peri-implantitis treatment with autogenous bone17 treatment of peri-implantitis using open flap...
TRANSCRIPT

The Journal of Implant & Advanced Clinical Dentistry
Volume 5, No. 1 JaNaury 2013
Peri-Implantitis Treatment with
Autogenous Bone
Intrusion of Maxillary Anterior Teeth with Mini Implants
PROVEN.PREFERRED.
CONSISTENT.
TRUSTWORTHY.PREDICTABLE.
RELIABLE.
CERTAIN.GUARANTEED.POSITIVE.
TESTED.
COST-EFFECTIVE.
EXCELLENT.A GAME CHANGER. RELEVANT. GREAT. USER-FRIENDLY.
IDEAL.TIME-
SAVING.
REMARKABLE.
EFFECTIVE.SUCCESSFUL.
DEPENDABLE.STABLE.
SURE.
OUTSTANDING.
osteogenics.com | 888.796.1923
Big words for such a small membrane, but Cytoplast™ TXT-200 Singles
have lived up to those words from your colleagues for more than 15 years.
“
Advancing the science of dental implant treatmentThe aim at Neoss has always been to provide an implant solution for dental professionals enabling treatment in the most safe, reliable and successful manner for their patients.
The Neoss Esthetiline Solution is the first to provide seamless restorative integration all the way through from implant placement to final crown restoration. The natural profile developed during healing is matched perfectly in permanent restorative components; Titanium and Zirconia prepapble abutments, custom abutments and copings and CAD-CAM solutions.
Neoss Inc., 21860 Burbank Blvd. #190, Woodland Hills, CA 91367 Ph. 866-626-3677 www.neoss.com
Esthetiline- the complete anatomicalrestorative solution

PROVEN.PREFERRED.
CONSISTENT.
TRUSTWORTHY.PREDICTABLE.
RELIABLE.
CERTAIN.GUARANTEED.POSITIVE.
TESTED.
COST-EFFECTIVE.
EXCELLENT.A GAME CHANGER. RELEVANT. GREAT. USER-FRIENDLY.
IDEAL.TIME-
SAVING.
REMARKABLE.
EFFECTIVE.SUCCESSFUL.
DEPENDABLE.STABLE.
SURE.
OUTSTANDING.
osteogenics.com | 888.796.1923
Big words for such a small membrane, but Cytoplast™ TXT-200 Singles
have lived up to those words from your colleagues for more than 15 years.
“
Advancing the science of dental implant treatmentThe aim at Neoss has always been to provide an implant solution for dental professionals enabling treatment in the most safe, reliable and successful manner for their patients.
The Neoss Esthetiline Solution is the first to provide seamless restorative integration all the way through from implant placement to final crown restoration. The natural profile developed during healing is matched perfectly in permanent restorative components; Titanium and Zirconia prepapble abutments, custom abutments and copings and CAD-CAM solutions.
Neoss Inc., 21860 Burbank Blvd. #190, Woodland Hills, CA 91367 Ph. 866-626-3677 www.neoss.com
Esthetiline- the complete anatomicalrestorative solution

ACE Surgical Supply Co., Inc • 1034 Pearl Street, Brockton, MANobelBiocare™ and NobelReplace® are trademarks of Nobel Biocare Services AG. • Zimmer® and Tapered Screw-Vent® are registered trademarks of of Zimmer Dental, USA
Familiar Confidence.The infinity System allows you to place our implants with the familiar confidence you get from your existing system.
Sensible Compatibility. Designed to work with your existing implant system, you have the flexibility to use your existing surgical drills, drivers, and prosthetics to place and restore the implant.
Endless Opportunities.You will notice one difference with the infinity Implant...pricing. We are committed to delivering a compatible implant at pricing that creates significant opportunities for both you and your patients.
Give us a call today to experience infinity!
acesurgical.com 1.800.441.3100
A L L N E W F R O M
E x p a n d a b l E b O n E G r a F t i n G C O m p O S i t E
Compressed
Expanded
NuOssXC™ the latest development in natural bone substitutes:• Supports bone growth in periodontal and oral maxillofacial defects. • Is a composite grafting material comprised of mineralized de-proteinated bovine granules
and purified type I bovine collagen.• When placed into a bleeding site, the material expands to a predetermined size and shape.• Available in sinus form and socket form, which is supplied pre-loaded in a delivery syringe.Features and Benefits:• Expanding composite material allows for placement in a compressed form with self-expansion
to fill the entire defect upon hydration.• Simple implantation technique.• Composite nature of the material enhances graft stability and minimizes particulate migration.• Optimizes spacing between particulate to allow for bone ingrowth .Expansion time: Immediately upon contact with blood source or by hydration with sterile saline after implantation.
NuOss XC™ Socket NuOss XC™ Sinus
each infinity implant only
tri-camSurgically compatible with NobelBiocare™ NobelReplace®
internal hexSurgically compatible with Zimmer® Tapered Screw-Vent®

Built-in platform shiftingDual-function prosthetic connection
Bone-condensing property
Adjustable implant orientation for optimal final placement
High initial stability, even in compromised
bone situations
NobelActive™
A new direction for implants.
Nobel Biocare USA, LLC. 22715 Savi Ranch Parkway, Yorba Linda, CA 92887; Phone 714 282 4800; Toll free 800 993 8100; Tech. services 888 725 7100; Fax 714 282 9023Nobel Biocare Canada, Inc. 9133 Leslie Street, Unit 100, Richmond Hill, ON L4B 4N1; Phone 905 762 3500; Toll free 800 939 9394; Fax 800 900 4243Disclaimer: Some products may not be regulatory cleared/released for sale in all markets. Please contact the local Nobel Biocare sales office for current product assortment and availability. Nobel Biocare, the Nobel Biocare logotype and all other trademarks are, if nothing else is stated or is evident from the context in a certain case, trademarks of Nobel Biocare.
NobelActive equally satisfies surgical and restorative clinical goals. NobelActive thread design progressively condenses bone with each turn during insertion, which is designed to enhance initial stability. The sharp apex and cutting blades allow surgical clinicians to adjust implant orientation for optimal positioning of the prosthetic
connection. Restorative clinicians benefit by a versatile and secure internal conical prosthetic connec-tion with built-in platform shifting upon which they can produce excellent esthetic results. Based on customer feedback and market demands for NobelActive, theproduct assortment has been expanded – dental professionals will
now enjoy even greater flexi bility in prosthetic and implant selection. Nobel Biocare is the world leader in innovative evidence-based dental solutions. For more information, con-tact a Nobel Biocare Representative at 800 322 5001 or visit our website.
www.nobelbiocare.com/nobelactive
© N
ob
el B
ioca
re S
ervi
ces
AG
, 2
01
1.
All
rig
hts
res
erve
d.
TIUNITE® SURFACE,
10-YEAR EXPERIENCE
New data confi rm
long-term stability.
NOW AVAILABLE
WITH NOBELGUIDE™
64_NA2010_8125x10875.indd 1 8/1/11 1:37:30 PM

Autoclavable LED's Progressive Pedal Controlled Power
- Three times more power than PIEZOTOME1! (60 watts vs 18 watts of output power in the handpiece) Procedures are faster than ever, giving you a clean and effortless cut- NEWTRON LED and PIEZOTOME2 LED Handpieces output 100,000 LUX!- Extremely precise irrigation flow to avoid any risk of bone necrosis- Selective cut: respect of soft tissue (nerves, membranes, arteries) - Less traumatic treatment: reduces bone loss and less bleeding- 1st EVER Autoclavable LED Surgical Ultrasonic Handpieces - Giant user-friendly 5.7" color touch-control screen - Ultra-sharp, robust and resistant tips (30+ Surgical & 80+ Conventional)
PIEZOTOME2 and IMPLANT CENTER2
- I-Surge Implant Motor (Contra-Angles not included)- Compatible with all electric contra-angles (any ratio)- Highest torque of any micro-motor on the market- Widest speed range on the market
All the benefits of the PIEZOTOME2...PLUS...
ACTEON North America 124 Gaither Drive, Suite 140 Mount Laurel, NJ 08054Tel - (800) 289 6367 Fax - (856) 222 4726
www.us.acteongroup.com E-mail: [email protected]
..
.
The Journal of Implant & Advanced Clinical Dentistry • 5
The Journal of Implant & Advanced Clinical DentistryVolume 5, No. 1 • JaNuary 2013
Table of Contents
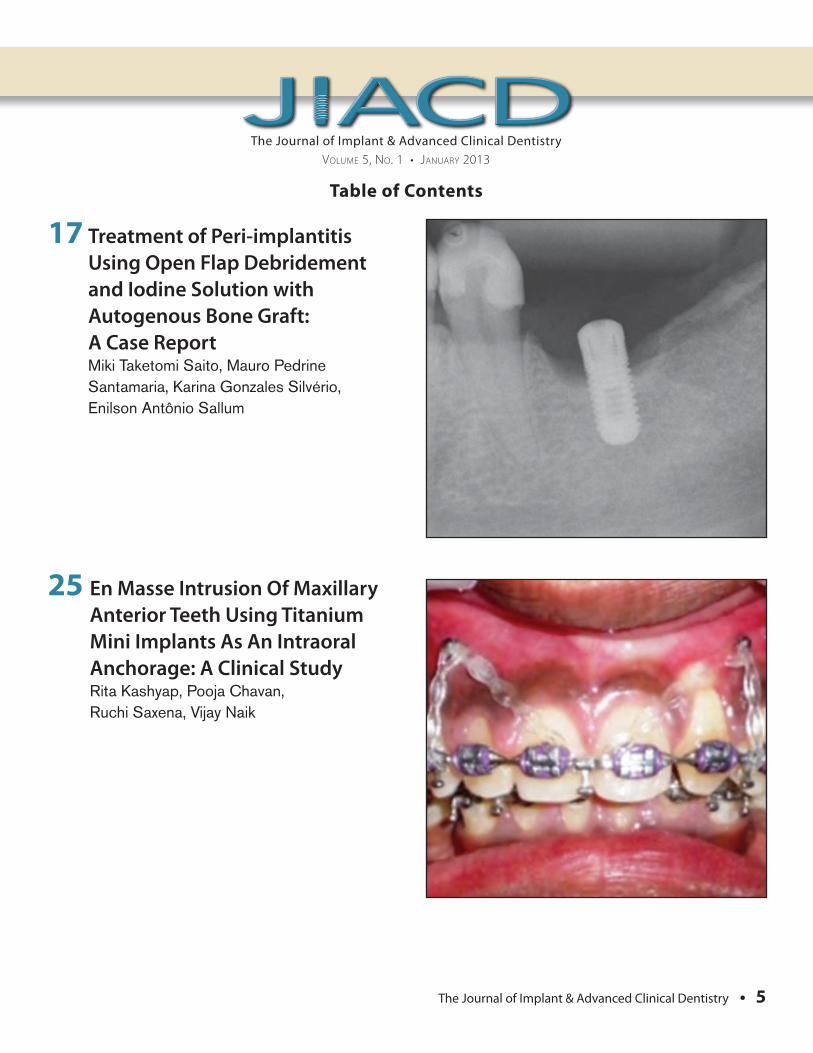
17 Treatment of Peri-implantitis Using Open Flap Debridement and Iodine Solution with Autogenous Bone Graft: A Case Report Miki Taketomi Saito, Mauro Pedrine Santamaria, Karina Gonzales Silvério, Enilson Antônio Sallum
25 En Masse Intrusion Of Maxillary Anterior Teeth Using Titanium Mini Implants As An Intraoral Anchorage: A Clinical Study Rita Kashyap, Pooja Chavan, Ruchi Saxena, Vijay Naik
GUIDOR® Bioresorbable Matrix BarrierBarrier function is maintained for 6 weeks after surgery and gradually degrades until the matrix is fully absorbed in 6 to 12 months.
IndicationsThe use of GUIDOR to aid in bone regeneration and augmentation should be limited to defects and concavities within skeletal contours and to defects/situations where moderate increase of bone volume beyond the skeletal contours is desirable. In all cases, appropriate space making support should be used.
ContraindicationsGUIDOR is contraindicated in those situations where general periodontal surgery should not be performed. Currently there are no known additional contraindications to the use of GUIDOR.
For Excellent predictability and ease of use in GBR
PrecautionsGUIDOR is not intended for use in cases other than those described under indications and has not been clinically tested in patients with extra large defects, for extensive bone augmentation, or for use in the treatment of failing implants.
GUIDOR has not been clinically tested in pregnant women or in immunocompromised patients (patients with diabetes, HIV, undergoing chemotherapy or irradiation).
Adverse ReactionsPossible complications following any oral surgery include thermal sensitivity, �ap sloughing, some loss of crestal bone height, abscess formation, infection, pain, and complications associated with the use of anesthesia; the patient may experience minor discomfort for a few days.
GUIDOR has not been clinically tested in pregnant women or in immunocompromised patients (patients with diabetes, HIV, undergoing chemotherapy or irradiation).
Adverse ReactionsPossible complications following any oral surgery include thermal sensitivity, �ap sloughing, some loss of crestal bone height, abscess formation, infection, pain, and complications associated with the use of anesthesia; the patient may experience minor discomfort for a few days.
1 2
©2010 Sunstar Americas, Inc. GDR10038 10272010 V1
GUIDOR® has a double layered matrix with two uniquely perforated layers:
The two layers are separated by inner spacers (1) to form an interspace (2) into which tissues can grow.
ORDER TODAY! 1-877-GUIDOR1 (1-877-484-3671)
www.GUIDOR.comORDER TODAY! 1-877-GUIDOR1 (1-877-484-3671)
SPECIAL PROMOTION!Buy 3 P3s get 1 P3 FREE!*
A $90.00Value
SSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSS
15.00mm
5090P3 - 15mm x 20mm Matrix Barrier
20.0
0mm
*This o�er ends 1/31/11
The Journal of Implant & Advanced Clinical Dentistry • 7
The Journal of Implant & Advanced Clinical DentistryVolume 5, No. 1 • JaNuary 2013
Table of Contents
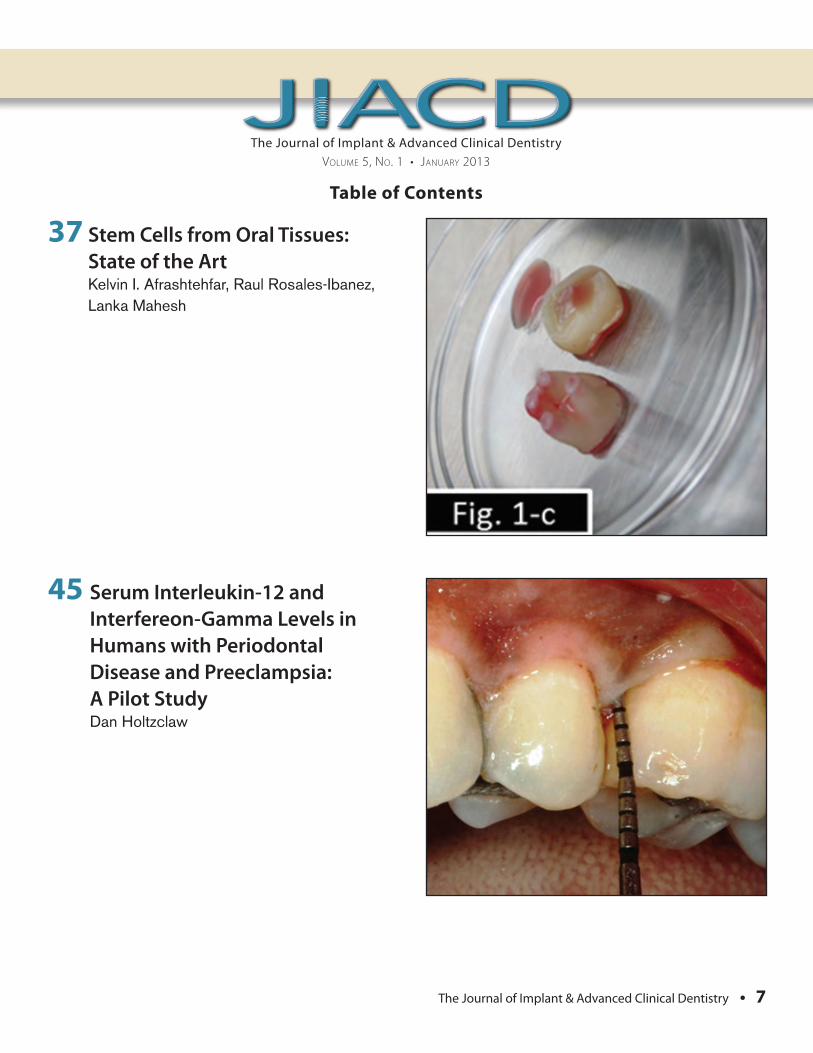
37 Stem Cells from Oral Tissues: State of the Art Kelvin I. Afrashtehfar, Raul Rosales-Ibanez, Lanka Mahesh
45 Serum Interleukin-12 and Interfereon-Gamma Levels in Humans with Periodontal Disease and Preeclampsia: A Pilot Study Dan Holtzclaw

IntroducIng
Less pain for your patients.1
Less chair side time for you.1
Mucograft® is a pure and highly biocompatible porcine collagen matrix. The spongious nature of Mucograft® favors early vascularization and integration of the soft tissues. It degrades naturally, without device related inflammation for optimal soft tissue regeneration. Mucograft® collagen matrix provides many clinical benefits:
For your patients...
Patients treated with Mucograft® require 5x less Ibuprofen than
those treated with a connective tissue graft1
Patients treated with Mucograft® are equally satisfied with esthetic outcomes when compared to connective tissue grafts2
For you...
Surgical procedures with Mucograft® are 16 minutes shorter in duration on average when compared to those involving connective tissue grafts1
Mucograft® is an effective alternative to autologous grafts3, is ready to use and does not require several minutes of washing prior to surgery
For full prescribing information, please visit us online at www.osteohealth.com or call 1-800-874-2334
References: 1Sanz M, et. al., J Clin Periodontol 2009; 36: 868-876. 2McGuire MK, Scheyer ET, J Periodontol 2010; 81: 1108-1117. 3Herford AS., et. al., J Oral Maxillofac Surg 2010; 68: 1463-1470. Mucograft® is a registered trademark of Ed. Geistlich Söhne Ag Fur Chemische Industrie and are marketed under license by Osteohealth, a Division of Luitpold Pharmaceuticals, Inc. ©2010 Luitpold Pharmaceuticals, Inc. OHD240 Iss. 10/2010
Mucograft® is indicated for guided tissue regeneration procedures in periodontal and recession defects, alveolar ridge reconstruction for prosthetic treatment, localized ridge augmentation for later implantation and covering of implants placed in immediate or delayed extraction sockets. For full prescribing information, visit www.osteohealth.com
Ask about our limited time, introductory special!

Scan With YourSmartphone!
In order to scan QR codes,your mobile device
must have a QR codereader installed.
Wan
t Reg
ener
ative
Trea
tmen
t Sol
utio
ns?
Try A
n Oss
eoGua
rd® M
embr
ane
And
Endo
bon
® Xeno
graf
t
Granu
les!
OsseoGuard® Membranes And Endobon® Xenograft Granules Provide Clinicians One Solution At A Time
Protect Sites For Consistent Results During
Grafting Procedures
Choose Between Two Levels Of Drapability For Ease Of Use In
Various Clinical Scenarios
Slow Resorption ForBone Volume Retention
Conveniently PackagedIn NEW Value Packs
For More InformationAbout BIOMET 3iRegenerative Treatment Solutions, Contact YourLocal Sales Representative Today! In the USA: 1-888-800-8045, Outside The USA: +1-561-776-6700 Or Visit Us Online At www.biomet3i.com
Endobon, OsseoGuard and RegenerOss are registered trademarks of BIOMET 3i LLC.OsseoGuard Flex and Providing Solutions - One Patient At A Time are trademarks ofBIOMET 3i LLC. ©2011 BIOMET 3i LLC.
ClinicallyManageable
Value Packs
Bone Volume
MaintenancePredictable
INTRODUCING
Join Us
Follow Us
Watch Us
DownloadIt
Regenerative Treatment Solutions
NEWPACKAGING
NEWOsseoGuard Flex™
Membrane
OsseoGuard® Membrane And The NEW OsseoGuard Flex™ Membrane
Endobon® Xenograft GranulesWith NEW Packaging
JIACD_Jan2012_BIOMET 3i 12/16/11 5:10 PM Page 1

Click For Our Quantity
Discount Options
www.exac.com/QuantityDiscountOptions
© 2
012
Exac
tech
, Inc
.
Oralife is a single donor grafting product processed in accordance with AATB standards as well as state and federal regulations (FDA and the states of Florida, California, Maryland and New York). Oralife allografts are processed by LifeLink Tissue Bank and distributed by Exactech Inc.1. Data on file at Exactech. 2. McAllister BS, Hagnignat K. Bone augmentation techniques. J Periodontal. 2007 Mar; 78(3):377-96. 3. Blum B, Moseley J, Miller L, Richelsoph K, Haggard W. Measurement of bone morphogenetic proteins and
other growth factors in demineralized bone matrix. Orthopedics. 2004 Jan;27(1 Suppl):s161-5.
What’s Your Sign?
www.exac.com/dental1-866-284-9690
• Cost-effectivegraftingmaterial
• Validatedtomaintainosteoinductivityand biomechanical integrity1
• MixtureofDBMwithmineral-retained cortical and cancellous chips, processed in a manner to retainthenaturally-occuringgrowthfactors(BMP)andbeaconductivelattice – all in one product1,2,3
NEW Oralife Plus Combination Allograft available now!
MEET OUR
PlusA QUALITY COMBINATION
The Journal of Implant & Advanced Clinical Dentistry • 11
The Journal of Implant & Advanced Clinical DentistryVolume 5, No. 1 • JaNuary 2013
PublisherSpecOps Media, LLC
DesignJimmydog Design Group www.jimmydog.com
Production ManagerStephanie Belcher 336-201-7475 • [email protected]
Copy EditorJIACD staff
Digital ConversionNxtBook Media
Internet ManagementInfoSwell Media
Subscription Information: Annual rates as follows: Non-qualified individual: $99(USD) Institutional: $99(USD). For more information regarding subscriptions, contact [email protected] or 1-888-923-0002.
Advertising Policy: All advertisements appearing in the Journal of Implant and Advanced Clinical Dentistry (JIACD) must be approved by the editorial staff which has the right to reject or request changes to submitted advertisements. The publication of an advertisement in JIACD does not constitute an endorsement by the publisher. Additionally, the publisher does not guarantee or warrant any claims made by JIACD advertisers.
For advertising information, please contact:[email protected] or 1-888-923-0002
Manuscript Submission: JIACD publishing guidelines can be found at http://www.jiacd.com/author-guidelines or by calling 1-888-923-0002.
Copyright © 2013 by SpecOps Media, LLC. All rights reserved under United States and International Copyright Conventions. No part of this journal may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying or any other information retrieval system, without prior written permission from the publisher.
Disclaimer: Reading an article in JIACD does not qualify the reader to incorporate new techniques or procedures discussed in JIACD into their scope of practice. JIACD readers should exercise judgment according to their educational training, clinical experience, and professional expertise when attempting new procedures. JIACD, its staff, and parent company SpecOps Media, LLC (hereinafter referred to as JIACD-SOM) assume no responsibility or liability for the actions of its readers.
Opinions expressed in JIACD articles and communications are those of the authors and not necessarily those of JIACD-SOM. JIACD-SOM disclaims any responsibility or liability for such material and does not guarantee, warrant, nor endorse any product, procedure, or technique discussed in JIACD, its affiliated websites, or affiliated communications. Additionally, JIACD-SOM does not guarantee any claims made by manufact-urers of products advertised in JIACD, its affiliated websites, or affiliated communications.
Conflicts of Interest: Authors submitting articles to JIACD must declare, in writing, any potential conflicts of interest, monetary or otherwise, that may exist with the article. Failure to submit a conflict of interest declaration will result in suspension of manuscript peer review.
Erratum: Please notify JIACD of article discrepancies or errors by contacting [email protected]
JIACD (ISSN 1947-5284) is published on a monthly basis by SpecOps Media, LLC, Saint James, New York, USA.

DID YOU KNOW?Roxolid implants deliver more treatment options
Roxolid is optimal for treatment of narrow interdental spaces.
Case courtesy of Dr. Mariano Polack and Dr. Joseph Arzadon, Gainesville, VA
Contact Straumann Customer Service at 800/448 8168 to learn more about Roxolid or to locate a representative in your area.
www.straumann.us
The Journal of Implant & Advanced Clinical Dentistry • 13
Tara Aghaloo, DDS, MDFaizan Alawi, DDSMichael Apa, DDSAlan M. Atlas, DMDCharles Babbush, DMD, MSThomas Balshi, DDSBarry Bartee, DDS, MDLorin Berland, DDSPeter Bertrand, DDSMichael Block, DMDChris Bonacci, DDS, MDHugo Bonilla, DDS, MSGary F. Bouloux, MD, DDSRonald Brown, DDS, MSBobby Butler, DDSNicholas Caplanis, DMD, MSDaniele Cardaropoli, DDSGiuseppe Cardaropoli DDS, PhDJohn Cavallaro, DDSJennifer Cha, DMD, MSLeon Chen, DMD, MSStepehn Chu, DMD, MSD David Clark, DDSCharles Cobb, DDS, PhDSpyridon Condos, DDSSally Cram, DDSTomell DeBose, DDSMassimo Del Fabbro, PhDDouglas Deporter, DDS, PhDAlex Ehrlich, DDS, MSNicolas Elian, DDSPaul Fugazzotto, DDSDavid Garber, DMDArun K. Garg, DMDRonald Goldstein, DDSDavid Guichet, DDSKenneth Hamlett, DDSIstvan Hargitai, DDS, MS
Michael Herndon, DDSRobert Horowitz, DDSMichael Huber, DDSRichard Hughes, DDSMian Iqbal, DMD, MSJames Jacobs, DMDZiad N. Jalbout, DDSJohn Johnson, DDS, MSSascha Jovanovic, DDS, MSJohn Kois, DMD, MSDJack T Krauser, DMDGregori Kurtzman, DDSBurton Langer, DMDAldo Leopardi, DDS, MSEdward Lowe, DMDMiles Madison, DDSLanka Mahesh, BDSCarlo Maiorana, MD, DDSJay Malmquist, DMDLouis Mandel, DDSMichael Martin, DDS, PhDZiv Mazor, DMDDale Miles, DDS, MSRobert Miller, DDSJohn Minichetti, DMDUwe Mohr, MDTDwight Moss, DMD, MSPeter K. Moy, DMDMel Mupparapu, DMDRoss Nash, DDSGregory Naylor, DDSMarcel Noujeim, DDS, MSSammy Noumbissi, DDS, MSCharles Orth, DDSAdriano Piattelli, MD, DDSMichael Pikos, DDSGeorge Priest, DMDGiulio Rasperini, DDS
Michele Ravenel, DMD, MSTerry Rees, DDSLaurence Rifkin, DDSGeorgios E. Romanos, DDS, PhDPaul Rosen, DMD, MSJoel Rosenlicht, DMDLarry Rosenthal, DDSSteven Roser, DMD, MDSalvatore Ruggiero, DMD, MDHenry Salama, DMDMaurice Salama, DMDAnthony Sclar, DMDFrank Setzer, DDSMaurizio Silvestri, DDS, MDDennis Smiler, DDS, MScDDong-Seok Sohn, DDS, PhDMuna Soltan, DDSMichael Sonick, DMDAhmad Soolari, DMDNeil L. Starr, DDSEric Stoopler, DMDScott Synnott, DMDHaim Tal, DMD, PhDGregory Tarantola, DDSDennis Tarnow, DDSGeza Terezhalmy, DDS, MATiziano Testori, MD, DDSMichael Tischler, DDSTolga Tozum, DDS, PhDLeonardo Trombelli, DDS, PhDIlser Turkyilmaz, DDS, PhDDean Vafiadis, DDSEmil Verban, DDSHom-Lay Wang, DDS, PhDBenjamin O. Watkins, III, DDSAlan Winter, DDSGlenn Wolfinger, DDSRichard K. Yoon, DDS
Editorial Advisory Board
Founder, Co-Editor in ChiefDan Holtzclaw, DDS, MS
Founder, Co-Editor in ChiefNicholas Toscano, DDS, MS
The Journal of Implant & Advanced Clinical Dentistry
DID YOU KNOW?Roxolid implants deliver more treatment options
Roxolid is optimal for treatment of narrow interdental spaces.
Case courtesy of Dr. Mariano Polack and Dr. Joseph Arzadon, Gainesville, VA
Contact Straumann Customer Service at 800/448 8168 to learn more about Roxolid or to locate a representative in your area.
www.straumann.us
www.dentalplanit.com/microsite
Guided implant dentistry without software investment.
Use promocode JIACDPA when placing a PlanAssist order. Offer valid until September 30th 2011. SurgiGuide® voucher valid for up to 3 months from the PlanAssist order date.
More info on this
summer deal?
Buy 1 PlanAssist ($517)
Get 1 FREE SurgiGuide®

All-Natural, Bioactive Products Designed to Stimulate the Healing Process
Biopsy of DynaMatrix
treated site
Biopsy of autogeneous gingival graft
Keystone Dental, Inc.144 Middlesex TurnpikeBurlington, MA 01803 USACall: 1-866-902-9272 / Fax: [email protected]
Outside the USA
Call: +1-781-328-3490Fax: +1-781-328-3400
www.keystonedental.com
• As an ECM, DynaMatrix retains both the 3-dimensional structure and the signaling proteins important for soft tissue regeneration1
• The signaling proteins (growth factors, glycoproteins, glycosaminoglycans) communicate with the body to help stimulate the natural healing process2
DynaMatrix® Extracellular Membrane is the only intact extracellular matrix (ECM) designed to remodel soft tissue.
• Accell has nearly 5 times more BMPs than DBM alone and each lot is validated for osteoinductive properties 3,4
• Accell in delivered as an easy-to-handle putty in a pre-fi lled syringe
• Accell is the only allograft product that contains this powerful combination of DBM, BMPs and Growth Factors
1 Hodde J, Janis A, Ernst D, et al. “Effects of sterilization on an extracellular matrix scaffold: part I. Composition and matrix architecture.” J Mater Sci Mater Med. 2007;18(4):537-543.
2 Hodde JP, Ernst DM, Hiles MC.”An investigation of the long-term bioactivity of endogenous growth factor in OASIS Wound Matrix.” J Wound Care. 2005 Jan;14(1):23-5.
3. Effective Design of Bone Graft Materials Using Osteoinductive and Osteoconductive Components. Kay, JF; Khaliq, SK; Nguyen, JT. Isotis Orthobiologics, Irvine, CA (abstract).
4. Amounts of BMP-2, BMP-4, BMP-7 and TGF-ß1 contained in DBM particles and DBM extract. Kay, JF; Khaliq, SK; King, E; Murray,SS; Brochmann, EJl. Isotis Orthobiologics, Irvine, CA (white paper/abstract).
Accell is an all-natural concentration of Bone Morphogenetic Proteins (BMPs) and Growth Factors with Demineralized Bone Matrix (DBM) that directs and charges stem cells to acclerate the body’s natural healing response.

Wilcko et al
Peri-implantitis is characterized by bone destruction around dental implants due to the host immune-inflamma-
tory response induced by biofilm accumula-tion. Several approaches have been proposed to treat peri-implantitis, including mechanic debridement, antimicrobial therapy, and resec-tive or regenerative surgical therapy. The pres-ent case report describes a peri-implantitis case treated by a surgical open flap debride-ment, decontamination of the implant surface
with povidone-iodine and fill of the adjacent osseous defect with autogenous bone graft. After 20-month follow-up, the pocket depth reduction and radiographic fill of the defect could be observed. Therefore, it can be con-cluded that this therapeutic approach could promote clinical and radiographic improve-ments to the patient. However, more random-ized controlled clinical trials are necessary for further understanding about the best approaches for the treatment of peri-implantitis.
Treatment of Peri-implantitis Using Open Flap Debridement and Iodine Solution with
Autogenous Bone Graft: A Case Report
Miki Taketomi Saito, DDS1 • Mauro Pedrine Santamaria, DDS, MS, PhD2
Karina Gonzales Silvério, DDS, MS, PhD,1 Enilson Antônio Sallum, DDS, MS, PhD, Professor3
1. Assistant Professor, Department of Prosthodontics and Periodontics, Division of Periodontics, Piracicaba Dental School, University of Campinas - UNICAMP, São Paulo, Brazil.
2. Assistant Professor Department of Periodontology, College of Dentistry, State University of São Paulo - UNESP, São José dos Campos, São Paulo, Brazil.
3. Professor, Department of Prosthodontics and Periodontics, Division of Periodontics, Piracicaba Dental School, University of Campinas - UNICAMP, São Paulo, Brazil.
Abstract
KEY WORDS: Peri-implantitis, dental implants, guided bone regeneration
The Journal of Implant & Advanced Clinical Dentistry • 17

18 • Vol. 5, No.1 • January 2013
IntRODuctIOnPeri-implant diseases are characterized by inflammatory lesions that involve tissues around dental implants, which is a result of biofilm accumulation. They can be classified into peri-implant mucositis or peri-implanti-tis.1 Peri-implant mucositis corresponds to an inflammatory reaction in the implant surround-ing soft tissues, whereas peri-implantitis is the inflammation of the soft tissues and involves the loss of supporting bone around an implant.2,3 Clinically, this inflammation is detected by the presence of bleeding on probing;1 other clini-cal signs (e.g., suppuration, redness, and swell-ing) may be observed.4 Radiographs may be required to evaluate bone loss around implants due to peri-implantitis and differentiate it from the normal bone remodeling.5 In studies about peri-implantitis prevalence, the reported esti-mate is that it occurs in about 28%6,7 to 56%8 of individuals and between 12%7 and 43%8 of the implants. Therefore, the peri-implantitis treatment is a topic of increasing interest. How-ever, only a few studies have provided data on the prevalence of peri-implant diseases; there-fore, these data may be underestimated.3,9
For treating peri-implant mucositis, the non-surgical mechanic therapy is effective in reducing the tissue inflammation; the adjunc-tive use of antimicrobial mouth rinse can improve the results of this therapy.10 With respect to peri-implantitis, the non-surgical mechanic therapy has not demonstrated to be equally effective.10 Therefore, surgical therapies have been proposed for treating peri-implan-titis, including open flap debridement as well as resective or regenerative approaches.3,11
Although some studies are aimed at
establishing protocols treatment for peri-implantitis, there is no consensus about the best way to perform the implant surface debridement, decontamination, and regen-eration of the bone defect.12 In this con-text, the aim of the present paper is to report a case of peri-implantitis treated with a sur-gical approach of open flap debridement for implant surface decontamination with iodine solution associated with a regenera-tive approach using autogenous bone graft.
cASE REPORtA 43-year-old white male, presenting a good general medical condition was referred to the Graduate Clinic of the Piracicaba Dental School reporting bad breath as chief complaint. He also reported he had difficulty maintaining hygiene on a dental implant placed 2 years before, as well as bleeding in this area. Clinical examina-tion revealed a dental implant (replacing the inferior left first molar) that has never received crown reconstruction; the implant presented a probing depth (PD) of 5 mm and bleeding on probing (BoP). Additionally, there was a bridle that made proper implant cleaning very demand-ing (Figure 1). Radiographs showed a crater-like peri-implant bone defect (3 mm) involving three implant screws (Figure 2). Thus, the diag-nosis of peri-implantitis was established. The patient was informed about his problem and all the treatment options for the case; thereaf-ter, he consented for the treatment as follows.
The initial treatment consisted of oral hygiene instructions, mechanical treatment with intrasulcular brushing and subgingival 10% povidone-iodine Riodeine® (Rioquímica™, São José do Rio Preto, SP, Brazil) irrigation,
Saito et al

The Journal of Implant & Advanced Clinical Dentistry • 19
which was performed during 5 to 7 minutes in a single session. Despite the improvement of the general oral hygiene observed afterwards, the dental implant still showed inflammation
signs after 1-month of follow-up. Then, a sur-gical approach was proposed for implant sur-face decontamination and filling of peri-implant defect with autogenous bone graft. Under local
Figure 1: Initial clinical aspect of the dental implant that was diagnosed with peri-implantitis.
Figure 2: Initial radiographic aspect of the dental implant that was diagnosed with peri-implantitis.
Figure 3: Peri-implant defect visualization after mucoperiosteal flap elevation. Note the presence of extensive granulation tissue.
Figure 4: Peri-implant defect visualization after granulation tissue removal.
Saito et al

20 • Vol. 5, No.1 • January 2013
anesthesia Alphacaine® (DFL™, Rio de Janeiro, RJ, Brazil), two incisions were made mesi-ally and distally to the dental implant; a muco-periosteal flap was raised to allow implant and bone defect visualization (Figure 3). After com-plete granulation tissue removal, the implant surface and bone defect could be observed (Figure 4). The implant surface decontamina-tion was performed using gauze soaked with 10% povidone-iodine. Afterward, autogenous bone graft was obtained from an adjacent area and placed into the peri-implant defect to cover all implant screws (Figure 5). The flap was then repositioned and sutured (Nylon 5.0, Ethicon™, São José dos Campos, SP, Brasil). After this surgical procedure, the patient was instructed to take analgesics (500 mg sodium dipyrone every 6 h for 2 d) and to discontinue toothbrushing around the surgical site for 15 days after surgery. During this period, plaque
control was achieved with a 0.12% chlorhexi-dine rinse twice a day. After this period, gentle toothbrushing with a soft-bristle toothbrush was allowed. Sutures were removed after 7 days; the patient was enrolled in a periodontal main-tenance program (i.e., professional plaque con-trol and oral hygiene instruction) weekly during the first month, then monthly during the con-secutive months. After 20-mouth follow-up, a reduction of probing depth to 3 mm and radio-graphic bone fill could be observed (Figure 6).
DIScuSSIOnBecause of the similarities between the inflam-matory diseases induced by biofilm accumula-tion on teeth and implants, some approaches that have been proposed to treat peri-implant diseases were initially based on previous evi-dences for treatments of periodontal dis-eases.10 In this context, the primary goal of
Figure 5: Peri-implant defect filled with autogenous bone graft obtained from adjacent area.
Figure 6: Radiographic aspect in 20-month follow-up after regenerative surgical approach suggesting defect bone filling.
Saito et al

The Journal of Implant & Advanced Clinical Dentistry • 21
peri-implant disease treatment is the reduc-tion of microbial challenge and control of the inflammatory reaction to re-establish a healthy peri-implant tissue.13 The therapeu-tic modalities for peri-implantitis comprise a non-surgical approach and surgical approach. The non-surgical approach includes mechani-cal debridement alone or combined with anti-septic agents or laser devices. The surgical approach includes open flap surgery that may be associated with resective or regenerative techniques. Although the non-surgical ther-apy could be effective for treating peri-implant mucositis, it does not seem to be as effective for peri-implantitis as it is for teeth.10 In peri-implantitis, the surgical approach has shown to perform better than non-surgical techniques.11,14
The surgical approach allows better access to defects and provides a better access for implant surface decontamination. In this con-text, the literature reports that only mechanical debridement on roughened implant surfaces contaminated with bacteria may have limited effect; the adjunctive use of chemical agents is recommended to improve treatment out-comes.12,15 However, there is no evidence in the literature to demonstrate a superior decontamination method.11 In order to decon-taminate the implant surface, a wide range of methods have been proposed in the litera-ture, such as mechanical debridement, the use of antiseptics/antibiotics and laser ther-apy.3,11 In an experimental study, the influence of the non-surgical approach associated with non-submerged healing and the surgi-cal approach associated with various implant surface decontamination methods (laser ther-apy; ultrasonic debridement; plastic curettes
associated with local application of metroni-dazole gel) and submerged healing was evalu-ated in peri-implantitis lesions in dogs.14 The authors observed that all treatments resulted in improvement of clinical parameters; however, the surgical approach associated with implant surface decontamination and submerged healing leads to better radiographic improve-ment. Moreover, when the specimens were evaluated histologically, surgical approaches also demonstrated better bone–implant con-tact compared to non-surgical approach.
In the present case, the surgical approach was performed and associated with decon-tamination of the implant surface using gauze soaked with 10% povidone-iodine solution. Povidone-iodine solution is considered an inex-pensive and nonhazardous broad-spectrum antiseptic that has been used as an adjunct in periodontal therapy; it has demonstrated by a systematic review that it may improve PD reduc-tion during scaling and root planing.16 The application of povidine-iodine with gauze was chosen to avoid damage to implant surface by metal curettes and ultrasonic tips or risk of sur-gical emphysema by air powder abrasives.11,13
Additionally, the correction of peri-implant defect should be one of the treatment objec-tives to allow efficient biofilm control by the patient and to eliminate micro-environments favorable for a pathogenic microbiota.3 The correction of these defects can be obtained by resective or regenerative techniques; how-ever, the latter are preferable because the ulti-mate goal of peri-implantitis treatment is to regenerate lost tissue11,17,18 and re-establish the osseointegration along the previously con-taminated implant surface.11,17 Autogenous
Saito et al

22 • Vol. 5, No.1 • January 2013
bone, xenografts, alloplastic materials and membranes have been used in regenerative techniques, which demonstrate variable lev-els of bone fill and re-osseointegration.11,17,18
In an animal model study, the regenerative treatments for bone defects around implants were evaluated. The defects were randomly assigned to receive the following: a bioabsorb-able membrane; a mineralized bone xenograft; or a combination of both. The results showed non-significant difference regarding the range of bone fill among all the three treatments.19 In a clinical study, the treatment of peri-implan-titis defects using autogenous bone grafts was evaluated in 25 implants diagnosed with peri-implantitis from 17 patients.18 During the observation period of up to 3 years, the use of autogenous bone graft demonstrated to be an efficacious treatment approach for restoring hard tissue lost by peri-implantitis. In another clinical study, three different techniques of bone regeneration in peri-implantitis lesions were compared: autogenous bone graft alone or associated with resorbable or non-resorbable barrier.20 At the 3-year follow-up evaluation, it was observed that all treatments revealed signif-icant improvement of peri-implant probing depth from baseline; however, differences in surgical approach did not affect the treatment outcome. Therefore, this study concluded that the addi-tional application of barrier does not improve the overall treatment outcome. This is in accor-dance with a case-control study comparing the use of a bone substitute alone or associated with a resorbable membrane with a follow-up over 3 years where no significant difference in defect bone fill was observed.21 The current lit-erature demonstrates no additional beneficial
effect on the use of membranes associated with grafts,11,19-21 membrane exposure as a frequent complication,11,20,22 and the use of autogenous bone graft is effective for treating peri-implant bone defects.18 Therefore, it was decided to use autogenous bone graft alone in the pres-ent case to avoid complications related to membrane exposure during the healing period.
Regarding the amount of defect bone fill, the chosen material as well as the peri-implant defect configuration are important and play a key role in treatment.11,23 A clinical study investigating the impact of defect con-figuration on the clinical outcome of surgical regenerative therapy using a xenograft in com-bination with a collagen membrane in peri-implantitis lesions demonstrated that intra-bony/circumferential defects tend to obtain higher improvements in probing depth reduction and clinical attachment level when compared with circumferential defects or semi-circumferential associated with buccal dehiscence at 6 and 12 month follow-up.23 In the present report, the peri-implant defect presented a favorable ana-tomical configuration. Despite a buccal bony dehiscence, the mesial, distal and lingual bone crest still remained in the level of the top of the implant, which could allow the autogenous graft placement and reposition of the mucoperi-osteal flap in an adequate position. The radio-graphic examination after 20 month follow-up reveals the defect filling (Figure 6). However, the radiographic image cannot elucidate the type of healing or if re-osseointegration has occurred in fact. Nevertheless, this result does not discredit the clinical benefits obtained in this case by the regenerative approach, such as probing depth reduction and peri-implant
Saito et al

The Journal of Implant & Advanced Clinical Dentistry • 23
defect filling, which can promote better con-ditions for adequate hygiene and a less favor-able environment for anaerobic pathogens.
cOncluSIOn The therapeutic approach for treatment of peri-implantitis using open flap debridement and iodine solution associated with autogenous bone graft was able to promote clinical and radiographic benefits in the case reported. How-ever, it is not established in the literature which is the most effective approach for the treat-ment of peri-implantitis. Therefore, randomized controlled clinical trials with long-term follow-up are necessary to elucidate this question. ●
correspondence:Miki Taketomi SaitoDept. of Prosthodontics and Periodontics, Division of Periodontics, Piracicaba Dental School, University of Campinas - UNICAMP, São Paulo, Brazil.Av. Limeira, n°. 901. Piracicaba. São Paulo. Brazil. P.O. Box 52.e-mail: [email protected]/ Fax: +55 19 2106-5301
DisclosureThe authors report no conflicts of interest with anything mentioned in this article.
References1. Zitzmann NU, Berglundh T. Definition and prevalence of peri-implant diseases.
J Clin Periodontol. Sep 2008;35(8 Suppl):286-291.2. Lindhe J, Meyle J. Peri-implant diseases: Consensus Report of the Sixth
European Workshop on Periodontology. J Clin Periodontol. Sep 2008;35(8 Suppl):282-285.
3. Esposito M, Grusovin MG, Coulthard P, Worthington HV. The efficacy of interventions to treat peri-implantitis: a Cochrane systematic review of randomised controlled clinical trials. Eur J Oral Implantol. Summer 2008;1(2):111-125.
4. Heitz-Mayfield LJ. Peri-implant diseases: diagnosis and risk indicators. J Clin Periodontol. Sep 2008;35(8 Suppl):292-304.
5. Adell R, Lekholm U, Rockler B, Branemark PI. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg. Dec 1981;10(6):387-416.
6. Fransson C, Wennstrom J, Berglundh T. Clinical characteristics at implants with a history of progressive bone loss. Clin Oral Implants Res. Feb 2008;19(2):142-147.
7. Fransson C, Lekholm U, Jemt T, Berglundh T. Prevalence of subjects with progressive bone loss at implants. Clin Oral Implants Res. Aug 2005;16(4):440-446.
8. Roos-Jansaker AM, Lindahl C, Renvert H, Renvert S. Nine- to fourteen-year follow-up of implant treatment. Part II: presence of peri-implant lesions. J Clin Periodontol. Apr 2006;33(4):290-295.
9. Berglundh T, Persson L, Klinge B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J Clin Periodontol. 2002;29 Suppl 3:197-212; discussion 232-193.
10. Renvert S, Roos-Jansaker AM, Claffey N. Non-surgical treatment of peri-implant mucositis and peri-implantitis: a literature review. J Clin Periodontol. Sep 2008;35(8 Suppl):305-315.
11. Claffey N, Clarke E, Polyzois I, Renvert S. Surgical treatment of peri-implantitis. J Clin Periodontol. Sep 2008;35(8 Suppl):316-332.
12. Kotsovilis S, Karoussis IK, Trianti M, Fourmousis I. Therapy of peri-implantitis: a systematic review. J Clin Periodontol. Jul 2008;35(7):621-629.
13. Schou S, Berglundh T, Lang NP. Surgical treatment of peri-implantitis. Int J Oral Maxillofac Implants. 2004;19 Suppl:140-149.
14. Schwarz F, Jepsen S, Herten M, Sager M, Rothamel D, Becker J. Influence of different treatment approaches on non-submerged and submerged healing of ligature induced peri-implantitis lesions: an experimental study in dogs. J Clin Periodontol. Aug 2006;33(8):584-595.
15. Mombelli A. Microbiology and antimicrobial therapy of peri-implantitis. Periodontol 2000. 2002;28:177-189.
16. Sahrmann P, Puhan MA, Attin T, Schmidlin PR. Systematic review on the effect of rinsing with povidone-iodine during nonsurgical periodontal therapy. J Periodontal Res. Apr 2010;45(2):153-164.
17. Renvert S, Polyzois I, Maguire R. Re-osseointegration on previously contaminated surfaces: a systematic review. Clin Oral Implants Res. Sep 2009;20 Suppl 4:216-227.
18. Behneke A, Behneke N, d’Hoedt B. Treatment of peri-implantitis defects with autogenous bone grafts: six-month to 3-year results of a prospective study in 17 patients. Int J Oral Maxillofac Implants. Jan-Feb 2000;15(1):125-138.
19. Nociti Junior FH, Caffesse RG, Sallum EA, Machado MA, Stefani CM, Sallum AW. Clinical study of guided bone regeneration and/or bone grafts in the treatment of ligature-induced peri-implantitis defects in dogs. Braz Dent J. 2001;12(2):127-131.
20. Khoury F, Buchmann R. Surgical therapy of peri-implant disease: a 3-year follow-up study of cases treated with 3 different techniques of bone regeneration. J Periodontol. Nov 2001;72(11):1498-1508.
21. Roos-Jansaker AM, Lindahl C, Persson GR, Renvert S. Long-term stability of surgical bone regenerative procedures of peri-implantitis lesions in a prospective case-control study over 3 years. J Clin Periodontol. Jun 2011;38(6):590-597.
22. Esposito M, Hirsch J, Lekholm U, Thomsen P. Differential diagnosis and treatment strategies for biologic complications and failing oral implants: a review of the literature. Int J Oral Maxillofac Implants. Jul-Aug 1999;14(4):473-490.
23. Schwarz F, Sahm N, Schwarz K, Becker J. Impact of defect configuration on the clinical outcome following surgical regenerative therapy of peri-implantitis. J Clin Periodontol. Mar 30 2010.
Saito et al

For more information, contact BioHorizonsCustomer Care: 1.888.246.8338 or shop online at www.biohorizons.com
SPMP12245 REV A SEP 2012
make the switch
The Tapered Plus implant system offers all the great benefits of BioHorizons highly successful Tapered Internal system PLUS it features a Laser-Lok treated beveled-collar for bone and soft tissue attachment and platform switching designed for increased soft tissue volume.
Laser-Lok® zoneCreates a connective tissue seal and maintains crestal bone
platform switchingDesigned to increase soft tissue volume around the implant connection
optimized threadformButtress thread for primary stability and maximum bone compression
prosthetic indexingConical connection with internal hex; color-coded for easy identification
Wilcko et al
Background: To evaluate efficacy of titanium mini implants as an effective means of anchorage for en masse intrusion of maxillary anterior teeth and to determine amount of intrusion achieved.
Materials and Methods: 10 subjects seeking orthodontic treatment in Department of Ortho-dontics, Institute of Dental Sciences, Belgaum, with deep bite requiring intrusion of maxillary anterior teeth. After initial alignment and level-ling, the maxillary arch was divided into one ante-rior segment and two posterior segments using 19 x 25 stainless steel arch wire. Mini implants between lateral incisor and canine were placed bilaterally and loaded immediately using pre-stretched elastic chains. Central incisor and canine linear vertical movement, and central inci-sor angular movement were evaluated before and after intrusion using lateral cephalograms.
Results: The amount of intrusion achieved for incisors was 2.90 + 0.84mm and canine was 3.05 + 0.64mm with axial inclination of inci-sors being relatively stable. Intrusion achieved was statistically as well as clinically signifi-cant (p < 0.01). The average duration of intru-sion was 3.75 + 0.85 months with a mean rate of intrusion of canine being 0.81mm/month and that of the incisors was 0.77mm/month.
Conclusion: Mini implants proved to be an efficient and stable source of anchorage for en masse intrusion of the six maxillary ante-rior teeth. The amount of intrusion of inci-sors and canine was statistically and clinically significant. However, long-term studies are required to evaluate the stability of the intru-sion achieved during the post treatment period.
En Masse Intrusion Of Maxillary Anterior Teeth Using Titanium Mini Implants As An Intraoral
Anchorage: A Clinical Study
Rita Kashyap, MDS1 • Pooja Chavan, MDS2 • Ruchi Saxena, MDS3 Vijay Naik, MDS4
1. Senior Lecturer, Department of Orthodontics, Bhojia Dental College and Hospital, Budh, Nalagarh, State: Himachal Pradesh-173205, Country: India.
2. Senior Lecturer, Department of Orthodontics, KLE Institute of Dental Sciences, KLE University, Belgaum. State: Karnataka-590010, Country: India.
3. Department of Orthodontics, Vydehi Institute of Dental Sciences & Research Centre, State: Bangalore, Country: India.
4. Professor, Department of Orthodontics, KLE Institute of Dental Sciences, KLE University, Belgaum, State: Karnataka-590010, Country: India.
Abstract
KEY WORDS: Orthodontics, anchorage, mini dental implants, occlusion
The Journal of Implant & Advanced Clinical Dentistry • 25

26 • Vol. 5, No. 1 • January 2013
IntRODuCtIOnDeep overbite is a common component of malocclu-sion in adults and children. It can be corrected with various treatment modalities, but the best option will depend on the patient’s characteristics and the treatment objectives. Esthetic considerations are also important in deep bite treatment. Nonsur-gical treatment alternatives include molar extru-sion, incisor intrusion, or a combination of both.1
Correction of deep bite by extrusion of poste-rior teeth is both more difficult to accomplish and less stable especially when it is performed on non-growing patients. Also deep bite with gummy smile would be improved by maxillary intrusion.2 Hence, true intrusion is often a desirable orthodontic tooth movement but limited principally by inadequate dental anchorage. When an arch wire develops an active intrusion force against the anterior teeth, it simultaneously develops an extrusive force and tip-back moment against the anchor molars. This reactive force and moment are opposed mainly by occlusal forces. In some instances, for exam-ple high angle cases, occlusal forces may be inadequate and the reactive forces of the anchor molars may cause downward and backward rota-tion of the mandible. In other cases, such as adult patients lacking posterior teeth for anchorage, orthodontic intrusion may not be a viable option.3
All intra-oral appliances show some degree of anchor loss while extra-oral appliances, although efficient, require extensive patient cooperation. Aesthetics and social issues are also a mat-ter of concern.4 Although endosseous implants, onplants, dental implants and miniplates have been used successfully for orthodontic anchor-age, their clinical applications are still limited. Mini-screws have recently been introduced as sim-pler alternatives with advantages of smaller size,
greater number of implant sites and indications, simpler surgical placement and removal, imme-diate loading and well tolerated by patients.5,6,7
When canines are in deep bite along with inci-sors, conventional methods cannot be used for intrusion of all the six anterior teeth, because en masse intrusion of six teeth is very difficult in terms of vertical anchorage as higher force values will be required. Thus incisor intrusion is done followed by separate canine intrusion. Various case reports have demonstrated the use of mini implants as a source of anchorage for maxillary incisor intru-sion2,8,9 either for intruding four upper incisors or for intruding two upper incisors. It is also stated that to provide anchorage during incisor intrusion, mini-screws can be placed between upper lateral inci-sors and canines.10 In a case report, mini-implants are used in severe Class II division 2 malocclusion to intrude all maxillary anterior teeth en masse in a single step and implants remained stable through-out treatment.11 Similar clinical study is done using implants as a source of anchorage for intru-sion of all the six teeth but had few limitations.12
Therefore, the present study was undertaken to evaluate whether titanium based mini-implants are really efficient as a rigid source of anchorage to achieve significant amount of intrusion of the six maxillary anterior teeth with the following objectives:1. To evaluate the efficacy of titanium mini
implants as an effective means of anchorage for en masse intrusion of maxillary anterior teeth.
2. To determine amount & rate of intrusion achieved of six anterior teeth.
MAtERIAlS AnD MEthODSTen subjects seeking orthodontic treatment in the Department Of Orthodontics And Dentofacial Orthopedics, Institute of Dental Sciences, Belgium
Kashyap et al

The Journal of Implant & Advanced Clinical Dentistry • 27
with deep bite requiring intrusion of maxillary ante-rior teeth were selected in the study with an informed consent. Patients with flared incisors were excluded.
The mini-implants were made by Denticon, Mumbai. They were self-drilling type, with 1.4mm diameter and 8 mm length. The site selected for the placement of implant was the alveolar bone between lateral incisor and canine at the level of attached gingiva. Availability of sufficient interdental bone and its density at implant site was assessed using panoramic x-rays, and intraoral periapical radio-graphs (IOPAs). A simplified stent13 for implant insertion was used with two L-shaped rectangular wires, facing each other, into the bracket slots adja-cent to the mini-screw site. IOPAs were taken to confirm proper position of the stent and corrected if required, for avoiding contact with dental roots. Implants were placed under local anesthesia. An IOPA was taken to confirm the position of implant. Lateral cephalograph was taken as a pre-intrusion record after implant placement. Ethical clear-ance for the same was obtained from the institute
.Clinical Set up (Figure 1)The maxillary dental arch was divided into one ante-rior segment (including six anterior teeth) and two posterior segments. A 19 x 25 stainless steel arch wire was placed in all the three segments. In the ante-rior segment, three crimpable hooks were placed, two between lateral incisor and canine bilaterally and one in between two central incisors. Implants were loaded immediately using pre-stretched short clear rabbit force elastomeric chain, placed in the form of M-configuration (stretched from crimpable hook between canine and lateral incisor on one side to the implant head, then to the hook between two central incisors, further to the implant head on contralateral side and finally to third hook).
A Dontrix gauge was used to measure the amount of force being applied. A total of 90 gm of intrusive force was applied to the six anterior teeth. The pre-stretched elastomeric chains were also extended from the maxillary molar hooks to the tags incorporated in wire segment distal to canines which delivered 25 gm of Class I force per side to prevent flaring. The patients were recalled every 4 weeks to change elastic chains. Stability of implants and oral hygiene were also checked and all measures were taken to minimize the possibility of soft tissue coverage and inflam-mation which could directly affect the retention of mini implants.14 After achievement of required intrusion, another lateral cephalogram was taken and implants were removed. Method of evaluating treatment changes: Two Lateral cephalometric radiographs taken immediately after the place-ment of implants and after intrusion of anterior segment were analyzed using three variables.
Cephalometric landmarks and planes used were as follows: (Figure 2)1. Anterior nasal plane(ANS)2. Posterior nasal plane(PNS)3. Incisor centroid(Ic)4. Canine centroid(Cc)5. PP- Palatal Plane- A line joining ANS- PNS6. UL1: Long axis of the maxillary incisor
Cephalometric measurements undertaken were:1. Maxillary central incisor vertical movement:
Ic – PP(mm) - Perpendicular distance between the incisor centroid and palatal plane. (Fig 3)
2. Maxillary central incisor angular movement: UL1 – PP(degree) - Angle between PP and long axis of the maxillary central incisor. (Fig 4)
Kashyap et al

28 • Vol. 5, No. 1 • January 2013
3. Maxillary canine vertical movement: Cc – PP(mm) - Perpendicular distance between the canine centroid and palatal plane. (Fig 5)The difference between pre and post intru-
sion cephalometric measurements was calcu-lated which provided data about linear intrusive movement of maxillary anteriors. The rate of intru-sion was derived by dividing the mean amount of intrusion of the anterior segment by the mean treatment time recorded in mm/ month.
The data obtained from the cephalomet-
ric measurements, was analyzed using descrip-tive statistics such as mean, standard deviation and inferential statistic such as paired ‘t’ test.
RESultSThe mean value of the difference of the pre and post intrusion value of variable Ic – PP (mm), was 2.90 + 0.84, which denotes the amount of incisor intrusion (Table 1), and for vari-able Cc – PP (mm), the difference was 3.05 + 0.64. The probability value and the ‘t’ value showed that the change in value was statisti-
Figure1a: Anterior segment (0.019’’ x 0.025’’ SS) with three crimpable hooks after implant placement.
Figure 1b: Elastic Chain in ‘M’ configuration used to apply intrusive force (45 gm/ side) from the implants to crimpable hooks.
Figure 1c: Distal force (25 gm) applied using elastic chain. (Right posterior segment).
Figure 1d: Distal force (25 gm) applied using elastic chain. (Left posterior segment).
Kashyap et al

The Journal of Implant & Advanced Clinical Dentistry • 29
Figure 2: Cephalometric Landmarks. Figure 3: Maxillary central incisor vertical movement: Ic – PP(mm) Perpendicular distance between the incisor centroid and palatal plane.
Figure 4: Maxillary central incisor angular movement: UL1
– PP(degree) Posterior-inferior angle between PP and long axis of the maxillary central incisor.
Figure 5: Maxillary canine vertical movement: Cc – PP(mm)Perpendicular distance between the canine centroid and palatal plane.
Kashyap et al
30 • Vol. 5, No. 1 • January 2013
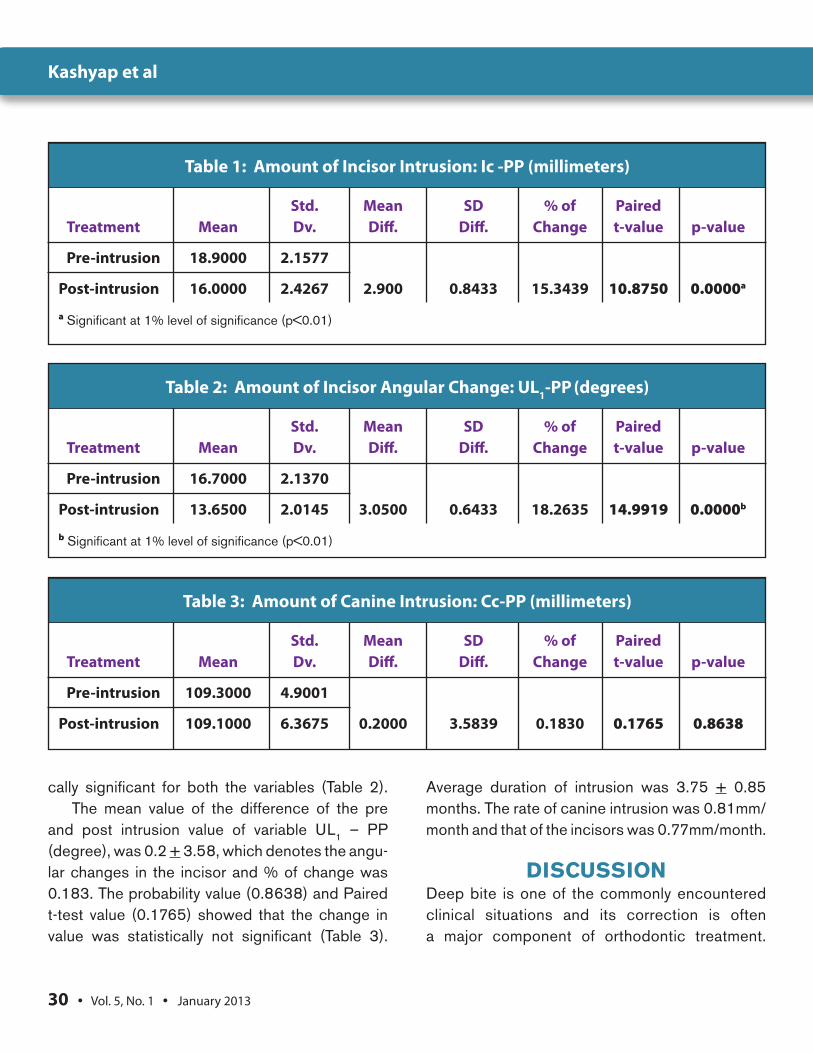
cally significant for both the variables (Table 2).The mean value of the difference of the pre
and post intrusion value of variable UL1 – PP (degree), was 0.2 + 3.58, which denotes the angu-lar changes in the incisor and % of change was 0.183. The probability value (0.8638) and Paired t-test value (0.1765) showed that the change in value was statistically not significant (Table 3).
Average duration of intrusion was 3.75 + 0.85 months. The rate of canine intrusion was 0.81mm/month and that of the incisors was 0.77mm/month.
DISCuSSIOnDeep bite is one of the commonly encountered clinical situations and its correction is often a major component of orthodontic treatment.
Table 1: Amount of Incisor Intrusion: Ic -PP (millimeters)
Std. Mean SD % of Paired Treatment Mean Dv. Diff. Diff. Change t-value p-value
Pre-intrusion 18.9000 2.1577
Post-intrusion 16.0000 2.4267 2.900 0.8433 15.3439 10.8750 0.0000a
a Significant at 1% level of significance (p<0.01)
Table 2: Amount of Incisor Angular Change: UL1-PP (degrees)
Std. Mean SD % of Paired Treatment Mean Dv. Diff. Diff. Change t-value p-value
Pre-intrusion 16.7000 2.1370
Post-intrusion 13.6500 2.0145 3.0500 0.6433 18.2635 14.9919 0.0000b
b Significant at 1% level of significance (p<0.01)
Table 3: Amount of Canine Intrusion: Cc-PP (millimeters)
Std. Mean SD % of Paired Treatment Mean Dv. Diff. Diff. Change t-value p-value
Pre-intrusion 109.3000 4.9001
Post-intrusion 109.1000 6.3675 0.2000 3.5839 0.1830 0.1765 0.8638
Kashyap et al
The Journal of Implant & Advanced Clinical Dentistry • 31
Review of the literature reveals a great contro-versy among the proponents of continuous arch and segmented arch leveling techniques. Various studies have shown that apart from some intru-sion and flaring of the anterior teeth, the continu-ous arch wire treatment predominantly caused deep bite correction by extrusive movement in molar area, concomitant with posterior (bite opening) rotation of the mandible. Also, the high initial vertical force levels resulted in an over-loading of the vertical anchorage. Incisor intru-sion with little extrusive movement in the molar area, however, is found with the segmented arch technique as recommended by Burstone.15,16
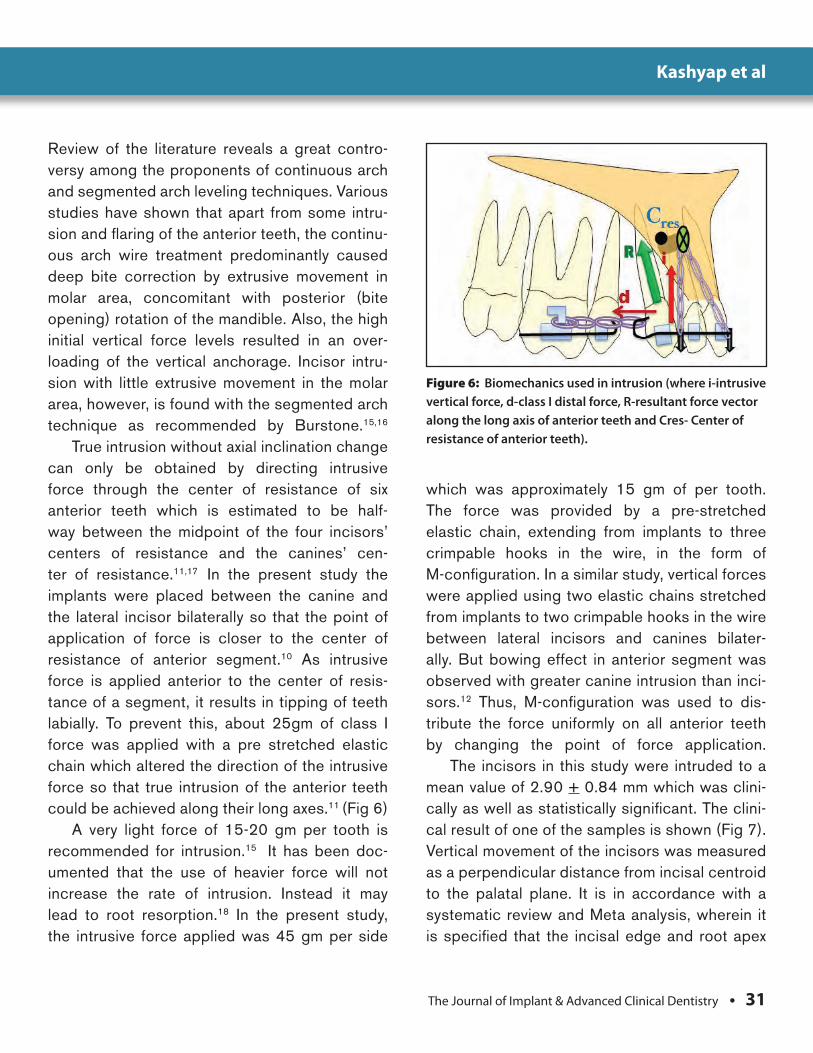
True intrusion without axial inclination change can only be obtained by directing intrusive force through the center of resistance of six anterior teeth which is estimated to be half-way between the midpoint of the four incisors’ centers of resistance and the canines’ cen-ter of resistance.11,17 In the present study the implants were placed between the canine and the lateral incisor bilaterally so that the point of application of force is closer to the center of resistance of anterior segment.10 As intrusive force is applied anterior to the center of resis-tance of a segment, it results in tipping of teeth labially. To prevent this, about 25gm of class I force was applied with a pre stretched elastic chain which altered the direction of the intrusive force so that true intrusion of the anterior teeth could be achieved along their long axes.11 (Fig 6)
A very light force of 15-20 gm per tooth is recommended for intrusion.15 It has been doc-umented that the use of heavier force will not increase the rate of intrusion. Instead it may lead to root resorption.18 In the present study, the intrusive force applied was 45 gm per side
which was approximately 15 gm of per tooth. The force was provided by a pre-stretched elastic chain, extending from implants to three crimpable hooks in the wire, in the form of M-configuration. In a similar study, vertical forces were applied using two elastic chains stretched from implants to two crimpable hooks in the wire between lateral incisors and canines bilater-ally. But bowing effect in anterior segment was observed with greater canine intrusion than inci-sors.12 Thus, M-configuration was used to dis-tribute the force uniformly on all anterior teeth by changing the point of force application.
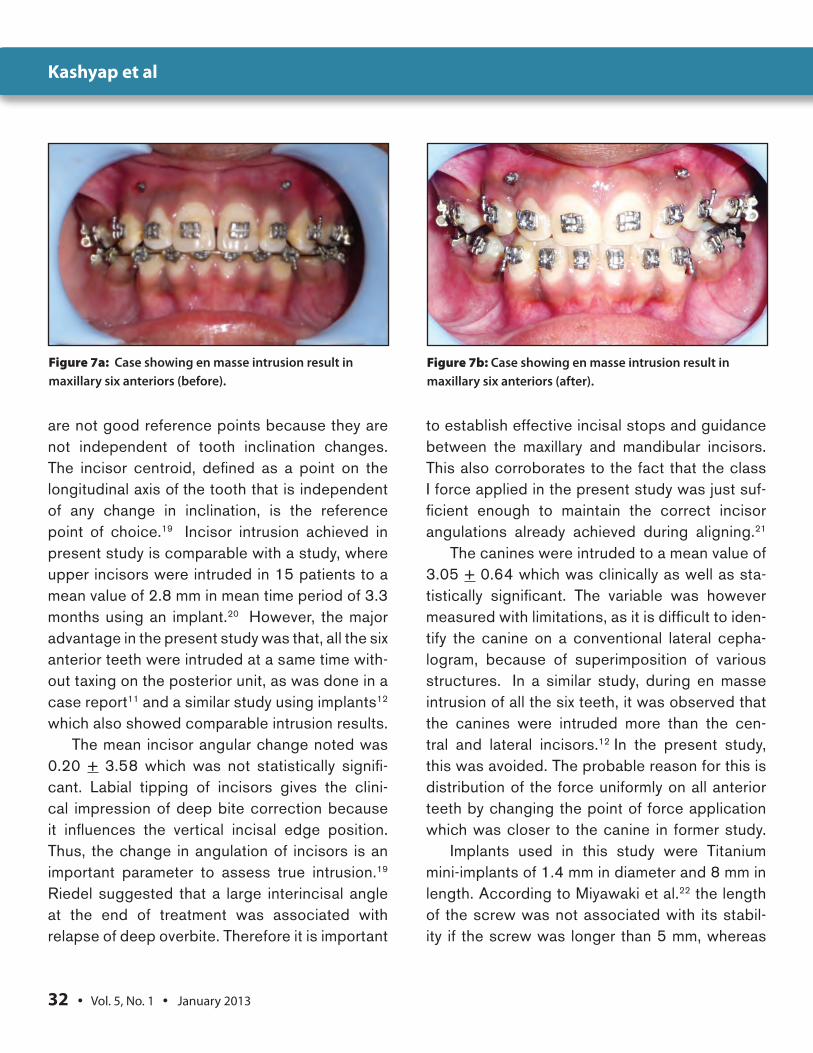
The incisors in this study were intruded to a mean value of 2.90 + 0.84 mm which was clini-cally as well as statistically significant. The clini-cal result of one of the samples is shown (Fig 7). Vertical movement of the incisors was measured as a perpendicular distance from incisal centroid to the palatal plane. It is in accordance with a systematic review and Meta analysis, wherein it is specified that the incisal edge and root apex
Figure 6: Biomechanics used in intrusion (where i-intrusive vertical force, d-class I distal force, R-resultant force vector along the long axis of anterior teeth and Cres- Center of resistance of anterior teeth).
Kashyap et al
32 • Vol. 5, No. 1 • January 2013
Figure 7a: Case showing en masse intrusion result in maxillary six anteriors (before).
Figure 7b: Case showing en masse intrusion result in maxillary six anteriors (after).
are not good reference points because they are not independent of tooth inclination changes. The incisor centroid, defined as a point on the longitudinal axis of the tooth that is independent of any change in inclination, is the reference point of choice.19 Incisor intrusion achieved in present study is comparable with a study, where upper incisors were intruded in 15 patients to a mean value of 2.8 mm in mean time period of 3.3 months using an implant.20 However, the major advantage in the present study was that, all the six anterior teeth were intruded at a same time with-out taxing on the posterior unit, as was done in a case report11 and a similar study using implants12 which also showed comparable intrusion results.
The mean incisor angular change noted was 0.20 + 3.58 which was not statistically signifi-cant. Labial tipping of incisors gives the clini-cal impression of deep bite correction because it influences the vertical incisal edge position. Thus, the change in angulation of incisors is an important parameter to assess true intrusion.19
Riedel suggested that a large interincisal angle at the end of treatment was associated with relapse of deep overbite. Therefore it is important
to establish effective incisal stops and guidance between the maxillary and mandibular incisors. This also corroborates to the fact that the class I force applied in the present study was just suf-ficient enough to maintain the correct incisor angulations already achieved during aligning.21
The canines were intruded to a mean value of 3.05 + 0.64 which was clinically as well as sta-tistically significant. The variable was however measured with limitations, as it is difficult to iden-tify the canine on a conventional lateral cepha-logram, because of superimposition of various structures. In a similar study, during en masse intrusion of all the six teeth, it was observed that the canines were intruded more than the cen-tral and lateral incisors.12 In the present study, this was avoided. The probable reason for this is distribution of the force uniformly on all anterior teeth by changing the point of force application which was closer to the canine in former study.
Implants used in this study were Titanium mini-implants of 1.4 mm in diameter and 8 mm in length. According to Miyawaki et al.22 the length of the screw was not associated with its stabil-ity if the screw was longer than 5 mm, whereas
Kashyap et al

The Journal of Implant & Advanced Clinical Dentistry • 33
the diameter of the screw was significantly asso-ciated with its stability. Screws ranging from 1.5 - 2 mm in diameter and 4 - 10 mm in length can potentially be in inter-radicular locations.23
All the implants showed primary stability upon insertion and were loaded immediately. Although some authors recommend a waiting period of about 2 weeks for soft tissue healing before applying orthodontic force, recent studies have proved that immediate loading can be done with no compromise in their stability because they rely on mechanical retention for the anchorage which is sufficient to sustain normal orthodontic loading.7,24 In the present study one mini implant showed clinical mobility after 3 months of its insertion. Patients included were observed peri-odically for periodontal complications but none showed any sign or symptom. So vitality test was not required at the start or during intrusion. The displacement of implant can harm the adjacent vital structures. Hence in a tooth-bearing area 2 mm of safety clearance should be allowed.24
Extrusion of the posterior segment is a com-mon side effect associated with conventional intrusion mechanics of the anterior teeth. Even with rigidly stabilized posterior units, only four teeth can be intruded at a time with conventional methods so as to keep undesirable forces and moments minimal.15 Since implants can with-stand high forces of as much as 450g,25 the intrusion of all the six teeth was attempted with-out adversely affecting the molar position. This study has elucidated the clinical effectiveness of mini implants as a rigid source of anchorage for the purpose of en masse intrusion of maxil-lary anterior teeth in a single step. This approach not only eases the biomechanics involved, but also reduces the overall duration of intrusion.
Although implants can be used as anchor-age during intrusion, yet this decision should be based on risk benefit ratio and individu-alized treatment plan. Sample size is one of the limitations of the study presented. In this study main focus was on the amount of intru-sion achieved. However, long-term studies are required to evaluate the stability of the intru-sion achieved during the post treatment period.
COnCluSIOnThe following conclusions were drawn from the study:1. Mini implants proved to be an efficient and
stable source of anchorage for en masse intrusion of the six maxillary anterior teeth
2. The amount of intrusion achieved for both incisors (2.90 + 0.84mm) and canine (3.05 + 0.64) was statistically as well as clinically significant with axial inclina-tion of incisors being relatively stable.
3. The average duration for intrusion was 3.75 + 0.85 months, with the mean rate of canine intrusion at 0.81mm/ month and that of the incisors at the rate of 0.77mm/ month. ●
Correspondence:Dr. Rita Kashyap, Senior Lecturer Department: Orthodontics & Dentofacial Orthopedics, Bhojia Dental College and Hospital, Budh, Nalagarh,Himachal Pradesh-173205. India.e-mail: [email protected]: 09915229091
Kashyap et al

34 • Vol. 5, No. 1 • January 2013
Kashyap et al
ADVERTISEADVERTISE WITH
TODAY!
Reach more customers with the dental
profession’s first truly interactive
paperless journal!
Using recolutionary online technology, JIACD provides its readers with an
experience that is simply not available with traditional hard copy paper journals.
WWW.JIACD.COM
DisclosureThe authors report no conflicts of interest with anything mentioned in this article.
References1. Julia Ng, Paul W. Major, Giseon Heo, and Carlos Flores-Mird. True incisor
intrusion attained during orthodontic treatment: A systematic review and meta-analysis. Am J Orthod Dentofacial Orthop 2005;128: 212-9
2. Ohnishi H, Yagi T, Yasuda Y, Takada K. A mini-implant for Orthodontic anchorage in a deep overbite case. Angle Orthod 2005; 75: 444-52.
3. Southard T.E, Buckley M.T, Spivey J.D, Krizen K.E, Casko J.S. Intrusion anchorage potential of teeth versus rigid endosseous implants; A clinical and radiographic evaluation. Am J Orthod Dentofacial Orthop. 1995;107: 115-20.
4. Egolf RJ, Begole EA, Upshaw HS. Factors associated with orthodontic patient compliance with intraoral elastic and headgear wear. Am J Orthod Dentofacial Orthop 1990; 112: 512–18.
5. Eric J. W. Liou, Betty C. J. Pai, and James C. Y. Lin, Do miniscrews remain stationary under orthodontic forces? Am J Orthod Dentofacial Orthop. 2004;126:42-7
6. Shingo Kuroda et al. Clinical use of miniscrew implants as orthodontic anchorage:Success rates and postoperative discomfort. Am J Orthod Dentofacial Orthop.2007;131:9-15
7. Miano GB, Bednar J, Pagin P, Mura P. The spider screw for skeletal anchorage. J Clin Orthod. 2003; 37: 90- 97.
8. Creekmore TD, Eklund MK. The possibility of skeletal anchorage. J Clin Orthod.1983;17: 266-271
9. Kim, T, Kim H, Lee S. Correction of deep overbite and gummy smile by using a mini implant with a segmented wire in a growing class II division 2 patient. Am J Orthod Dentofacial Orthop 2006; 130: 676-85.
10. Carano A. StefanoV, Leone P, Siciliani G. Clinical application of the miniscrew anchorage system. J Clin orthod 2005;1:9-24
11. Upadhyay M, Nagaraj K, Yadav S, Saxena R. Mini-implants for en masse intrusion of maxillary anterior teeth in a severe Class II division 2 malocclusion. J Orthod. 2008 Jun; 35(2):79-89.
12. Ruchi S. A clinical evaluation of orthodontic mini implants as a source of intraoral anchorage for intrusion of maxillary anterior teeth. In press World J Orthod.
13. Kravitz, Kusnoto, Hohlt. A simplified stent for anterior miniscrew insertion. J Clin orthod 2007 apr;41(4):224-6.
14. Favero L, Brollo p, Bressan E. Orthodontic anchorage with specific fixtures: related study analysis. Am J Orthod Dentofac Orthop. 2002; 122: 84-94.
15. Burstone C J. Deep overbite correction by intrusion. AM J orthod. 1977; 72: 1-22.
16. Weiland FJ, Bantleon HP, Droschl H. Evaluation of continious arch and segmented arc leveling techniques in adult patients- a clinical study. Am J orthod Dentofacial Orthop. 1996; 110: 647- 652.
17. Melsen B, Fotis V, Burstone CJ. Vertical force considerations in differential space closure. J Clin Orthod 1990; 24: 678–83.
18. Melson B, Agerback N, Makenstamm G. Intrusion of incisors in adult patients with marginal bone loss. Am J Orthod Dentofac Orthop 1989 ; 96:232-41.
19. Julia Ng et al. True incisor intrusion attained during orthodontic treatment: A systematic review and meta-analysis. Am J Orthod Dentofacial Orthop 2005; 128: 212-9.
20. R Mittal, Anand K Patil, Sanjay v Ganeshkar. Correction of deep overbite with Mini-implants using a 2 x 4 appliance design in adult patients: A prospective clinical study. Cyber J Orthod. 2009
21. Riedel RA. A review of the retention problem. Angle Orthod 1960; 30: 179–94.
22. Miyaki S, Koyana I, Inove M, Mishama K, Sughara T, Yamamoto T. Factors associated with the stability of titanium screws placed in the posterior region for orthodontic anchorage, Am J Orthod Dentofacial Orthop. 2003; 124: 373-8.
23. Huja SS, Litsky AS, Beck FH, Johnson KA, Larsen PE. Pull out strength of mono cortical screws placed in the maxillae and mandible of dogs. Am J Orthod. 2005; 127: 307-13.
24. Liou EJW, Pai BCJ, James CY. Do mini screws remain stationary under orthodontic forces. Am J Orthod Orthop.2004; 126: 42-7.
25. Kyung HM, Park HS, Bae SM, Sung JH, Kim B. Development of orthodontic micro implants for intraoral anchorage. J clin orthod; 2003; 37: 321-328.
Kashyap et al
PLANMECA®
ProMax® 3D Max
Introducing thePLANMECA® ProMax® 3D
Max...
PLANMECA®
• Automatically adjusts volume sizesfor childrenWhen the child patient size is selected, the fields of view(volume sizes) and the dosage parameters areslightly reduced
• More than 36 pre-programmed targetsFrom a single tooth scan to the whole skull, theProMax 3D Max has 18 pre-programmed targets,5 adult fields of view, 5 child fields of view, and more
• Patented SCARA technology allowslimitless imaging possibilities
• Full view, open patient positioning forstanding, sitting, and wheelchair accessibility
• Space savingA small footprint and compact design make theProMax 3D Max the smallest large FOV on the market
• High resolution, flat panel technology
• Now compatible with Mac OS environment
Features• 5 selectable, single scan fields of viewMost common uses:ø5 x 5.5 cm - Individual tooth or other point of interestø10 x 5.5 cm - Mandible or maxillaø10 x 9 cm - Mandible and maxillaø10 x 13 cm - Mandible or maxilla and sinusø23 x 16 cm - Full maxillofacial image, upper or lower skull
• The smallest and largest fields of view onthe market giving the ProMax 3D Max moreversatility then any other comparableX-ray unit
• Large view, single acquisition - dual scanfor full maxillofacial and skull imagingø23 x 26 - Full skull covers the whole head and istherefore extremely useful for surgical and orthodonticprocedures, as well as TMJ, ear, sinus, and airwaystudies. Using the large volume size, it is possible togenerate a 2D cephalometric image with asingle mouse click.
For more information onPLANMECA ProMax 3D Max
please call...
1-630-529-2300or visit us on the web @www.planmecausa.com
Planmeca ProMax3dMax_JAIC102710:Layout 1 10/27/10 4:37 PM Page 1

© MIS Corporation. All rights Reserved.
INNOVATION
MIS offers a wide range of innovative kits and accessories that provide creative and simple solutions for the varied challenges encountered in implant dentistry. To learn more about MIS visit our website: misimplants.com or call us:
866-797-1333 (toll-free)
MIS’ Complete Prosthetic Kit (CPK) contains the components you need to restore a "straightforward" implant case.
The offer cannot be combined with other offers. Free items may not be returned or exchanged.*First time MIS user ?Ask for our free implant delivery system.
It’s Free. Just Ask for It !
Purchase any MIS implants in multiples of 5 (minimum 10 implants) and receive one free CPK - Complete Prosthetic Kit, with each implant.
M a k e i t S i m p l eUSA
®

Wilcko et al
This brief review is an update about adult stem cells obtained from oral tissues and their therapeutic use
through tissue engineering techniques in
order to produce the tissues needed to repair/regenerate, from bone or tooth tis-sue lost to an entire bioengineered tooth.
Stem Cells from Oral Tissues: State of the Art
Kelvin I. Afrashtehfar, DDS. FADI1 • Raul Rosales-Ibanez, DDS, PhD2
Lanka Mahesh, BDS, MBA3
1. Private practice, Quebec, Canada.
2. Researcher Professor, Tissue Engineering Research Group, Faculty of Stomatology, UASLP. San Luis Potosi, Mexico.
3. Private practice, New Delhi, India.
Abstract
KEY WORDS: Stem cells, dental progenitor cells, tissue engineering, periodontal regeneration.
The Journal of Implant & Advanced Clinical Dentistry • 37

38 • Vol. 5, No. 1 • January 2013
INTRODUCTIONThe stem cell studies in recent years have been considered the most advanced type of medical-scientific research and early results have aroused great expectations.1 Also in dentistry many studies were performed with the final aim of obtaining new bone and new teeth.2 Tooth maladies are wide-spread in industrial countries; for example, approx-imately two thirds of German citizens suffer from periodontal disease, which is a frequent cause of tooth loss.3 When permanent teeth are damaged or lost, they do not regenerate therefore, compro-mises oral health. Although several clinical thera-pies to solve tooth loss problems, such as artificial denture and dental implants, there are consid-eration about safety and treatment time issues.4
Scientists in the field of regenerative medicine and tissue engineering are now applying the prin-ciples of cell transplantation, material science, and bioengineering to construct biological substitutes
that will restore and maintain normal function in diseased and injured tissues.5 Tissue engineering aims to stimulate the body either to regenerate tis-sue on its own or to grow tissue outside the body which can then be implanted as natural tissue. The tooth tissue engineering field has evolved rapidly because of the advantages that would represent to health.4 Stem cell biology provides promis-ing methods in vitro as well as in vivo in animal models which make speculation about a future application in human dentistry reasonable6 and is thought to be a promising way to replace the missing tooth.4 Stem cells are cells which divide to produce one stem cell and one cell capable of differentiation even as necessity demands.6
Stems cells classified into embryonic and adult or post-natal. The use of embryonic stem cells which are pluripotent generates many ethi-cal concerns regarding the consumption of blas-tocystes.7-9 This makes adult stem cells a more
Figure 1a: Dental pulp. Figure 1b: SHED is pointed by blue arrow.
Afrashtehfar et al
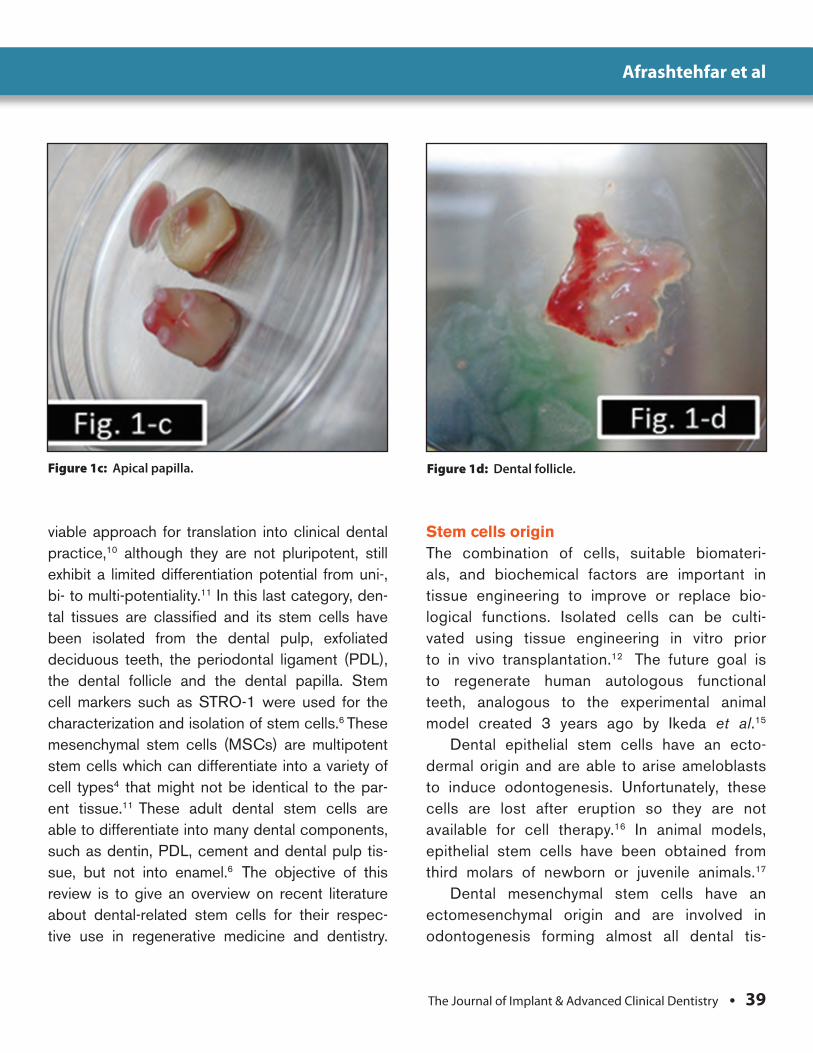
The Journal of Implant & Advanced Clinical Dentistry • 39
viable approach for translation into clinical dental practice,10 although they are not pluripotent, still exhibit a limited differentiation potential from uni-, bi- to multi-potentiality.11 In this last category, den-tal tissues are classified and its stem cells have been isolated from the dental pulp, exfoliated deciduous teeth, the periodontal ligament (PDL), the dental follicle and the dental papilla. Stem cell markers such as STRO-1 were used for the characterization and isolation of stem cells.6 These mesenchymal stem cells (MSCs) are multipotent stem cells which can differentiate into a variety of cell types4 that might not be identical to the par-ent tissue.11 These adult dental stem cells are able to differentiate into many dental components, such as dentin, PDL, cement and dental pulp tis-sue, but not into enamel.6 The objective of this review is to give an overview on recent literature about dental-related stem cells for their respec-tive use in regenerative medicine and dentistry.
Stem cells origin The combination of cells, suitable biomateri-als, and biochemical factors are important in tissue engineering to improve or replace bio-logical functions. Isolated cells can be culti-vated using tissue engineering in vitro prior to in vivo transplantation.12 The future goal is to regenerate human autologous functional teeth, analogous to the experimental animal model created 3 years ago by Ikeda et al.15
Dental epithelial stem cells have an ecto-dermal origin and are able to arise ameloblasts to induce odontogenesis. Unfortunately, these cells are lost after eruption so they are not available for cell therapy.16 In animal models, epithelial stem cells have been obtained from third molars of newborn or juvenile animals.17
Dental mesenchymal stem cells have an ectomesenchymal origin and are involved in odontogenesis forming almost all dental tis-
Figure 1c: Apical papilla. Figure 1d: Dental follicle.
Afrashtehfar et al

40 • Vol. 5, No. 1 • January 2013
sues with the exeption of enamel.9 Mesenchy-mal stem cells can differentiate into nerve, muscle, fat, cartilage or even bone cells.6
Non-dental stem cells are multipotent cells that can also regenerate dental tissue.18 They have been harvested from embryonic oral epi-thelium, human bone marrow, odontomas, hair follicles, adipose and dermal tissue.6
Dental Pulp Stem Cells – DPSCsThese DPSCs display similar features as bone-marrow-derived mesenchymal stem cells (BMSCs). That is why both cell types adhere to plastic and are colony-forming cells. In contrast to bone-marrow-derived cells, DPSCs were found to differentiate into odontoblast-like cells. These cells also shared characteristics of osteo-blast-like cells. Since 2008, BMSCs are being used in humans in sinus augmentation proce-dures,19 suggesting that DPSCs might work as well being less invasive when extraction is indi-cated according to the dental Implant treatment.
A DNA microarray study could distinguish DPSCs from bone-marrow-derived mesenchy-mal stem cells,20 where DPSCs differentially express cell-cycle-associated genes.21 In other study, DPSCs were also found to differentiate into adipocytes or neural-like cells.22 Fascinat-ingly, dental stem cells are located in the peri-vascular niche and express the stem cell marker Stro-1.23 Recently, a special stem cell popula-tion was isolated from the dental pulp.24 These cells can be induced to undergo uniform dif-ferentiation into smooth and skeletal muscle cells, neurons, cartilage and bone cells under chemically defined culture conditions. Stem cells derived from the dental pulp are often mentioned in recent discussions about regen-erative endodontics,25,26 inducing differentia-tion into odontoblasts similar to the therapy that induce tertiary dentin, giving a new approach to heal perforated roots.27 Dental pulp can be harvested from third molars or pulp-ectomized teeth left in situ,28 therefore some organ stor-age companies around the globe are taking advantage of these potential therapy alternative.
DPSCs while having an in vitro analy-sis may differentiate into osteo/dentinogenic, adipogenic, chondrogenic, myogenic and neurogenic cells.21,22 The ectopic tissue for-mation displayed in vivo is dentin-pulp-like complex, odontoblast-like cells29 and bone-like tissue with Haversian canals and liv-ing autologous fibrous bone tissue,30,31 besides promotes angiogenesis (Fig. 1a).32
Stem cells from Human Exfoliated Deciduous teeth – SHEDsSHEDs while having an in vitro analysis may differentiate into dentinogenic, adipogenic,
Figure 2: Periodontal ligament detached (arrowed).
Afrashtehfar et al
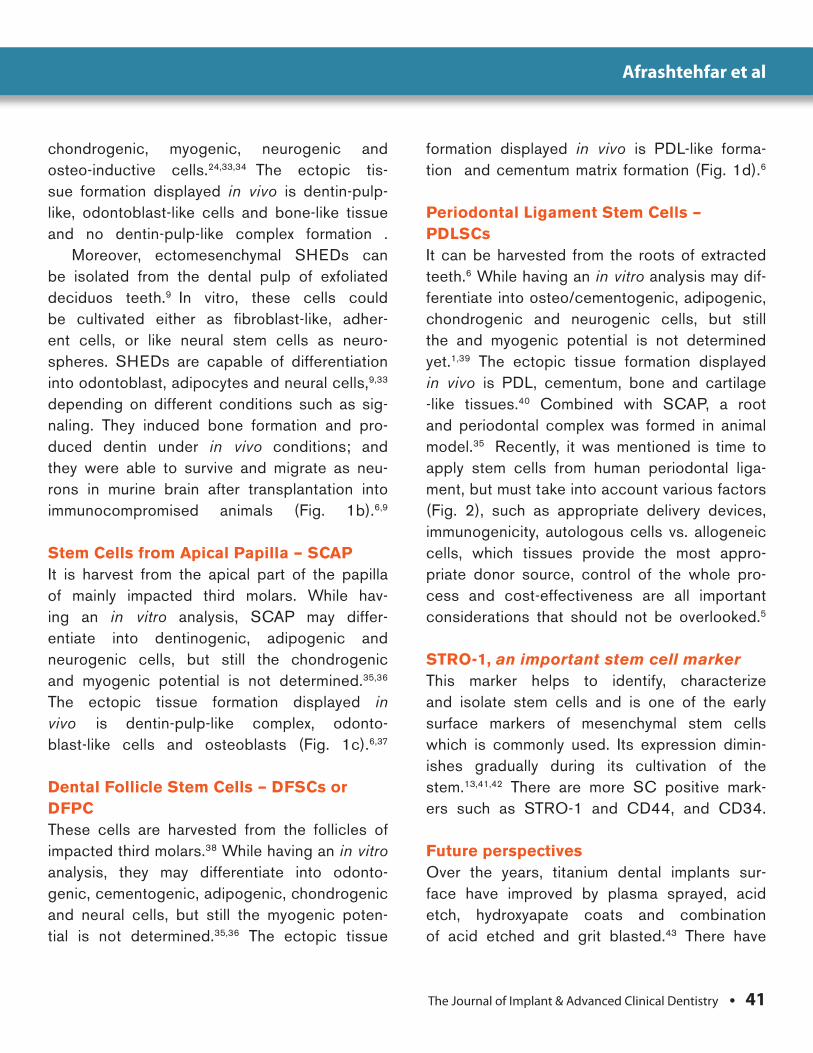
The Journal of Implant & Advanced Clinical Dentistry • 41
chondrogenic, myogenic, neurogenic and osteo-inductive cells.24,33,34 The ectopic tis-sue formation displayed in vivo is dentin-pulp-like, odontoblast-like cells and bone-like tissue and no dentin-pulp-like complex formation .
Moreover, ectomesenchymal SHEDs can be isolated from the dental pulp of exfoliated deciduos teeth.9 In vitro, these cells could be cultivated either as fibroblast-like, adher-ent cells, or like neural stem cells as neuro-spheres. SHEDs are capable of differentiation into odontoblast, adipocytes and neural cells,9,33 depending on different conditions such as sig-naling. They induced bone formation and pro-duced dentin under in vivo conditions; and they were able to survive and migrate as neu-rons in murine brain after transplantation into immunocompromised animals (Fig. 1b).6,9
Stem Cells from Apical Papilla – SCAPIt is harvest from the apical part of the papilla of mainly impacted third molars. While hav-ing an in vitro analysis, SCAP may differ-entiate into dentinogenic, adipogenic and neurogenic cells, but still the chondrogenic and myogenic potential is not determined.35,36 The ectopic tissue formation displayed in vivo is dentin-pulp-like complex, odonto-blast-like cells and osteoblasts (Fig. 1c).6,37
Dental Follicle Stem Cells – DFSCs or DFPCThese cells are harvested from the follicles of impacted third molars.38 While having an in vitro analysis, they may differentiate into odonto-genic, cementogenic, adipogenic, chondrogenic and neural cells, but still the myogenic poten-tial is not determined.35,36 The ectopic tissue
formation displayed in vivo is PDL-like forma-tion and cementum matrix formation (Fig. 1d).6
Periodontal Ligament Stem Cells – PDLSCsIt can be harvested from the roots of extracted teeth.6 While having an in vitro analysis may dif-ferentiate into osteo/cementogenic, adipogenic, chondrogenic and neurogenic cells, but still the and myogenic potential is not determined yet.1,39 The ectopic tissue formation displayed in vivo is PDL, cementum, bone and cartilage -like tissues.40 Combined with SCAP, a root and periodontal complex was formed in animal model.35 Recently, it was mentioned is time to apply stem cells from human periodontal liga-ment, but must take into account various factors (Fig. 2), such as appropriate delivery devices, immunogenicity, autologous cells vs. allogeneic cells, which tissues provide the most appro-priate donor source, control of the whole pro-cess and cost-effectiveness are all important considerations that should not be overlooked.5
STRO-1, an important stem cell markerThis marker helps to identify, characterize and isolate stem cells and is one of the early surface markers of mesenchymal stem cells which is commonly used. Its expression dimin-ishes gradually during its cultivation of the stem.13,41,42 There are more SC positive mark-ers such as STRO-1 and CD44, and CD34.
Future perspectivesOver the years, titanium dental implants sur-face have improved by plasma sprayed, acid etch, hydroxyapate coats and combination of acid etched and grit blasted.43 There have
Afrashtehfar et al

42 • Vol. 5, No. 1 • January 2013
been even intentions to combine osseointe-gration with stem cells for humans by bioengi-neered periodontal tissue formed on titanium implants. In 2010 was reported the develop-ment of clinically relevant methods for autolo-gous PDL regeneration on titanium implants.44
We might be close to accept the transi-tion from xenodontics (titanium implants), which will be considered in the category of traditional dentistry, to biodontics (tissue-engineered tooth derived from SC).4,15,45,46
CONCLUSIONThe adult dental stem cells can be used to regenerate different dental tissues. To regen-erate dentin or pulp tissue, DPSCs, SHEDs and SCAPs are suitable. The periodontium can be generated from PDLSCs or DFSCs.In a near future, it is possible that clinicians use these forms of tissue engineering to regenerate lost portions of the periodontium and teeth based on these concepts of tis-sues development. These types of therapeutic approaches based on tissue engineering and stem cell biology for organogenesis have con-siderable potential; even an entire tooth could be developed. The time is now ripe to move from animal studies to human clinical trials. ●
Correspondence:Dr. Lanka [email protected]
ATTENTION PROSPECTIVE
AUTHORSJIACD wants
to publish your article!
The Journal of Implant & Advanced Clinical Dentistry
For complete details regarding publication in
JIACD, please refer to our author guidelines at
the following link: http://www.jiacd.com/
authorinfo/ author-guidelines.pdf
or email us at: [email protected]
Afrashtehfar et al
The Journal of Implant & Advanced Clinical Dentistry • 43
Disclosure The authors report no conflicts of interest with anything mentioned in this article.
AcknowledgmentsThe first author would like to give special thanks to his dear friend and professor, Dr Raul Rosales-Ibanez, for his support and trust to continue future research studies together.
References1. Afrashtehfar KI, Zeron A. Potencial de regeneración
periodontal por medio de células progenitoras obtenidas del ligamento periodontal. Fac Med UNAM 2011; (in-press)
2. Giordano G, La Monaca G, Annibali S, Cicconetti A, Ottolenghi L. Stem cells from oral niches: a review. Ann Stomatol 2011; (1-2): 3-8.
3. Geerts SO, Legrand V, Charpentier J, Albert A, Rompen EH. Further evidence of the association between periodontal conditions and coronary artery disease. J Periodontol 2004; 75:1274–80.
4. Peng L, Ye L, Zhou XD. Mesenchymal stem cells and tooth engineering. Int J Oral Sci. 2009;1(1):6-12.
5. Hynes K, Menicanin D, Gronthos S, Bartold M. Clinical utility of stem cells for periodontal regeneration. Periodontol 2000 2012;59(1):203-27.
6. Ulmer FL, Winkel A, Kohorst P, Stiesch M. Stem Cells – Prospects in Dentistry. Schweiz Monatsschr Zahnmed 2010; 120:10:860-72.
7. Conrad C, Huss R. Adult stem cell lines in renegerative medicine and reconstructive surgery. J Surg Res. 2005; 124(2):201-8.
8. Cowan C A, Klimanskaya I, McMahon J, Atienza J, Witmyer J, Zucker J P, Wang S, Morton C C, McMahon A P, Powers D, Melton D A: Derivation of embryonic stem-cell lines from human blastocysts. N Engl J Med 2004;350: 1353–6.
9. Moore KL, Persaud TVN. The developing human: Clinically oriented embryology. Ed 8. Philadelphia: Elsevier; 2007.
10. Krebsbach PH, Robey PG. Dental and skeletal stem cells: potential cellular therapeutics for craniofacial regeneration. J Dent Educ. 2002; 66(6):766-73.
11. Morsczeck C, Reichert T E, Vollner F, Gerlach T, Driemel O. The state of the art in human dental stem cell research. Mund Kiefer Gesichtschir 2007;11: 259–66.
12. Gebhardt M, Murray PE, Namerow KN, Kuttler S, Garcia-Godoy F. Cell survival within pulp and periodontal constructs. J Endod 2009;35: 63–6.
13. Yang X, Walboomers X F, van den Dolder J, Yang F, Bian Z, Fan M, Jansen JA. Non-viral bone morphogenetic protein 2 transfection of rat dental pulp stem cells using calcium phosphate nanoparticles as carriers. Tissue Eng Part A 2008;14: 71–81.
14. Yang X, Yang F, Walboomers XF, Bian Z, Fan M, Jansen JA. The performance of dental pulp stem cells on nanofibrous PCL/gelatin/nHA scaffolds. J Biomed Mater Res A 2010;93(1):247-57.
15. Ikeda E, Morita R, Nakao K, Ishida K, Nakamura T, Takano-Yamamoto T, Ogawa M, Minuzo M, Kasugai S, Tsuji T. Fully functional bioengineered tooth replacement as an organ replacement therapy. PNAS 2009;106: 13475–80.
16. Ohazama A, Modino SA, Miletich I, Sharpe PT. Stem-cell-based tissue engineering of murine teeth. J Dent Res 2004;83: 518–22.
17. Honda M J, Shinohara Y, Hata K I, Ueda M. Subcultured odontogenic epithelial cells in combination with dental mesenchymal cells produce enamel-dentin-like complex structures. Cell Transplant 2007;16: 833–47.
18. Yokoi T, Saito M, Kiyono T, Iseki S, Kosaka K, Nishida E, Tsubakimoto T, Harada H, Eto K, Noguchi T, Teranaka T. Establishment of immortalized dental follicle cells for generating periodontal ligament in vivo. Cell Tissue Res 2007;327: 301–11.
19. Shayesteh Y S, Khojasteh A, Soleimani M, Alikhasi M, Khoshzaban A, Ahmadbeigi N. Sinus augmentation using human mesenchymal stem cells loaded into a beta-tricalcium phosphate/hydroxyapatite scaffold. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106: 203–9.
20. Shi S, Robey PG, Gronthos S. Comparison of human dental pulp and bone marrow stromal stem cells by cDNA microarray analysis. Bone 2001;29:532–9.
21. Gronthos S, Mankani M, Brahim J, Robey PG, Shi S. Postnatal human dental pulp stem cells (DPSCs) in vitro and in vivo. Proc Natl Acad Sci USA 2000;97:13625–30.
22. Gronthos S, Brahim J, Li W, Fisher LW, Cherman N, Boyde A, DenBesten P, Robey PG, Shi S. Stem cell properties of human dental pulp stem cells. J Dent Res 2002;81:531–5.
23. Shi S, Gronthos S. Perivascular niche of postnatal mesenchymal stem cells in human bone marrow and dental pulp. J Bone Miner Res 2003;18:696–704.
24. Kerkis I, Kerkis A, Dozortsev D, Stukart-Parsons GC, Massironi SM, Pereira LV, Caplan AI, Cerruti HF. Isolation and characterization of a population of immature dental pulp stem cells expressing OCT-4 and other embryonic stem cell markers. Cells Tissues Organs 2006; 184:105–16.
25. Murray PE, Garcia-Godoy F, Hargreaves KM. Regenerative endodontics: a review of current status and a call for action. J Endod 2007;33:377–90.
26. Sloan AJ, Smith AJ. Stem cells and the dental pulp: potential roles in dentine regeneration and repair. Oral Dis 2007;13:151–157
27. Prescott RS, Alsanea R, Fayad MI, Johnson BR, Wenckus CS, Hao J, John AS, George A. In vivo generation of dental pulp-like tissue by using dental pulp stem cells, a collagen scaffold, and dentin matrix protein 1 after subcutaneous transplantation in mice. J Endod 2008;34: 421–6.
28. d’Aquino R, De Rosa A, Laino G, Caruso F, Guida L, Rullo R, Checchi V, Laino L, Tirino V, Papaccio G. Human dental pulp stem cells: from biology to clinical applications. J Exp Zoolog B Mol Dev Evol 2009 Jul 15;312B(5):408-15.
29. El-Backly RM, Massoud AG, El-Badry AM, Sherif RA, Marei MK. Regeneration of dentine/pulplike tissue using a dental pulp stem cell/poly (lactic-co-glycolic) acid scaffold construct in New Zealand white rabbits. Aust Endod J 2008;34: 52–67.
30. Zhang W, Walboomers XF, Shi S, Fan M, Jansen JA. Multilineage differentiation potential of stem cells derived from human dental pulp after cryopreservation. Tissue Eng 2006; 12: 2813–23.
31. Laino G, d’Aquino R, Graziano A, Lanza V, Carinci F, Naro F, Pirozzi G, Papaccio G. A new population of human adult dental pulp stem cells: a useful source of living autologous fibrous bone tissue (LAB). J Bone Miner Res 2005;20: 1394–402.
32. d’Aquino R, Graziano A, Sampaolesi M, Laino G, Pirozzi G, De Rosa A, Papaccio G: Human postnatal dental pulp cells co-differentiate into osteoblasts and endotheliocytes: a pivotal synergy leading to adult bone tissue formation. Cell Death Differ 2007;14: 1162–71.
33. Miura M, Gronthos S, Zhao M, Lu B, Fisher LW, Robey PG, Shi S. SHED: stem cells from human exfoliated deciduous teeth. Proc Natl Acad Sci USA 2003;100:5807–12.
34. Seo BM, Sonoyama W, Yamaza T, Coppe C, Kikuiri T, Akiyama K, Lee JS, Shi S. SHED repair critical-size calvarial defects in mice. Oral Dis 2008;14:428–34.
35. Sonoyama W, Liu Y, Fang D, Yamaza T, Seo BM, Zhang C, Liu H, Gronthos S, Wang CY, Wang S, Shi S. Mesenchymal stem cell-mediated functional tooth regeneration in swine. PLoS ONE 2006;1:e79.
36. Sonoyama W, Liu Y, Yamaza T, Tuan RS, Wang S, Shi S, Huang GT. Characterization of the apical papilla and its residing stem cells from human immature permanent teeth: a pilot study. J Endod 2008;34:166–71.
37. Huang GT. Pulp and dentin tissue engineering and regeneration: current progress. Regen Med. 2009;4(5):697-707.
38. Yang X, van den Dolder J, Walboomers XF, Zhang W, Bian Z, Fan M, Jansen JA. The odontogenic potential of STRO-1 sorted rat dental pulp stem cells in vitro. J Tissue Eng Regen Med 2007;1: 66–73.
39. Seo BM, Miura M, Gronthos S, Bartold PM, Batouli S, Brahim J, Young M, Robey PG, Wang CY, Shi S. Investigation of multipotent postnatal stem cells from human periodontal ligament. Lancet 2004;364:149–55.
40. Liu Y, Zheng Y, Ding G, Fang D, Zhang C, Bartold P M, Gronthos S, Shi S, Wang S. Periodontal ligament stem cell-mediated treatment for periodontitis in miniature swine. Stem Cells 2008;26: 1065–73.
41. Xu L, Tang L, Jin F, Liu X H, Yu J H, Wu J J, Yang Z H, Wang Y X, Duan Y Z, Jin Y. The apical region of developing tooth root constitutes a complex and maintains the ability to generate root and periodontium-like tissues. J Periodontal Res 2009; 44: 275–82.
42. Nedel F, André Dde A, de Oliveira IO, Cordeiro MM, Casagrande L, Tarquinio SB, Nor JE, Demarco FF. Stem cells: therapeutic potential in dentistry. J Contemp Dent Pract. 2009;1;10(4):90-6.
43. Wood MR, Vermilyea SG. A review of selected dental literature on evidence-based treatment planning for dental implants: Report of the Committee on Research in Fixed Prosthodontics of the Academy of Fixed Prosthodontics. J Prosthet Dent 2004;92:447-62.
44. Lin Y, Gallucci GO, Busser GD, Bosshardt D, Belser UC, Yelick PC. Bioengineered Periodontal Tissue Formed on Titanium Dental Implants. J Dent Res 2011;90(2): 251-6.
45. Rossomando EF. Prosthodontics and Implants: from xenodontics to biodontics. Compend Contin Educ Dent. 2007;28(8):418-20.
46. Catón J, Bostanci N, Remboutsika E, De Bari C, Mitsiadis TA. Future dentistry: cell therapy meets tooth and periodontal repair and regeneration. J Cell Mol Med. 2011 May;15(5):1054-65.
Afrashtehfar et al

Call now for a demo | 1 800 438 7864 | www.suni.com
Go digital today. 3D tomorrow.
3D diagnosis and planning are rapidly emerging as the new standard for comprehensive dental care. With Suni’s
modular design, you can choose a digital pan today, and cost-effectively upgrade to a One-shot Ceph and/or 3D cone
beam whenever you’re ready. Or, simply go with cone beam right from the start. With Suni3D, you have the flexibility to
choose the system that works best for you. The base unit stays the same, so your investment is safe with Suni! Suni3D
comes standard with 5X5 cm field of view (upgradable to 8 x 5 cm), ideal for implant, TMJ and endodontic procedures.
Exceptional technology at a most affordable price from Suni – The value leader in digital imaging!
Introducing Suni3D –All New 3-in-1 System! Go digital today, and upgrade to 3D cone beam when you’re ready!
The value leader in digital imaging
Best Integrated
Cone Beam/
Pan Solution for
Under $100k

Wilcko et al
Background: Preeclampsia is an obstetric com-plication that affects 7-10% of pregnant patients resulting in significant morbidity and/or mortality to the mother and fetus. Though the biologic basis for the development of preeclampsia is poorly understood, current research indicates that the disorder is a syndrome of excessive inflammatory immune responses. Recent studies have shown an association between periodontal disease and a number of systemic diseases including pre-eclampsia. The link between these maladies this thought to arise from immunologic responses to the chronic burden of endotoxin elicited inflamma-tory cytokines of periodontal disease. Previous studies examining the relationship between peri-odontal disease and obstetric complications such as preterm labor and preeclampsia have focused on inflammatory cytokines such as prostaglan-din PGE2, interleukin-1β (IL-1β), and C-reactive protein. With current theories on the etiology of preeclampsia focusing on Th-1 cytokines such as interfereon gamma (IFN-ϒ) and interleukin-12 (IL-12), the goal of this pilot study was to compare serum levels of IFN-ϒ and IL-12 in preeclamp-tic women with and without periodontal disease.
Materials and Methods: A study popula-tion of 8 total women, 5 with no periodontal dis-ease and preeclampsia (Group 1) and 3 with periodontal disease and preeclampsia (Group 2) had peripheral venous blood sampled at
the time of parturition. Serum IFN-ϒ and IL-12 concentrations were determined via enzyme linked immunosorbent assay (ELISA). Addi-tional data such as gestational age, birth weight, and demographic data were also collected.
Results: The differences in p-value between Groups 1 and 2 for IFN-ϒ and IL-12 blood con-centrations were statically significant. In all cases of this pilot study, preeclamptic patients with periodontal disease had elevated levels of both IL-12 and IFN-ϒ when compared to preeclamp-tic patients without periodontal disease (Fig-ures 4, 5). In no case did the maximum Group 1 IFN-γ or IL-12 concentrations exceed the mini-mum IL-12 or IFN-ϒ concentrations of Group 2.
Conclusions: In this pilot study of 8 pre-eclamptic patients, serum concentrations of IL-12 and IFN-ϒ were elevated to statistically significant levels in patients with untreated periodontal disease. Although promising, the results of this pilot study must be critically examined. The small study population in this pilot study does not provide adequate statisti-cal power to make definitive conclusions about the potential for elevated IL-12 and IFN-ϒ lev-els in periodontitis patients to contribute to the pathogenesis of preeclampsia. To confirm the results of this pilot study, additional studies with larger sample populations are warranted.
Serum Interleukin-12 and Interfereon-Gamma Levels in Humans with Periodontal Disease and Preeclampsia: A Pilot Study
Dan Holtzclaw, DDS, MS1
1. Private practice, Austin, Texas, USA
Abstract
KEY WORDS: Preeclampsia, periodontal disease, interleukin-12, interfereon gamma
The Journal of Implant & Advanced Clinical Dentistry • 45
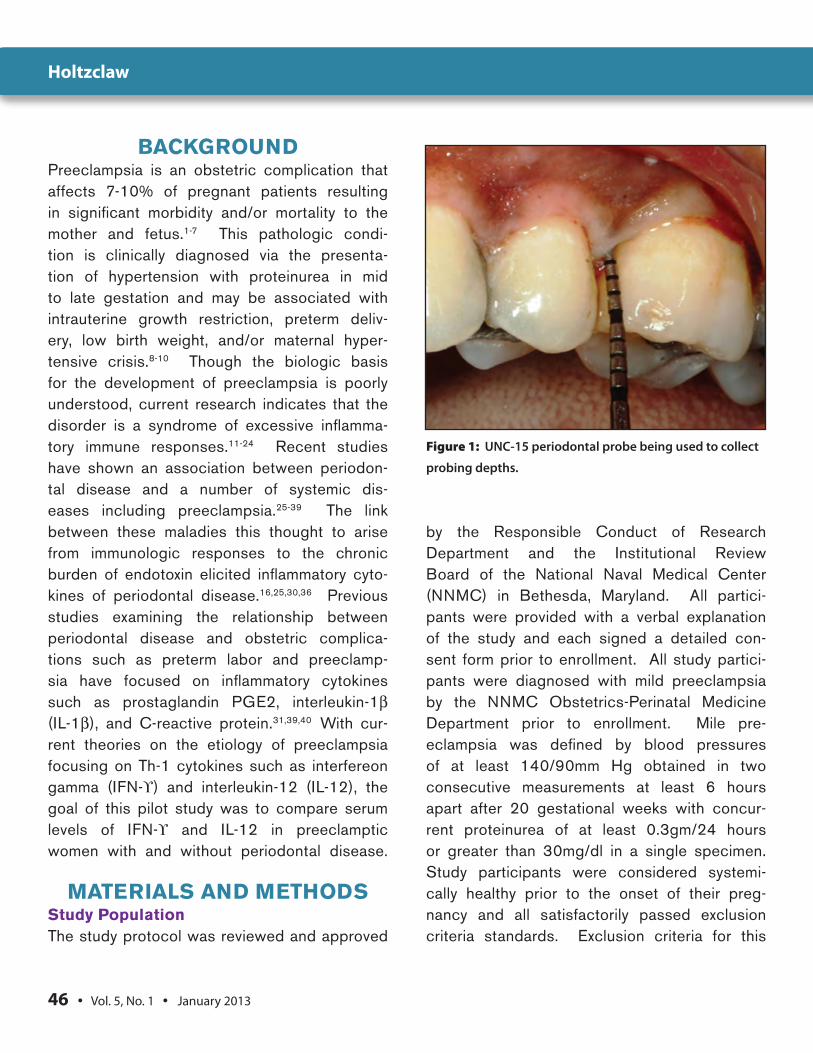
46 • Vol. 5, No. 1 • January 2013
BACKgROunDPreeclampsia is an obstetric complication that affects 7-10% of pregnant patients resulting in significant morbidity and/or mortality to the mother and fetus.1-7 This pathologic condi-tion is clinically diagnosed via the presenta-tion of hypertension with proteinurea in mid to late gestation and may be associated with intrauterine growth restriction, preterm deliv-ery, low birth weight, and/or maternal hyper-tensive crisis.8-10 Though the biologic basis for the development of preeclampsia is poorly understood, current research indicates that the disorder is a syndrome of excessive inflamma-tory immune responses.11-24 Recent studies have shown an association between periodon-tal disease and a number of systemic dis-eases including preeclampsia.25-39 The link between these maladies this thought to arise from immunologic responses to the chronic burden of endotoxin elicited inflammatory cyto-kines of periodontal disease.16,25,30,36 Previous studies examining the relationship between periodontal disease and obstetric complica-tions such as preterm labor and preeclamp-sia have focused on inflammatory cytokines such as prostaglandin PGE2, interleukin-1β (IL-1β), and C-reactive protein.31,39,40 With cur-rent theories on the etiology of preeclampsia focusing on Th-1 cytokines such as interfereon gamma (IFN-ϒ) and interleukin-12 (IL-12), the goal of this pilot study was to compare serum levels of IFN-ϒ and IL-12 in preeclamptic women with and without periodontal disease.
MAtERiAlS AnD MEthODSStudy PopulationThe study protocol was reviewed and approved
by the Responsible Conduct of Research Department and the Institutional Review Board of the National Naval Medical Center (NNMC) in Bethesda, Maryland. All partici-pants were provided with a verbal explanation of the study and each signed a detailed con-sent form prior to enrollment. All study partici-pants were diagnosed with mild preeclampsia by the NNMC Obstetrics-Perinatal Medicine Department prior to enrollment. Mile pre-eclampsia was defined by blood pressures of at least 140/90mm Hg obtained in two consecutive measurements at least 6 hours apart after 20 gestational weeks with concur-rent proteinurea of at least 0.3gm/24 hours or greater than 30mg/dl in a single specimen. Study participants were considered systemi-cally healthy prior to the onset of their preg-nancy and all satisfactorily passed exclusion criteria standards. Exclusion criteria for this
Figure 1: UNC-15 periodontal probe being used to collect
probing depths.
Holtzclaw

The Journal of Implant & Advanced Clinical Dentistry • 47
study included a history of diabetes, asthma, cardiovascular complications, chronic hyper-tension, renal disorders, gastric ulcers, chronic infectious diseases, and/or any condition that required antibiotic prophylaxis prior to dental treatment. Patients with severe preeclampsia, defined by blood pressures ≥ 160/110mm Hg obtained in two consecutive measurements at least 6 hours apart, serologic evidence of end organ damage, or > 5gm of proteinurea in 24 hours, were also excluded as immediate deliv-ery was typically indicated in such situations.
Measurements of Periodontal StatusUpon enrollment in the study, subjects received a full mouth periodontal examination (Figure 1) evaluating the following clinical parameters: probing depth (PD), clinical attachment loss (CAL), furcation involvement, tooth mobility, bleeding upon probing (BOP), and oral hygiene
status. Oral hygiene was assessed by the per-centage of tooth surfaces (4 per tooth) dem-onstrating plaque. Measures of supragingival plaque were made by staining the teeth with an Erythrosin disclosing tablet. PD, CAL, and BOP measurements were made by a single examiner (DH) at six sites per tooth using a 15mm UNC probe. CAL was measured using the cemento-enamel junction (CEJ) as a refer-ence point and BOP was determined by the presence of blood within 30 seconds of prob-ing. Patients with PD ≥ 5mm on 3 or more teeth with concurrent CAL ≥ 3mm and a bleeding index score of 33% were diagnosed as having periodontal disease. Patients not meeting these criteria were considered periodontally healthy.
Study group AssignmentUpon determination of their periodontal health status, study participants were assigned to one
Figure 2: Blood sampling taken at time of parturition. Figure 3: ELISA testing of blood samples for IFN-ϒ and IL-12.
Holtzclaw

48 • Vol. 5, No. 1 • January 2013
of two groups: (Group 1) Preeclamptic patients without periodontal disease or (Group 2) Pre-eclamptic patients with periodontal disease.
Recording of Maternal CharacteristicsDemographic data and maternal obstetric measurements such as blood pressure, ges-tational age and birth weight of the child at delivery were recorded. Parturition prior to 37 weeks was considered preterm labor while infants with a delivery weight under 2500gm were considered to be of low birth weight.
Serum SamplingParticipants had peripheral venous blood sampled at the time of parturition (Figure 2). At each sampling, 20ml of blood was drawn into sterile plastic blood collection tubes and centrifuged at a rate of 3,100 RPM for 10 minutes to separate serum. Sepa-rated serum samples were transferred to
plastic vials and stored at a temperature of -70° C until all samples were collected.
Determination of Cytokine ConcentrationSerum IFN-ϒ and IL-12 concentrations were determined via enzyme linked immunosorbent assay (ELISA) (Figure 3) using commercially available kits (R&D Systems, Minneapolis, Min-nesota, USA). IFN-ϒ ELISA Kit #DIF50 and IL-12 Kit #D1200 were run according to the manufacturer’s directions. Optical densities of the processed samples were determined in a microplate reader with wavelength cor-rection set to 550nm. Duplicates of each serum sample were tested and the mean value for each combination was reported.
Statistical AnalysisAll data analyses were performed with the InStat statistical analysis program (GraphPad Soft-ware, Inc., San Diego, California, USA). The
Table 1: Study Participant Data
Participant Age Gestational Age
Group 1 Preeclamptic women without 28.4 (±4.87) years 37.4 (±1.52) weeks periodontal disease n=5
Group 2 Preeclamptic women with 35.6 (±2.08) years 31.0 (±7.21) weeks periodontal disease n=3
p Value 0.0539 0.0902
Holtzclaw

The Journal of Implant & Advanced Clinical Dentistry • 49
data reported in this pilot study are presented as means ± standard deviation. Differences in meaned data were tested with a paired Stu-dent’s T test and a two-tailed p value of < 0.05 was considered to be statistically significant.
RESultSA total of 8 women (Table 1) participated in this pilot study with 5 women comprising Group 1 (preeclamptic patients without peri-odontal disease) and 3 women comprising
Table 2: Gestational and Birth Weight Data
Gestational Age Birth Weight
Group 1 Preeclamptic women without 37.4 (±1.52) weeks 3063 (±860.4) grams periodontal disease n=5
Group 2 Preeclamptic women with 31.0 (±7.21) weeks 1843 (±1443.7) grams periodontal disease n=3
p Value 0.0902 0.1606
Table 3: Blood Concentrations of IFN-ϒ and IL-12 in Study Participants as Determined by ELISA Testing
IFN-ϒ IL-12
Group 1 Preeclamptic women without 15.61 (±0.95) Pg/ml 3.98 (±0.66) Pg/ml periodontal disease n=5
Group 2 Preeclamptic women with 18.78 (±0.89) Pg/ml 5.64 (±0.04) Pg/ml periodontal disease n=3
p Value 0.0003 0.0015
Holtzclaw

50 • Vol. 5, No. 1 • January 2013
Group 2 (preeclamptic patients with periodon-tal disease). The mean gestational ages of infants delivered to patients in Groups 1 and 2 were 37.4 weeks (± 1.52) and 31.0 weeks (±7.21) respectively (p=0.09) while the mean birth weights of these same infants were 3,063 grams (±860.4) and 1,843 grams (±1,443.7) (p=0.16) (Table 2). The differences in p-value between Groups 1 and 2 for gestational age and birth weight were statically significant. Mean serum sample concentrations for IFN-ϒ and IL-12 are reported in Table 3. Again, the differences in p-value between Groups 1 and 2 for IFN-ϒ and IL-12 blood concentrations were statically significant. In all cases of this pilot
study, preeclamptic patients with periodon-tal disease had elevated levels of both IL-12 and IFN-ϒ when compared to preeclamptic patients without periodontal disease (Figures 4, 5). In no case did the maximum Group A IFN-ϒ or IL-12 concentrations exceed the mini-mum IL-12 or IFN-ϒ concentrations of Group B.
DiSCuSSiOnMultiple studies have proposed that abnormal activation of the maternal immune system plays an important role in the etiology of preeclamp-sia.2-5,16-13,41,42,102,103 The maternal immune sys-tem of normal pregnancies displays a Th2 cytokine profile composed of interleukin-4 (IL-
Figure 4: IL-12 blood concentrations of study participants. Blood samples of preeclamptic patients with periodontal disease are circled in red.
Holtzclaw
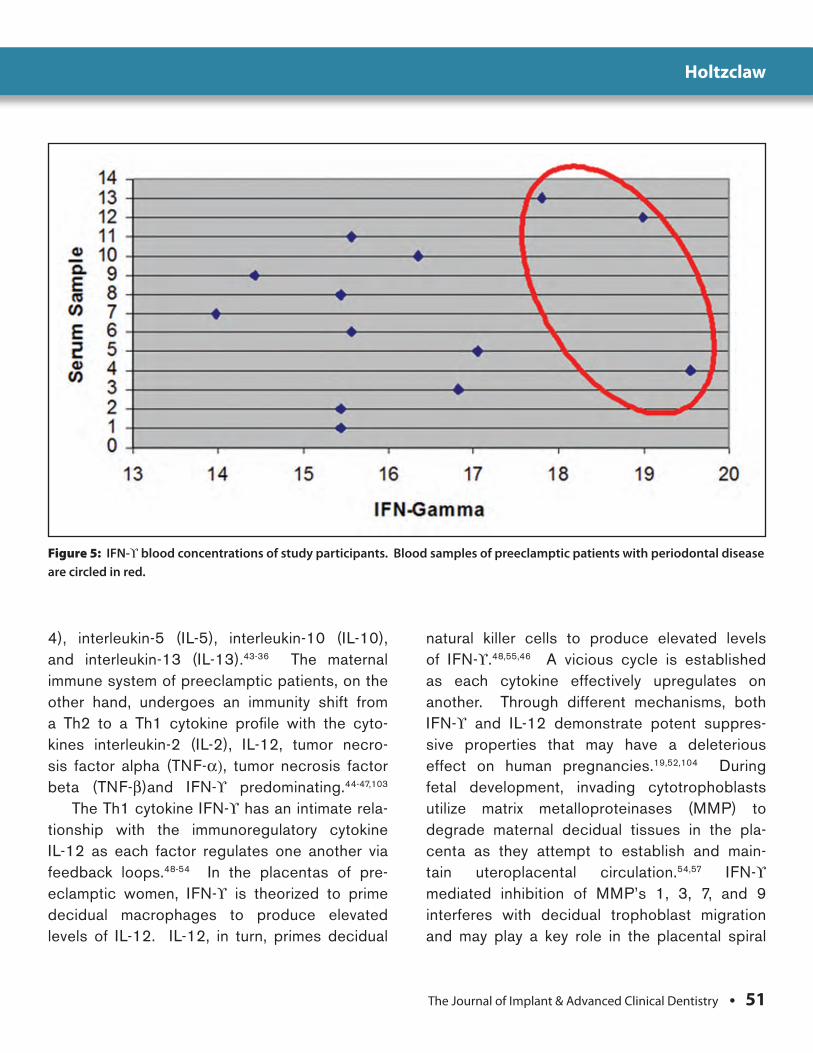
The Journal of Implant & Advanced Clinical Dentistry • 51
Figure 5: IFN-ϒ blood concentrations of study participants. Blood samples of preeclamptic patients with periodontal disease are circled in red.
4), interleukin-5 (IL-5), interleukin-10 (IL-10), and interleukin-13 (IL-13).43-36 The maternal immune system of preeclamptic patients, on the other hand, undergoes an immunity shift from a Th2 to a Th1 cytokine profile with the cyto-kines interleukin-2 (IL-2), IL-12, tumor necro-sis factor alpha (TNF-α), tumor necrosis factor beta (TNF-β)and IFN-ϒ predominating.44-47,103
The Th1 cytokine IFN-ϒ has an intimate rela-tionship with the immunoregulatory cytokine IL-12 as each factor regulates one another via feedback loops.48-54 In the placentas of pre-eclamptic women, IFN-ϒ is theorized to prime decidual macrophages to produce elevated levels of IL-12. IL-12, in turn, primes decidual
natural killer cells to produce elevated levels of IFN-ϒ.48,55,46 A vicious cycle is established as each cytokine effectively upregulates on another. Through different mechanisms, both IFN-ϒ and IL-12 demonstrate potent suppres-sive properties that may have a deleterious effect on human pregnancies.19,52,104 During fetal development, invading cytotrophoblasts utilize matrix metalloproteinases (MMP) to degrade maternal decidual tissues in the pla-centa as they attempt to establish and main-tain uteroplacental circulation.54,57 IFN-ϒ mediated inhibition of MMP’s 1, 3, 7, and 9 interferes with decidual trophoblast migration and may play a key role in the placental spiral
Holtzclaw
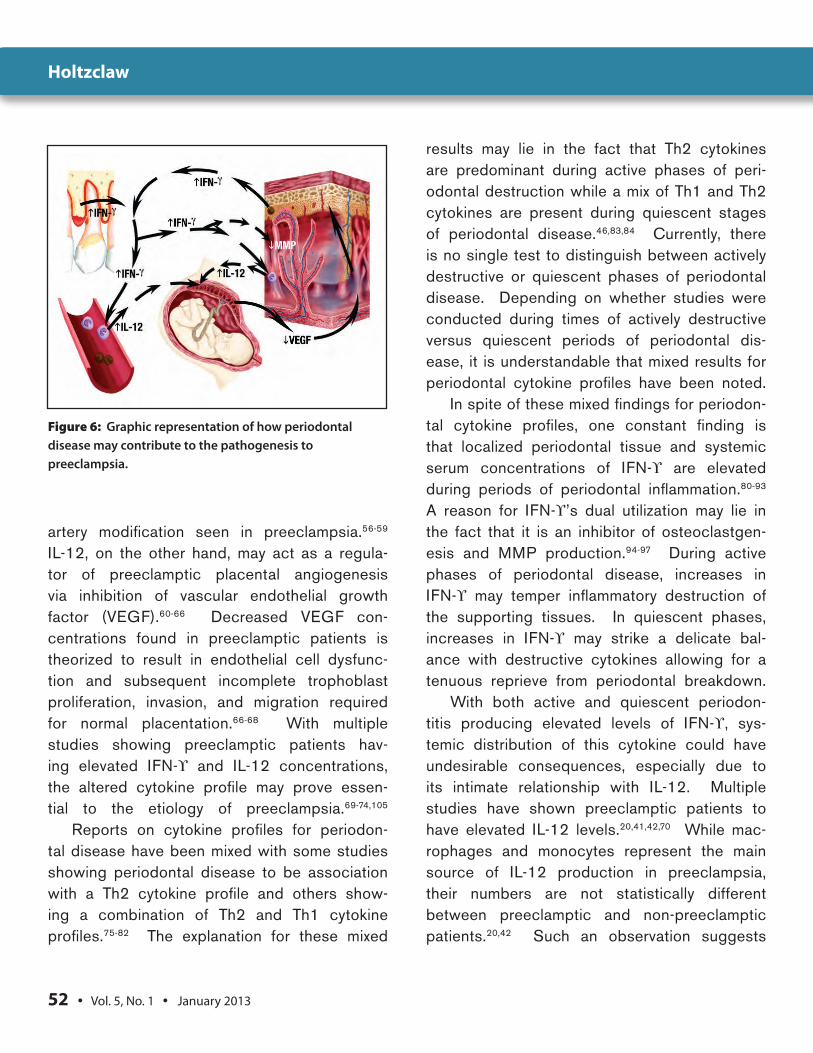
52 • Vol. 5, No. 1 • January 2013
artery modification seen in preeclampsia.56-59 IL-12, on the other hand, may act as a regula-tor of preeclamptic placental angiogenesis via inhibition of vascular endothelial growth factor (VEGF).60-66 Decreased VEGF con-centrations found in preeclamptic patients is theorized to result in endothelial cell dysfunc-tion and subsequent incomplete trophoblast proliferation, invasion, and migration required for normal placentation.66-68 With multiple studies showing preeclamptic patients hav-ing elevated IFN-ϒ and IL-12 concentrations, the altered cytokine profile may prove essen-tial to the etiology of preeclampsia.69-74,105
Reports on cytokine profiles for periodon-tal disease have been mixed with some studies showing periodontal disease to be association with a Th2 cytokine profile and others show-ing a combination of Th2 and Th1 cytokine profiles.75-82 The explanation for these mixed
results may lie in the fact that Th2 cytokines are predominant during active phases of peri-odontal destruction while a mix of Th1 and Th2 cytokines are present during quiescent stages of periodontal disease.46,83,84 Currently, there is no single test to distinguish between actively destructive or quiescent phases of periodontal disease. Depending on whether studies were conducted during times of actively destructive versus quiescent periods of periodontal dis-ease, it is understandable that mixed results for periodontal cytokine profiles have been noted.
In spite of these mixed findings for periodon-tal cytokine profiles, one constant finding is that localized periodontal tissue and systemic serum concentrations of IFN-ϒ are elevated during periods of periodontal inflammation.80-93 A reason for IFN-ϒ’s dual utilization may lie in the fact that it is an inhibitor of osteoclastgen-esis and MMP production.94-97 During active phases of periodontal disease, increases in IFN-ϒ may temper inflammatory destruction of the supporting tissues. In quiescent phases, increases in IFN-ϒ may strike a delicate bal-ance with destructive cytokines allowing for a tenuous reprieve from periodontal breakdown.
With both active and quiescent periodon-titis producing elevated levels of IFN-ϒ, sys-temic distribution of this cytokine could have undesirable consequences, especially due to its intimate relationship with IL-12. Multiple studies have shown preeclamptic patients to have elevated IL-12 levels.20,41,42,70 While mac-rophages and monocytes represent the main source of IL-12 production in preeclampsia, their numbers are not statistically different between preeclamptic and non-preeclamptic patients.20,42 Such an observation suggests
Figure 6: Graphic representation of how periodontal disease may contribute to the pathogenesis to preeclampsia.
Holtzclaw

The Journal of Implant & Advanced Clinical Dentistry • 53
that the properties of monocytes and macro-phages are altered in preeclamptic patients. A potential cause for altered monocyte proper-ties in preeclamptic patients may be linked to IFN-ϒ. It is well documented that IFN-ϒ has the ability to prime monocytic cells for exces-sive cytokine production and recent studies have proposed that in preeclamptic patients, macrophages are a likely source of increased IL-12 production.41,42 Because periodontal dis-ease increases systemic IFN-ϒ levels, hema-togenous dissemination of this cytokine may be a contributory monocyte/macrophage priming agent in preeclampsia (Figure 6).
Linking periodontal disease to an increased risk for preeclampsia has been accomplished with numerous comparative case controlled studies.25-27,36,39,97,98,99,100 While there is convinc-ing evidence showing an association between the two diseases, the mechanism of action conjoining periodontitis with preeclampsia is poorly understood. A recent study by Poli-tano et al.101 performed a case control analysis of 116 pregnant women, 58 with preeclamp-sia and 58 without. This study found a corre-lation between periodontitis and preeclampsia (adjusted odds ratio of 3.73, 95% confidence interval 1.32-10.58), but failed to demonstrate a link between the diseases via the cytokine profile of IL-6 and TNF-α. Multiple independent studies have demonstrated both disease pro-cesses have elevated IL-12 and IFN-ϒ levels and the results of this pilot study show trends in which periodontitis may contribute to the pathogenesis of preeclampsia via the IL-12/INF-ϒ pathway. In all cases of this pilot study, preeclamptic patients with periodontal disease had elevated levels of both IL-12 and IFN-ϒ
when compared to preeclamptic patients with-out periodontal disease. In no case did the maximum Group 1 (preeclamptic patients with-out periodontal disease) blood concentrations IFN-ϒ or IL-12 exceed the minimum IL-12 or IFN-ϒ blood concentrations of Group 2 (pre-eclamptic patients with periodontal disease) .
COnCluSiOnSIn this pilot study of 8 preeclamptic patients, serum concentrations of IL-12 and IFN-ϒ were elevated to statistically significant lev-els in patients with untreated periodontal dis-ease. Although promising, the results of this pilot study must be critically examined. The small study population in this pilot study does not provide adequate statistical power to make definitive conclusions about the potential for elevated IL-12 and IFN-ϒ levels in periodon-titis patients to contribute to the pathogen-esis of preeclampsia. To confirm the results of this pilot study, additional studies with larger sample populations are warranted. ●
Correspondence:Dr. Dan Holtzclaw711 W. 38th StreetSuite G5Austin, TX [email protected]
Holtzclaw

54 • Vol. 5, No. 1 • January 2013
DisclosureThe author reports no conflicts of interest with anything mentioned in this paper.
DisclaimerThe opinions expressed in this article are those of the author and do not represent the views nor the endorsement of the United States Government, Department of Defense, or Navy Medicine. References1. Madazli R, Aydin S, Uludag S, Vildan O, Tolun
N. Maternal plasma levels of cytokines in normal and preeclamptic pregnancies and their relationship with diastolic blood pressure and fibronectin levels. Acta Obstet Gynecol Scand 2003; 82(9):797-802.
2. Darmochwal-Kolarz D, Leszczynska-Gorzelak B, Rolinski J, Oleszczuk J. T helper 1- and T helper 2-type cytokine imbalance in pregnant women with pre-eclampsia. Eur J Obstet Gynecol Reprod Biol 1999; 86(2):165-170.
3. Darmochwal-Kolarz D, Rolinski J, Leszczynska-Goarzelak B, Oleszczuk. The expressions of intracellular cytokines in the lymphocytes of preeclamptic patients. J.Am J Reprod Immunol 2002; 48(6):381-386.
4. Davison JM, Homuth V, Jeyabalan A, Conrad KP, Karumanchi SA, Quaggin S, Dechend R, Luft FC. New aspects in the pathophysiology of preeclampsia. J Am Soc Nephrol 2004;15(9):2440-2448.
5. Tannetta DS, Muttukrishna S, Groome NP, Redman CW, Sargent IL. Endothelial cells and peripheral blood mononuclear cells are a potential source of extraplacental activin a in preeclampsia. J Clin Endocrinol Metab 2003; 88(12):5995-6001.
6. Banerjee S, Smallwood A, Moorhead J, Chambers AE, Papageorghiou A, Campbell S, Nicolaides K. Placental expression of interferon-gamma (IFN-gamma) and its receptor IFN-gamma R2 fail to switch from early hypoxic to late normotensive development in preeclampsia. J Clin Endocrinol Metab 2005; 90(2):944-952.
7. Thadhani R, Mutter WP, Wolf M, Levine RJ, Taylor RN, Sukhatme VP, Ecker J, Karumanchi SA. First trimester placental growth factor and soluble fms-like tyrosine kinase 1 and risk for preeclampsia. J Clin Endocrinol Metab. 2004 Feb; 89(2):770-775.
8. Vatten LJ, Skjaerven R. Is pre-eclampsia more than one disease? BJOG 2004;111(4):298-302.
9. Lasker JN, Coyle B, Li K, Ortynsky M. Assessment of risk factors for low birth weight deliveries. Health Care Women Int 2005; 26(3):262-280.
10. Bozhinova S, Poroshanova V, Sampat D. Delivery and perinatal aspects of pregnant women with pre-eclampsia-eclampsia]. Akush Ginekol (Sofiia). 2004;43(7):3-9.
11. Saito S, Umekage H, Sakamoto Y, Sakai M, Tanebe K, Sasaki Y, Morikawa H. Increased T-helper-1-type immunity and decreased T-helper-2-type immunity in patients with preeclampsia. Am J Reprod Immunol 1999;41(5):297-306.
12. Galewska Z, Bańkowski E, Romanowicz L, Jaworski S. Pre-eclampsia (EPH-gestosis)-induced decrease of MMP-s content in the umbilical cord artery. Clin Chim Acta 2003; 335:109-15.
13. Wilczynski JR, Tchórzewski H, Banasik M, Głowacka E, Wieczorek A, Lewkowicz P, Malinowski A, Szpakowski M, Wilczynski . Lymphocyte subset distribution and cytokine secretion in third trimester decidua in normal pregnancy and preeclampsia. J Eur J Obstet Gynecol Reprod Biol 2003; 109(1):8-15.
14. Qian C, Lim KH, England LJ, Yu KF, Schisterman EF, Thadhani R, Sachs BP, Epstein FH, Sibai BM, Sukhatme VP, Karumanchi SA. Circulating angiogenic factors and the risk of preeclampsia. Levine RJ, Maynard SE. N Engl J Med 2004; 350(7):672-683.
15. Redman CW, Sacks GP, Sargent IL. Preeclampsia: an excessive maternal inflammatory response to pregnancy. Am J Obstet Gynecol 1999; 180:499-506.
16. Redman C, Sargen I. Preeclampsia: an excessive maternal inflammatory response to pregnancy. Am J Obstet Gynecol 1999; 180:499-506.
17. Chaouat G, Robillard PY, Dekker G. Fourth International Workshop on immunology of pre-eclampsia, December 2004, Reunion, France. J Reprod Immunol 2005; 67:103-111.
18. Jonsson Y, Rubèr M, Matthiesen L, Berg G, Nieminen K, Sharma S, Ernerudh J, Ekerfelt C. Cytokine mapping of sera from women with preeclampsia and normal pregnancies. J Reprod Immunol 2006; 70:83-91.
19. Hu Y, Dutz JP, MacCalman CD, Yong P, Tan R, von Dadelszen P. Decidual NK cells alter in vitro first trimester extravillous cytotrophoblast migration: a role for IFN-gamma. J Immunol 2006; 177(12):8522-8530.
20. Sakai M, Tsuda H, Tanebe K, Sasaki Y, Saito S. Interleukin-12 secretion by peripheral blood mononuclear cells is decreased in normal pregnant subjects and increased in preeclamptic patients. Am J Reprod Immunol 2002; 47(2):91-97.
21. Gallery ED, Campbell S, Arkell J, Nguyen M, Jackson CJ. Preeclamptic decidual microvascular endothelial cells express lower levels of matrix metalloproteinase-1 than normal. Microvasc Res 1999; 57(3):340-346.
22. Helske S, Vuorela P, Carpén O, Hornig C, Weich H, Halmesmäki E. Mol Hum Reprod. Expression of vascular endothelial growth factor receptors 1, 2 and 3 in placentas from normal and complicated pregnancies. Mol Hum Reprod 2001; 7(2):205-210.
23. Maynard S, et al. Excess placental soluble fms-like tyrosine kinase 1 (sFltl) may contribute to endothelial dysfunction, hypertension, and proteinuria in preeclampsia. J Clin Invest 2003; 111(5):649-658.
24. Reister F et al. Altered protease expression by periarterial trophoblast cells in severe early-onset preeclampsia with IUGR. J Perinat Med 2006; 34(4):272-279.
25. Boggess K et al. Maternal periodontal disease is associated with an increased risk for preeclampsia. Obstet Gynecol 2003; 101(2): 227-231.
26. Canacki V, et al. Periodontal disease as a risk factor for preeclampsia: a case control study. Aust N Z J Obstet Gynaecol 2004; 44(6):568-573.
27. Meurman JH, Furuholm J, Kaaja R, Rintamäki H, Tikkanen U. Oral health in women with pregnancy and delivery complications. Clin Oral Investig. 2006 Jun;10(2):96-101.
28. Radnai M., et al. A possible association between preterm birth and early periodontitis. A pilot study. J Clin Periodontol 2004; 31(9):736-741.
29. Radnai, M, Gorzo I. Periodontal disease as a potential risk factor for preterm and low birth weight. Fogorv Sz 2002; 95(6):241-244.
30. Davenport E, et al. Maternal periodontal disease and preterm low birth weight: case-control study. J Dent Res 2002; 81(5):313-318.
31. Lopez, N.J., P.C. Smith, and J. Gutierrez, Periodontal therapy may reduce the risk of preterm low birth weight in women with periodontal disease: a randomized controlled trial. J Periodontol 2002; 73(8):911-924.
32. Jeffcoat M, et al. Periodontal disease and preterm birth: results of a pilot intervention study. J Periodontol 2003; 74(8):1214-1218.
33. Jeffcoat M, et al. Current evidence regarding periodontal disease as a risk factor in preterm birth. Ann Periodontol, 2001; 6(1):183-188.
34. Jeffcoat M, et al. Periodontal infection and preterm birth: results of a prospective study. J Am Dent Assoc 2001;132(7):875-880.
35. Jeffcoat, M, et AL. Preterm birth, osteoporosis, and periodontal disease. Compend Contin Educ Dent Suppl 2000;(30):5-11.
36. oettinger-Barak O, Ohel G, Oettinger MI, Kreutrer HI, Peled M, Machtei E. Severe pregnancy complication (Preeclampsia) is associated with greater periodontal destruction. J periodontol 2005; 76(1):134-137.
37. Moreu G, Gonzalez-January M. Relationship between maternal periodontal disease and low birth weight preterm infants. J Clin Periodontol 2005;3 2(6):622-627.
38. Offenbacher S, ET AL. Periodontal infection as a possible risk factor for preterm low birth. J Periodontol 1996; 67: 1103-1113.
39. Herrera J, et al. Periodontal disease severity is related to high levels of C-reactive protein in pre-eclampsia. J Hypertens 2007;25(7):1459-1464.
40. Konopka T, Hirnle L, Kopec W, Karolewska E. The Secretion of Prostaglandin E2 and Interleukin 1-Beta in Women with Periodontal Diseases and Preterm Low-Birth-Weight. Rech Sci Stomatol Odontol 2003; 45(1): 18-28.
41. Yun P, et al. Modulation of an interleukin-12 and gamma interferon synergistic feedback regulatory cycle of T-cell and monocyte cocultures by Porphyromonas gingivalis lipopolysaccharide in the absence or presence of cysteine proteinases. Infect Immun 2002; 70(10):5695-5705.
42. Daniel Y, et al. Plasma interleukin-12 is elevated in patients with preeclampsia. Am J Reprod Immunol 1998; 3916:376-380.
43. Wegmann T, et al. Bidirectional cytokine interactions in the maternal-fetal relationship: is successful pregnancy a TH2 phenomenon? Immunol Today 1993; 14(7):353-356.
44. Saito S, Sakai M. Thl/Th2 balance in preeclampsia. J Reprod Immunol 2003; 59(2):161-173.
45. Hyashi M, et al. Tumor Necrosis Factor Alpha in the Placenta is not Elevated in Preeclamptic Patients Despite its Elevation in Peripheral Blood. AJRI 2005; (53):113-119.
46. Gemmell E, Seymour G. Cytokine Profiles of Cells Extracted from Humans with Periodontal Disease. J Dent Res 1998; 77(1):16-26.
47. Omu A, et al. Connection between human leucocyte antigens D region and T helper cytokines in preeclampsia. Arch Gynecol Obstet 2004; 269(2): 79-84.
48. Wilczynski J, et al. Cytokine secretion by decidual lymphocytes in transient hypertension of pregnancy and preeclampsia. Mediators Inflamm 2002; 1112:105-111.
Holtzclaw
The Journal of Implant & Advanced Clinical Dentistry • 55
49. Voest E, et al. Inhibition of angiogenesis in vivo by lnterleukin 12. J Natl Cancer Inst 1995; 87(8): 581-586.
50. Trinchieri G, et al. Interleukin-12 and the regulation of innate resistance and adaptive immunity. Nat Rev Immunol 2003; 3(2):133-146.
51. Trinchieri G, et al. Cytokines acting on or secreted by macrophages during intracellular infection (IL-10, IL-12, IFN-gamma). Curr Opin Immunol 1997; 9(1):17-23.
52. Gee M, et al. Hypoxia-mediated apoptosis from angiogenesis inhibition underlies tumor control by recombinant interleukin 12. Cancer Res 1999; 59(19): 4882-4889.
53. Tsai I, et al. Interleukin-12 and interleukin-16 in periodontal disease. Cytokine 2005; 31(1): 34-40.
54. Chaouat G, Robillard PY, Dekker G. Fourth International Workshop on immunology of pre-eclampsia, December 2004, Reunion, France. J Reprod Immunol 2005; 67:103-111.
55. Hu Y, MacCalman C, Yong P, Tan R, von Dadelsren P. Decidual NK Cells Alter In Vitro First Trimester Extravillous Cytotrophoblast Migration: A Role for Interfereon-Gamma. J Immunol 2006; 177: 8522-8530.
56. Ma Z, Shah R, Benveniste E. Interfereon-Gamma activated STAT-1 Alpha suppresses MMP-9 gene transcription by sequestration of the coactivators CBP/p300. J Leukoc Biol 2005; 78: 515-523.
58. Ala-Aho R, Grenman R, Fusenig NE, Lopez C. Inhibition of collagenase-3 (MMP-13) expression in transformed human keratinocytes by interfereon-gamma is associated with activation of extracellular signal-regulated kinase-1, 2 and STATl. Oncogene 2000; 19: 248-257.
60. Curiel T, et al. Dendritic cell subsets differentially regulate angiogenesis in human ovarian cancer. Cancer Res 2004; 64(16): 5535-5538.
61. Taylor R, et al; Longitudinal serum concentrations of placental growth factor: evidence for abnormal placental angiogenesis in pathologic pregnancies. Am J Obstet Gynecol 2003; 101(6): 1266-1274.
62. Pollioti B, et al. Second-trimester maternal serum placental growth factor and vascular endothelial growth factor for predicting severe, early-onset preeclampsia. Obstet Gynecol 2003; 101(6): 1266-74.
63. Cooper J, et al. VEGF mRNA levels in placenta from pregnancies complicated by preeclampsia. Br J Obstet Gynaecol 1996; 103(12): 1191-1196.
64. Lyall F, et al. Suppression of serum vascular endothelial growth factor immunoreactivity in normal pregnancy and in preeclampsia. Br J Obstet Gynaecol 1997; 104(2): 223-228.
65. Lyall F, et al. Placental expression of vascular endothelial growth factor in placentae from pregnancies complicated by preeclampsia and intrauterine growth restriction does not support placental hypoxia at delivery. Placenta 1997; 18(4): 269-276.
66. Chaiworapongsa T, et al. Evidence supporting a role for blockade of the vascular endothelial growth factor system in the pathophysiology of preeclampsia. Am J Obstet Gynecol 2004; 190(6): 1541-1547.
69. Nakayama Y, et al. Relationships between local and systemic expression of interleukin-12 and plasma levels of vascular endothelial growth factor in patients with gastric cancer. Anticancer Res 2004; 24:3289-3294.
70. Dudley D, et al. Elevations of serum interleukin-12 concentrations in women with severe pre-eclampsia and HELLP syndrome. J Reprod Immunol 1996; 31: 97-107.
71. Masztalerz A, et al. Treatment with IL-2 and IL-12 inhibits tumour cell division in SL2 lymphoma. Anticancer Res, 2004; 24: 2633-2642.
72. McKeeman G, et al. Soluble vascular endothelial growth factor receptor-1 (sFlt-1) is increased throughout gestation in patients who have preeclampsia develop. Am J Obstet Gynecol 2004; 191(4): 1240-6.
73. Indraccolo S, et al. Undermining tumor angiogenesis by gene therapy: an emerging field. Curr Gene Ther 2004; 4(3): 297-308.
74. Bonfanti A, et al. Changes in circulating dendritic cells and IL-12 in relation to the angiogenic factor VEGF during IL-2 immunotherapy of metastatic renal cell cancer. Int J Biol Markers 2000; l5(2): 161-164.
75. Gorska R, et al. Relationship between clinical parameters and cytokine profiles in inflamed gingival tissue and serum samples from patients with chronic periodontitis. J Clin Periodontal 2003; 30(12): 1046-1052.
76. Mackler B, et al. Immunoglobulin bearing lymphocytes and plasma cells in human periodontal disease. J Periodontal Res 1977; 12(1):. 37-45.
77. Seymour G, Powell R, Davies W. Conversion of a stable T-cell lesion to a progressive B-cell lesion in the pathogenesis of chronic inflammatory periodontal disease: an hypothesis. J Clin Periodontol 1979; 6(5): 267-277.
78. Malberg R, et al. Determination of lymphocyte populations and subpopulations extracted from chronically inflamed human periodontal tissues. J Clin Periodontol 1992; 19(3): 155-158.
79. Page R, et al. The role of inflammatory mediators in the pathogenesis of periodontal disease. J Periodontal Res 1991; 26(3): 230-242.
80. Berglundh T, Liljenberg B, Lindhe J. Some cytokine profiles of T-helper cells in lesions of advanced periodontitis. J Clin Periodontol 2002; 29(8): 705-709.
81. Teng Y, et al. Mixed periodontal Thl-Th2 cytokine profile in Actinobacillus actinomycetemcomitans-specific osteoprotegerin ligand (or RANK-L)- mediated alveolar bone destructio sn in vivo. Infect Immun 2002; 70(9): 5269-5273.
82. Ito H, et al. Gene expression analysis of the CD4t T-cell clones derived from gingival tissues of periodontitis patients. Oral Microbiol Immunol 2005; 20(6): 382-386.
83. Choi Y, Kim J. B cells activated in the presence of Thl cytokines inhibit osteoclastogenesis. Exp Mol Med 2003; 35(5): 385-392.
84. Choi J, et al. Identification of T-cell epitopes of Porphyromonas gingivalis heat-shock-protein 60 in periodontitis. Oral Microbiol Immunol 2004; 19(1): 1-5.
85. Garlet G, et al. Patterns of chemokines and chemokine receptors expression in different forms of human periodontal disease. J Periodontal Res 2003; 38(2): 210-217.
86. Prabhu A, Michalowicz B, Mathur A. Detection of local systemic cytokines in adult periodontitis. J Periodontol 1996; 67(5): 515-522.
87. Takeichi O, et al. Cytokine profiles of T-lymphocytes from gingival tissues with pathological pocketing. J Dent Res 2000; 9(8): 1548-1555.
88. Ukai T, et al. Immunohistological study of interferon-gamma and interleukin-4-bearing cells in human periodontitis gingiva. Arch Oral Biol 2001; 46(10): 901-908.
89. Okada H, et al. Diagnostic strategies of periodontitis based on the molecular mechanisms of periodontal tissue destruction. Oral Dis 1996; 2(1): 87-95.
90. Johnson R, et al. Interleukin-18 concentrations and the pathogenesis of periodontal disease. J Periodontol 2005; 76(5):p. 785-790.
91. Wassenaar A, et al. CD40 engagement modulates the production of matrix metalloproteinases by gingival fibroblasts. Clin Exp Immunol 1999; 115(1): 161-167.
92. Tsai C, et al. Changes in gingival crevicular fluid interleukin-4 and interferon-gamma in patients with chronic periodontitis before and after periodontal initial therapy. Kaohsiung J Med Sci 2007; 23(1): 1-7.
93. Zong M, et al. Changes of circulating IFN-gamma, IL-4 in patients with chronic periodontitis before and after periodontal initial therapy. Shanghai Kou Qiang Yi Xue 2005; 14(2): 131-133.
94. Horwood NJ, Elliott J, Martin TJ, Gillespie MT. IL-12 alone and in synergy with IL-18 inhibits osteoclast formation in vitro. J Immunol 2001; 166(8):4915-4921.
95. Takayanagi H, Ogasawara K, Hida S, Chiba T, Murata S, Sato K, Takaoka A, Yokochi T, Oda H, Tanaka K, Nakamura K, Taniguchi T. T-cell-mediated regulation of osteoclastogenesis by signalling cross-talk between RANKL and IFN-gamma. Nature 2000; 408(6812): 600-605.
96. Shinoda K, Sugiyama E, Taki H, Harada S, Mino T, Maruyama M, Kobayashi M. Resting T cells negatively regulate osteoclast generation from peripheral blood monocytes. Bone 2003; 33(4): 711-720.
97. Vergnes JN. Studies suggest an association between maternal periodontal disease and pre-eclampsia. Evid Based Dent 2008; 9(2): 46-7.
98. Shetty M, Shetty PK, Ramesh A, Thomas B, Prabhu S, Rao A. Periodontal disease in pregnancy is a risk factor for preeclampsia. Acta Obstet Gynecol Scand. 2010 May;89(5):718-21.
100. Cota LO, Guimarães AN, Costa JE, Lorentz TC, Costa FO. Association between maternal periodontitis and an increased risk of preeclampsia. J Periodontol 2006; 77(12): 2063-2069.
101. Politano GT, Passini R, Nomura ML, Velloso L, Morari J, Couto E. Correlation between periodontal disease, inflammatory alterations and pre-eclampsia. J Periodontal Res 2011; 46(4): 505-511.
102. Sharma D, Singh A, Trivedi SS, Bhattacharjee J. Role of endothelin and inflammatory cytokines in pre-eclampsia - A pilot North Indian study. Am J Reprod Immunol 2011; 65(4): 428-432.
103. Laresgoiti-Servitje E, Gómez-López N, Olson DM. An immunological insight into the origins of pre-eclampsia. Hum Reprod Update 2010; 16(5): 510-524.
104. Hu Y, Tan R, MacCalman CD, Eastabrook G, Park SH, Dutz JP, von Dadelszen P. IFN-gamma-mediated extravillous trophoblast outgrowth inhibition in first trimester explant culture: a role for insulin-like growth factors. Mol Hum Reprod 2008; 14(5): 281-289.
105. Mansouri R, Akbari F, Vodjgani M, Mahboudi F, Kalantar F, Mirahmadian M. Serum cytokines profiles in Iranian patients with preeclampsia. Iran J Immunol 2007; 4(3):179-185.
Holtzclaw
