPAREDNESS for experiential work following training:8 Would you recommend this site to future students? YES NO9 Comments:
Pharmacy Informatics Workgroup
31
ROTATION END (CONT’)
> Evaluation for employment
- resume
- conference with supervisor for review
of evaluations done throughout
student rotation (if position available)
- keep student information on file for
possible future hire
Pharmacy Informatics Workgroup
32
PROGRAM STATS
> First Year 2009 (10/08-10/09) - 13 students enrolled in program
- 1 student failed
- 5 students hired in contract positions
(2 in IP -one on medical leave- & 3 in OP)
- 1 on hire wait list
- 1 needing 90 hours/1 needing 40 hours only
> Second year 2010 (10/09 to date) - 1 on hiring wait list
- 1 currently in program
Pharmacy Informatics Workgroup
33
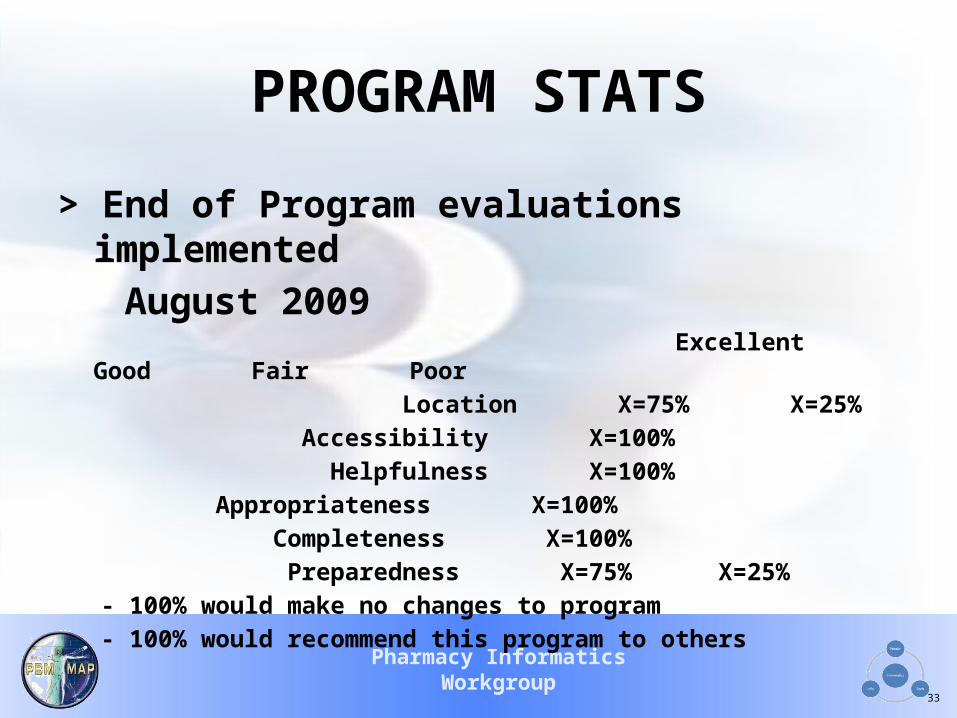
PROGRAM STATS
> End of Program evaluations implemented
August 2009 Excellent Good Fair Poor
Location X=75% X=25%
Accessibility X=100%
Helpfulness X=100%
Appropriateness X=100%
Completeness X=100%
Preparedness X=75% X=25%
- 100% would make no changes to program
- 100% would recommend this program to others

Pharmacy Informatics Workgroup
34
?QUESTIONS?
Lezlie Cohn-Oswald, CPhTPharmacy Technician Externship
Program Associate DirectorVA Salt Lake City Health Care
System(801) 582-1565 ext. 4208