perinatal mental health care pathway
TRANSCRIPT
PAN LONDON PERINATAL MENTAL HEALTH
NETWORK
PERINATAL MENTAL HEALTH CARE PATHWAYS
October 2015
Authors ©:
Dr Lucinda Green - Consultant Perinatal Psychiatrist, St Thomas
Hospital, SLAM NHS Foundation Trust, Chair of the South London
Perinatal Mental Health Clinical Network
Dr Maddalena Miele - Consultant Perinatal Psychiatrist, St Mary’s
Hospital, CNWL NHS Foundation Trust, Chair of the North West
London Perinatal Mental Health Clinical Network
Dr Olivia Protti - Consultant Perinatal Psychiatrist , MBU Homerton
Hospital, East London NHS Foundation Trust, Chair of the North East
London Perinatal Mental Health Clinical Network
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
2
CONTENTS
FOREWORD ................................................................................................... 4
INTRODUCTORY NOTES AND THEORETICAL FRAMEWORK .......................... 6
The Pan London Perinatal Mental Health Network ............................... 6
Consultation process and pathway development .................................. 6
Clinical Guidance and Perinatal Clinical Standards .............................. 7
Background and explanatory notes ......................................................... 8
Principles of Care ..................................................................................... 12
PERINATAL MENTAL HEALTH CARE PATHWAYS: OVERVIEW OF THE
PERINATAL MENTAL HEALTH SERVICE LINE STRANDS ................................ 14
PERINATAL MENTAL HEALTH CARE PATHWAYS: MATERNAL MENTAL
HEALTH - PSYCHIATRY SERVICE LINE STRAND ............................................ 16
PERINATAL MENTAL HEALTH CARE PATHWAYS: MATERNAL MENTAL
HEALTH- PSYCHOLOGICAL THERAPIES SERVICE LINE STRAND ................... 17
PERINATAL MENTAL HEALTH CARE PATHWAYS: PARENT - INFANT MENTAL
HEALTH SERVICE LINE STRAND ................................................................... 18
PERINATAL MENTAL HEALTH CARE PATHWAYS: SOCIAL CARE SERVICE LINE
STRAND ....................................................................................................... 19
MATERNAL MENTAL HEALTH - PERINATAL PSYCHIATRIC SERVICES:
ALGORITHM FOR PRECONCEPTION ADVICE ............................................... 20
MATERNAL MENTAL HEALTH PERINATAL PSYCHIATRIC SERVICES:
ALGORITHM FOR PREGNANCY .................................................................... 21

PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
3
MATERNAL MENTAL HEALTH - PERINATAL PSYCHIATRIC SERVICES:
ALGORITHM FOR DELIVERY......................................................................... 22
MATERNAL MENTAL HEALTH - PERINATAL PSYCHIATRIC SERVICES:
ALGORITHM FOR THE POSTPARTUM .......................................................... 23
MATERNAL MENTAL HEALTH - PRIMARY CARE PATHWAY ......................... 24
Maternal Mental Health – Perinatal Psychiatric Services Algorithms –
additional information ................................................................................ 25
Appendix 1................................................................................................. 31
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
4
FOREWORD
On behalf of the Mental Health and Maternity Strategic Clinical Leadership Groups Having a baby is a major life transition for all women, a joyful and
exciting time for many and a very challenging period for others.
Between 10 and 20% of women develop a mental health problem
during pregnancy or within the first year after having a baby. Perinatal
mental health problems are an important cause of maternal mortality
and if untreated may not resolve for a long time and can have a
devastating impact on both women and their families.
Mental disorders in the perinatal period include antenatal and postnatal
depression, anxiety disorders including obsessive compulsive disorder
and panic disorder, eating disorders, post-traumatic stress disorder,
relapse of known severe mental illnesses including schizophrenia,
schizoaffective disorder and bipolar affective disorder and postpartum
psychosis. These conditions may develop insidiously or extremely
suddenly during pregnancy and post-delivery. Post-partum psychosis
and severe affective illnesses are particularly likely to occur close to
delivery and are severe and sudden in their presentation, constituting a
medical emergency. Perinatal mental health problems range from mild
to extremely severe, requiring different pathways, management and
care. However, if individuals prone to relapse and those who do
develop an illness are identified early, it is possible to promote recovery
in a timely way and mitigate many of the negative effects of perinatal
mental health problems for women, their infants and their families.
The perinatal mental health care pathway in this document has been
developed by senior practitioners within perinatal mental health
services in London and sets out guidance on the key components
required to develop and deliver perinatal mental health services that
meet the needs of women and their families. It is concordant with NICE
guidance (NICE APMH 2014) and the Perinatal Quality Network
(PQN/CCQI) service standards.
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
5
The key to successful implementation of this pathway lies in the close
integration of community perinatal mental health services and maternity
provider based obstetric and midwifery leads. Given the complex
geography of London, commissioners will play an important role in
configuring these services and ensuring seamless integration.
The London mental health and maternity clinical strategic networks are
very pleased to be able to endorse this care pathway. This pathway is
an important tool that will support commissioners to improve perinatal
care through enabling prevention, prediction, detection and treatment
of perinatal mental health problems. Perinatal mental health provision
needs to be comprehensive, accessible, equitable and available within
a timely manner. This document sets out how this may be achieved to
ensure that women and their families in London get the right treatment,
from the right services at the right time.
Matthew Patrick Co-clinical Director, London Mental Health SCN Chief Executive, South London and the Maudsley NHS Trust
Nick Broughton Co-clinical Director, London Mental Health SCN Medical Director, West London Mental Health NHS Trust
Professor Donald Peebles Co-clinical Director, London Maternity SCN Professor of Fetal Medicine University College London
Donna Ockenden Co-clinical Director, London Maternity SCN Formerly Chief Midwife & Care Group University Director – Family Health Services South London Healthcare Trust
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
6
INTRODUCTORY NOTES AND THEORETICAL FRAMEWORK
The Pan London Perinatal Mental Health Network
The Pan London Perinatal Mental Health Network was formed in 2013. It is a multidisciplinary network accountable to the Clinical Director of the London Mental Health Strategic Clinical Network (SCN). It oversees the North West, North East and South London Perinatal Mental Health Clinical Networks, which each have a chair and a co-chair. The following initial priorities were set for the Network in 2013:
• To develop standardised Perinatal Mental Health Training for London
• To develop a Pan London MBU Admission Protocol
• To develop a London Perinatal Mental Health Care Pathway & standard protocols
• To undertake a Pan London Perinatal Mental Health Needs Assessment
• To develop a London Perinatal information sharing ‘Electronic Hub’
Consultation process and pathway development
• The present document is the result of an extensive consultation exercise over a period of two years involving a wide range of stakeholders across maternity, health visiting, social care, psychology, psychotherapy, psychiatry, the third sector and service users. The views, opinions and experiences of the stake holders were collated through regular meetings of the North West, North East and South London Perinatal Mental Health Clinical Network Meetings and through reporting to the Pan London Perinatal and Mental Health Strategic Clinical Networks. The authors have combined the views of the various stakeholders with the recommendations of all the relevant guidelines, policies and reports on perinatal mental health available at the time of writing.
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
7
• It is anticipated that the care pathway will be updated to incorporate any updates to existing guidance as well as newly launched professional guidelines and government policies.
• The aim is for this pathway to be on a website. If users click on boxes in the pathway additional, more detailed, information will be available. The first set of diagrams, outlining service line strands will lead to the more specific algorithms. An example is included of the algorithms for the perinatal psychiatric service line strand. Work needs to be completed for the other service line strands. Potentially, localised information about specific services and resources can be added in to make the pathways more specific to local boroughs.
Clinical Guidance and Perinatal Clinical Standards
• National Institute for Health and Clinical Excellence (NICE) Antenatal and Postnatal Mental Health: Clinical management and service guidance. CG192. (2014)
• Royal College of Psychiatrist’s Perinatal Quality Network Service Standards: Perinatal Community Mental Health Services - 2nd Edition (April 2014)
• The Royal College of Psychiatrist’s Perinatal Quality Network Service Standards for Mother & Baby Units - 4th Edition (2014)
• Perinatal mental health services: Recommendations for provision of services for childbearing women. Royal College of Psychiatrists. CR197 ( 2015)
• Management of Women with Mental Health Issues during Pregnancy and the Postnatal Period. Royal College of Obstetricians and Gynaecologists (2011)
• Saving Mothers’ Lives: Reviewing maternal deaths to make motherhood safer: 2006–2008. The Eighth Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom (2011)
• Falling Through the Gaps: perinatal mental health and general practice – Centre for Mental Health/Royal College of GPs/Boots Family Trust (2015)
• Joint Commissioning Panel for Mental Health: Guidance for Commissioners of Perinatal Mental Health Services ( 2012)
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
8
• London Child Protection Procedures – 5th Edition (2015)
• Closing the Gap – Priorities for Essential Change in Mental Health - Department of Health (2013)
• NSPCC: Prevention in mind. All Babies Count: Spotlight on Perinatal Mental Health (2011)
• The 1001 Critical Days – The importance of the Conception to Age Two Period. A Cross Party Manifesto.(2013)
• “Everyone’s business” campaign - Maternal Mental Health Alliance
• The Cost of Perinatal Mental Health Problems - London School of Economic & Centre for Mental Health (2014)
• 4-5-6 Model for Health Visiting- Institute of Health Visiting (2015)
• Healthy Child Programme: Pregnancy and the First Five Years – Department of Health (2009)
• Perinatal Mental Health – Experiences of Women and Health Professionals - Boots Family Trust( 2013)
Background and explanatory notes
• The Perinatal Mental Health Pathway (PMHP) presented in this document is designed on the principle that each London borough should have access to an accredited perinatal mental health service (PMHS) with capacity to consider referrals and to provide care at any reproductive stage, i.e. pre-conception, pregnancy, birth and up to 12 months postpartum.
• The Royal College of Psychiatrist’s Perinatal Quality Network defines standards for community perinatal mental health services which will become part of an accreditation process. Standards are defined for the following areas:
o Access and referral o Assessment o Care plans o Care and treatment o Discharge o Infant welfare and safeguarding o Staffing and Training o Recording and Audit
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
9
• The Royal College of Psychiatrist’s Perinatal Quality Network standards require that community perinatal mental health services be staffed as follows in order to be accredited as a good psychiatric service:
o Consultant Perinatal Psychiatrist (Adult); o Non-consultant medical staff; o Perinatal community psychiatric nurses; o Social worker; o Clinical psychologist; o Nursery nurse; o Occupational therapist o Administrative and data entry support
• The Royal College of Psychiatrists (Council Report CR197 – July 2015) suggests staffing levels for specialised perinatal community mental health teams as follows:
o The team must be led by an adult consultant perinatal psychiatrist (at least 1PA per 1000 births). This should be increased if there is no junior doctor support.
o The team should have specialist perinatal mental health nurses (at least 0.5WTE for 1,000 births). Nurses should have caseloads of around 25 women each
It is expected that the composition and the capacity of the workforce should be carefully tailored to the local needs of the geographical area and maternity service served by the perinatal mental health team
• The Royal College of Psychiatrist’s Perinatal Quality Network Service Standards for Mother & Baby Units is associated with an accreditation process.
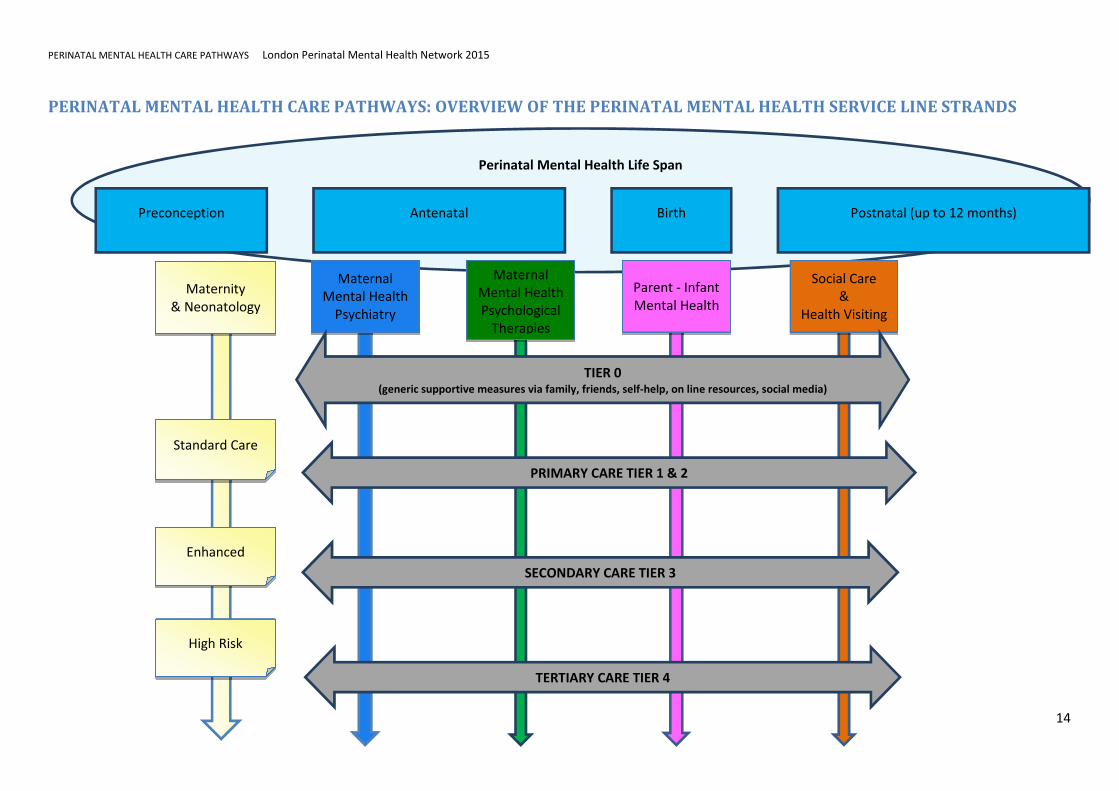
• The London Perinatal Network is mindful that perinatal mental health encompasses a wide range of disciplines –psychiatry, psychology, and psychotherapy – across both adult and early year’s services and that it should be fully integrated with maternity care and health visiting. Therefore, this care pathway incorporates five main interfacing strands: Maternity & Neonatology, Maternal Psychiatry, Maternal Psychological
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
10
Therapies, Infant Mental Health, Social Care and Health Visiting each with clearly defined professional, clinical and managerial service line accountability. The diagrammatic divide is a construct for ease of reference. In practice services may include aspects of more than one service line strand (e.g. a perinatal psychological therapies service may include psychological therapies for the mother as well as parent-infant psychotherapies; or one “perinatal mental health service” may include both the maternal mental health psychiatric and psychological therapies service line strands)
• The Maternity & Neonatology service line strand is expanded with a focus on integrating physical and mental health. The Social Care service line strand, is explored with a focus on the interface with perinatal mental health, when the needs/risks are contingent upon parental psychiatric illness. Health visiting is envisaged as an essential component of the care-pathway. Therefore it is expected that adequate health visiting and perinatal specialist health visiting provisions are ensured.
• The maternity service must factor in specialist provisions to facilitate integration of physical and mental health through joint clinical management, education, training and supervision and establishment of an adequate specialist workforce, namely mental health lead midwives and obstetricians. The partnership among the two services should take the form of robust regular training and education packages for midwives and obstetricians, joint and co-located obstetric psychiatric liaison clinics, joint management plans with active involvement of obstetric and midwifery teams for women with complex needs (e.g. medical complications in pregnancy) and/or severe and enduring mental illness.
• Each maternity unit should have a dedicated (i.e. with clinical sessions additionally funded) obstetric consultant as the Obstetric Perinatal Mental Health lead and at least one WTE specialist perinatal mental health midwife who will work closely with the child safeguarding midwife, the perinatal psychiatrist and specialist perinatal mental health nurses forming a
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
11
dedicated multi-professional team. The specialist perinatal mental health midwife role should be in addition to and not merged with the pre-existing child safeguarding midwife.
• The service line strands span through service tiers 1, 2, 3 & 4 according to the level of complexity and risk; some interventions are likely to overlap.
• It is expected that Perinatal Mental Health teams will have a multi- and inter-disciplinary composition and work philosophy. However, the clinical and managerial accountability should be in accordance with the relevant professional specialty, code of practice and clinical governance.
• Women referred to a PMHS may present with multiple risks at a variable level e.g. high psychiatric low obstetric risk; high mental health, high social but low psychiatric risk. The coordination of care should be led by the service or services managing the highest level of risk.
• Psychological therapies may be accessed either through the mother (Psychological Therapies strand) or through the infant (Infant Mental Health strand). Both routes of access should work with the mother and infant as a system, with an awareness of the forming attachment. Although access to these therapies has been categorised in separate strands, there is likely to be an overlap in the therapy implemented in both pathways.
• Psychological therapies should be delivered by practitioners with expertise and training in perinatal mental health. This is in order to provide optimum interventions for women, which also takes into account the baby and the developing attachment, to safely and effectively manage risk and to allow the interagency working necessary during the perinatal period. Where specialist perinatal psychological therapies are not available, therapies will be delivered by practitioners in generic adult mental health services. Although women in the perinatal period
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
12
are often prioritised by these services, the provision is unlikely to be as specialised.
• The care pathway for young people (<18 years old) is the same with the exception that the psychiatric care is led by a CAMHS consultant psychiatrist. Perinatal mental health services can work jointly with CAMHS services.
• It is expected that the relevant commissioning process across London reflects the composite multiagency nature of the PMHS care pathway coherently and that all the relevant CCGs contribute to the establishment of the services accordingly.
• It is anticipated that the final configuration and the level of investment required to bring perinatal mental health care pathways up to standard across London will be determined by the extent and sustainability of pre-existing service provision and local need.
Principles of Care
• Training and supervision should be available for all professionals and agencies involved in the care of pregnant and postnatal women with mental illness. Practitioners with the relevant competencies and professional accreditations should deliver this training.
• Professionals should work in partnership with women (and others she wishes to include: partner, family & carers).
• Service provision should be matched to the woman’s needs.
• All professionals should be sensitive to cultural needs.
• Advice and support should be offered to partners (and carers).
• Good communication and information sharing between all professionals, the woman (and partner and family, if she wishes to involve them) is essential.
• Information needs to be available for women, partners/family and professionals about: perinatal mental health services, mental disorders, treatments, voluntary sector services, other sources of information/support and advice.
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
13
• Professionals should consider risk at points of transition (e.g. to new midwife or GP, or move to new area).When women move to a new area or transfer their maternity care it is essential to ensure that all relevant information is shared appropriately with the professionals in the new area.
• It is important to ensure women who are homeless, those who move frequently and those who have no recourse to public funds, do not fall between services.
• There should be systems in place to ensure that if there is significant change (e.g. relapse; domestic violence; relationship breakdown) this is identified, communicated to all involved professionals and that a multiagency meeting is held if needed.
• Women with a primary substance misuse diagnosis should be referred to a substance misuse service. In pregnancy this should preferably be a specialist antenatal substance misuse service.
• Prescribers can access information on prescribing in pregnancy and breastfeeding from the following: o NICE Guideline for Antenatal and Postnatal Mental Health (2014) o UK Teratology Information Service (www.uktis.org)
• Psychological therapies services should prioritise women who are pregnant or in the first postnatal year.
• When many professionals are involved in a woman’s care, it is important to clarify professionals’ roles and clinical accountability.
• All professionals should consider the need for referral to Children and Young People’s Services (CYPS) for Safeguarding or Early Help.
• There should be a thorough review of previous mental health and CYPS records as part of the assessment by the relevant agencies.
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
14
PERINATAL MENTAL HEALTH CARE PATHWAYS: OVERVIEW OF THE PERINATAL MENTAL HEALTH SERVICE LINE STRANDS
Perinatal Mental Health Life Span
Preconception Antenatal Birth Postnatal (up to 12 months)
Maternal
Mental Health
Psychiatry
Maternal
Mental Health
Psychological
Therapies
Parent - Infant
Mental Health
Social Care
&
Health Visiting
Maternity
& Neonatology
Standard Care
Enhanced
High Risk
PRIMARY CARE TIER 1 & 2
TERTIARY CARE TIER 4
SECONDARY CARE TIER 3
TIER 0 (generic supportive measures via family, friends, self-help, on line resources, social media)

PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
15
PERINATAL MENTAL HEALTH CARE PATHWAYS: INTEGRATIVE INTERFACE WITH
MATERNITY & NEONATOLOGY SERVICE LINE STRAND
PRIMARY CARE TIER 1 & 2
SECONDARY CARE TIER 3
TIER 0
• Joint high risk obstetric-psychiatric clinics for women
with Severe Mental Illness
• Multidisciplinary management of irrational fear of
childbirth
• Pre-birth planning meeting
• Intrapartum care planning involving obstetric
anaesthetist
• Joint review of maternity inpatients and multidisciplinary
postnatal review and pre-discharge meetings for
complex cases
Maternity
&
Neonatology
Antenatal and Psychiatric Clinics co-
located in hospital and community
settings.
MDT referral meeting
• Perinatal Psychiatrist
• Perinatal Mental Health
Nurses
• Mental Health Obstetric lead
• Mental Health specialist
midwife
• Child Safeguarding midwife
• Psychologist
Midwifery (and neonatal
nursing) training in mental
health and referral pathways
Cross disciplinary training
placements for Obstetric,
Psychiatry, and Psychology
Trainees
Weekly supervision of Mental Health Lead
Midwife, Child Safeguarding Midwife and
neonatal nurses
Midwives to shadow specialist midwife and
specialist perinatal psychiatric nurse to
improve skills in detection and awareness of
care pathways.
Joint Obstetric/Neonatal/
Psychiatric Academic events
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
16
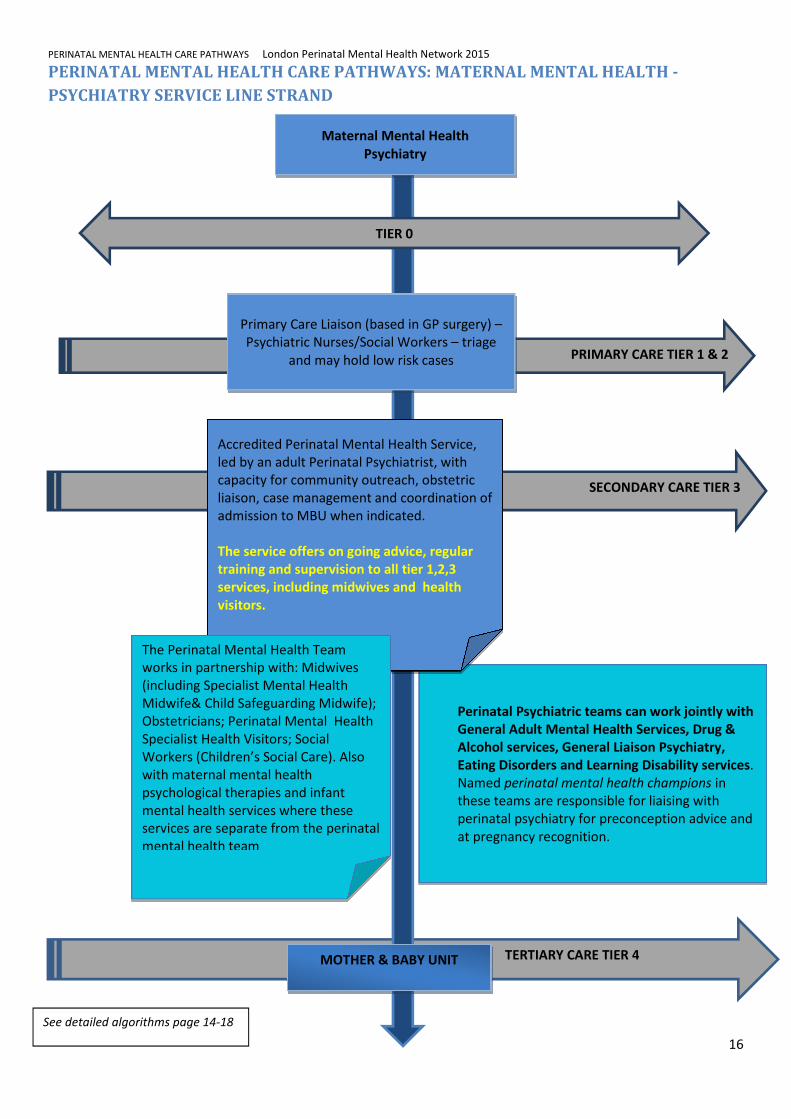
PERINATAL MENTAL HEALTH CARE PATHWAYS: MATERNAL MENTAL HEALTH -
PSYCHIATRY SERVICE LINE STRAND
TERTIARY CARE TIER 4
Perinatal Psychiatric teams can work jointly with
General Adult Mental Health Services, Drug &
Alcohol services, General Liaison Psychiatry,
Eating Disorders and Learning Disability services.
Named perinatal mental health champions in
these teams are responsible for liaising with
perinatal psychiatry for preconception advice and
at pregnancy recognition.
MOTHER & BABY UNIT
PRIMARY CARE TIER 1 & 2
SECONDARY CARE TIER 3
Maternal Mental Health
Psychiatry
Primary Care Liaison (based in GP surgery) –
Psychiatric Nurses/Social Workers – triage
and may hold low risk cases
Accredited Perinatal Mental Health Service,
led by an adult Perinatal Psychiatrist, with
capacity for community outreach, obstetric
liaison, case management and coordination of
admission to MBU when indicated.
The service offers on going advice, regular
training and supervision to all tier 1,2,3
services, including midwives and health
visitors.
The Perinatal Mental Health Team
works in partnership with: Midwives
(including Specialist Mental Health
Midwife& Child Safeguarding Midwife);
Obstetricians; Perinatal Mental Health
Specialist Health Visitors; Social
Workers (Children’s Social Care). Also
with maternal mental health
psychological therapies and infant
mental health services where these
services are separate from the perinatal
mental health team
TIER 0
See detailed algorithms page 14-18
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
17
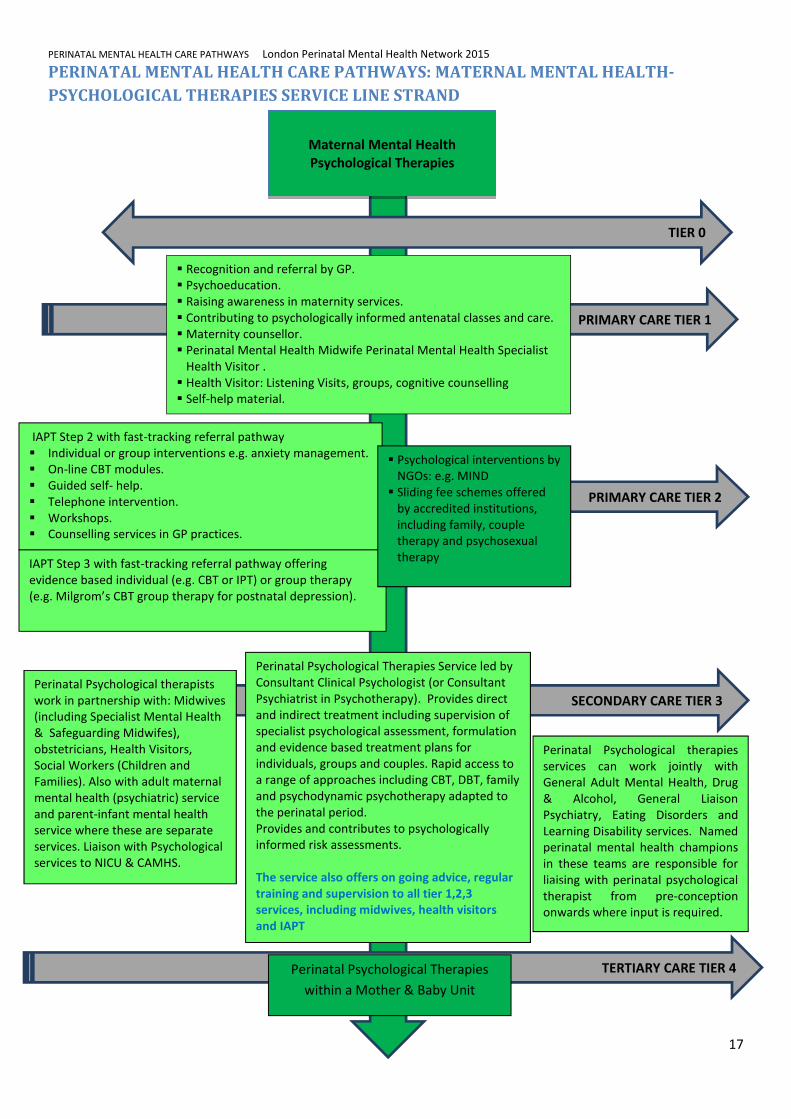
PERINATAL MENTAL HEALTH CARE PATHWAYS: MATERNAL MENTAL HEALTH-
PSYCHOLOGICAL THERAPIES SERVICE LINE STRAND
SECONDARY CARE TIER 3
Maternal Mental Health
Psychological Therapies
TIER 0
PRIMARY CARE TIER 2
PRIMARY CARE TIER 1
� Recognition and referral by GP.
� Psychoeducation.
� Raising awareness in maternity services.
� Contributing to psychologically informed antenatal classes and care.
� Maternity counsellor.
� Perinatal Mental Health Midwife Perinatal Mental Health Specialist
Health Visitor .
� Health Visitor: Listening Visits, groups, cognitive counselling
� Self-help material.
IAPT Step 2 with fast-tracking referral pathway
� Individual or group interventions e.g. anxiety management.
� On-line CBT modules.
� Guided self- help.
� Telephone intervention.
� Workshops.
� Counselling services in GP practices.
IAPT Step 3 with fast-tracking referral pathway offering
evidence based individual (e.g. CBT or IPT) or group therapy
(e.g. Milgrom’s CBT group therapy for postnatal depression).
Perinatal Psychological Therapies Service led by
Consultant Clinical Psychologist (or Consultant
Psychiatrist in Psychotherapy). Provides direct
and indirect treatment including supervision of
specialist psychological assessment, formulation
and evidence based treatment plans for
individuals, groups and couples. Rapid access to
a range of approaches including CBT, DBT, family
and psychodynamic psychotherapy adapted to
the perinatal period.
Provides and contributes to psychologically
informed risk assessments.
The service also offers on going advice, regular
training and supervision to all tier 1,2,3
services, including midwives, health visitors
and IAPT
Perinatal Psychological therapies
services can work jointly with
General Adult Mental Health, Drug
& Alcohol, General Liaison
Psychiatry, Eating Disorders and
Learning Disability services. Named
perinatal mental health champions
in these teams are responsible for
liaising with perinatal psychological
therapist from pre-conception
onwards where input is required.
Perinatal Psychological therapists
work in partnership with: Midwives
(including Specialist Mental Health
& Safeguarding Midwifes),
obstetricians, Health Visitors,
Social Workers (Children and
Families). Also with adult maternal
mental health (psychiatric) service
and parent-infant mental health
service where these are separate
services. Liaison with Psychological
services to NICU & CAMHS.
TERTIARY CARE TIER 4 Perinatal Psychological Therapies
within a Mother & Baby Unit
� Psychological interventions by
NGOs: e.g. MIND
� Sliding fee schemes offered
by accredited institutions,
including family, couple
therapy and psychosexual
therapy
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
18
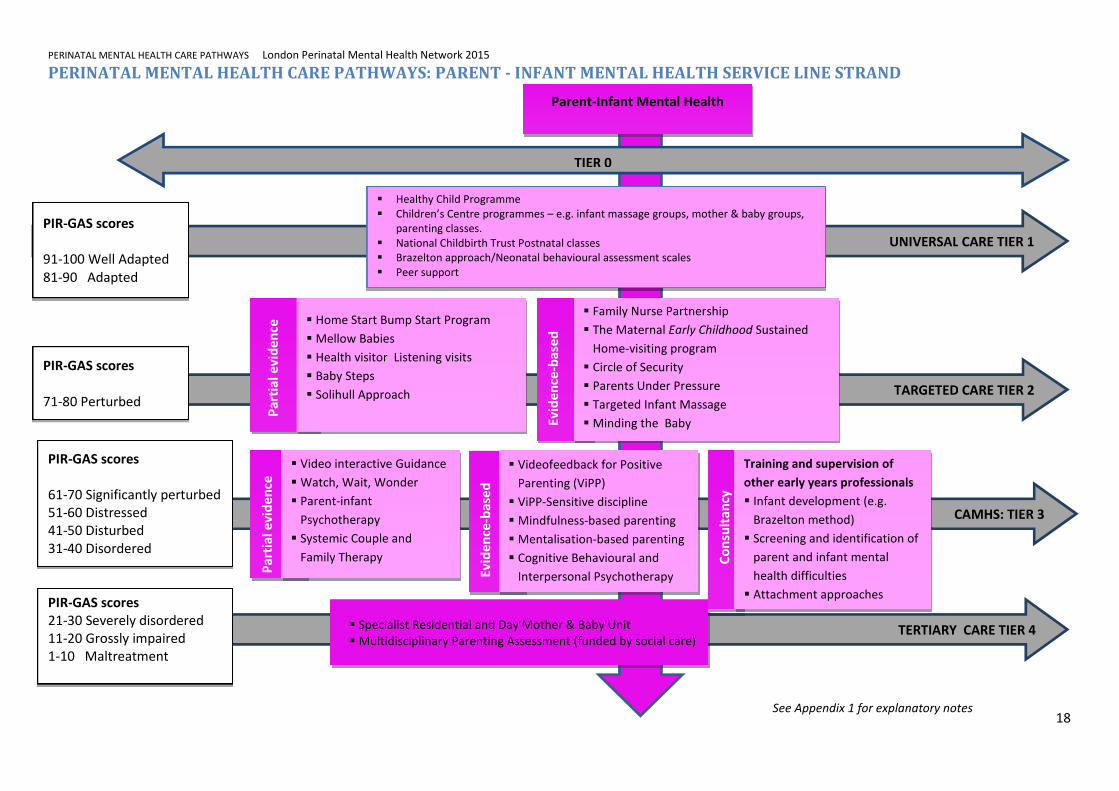
PERINATAL MENTAL HEALTH CARE PATHWAYS: PARENT - INFANT MENTAL HEALTH SERVICE LINE STRAND
CAMHS: TIER 3
TERTIARY CARE TIER 4
UNIVERSAL CARE TIER 1
TARGETED CARE TIER 2
TIER 0
Parent-Infant Mental Health
PIR-GAS scores
91-100 Well Adapted
81-90 Adapted
PIR-GAS scores
61-70 Significantly perturbed
51-60 Distressed
41-50 Disturbed
31-40 Disordered
PIR-GAS scores
21-30 Severely disordered
11-20 Grossly impaired
1-10 Maltreatment
PIR-GAS scores
71-80 Perturbed
� Healthy Child Programme
� Children’s Centre programmes – e.g. infant massage groups, mother & baby groups,
parenting classes.
� National Childbirth Trust Postnatal classes
� Brazelton approach/Neonatal behavioural assessment scales
� Peer support
� Specialist Residential and Day Mother & Baby Unit
� Multidisciplinary Parenting Assessment (funded by social care)
P
art
ial
ev
ide
nce
� Home Start Bump Start Program
� Mellow Babies
� Health visitor Listening visits
� Baby Steps
� Solihull Approach
E
vid
en
ce-b
ase
d
� Family Nurse Partnership
� The Maternal Early Childhood Sustained
Home-visiting program
� Circle of Security
� Parents Under Pressure
� Targeted Infant Massage
� Minding the Baby
C
on
sult
an
cy
E
vid
en
ce-b
ase
d
Pa
rtia
l e
vid
en
ce
Training and supervision of
other early years professionals
� Infant development (e.g.
Brazelton method)
� Screening and identification of
parent and infant mental
health difficulties
� Attachment approaches
� Video interactive Guidance
� Watch, Wait, Wonder
� Parent-infant
Psychotherapy
� Systemic Couple and
Family Therapy
� Videofeedback for Positive
Parenting (ViPP)
� ViPP-Sensitive discipline
� Mindfulness-based parenting
� Mentalisation-based parenting
� Cognitive Behavioural and
Interpersonal Psychotherapy
See Appendix 1 for explanatory notes
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
19
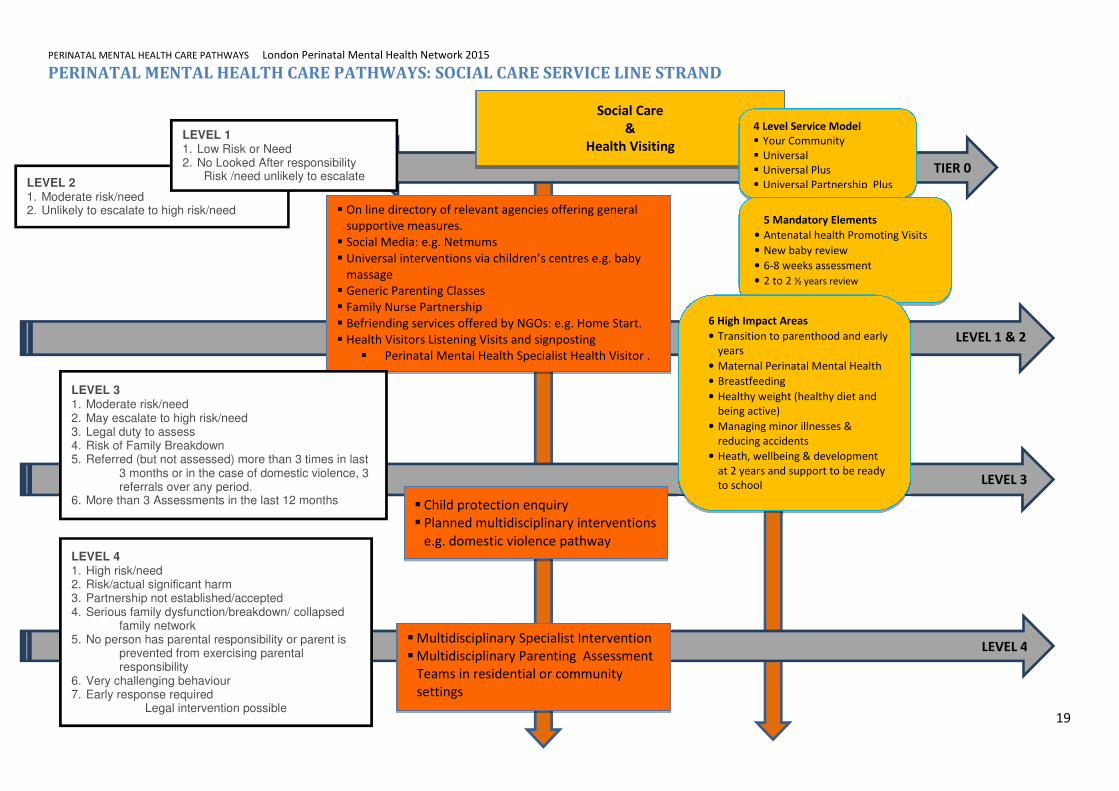
PERINATAL MENTAL HEALTH CARE PATHWAYS: SOCIAL CARE SERVICE LINE STRAND
TIER 0
LEVEL 1 & 2
LEVEL 4
LEVEL 3
Social Care
&
Health Visiting
� On line directory of relevant agencies offering general
supportive measures.
� Social Media: e.g. Netmums
� Universal interventions via children’s centres e.g. baby
massage
� Generic Parenting Classes
� Family Nurse Partnership
� Befriending services offered by NGOs: e.g. Home Start.
� Health Visitors Listening Visits and signposting
� Perinatal Mental Health Specialist Health Visitor .
� Multidisciplinary Specialist Intervention
� Multidisciplinary Parenting Assessment
Teams in residential or community
settings
� Child protection enquiry
� Planned multidisciplinary interventions
e.g. domestic violence pathway
4 Level Service Model
� Your Community
� Universal
� Universal Plus
� Universal Partnership Plus
LEVEL 4 1. High risk/need 2. Risk/actual significant harm 3. Partnership not established/accepted 4. Serious family dysfunction/breakdown/ collapsed
family network 5. No person has parental responsibility or parent is
prevented from exercising parental responsibility
6. Very challenging behaviour 7. Early response required
Legal intervention possible
LEVEL 3 1. Moderate risk/need 2. May escalate to high risk/need 3. Legal duty to assess 4. Risk of Family Breakdown 5. Referred (but not assessed) more than 3 times in last
3 months or in the case of domestic violence, 3 referrals over any period.
6. More than 3 Assessments in the last 12 months
LEVEL 2 1. Moderate risk/need 2. Unlikely to escalate to high risk/need
LEVEL 1 1. Low Risk or Need 2. No Looked After responsibility
Risk /need unlikely to escalate
5 Mandatory Elements
• Antenatal health Promoting Visits
• New baby review
• 6-8 weeks assessment
• 2 to 2 ½ years review
6 High Impact Areas
• Transition to parenthood and early
years
• Maternal Perinatal Mental Health
• Breastfeeding
• Healthy weight (healthy diet and
being active)
• Managing minor illnesses &
reducing accidents
• Heath, wellbeing & development
at 2 years and support to be ready
to school
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
20
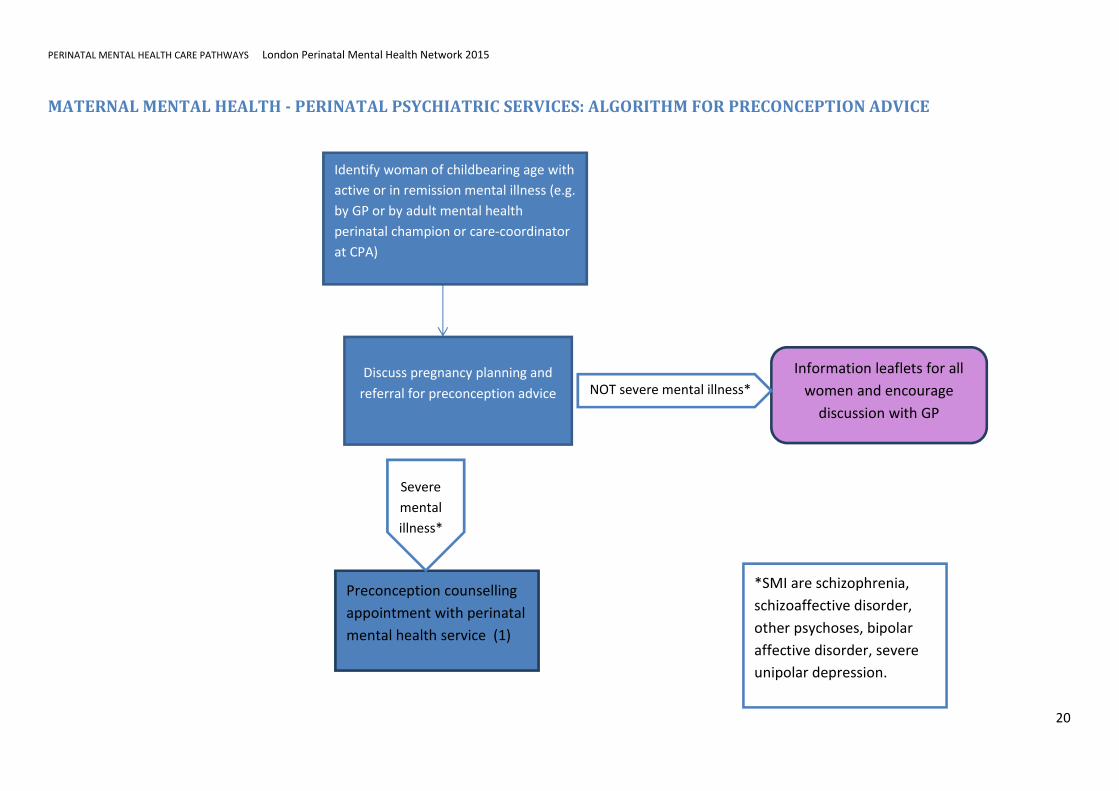
MATERNAL MENTAL HEALTH - PERINATAL PSYCHIATRIC SERVICES: ALGORITHM FOR PRECONCEPTION ADVICE
Identify woman of childbearing age with
active or in remission mental illness (e.g.
by GP or by adult mental health
perinatal champion or care-coordinator
at CPA)
Discuss pregnancy planning and
referral for preconception advice
Preconception counselling
appointment with perinatal
mental health service (1)
Information leaflets for all
women and encourage
discussion with GP
*SMI are schizophrenia,
schizoaffective disorder,
other psychoses, bipolar
affective disorder, severe
unipolar depression.
NOT severe mental illness*
Severe
mental
illness*
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
21
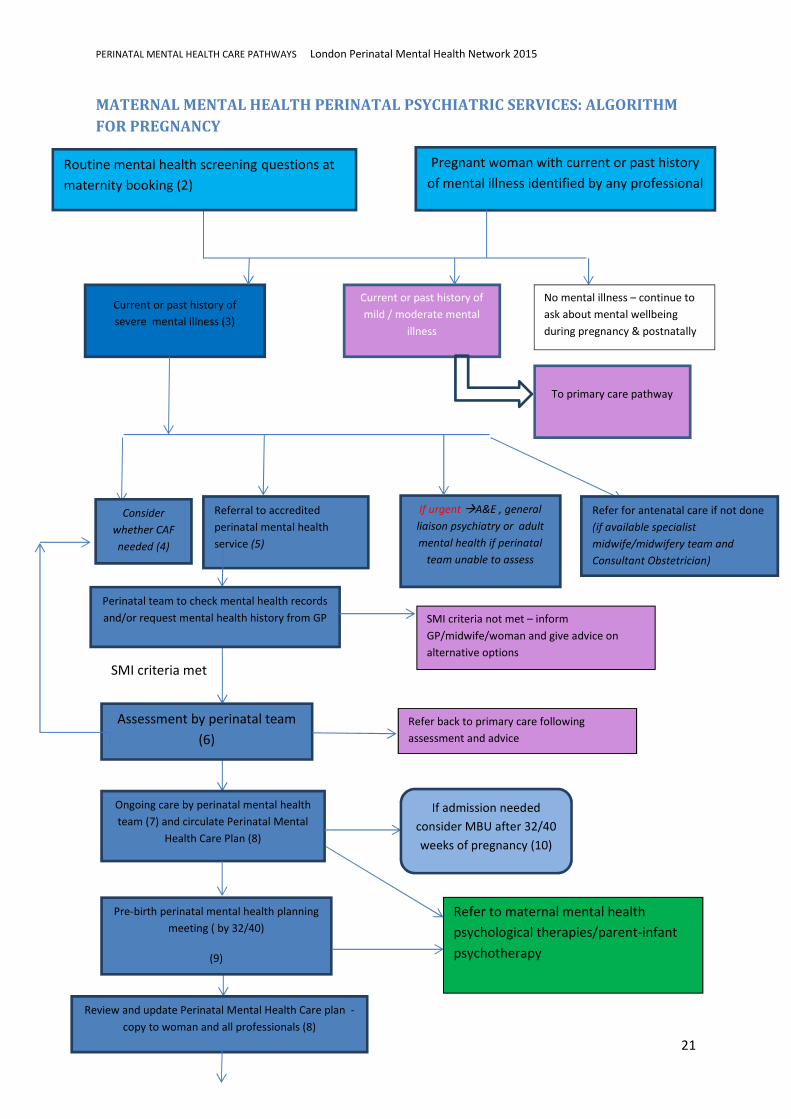
MATERNAL MENTAL HEALTH PERINATAL PSYCHIATRIC SERVICES: ALGORITHM
FOR PREGNANCY
Routine mental health screening questions at maternity booking (2)
Pregnant woman with current or past history
of mental illness identified by any professional
Current or past history of
severe mental illness (3)
Current or past history of
mild / moderate mental
illness
Referral to accredited
perinatal mental health
service (5)
If urgent �A&E , general
liaison psychiatry or adult
mental health if perinatal
team unable to assess
Consider
whether CAF
needed (4)
Refer for antenatal care if not done
(if available specialist
midwife/midwifery team and
Consultant Obstetrician)
Perinatal team to check mental health records
and/or request mental health history from GP SMI criteria not met – inform
GP/midwife/woman and give advice on
alternative options
SMI criteria met
Assessment by perinatal team
(6)
Refer back to primary care following
assessment and advice
Ongoing care by perinatal mental health
team (7) and circulate Perinatal Mental
Health Care Plan (8)
Pre-birth perinatal mental health planning
meeting ( by 32/40)
(9)
If admission needed
consider MBU after 32/40
weeks of pregnancy (10)
No mental illness – continue to
ask about mental wellbeing
during pregnancy & postnatally
Review and update Perinatal Mental Health Care plan -
copy to woman and all professionals (8)
To primary care pathway
Refer to maternal mental health
psychological therapies/parent-infant
psychotherapy
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
22
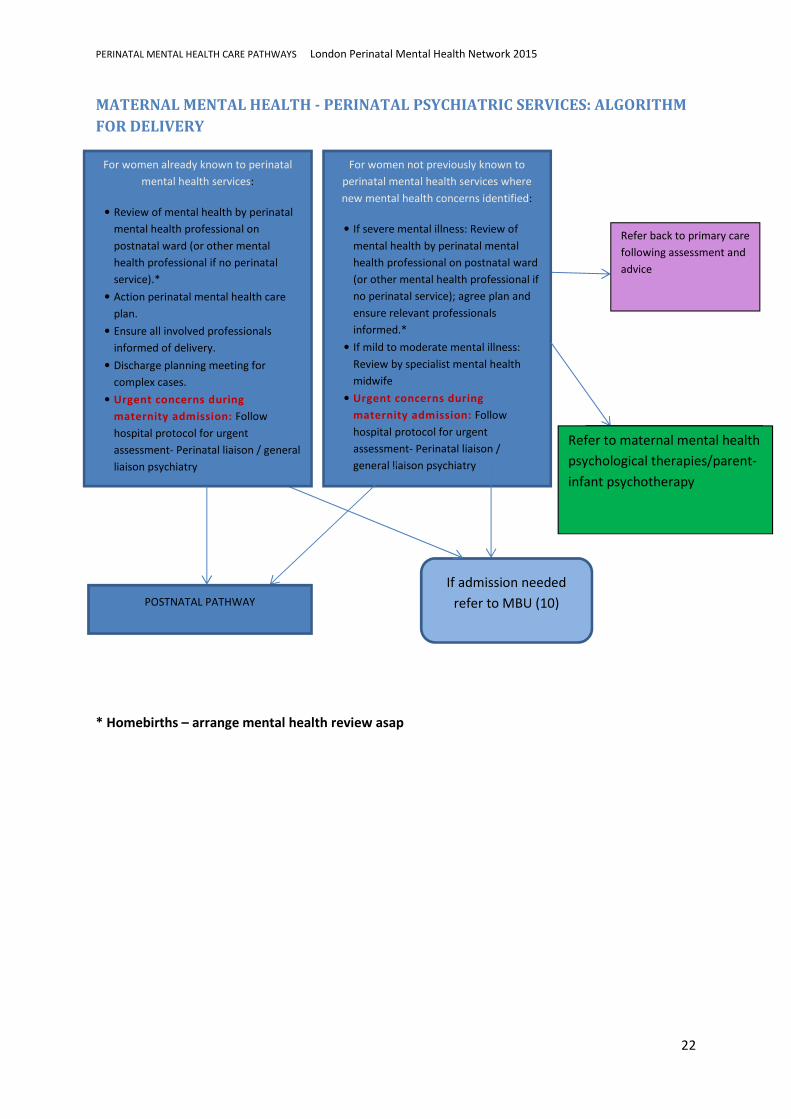
MATERNAL MENTAL HEALTH - PERINATAL PSYCHIATRIC SERVICES: ALGORITHM
FOR DELIVERY
* Homebirths – arrange mental health review asap
For women not previously known to
perinatal mental health services where
new mental health concerns identified:
• If severe mental illness: Review of
mental health by perinatal mental
health professional on postnatal ward
(or other mental health professional if
no perinatal service); agree plan and
ensure relevant professionals
informed.*
• If mild to moderate mental illness:
Review by specialist mental health
midwife
• Urgent concerns during
maternity admission: Follow
hospital protocol for urgent
assessment- Perinatal liaison /
general liaison psychiatry
Refer back to primary care
following assessment and
advice
POSTNATAL PATHWAY
If admission needed
refer to MBU (10)
For women already known to perinatal
mental health services:
• Review of mental health by perinatal
mental health professional on
postnatal ward (or other mental
health professional if no perinatal
service).*
• Action perinatal mental health care
plan.
• Ensure all involved professionals
informed of delivery.
• Discharge planning meeting for
complex cases.
• Urgent concerns during
maternity admission: Follow
hospital protocol for urgent
assessment- Perinatal liaison / general
liaison psychiatry
Refer to perinatal
psychology/infant mental
health
Refer to maternal mental health
psychological therapies/parent-
infant psychotherapy
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
23
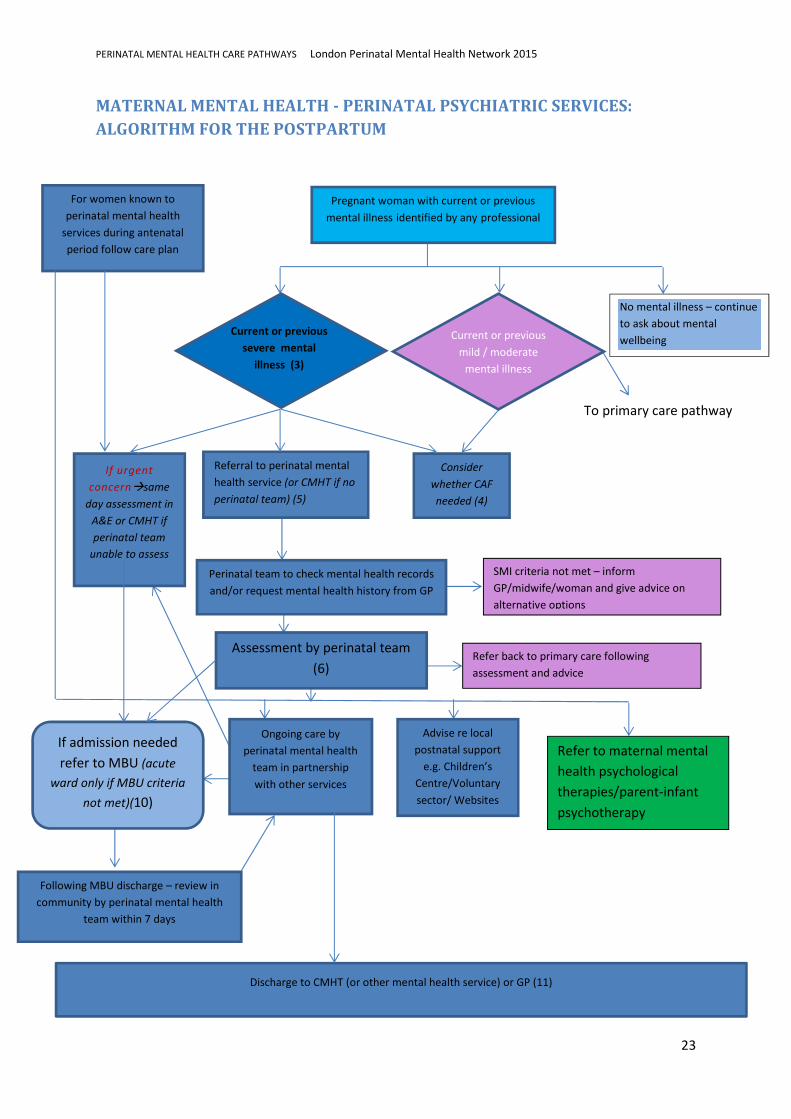
MATERNAL MENTAL HEALTH - PERINATAL PSYCHIATRIC SERVICES:
ALGORITHM FOR THE POSTPARTUM
Protocol for joint working with CMHT
To primary care pathway
Discharge to CMHT (or other mental health service) or GP (11)
If admission needed
refer to MBU (acute
ward only if MBU criteria
not met)(10)
Advise re local
postnatal support
e.g. Children’s
Centre/Voluntary
sector/ Websites
etc
Following MBU discharge – review in
community by perinatal mental health
team within 7 days
For women known to
perinatal mental health
services during antenatal
period follow care plan
Current or previous
severe mental
illness (3)
Current or previous
mild / moderate
mental illness
Pregnant woman with current or previous
mental illness identified by any professional
Consider
whether CAF
needed (4)
Referral to perinatal mental
health service (or CMHT if no
perinatal team) (5)
If urgent
concern�same
day assessment in
A&E or CMHT if
perinatal team
unable to assess
Perinatal team to check mental health records
and/or request mental health history from GP
SMI criteria not met – inform
GP/midwife/woman and give advice on
alternative options
Assessment by perinatal team
(6)
Ongoing care by
perinatal mental health
team in partnership
with other services
Refer back to primary care following
assessment and advice
No mental illness – continue
to ask about mental
wellbeing
Refer to maternal mental
health psychological
therapies/parent-infant
psychotherapy
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
24
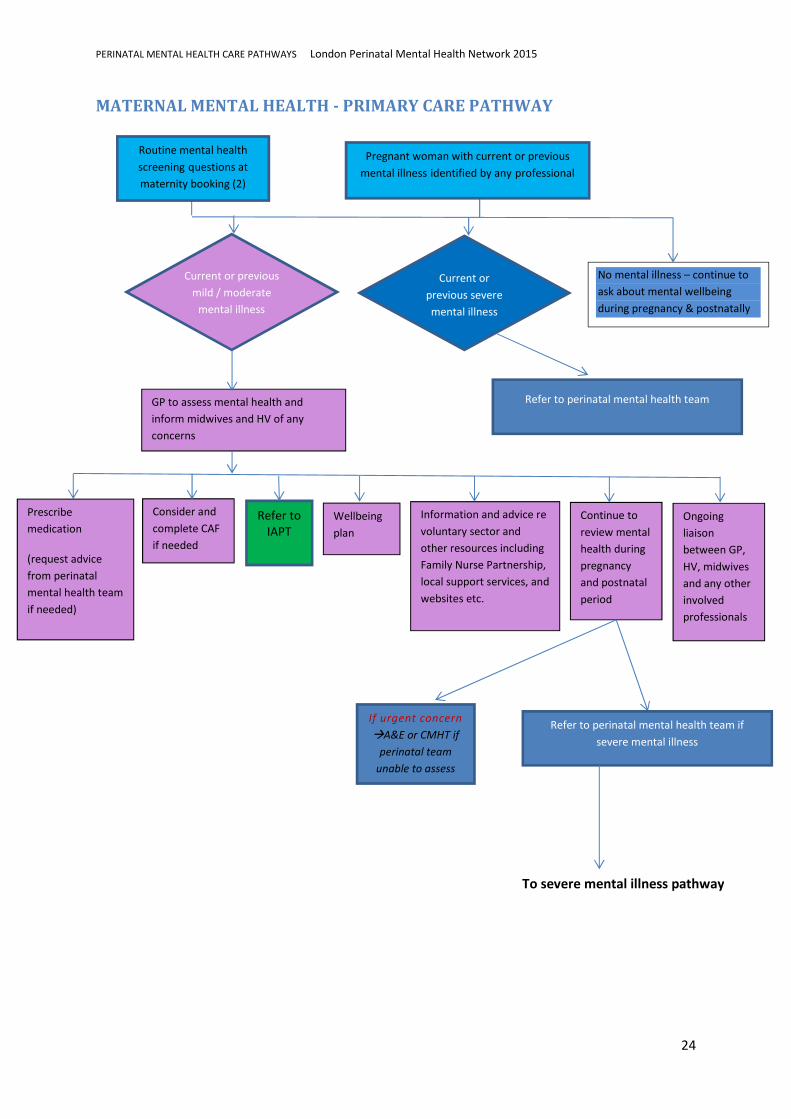
MATERNAL MENTAL HEALTH - PRIMARY CARE PATHWAY
No mental illness – continue to
ask about mental wellbeing
during pregnancy & postnatally
GP to assess mental health and
inform midwives and HV of any
concerns
To severe mental illness pathway
Routine mental health
screening questions at
maternity booking (2)
Pregnant woman with current or previous
mental illness identified by any professional
Current or previous
mild / moderate
mental illness
Current or
previous severe
mental illness
Refer to perinatal mental health team
Information and advice re
voluntary sector and
other resources including
Family Nurse Partnership,
local support services, and
websites etc.
Wellbeing
plan
Consider and
complete CAF
if needed
Prescribe
medication
(request advice
from perinatal
mental health team
if needed)
Refer to
IAPT
Continue to
review mental
health during
pregnancy
and postnatal
period
Ongoing
liaison
between GP,
HV, midwives
and any other
involved
professionals
Refer to perinatal mental health team if
severe mental illness
If urgent concern
�A&E or CMHT if
perinatal team
unable to assess
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
25
Maternal Mental Health – Perinatal Psychiatric Services Algorithms – additional
information
(When the pathways are on a website, clicking on the numbers within the boxes in the algorithm
flowcharts will lead to the information listed for each number below)
1) Preconception counselling
Include in discussion:
• General health issues – including weight/ smoking/ drugs alcohol/folic acid
• Risks and benefits of medication in pregnancy
• Risk of relapse in pregnancy/postpartum
• Genetic risk
• Maternity and mental health care available locally
• Likelihood of involvement of Children’s Social Care
• Written information for women
• Clarify which women should be seen by perinatal mental health services
2) Mental health screening questions
• Add NICE APMH questions
i. SMI questions – if YES refer to Perinatal Mental Health Service (or
CMHT if no perinatal mental health service available)
ii. Whooley questions – if YES – GP to assess � primary care or
perinatal psychiatric service
iii. Anxiety questions – if YES – GP to assess� primary care or perinatal
psychiatric service
• Clarify: severity of disorder; current and previous treatment etc. Questions
should to be asked for late bookers / women who have had no antenatal
care.
3) Definition of SMI
Severe mental illness includes Schizophrenia, Schizoaffective Disorder, other
psychoses, Bipolar Affective Disorder and Severe Unipolar Depression.
4) Criteria for CAF
5) Criteria for referral to perinatal mental health services (or CMHT)
• Add information about London Perinatal Mental Health Services and
contact details
• Women with current or previous severe mental illness, including
Schizophrenia, Bipolar Disorder, Postpartum Psychosis, other psychotic
disorders, severe affective disorder, severe anxiety disorders e.g. Post
Traumatic Stress Disorder, Obsessive Compulsive Disorder, personality
disorder.
• Women who are pregnant or up to 6 months postpartum with follow-up to 12
months.
• Women over 18 years old
• Women under 18 years can be referred if perinatal psychiatric disorder
dominates the picture and care is joint with CAMHS
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
26
• A clinical member of the team is available to discuss urgent referrals during
working hours.
• Women currently in the care of psychiatric services should be referred.
Assessment, advice and treatment should be in collaboration with the
woman’s usual psychiatric team.
6) What to include in initial perinatal mental health assessment
• Before assessment
o Written acknowledgement sent to women whose referral is accepted
within 2 weeks of receipt of the referral, giving proposed actions.
o Send woman information about the service
o Copy appointment letter to GP and midwife (and CMHT care co-
ordinator if there is one)
o Women are offered choice of where they would like their assessment
to take place, taking into consideration clinical need.
o Pregnant women receiving mood stabiliser medication should be
discussed with the referrer and their usual psychiatrist within 2
working days and appropriate advice given
o Thorough review of previous mental health clinical records
• Timing of assessment (these timings may be subject to change with the
publication of the National Perinatal Access and Waiting Time targets)
o Non-urgent referrals seen within 6 weeks
o Pregnant women receiving mood stabiliser medication should be
offered an appointment that is within the two weeks after referral.
o Women referred with new onset conditions after 28 weeks of
pregnancy and within 6 weeks of delivery should be discussed with
the referrer within 5 working days and appropriate advice given.
o Women referred with new onset conditions after 28 weeks of
pregnancy and within 6 weeks of delivery should be offered an
assessment appointment that takes place within the 2 weeks after the
referral
o Women referred before 28 weeks of pregnancy, should be seen no
later than this point in their pregnancy or within 2 weeks.
• At assessment
o Thorough review of mental health history
o Current and previous treatment and woman’s views about treatment
o Risk history
o Previous pregnancies/children
o Woman’s thoughts about current pregnancy / baby
o Woman’s own experience of being parented
o Discuss risk of relapse in pregnancy and postpartum period
o Discuss risks and benefits of medication in pregnancy/lactation (could
add list of issues to consider in this discussion)
o Discuss (if appropriate) referral to Children’s Social Care
o Discuss services which will be involved, importance of joint working
and how information will be shared
o Contraception
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
27
• After assessment
o Write and circulate Perinatal Mental Health Care Plan (see number 8)
o Refer to other services as needed e.g. Children’s Social Care;
Psychological Therapies/Voluntary sector(e.g. re Domestic Violence)
o Send woman copy of assessment, including information about
risks/benefits of medications discussed, and relevant information
leaflets e.g. Royal College of Psychiatrists leaflets
• Links to further information about the management of specific disorders
could be added here
• Referral to specialist midwife/midwifery team (where this exists)could be
added here
7) Ongoing perinatal mental health care during pregnancy
8) Perinatal Care Plan
• Should be written collaboratively with the pregnant woman
• Should very briefly highlight the main problems/ needs and risks.
• Should incorporate the views of the woman’s partner, family and carers.
• A copy should be sent to the woman for her handheld maternity records. Copies should be sent to all involved professionals and included in all versions of the woman’s notes (maternity, primary care, mental health)
• Should include the diagnosis, current treatment, problems, needs and risks.
• There should be a clear plan for women who do not attend (DNA)
• Should include a plan including the following:
(a) Pregnancy
• Frequency of contact with professionals
• Antenatal care
• Psychotropic medication
• Psychiatric admission
• Concern regarding likelihood of unattended delivery and plan to address this.
• Liaison with other services e.g. substance misuse
• Need for pre-birth planning meeting
(b) Admission to maternity unit at time of delivery
• Changes to psychotropic medication / new medication immediately post delivery
• Whether woman can breastfeed on medication
• The need for an RMN or HCA on the postnatal ward.
• Request for woman to have side room on the postnatal ward
• The need for the perinatal mental health team to be informed of delivery and review the woman before discharge from the maternity unit.
• The need for paediatricians to be aware of potential complications resulting from exposure to psychotropic medication in utero.
• The professionals who need to be contacted before discharge from the maternity unit.
• Child Protection Plan e.g. can woman be alone with baby on postnatal ward; social services department to be alerted
• Contact numbers for perinatal mental health team / duty psychiatrist
• Professionals to be contacted prior to discharge
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
28
(c) Postnatal
• If discharged home, plans for monitoring of mental state closely if high risk of relapse of SMI. Professionals who may be involved in monitoring mental state postnatally may include Community Mental Health Team, Home Treatment Team and Perinatal Mental Health Professionals
• Medication
• Plan for what the mother or her family should do if they have concerns about her mental health
• Mother and Baby Unit admission– elective / acute
• Parenting assessment
• Admission to an Acute Psychiatric Ward
• Role of professionals
• Child Protection Plan
• Information about local postnatal support
• Practical support
(d) Crisis plans (e) Contact details of all professionals
9) Pre-birth perinatal mental health planning meeting
• The following people should be invited (and minutes of meeting circulated to
them):
The woman, her partner, and other family members she wishes to involve.
The following professionals, if involved
• CMHT Care-coordinator
• Midwife
• Health visitor
• Perinatal Mental health professionals
• Social worker for unborn baby
• Obstetrician
• CMHT Consultant
• CAMHS professionals
• GP
• Substance Misuse Service
• Domestic violence service
• Other voluntary organisations
• Interpreter
• Independent advocate
• The following should be discussed:
a. A thorough review of the past history based on a review of all the previous mental health records. This should include:
• Past psychiatric history including diagnosis, admissions, postnatal episodes of illness
• Treatment history including medication (duration of treatment, response, side effects and compliance) and psychological therapies
• Engagement with mental health services
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
29
• Engagement with other services e.g. social services
• Level of functioning when well
• Drug and alcohol history
• Forensic history
• Any previous parenting or child protection concerns
• Relapse signature
• Risk indicators.
b. Current mental state and level of functioning.
c. Current psychiatric treatment and adherence. d. Current drug or alcohol abuse.
e. Risk assessment
• Consider past, current and future risks
• Consider risks to unborn baby, other children, self, other adults.
• Consider pregnancy related issues e.g. risk of untreated illness resulting in poor antenatal care; implications of impulsive behaviour on unborn baby / children
• Consider risk related to lack of insight and compliance
• Child protection concerns.
f. Pregnancy details
• EDD
• Previous pregnancies (including previous attendance for antenatal care)
• Hospital booked for antenatal care
• Planned / unplanned
• Attitude to pregnancy
• Consideration re place of birth (e.g. concerns / risks around home birth)
• Attendance for antenatal care appointments
• Known fetal complications. g. Other children
• main carer
• any concerns
• Children’s Social Care involvement or need for referral. h. Quality of current relationship. i. Other social support.
j. Antenatal education classes, breastfeeding support, parenting classes, voluntary
sector pregnancy and parenting groups and courses. k. Current accommodation.
l. Education (for school age women) m. Asylum / immigration issues. n. Family’s understanding of illness and relapse signature.

PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
30
o. Need for Mother and Baby Unit admission – elective / acute. p. Need for parenting assessment.
q. Clarify whether referral to Children’s Social Care has been discussed and /or sent.
Clarify stage of social services assessment process. This will ensure a Pre-birth Child Protection Conference is arranged sufficiently early (N.B. London Child Protection Procedures recommend this should be held 10 weeks prior to the expected delivery date). If a decision has been made that referral to Children’s Social Care is not necessary then the rationale for this decision must be documented
r. Clarify roles of professionals
10) MBU admission – link to MBU protocol
• Prophylactic admissions for women at high risk of postpartum relapse
• Admissions for treatment from 32 weeks gestation to 12 months postnatal
• Parenting assessment - funded by the Local Authority.
• A&E staff, Home Treatment Teams, and other mental health services, to have
low threshold for considering MBU admission.
11) Discharge summary to include:
• Current mental state
• Risk assessment
• Advice regarding future pregnancies
• Contraceptive advice
• Safeguarding concerns
• Concerns re mother-infant interaction or care of children
• Copy to all involved professionals
PERINATAL MENTAL HEALTH CARE PATHWAYS London Perinatal Mental Health Network 2015
31
Appendix 1 PARENT-INFANT MENTAL HEALTH SERVICE LINE STRAND- Notes
• This pathway refers to infants from birth to 12 months
• Tiers are defined according to scores on the Parent-Infant Relationship Global Assessment
Scale (PIR-GAS), a scale from the Diagnostic Classification of Mental Health and
Development Disorders of Infancy and Early Childhood (DC: 0-3). National Centre for Infants,
Toddlers and Families. Washington DC.
• The interventions available in the tiers described above are not mutually exclusive and
parents may receive interventions that are available across two tiers.
• ‘Evidence-based’ is defined as an intervention that has shown consistent clinical
effectiveness (a significant improvement in parenting, sensitive interactions, attachment or
infant behaviour) in at least one randomised controlled trial. In the case of family therapy,
evidence was only found for its effectiveness in improving sleeping and eating difficulties.
• Staff teams. It is recommended that teams should be formed based on practitioners’ clinical
skills and their ability to provide the most evidence-based interventions. It is therefore
recommended that staff are recruited into generic posts – ‘parent-infant mental health
practitioner’ which reflect a range of seniority (i.e. 1 x band 6, 1x band 7, 1x band 8 and a
consultant post). At least one member of staff should have an intensive outreach role to
engage families in the community. Clinical backgrounds that might fit these posts include
Child Psychiatrists, Clinical Psychologists, Parent-infant Psychotherapists, therapeutically
trained Nurses and Social Workers, Child Counsellors and Systemic Family and Couples
Therapists.