peri-implantitis therapy with an er:yag laserperi-implantitis therapy with an er:yag laser see the...
TRANSCRIPT
• Clinical Reviews and Case Reports: Er:YAG Laser in RestorativeDentistry; Er:YAG Laser for Pulpotomies in Primary Teeth
• Case Reports: Gingivoplasty, Osseous Recontouring, CrownLengthening, and Frenectomy; Gingivoplasty Associated withRestorative Dental Care; Treatment of Moderate ChronicPeriodontitis and Aphthous Ulcers
The Official Journal of the Academy of Laser Dentistry 2008 • Vol. 16 No. 2The Official Journal of the Academy of Laser Dentistry 2008 • Vol. 16 No. 2
Peri-Implantitis Therapy with an Er:YAG LaserSee the clinical review and case report on page 69
Academy of Laser Dentistry3300 University Drive, Suite 704
Coral Springs, FL 33065
In This Issue CE Credits Available

JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
TA B L E O F CO N T E N T SThe official journal of the
Academy of Laser Dentistry
Editor in ChiefJohn D.B. Featherstone, MSc, PhDSan Francisco, CA [email protected]
Incoming Editor in ChiefDonald J. Coluzzi, DDSPortola Valley, CA [email protected]
Managing EditorGail S. Siminovsky, CAE, Executive DirectorCoral Springs, FL [email protected]
Consulting EditorJohn G. Sulewski, MA Huntington Woods, MI [email protected]
Associate Editors Donald J. Coluzzi, DDSPortola Valley, CA [email protected] P.A. Parker, BDS, LDS RCS, MFGDP Harrogate, Great Britain
Editorial BoardDonald J. ColuzziGail S. Siminovsky, CAEJohn G. Sulewski, MADonald J. Coluzzi, DDSSteven P.A. Parker, BDS, LDS RCS, MFGDPAlan J. Goldstein, DMDDonald E. Patthoff, DDSPeter Rechmann, Prof. Dr. med. dent.
PublisherMax G. MosesMember Media
1844 N. Larrabee • Chicago, IL 60614312-296-7864 • Fax: 312-896-9119
Design and LayoutDiva Design
2616 Missum Pointe • San Marcos, TX 78666512-665-0544 • Fax 609-678-0544
Editorial Office3300 University Drive, Suite 704
Coral Springs, FL 33065
954-346-3776 Fax 954-757-2598
The Academy of Laser Dentistry is a not-for-profitorganization qualifying under Section 501(c)(3) ofthe Internal Revenue Code. The Academy of LaserDentistry is an international professional member-ship association of dental practitioners and sup-porting organizations dedicated to improving thehealth and well-being of patients through theproper use of laser technology. The Academy isdedicated to the advancement of knowledge,research and education and to the exchange ofinformation relative to the art and science of theuse of lasers in dentistry. The Academy endorsesthe Curriculum Guidelines and Standards forDental Laser Education.
Member American Association of Dental Editors The Journal of Laser DentistryThe mission of the Journal of Laser Dentistry is to provide a professional journal that helps tofulfill the goal of information dissemination by the Academy of Laser Dentistry. The purpose ofthe Journal of Laser Dentistry is to present information about the use of lasers in dentistry.All articles are peer-reviewed. Issues include manuscripts on current indications for uses oflasers for dental applications, clinical case studies, reviews of topics relevant to laser dentistry,research articles, clinical studies, research abstracts detailing the scientific basis for the safetyand efficacy of the devices, and articles about future and experimental procedures. In addition,featured columnists offer clinical insights, and editorials describe personal viewpoints.
E D I TO R ’ S V I E WKeeping up with the Times ..............................................................................57John D.B. Featherstone, MSc, PhD
C L I N I C A L R E V I E W A N D C A S E R E P O RTClinical Considerations for the Use of Er:YAG Lasers in Restorative Dentistry ............................................................58Giuseppe Iaria, Dr. Prof. Med. Dent., Brescia, Italy; Steven P.A. Parker,BDS, LDS RCS, MFGDP, Harrogate, North Yorks, Great Britain
COV E R F E AT U R EC L I N I C A L R E V I E W A N D C A S E R E P O RTPeri-Implantitis Therapy with an Erbium:YAG Laser ..................................69Avi Reyhanian, DDS, Natanya, Israel; Donald J. Coluzzi, DDS, PortolaValley, California
C L I N I C A L R E V I E W A N D C A S E R E P O RTUse of an Er:YAG Laser for Pulpotomies in Vital and Nonvital Primary Teeth ................................................................75Lawrence Kotlow, DDS, Albany, New York
A DVA N C E D P R O F I C I E N C Y C A S E ST U D I E SIntroduction ............................................................................................................80
Soft Tissue Gingivoplasty, Osseous Recontouring / Crown Lengthening, and Frenectomy Using an Er:YAG Laser ..............................81Charles R. Hoopingarner, DDS, Houston, Texas
Use of an 810-nm Diode Laser in a Gingivoplasty ProcedureAssociated with Restorative Dental Care ......................................................87Steven Parker, BDS, LDS RCS, MFGDP, Harrogate, North Yorks, Great Britain
Nd:YAG Laser-Assisted Treatment of Moderate Chronic Periodontitisand Nd:YAG Laser Treatment of Two Aphthous Ulcerative Lesions ......93Mary Lynn Smith, RDH, McPherson, Kansas
R E S E A R C H A B ST R AC T SLaser Treatment of Aphthous Ulcers ............................................................101
CO N T I N U I N G E D U C AT I O NCE Program ..........................................................................................................104CE Questions ........................................................................................................105CE Registration Form & Answer Sheets ......................................................108
Journal of Laser Dentistry
Journal of Laser Dentistry: Guidelines for AuthorsThe Academy of Laser Dentistry Welcomes Your Articles for Submission
The Journal of Laser Dentistry publish-es articles pertaining to the art, science,and practice of laser dentistry andother relevant light-based technologies.Articles may be scientific and clinical innature discussing new techniques,research, and programs, or may beapplications-oriented describing specificproblems and solutions. While lasersare our preferred orientation, otherhigh-technology articles, as well asinsights into marketing, practice man-agement, regulation, and other aspectsof dentistry that may be of interest tothe dental profession, may be appropri-ate. All articles are peer-reviewed priorto acceptance, modification, or rejection.
These guidelines are designed tohelp potential authors in writing andsubmitting manuscripts to the Journalof Laser Dentistry, the official publica-tion of the Academy of Laser Dentistry(ALD). Please follow these instructionscarefully to expedite review and process-ing of your submission. Manuscriptsthat do not adhere to these instructionswill not be accepted for consideration.The Academy of Laser Dentistry and theeditors and publisher of the Journal ofLaser Dentistry endorse the “UniformRequirements of Manuscripts Submittedto Biomedical Journals” (www.icmje.org).The Journal reserves the right to reviseor rescind these guidelines.
Authors are advised to read the morecomprehensive Guidelines for Authorsand required forms available by mail oronline at www.laserdentistry.org.
Manuscript EligibilitySubmitted manuscripts must be writtenclearly and concisely in AmericanEnglish and appropriate for a scholarlyjournal. Write in active voice and usedeclarative sentences. Manuscripts willbe considered for publication on the con-dition that they have been submittedexclusively to the Journal, and have notbeen published or submitted for publica-tion in any part or form in another publi-cation of any type, professional or lay, orin any language elsewhere, and with theunderstanding that they will not bereprinted without written consent fromboth the managing editor and the author.
PermissionsDirect quotations of 100 or more words,and illustrations, figures, tables, orother materials (or adaptations thereof)that have appeared in copyrightedmaterial or are in press must be accom-panied by written permission for theiruse in the Journal of Laser Dentistryfrom the copyright owner and originalauthor along with complete informationregarding source, including (as applica-
ble) author(s), title of article, title ofjournal or book, year, volume number,issue number, pages. Photographs ofidentifiable persons must be accompa-nied by valid signed releases indicatinginformed consent. When informed con-sent has been obtained from anypatient, identifiable or not, it should benoted in the manuscript. The appropri-ate Permission Letters must be submit-ted with the manuscript. Suggestedtemplate letters are available online.
CopyrightAll manuscript rights shall be trans-ferred to the Journal of Laser Dentistryupon submission. Upon submission ofthe manuscript, authors agree to sub-mit a completed Copyright TransferAgreement form, available online. If themanuscript is rejected for publication,all copyrights will be retained by theauthor(s).
CommercialismALD members are interested in learn-ing about new products and serviceofferings, however ALD stresses thatsubmitted manuscripts should be edu-cational in nature. The emphasis is onscientific research and sound clinicaland practical advice, rather than pro-motion of a specific product or service.
Disclosure of Commercial RelationshipsAccording to the Academy’s Conflict ofInterest and Disclosure policy, manu-script authors and their institutions areexpected to disclose any economic orfinancial support, as well as any per-sonal, commercial, technological, aca-demic, intellectual, professional, philo-sophical, political, or religious interestsor potential bias that may be perceivedas creating a conflict related to thematerial being published. Such condi-tions may include employment, consul-tancies, stock ownership or other equityinterests, honoraria, stipends, paidexpert testimony, patent ownership,patent licensing arrangements, royal-ties, or serving as an officer, director, orowner of a company whose products, orproducts of a competitor, are identified.Sources of support in the form of con-tracts, grants, equipment, drugs, mate-rial donations, clinical materials, specialdiscounts or gifts, or other forms of sup-port should be specified. The roles of thestudy or manuscript sponsor(s), if any,are to be described. Disclosure state-ments are printed at the end of the arti-cle following the author’s biography.This policy is intended to alert the audi-ence to any potential bias or conflict sothat readers may form their own judg-ments about the material being pre-
sented. Disclosure forms are to besigned by each author. Manuscripts willnot be reviewed without the Journalhaving this form on file.
The Academy of Laser Dentistry alsorequires that authors disclose whetherany product discussed in their manu-script is unlabeled for the use discussedor is investigational.
The Disclosure Statement form isavailable online and must be submittedwith the manuscript.
Manuscript TypesSubmissions to the Journal should belimited to one of the types indicatedbelow.• Scientific / Technology / Clinical
Review• Case Reports and Clinical Case
Studies• Scientific / Clinical Research• Randomized Clinical Trials• Advances in Dental Products• Trends• Practice Management• Guest Editorials and Essays• Letters to the Editor• Book Reviews
Manuscript Preparation andSubmissionFormatAll submitted manuscripts should bedouble-spaced, using 12 pt. font sizewith at least 6 mm between lines.Submit manuscripts in Microsoft Word(.doc), using either the Windows orMacintosh platform. Manuscripts mustbe submitted electronically in this for-mat. Hard copy-only submissions willnot be accepted.
Unacceptable FormatsThe following submission formats areunacceptable and will be returned:• Manuscripts submitted in desktop
publishing software• PowerPoint presentations• Any text files with embedded images• Images in lower than the minimum
prescribed resolution.
Manuscript ComponentsTitle PageThe title page of the manuscript shouldinclude a concise and informative titleof the article; the first name, middle ini-tial(s), and last name of each author,along with the academic degree(s), pro-fessional title(s), and the name andlocation (city, state, zip code) of currentinstitutional affiliation(s) and depart-ment(s). Authors who are private prac-titioners should identify their location(city, state, and country). Include allinformation in the title that will make
electronic retrieval of the article sensi-tive and specific. Titles of case studiesshould include the laser wavelength(s)and type(s) utilized for treatment (forexample, “810-nm GaAlAs diode”).
Identify the complete address, busi-ness and home telephone numbers, faxnumber, e-mail address, and Web siteaddress (if any) for all authors. Identifyone author as the corresponding author.Unless requested otherwise, the e-mailaddress is published in the Journal.
AbstractA self-standing summary of the text ofup to 250 words should precede theintroduction. It should provide an accu-rate summary of the most significantpoints and be representative of theentire article’s content. Provide the con-text or background for the article, basicprocedures, main findings and conclu-sions. Emphasize new or importantaspects. Do not use abbreviations (otherthan standard units of measurement) orreferences in the abstract.
Author(s) BiographyProvide a brief, current biographicalsketch of each author that includes pro-fessional education and professionalaffiliations. For authors who hold teach-ing positions, include the title, depart-ment, and school. For authors who arein federal service, include rank or titleand station.
ReferencesReferences are to be cited in the text bynumber in order of appearance, withthe number appearing either as asuperscript or in brackets. The refer-ence list should appear at the end of themanuscript with references in order offirst appearance in the text of the man-uscript. The reference list must betyped double-spaced on a separate pageand numbered in the same sequence asthe reference citations appear in thetext. Prior to submission, all referencesare to be properly prepared in the cor-rect format, checked for completeness,carefully verified against their originaldocuments, and checked for accuratecorrespondence between referencescited in the text and listed in theReferences section.• For journal citations, include sur-
names and all initials of all authors,complete title of article, name of jour-nal (abbreviated according to the U.S.National Library of Medicine(www.nlm.nih.gov/services/lpabbrev.html), year of publication,volume, issue number, and completeinclusive page numbers. If abstractsare cited, add the abstract numberafter the page number.
• For book citations, specify surnamesand initials of all authors, chapternumber and title (if applicable), edi-
tors’ surnames and initials, booktitle, volume number (if applicable),edition number (if applicable), cityand full name of publisher, year ofpublication, and inclusive page num-bers of citation.
• For government publications or bul-letins, identify the author(s) (if given);title; department, bureau, agency, oroffice; the publication series, report,or monograph number; location ofpublisher; publisher; year of publica-tion; and inclusive page numbers.
• For articles published online but notyet in print, cite with the paper’sDigital Object Identifier (DOI) addedto the end of the reference.
• For Web citations, list the authorsand titles if known, then the URLand date it was accessed.
• For presentations, list the authors,title of presentation, indication thatthe reference is a lecture, name ofconference or presentation venue,date, and location.
Illustration Captions and LegendsAll illustrations must be accompanied byindividual explanatory captions whichshould be typed double-spaced on a sepa-rate page with Arabic numerals corre-sponding to their respective illustration.
TablesTables must be typewritten double-spaced, including column heads, data,and footnotes, and submitted on sepa-rate pages. The tables are to be cited inthe text and numbered consecutively inArabic numerals in the order of theirappearance in the text. Provide a con-cise title for each table that highlightsthe key result.
IllustrationsIllustrations include photographs, radi-ographs, micrographs, charts, graphs,and maps. Each should be numbered andcited in the text in the order of appear-ance and be accompanied by explanatorycaptions. Do not embed figures withinthe manuscript text. Each figure andtable should be no larger than 8-1/2 x 11inches. Digital files must measure at
least 5 inches (127 mm) in width. Theimage must be submitted in the size itwill be printed, or larger. Illustrationsare to augment, not repeat, material inthe text. Graphs must not repeat datapresented in tables. Clinical photographsmust comply with ALD’s Guidelines forClinical Photography, available online.Authors are to certify in a cover letterthat digitized illustrations accuratelyrepresent the original data, condition, orimage and are not electronically edited.
Publisher and Copyright HolderThe Journal of Laser Dentistry is pub-lished by Max G. Moses, MemberMedia, 1844 N. Larrabee, Chicago, IL60614, Telephone: (312) 296-7864; Fax:(312) 896-9119. The Journal of LaserDentistry is copyrighted by TheAcademy of Laser Dentistry, 3300University Drive, Suite 704, CoralSprings, FL 33065, Telephone: (954)346-3776; Fax: (954) 757-2598.
Articles, Questions, IdeasQuestions about clinical cases, scientificresearch, or ideas for other articles maybe directed to Donald J. Coluzzi, Editor-in-Chief, by e-mail: [email protected].
Submission of Filesby E-mail:Send your completed files by e-mail(files up to 10 MB are acceptable). Iffiles are larger than 10 MB, they maybe compressed or sent as more than onefile, with appropriate labels. Filesshould be submitted to: Donald J.Coluzzi, Editor-in-Chief, by e-mail:[email protected].
By Federal Express or OtherInsured Courier:If using a courier, please send the file asa CD-ROM, include a hard copy of yourmanuscript and also send a verificationby e-mail to Gail Siminovsky ([email protected]).Gail SiminovskyAcademy of Laser Dentistry3300 University Drive, Suite 704Coral Springs, FL 33065Phone: (954) 346-3776.
Summary of Illustration Types and Specifications
IllustrationType
Definition and ExamplesPreferredFormat
RequiredResolution
Line Art andVector Graphics
Black and white graphic with noshading (e.g., graphs, charts, maps)
EPS or JPG 1200 DPI
Halftone Art
Photographs, drawings, or paint-ing with fine shading (e.g., radi-ographs, micrographs with scalebars, intraoral photographs)
TIFF orJPG
300 DPI (black &white) 600 DPI (color)
CombinationArt
Combination of halftone and lineart (e.g., halftones containingline drawing, extensive lettering,color diagrams)
EPS or JPG 1200 DPI
Editorial PolicyThe Journal of Laser Dentistry is devoted to providing the Academy and its members with comprehensive clinical, didactic andresearch information about the safe and effective uses of lasers in dentistry. All statements of opinions and/or fact are publishedunder the authority of the authors, including editorials and articles. The Academy is not responsible for the opinions expressedby the writers, editors or advertisers. The views are not to be accepted as the views of the Academy of Laser Dentistry unlesssuch statements have been expressly adopted by the organization. Information on any research, clinical procedures or productsmay be obtained from the author. Comments concerning content may be directed to the Academy’s main office by e-mail [email protected]
SubmissionsWe encourage prospective authors to follow JLD’s “Instructions to Authors” before submitting manuscripts. To obtain a copy,please go to our Web site www.laserdentistry.org/press.cfm. Please send manuscripts by e-mail to the Editor at [email protected].
Disclosure Policy of Contributing Authors’ Commercial RelationshipsAccording to the Academy’s Conflict of Interest and Disclosure policy, authors of manuscripts for JLD are expected to discloseany economic support, personal interests, or potential bias that may be perceived as creating a conflict related to the materialbeing published. Disclosure statements are printed at the end of the article following the author’s biography. This policy isintended to alert the audience to any potential bias or conflict so that readers may form their own judgments about the materialbeing presented.
Disclosure Statement for the Academy of Laser DentistryThe Academy of Laser Dentistry has no financial interest in any manufacturers or vendors of dental supplies.
Reprint Permission PolicyWritten permission must be obtained to duplicate and/or distribute any portion of the Journal of Laser Dentistry. Reprints maybe obtained directly from the Academy of Laser Dentistry provided that any appropriate fee is paid.
Copyright 2008 Academy of Laser Dentistry. All rights reserved unless other ownership is indicated. If any omission or infringementof copyright has occurred through oversight, upon notification amendment will be made in a future issue. No part of this publica-tion may be reproduced or transmitted in any form or by any means, individually or by any means, without permission from thecopyright holder.
The Journal of the Academy of Laser Dentistry ISSN# 1935-2557.
JLD is published quarterly and mailed nonprofit standard mail to all ALD members. Issues are also mailed to new memberprospects and dentists requesting information on lasers in dentistry.
Advertising Information and RatesDisplay rates are available at www.laserdentistry.org/press.cfm and/or supplied upon request. Insertion orders and materials shouldbe sent to Bill Spilman, Innovative Media Solutions, P.O. Box 399, Oneida, IL 61467, 877-878-3260, fax: 309-483-2371, [email protected]. For a copy of JLD Advertising Guidelines go to www.laserdentistry.org/press_advguide_policy.cfm.The cost for a classified ad in one issue is $50 for the first 25 words and $2.00 for each additional word beyond 25. ALD membersreceive a 20% discount. Payment must accompany ad copy and is payable to the Academy of Laser Dentistry in U.S. funds only.Classified advertising is not open to commercial enterprises. Companies are encouraged to contact Bill Spilman for information on dis-play advertising specifications and rates. The Academy reserves the right to edit or refuse ads.
Editor’s Note on Advertising: The Journal of Laser Dentistry currently accepts advertisements for different dental laser educational programs. Not all dental laser educationalcourses are recognized by the Academy of Laser Dentistry. ALD as an independent professional dental organization is concerned that coursesmeet the stringent guidelines following professional standards of education. Readers are advised to verify with ALD whether or not specificcourses are recognized by the Academy of Laser Dentistry in their use of the Curriculum Guidelines and Standards for Dental Laser Education.

57
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
E D I TO R ’ S V I E W
This is my last issue of the Journalof Laser Dentistry as editor-in-chief.I have enjoyed the last couple ofyears as we changed the face of thejournal. I have stepped down forpersonal reasons and I am pleasedthat Don Coluzzi has taken over forthe future. The Journal will be ingood hands. I would like this oppor-tunity to thank my editorial boardand the additional reviewers for alltheir work. Thanks too for all theefforts made by the contributors towrite their articles and to conform tothe rigors of peer review. Thank youfor the opportunity to serve you all.
There are several articles in thisissue dealing with uses of theEr:YAG laser. The laser-tissue inter-actions are used to enable dentalprocedures of various types to beperformed for the benefit of thepatient. I encourage you to studyeach of the articles so that you canbetter understand how these laserswork for each of the applicationsdescribed. Every wavelength andevery set of irradiation parameters
can be used for various purposes.The task of the practitioner is totruly understand how to optimizethese conditions.
The three advanced proficiencycase studies provide illustrations ofthree different laser wavelengths,namely 810-nm diode, Er:YAG, andNd:YAG, that can be exploited indifferent ways. Again the laser-tissue interactions are used toenable the final clinical outcomes.
In conclusion, I wish all who readthis journal every success within thevarious aspects of laser dentistry.Please look to the future as new andimproved lasers come on themarket. Your fundamental under-standing of how lasers interact withtissue is critical to your decision asto what laser to buy and what to usefor which procedure. Be a continualstudent. Laser dentistry is a compli-cated activity that demands ourclose attention at all times.
A U T H O R B I O G R A P H YDr. John D.B. Featherstone isProfessor of Preventive andRestorative Dental Sciences andInterim Dean in the School ofDentistry at the University ofCalifornia, San Francisco (UCSF).He has a PhD in chemistry from theUniversity of Wellington (NewZealand). His research over the past33 years has covered several aspectsof cariology (study of tooth decay)including fluoride mechanisms ofaction, de- and remineralization ofthe teeth, apatite chemistry, salivarydysfunction, caries (tooth decay)prevention, caries risk assessment,and laser effects on dental hardtissues with emphasis on cariesprevention and early caries removal.He has won numerous national andinternational awards including theT.H. Maiman award for research inlaser dentistry from the Academy ofLaser Dentistry in 2002, and theNorton Ross Award for ClinicalResearch from the American DentalAssociation in 2007. In 2005 he washonored as the first lifetimehonorary member of the Academy ofLaser Dentistry. Dr. Featherstonehas published more than 200papers. Through the current issue,he is the editor-in-chief of theJournal of Laser Dentistry.
Disclosure: Dr. Featherstone has noaffiliation with any company thatmarkets lasers for dentistry. ■■
Featherstone
Keeping up with the TimesJohn D.B. Featherstone, MSc, PhD, San Francisco, CaliforniaJ Laser Dent 2008;16(2):57
SY N O P S I S
John Featherstone, editor-in-chief, describes some of the highlights of
this issue of the Journal of Laser Dentistry, and hands over to the new
editor-in-chief Don Coluzzi.
Clinical Considerations for the Use of Er:YAGLasers in Restorative DentistryGiuseppe Iaria, Dr. Prof. Med. Dent.,1 Brescia, Italy; Steven P.A. Parker, BDS, LDS RCS, MFGDP,
Harrogate, North Yorks, Great Britain1Di.S.T.Bi.M.O. – Dipartimento di Scienze e Tecnologie Biofisiche, Mediche e Odontostomatologiche, University of Genoa, Italy
J Laser Dent 2008;16(2):58-68
I N T R O D U C T I O NKeller and Hibst1 illustrated thepotential of the Er:YAG laser forthe effective ablation of dental hardtissues. As a result there followedthe development and marketing offree-running pulsed, mid-infraredwavelength lasers during the mid-1990s. This offered advantages inaddressing laser wavelengths thatwere complementary to targettissue elements, allowing clinicallysignificant ablation rates that didnot cause pulpal or collateralthermal injury using proper energylevels.2-7 The erbium YAG anderbium, chromium YSGG laserwavelengths are strongly absorbedprimarily by water and to a smallextent by hydroxyapatite containedin varying component ratios inhard dental tissue.8
The use of the erbium lasers inrestorative dentistry can offer
multiple advantages and thefollowing 10 guidelines are offeredto maximize successful outcomes:• Basic considerations• Laser-tissue interaction consider-
ations• Use of coaxial water spray• Exceptions to using water spray• Cavity margin considerations• Acid-etch considerations• Avoidance of dehydration• Choice of composite restorative
materials• Isolation and safety considera-
tions• Miracles don’t happen!
1. Basic ConsiderationsSo that laser-tissue interaction istherapeutically effective and effi-cient, it is necessary to deliver lightenergy of sufficient value over timeto effect tissue change withoutcausing unwanted collateral
A B ST R AC TThere are two wavelengths currentlyavailable that comprise the erbiumfamily of dental lasers. TheEr,Cr:YSGG laser has an activemedium of yttrium scandiumgallium garnet doped with erbiumand chromium ions, operates in afree-running pulsed mode at anemission wavelength of 2780 nm.The Er:YAG laser has an activemedium of yttrium aluminumgarnet doped with erbium ions andemits free-running pulsed laserenergy at a wavelength of 2940nm. Both wavelengths have a highabsorption in water, and are appro-priate for ablating oral soft tissue aswell as dental hard tissue. With thelatter, the rapid vaporization of inter-stitial water results in an explosivedislocation of target hard tissue.
Advantages of using this laserfamily in restorative dentistryinclude precision, selective ablationof target hard tissue and cariouslesions, reduced collateral damagethat might be due to rotary instru-mentation (tactile and thermaldamage), and less conductivethermal stimulation of the pulp.
Laser use in restorative dentistryis technique-sensitive, and inappro-priate or poor operating parameterscan result in less-than-expectedresults. This paper examines 10principles of use of these erbiumlaser wavelengths in clinical restora-tive dentistry, together with areview of the literature regardingdifferent aspects of the use of laserenergy on hard tissues.
Key Words: acid etching, dental;dental bonding; dental enamel;dental pulp capping; dentalveneers; dentin; dentin sensitivity;laser ablation; safety, medicaldevice; tooth fractures
58
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
Iaria et al.
SY N O P S I S
This article draws on the principles outlined in the Academy of Laser
Dentistry Position Paper on the Use of Laser Energy for Therapeutic
Ablation of Intraoral Hard Tissues, published in the Journal of Laser
Dentistry (J Laser Dent 2007;15(2):78-86) and adopted in March
2007 by the Academy of Laser Dentistry.
The authors illustrate 10 principles that govern erbium laser use on
tooth structure, and three clinical case examples utilizing a specific
Er:YAG laser. The authors utilize only the Er:YAG wavelength in their
clinical practices.

59
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
thermal damage by conduction ofexcess heat into the surroundingtissues.8 An essential requirementis to establish a rate of interactionthat is commensurate with a timeframe allowing such interaction tobe clinically acceptable. This isachieved through a suitable choiceof incident laser energy deliveredto the tissue as well as the effectsof wavelength, pulse duration, repe-tition rate, power density, and thethermal relaxation time of thetissue; all of these factors willdetermine the rate (speed) of abla-tion of dental hard tissue.9-11
The speed of ablation is alsoaffected by the incident angle of thedelivery tip relative to the toothand the presence of ablation prod-ucts. Addressing the delivery tipparallel to the axis of the enamelprisms in order to access the inter-prismatic, higher-water contentstructure maximizes the speed ofablation. Ablation is more efficientand heat transfer is minimizedwhen the pulse width is reducedand peak power values rise.6, 12-13 Inaddition, the use of sharp curettesto remove gross caries can reducelaser use to an acceptable timeframe.
The depth of laser ablationdepends principally on the parame-ters utilized and is a consequenceof the energy used per pulse andthe number of pulses delivered. Inaddition, to avoid and preventcracks or structural modifications,the tip, where present, must nottouch the surface and excessenergy must not be applied.
The ablation threshold of humanenamel has been reported14 to be inthe range of 12-20 Joules/cm2 andfor dentin, 8-14 Joules/cm2 for boththe Er:YAG and Er,Cr:YSGG laserwavelengths, and each availableinstrument can provide thisfluence. It is recommended that theclinician follow the manufacturer’sguidelines in establishing lasertreatment protocols for a givenlaser, keeping in mind the differingoperating parameters of air / water
/ spot size and any power lossesthat may occur within differingdelivery systems.
2. Laser-Tissue InteractionConsiderationsIn determining effective treatmentthe following factors may apply:a.Target chromophoresb. Mode of interactionc. Emission mode (pulsed or contin-
uous wave, chopped) / pulseduration
d.General thermal effectse. Relationship of laser action to
cavity design / restoration reten-tion
f. Speed of “cutting” / power values.
a. Target ChromophoresBoth Er,Cr:YSGG and Er:YAGlaser wavelengths are wellabsorbed in water due to the broadabsorption band of water aroundand below 3,000 nm. In addition,there is a small absorption peak ataround 2,800 nm by the hydroxylion of hydroxyapatite mineralcontent of the hard tissues.Enamel, dentin, bone, cementum,and carious tissue have relativelydescending mineral density andascending water composition.
b. Mode of InteractionConstituent water, when exposed tolaser energy in this wavelengthrange, absorbs the light efficientlyand the energy is rapidly convertedto heat, resulting in a disruptiveexpansion of water molecules in thetissue. As such, small tissue frag-ments may be ejected with little orno alteration to the mineral itself.With relatively high fluences it ispossible that the laser light isabsorbed by the mineral as well asthe water resulting in ablation ofthe mineral and/or disruption withsome structural modification.15-17
c. Emission ModeThe emission mode of currenterbium lasers is defined as free-running pulsed and the pulsedurations are close to the thermal
relaxation times of enamel anddentin.18
d. General Thermal EffectThe use of water-assisted mid-infrared wavelengths allows workon hard tissues with thermal risesof less than 5° C in the pulp. It isnecessary to avoid an accumulationof debris at the bottom of the cavitywhich can lead to conductive heatdamage.7, 17, 19-20
e. Relationship of Laser Action toCavity Design / RestorationRetentionLaser irradiation of enamel anddentin results in a micro-cavitatedsurface. While this roughnessmight be beneficial for retention ofrestorative materials, unsupportedenamel rods can remain, whichcould compromise a marginal seal.The lased dentin surface shows anabsence of a smear layer.21
f. Speed of “Cutting” / Power ValuesThe speed of ablation is a result ofthe amount of incident laserenergy, the pulse duration, therepetition rate, and the thermalrelaxation time. In addition otherfactors must be considered such asthe speed of the movement of thelaser handpiece relative to thetarget tissue, the focus distance ofthe laser beam, the incident angleof the delivery tip relative to thetooth, and the presence of ablationproducts.
3. Use of Coaxial Water SprayStudies have investigated theeffects of excessive incident powerand the build-up of ablation prod-ucts, or their removal by means ofa coaxial water spray.7, 22-25 Theexplosive defragmentationresulting from water-assisted mid-infrared wavelengths allows muchof the heat to escape from thecavity carried in the ablated parti-cles, resulting in pulpal thermalrises of less than 5° C. The affinityof mid-infrared laser wavelengths
Iaria et al.
Continued on p. 62
60
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
Iaria et al.
Case #1ER :YAG L ASER-ASS ISTED TR EATM ENTOF F R ACTU R ED TEETH
PRETREATMENTA. Outline of Case1. FULL CLINICAL DESCRIPTION
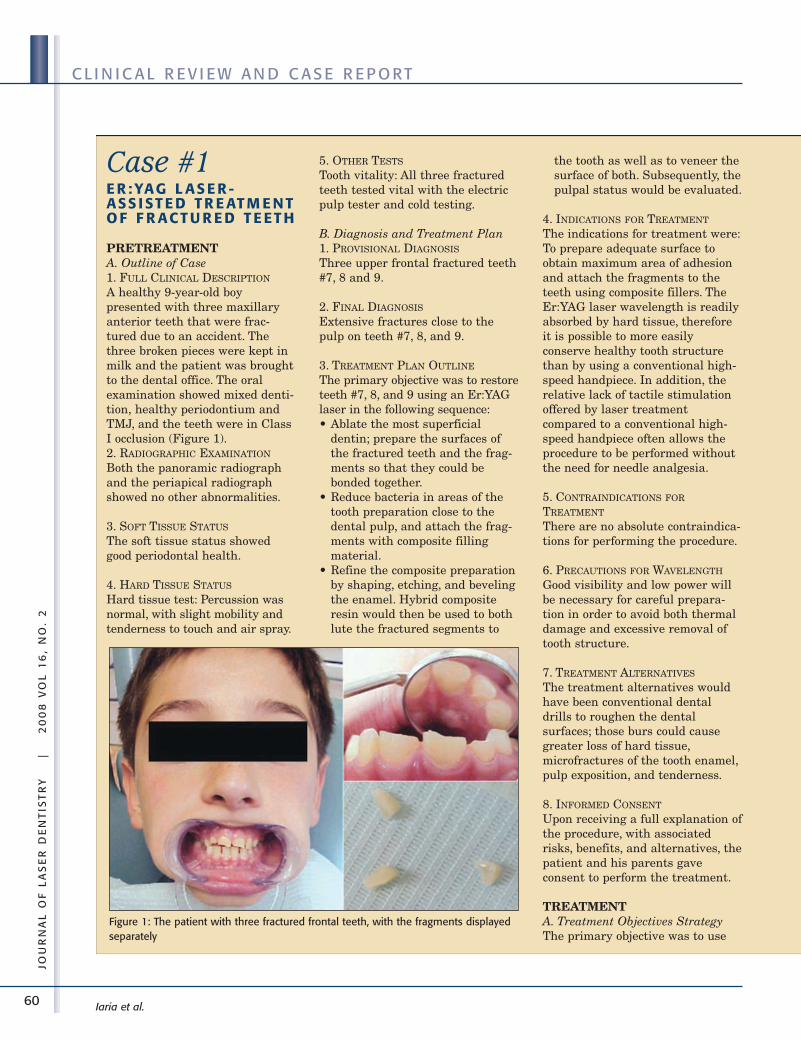
A healthy 9-year-old boypresented with three maxillaryanterior teeth that were frac-tured due to an accident. Thethree broken pieces were kept inmilk and the patient was broughtto the dental office. The oralexamination showed mixed denti-tion, healthy periodontium andTMJ, and the teeth were in ClassI occlusion (Figure 1).2. RADIOGRAPHIC EXAMINATION
Both the panoramic radiographand the periapical radiographshowed no other abnormalities.
3. SOFT TISSUE STATUS
The soft tissue status showedgood periodontal health.
4. HARD TISSUE STATUS
Hard tissue test: Percussion wasnormal, with slight mobility andtenderness to touch and air spray.
5. OTHER TESTS
Tooth vitality: All three fracturedteeth tested vital with the electricpulp tester and cold testing.
B. Diagnosis and Treatment Plan1. PROVISIONAL DIAGNOSIS
Three upper frontal fractured teeth#7, 8 and 9.
2. FINAL DIAGNOSIS
Extensive fractures close to thepulp on teeth #7, 8, and 9.
3. TREATMENT PLAN OUTLINE
The primary objective was to restoreteeth #7, 8, and 9 using an Er:YAGlaser in the following sequence:• Ablate the most superficial
dentin; prepare the surfaces ofthe fractured teeth and the frag-ments so that they could bebonded together.
• Reduce bacteria in areas of thetooth preparation close to thedental pulp, and attach the frag-ments with composite fillingmaterial.
• Refine the composite preparationby shaping, etching, and bevelingthe enamel. Hybrid compositeresin would then be used to bothlute the fractured segments to
the tooth as well as to veneer thesurface of both. Subsequently, thepulpal status would be evaluated.
4. INDICATIONS FOR TREATMENT
The indications for treatment were:To prepare adequate surface toobtain maximum area of adhesionand attach the fragments to theteeth using composite fillers. TheEr:YAG laser wavelength is readilyabsorbed by hard tissue, thereforeit is possible to more easilyconserve healthy tooth structurethan by using a conventional high-speed handpiece. In addition, therelative lack of tactile stimulationoffered by laser treatmentcompared to a conventional high-speed handpiece often allows theprocedure to be performed withoutthe need for needle analgesia.
5. CONTRAINDICATIONS FOR
TREATMENT
There are no absolute contraindica-tions for performing the procedure.
6. PRECAUTIONS FOR WAVELENGTH
Good visibility and low power willbe necessary for careful prepara-tion in order to avoid both thermaldamage and excessive removal oftooth structure.
7. TREATMENT ALTERNATIVES
The treatment alternatives wouldhave been conventional dentaldrills to roughen the dentalsurfaces; those burs could causegreater loss of hard tissue,microfractures of the tooth enamel,pulp exposition, and tenderness.
8. INFORMED CONSENT
Upon receiving a full explanation ofthe procedure, with associatedrisks, benefits, and alternatives, thepatient and his parents gaveconsent to perform the treatment.
TREATMENTA. Treatment Objectives StrategyThe primary objective was to use
Figure 1: The patient with three fractured frontal teeth, with the fragments displayedseparately
61
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
Iaria et al.
the Er:YAG laser to prepare thetwo surfaces, one of the fracturedteeth and one of the fragments, formaximum adhesion withoutgreater loss of hard tissue ormicrofractures and without the useof injectable dental anesthetics.
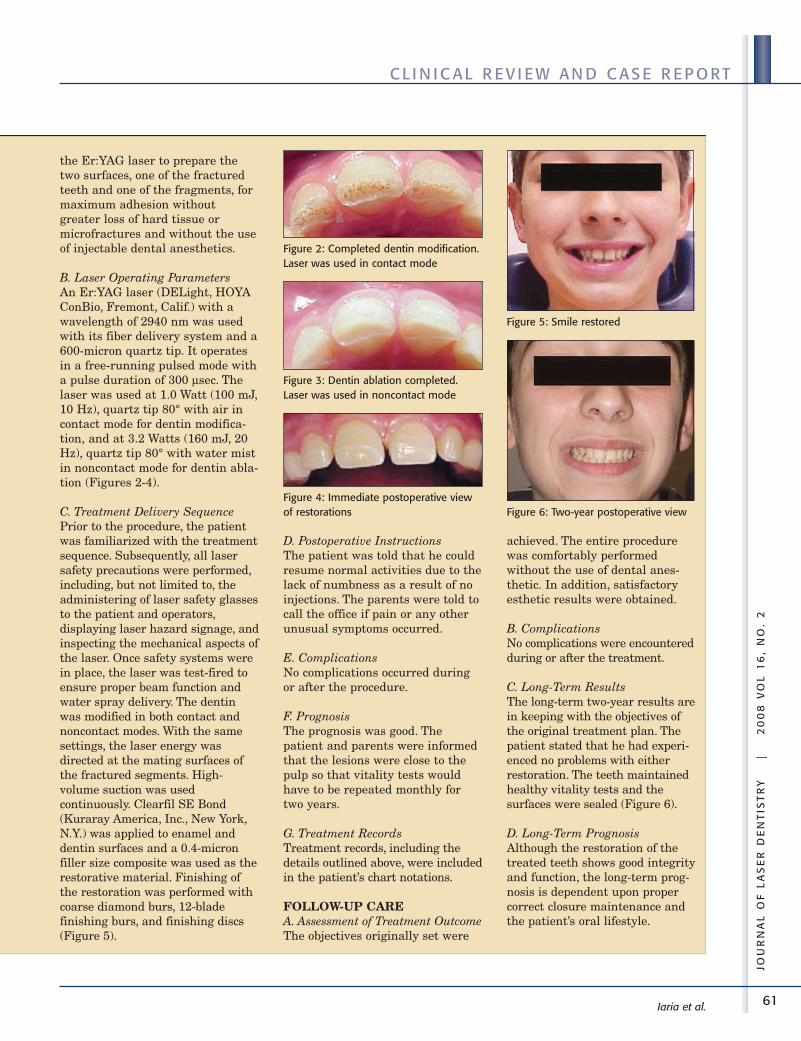
B. Laser Operating ParametersAn Er:YAG laser (DELight, HOYAConBio, Fremont, Calif.) with awavelength of 2940 nm was usedwith its fiber delivery system and a600-micron quartz tip. It operatesin a free-running pulsed mode witha pulse duration of 300 μsec. Thelaser was used at 1.0 Watt (100 mJ,10 Hz), quartz tip 80° with air incontact mode for dentin modifica-tion, and at 3.2 Watts (160 mJ, 20Hz), quartz tip 80° with water mistin noncontact mode for dentin abla-tion (Figures 2-4).
C. Treatment Delivery SequencePrior to the procedure, the patientwas familiarized with the treatmentsequence. Subsequently, all lasersafety precautions were performed,including, but not limited to, theadministering of laser safety glassesto the patient and operators,displaying laser hazard signage, andinspecting the mechanical aspects ofthe laser. Once safety systems werein place, the laser was test-fired toensure proper beam function andwater spray delivery. The dentinwas modified in both contact andnoncontact modes. With the samesettings, the laser energy wasdirected at the mating surfaces ofthe fractured segments. High-volume suction was usedcontinuously. Clearfil SE Bond(Kuraray America, Inc., New York,N.Y.) was applied to enamel anddentin surfaces and a 0.4-micronfiller size composite was used as therestorative material. Finishing ofthe restoration was performed withcoarse diamond burs, 12-bladefinishing burs, and finishing discs(Figure 5).
D. Postoperative InstructionsThe patient was told that he couldresume normal activities due to thelack of numbness as a result of noinjections. The parents were told tocall the office if pain or any otherunusual symptoms occurred.
E. ComplicationsNo complications occurred duringor after the procedure.
F. PrognosisThe prognosis was good. Thepatient and parents were informedthat the lesions were close to thepulp so that vitality tests wouldhave to be repeated monthly fortwo years.
G. Treatment RecordsTreatment records, including thedetails outlined above, were includedin the patient’s chart notations.
FOLLOW-UP CAREA. Assessment of Treatment OutcomeThe objectives originally set were
achieved. The entire procedurewas comfortably performedwithout the use of dental anes-thetic. In addition, satisfactoryesthetic results were obtained.
B. ComplicationsNo complications were encounteredduring or after the treatment.
C. Long-Term ResultsThe long-term two-year results arein keeping with the objectives ofthe original treatment plan. Thepatient stated that he had experi-enced no problems with eitherrestoration. The teeth maintainedhealthy vitality tests and thesurfaces were sealed (Figure 6).
D. Long-Term PrognosisAlthough the restoration of thetreated teeth shows good integrityand function, the long-term prog-nosis is dependent upon propercorrect closure maintenance andthe patient’s oral lifestyle.
Figure 2: Completed dentin modification.Laser was used in contact mode
Figure 3: Dentin ablation completed.Laser was used in noncontact mode
Figure 4: Immediate postoperative viewof restorations
Figure 5: Smile restored
Figure 6: Two-year postoperative view
62
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
for water allows for selective abla-tion, whereby greater absorptiontakes place in demineralizedtissue richer in organic materialand with a higher percentage ofwater; this allows some protectionof the sound underlying tissuewith a reduced penetration of thebeam. The accumulation of abla-tion debris within a deep cavitycan lead to “superheating” whichcan lead to conductive heatdamage. Without water use, laserlight may be absorbed by themineral and the crystals them-selves may be heated above theirmelting point.
Furthermore, any lack of watercan lead to cracks in enamel or canresult in melting of dentin withconsequent flat adhesion surfaces.Thus negative effects for the enamelmean possible marginal leakage,and for the dentin possible nonad-hesion of the completed restoration.
4. Exceptions to Using WaterSprayThere are two clinical situationsthe restorative dentist mightencounter which can be treatedwith lasers without the simulta-neous use of a coaxial water spray:
a. Desensitizing TechniqueThis technique must be donewithout water and without contactwith the tooth, for a short time onlyand with low power (using low Hzand low mJ).26
b. Pulp CappingThis technique must be carried outwithout water but with air cooling,and the tip must touch the surfacefor only a few seconds.27
5. Cavity MarginConsiderationsA succession of studies has identi-fied the fragility of laser-irradiatedenamel, relative to the stability ofthe postrestoration margins.Studies have proposed an approachof combined laser-irradiation, acid-etch techniques to overcome such
potential problems. Laser irradia-tion of enamel is not a validalternative to acid-etchingpretreatment for resin compositematerials adhesion.
Irrespectively, there may wellremain the need to remove grosslyoverhanging and unsupportedenamel with a rotary bur, in orderto either expedite cavity prepara-
tion or provide a stable postrestora-tion margin.28-33
6. Acid-Etch ConsiderationsWhile the surface produced by thelaser is similar to the convention-ally prepared, etched enamelsurface, it still requires acidetching to obtain an equivalent
Iaria et al.
Case #2U S E O F A N E R : YAGL AS E R TO P R E PA R ET E ET H F O R V E N E E RP L AC E M E N T
PRETREATMENTA. Outline of Case1. FULL CLINICAL DESCRIPTION
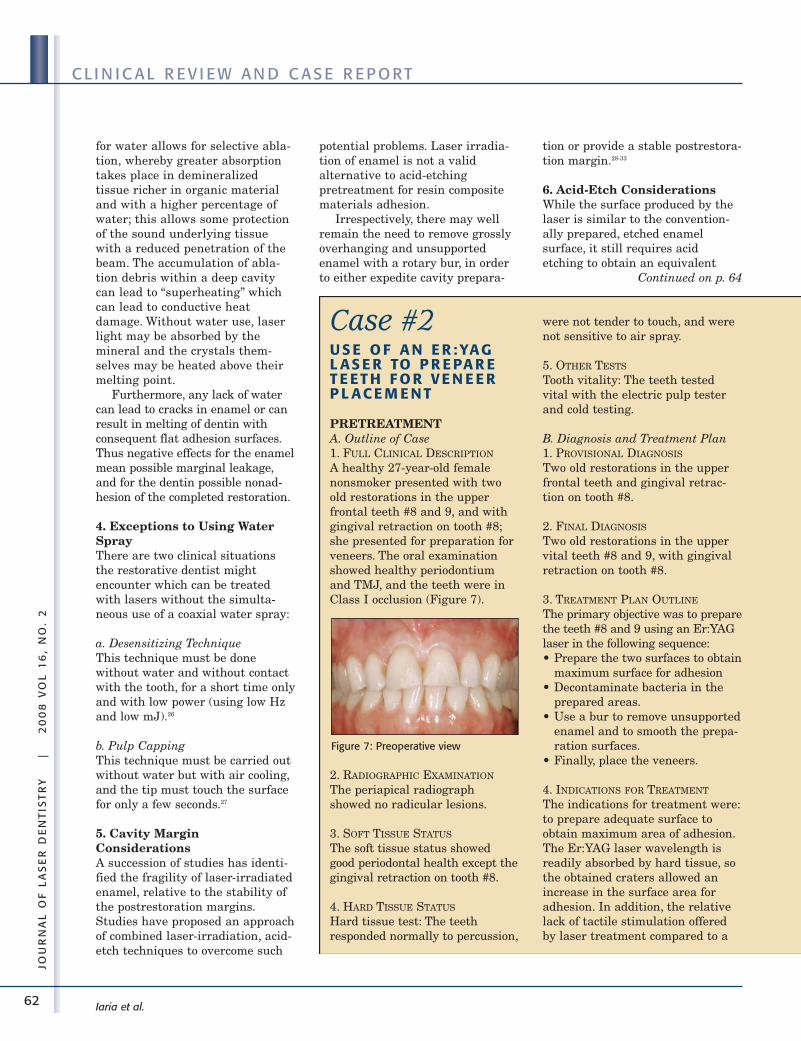
A healthy 27-year-old femalenonsmoker presented with twoold restorations in the upperfrontal teeth #8 and 9, and withgingival retraction on tooth #8;she presented for preparation forveneers. The oral examinationshowed healthy periodontiumand TMJ, and the teeth were inClass I occlusion (Figure 7).
2. RADIOGRAPHIC EXAMINATION
The periapical radiographshowed no radicular lesions.
3. SOFT TISSUE STATUS
The soft tissue status showedgood periodontal health except thegingival retraction on tooth #8.
4. HARD TISSUE STATUS
Hard tissue test: The teethresponded normally to percussion,
were not tender to touch, and werenot sensitive to air spray.
5. OTHER TESTS
Tooth vitality: The teeth testedvital with the electric pulp testerand cold testing.
B. Diagnosis and Treatment Plan1. PROVISIONAL DIAGNOSIS
Two old restorations in the upperfrontal teeth and gingival retrac-tion on tooth #8.
2. FINAL DIAGNOSIS
Two old restorations in the uppervital teeth #8 and 9, with gingivalretraction on tooth #8.
3. TREATMENT PLAN OUTLINE
The primary objective was to preparethe teeth #8 and 9 using an Er:YAGlaser in the following sequence:• Prepare the two surfaces to obtain
maximum surface for adhesion• Decontaminate bacteria in the
prepared areas.• Use a bur to remove unsupported
enamel and to smooth the prepa-ration surfaces.
• Finally, place the veneers.
4. INDICATIONS FOR TREATMENT
The indications for treatment were:to prepare adequate surface toobtain maximum area of adhesion.The Er:YAG laser wavelength isreadily absorbed by hard tissue, sothe obtained craters allowed anincrease in the surface area foradhesion. In addition, the relativelack of tactile stimulation offeredby laser treatment compared to a
Figure 7: Preoperative view
Continued on p. 64
63
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
Iaria et al.
conventional high-speed handpieceoften allows the procedure to beperformed without the need forneedle analgesia.
5. CONTRAINDICATIONS FOR
TREATMENT
There are no absolute contraindica-tions for performing the procedure.
6. PRECAUTIONS FOR WAVELENGTH
Adequate water spray must bemaintained as the procedure isbeing performed. Good visibility andlow power will be necessary forcareful preparation in order to avoidboth thermal damage and excessiveremoval of tooth structure.
7. TREATMENT ALTERNATIVES
The treatment alternatives wouldhave been conventional dentaldrills to roughen the dentalsurfaces; those burs could causegreater loss of hard tissue andincrease of pulp temperature.
8. INFORMED CONSENT
Upon receiving a full explanation ofthe procedure, with associatedrisks, benefits, and alternatives, thepatient gave consent to perform thetreatment.
TREATMENTA. Treatment Objectives StrategyThe primary objective was to usethe Er:YAG laser to prepare the twosurfaces for maximum adhesionwithout greater loss of hard tissueor microfractures and without theuse of injectable dental anesthetics.
B. Laser Operating ParametersAn Er:YAG laser (DELight, HOYAConBio, Fremont, Calif.) with awavelength of 2940 nm was usedwith its fiber delivery system and a600-micron quartz tip. It operatesin a free-running pulsed mode witha pulse duration of 300 μ sec. Thelaser was used at 0.65 Watt (65 mJ,10 Hz) quartz tip 30° with watermist in noncontact mode.
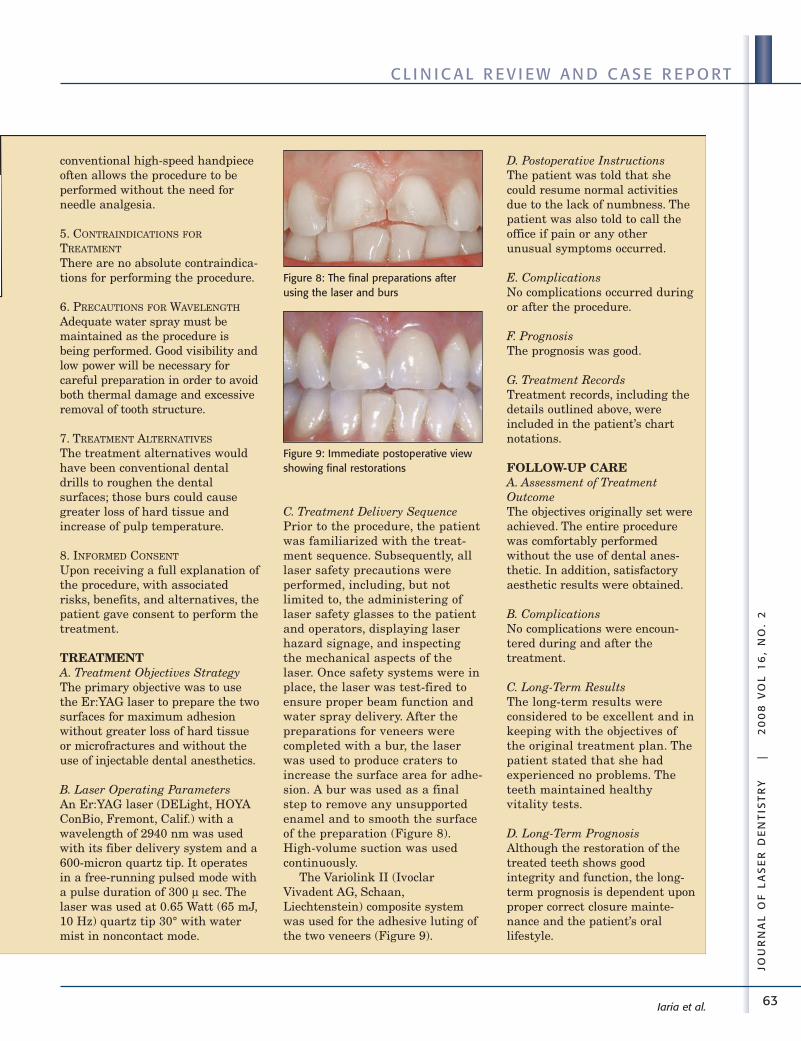
C. Treatment Delivery SequencePrior to the procedure, the patientwas familiarized with the treat-ment sequence. Subsequently, alllaser safety precautions wereperformed, including, but notlimited to, the administering oflaser safety glasses to the patientand operators, displaying laserhazard signage, and inspectingthe mechanical aspects of thelaser. Once safety systems were inplace, the laser was test-fired toensure proper beam function andwater spray delivery. After thepreparations for veneers werecompleted with a bur, the laserwas used to produce craters toincrease the surface area for adhe-sion. A bur was used as a finalstep to remove any unsupportedenamel and to smooth the surfaceof the preparation (Figure 8).High-volume suction was usedcontinuously.
The Variolink II (IvoclarVivadent AG, Schaan,Liechtenstein) composite systemwas used for the adhesive luting ofthe two veneers (Figure 9).
Figure 8: The final preparations afterusing the laser and burs
Figure 9: Immediate postoperative viewshowing final restorations
D. Postoperative InstructionsThe patient was told that shecould resume normal activitiesdue to the lack of numbness. Thepatient was also told to call theoffice if pain or any otherunusual symptoms occurred.
E. ComplicationsNo complications occurred duringor after the procedure.
F. PrognosisThe prognosis was good.
G. Treatment RecordsTreatment records, including thedetails outlined above, wereincluded in the patient’s chartnotations.
FOLLOW-UP CAREA. Assessment of TreatmentOutcomeThe objectives originally set wereachieved. The entire procedurewas comfortably performedwithout the use of dental anes-thetic. In addition, satisfactoryaesthetic results were obtained.
B. ComplicationsNo complications were encoun-tered during and after thetreatment.
C. Long-Term ResultsThe long-term results wereconsidered to be excellent and inkeeping with the objectives ofthe original treatment plan. Thepatient stated that she hadexperienced no problems. Theteeth maintained healthyvitality tests.
D. Long-Term PrognosisAlthough the restoration of thetreated teeth shows goodintegrity and function, the long-term prognosis is dependent uponproper correct closure mainte-nance and the patient’s orallifestyle.
64
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
Iaria et al.
bond strength. Laser irradiation ofenamel is not a valid alternative toacid-etching pretreatment for resincomposite materials adhesion.28-40
7. Avoidance of Dehydration ofDentinAs stated above, laser ablation ofdentin does not produce a smearlayer so this layer cannot impedeadhesion to laser-irradiated surfaces.Nevertheless when the erbium lasersare used, there is a selective ablationof organic tissue so that after acid-etching and laser conditioning ofdentin there is less collagen left to beexposed and consequently to behybridized. The weakest point withlaser-treated dentin is the regionimmediately below the dentin layerinfiltrated by resin.36 A study byCeballos and colleagues37 usingtransmission electron microscopyshowed a 3-4 nm altered dentinsubsurface, with collagen fibrilswithout cross-banding and fusedtogether, and elimination of interfib-rillar space. Thus a bonding systemmust be used to ensure restorationretention.38
8. Choice of CompositeRestorative MaterialsThe choice of composite materialsmust be made on the basis of thedepth and width of dentin craters,and the use of composite nano- ormicro-fillers is fundamental to theproper restoration of laser-ablatedcavities. Whenever possible, the useof a first layer of composite flow isadvisable.
Studies have shown that theseal at enamel margins in Er:YAGlaser-irradiated preparationsdepends on the resin compositeformulation of the correspondingadhesive.39-40
9. Isolation and SafetyConsiderationsStudies have shown that theEr:YAG laser demonstrates bacteri-cidal potential for dentin.41-42 Arubber dam isolation technique
Case #3ER:YAG LASER-ASSISTEDTREATMENT OF ANENAMEL DEFECT
PRETREATMENTA. Outline of Case1. FULL CLINICAL DESCRIPTION
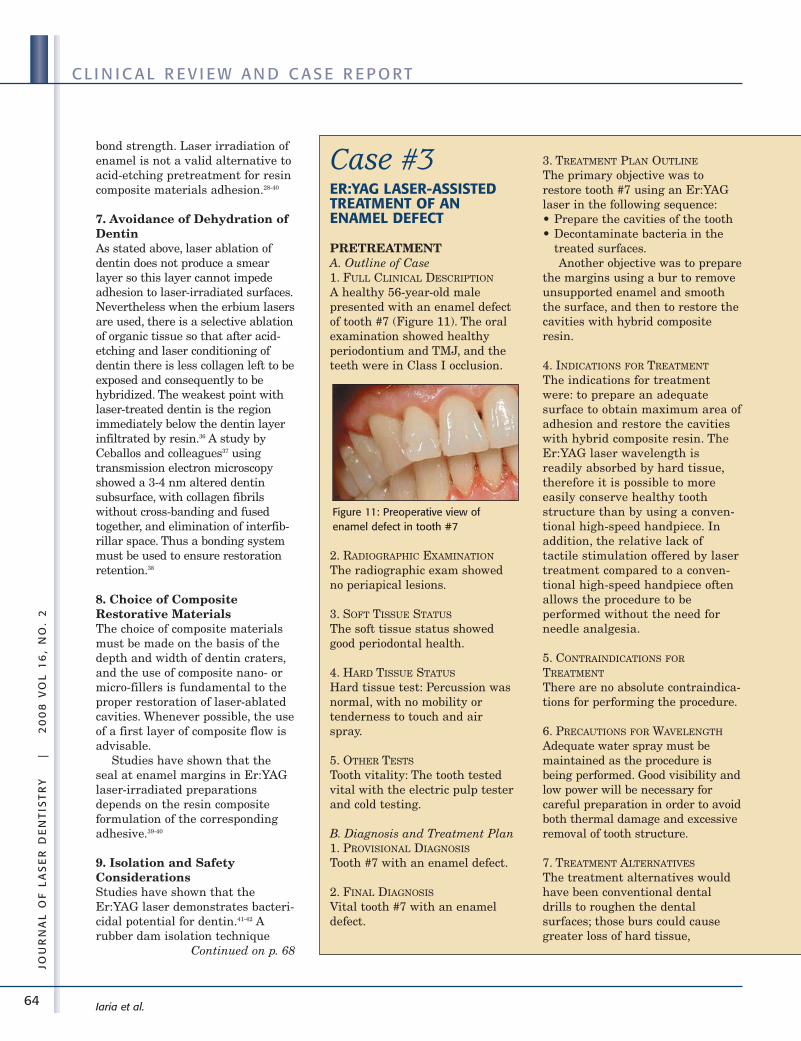
A healthy 56-year-old malepresented with an enamel defectof tooth #7 (Figure 11). The oralexamination showed healthyperiodontium and TMJ, and theteeth were in Class I occlusion.
2. RADIOGRAPHIC EXAMINATION
The radiographic exam showedno periapical lesions.
3. SOFT TISSUE STATUS
The soft tissue status showedgood periodontal health.
4. HARD TISSUE STATUS
Hard tissue test: Percussion wasnormal, with no mobility ortenderness to touch and airspray.
5. OTHER TESTS
Tooth vitality: The tooth testedvital with the electric pulp testerand cold testing.
B. Diagnosis and Treatment Plan1. PROVISIONAL DIAGNOSIS
Tooth #7 with an enamel defect.
2. FINAL DIAGNOSIS
Vital tooth #7 with an enameldefect.
3. TREATMENT PLAN OUTLINE
The primary objective was torestore tooth #7 using an Er:YAGlaser in the following sequence:• Prepare the cavities of the tooth• Decontaminate bacteria in the
treated surfaces.Another objective was to prepare
the margins using a bur to removeunsupported enamel and smooththe surface, and then to restore thecavities with hybrid compositeresin.
4. INDICATIONS FOR TREATMENT
The indications for treatmentwere: to prepare an adequatesurface to obtain maximum area ofadhesion and restore the cavitieswith hybrid composite resin. TheEr:YAG laser wavelength isreadily absorbed by hard tissue,therefore it is possible to moreeasily conserve healthy toothstructure than by using a conven-tional high-speed handpiece. Inaddition, the relative lack oftactile stimulation offered by lasertreatment compared to a conven-tional high-speed handpiece oftenallows the procedure to beperformed without the need forneedle analgesia.
5. CONTRAINDICATIONS FOR
TREATMENT
There are no absolute contraindica-tions for performing the procedure.
6. PRECAUTIONS FOR WAVELENGTH
Adequate water spray must bemaintained as the procedure isbeing performed. Good visibility andlow power will be necessary forcareful preparation in order to avoidboth thermal damage and excessiveremoval of tooth structure.
7. TREATMENT ALTERNATIVES
The treatment alternatives wouldhave been conventional dentaldrills to roughen the dentalsurfaces; those burs could causegreater loss of hard tissue,
Figure 11: Preoperative view ofenamel defect in tooth #7
Continued on p. 68
65
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
Iaria et al.
microfractures of the tooth enamel,and tenderness.
8. INFORMED CONSENT
Upon receiving a full explanation ofthe procedure, with associatedrisks, benefits, and alternatives, thepatient gave consent to perform thetreatment.
TREATMENTA. Treatment Objectives StrategyThe primary objective was to usethe Er:YAG laser to prepare thesurfaces of the cavities in order toobtain the maximum adhesionwithout greater loss of hardtissue or microfractures andwithout the use of injectabledental anesthetics.
B. Laser Operating ParametersAn Er:YAG laser (DELight, HOYAConBio, Fremont, Calif.) with awavelength of 2940 nm was usedwith its fiber delivery system and a600-micron quartz tip. It operatesin a free-running pulsed mode witha pulse duration of 300 μsec. Thelaser was used at 5 Watts (200 mJ,25 Hz), quartz tip 80° with watermist in noncontact mode forenamel ablation, and at 3.2 Watts(160 mJ, 20 Hz), quartz tip 80°with water mist in noncontactmode for dentin ablation.
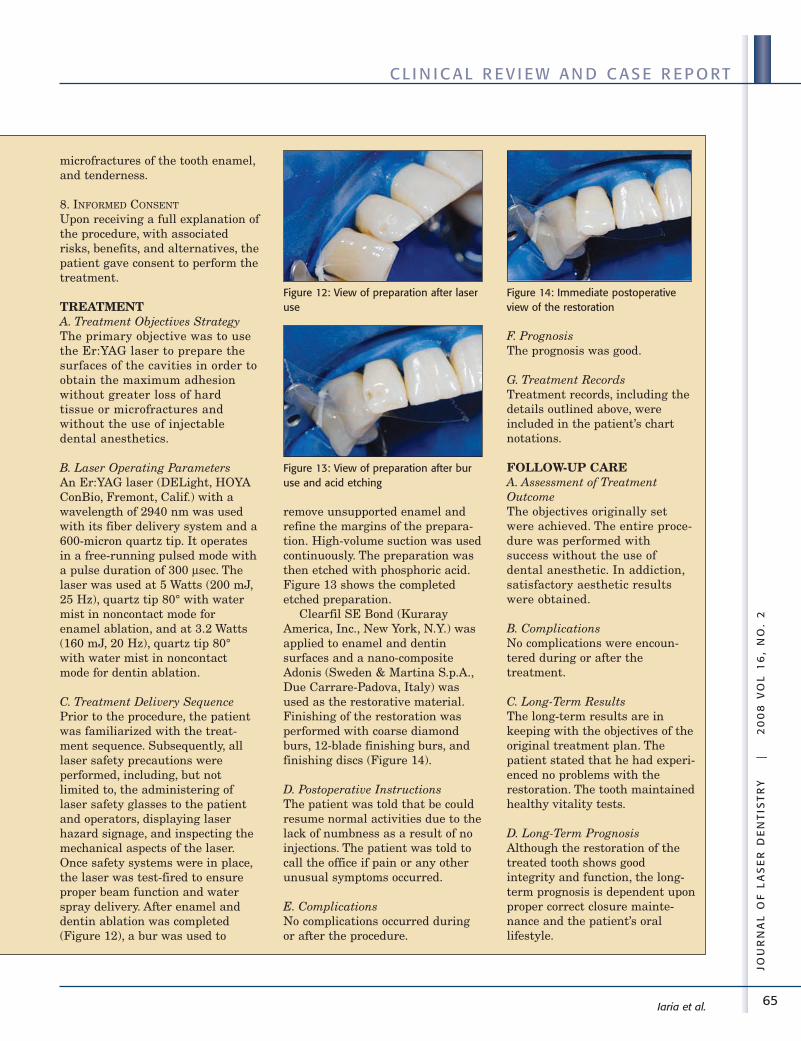
C. Treatment Delivery SequencePrior to the procedure, the patientwas familiarized with the treat-ment sequence. Subsequently, alllaser safety precautions wereperformed, including, but notlimited to, the administering oflaser safety glasses to the patientand operators, displaying laserhazard signage, and inspecting themechanical aspects of the laser.Once safety systems were in place,the laser was test-fired to ensureproper beam function and waterspray delivery. After enamel anddentin ablation was completed(Figure 12), a bur was used to
remove unsupported enamel andrefine the margins of the prepara-tion. High-volume suction was usedcontinuously. The preparation wasthen etched with phosphoric acid.Figure 13 shows the completedetched preparation.
Clearfil SE Bond (KurarayAmerica, Inc., New York, N.Y.) wasapplied to enamel and dentinsurfaces and a nano-compositeAdonis (Sweden & Martina S.p.A.,Due Carrare-Padova, Italy) wasused as the restorative material.Finishing of the restoration wasperformed with coarse diamondburs, 12-blade finishing burs, andfinishing discs (Figure 14).
D. Postoperative InstructionsThe patient was told that be couldresume normal activities due to thelack of numbness as a result of noinjections. The patient was told tocall the office if pain or any otherunusual symptoms occurred.
E. ComplicationsNo complications occurred duringor after the procedure.
F. PrognosisThe prognosis was good.
G. Treatment RecordsTreatment records, including thedetails outlined above, wereincluded in the patient’s chartnotations.
FOLLOW-UP CAREA. Assessment of TreatmentOutcomeThe objectives originally setwere achieved. The entire proce-dure was performed withsuccess without the use ofdental anesthetic. In addiction,satisfactory aesthetic resultswere obtained.
B. ComplicationsNo complications were encoun-tered during or after thetreatment.
C. Long-Term ResultsThe long-term results are inkeeping with the objectives of theoriginal treatment plan. Thepatient stated that he had experi-enced no problems with therestoration. The tooth maintainedhealthy vitality tests.
D. Long-Term PrognosisAlthough the restoration of thetreated tooth shows goodintegrity and function, the long-term prognosis is dependent uponproper correct closure mainte-nance and the patient’s orallifestyle.
Figure 12: View of preparation after laseruse
Figure 13: View of preparation after buruse and acid etching
Figure 14: Immediate postoperativeview of the restoration

66
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
Iaria et al.
must be used in every procedure tomaintain the decontaminationprovided by the laser. As illustratedin Figure 10, safety measuresshould include the use of:• wavelength- and device-specific
protection glasses for the doctor,the assistant, and patient
• appropriate face masks to avoidplume aspiration
• high-speed evacuation of plumeand debris
• nonreflecting instruments• magnification to better visualize
and control the dentist’s work.
10. Miracles Don’t Happen!Finally, it should be rememberedthat lasers are not magic wands —a lot can be done with lasers, butthe dentist’s knowledge and experi-ence take precedence over the tools.An accurate diagnosis is the onlybasis to offer the patient thecorrect therapy which must becarried out with due expertise.
A U T H O R B I O G R A P H I ESDr. Prof. Giuseppe Iaria qualified inMedicine and Surgery at Universityof Milan in 1984. His postgraduatedental qualifications — Dentist and
Orthodontist – were obtained at theUniversity of Milan in 1987 and1989 with the highest marks.During the Sixth InternationalConference of the Academy of LaserDentistry in Palm Springs,California in February 1999, heachieved his certificate of Master ofthe Academy of Laser Dentistry. OnOctober 22, 2000 he obtained thecertification of Dental LaserEducator at the University ofCalifornia San Francisco. In 2001,the publishing house UTETpublished his text entitled TheLasers in Dentistry and OralSurgery. On April 16, 2004 he wascertified with the InternationalSociety for Lasers in Dentistry.
Currently Dr. Prof. Iaria is amember of the Science and ResearchCommittee of the Academy of LaserDentistry. He serves as a referee andeditorial board member for severalinternational dental journals andhas held consultancies with manyinternational laser companies. Heparticipated as a speaker at impor-tant national and internationalconferences and has conductedseveral courses on the use of lasersin dentistry.
Dr. Prof. Iaria is a consultingteacher for Masters in LaserDentistry at University Courses inGenoa and Rome. He is VicePresident of the InternationalAcademy of High Tech (IAHT) andChairman of the Accademia LaserDentale Italiana (ALDI), the ItalianStudy Club of the Academy of LaserDentistry. He is a teacher at theUniversity of Genoa and a lectureron lasers in dentistry at theUniversity of Genoa and Rome. Heworks and lives in Brescia, Italy.
Dr. Prof. Iaria may be contactedby e-mail at [email protected].
Disclosure: Dr. Prof. Iaria has nocurrent affiliations with anycompany.
Dr. Steven Parker studieddentistry at University CollegeHospital Medical School,University of London, UK andgraduated in 1974. He maintains aPrivate Practice in Harrogate, UK.He holds Fellowship and Diplomatestatus with the InternationalCongress of Oral Implantologists.
Dr. Parker has been involved inthe use of lasers in dentistry since1990. Prior to joining the Academyof Laser Dentistry in 1993, he wasPresident of the British DentalLaser Association. He joined theBoard of Directors of the Academyin 1996 and became chair of theInternational RelationsCommittee. From 1999 through2004, he was chair of theCommittee for ProficiencyRecognition and co-editor ofWavelengths, the former journal ofthe Academy of Laser Dentistry.He was awarded the LeonGoldman award for Excellence inClinical Laser Dentistry by theAcademy in 1998. In addition, Dr.Parker holds Advanced Proficiencystatus in multiple laser wave-lengths and completed theAcademy Educator Course at theUniversity of California SanFrancisco.
Figure 10: Correct mode of operation using lasers with proper safety measures depicted
67
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
Dr. Parker may be contacted bye-mail at [email protected].
Disclosure: Dr. Parker has nocurrent commercial affiliation.
R E F E R E N C ES1. Keller U, Hibst R. Zur ablativen
wirkung des Er:YAG-lasers aufschmelz und dentin. [Ablative effectof an Er:YAG laser on enamel anddentin.] Dtsch Zahnarztl Z1989;44(8):600-602. German.
2. Pelagalli J, Gimbel CB, Hansen RT,Swett A, Winn DW 2nd.Investigational study of the use ofEr:YAG laser versus dental drill forcaries removal and cavity prepara-tion – Phase I. J Clin Laser MedSurg 1997;15(3):109-115.
3. Takamori K, Furukawa H,Morikawa Y, Katayama T, WatanabeS. Basic study on vibrations duringtooth preparations caused by high-speed drilling and Er:YAG laserirradiation. Lasers Surg Med2003;32(1):25-31.
4. Glockner K, Rumpler J, EbelesederK, Städtler P. Intrapulpal tempera-ture during preparation with theEr:YAG laser compared to theconventional burr: An in vitro study.J Clin Laser Med Surg1998;16(3):153-157.
5. Miserendino LJ, Cozean CD.Histological results following in-vivocavity preparation with an Er:YAGlaser. In: Featherstone JDB,Rechmann P, Fried DS, editors.Lasers in dentistry IV, January 25-26, 2998, San Jose, Calif. Proc. SPIE3248. Bellingham, Wash.:SPIE –The International Society forOptical Engineering, 1998:46-50.
6. Dostálová T, Jelínková H, Krejsa O,Hamal K, Kubelka J, Procházka S,Himmlová L. Dentin and pulpresponse to erbium:YAG laser abla-tion: A preliminary evaluation ofhuman teeth. J Clin Laser MedSurg 1997;15(3):117-121.
7. Oelgiesser D, Blasbalg J, Ben-AmarA. Cavity preparation by Er-YAGlaser on pulpal temperature rise.Am J Dent 2003;16(2):96-98.
8. Parker SPA, Darbar AA,Featherstone JDB, Iaria G, Kesler
G, Rechmann P, Swick MD, WhiteJM, Wigdor HA. The use of laserenergy for therapeutic ablation ofintraoral hard tissues. PositionPaper: Science and ResearchCommittee, Academy of LaserDentistry, Adopted March 2007. JLaser Dent 2007;15(2):78-86.
9. Mercer CE, Anderson P, Davis GR.Sequential 3D X-ray microtomo-graphic measurement of enamel anddentine ablation by an Er:YAGlaser. Br Dent J 2003;194(2):99-104;discussion 89.
10. Mehl A, Kremers L, Salzmann K,Hickel R. 3D volume-ablation rateand thermal side effects with theEr:YAG and Nd:YAG laser. DentMater 1997;13(4):246-251.
11. Delmé KIM, Deman PJ, De BruyneMAA, De Moor RJG. Influence ofdifferent Er:YAG laser energies andfrequencies on the surfacemorphology of dentin and enamel. JOral Laser Appl 2006;6(1):43-52.
12. Fried D. IR laser ablation of dentalenamel. In: Featherstone JDB,Rechmann P, Fried D, editors.Lasers in Dentistry VI, January 23-24, 2000 San Jose, Calif. Proc. SPIE3910. Bellingham, Wash.:SPIE –The International Society forOptical Engineering, 2000:136-148.
13. Keller U, Raab WH, Hibst R. Diepulpareaktion während derbestrahlung von zahnhartsub-stanzen mit dem erbium-YAG-laser.[Pulp reactions during erbium:YAGlaser irradiation of hard tooth struc-ture.] Dtsch Zahnarztl Z1991;46(2):158-160. German.
14. Apel C, Meister J, Ioana RS,Franzen R, Hering P, Gutknecht N.The ablation threshold of Er:YAGand Er:YSGG laser radiation indental enamel. Lasers Med Sci2002;17(4):246-252.
15. Moshonov J, Stabholz A, Leopold Y,Rosenberg I, Stabholz A. [Lasers indentistry. Part B – Interaction withbiological tissues and the effect onthe soft tissues of the oral cavity, thehard tissues of the tooth and thedental pulp.] Refuat HapehVehashinayim 2001;18(3-4):21-28,107-108. Hebrew.
16. Cozean C, Arcoria CJ, Pelagalli J,Powell GL. Dentistry for the 21st
century? Erbium:YAG laser forteeth. J Am Dent Assoc1997;128(8):1080-1087.
17. Curti M, Rocca JP, Bertrand MF,Nammour S. Morpho-structuralaspects of erbium:YAG-preparedclass V cavities. J Clin Laser MedSurg 2004;22(2):119-123.
18. Featherstone JDB, Fried D.Fundamental interactions of laserswith dental hard tissues. Med LaserApp 2001;16(3):181-194.
19. Rizoiu I, Kohanghadosh F, KimmelAI, Eversole LR. Pulpal thermalresponses to anerbium,chromium:YSGG pulsedlaser hydrokinetic system. OralSurg Oral Med Pathol Oral RadiolEndod 1998;86(2):220-223.
20. Paghdiwala AF, Vaidyanathan TK,Paghdiwala MF. Evaluation oferbium:YAG laser radiation of harddental tissues: Analysis of tempera-ture changes, depth of cuts andstructural effects. Scanning Microsc1993;7(3):989-997.
21. Trajtenberg CP, Pereria PNR,Powers JM. Resin bond strengthand micromorphology of humanteeth prepared with an Erbium:YAGlaser. Am J Dent 2004;17(5):331-336.
22. Hoke JA, Burkes EJ Jr, Gomes ED,Wolbarsht ML. Er:YAG (2.94-µm)laser effects on dental hard tissues.J Laser Appl 1990;2(3-4):61-65.
23. Dostálová T, Jelínková H, Krejsã O,Hamal K. Evaluation of the surfacechanges in enamel and dentin dueto possibility of thermal overheatinginduced by erbium:YAG laser radia-tion. Scanning Microsc1996;10(1):285-291.
24. Wigdor H, Abt E, Ashrafi S, WalshJT Jr. The effect of lasers on dentalhard tissues. J Am Dent Assoc1993;124(2):65-70.
25. Visuri SR, Walsh JT Jr, Wigdor HA.Erbium laser ablation of dental hardtissue: Effect of water cooling. LasersSurg Med 1996;18(3):294-300.
26. Schwarz F, Arweiler N, Georg T,Reich E. Desensitizing effects of anEr:YAG laser on hypersensitivedentine. J Clin Periodontol2002;29(3):211-215.
Iaria et al.
68
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
27. Olivi G, Genovese MD, Maturo P,Docimo R. Pulp capping: Advantagesof using laser technology. Eur JPaediatr Dent 2007;8(2):89-95.
28. Niu W, Eto JN, Kimura Y, TakedaFH, Matsumoto K. A study onmicroleakage after resin filling ofclass V cavities prepared by Er:YAGlaser. J Clin Laser Med Surg1998;16(4):227-231.
29. Gutknecht N, Apel C, Schäfer C,Lampert F. Microleakage ofcomposite fillings in Er,Cr:YSGGlaser-prepared class II cavities.Lasers Surg Med 2001;28(4):371-374.
30. Kohara EK, Hossain M, Kimura Y,Matsumoto K, Inoue M, Sasa R.Morphological and microleakagestudies of the cavities prepared byEr:YAG laser irradiation in primaryteeth. J Clin Laser Med Surg2002;20(3):141-147.
31. Corona SA, Borsatto M, Dibb RG,Ramos RP, Brugnera A, Pécora JD.Microleakage of class V resincomposite restorations after bur, air-abrasion or Er:YAG laserpreparation. Oper Dent2001;26(5):491-497.
32. Corona SA, Borsatto MC, Pecora JD,De SA Rocha RA, Ramos TS, Palma-Dibb RG. Assessing microleakage ofdifferent class V restorations afterEr:YAG laser and bur preparation. JOral Rehabil 2003;30(10):1008-1014.
33. Chinelatti MA, Ramos RP, ChimelloDT, Borsatto MC, Pécora JD, Palma-
Dibb RG. Influence of the use ofEr:YAG laser for cavity preparationand surface treatment inmicroleakage of resin-modified glassionomer restorations. Oper Dent2004;29(4):430-436.
34. Ceballos L, Osorio R, Toledano M,Marshall GW. Microleakage ofcomposite restorations after acid orEr-YAG laser cavity treatments.Dent Mater 2001;17(4):340-346.
35. Luddin N, Ngo H, McIntyre J,Abbott J. Comparative study of theultrastructure and adhesive proper-ties of enamel prepared by Er:YAGlaser and conventional bur. J OralLaser Appl 2006;6(2):89-94.
36. De Munck J, Van Meerbeek B,Yudhira R, Lambrechts P, VanherleG. Micro-tensile bond strength oftwo adhesives to erbium:YAG-lasedvs. bur-cut enamel and dentin. EurJ Oral Sci 2002;110(4):322-329.
37. Ceballos L, Toledano M, Osorio R,Tay FR, Marshall GW. Bonding toEr-YAG-laser-treated dentin. J DentRes 2002;81(2):119-122.
38. Esteves-Oliveira M, Zezell DM, ApelC, Turbino ML, Aranha ACC,Eduardo Cde P, Gutknecht N. Bondstrength of self-etching primer tobur cut, Er,Cr:YSGG, and Er:YAGlased dental surfaces. PhotomedLaser Surg 2007;25(5):373-380.
39. Delme KI, Deman PJ, De Moor RJ.Microleakage of class V resincomposite restorations after conven-tional and Er:YAG laser
preparation. J Oral Rehabil2005;32(9):676-685.
40. Donadio-Moura J, Gouw-Soares S,de Freitas PM, Navarro RS, PowellLG, Eduardo Cde P. Tensile bondstrength of a flowable compositeresin to Er:YAG-laser-treateddentin. Lasers Surg Med2005;36(5):351-355.
41. Aoki A, Ishikawa I, Yamada T,Otsuki M, Watanabe H, Tagami J,Ando Y, Yamamoto H. Comparisonbetween Er:YAG laser and conven-tional technique for root cariestreatment in vitro. J Dent Res1998;77(6):1404-1414.
42. Hibst R, Stock K, Gall R, Keller U.Controlled tooth surface heatingand sterilisation by the Er:YAGlaser radiation. In: Altshuler GB,Chiesa F, Geschwind HJ, Hibst R,Krasner N, Laffitté F, Maira G,Neumann R, Pini R, Reidenbach H-D, Roggan A, Serra I Mila M,editors. Laser applications in medi-cine and dentistry, September 7-10,1996, Vienna, Austria. Proc. SPIE2922. Bellingham, Wash.:SPIE –The International Society forOptical Engineering, 1996:119-126.
Editor’s Note: USA clinicians areadvised that no erbium laser has beencleared by the U.S. Food and DrugAdministration for the desensitization,pulp capping, and decontaminationprocedures and bactericidal propertiesidentified in this article. ■■
Iaria et al.
69
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
COV E R F E AT U R E
Peri-Implantitis Therapy with an Er:YAG LaserAvi Reyhanian, DDS, Natanya, Israel
Donald J. Coluzzi, DDS, Portola Valley, CaliforniaJ Laser Dent 2008;16(2):69-74
I N T R O D U C T I O NOsseointegrated dental implantshave become a routinely recom-mended procedure in the clinicalpractice of dentistry.1-4 Althoughthey can be highly successfulrestorations, implant failure canand does still occur.5-8 Among themany complications possible in theprocedure, one of the more commonpostoperative ones is peri-implantdisease and, within this category,peri-implantitis.9
Three major factors contributeto the failure and complications ofimplants:1. Patient-related factors2. Iatrogenic (doctor/team) factors3. Surgical equipment / manufac-
turer problems.Patient and iatrogenic factors
are more prevalent than implantmanufacturing problems.
Implant complications aredivided into two main categories:Intraoperative and postoperative.9
Peri-implantitis is a postoperativecomplication.
Biofilms form on all hard,nonshedding surfaces in a fluidsystem, i.e., both on teeth and onoral implants. As a result of thebacterial challenge, the hostresponds by mounting a defensemechanism leading to inflamma-tion of the soft tissue. In theimplantomucosal unit this inflam-mation is termed “mucositis” which
may develop into “peri-implantitis.”9
Peri-implantitis is an inflamma-tory reaction that is associatedwith the presence of a submarginalbiofilm, with advanced breakdownof soft and hard tissue surroundingthe endosseous implant: loss of thebony support of the implant.10
The etiology of the disease isconditioned by the status of thetissue surrounding the implant,design of the implant, degree ofroughness, poor alignment of implantcomponents, external morphology,and excessive mechanical load.10
There are two major factors that,separately or combined, contribute tothe formation of peri-implantitis:1. Bacterial exposure, especially
gram-negative and anaerobicspecies11-12
2. Overload.13-14
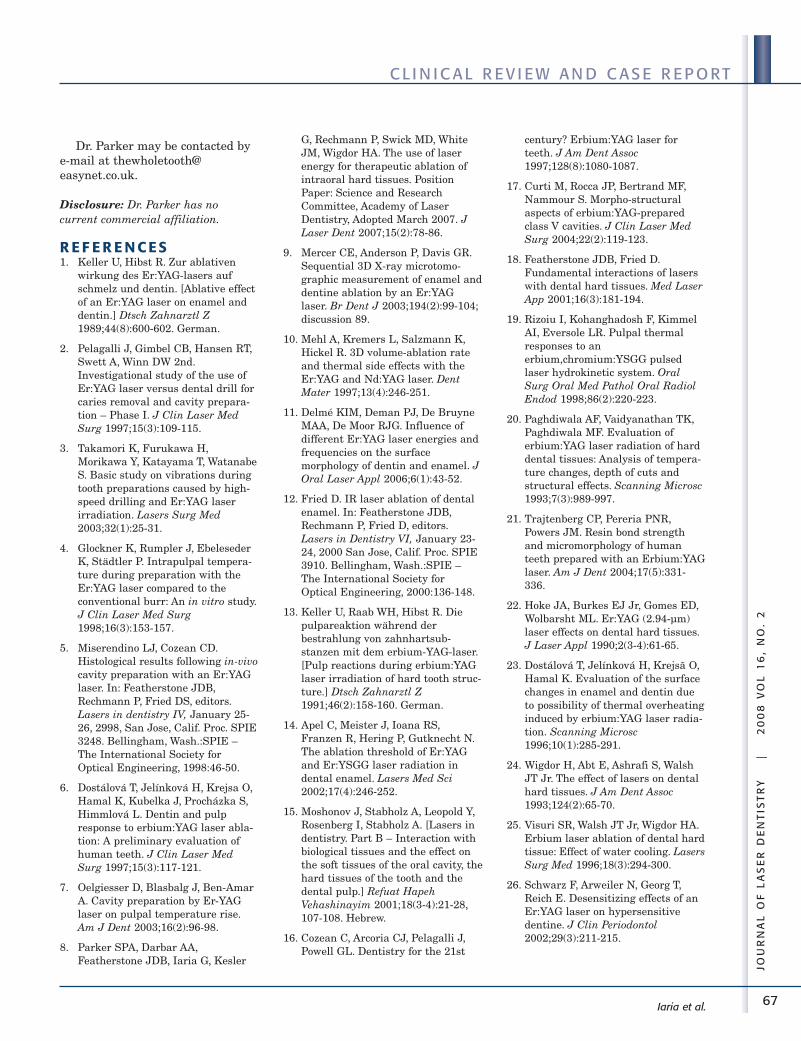
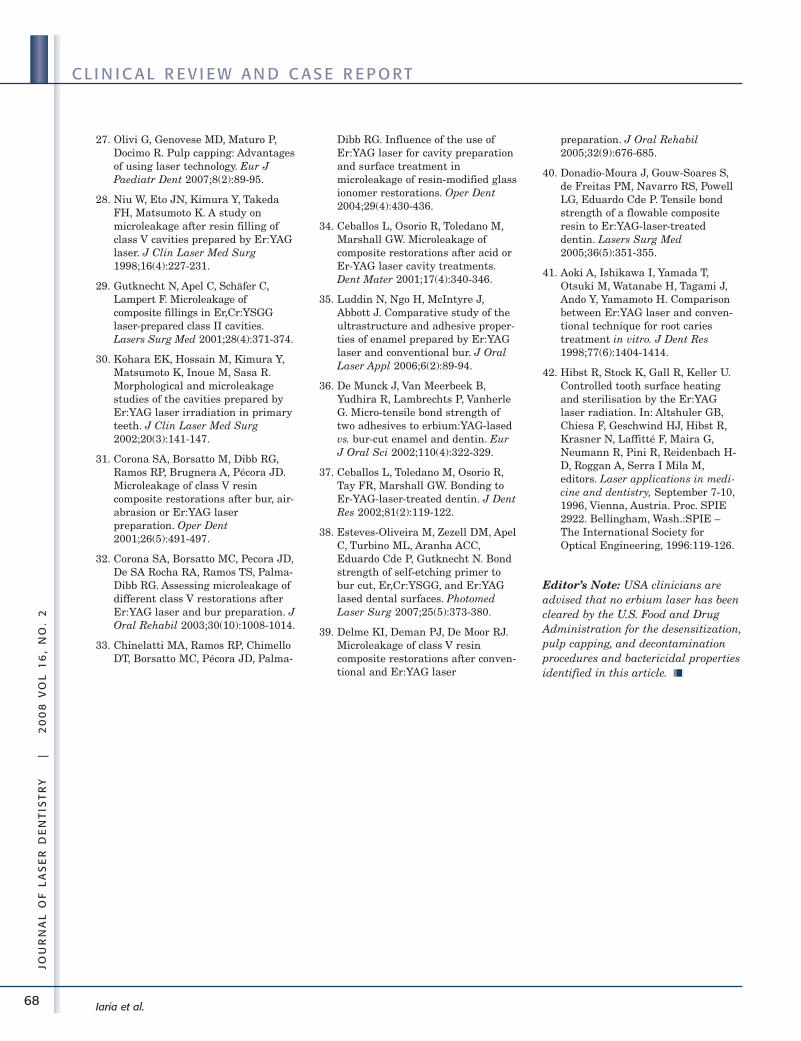
Clinical signs and diagnosisinclude: Bleeding on probing, puru-lence, bone loss, pocketing, dullsound on percussion, peri-implantradiolucent mobility of the implant,fistula, and changes of color in thegingiva and/or the mucosa.10
Treatment involves eitherimplant removal, especially if thefixture is mobile, or therapy,usually involving surgery anddebridement techniques.
Conventional approaches include:• Systemic administration of
antibiotics
• Removal of supragingival bacte-rial plaque
• Removal of granulation tissuewith plastic curettes
• Debridement of the exposedsurface by using mechanicalbrushing, air powder abrasives,citric acid, disinfectants likechlorhexidine or topical tetracy-cline, plaque inhibitor likedelmopinol, or low-intensityultraviolet radiation
• Removal of the peri-implant pocket• Regeneration of peri-implant
hard tissue by means of guidedtissue regeneration
• Plaque control and oral hygiene.
The Use of the Er:YAG Laser inTreatment of Peri-ImplantitisThe Er:YAG laser interacts withboth hard and soft dental tissues,
Reyhanian et al.
A B ST R AC TPeri-implantitis is one of thecomplications possible in osseo -integrated dental implants.
This article discusses the wisdomand utility of employing an Er:YAGlaser for peri-implantitis therapy. Aclinical case study will demonstratehow this procedure could replacethe gold standard for peri-implantitistherapy. This technique using theEr:YAG laser presents several advan-tages vs. conventional treatmentmethods, and there are minimalpostoperative complications coupledwith a high rate of success.
Key Words: antimicrobial agents;bone grafting; bone tissue;debridement; dental implants;granulation tissue; guided tissueregeneration; laser ablation
SY N O P S I S
The etiology of peri-implantitis and a treatment protocol using an
Er:YAG laser are described along with a clinical case study with a
successful outcome.
70
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
COV E R F E AT U R E
and thus can be effectively utilizedfor both surgery and debridementof the infected implant area.• The laser can make crestal,
intrasulcular, or vertical releaseincisions in raising a flap. TheEr:YAG laser produces a wetincision (some bleeding) asopposed to the dry incision (nobleeding) produced by other softtissue lasers.15
• The laser easily vaporizes anyexisting granulation tissue, witha lower risk of overheating thebone than those posed by thecurrent diode or CO2 lasers.16-17
The Er:YAG laser wavelength’sexcellent ability to effectivelyablate soft tissue withoutproducing major thermal side-effects to adjacent tissue hasbeen demonstrated in numerousstudies.18-20
• The implant surface can bedebrided by lasing directly on theimplant’s exposed screws with alow-energy setting. Both thetarget tissue and implant surfaceare disinfected without damage.21-25
• Ablating the bone with theEr:YAG laser also ablatesnecrotic bone, as well as contoursand reshapes the surroundingosseous tissue.26-28
• The laser is bactericidal.29-30
C AS E ST U DYThis case describes treatment ofperi-implantitis with an Er:YAGlaser.
P R ET R E AT M E N TA. Outline of Case1. Clinical ExaminationA 51-year old male presented withno medical abnormalities. Thepatient presented by referral fourmonths after having implantsinserted in the location of the lowerleft and right lateral incisors.
2. Soft- and Hard-TissueExaminationPeriodontal probing showed gener-alized 4 mm pockets with bleeding.The patient had very ineffective
oral hygiene, and does not brush orfloss at all; consequently, all teethwere covered with plaque. Both ofthe implants were nonsubmergedwith abutments present. The lowerright implant presented a labialfistula, the probing of which led tothe apical end of the implant(Figures 1 and 2). The left implantpresented without complications.The remaining soft tissue waswithin normal limits.
3. Radiographic ExaminationPanoramic and periapical X-raysshowed a large radiolucency areasurrounding about 70% of the rightimplant, implying massive boneloss (Figure 3).
4. Mobility TestsThe infected implant was stablewith no mobility.
B. Diagnosis and Treatment Plan1. Provisional and Final DiagnosisAdvanced peri-implantitis withmassive bone loss around theimplant.
2. Treatment PlanAn Er:YAG laser will be used forflap incision, ablation of granula-tion tissue around the implant,remodeling, shaping and decortica-tion of the bone, debridement ofexposed implant screw and guidedbone regeneration (GBR) techniquefor the bone loss.
3. Treatments AlternativesTraditional scalpel, curettes, citricacid, air flow, air abrasion, androtary tools.
T R E AT M E N TA. Laser Operating Parameters An intrasulcular incision was madewith an Er:YAG laser (OpusDuo™AquaLite™, Lumenis Ltd.,Yokneam, Israel) (2940 nm), using
Reyhanian et al.
Figure 1: Patient condition upon presen-tation. Note the buccal fistula from theimplant at tooth #25
Figure 2: A periodontal probe insertedinto the fistula
Figure 3: X-ray image with gutta-perchainside the fistula, pointing into the defect
Figure 4: The Er:YAG handpiece with the200-micron sapphire tip ready for theincision
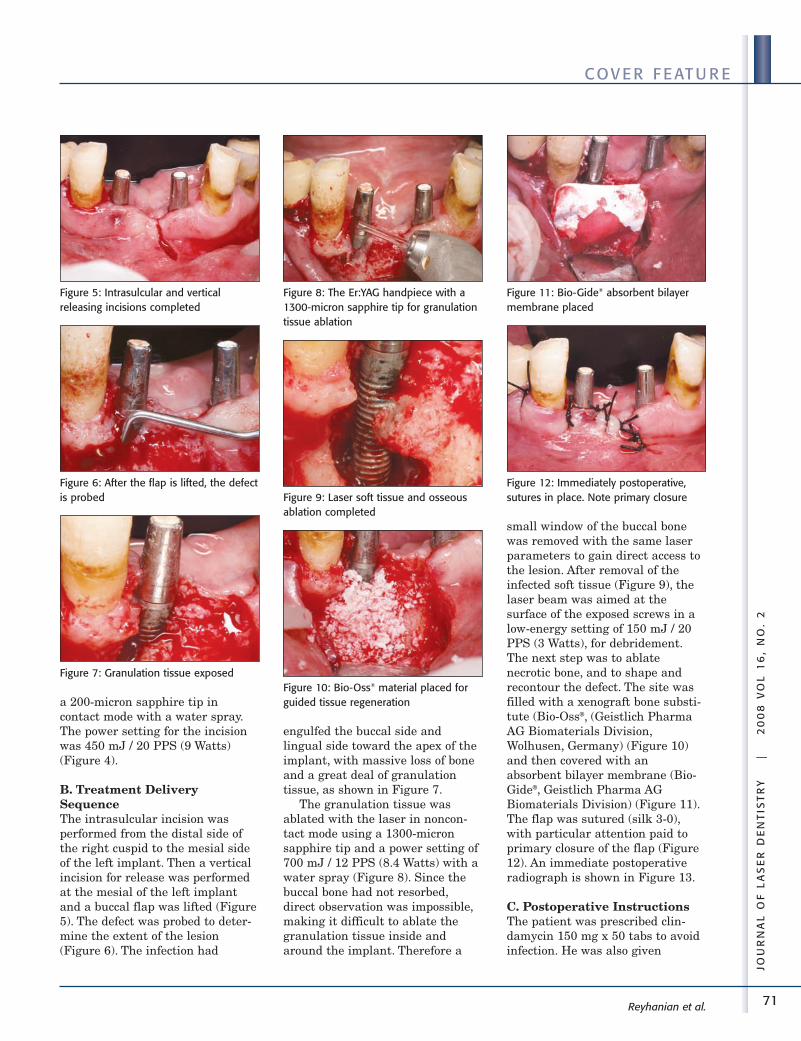
71
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
COV E R F E AT U R E
a 200-micron sapphire tip incontact mode with a water spray.The power setting for the incisionwas 450 mJ / 20 PPS (9 Watts)(Figure 4).
B. Treatment DeliverySequenceThe intrasulcular incision wasperformed from the distal side ofthe right cuspid to the mesial sideof the left implant. Then a verticalincision for release was performedat the mesial of the left implantand a buccal flap was lifted (Figure5). The defect was probed to deter-mine the extent of the lesion(Figure 6). The infection had
engulfed the buccal side andlingual side toward the apex of theimplant, with massive loss of boneand a great deal of granulationtissue, as shown in Figure 7.
The granulation tissue wasablated with the laser in noncon-tact mode using a 1300-micronsapphire tip and a power setting of700 mJ / 12 PPS (8.4 Watts) with awater spray (Figure 8). Since thebuccal bone had not resorbed,direct observation was impossible,making it difficult to ablate thegranulation tissue inside andaround the implant. Therefore a
small window of the buccal bonewas removed with the same laserparameters to gain direct access tothe lesion. After removal of theinfected soft tissue (Figure 9), thelaser beam was aimed at thesurface of the exposed screws in alow-energy setting of 150 mJ / 20PPS (3 Watts), for debridement.The next step was to ablatenecrotic bone, and to shape andrecontour the defect. The site wasfilled with a xenograft bone substi-tute (Bio-Oss®, (Geistlich PharmaAG Biomaterials Division,Wolhusen, Germany) (Figure 10)and then covered with anabsorbent bilayer membrane (Bio-Gide®, Geistlich Pharma AGBiomaterials Division) (Figure 11).The flap was sutured (silk 3-0),with particular attention paid toprimary closure of the flap (Figure12). An immediate postoperativeradiograph is shown in Figure 13.
C. Postoperative InstructionsThe patient was prescribed clin-damycin 150 mg x 50 tabs to avoidinfection. He was also given
Reyhanian et al.
Figure 5: Intrasulcular and verticalreleasing incisions completed
Figure 6: After the flap is lifted, the defectis probed
Figure 7: Granulation tissue exposed
Figure 8: The Er:YAG handpiece with a1300-micron sapphire tip for granulationtissue ablation
Figure 9: Laser soft tissue and osseousablation completed
Figure 10: Bio-Oss® material placed forguided tissue regeneration
Figure 11: Bio-Gide® absorbent bilayermembrane placed
Figure 12: Immediately postoperative,sutures in place. Note primary closure
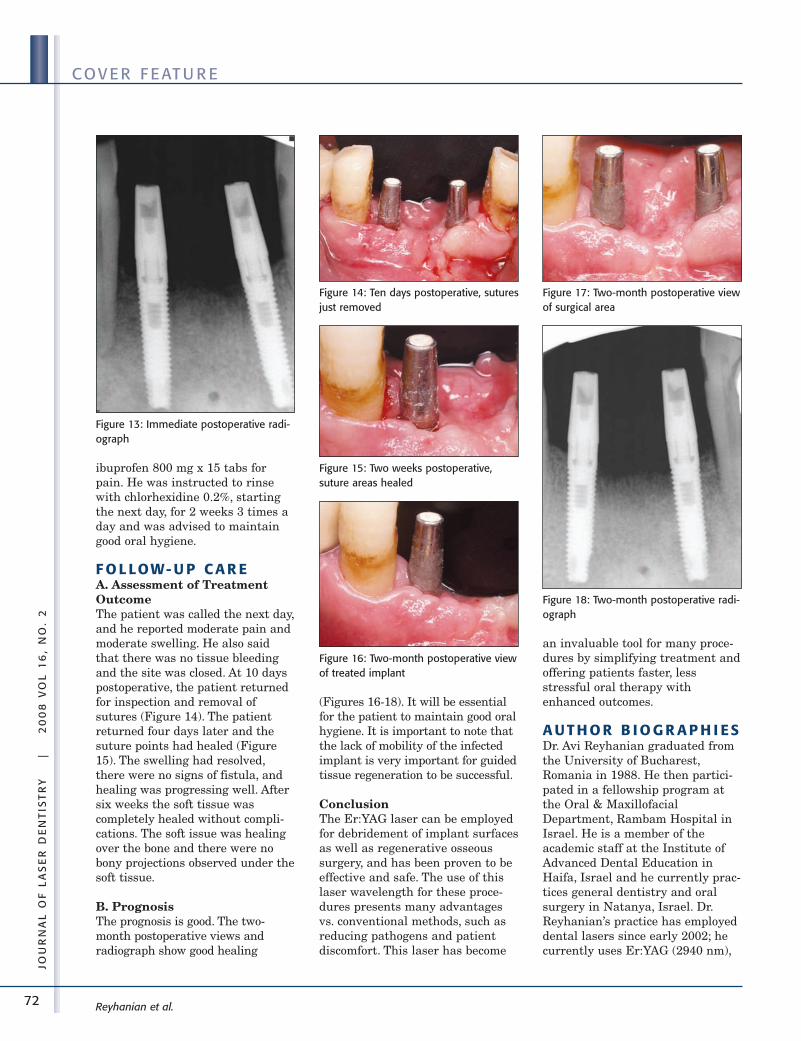
72
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
COV E R F E AT U R E
ibuprofen 800 mg x 15 tabs forpain. He was instructed to rinsewith chlorhexidine 0.2%, startingthe next day, for 2 weeks 3 times aday and was advised to maintaingood oral hygiene.
F O L LOW- U P C A R EA. Assessment of TreatmentOutcomeThe patient was called the next day,and he reported moderate pain andmoderate swelling. He also saidthat there was no tissue bleedingand the site was closed. At 10 dayspostoperative, the patient returnedfor inspection and removal ofsutures (Figure 14). The patientreturned four days later and thesuture points had healed (Figure15). The swelling had resolved,there were no signs of fistula, andhealing was progressing well. Aftersix weeks the soft tissue wascompletely healed without compli-cations. The soft issue was healingover the bone and there were nobony projections observed under thesoft tissue.
B. PrognosisThe prognosis is good. The two-month postoperative views andradiograph show good healing
(Figures 16-18). It will be essentialfor the patient to maintain good oralhygiene. It is important to note thatthe lack of mobility of the infectedimplant is very important for guidedtissue regeneration to be successful.
ConclusionThe Er:YAG laser can be employedfor debridement of implant surfacesas well as regenerative osseoussurgery, and has been proven to beeffective and safe. The use of thislaser wavelength for these proce-dures presents many advantagesvs. conventional methods, such asreducing pathogens and patientdiscomfort. This laser has become
an invaluable tool for many proce-dures by simplifying treatment andoffering patients faster, lessstressful oral therapy withenhanced outcomes.
A U T H O R B I O G R A P H I ESDr. Avi Reyhanian graduated fromthe University of Bucharest,Romania in 1988. He then partici-pated in a fellowship program atthe Oral & MaxillofacialDepartment, Rambam Hospital inIsrael. He is a member of theacademic staff at the Institute ofAdvanced Dental Education inHaifa, Israel and he currently prac-tices general dentistry and oralsurgery in Natanya, Israel. Dr.Reyhanian’s practice has employeddental lasers since early 2002; hecurrently uses Er:YAG (2940 nm),
Reyhanian et al.
Figure 13: Immediate postoperative radi-ograph
Figure 14: Ten days postoperative, suturesjust removed
Figure 15: Two weeks postoperative,suture areas healed
Figure 16: Two-month postoperative viewof treated implant
Figure 17: Two-month postoperative viewof surgical area
Figure 18: Two-month postoperative radi-ograph

73
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
COV E R F E AT U R E
CO2 (10,600 nm), and diode (830nm) lasers in his practice. He is amember of the Academy of LaserDentistry and the Israel Society ofDental Implantology. Dr.Reyhanian presents lectures inIsrael, Europe, USA, and Asia onthe topic of dental lasers, and haspublished several articles. Dr.Reyhanian may be contacted by e-mail at [email protected].
Disclosure: Dr. Reyhanian is amember of the academic staff at theInstitute of Advanced DentalEducation in Haifa, Israel, and is aconsultant to the Lumenis Company.
Dr. Donald Coluzzi, a 1970 grad-uate of the University of SouthernCalifornia School of Dentistry, is anassociate clinical professor in theDepartment of Preventive andRestorative Dental Sciences at theUniversity of California SanFrancisco School of Dentistry. Acharter member and past Presidentof the Academy of Laser Dentistry,he has used dental lasers sinceearly 1991. He has AdvancedProficiency in Nd:YAG and Er:YAGlaser wavelengths. He is the 1999recipient of the Leon GoldmanAward for Clinical Excellence andthe 2006 Distinguished ServiceAward from the Academy of LaserDentistry, and is a Fellow of theAmerican College of Dentists. Dr.Coluzzi has presented about lasersworldwide, co-authored two books,and published several peer-reviewed articles.
Disclosure: Dr. Coluzzi is an occa-sional presenter and trainer for HoyaConBio, and receives an honorariumfor that service.
R E F E R E N C ES1. Adell R, Lekholm U, Rockler B,
Brånemark P-I. A 15-year study ofosseointegrated implants in thetreatment of the edentulous jaw. IntJ Oral Surg 1981;10(6):387-416.
2. Albrektsson T. A multicenter reporton osseointegrated oral implants. JProsthet Dent 1988;60(1):75-84.
3. Buser D, Mericske-Stern R, Dula K,Lang NP. Clinical experience withone-stage, non-submerged dentalimplants. Adv Dent Res1999;13:153-161.
4. Olsson M, Friberg B, Nilson H,Kultje C. MkII – A modified self-tapping Brånemark implant: 3-yearresults of a controlled prospectivepilot study. Int J Oral MaxillofacImplants 1995;10(1):15-21; Erratumin: Int J Oral Maxillofac Implants1995;10(2):243.
5. Jaffin RA, Berman CL. The exces-sive loss of Branemark fixtures intype IV bone: A 5-year analysis. JPeriodontol 1991;62(1):2-4.
6. Esposito M, Hirsch J, Lekholm U,Thomsen P. Differential diagnosisand treatment strategies for biologiccomplications and failing oralimplants: A review of the literature.Int J Oral Maxillofac Implants1999;14(4):473-490
7. Brisman DL, Brisman AS, MosesMS. Implant failures associatedwith asymptomatic endodonticallytreated teeth. J Am Dent Assoc2001;132(2):191-195.
8. Ayangco L, Sheridan PJ.Development and treatment ofretrograde peri-implantitisinvolving a site with a history offailed endodontic and apicoectomyprocedures: A series of reports. Int JOral Maxillofac Implants2001;16(3):412-417.
9. Reyhanian A, Coluzzi DJ. Er:YAGlaser-assisted implant periapicallesion therapy (IPL) and guidedbone regeneration (GBR) technique:New challenges and new instrumen-tation. J Laser Dent2007;15(3):135-141.
10. Sánchez-Gárces MA, Gay-Escoda C.Periimplantitis. Med Oral Patol OralCir Bucal 2004;9 Suppl:69-74; 63-69.
11. Albrektsson TO, Johansson CB,Sennerby L. Biological aspects ofimplant dentistry: Osseointegration.Periodontol 2000 1994;4:58-73.
12. Meffert RM. Periodontitis and peri-implantitis: One and the same?Pract Periodontics Aesthet Dent1993;5(9):79-80, 82.
13. Uribe R, Peñarrocha M, Sanchis JM,García O. Marginal peri-implantitis
due to occlusal overload. A casereport. Med Oral 2004;9(2):160-162,159-160.
14. Isidor F. Loss of osseointegrationcaused by occlusal load of oralimplants. A clinical and radi-ographic study in monkeys. ClinOral Implants Res 1996;7(2):143-152.
15. Watanabe H, Ishikawa I, Suzuki M,Hasegawa K. Clinical assessmentsof the erbium:YAG laser for softtissue surgery and scaling. J ClinLaser Med Surg 1996;14(2):67-75.
16. Kreisler M, Al Haj H, d’Hoedt B.Temperature changes at theimplant-bone interface during simu-lated surface decontamination withan Er:YAG laser. Int J Prosthodont2002;15(6):582-587.
17. Sasaki KM, Aoki A, Ichinose S,Yoshino T, Yamada S, Ishikawa I.Scanning electron microscopy andFourier transformed infrared spec-troscopy analysis of bone removalusing Er:YAG and CO2 lasers. JPeriodontol 2002;73(6):643-652.
18. Ishikawa I, Aoki A, Takasaki AA.Potential applications oferbium:YAG laser in periodontics. JPeriodontal Res 2004;39(4):275-285.
19. Ishikawa I, Sasaki KM, Aoki A,Watanabe H. Effects of Er:YAGlaser on periodontal therapy. J IntAcad Periodontol 2003;5(1):23-28.
20. Schwarz F, Bieling K, Sculean A,Herten M, Becker J. Laser undultraschall in der therapie periim-plantärer infektionen – Eineliteraturübersicht. [Treatment ofperiimplantitis with laser or ultra-sound. A review of the literature.]Schweiz Monatsschr Zahnmed2004;114(12):1228-1235. German.
21. Schwarz F, Rothamel D, Becker J.Einfluss eines Er:YAG-lasers auf dieoberflächen-struktur von Titan-implantaten. [Influence of anEr:YAG laser on the surface struc-ture of titanium implants.] SchweizMonatsschr Zahnmed2003;113(6):660-671. French,German.
22. Jovanovic SA. The management ofperi-implant breakdown aroundfunctioning osseointegrated dentalimplants. J Periodontol 1993;64(11Suppl):1176-1183.
Reyhanian et al.
74
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
COV E R F E AT U R E
23. Matsuyama T, Aoki A, Oda S,Yoneyama T, Ishikawa I. Effect ofthe Er:YAG laser irradiation on tita-nium implant materials andcontaminated implant abutmentsurfaces. J Clin Laser Med Surg2003;21(1):7-17.
24. Schwarz F, Rothamel D, Sculean A,Georg T, Scherbaum W, Becker J.Effects of an Er:YAG laser and theVector ultrasonic system on thebiocompatibility of titaniumimplants in cultures of humanosteoblast-like cells. Clin OralImplants Res 2003;14(6):784-792.
25. Kreisler M, Kohnen W, ChristoffersAB, Götz H, Jansen B, Duschner H,d’Hoedt B. In vitro evaluation of thebiocompatibility of contaminated
implant surfaces treated with anEr:YAG laser and an air powdersystem. Clin Oral Implants Res2005;16(1):36-43.
26. Nelson JS, Orenstein A, Liaw LH,Berns MW. Mid-infrarederbium:YAG laser ablation of bone:The effect of laser osteotomy onbone healing. Lasers Surg Med1989;9(4):362-374.
27. “Use Of the Dental Erbium Laser(2940nm) For Contouring AndResection Of Osseous Tissue (Bone)And The Preparation Of EndodonticCanals,” Copyright 2000 to 2002Institute for Laser Dentistry,www.laserdentistry.ca/erbium.html,accessed May 24, 2008.
28. Rupprecht S, Tangermann K,Kessler P, Neukam FW, Wiltfang J.Er:YAG laser osteotomy directed bysensor controlled systems. JCraniomaxillofac Surg2003;31(6):337-342.
29. Folwaczny M, Mehl A, Aggstaller H,Hickel R. Antimicrobial effects of2.94 µm Er:YAG laser radiation onroot surfaces: An in vitro study. JClin Periodontol 2002;29(1):73-78.
30. Kreisler M, Kohnen W, Marinello C,Götz H, Duschner H, Jansen B,d’Hoedt B. Bactericidal effect of theEr:YAG laser on dental implantsurfaces: An in vitro study. JPeriodontol 2002;73(11):1292-1298. ■■
Reyhanian et al.
75
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
Use of an Er:YAG Laser for Pulpotomies in Vital and Nonvital Primary TeethLawrence Kotlow, DDS, Albany, New YorkJ Laser Dent 2008;16(2):75-79
I N T R O D U C T I O NPrimary teeth that have the pulptissue exposed due to caries,mechanical removal of carioustissue, or as a preventive procedureon severely abraded teeth requirethe completion of a pulpotomy. TheAmerican Academy of PediatricDentistry defines a pulpotomy1 aswhen the coronal pulp is ampu-tated, and the remaining vitalradicular pulp tissue surface istreated with a medicament such asformocresol2-3 or ferric sulfate4 orwith electrocautery5 to preserve theradicular pulp’s health. Mineraltrioxide aggregate (MTA)6 has alsobeen used as pulp dressing agent forpulp therapy treatment. A pulpec-tomy1 is defined as a root canalprocedure for pulp tissue that isirreversibly infected or necrotic dueto caries or trauma. The objective ofeither procedure is to maintain thetooth or teeth involved – function-ally and painlessly – withoutpathology until the primary toothnormally exfoliates upon eruption ofthe underlying permanent tooth oruntil the tooth is adequately devel-oped for the root canal completion.
Lasers are an effective alterna-tive for treating pulps with theadditional the benefits ofproviding pulp therapy withoutthe need to introduce chemicalsinto children’s systems. It hasbeen demonstrated that small
amounts of formocresol may beabsorbed and distributedthroughout the child’s body withinminutes of its use at the pulpo-tomy site.7
Pulpotomy is one of the clinicalindications for use of the Er:YAGlaser (2940 nm), which is useful intreating both vital and nonvitalprimary teeth where a pulpotomyis required to maintain the primarytooth until it is ready to exfoliate.8-10
In addition, successful treatmentcan delay the need to extract anonvital primary tooth until aspace maintainer can be inserted.
C L I N I C A L C AS ES U M M A R I ESThis report presents a series ofclinical cases of treating primaryteeth, using the Er:YAG laser forpulpotomies in primary teeth.
P R ET R E AT M E N TThe teeth included in this reportwere performed on children whohad medical histories completed bytheir parents which the indicatedthe children were healthy.Pulpotomies in the report areselected examples of more than4,000 pulp treatments necessitatedby traumatic injuries, mechanical orcaries exposure, or in teeth deter-mined to be nonvital due to cariesor trauma. Cases represent exam-ples of teeth treated with an
Er:YAG laser in 2002 or later, withfollow-up radiographs extendingfrom 2 months to 5 years post-treat-ment. In anterior pulp therapycases, the pulp therapy treatmentwas completed on children as youngas 8 months of age. These casesrepresented children suffering fromnursing bottle dental caries or whohad traumatized the upper anteriorteeth which resulted in the teethbecoming nonvital. In the posteriorteeth, children had treatment asearly as 16 months on first primarymolar teeth and as early as 24months for second primary molarteeth which had erupted prior to thenormal eruption time of 36 months.
Radiographic DocumentationExamples in this report werechosen from those cases where thechild was able to accept the takingof dental radiographs prior tobeginning the treatment.
Kotlow
A B ST R AC TPulp therapy for vital and nonvitalprimary teeth usually involves theuse of chemical agents, such asformocresol, or electrocautery.This article reviews the results ofusing the Er:YAG laser to achievesimilar results. Clinical and radi-ographic evidence indicates thatusing the Er:YAG laser results insafe, successful treatment ofpulpotomies in primary teeth,similar to the successful treatmentof other modalities.
Key Words: amoxicillin; dentalpulp exposure; electrocautery;formocresol; radiography, dental;root canal irrigants; zinc oxide-eugenol cement
SY N O P S I S
A protocol for performing a primary tooth pulpotomy utilizing an
Er:YAG laser is described. Radiographic histories of several clinical
cases are also shown.
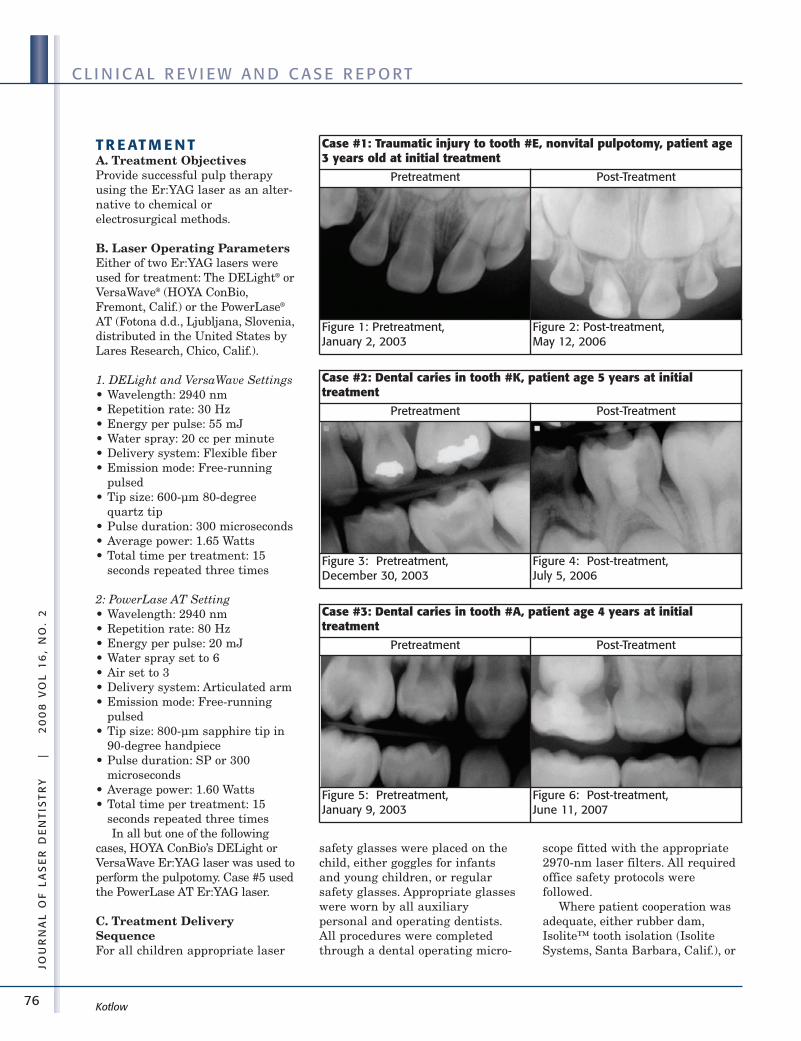
76
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
T R E AT M E N TA. Treatment ObjectivesProvide successful pulp therapyusing the Er:YAG laser as an alter-native to chemical orelectrosurgical methods.
B. Laser Operating ParametersEither of two Er:YAG lasers wereused for treatment: The DELight® orVersaWave® (HOYA ConBio,Fremont, Calif.) or the PowerLase®
AT (Fotona d.d., Ljubljana, Slovenia,distributed in the United States byLares Research, Chico, Calif.).
1. DELight and VersaWave Settings• Wavelength: 2940 nm• Repetition rate: 30 Hz• Energy per pulse: 55 mJ• Water spray: 20 cc per minute• Delivery system: Flexible fiber• Emission mode: Free-running
pulsed• Tip size: 600-µm 80-degree
quartz tip• Pulse duration: 300 microseconds• Average power: 1.65 Watts• Total time per treatment: 15
seconds repeated three times
2: PowerLase AT Setting• Wavelength: 2940 nm• Repetition rate: 80 Hz• Energy per pulse: 20 mJ• Water spray set to 6• Air set to 3• Delivery system: Articulated arm• Emission mode: Free-running
pulsed• Tip size: 800-µm sapphire tip in
90-degree handpiece• Pulse duration: SP or 300
microseconds• Average power: 1.60 Watts• Total time per treatment: 15
seconds repeated three timesIn all but one of the following
cases, HOYA ConBio’s DELight orVersaWave Er:YAG laser was used toperform the pulpotomy. Case #5 usedthe PowerLase AT Er:YAG laser.
C. Treatment DeliverySequenceFor all children appropriate laser
safety glasses were placed on thechild, either goggles for infantsand young children, or regularsafety glasses. Appropriate glasseswere worn by all auxiliarypersonal and operating dentists.All procedures were completedthrough a dental operating micro-
scope fitted with the appropriate2970-nm laser filters. All requiredoffice safety protocols werefollowed.
Where patient cooperation wasadequate, either rubber dam,Isolite™ tooth isolation (IsoliteSystems, Santa Barbara, Calif.), or
Kotlow
Case #1: Traumatic injury to tooth #E, nonvital pulpotomy, patient age3 years old at initial treatment
Pretreatment Post-Treatment
Figure 1: Pretreatment, January 2, 2003
Figure 2: Post-treatment, May 12, 2006
Case #2: Dental caries in tooth #K, patient age 5 years at initial treatment
Pretreatment Post-Treatment
Figure 3: Pretreatment, December 30, 2003
Figure 4: Post-treatment, July 5, 2006
Case #3: Dental caries in tooth #A, patient age 4 years at initial treatment
Pretreatment Post-Treatment
Figure 5: Pretreatment, January 9, 2003
Figure 6: Post-treatment, June 11, 2007
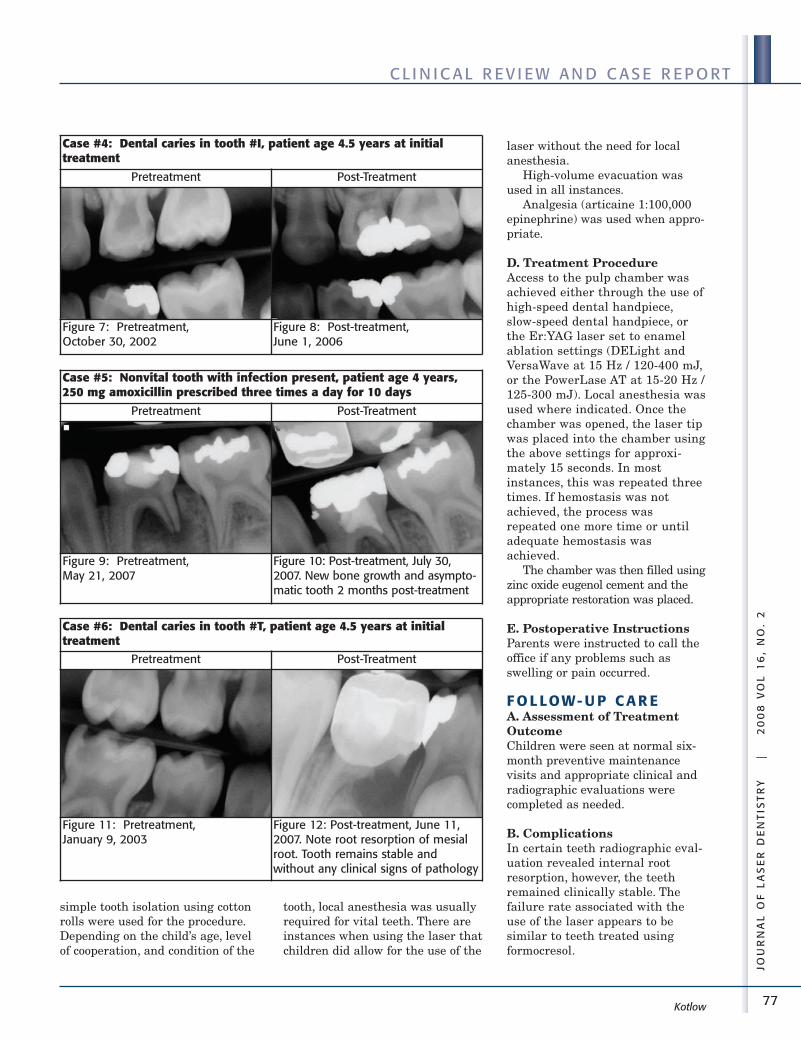
77
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
simple tooth isolation using cottonrolls were used for the procedure.Depending on the child’s age, levelof cooperation, and condition of the
tooth, local anesthesia was usuallyrequired for vital teeth. There areinstances when using the laser thatchildren did allow for the use of the
laser without the need for localanesthesia.
High-volume evacuation wasused in all instances.
Analgesia (articaine 1:100,000epinephrine) was used when appro-priate.
D. Treatment ProcedureAccess to the pulp chamber wasachieved either through the use ofhigh-speed dental handpiece,slow-speed dental handpiece, orthe Er:YAG laser set to enamelablation settings (DELight andVersaWave at 15 Hz / 120-400 mJ,or the PowerLase AT at 15-20 Hz /125-300 mJ). Local anesthesia wasused where indicated. Once thechamber was opened, the laser tipwas placed into the chamber usingthe above settings for approxi-mately 15 seconds. In mostinstances, this was repeated threetimes. If hemostasis was notachieved, the process wasrepeated one more time or untiladequate hemostasis wasachieved.
The chamber was then filled usingzinc oxide eugenol cement and theappropriate restoration was placed.
E. Postoperative InstructionsParents were instructed to call theoffice if any problems such asswelling or pain occurred.
F O L LOW- U P C A R EA. Assessment of TreatmentOutcomeChildren were seen at normal six-month preventive maintenancevisits and appropriate clinical andradiographic evaluations werecompleted as needed.
B. ComplicationsIn certain teeth radiographic eval-uation revealed internal rootresorption, however, the teethremained clinically stable. Thefailure rate associated with theuse of the laser appears to besimilar to teeth treated usingformocresol.
Kotlow
Case #4: Dental caries in tooth #I, patient age 4.5 years at initial treatment
Pretreatment Post-Treatment
Figure 7: Pretreatment, October 30, 2002
Figure 8: Post-treatment, June 1, 2006
Case #5: Nonvital tooth with infection present, patient age 4 years,250 mg amoxicillin prescribed three times a day for 10 days
Pretreatment Post-Treatment
Figure 9: Pretreatment, May 21, 2007
Figure 10: Post-treatment, July 30,2007. New bone growth and asympto-matic tooth 2 months post-treatment
Case #6: Dental caries in tooth #T, patient age 4.5 years at initialtreatment
Pretreatment Post-Treatment
Figure 11: Pretreatment, January 9, 2003
Figure 12: Post-treatment, June 11,2007. Note root resorption of mesialroot. Tooth remains stable andwithout any clinical signs of pathology
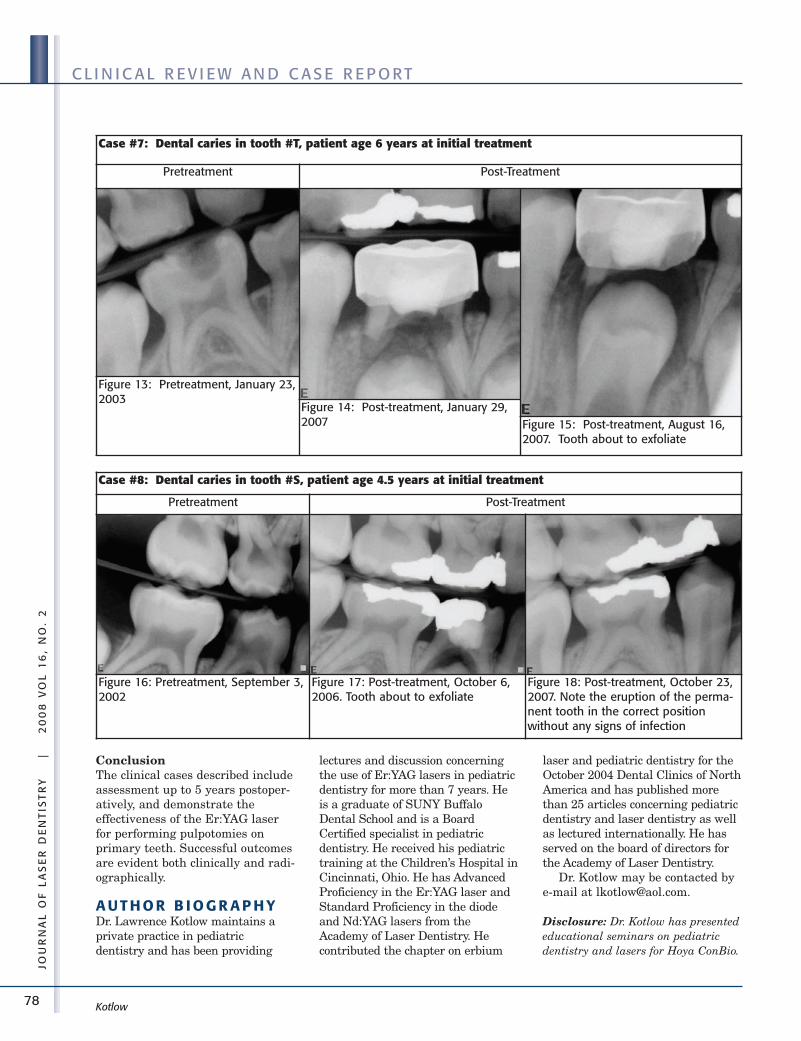
78
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
ConclusionThe clinical cases described includeassessment up to 5 years postoper-atively, and demonstrate theeffectiveness of the Er:YAG laserfor performing pulpotomies onprimary teeth. Successful outcomesare evident both clinically and radi-ographically.
A U T H O R B I O G R A P H YDr. Lawrence Kotlow maintains aprivate practice in pediatricdentistry and has been providing
lectures and discussion concerningthe use of Er:YAG lasers in pediatricdentistry for more than 7 years. Heis a graduate of SUNY BuffaloDental School and is a BoardCertified specialist in pediatricdentistry. He received his pediatrictraining at the Children’s Hospital inCincinnati, Ohio. He has AdvancedProficiency in the Er:YAG laser andStandard Proficiency in the diodeand Nd:YAG lasers from theAcademy of Laser Dentistry. Hecontributed the chapter on erbium
laser and pediatric dentistry for theOctober 2004 Dental Clinics of NorthAmerica and has published morethan 25 articles concerning pediatricdentistry and laser dentistry as wellas lectured internationally. He hasserved on the board of directors forthe Academy of Laser Dentistry.
Dr. Kotlow may be contacted bye-mail at [email protected].
Disclosure: Dr. Kotlow has presentededucational seminars on pediatricdentistry and lasers for Hoya ConBio.
Kotlow
Case #7: Dental caries in tooth #T, patient age 6 years at initial treatment
Pretreatment Post-Treatment
Figure 13: Pretreatment, January 23,2003
Figure 14: Post-treatment, January 29,2007 Figure 15: Post-treatment, August 16,
2007. Tooth about to exfoliate
Case #8: Dental caries in tooth #S, patient age 4.5 years at initial treatment
Pretreatment Post-Treatment
Figure 16: Pretreatment, September 3,2002
Figure 17: Post-treatment, October 6,2006. Tooth about to exfoliate
Figure 18: Post-treatment, October 23,2007. Note the eruption of the perma-nent tooth in the correct positionwithout any signs of infection

79
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L R E V I E W A N D C A S E R E P O RT
He consults and provides professionalguidance in development of productsfor many laser- and technology-associ-ated manufacturers such as Isolite,Schick, and Lares Research andvarious laser safety glass manufac-turers. For his professional speakingengagements or product input hereceives an honorarium or new prod-ucts to evaluate.
R E F E R E N C ES1. American Academy of Pediatric
Dentistry Clinical AffairsCommittee – Pulp TherapySubcommittee; American Academyof Pediatric Dentistry Council onClinical Affairs. Pediatric DentistryReference Manual: Guideline onpulp therapy for primary and youngpermanent teeth. Pediatr Dent 2006-2007;28(7):144-148.
2. Camp JH, Barrett EJ, Pulver F.Pediatric endodontics: Endodontic
treatment for the primary andyoung, permanent dentition.Chapter 23 in: Cohen S. Burns RC,editors. Pathways of the Pulp. 8thed. St. Louis, Mo.: Mosby, Inc.,2002:797-844.
3. Farooq NS, Coll JA, Kuwabara A.Shelton P. Success rates offormocresol pulpotomy and indirectpulp therapy in the treatment of deepdentinal caries in primary teeth.Pediatr Dent 2000;22(4):278-286.
4. Smith NL, Seale NS, Nunn ME.Ferric sulfate pulpotomy in primarymolars: A retrospective study.Pediatr Dent 2000:22(3):192-199.
5. Dean JA, Mack RB, Fulkerson BT,Sanders BJ. Comparison of electro-surgical and formocresol pulpotomyprocedures in children. Int JPaediatr Dent 2002;12(3):177-182.
6. Eidelman E, Holan G, Fuks AB.Mineral trioxide aggregate vs.formocresol in pulpotomized primary
molars: A preliminary report.Pediatr Dent 2001;23(1):15-18.
7. Pashley EL, Myers DR, Pashley DH,Whitford GM. Systemic distributionof 14C-formaldehyde fromformocresol-treated pulpotomy sites.J Dent Res 1980;59(3):602-608.
8. Kimura Y, Yonaga K, Yokoyama K,Watanabe H, Wang X, Matsumoto K.Histopathological changes in dentalpulp irradiated by Er:YAG laser: Apreliminary report on laser pulpo-tomy. J Clin Laser Med Surg2003;21(6):345-350.
9. Liu J-F, Chen L-R, Chao S-Y. Laserpulpotomy of primary teeth. PediatrDent 1999;21(2):128-129.
10. Church A, Henson T. Recall evalua-tion of primary pulp therapy using adental laser. [Poster.] AmericanAcademy of Pediatric Dentistry 60thAnnual Session, May 23-27, 2007,San Antonio, Texas. ■■
Kotlow
Advanced Proficiency Case Studies
80
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E ST U D I E S
As featured in the previous two issues, the three mostrecent recipients of the ALD Advanced Proficiency areCharles Hoopingarner, DDS; Steven Parker, BDS, LDS,RCS, MFGDP; and Mary Lynn Smith, RDH.
Dr. Hoopingarner treats a patient who desired amore aesthetic smile without restorations. To accom-plish that objective, he performed a maxillary anteriorfrenectomy together with soft and hard tissue crownlengthening utilizing a closed flap technique for theremoval and recontour of the osseous crest tissues.Using an Er:YAG laser, he contours the periodontaltissues to ensure an adequate biologic width.
Dr. Parker utilizes an 810-nm diode laser to removehyperplastic gingival tissues in preparation for a newfixed bridge. The diode wavelength is an excellentchoice for this procedure since it has very little interac-tion with tooth structure while offering precision oftissue removal and excellent hemostasis.
Ms. Smith treats a patient with chronic generalizedperiodontitis, using the Nd:YAG laser after scaling withconventional instrumentation was completed. Thephotographs feature two specific tooth areas duringinitial therapy and follow-up evaluation appointments.This laser wavelength (1064 nm) is indicated for theremoval of the diseased epithelial lining of the peri-odontal pocket, and thus can be a good addition to theprotocol for the initial treatment of the disease. Shealso uses this instrument for the treatment of aphthousulcers, another indication for use.
These three cases show how various treatments canemploy different laser wavelengths with successfulresults.
Soft Tissue Gingivoplasty, Osseous Recontouring/ Crown Lengthening, and Frenectomy Using anEr:YAG LaserCharles R. Hoopingarner, DDSHouston, Texas
Use of an 810-nm Diode Laser in a GingivoplastyProcedure Associated with Restorative DentalCareSteven Parker, BDS, LDS RCS, MFGDPHarrogate, North Yorks, Great Britain
Nd:YAG Laser-Assisted Treatment of ModerateChronic Periodontitis and Nd:YAG LaserTreatment of Two Aphthous Ulcerative LesionsMary Lynn Smith, RDHMcPherson, Kansas ■■
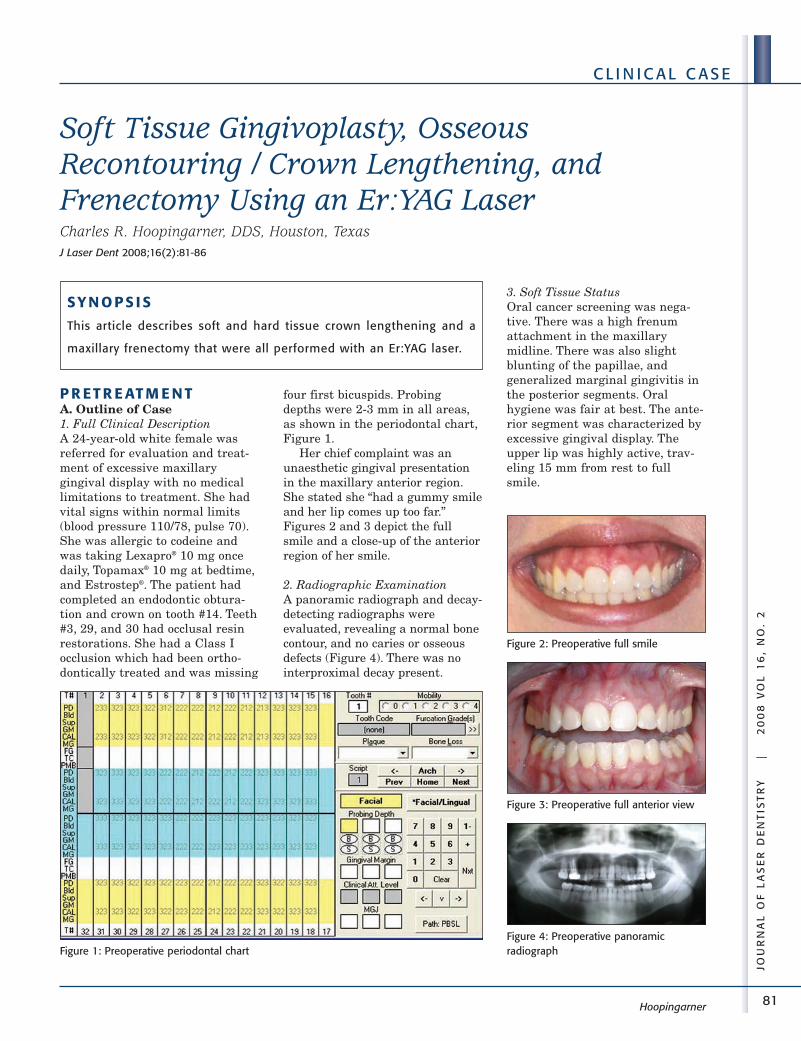
81
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Hoopingarner
Soft Tissue Gingivoplasty, OsseousRecontouring / Crown Lengthening, andFrenectomy Using an Er:YAG LaserCharles R. Hoopingarner, DDS, Houston, TexasJ Laser Dent 2008;16(2):81-86
P R ET R E AT M E N TA. Outline of Case1. Full Clinical DescriptionA 24-year-old white female wasreferred for evaluation and treat-ment of excessive maxillarygingival display with no medicallimitations to treatment. She hadvital signs within normal limits(blood pressure 110/78, pulse 70).She was allergic to codeine andwas taking Lexapro® 10 mg oncedaily, Topamax® 10 mg at bedtime,and Estrostep®. The patient hadcompleted an endodontic obtura-tion and crown on tooth #14. Teeth#3, 29, and 30 had occlusal resinrestorations. She had a Class Iocclusion which had been ortho-dontically treated and was missing
four first bicuspids. Probingdepths were 2-3 mm in all areas,as shown in the periodontal chart,Figure 1.
Her chief complaint was anunaesthetic gingival presentationin the maxillary anterior region.She stated she “had a gummy smileand her lip comes up too far.”Figures 2 and 3 depict the fullsmile and a close-up of the anteriorregion of her smile.
2. Radiographic ExaminationA panoramic radiograph and decay-detecting radiographs wereevaluated, revealing a normal bonecontour, and no caries or osseousdefects (Figure 4). There was nointerproximal decay present.
3. Soft Tissue StatusOral cancer screening was nega-tive. There was a high frenumattachment in the maxillarymidline. There was also slightblunting of the papillae, andgeneralized marginal gingivitis inthe posterior segments. Oralhygiene was fair at best. The ante-rior segment was characterized byexcessive gingival display. Theupper lip was highly active, trav-eling 15 mm from rest to fullsmile.
SY N O P S I S
This article describes soft and hard tissue crown lengthening and a
maxillary frenectomy that were all performed with an Er:YAG laser.
Figure 1: Preoperative periodontal chart
Figure 2: Preoperative full smile
Figure 3: Preoperative full anterior view
Figure 4: Preoperative panoramic radiograph
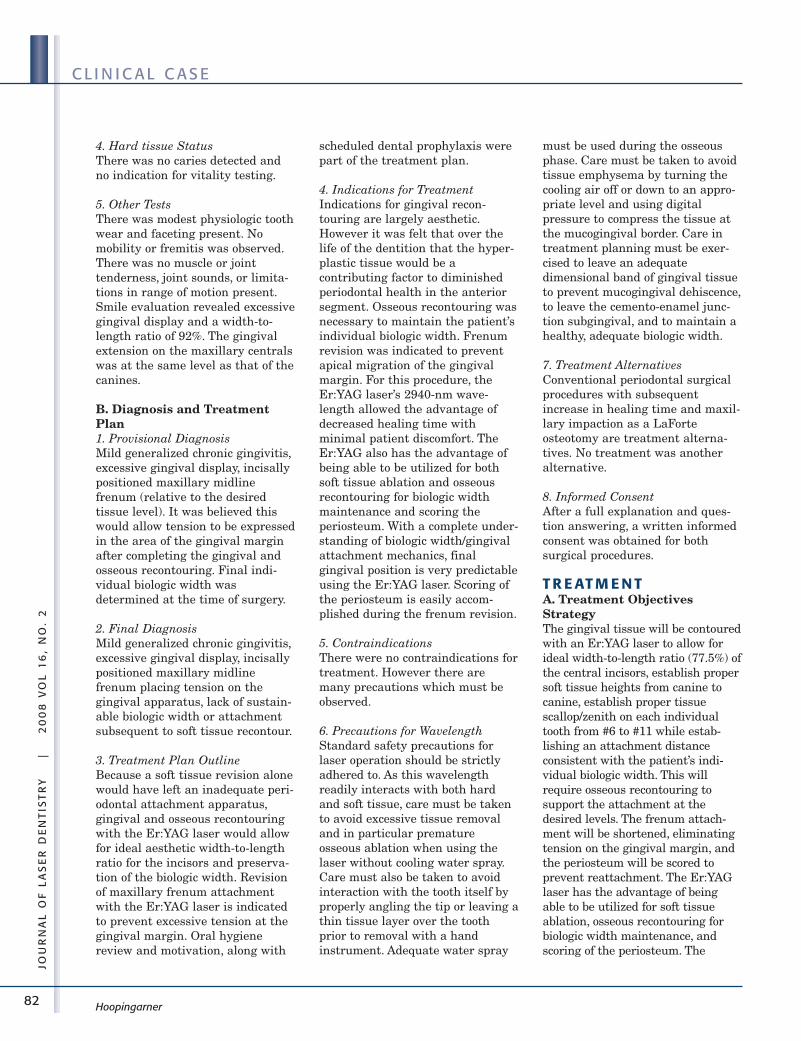
82
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
4. Hard tissue StatusThere was no caries detected andno indication for vitality testing.
5. Other TestsThere was modest physiologic toothwear and faceting present. Nomobility or fremitis was observed.There was no muscle or jointtenderness, joint sounds, or limita-tions in range of motion present.Smile evaluation revealed excessivegingival display and a width-to-length ratio of 92%. The gingivalextension on the maxillary centralswas at the same level as that of thecanines.
B. Diagnosis and TreatmentPlan1. Provisional DiagnosisMild generalized chronic gingivitis,excessive gingival display, incisallypositioned maxillary midlinefrenum (relative to the desiredtissue level). It was believed thiswould allow tension to be expressedin the area of the gingival marginafter completing the gingival andosseous recontouring. Final indi-vidual biologic width wasdetermined at the time of surgery.
2. Final DiagnosisMild generalized chronic gingivitis,excessive gingival display, incisallypositioned maxillary midlinefrenum placing tension on thegingival apparatus, lack of sustain-able biologic width or attachmentsubsequent to soft tissue recontour.
3. Treatment Plan OutlineBecause a soft tissue revision alonewould have left an inadequate peri-odontal attachment apparatus,gingival and osseous recontouringwith the Er:YAG laser would allowfor ideal aesthetic width-to-lengthratio for the incisors and preserva-tion of the biologic width. Revisionof maxillary frenum attachmentwith the Er:YAG laser is indicatedto prevent excessive tension at thegingival margin. Oral hygienereview and motivation, along with
scheduled dental prophylaxis werepart of the treatment plan.
4. Indications for TreatmentIndications for gingival recon-touring are largely aesthetic.However it was felt that over thelife of the dentition that the hyper-plastic tissue would be acontributing factor to diminishedperiodontal health in the anteriorsegment. Osseous recontouring wasnecessary to maintain the patient’sindividual biologic width. Frenumrevision was indicated to preventapical migration of the gingivalmargin. For this procedure, theEr:YAG laser’s 2940-nm wave-length allowed the advantage ofdecreased healing time withminimal patient discomfort. TheEr:YAG also has the advantage ofbeing able to be utilized for bothsoft tissue ablation and osseousrecontouring for biologic widthmaintenance and scoring theperiosteum. With a complete under-standing of biologic width/gingivalattachment mechanics, finalgingival position is very predictableusing the Er:YAG laser. Scoring ofthe periosteum is easily accom-plished during the frenum revision.
5. ContraindicationsThere were no contraindications fortreatment. However there aremany precautions which must beobserved.
6. Precautions for WavelengthStandard safety precautions forlaser operation should be strictlyadhered to. As this wavelengthreadily interacts with both hardand soft tissue, care must be takento avoid excessive tissue removaland in particular prematureosseous ablation when using thelaser without cooling water spray.Care must also be taken to avoidinteraction with the tooth itself byproperly angling the tip or leaving athin tissue layer over the toothprior to removal with a handinstrument. Adequate water spray
must be used during the osseousphase. Care must be taken to avoidtissue emphysema by turning thecooling air off or down to an appro-priate level and using digitalpressure to compress the tissue atthe mucogingival border. Care intreatment planning must be exer-cised to leave an adequatedimensional band of gingival tissueto prevent mucogingival dehiscence,to leave the cemento-enamel junc-tion subgingival, and to maintain ahealthy, adequate biologic width.
7. Treatment AlternativesConventional periodontal surgicalprocedures with subsequentincrease in healing time and maxil-lary impaction as a LaForteosteotomy are treatment alterna-tives. No treatment was anotheralternative.
8. Informed ConsentAfter a full explanation and ques-tion answering, a written informedconsent was obtained for bothsurgical procedures.
T R E AT M E N TA. Treatment ObjectivesStrategyThe gingival tissue will be contouredwith an Er:YAG laser to allow forideal width-to-length ratio (77.5%) ofthe central incisors, establish propersoft tissue heights from canine tocanine, establish proper tissuescallop/zenith on each individualtooth from #6 to #11 while estab-lishing an attachment distanceconsistent with the patient’s indi-vidual biologic width. This willrequire osseous recontouring tosupport the attachment at thedesired levels. The frenum attach-ment will be shortened, eliminatingtension on the gingival margin, andthe periosteum will be scored toprevent reattachment. The Er:YAGlaser has the advantage of beingable to be utilized for soft tissueablation, osseous recontouring forbiologic width maintenance, andscoring of the periosteum. The
Hoopingarner
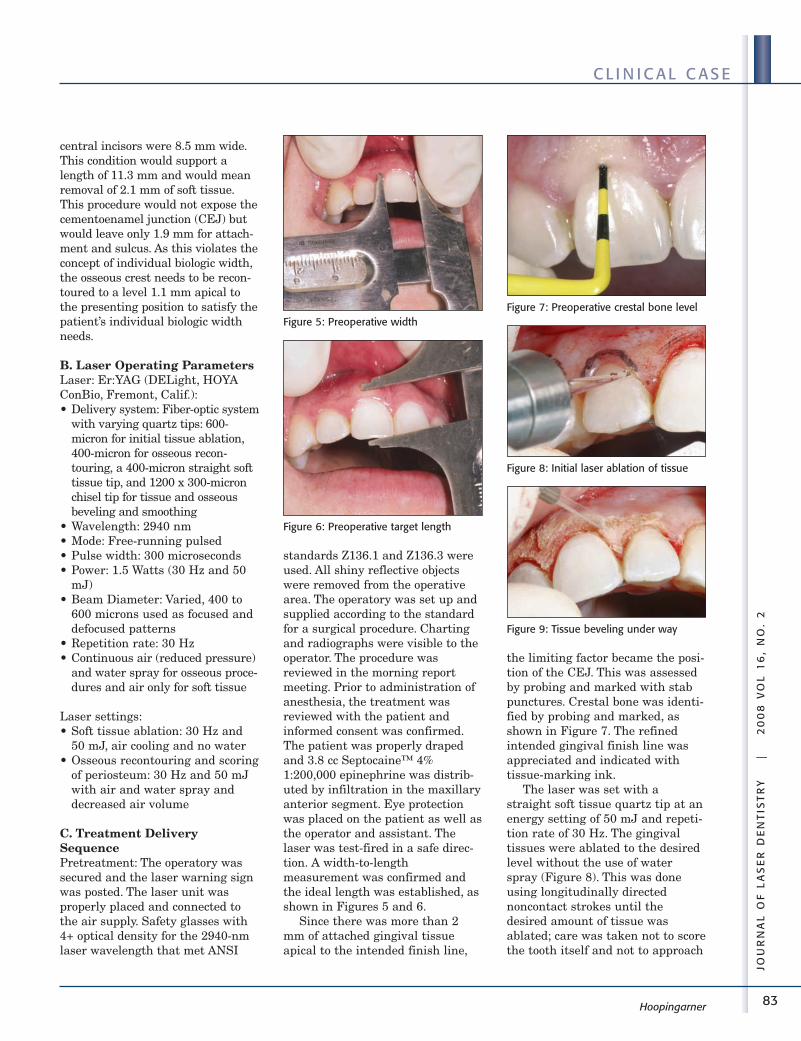
83
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Hoopingarner
central incisors were 8.5 mm wide.This condition would support alength of 11.3 mm and would meanremoval of 2.1 mm of soft tissue.This procedure would not expose thecementoenamel junction (CEJ) butwould leave only 1.9 mm for attach-ment and sulcus. As this violates theconcept of individual biologic width,the osseous crest needs to be recon-toured to a level 1.1 mm apical tothe presenting position to satisfy thepatient’s individual biologic widthneeds.
B. Laser Operating ParametersLaser: Er:YAG (DELight, HOYAConBio, Fremont, Calif.):• Delivery system: Fiber-optic system
with varying quartz tips: 600-micron for initial tissue ablation,400-micron for osseous recon-touring, a 400-micron straight softtissue tip, and 1200 x 300-micronchisel tip for tissue and osseousbeveling and smoothing
• Wavelength: 2940 nm• Mode: Free-running pulsed• Pulse width: 300 microseconds• Power: 1.5 Watts (30 Hz and 50
mJ)• Beam Diameter: Varied, 400 to
600 microns used as focused anddefocused patterns
• Repetition rate: 30 Hz• Continuous air (reduced pressure)
and water spray for osseous proce-dures and air only for soft tissue
Laser settings:• Soft tissue ablation: 30 Hz and
50 mJ, air cooling and no water• Osseous recontouring and scoring
of periosteum: 30 Hz and 50 mJwith air and water spray anddecreased air volume
C. Treatment DeliverySequencePretreatment: The operatory wassecured and the laser warning signwas posted. The laser unit wasproperly placed and connected tothe air supply. Safety glasses with4+ optical density for the 2940-nmlaser wavelength that met ANSI
standards Z136.1 and Z136.3 wereused. All shiny reflective objectswere removed from the operativearea. The operatory was set up andsupplied according to the standardfor a surgical procedure. Chartingand radiographs were visible to theoperator. The procedure wasreviewed in the morning reportmeeting. Prior to administration ofanesthesia, the treatment wasreviewed with the patient andinformed consent was confirmed.The patient was properly drapedand 3.8 cc Septocaine™ 4%1:200,000 epinephrine was distrib-uted by infiltration in the maxillaryanterior segment. Eye protectionwas placed on the patient as well asthe operator and assistant. Thelaser was test-fired in a safe direc-tion. A width-to-lengthmeasurement was confirmed andthe ideal length was established, asshown in Figures 5 and 6.
Since there was more than 2mm of attached gingival tissueapical to the intended finish line,
the limiting factor became the posi-tion of the CEJ. This was assessedby probing and marked with stabpunctures. Crestal bone was identi-fied by probing and marked, asshown in Figure 7. The refinedintended gingival finish line wasappreciated and indicated withtissue-marking ink.
The laser was set with astraight soft tissue quartz tip at anenergy setting of 50 mJ and repeti-tion rate of 30 Hz. The gingivaltissues were ablated to the desiredlevel without the use of waterspray (Figure 8). This was doneusing longitudinally directednoncontact strokes until thedesired amount of tissue wasablated; care was taken not to scorethe tooth itself and not to approach
Figure 5: Preoperative width
Figure 6: Preoperative target length
Figure 7: Preoperative crestal bone level
Figure 8: Initial laser ablation of tissue
Figure 9: Tissue beveling under way
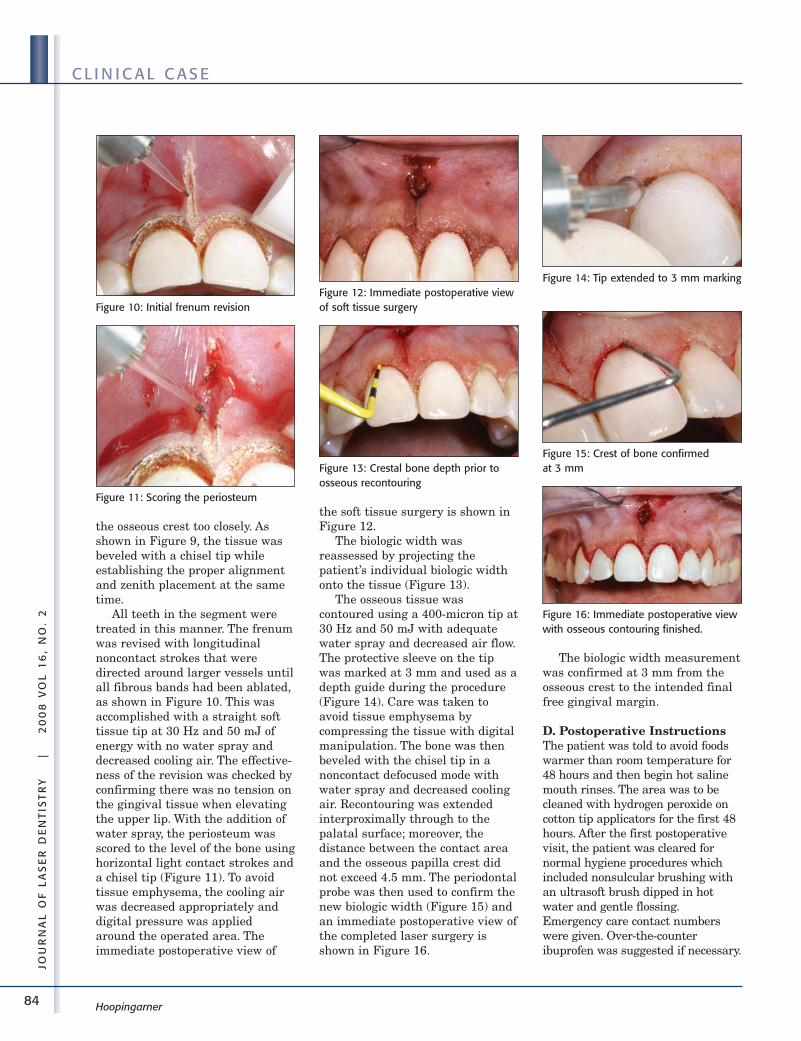
84
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Hoopingarner
the osseous crest too closely. Asshown in Figure 9, the tissue wasbeveled with a chisel tip whileestablishing the proper alignmentand zenith placement at the sametime.
All teeth in the segment weretreated in this manner. The frenumwas revised with longitudinalnoncontact strokes that weredirected around larger vessels untilall fibrous bands had been ablated,as shown in Figure 10. This wasaccomplished with a straight softtissue tip at 30 Hz and 50 mJ ofenergy with no water spray anddecreased cooling air. The effective-ness of the revision was checked byconfirming there was no tension onthe gingival tissue when elevatingthe upper lip. With the addition ofwater spray, the periosteum wasscored to the level of the bone usinghorizontal light contact strokes anda chisel tip (Figure 11). To avoidtissue emphysema, the cooling airwas decreased appropriately anddigital pressure was appliedaround the operated area. Theimmediate postoperative view of
the soft tissue surgery is shown inFigure 12.
The biologic width wasreassessed by projecting thepatient’s individual biologic widthonto the tissue (Figure 13).
The osseous tissue wascontoured using a 400-micron tip at30 Hz and 50 mJ with adequatewater spray and decreased air flow.The protective sleeve on the tipwas marked at 3 mm and used as adepth guide during the procedure(Figure 14). Care was taken toavoid tissue emphysema bycompressing the tissue with digitalmanipulation. The bone was thenbeveled with the chisel tip in anoncontact defocused mode withwater spray and decreased coolingair. Recontouring was extendedinterproximally through to thepalatal surface; moreover, thedistance between the contact areaand the osseous papilla crest didnot exceed 4.5 mm. The periodontalprobe was then used to confirm thenew biologic width (Figure 15) andan immediate postoperative view ofthe completed laser surgery isshown in Figure 16.
The biologic width measurementwas confirmed at 3 mm from theosseous crest to the intended finalfree gingival margin.
D. Postoperative InstructionsThe patient was told to avoid foodswarmer than room temperature for48 hours and then begin hot salinemouth rinses. The area was to becleaned with hydrogen peroxide oncotton tip applicators for the first 48hours. After the first postoperativevisit, the patient was cleared fornormal hygiene procedures whichincluded nonsulcular brushing withan ultrasoft brush dipped in hotwater and gentle flossing.Emergency care contact numberswere given. Over-the-counteribuprofen was suggested if necessary.
Figure 10: Initial frenum revision
Figure 11: Scoring the periosteum
Figure 12: Immediate postoperative viewof soft tissue surgery
Figure 13: Crestal bone depth prior toosseous recontouring
Figure 14: Tip extended to 3 mm marking
Figure 15: Crest of bone confirmed at 3 mm
Figure 16: Immediate postoperative viewwith osseous contouring finished.
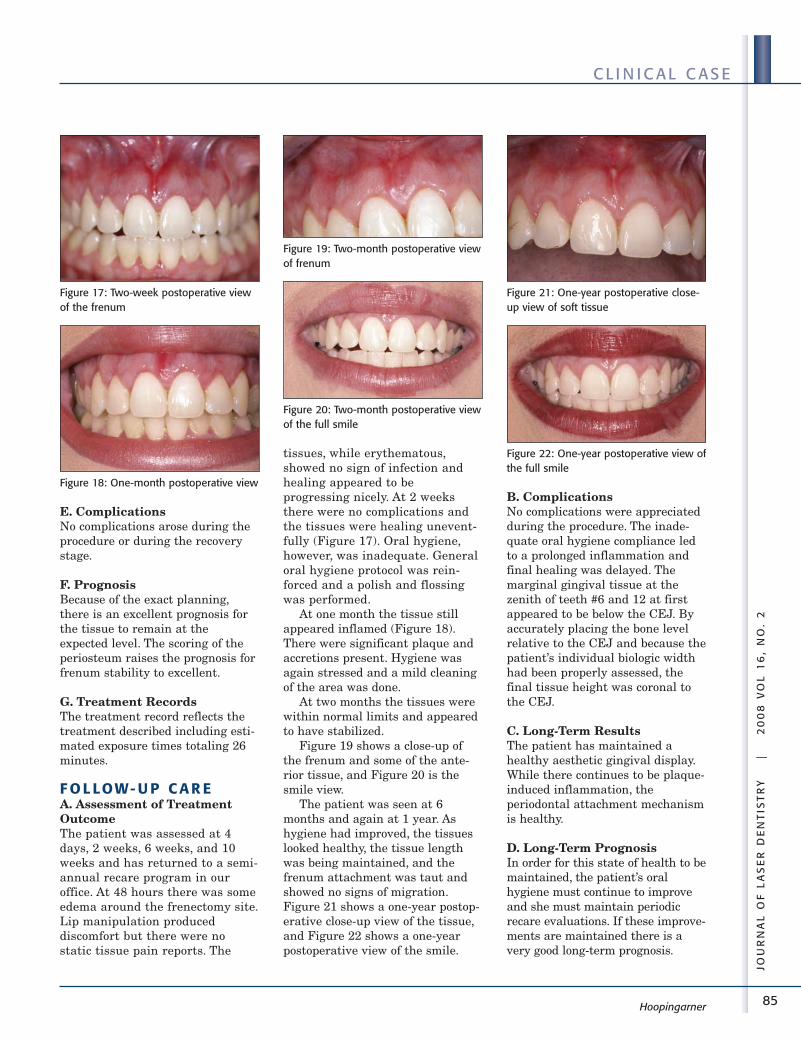
85
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Hoopingarner
E. ComplicationsNo complications arose during theprocedure or during the recoverystage.
F. PrognosisBecause of the exact planning,there is an excellent prognosis forthe tissue to remain at theexpected level. The scoring of theperiosteum raises the prognosis forfrenum stability to excellent.
G. Treatment RecordsThe treatment record reflects thetreatment described including esti-mated exposure times totaling 26minutes.
F O L LOW- U P C A R EA. Assessment of TreatmentOutcomeThe patient was assessed at 4days, 2 weeks, 6 weeks, and 10weeks and has returned to a semi-annual recare program in ouroffice. At 48 hours there was someedema around the frenectomy site.Lip manipulation produceddiscomfort but there were nostatic tissue pain reports. The
tissues, while erythematous,showed no sign of infection andhealing appeared to beprogressing nicely. At 2 weeksthere were no complications andthe tissues were healing unevent-fully (Figure 17). Oral hygiene,however, was inadequate. Generaloral hygiene protocol was rein-forced and a polish and flossingwas performed.
At one month the tissue stillappeared inflamed (Figure 18).There were significant plaque andaccretions present. Hygiene wasagain stressed and a mild cleaningof the area was done.
At two months the tissues werewithin normal limits and appearedto have stabilized.
Figure 19 shows a close-up ofthe frenum and some of the ante-rior tissue, and Figure 20 is thesmile view.
The patient was seen at 6months and again at 1 year. Ashygiene had improved, the tissueslooked healthy, the tissue lengthwas being maintained, and thefrenum attachment was taut andshowed no signs of migration.Figure 21 shows a one-year postop-erative close-up view of the tissue,and Figure 22 shows a one-yearpostoperative view of the smile.
B. ComplicationsNo complications were appreciatedduring the procedure. The inade-quate oral hygiene compliance ledto a prolonged inflammation andfinal healing was delayed. Themarginal gingival tissue at thezenith of teeth #6 and 12 at firstappeared to be below the CEJ. Byaccurately placing the bone levelrelative to the CEJ and because thepatient’s individual biologic widthhad been properly assessed, thefinal tissue height was coronal tothe CEJ.
C. Long-Term ResultsThe patient has maintained ahealthy aesthetic gingival display.While there continues to be plaque-induced inflammation, theperiodontal attachment mechanismis healthy.
D. Long-Term PrognosisIn order for this state of health to bemaintained, the patient’s oralhygiene must continue to improveand she must maintain periodicrecare evaluations. If these improve-ments are maintained there is avery good long-term prognosis.
Figure 17: Two-week postoperative viewof the frenum
Figure 18: One-month postoperative view
Figure 19: Two-month postoperative viewof frenum
Figure 20: Two-month postoperative viewof the full smile
Figure 21: One-year postoperative close-up view of soft tissue
Figure 22: One-year postoperative view ofthe full smile

86
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Hoopingarner
A U T H O R B I O G R A P H YDr. Charles Hoopingarner attendedthe University of Texas HealthScience Center at Houston(UTHSCH) Dental Branch, gradu-ating with a DDS in 1973. He hasmaintained a private practice inHouston, Texas since 1973. He wasan adjunct associate professor inanatomical sciences at UTHSCHDental Branch for 11 years.Currently he is adjunct clinicalfaculty in the Restorative DentistryDepartment at UTHSCH and has
been a clinical instructor at the LasVegas Institute for AdvancedDental Studies since 1997, teachingAdvanced Anterior Aesthetics andComprehensive AestheticReconstruction and Laser Dentistry.Dr. Hoopingarner is a member ofthe Academy of Laser Dentistry(ALD) and has used dental lasers ofvarious wavelengths as integralparts of his patient care deliverysystem for the last 10 years. Heholds Advanced and StandardProficiency certification from the
ALD and has lectured internation-ally on the safety and use of lasertechnology in the dental practice.He may be contacted by e-mail [email protected].
Disclosure: Dr. Hoopingarner has nodirect financial or ownership posi-tions with commercial companiesrelative to this case presentation. Hehas received honoraria and expensesfrom HOYA ConBio to present mate-rial on laser dentistry. ■■
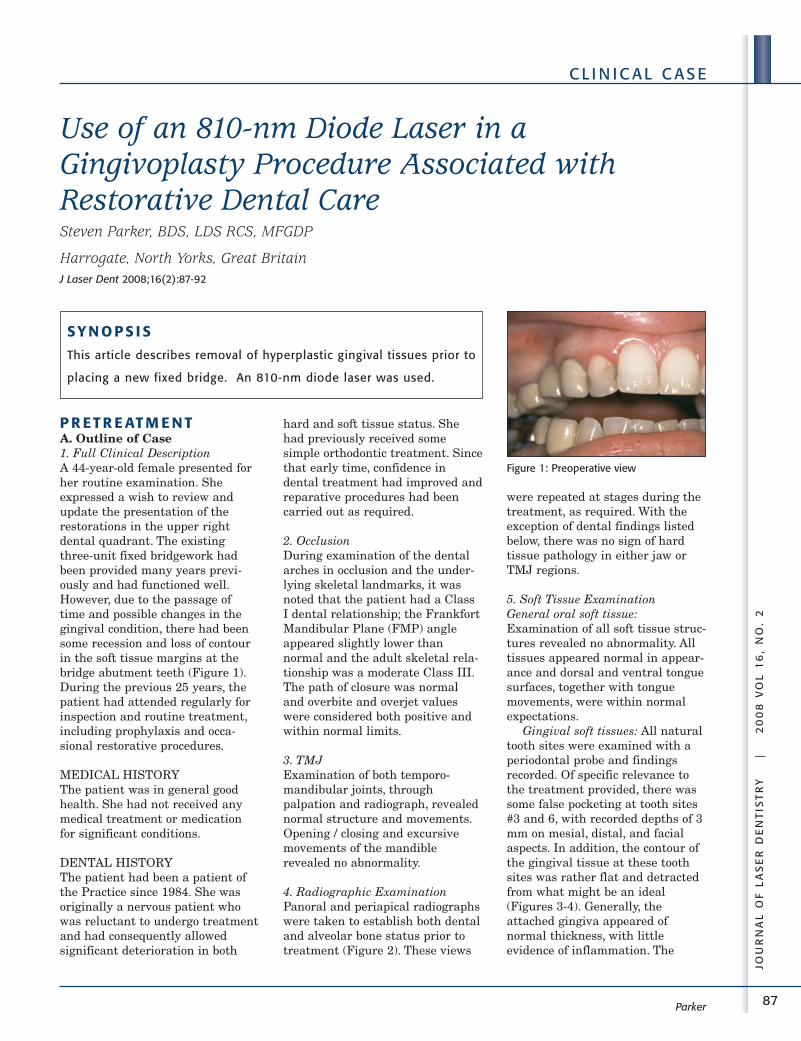
87
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Use of an 810-nm Diode Laser in aGingivoplasty Procedure Associated withRestorative Dental CareSteven Parker, BDS, LDS RCS, MFGDP
Harrogate, North Yorks, Great BritainJ Laser Dent 2008;16(2):87-92
P R ET R E AT M E N TA. Outline of Case1. Full Clinical DescriptionA 44-year-old female presented forher routine examination. Sheexpressed a wish to review andupdate the presentation of therestorations in the upper rightdental quadrant. The existingthree-unit fixed bridgework hadbeen provided many years previ-ously and had functioned well.However, due to the passage oftime and possible changes in thegingival condition, there had beensome recession and loss of contourin the soft tissue margins at thebridge abutment teeth (Figure 1).During the previous 25 years, thepatient had attended regularly forinspection and routine treatment,including prophylaxis and occa-sional restorative procedures.
MEDICAL HISTORYThe patient was in general goodhealth. She had not received anymedical treatment or medicationfor significant conditions.
DENTAL HISTORYThe patient had been a patient ofthe Practice since 1984. She wasoriginally a nervous patient whowas reluctant to undergo treatmentand had consequently allowedsignificant deterioration in both
hard and soft tissue status. Shehad previously received somesimple orthodontic treatment. Sincethat early time, confidence indental treatment had improved andreparative procedures had beencarried out as required.
2. OcclusionDuring examination of the dentalarches in occlusion and the under-lying skeletal landmarks, it wasnoted that the patient had a ClassI dental relationship; the FrankfortMandibular Plane (FMP) angleappeared slightly lower thannormal and the adult skeletal rela-tionship was a moderate Class III.The path of closure was normaland overbite and overjet valueswere considered both positive andwithin normal limits.
3. TMJExamination of both temporo-mandibular joints, throughpalpation and radiograph, revealednormal structure and movements.Opening / closing and excursivemovements of the mandiblerevealed no abnormality.
4. Radiographic ExaminationPanoral and periapical radiographswere taken to establish both dentaland alveolar bone status prior totreatment (Figure 2). These views
were repeated at stages during thetreatment, as required. With theexception of dental findings listedbelow, there was no sign of hardtissue pathology in either jaw orTMJ regions.
5. Soft Tissue ExaminationGeneral oral soft tissue:Examination of all soft tissue struc-tures revealed no abnormality. Alltissues appeared normal in appear-ance and dorsal and ventral tonguesurfaces, together with tonguemovements, were within normalexpectations.
Gingival soft tissues: All naturaltooth sites were examined with aperiodontal probe and findingsrecorded. Of specific relevance tothe treatment provided, there wassome false pocketing at tooth sites#3 and 6, with recorded depths of 3mm on mesial, distal, and facialaspects. In addition, the contour ofthe gingival tissue at these toothsites was rather flat and detractedfrom what might be an ideal(Figures 3-4). Generally, theattached gingiva appeared ofnormal thickness, with littleevidence of inflammation. The
Parker
SY N O P S I S
This article describes removal of hyperplastic gingival tissues prior to
placing a new fixed bridge. An 810-nm diode laser was used.
Figure 1: Preoperative view
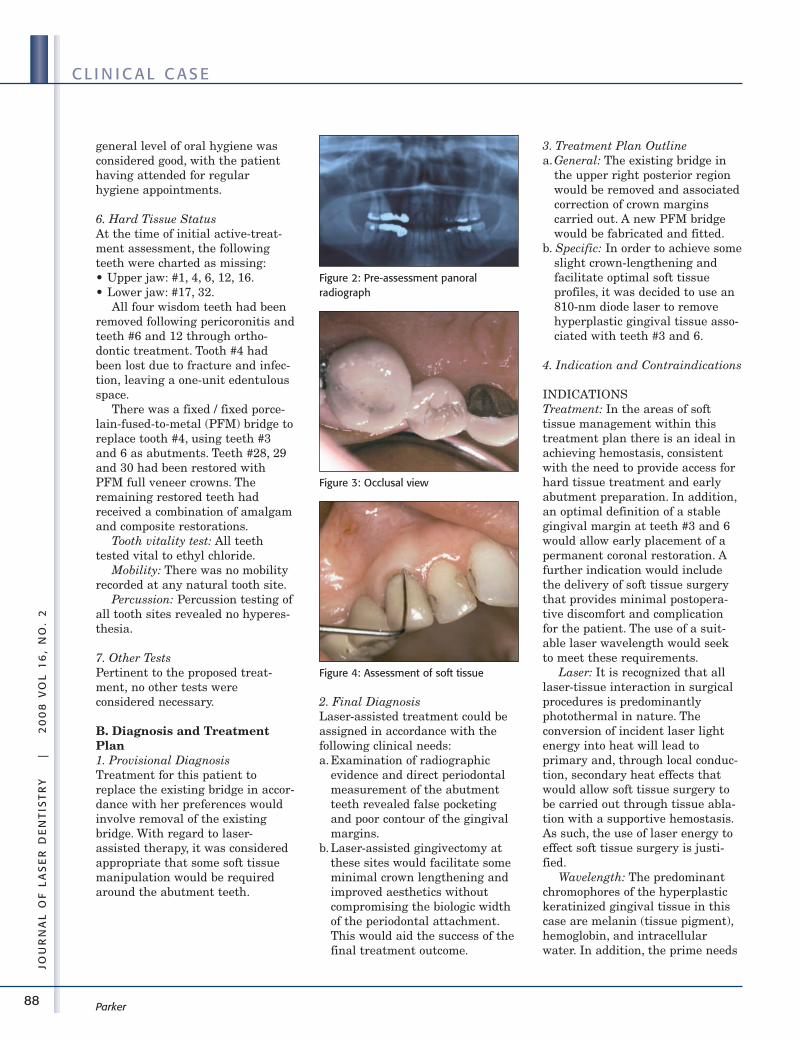
88
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Parker
general level of oral hygiene wasconsidered good, with the patienthaving attended for regularhygiene appointments.
6. Hard Tissue StatusAt the time of initial active-treat-ment assessment, the followingteeth were charted as missing:• Upper jaw: #1, 4, 6, 12, 16.• Lower jaw: #17, 32.
All four wisdom teeth had beenremoved following pericoronitis andteeth #6 and 12 through ortho-dontic treatment. Tooth #4 hadbeen lost due to fracture and infec-tion, leaving a one-unit edentulousspace.
There was a fixed / fixed porce-lain-fused-to-metal (PFM) bridge toreplace tooth #4, using teeth #3and 6 as abutments. Teeth #28, 29and 30 had been restored withPFM full veneer crowns. Theremaining restored teeth hadreceived a combination of amalgamand composite restorations.
Tooth vitality test: All teethtested vital to ethyl chloride.
Mobility: There was no mobilityrecorded at any natural tooth site.
Percussion: Percussion testing ofall tooth sites revealed no hyperes-thesia.
7. Other TestsPertinent to the proposed treat-ment, no other tests wereconsidered necessary.
B. Diagnosis and TreatmentPlan1. Provisional DiagnosisTreatment for this patient toreplace the existing bridge in accor-dance with her preferences wouldinvolve removal of the existingbridge. With regard to laser-assisted therapy, it was consideredappropriate that some soft tissuemanipulation would be requiredaround the abutment teeth.
2. Final DiagnosisLaser-assisted treatment could beassigned in accordance with thefollowing clinical needs:a.Examination of radiographic
evidence and direct periodontalmeasurement of the abutmentteeth revealed false pocketingand poor contour of the gingivalmargins.
b. Laser-assisted gingivectomy atthese sites would facilitate someminimal crown lengthening andimproved aesthetics withoutcompromising the biologic widthof the periodontal attachment.This would aid the success of thefinal treatment outcome.
3. Treatment Plan Outlinea.General: The existing bridge in
the upper right posterior regionwould be removed and associatedcorrection of crown marginscarried out. A new PFM bridgewould be fabricated and fitted.
b. Specific: In order to achieve someslight crown-lengthening andfacilitate optimal soft tissueprofiles, it was decided to use an810-nm diode laser to removehyperplastic gingival tissue asso-ciated with teeth #3 and 6.
4. Indication and Contraindications
INDICATIONSTreatment: In the areas of softtissue management within thistreatment plan there is an ideal inachieving hemostasis, consistentwith the need to provide access forhard tissue treatment and earlyabutment preparation. In addition,an optimal definition of a stablegingival margin at teeth #3 and 6would allow early placement of apermanent coronal restoration. Afurther indication would includethe delivery of soft tissue surgerythat provides minimal postopera-tive discomfort and complicationfor the patient. The use of a suit-able laser wavelength would seekto meet these requirements.
Laser: It is recognized that alllaser-tissue interaction in surgicalprocedures is predominantlyphotothermal in nature. Theconversion of incident laser lightenergy into heat will lead toprimary and, through local conduc-tion, secondary heat effects thatwould allow soft tissue surgery tobe carried out through tissue abla-tion with a supportive hemostasis.As such, the use of laser energy toeffect soft tissue surgery is justi-fied.
Wavelength: The predominantchromophores of the hyperplastickeratinized gingival tissue in thiscase are melanin (tissue pigment),hemoglobin, and intracellularwater. In addition, the prime needs
Figure 3: Occlusal view
Figure 4: Assessment of soft tissue
Figure 2: Pre-assessment panoral radiograph
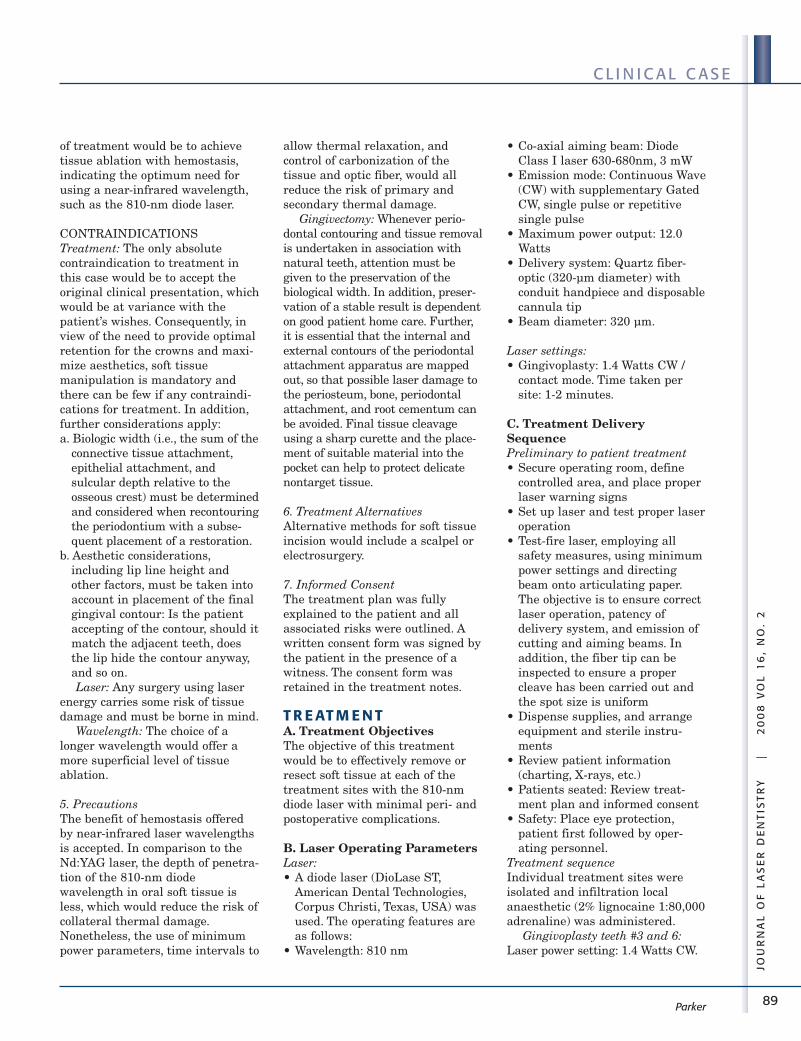
89
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Parker
of treatment would be to achievetissue ablation with hemostasis,indicating the optimum need forusing a near-infrared wavelength,such as the 810-nm diode laser.
CONTRAINDICATIONSTreatment: The only absolutecontraindication to treatment inthis case would be to accept theoriginal clinical presentation, whichwould be at variance with thepatient’s wishes. Consequently, inview of the need to provide optimalretention for the crowns and maxi-mize aesthetics, soft tissuemanipulation is mandatory andthere can be few if any contraindi-cations for treatment. In addition,further considerations apply:a. Biologic width (i.e., the sum of the
connective tissue attachment,epithelial attachment, andsulcular depth relative to theosseous crest) must be determinedand considered when recontouringthe periodontium with a subse-quent placement of a restoration.
b. Aesthetic considerations,including lip line height andother factors, must be taken intoaccount in placement of the finalgingival contour: Is the patientaccepting of the contour, should itmatch the adjacent teeth, doesthe lip hide the contour anyway,and so on.Laser: Any surgery using laser
energy carries some risk of tissuedamage and must be borne in mind.
Wavelength: The choice of alonger wavelength would offer amore superficial level of tissueablation.
5. PrecautionsThe benefit of hemostasis offeredby near-infrared laser wavelengthsis accepted. In comparison to theNd:YAG laser, the depth of penetra-tion of the 810-nm diodewavelength in oral soft tissue isless, which would reduce the risk ofcollateral thermal damage.Nonetheless, the use of minimumpower parameters, time intervals to
allow thermal relaxation, andcontrol of carbonization of thetissue and optic fiber, would allreduce the risk of primary andsecondary thermal damage.
Gingivectomy: Whenever perio -dontal contouring and tissue removalis undertaken in association withnatural teeth, attention must begiven to the preservation of thebiological width. In addition, preser-vation of a stable result is dependenton good patient home care. Further,it is essential that the internal andexternal contours of the periodontalattachment apparatus are mappedout, so that possible laser damage tothe periosteum, bone, periodontalattachment, and root cementum canbe avoided. Final tissue cleavageusing a sharp curette and the place-ment of suitable material into thepocket can help to protect delicatenontarget tissue.
6. Treatment AlternativesAlternative methods for soft tissueincision would include a scalpel orelectrosurgery.
7. Informed ConsentThe treatment plan was fullyexplained to the patient and allassociated risks were outlined. Awritten consent form was signed bythe patient in the presence of awitness. The consent form wasretained in the treatment notes.
T R E AT M E N TA. Treatment ObjectivesThe objective of this treatmentwould be to effectively remove orresect soft tissue at each of thetreatment sites with the 810-nmdiode laser with minimal peri- andpostoperative complications.
B. Laser Operating ParametersLaser:• A diode laser (DioLase ST,
American Dental Technologies,Corpus Christi, Texas, USA) wasused. The operating features areas follows:
• Wavelength: 810 nm
• Co-axial aiming beam: DiodeClass I laser 630-680nm, 3 mW
• Emission mode: Continuous Wave(CW) with supplementary GatedCW, single pulse or repetitivesingle pulse
• Maximum power output: 12.0Watts
• Delivery system: Quartz fiber-optic (320-µm diameter) withconduit handpiece and disposablecannula tip
• Beam diameter: 320 µm.
Laser settings:• Gingivoplasty: 1.4 Watts CW /
contact mode. Time taken persite: 1-2 minutes.
C. Treatment DeliverySequencePreliminary to patient treatment• Secure operating room, define
controlled area, and place properlaser warning signs
• Set up laser and test proper laseroperation
• Test-fire laser, employing allsafety measures, using minimumpower settings and directingbeam onto articulating paper.The objective is to ensure correctlaser operation, patency ofdelivery system, and emission ofcutting and aiming beams. Inaddition, the fiber tip can beinspected to ensure a propercleave has been carried out andthe spot size is uniform
• Dispense supplies, and arrangeequipment and sterile instru-ments
• Review patient information(charting, X-rays, etc.)
• Patients seated: Review treat-ment plan and informed consent
• Safety: Place eye protection,patient first followed by oper-ating personnel.
Treatment sequenceIndividual treatment sites wereisolated and infiltration localanaesthetic (2% lignocaine 1:80,000adrenaline) was administered.
Gingivoplasty teeth #3 and 6:Laser power setting: 1.4 Watts CW.
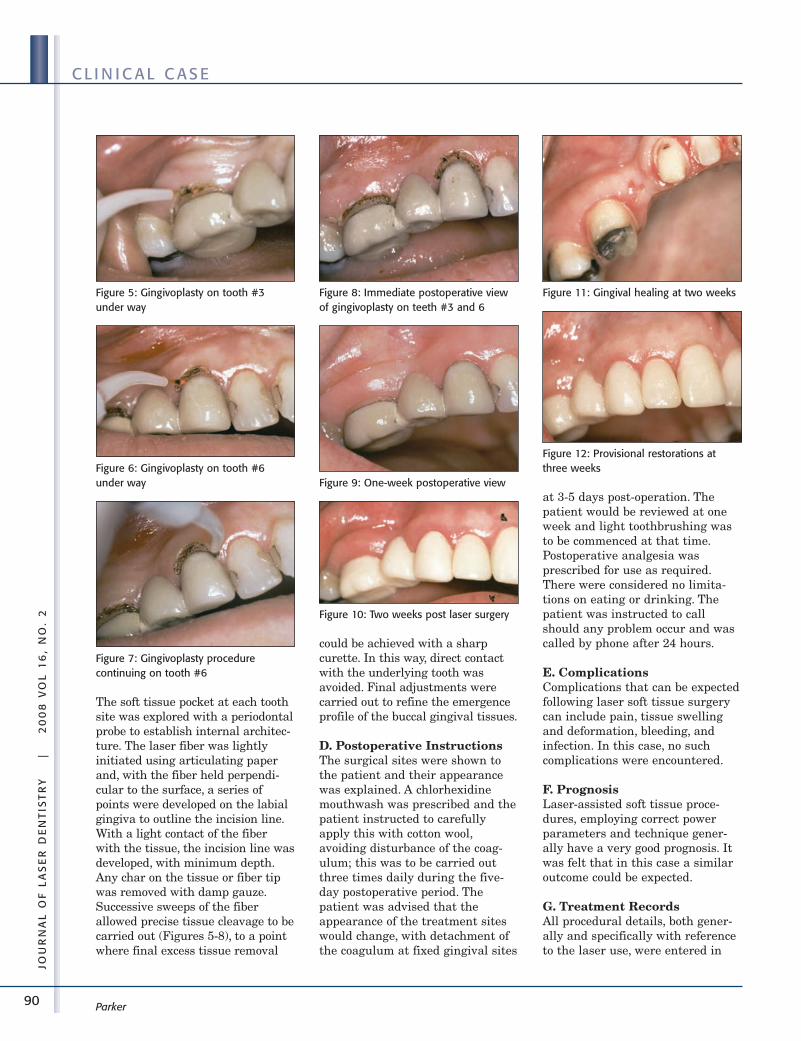
90
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Parker
The soft tissue pocket at each toothsite was explored with a periodontalprobe to establish internal architec-ture. The laser fiber was lightlyinitiated using articulating paperand, with the fiber held perpendi-cular to the surface, a series ofpoints were developed on the labialgingiva to outline the incision line.With a light contact of the fiberwith the tissue, the incision line wasdeveloped, with minimum depth.Any char on the tissue or fiber tipwas removed with damp gauze.Successive sweeps of the fiberallowed precise tissue cleavage to becarried out (Figures 5-8), to a pointwhere final excess tissue removal
could be achieved with a sharpcurette. In this way, direct contactwith the underlying tooth wasavoided. Final adjustments werecarried out to refine the emergenceprofile of the buccal gingival tissues.
D. Postoperative InstructionsThe surgical sites were shown tothe patient and their appearancewas explained. A chlorhexidinemouthwash was prescribed and thepatient instructed to carefullyapply this with cotton wool,avoiding disturbance of the coag-ulum; this was to be carried outthree times daily during the five-day postoperative period. Thepatient was advised that theappearance of the treatment siteswould change, with detachment ofthe coagulum at fixed gingival sites
at 3-5 days post-operation. Thepatient would be reviewed at oneweek and light toothbrushing wasto be commenced at that time.Postoperative analgesia wasprescribed for use as required.There were considered no limita-tions on eating or drinking. Thepatient was instructed to callshould any problem occur and wascalled by phone after 24 hours.
E. ComplicationsComplications that can be expectedfollowing laser soft tissue surgerycan include pain, tissue swellingand deformation, bleeding, andinfection. In this case, no suchcomplications were encountered.
F. PrognosisLaser-assisted soft tissue proce-dures, employing correct powerparameters and technique gener-ally have a very good prognosis. Itwas felt that in this case a similaroutcome could be expected.
G. Treatment RecordsAll procedural details, both gener-ally and specifically with referenceto the laser use, were entered in
Figure 5: Gingivoplasty on tooth #3under way
Figure 6: Gingivoplasty on tooth #6under way
Figure 7: Gingivoplasty procedure continuing on tooth #6
Figure 8: Immediate postoperative viewof gingivoplasty on teeth #3 and 6
Figure 9: One-week postoperative view
Figure 11: Gingival healing at two weeks
Figure 12: Provisional restorations atthree weeks
Figure 10: Two weeks post laser surgery
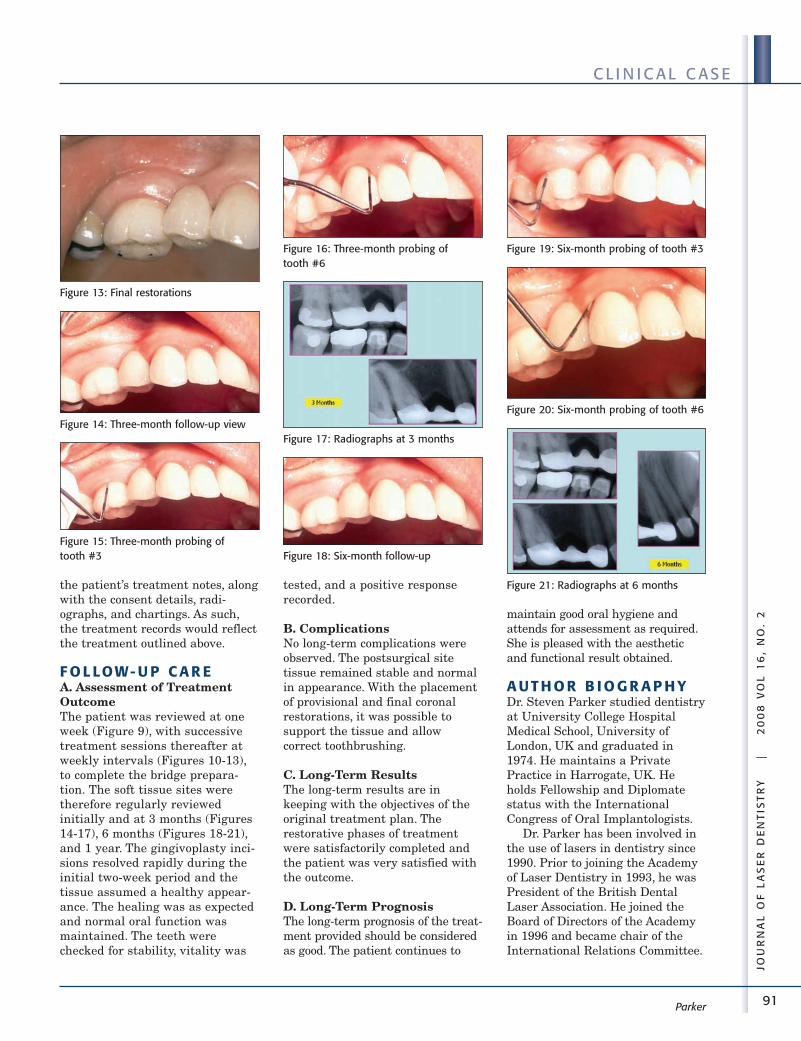
91
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Parker
the patient’s treatment notes, alongwith the consent details, radi-ographs, and chartings. As such,the treatment records would reflectthe treatment outlined above.
F O L LOW- U P C A R EA. Assessment of TreatmentOutcomeThe patient was reviewed at oneweek (Figure 9), with successivetreatment sessions thereafter atweekly intervals (Figures 10-13),to complete the bridge prepara-tion. The soft tissue sites weretherefore regularly reviewedinitially and at 3 months (Figures14-17), 6 months (Figures 18-21),and 1 year. The gingivoplasty inci-sions resolved rapidly during theinitial two-week period and thetissue assumed a healthy appear-ance. The healing was as expectedand normal oral function wasmaintained. The teeth werechecked for stability, vitality was
tested, and a positive responserecorded.
B. ComplicationsNo long-term complications wereobserved. The postsurgical sitetissue remained stable and normalin appearance. With the placementof provisional and final coronalrestorations, it was possible tosupport the tissue and allowcorrect toothbrushing.
C. Long-Term ResultsThe long-term results are inkeeping with the objectives of theoriginal treatment plan. Therestorative phases of treatmentwere satisfactorily completed andthe patient was very satisfied withthe outcome.
D. Long-Term PrognosisThe long-term prognosis of the treat-ment provided should be consideredas good. The patient continues to
maintain good oral hygiene andattends for assessment as required.She is pleased with the aestheticand functional result obtained.
A U T H O R B I O G R A P H YDr. Steven Parker studied dentistryat University College HospitalMedical School, University ofLondon, UK and graduated in1974. He maintains a PrivatePractice in Harrogate, UK. Heholds Fellowship and Diplomatestatus with the InternationalCongress of Oral Implantologists.
Dr. Parker has been involved inthe use of lasers in dentistry since1990. Prior to joining the Academyof Laser Dentistry in 1993, he wasPresident of the British DentalLaser Association. He joined theBoard of Directors of the Academyin 1996 and became chair of theInternational Relations Committee.
Figure 13: Final restorations
Figure 15: Three-month probing of tooth #3
Figure 16: Three-month probing of tooth #6
Figure 17: Radiographs at 3 months
Figure 18: Six-month follow-up
Figure 19: Six-month probing of tooth #3
Figure 20: Six-month probing of tooth #6
Figure 21: Radiographs at 6 months
Figure 14: Three-month follow-up view
92
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Parker
From 1999 through 2004, he waschair of the Committee forProficiency Recognition and co-editor of Wavelengths, the formerjournal of the Academy of LaserDentistry. He was awarded theLeon Goldman award for Excellence
in Clinical Laser Dentistry by theAcademy in 1998. In addition, Dr.Parker holds Advanced Proficiencystatus in multiple laser wave-lengths and completed the AcademyEducator Course at the Universityof California San Francisco.
Dr. Parker may be contacted bye-mail at [email protected].
Disclosure: Dr. Parker has nocurrent commercial affiliation. ■■
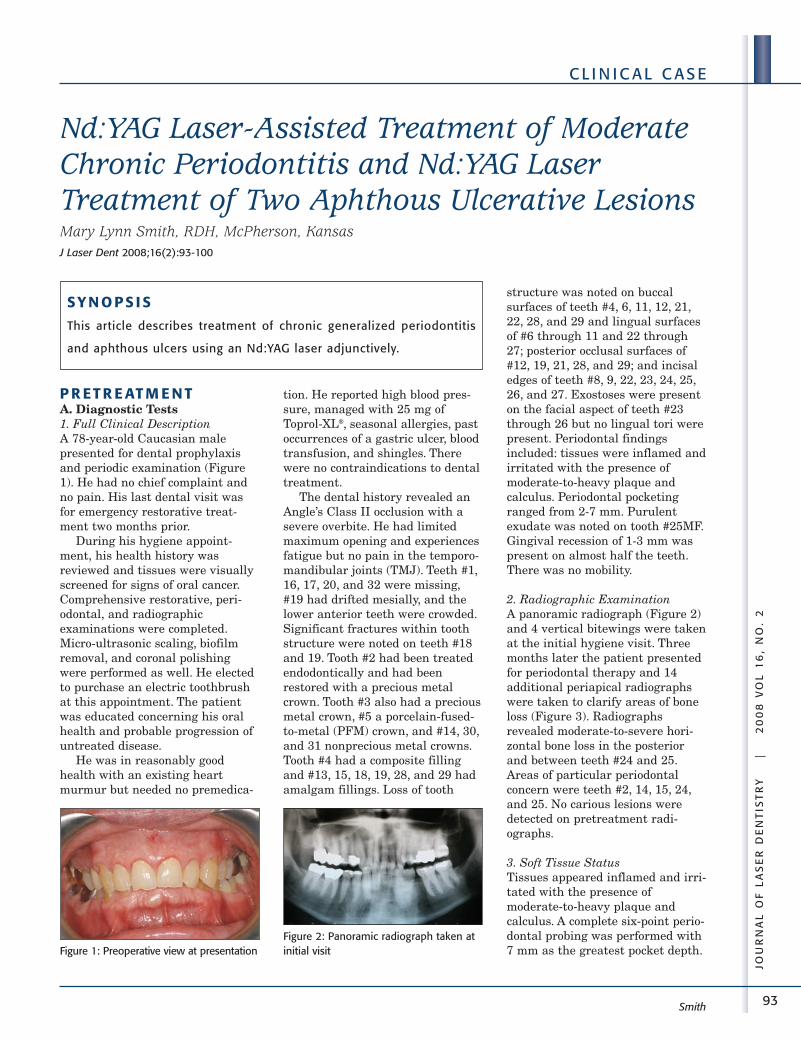
93
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Nd:YAG Laser-Assisted Treatment of ModerateChronic Periodontitis and Nd:YAG LaserTreatment of Two Aphthous Ulcerative LesionsMary Lynn Smith, RDH, McPherson, KansasJ Laser Dent 2008;16(2):93-100
P R ET R E AT M E N TA. Diagnostic Tests1. Full Clinical DescriptionA 78-year-old Caucasian malepresented for dental prophylaxisand periodic examination (Figure1). He had no chief complaint andno pain. His last dental visit wasfor emergency restorative treat-ment two months prior.
During his hygiene appoint-ment, his health history wasreviewed and tissues were visuallyscreened for signs of oral cancer.Comprehensive restorative, peri-odontal, and radiographicexaminations were completed.Micro-ultrasonic scaling, biofilmremoval, and coronal polishingwere performed as well. He electedto purchase an electric toothbrushat this appointment. The patientwas educated concerning his oralhealth and probable progression ofuntreated disease.
He was in reasonably goodhealth with an existing heartmurmur but needed no premedica-
tion. He reported high blood pres-sure, managed with 25 mg ofToprol-XL®, seasonal allergies, pastoccurrences of a gastric ulcer, bloodtransfusion, and shingles. Therewere no contraindications to dentaltreatment.
The dental history revealed anAngle’s Class II occlusion with asevere overbite. He had limitedmaximum opening and experiencesfatigue but no pain in the temporo-mandibular joints (TMJ). Teeth #1,16, 17, 20, and 32 were missing,#19 had drifted mesially, and thelower anterior teeth were crowded.Significant fractures within toothstructure were noted on teeth #18and 19. Tooth #2 had been treatedendodontically and had beenrestored with a precious metalcrown. Tooth #3 also had a preciousmetal crown, #5 a porcelain-fused-to-metal (PFM) crown, and #14, 30,and 31 nonprecious metal crowns.Tooth #4 had a composite fillingand #13, 15, 18, 19, 28, and 29 hadamalgam fillings. Loss of tooth
structure was noted on buccalsurfaces of teeth #4, 6, 11, 12, 21,22, 28, and 29 and lingual surfacesof #6 through 11 and 22 through27; posterior occlusal surfaces of#12, 19, 21, 28, and 29; and incisaledges of teeth #8, 9, 22, 23, 24, 25,26, and 27. Exostoses were presenton the facial aspect of teeth #23through 26 but no lingual tori werepresent. Periodontal findingsincluded: tissues were inflamed andirritated with the presence ofmoderate-to-heavy plaque andcalculus. Periodontal pocketingranged from 2-7 mm. Purulentexudate was noted on tooth #25MF.Gingival recession of 1-3 mm waspresent on almost half the teeth.There was no mobility.
2. Radiographic ExaminationA panoramic radiograph (Figure 2)and 4 vertical bitewings were takenat the initial hygiene visit. Threemonths later the patient presentedfor periodontal therapy and 14additional periapical radiographswere taken to clarify areas of boneloss (Figure 3). Radiographsrevealed moderate-to-severe hori-zontal bone loss in the posteriorand between teeth #24 and 25.Areas of particular periodontalconcern were teeth #2, 14, 15, 24,and 25. No carious lesions weredetected on pretreatment radi-ographs.
3. Soft Tissue StatusTissues appeared inflamed and irri-tated with the presence ofmoderate-to-heavy plaque andcalculus. A complete six-point perio -dontal probing was performed with7 mm as the greatest pocket depth.
Smith
SY N O P S I S
This article describes treatment of chronic generalized periodontitis
and aphthous ulcers using an Nd:YAG laser adjunctively.
Figure 1: Preoperative view at presentationFigure 2: Panoramic radiograph taken atinitial visit
94
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Out of 27 teeth present, 20 teethexhibited signs of periodontaldisease. Generalized bleeding wasevident and moderate subgingivalcalculus present. Recession of 1-3mm was noted on teeth #7, 8, 9, 10,24, 25, and 26 lingually, and #4, 6,11, 12, 13,15, 18, 19, 21, 22, 28, and31 facially. No mobility waspresent. Class I furcation involve-ments were noted on teeth #2ML,14DL, 15ML, 18B, 19B, and 31B.The initial periodontal probingchart is shown in Figure 4. Oralcancer screening was withinnormal limits.
4. Hard Tissue Status• Occlusion classification was
Angle’s Class II, bilateral withsevere overbite.
• Missing teeth were #1, 16, 17, 20,and 32; #19 had drifted mesially.
• Lower anterior teeth werecrowded.
• Teeth #18 and 19 had significantfractures.
• All teeth were vital except #2,which had been treated endodon-tically, and restored with aprecious metal crown.
• Other restorations included PFMcrown in tooth #5; nonpreciouscrowns in #14, 30, and 31;composite filling in #4; amalgamfillings in #13, 15, 18, 19, 28, and29.
• Loss of cervical tooth structurewas noted on the buccal aspect ofteeth #4, 6, 11, 12, 21, 22, 28, and
29, and on thelingual aspectof #6, 7, 8, 9,10, 11, 22, 23,24, 25, 26, and27.
• Wear facetswere noted onposteriorocclusalsurfaces ofteeth #12, 19, 21, 28, and 29.
• Attrition was noted on the incisaledges of teeth #8, 9, 22, 23, 24,25, 26, and 27 (Figure 5).
• Exostoses were noted faciallyinferior to teeth #23-26.
5. Other TestsTMJ: The patient had a limitedopening of 27 mm with aShimbashi (vertical measurementof occlusion) of 9 mm. There was nopain associated with function, butfatigue was reported.
B. Diagnosis and TreatmentPlan1. DiagnosisProvisional diagnosis includedchronic periodontitis.
The doctor’s final diagnosisstated: Severe generalized chronicperiodontitis with poor prognosis ofteeth #24 and 25; mildly sympto-matic temporomandibular jointdysfunction (TMD); generalizedloss of tooth structure related tothe patient’s occlusal relationshipand function; teeth #18 and 19 had
significant fractures, weakeningthe teeth.
2. Treatment Plan Outlinea. Restorative treatment to include:• Manage possible inflammation of
TMJ during treatment by frequentjaw rest and shorter appointmentsas the patient indicates.
• Restorative treatment to includerebuilding patient’s occlusion orusing an appliance to open thebite and preserve tooth structure.Restore teeth #18 and 19 withcrowns.
Smith
Figure 3: Full-mouth radiographs taken at initial therapy visit, 3months later
Figure 4: Initial periodontal probe chart
Figure 5: Occlusal view of maxillary ante-rior lingual surface of the incisorsshowing wear
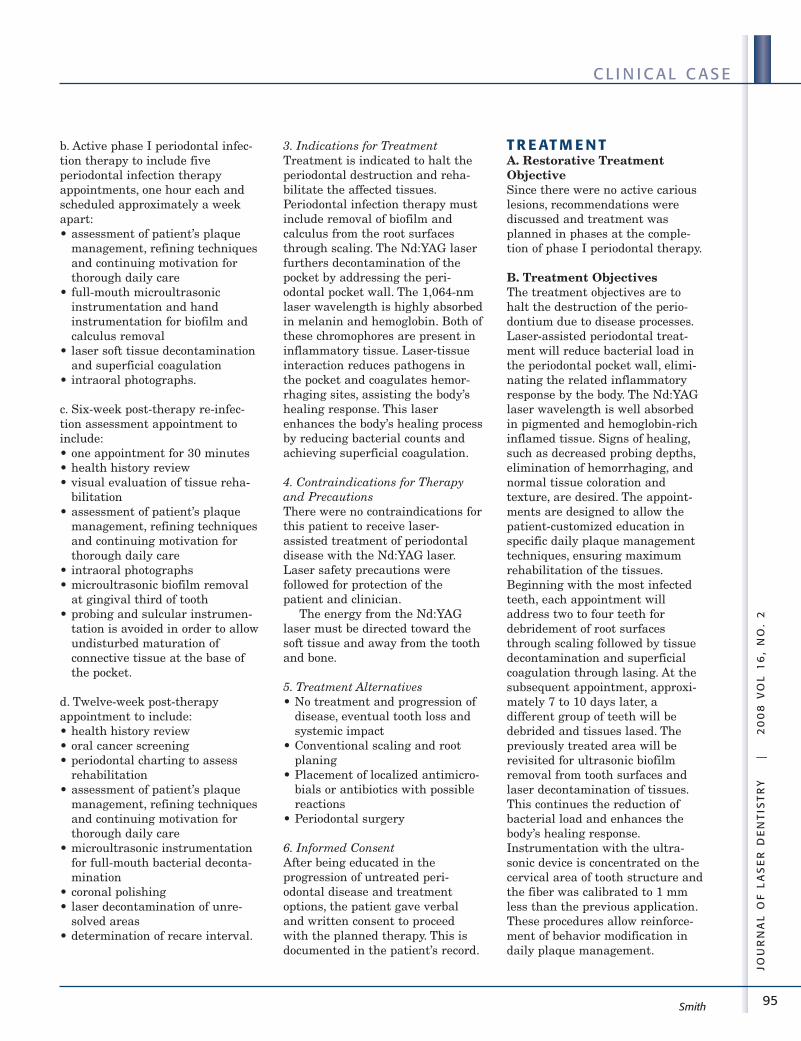
95
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Smith
b. Active phase I periodontal infec-tion therapy to include fiveperiodontal infection therapyappointments, one hour each andscheduled approximately a weekapart: • assessment of patient’s plaque
management, refining techniquesand continuing motivation forthorough daily care
• full-mouth microultrasonicinstrumentation and handinstrumentation for biofilm andcalculus removal
• laser soft tissue decontaminationand superficial coagulation
• intraoral photographs.
c. Six-week post-therapy re-infec-tion assessment appointment toinclude:• one appointment for 30 minutes• health history review• visual evaluation of tissue reha-
bilitation• assessment of patient’s plaque
management, refining techniquesand continuing motivation forthorough daily care
• intraoral photographs• microultrasonic biofilm removal
at gingival third of tooth• probing and sulcular instrumen-
tation is avoided in order to allowundisturbed maturation ofconnective tissue at the base ofthe pocket.
d. Twelve-week post-therapyappointment to include:• health history review• oral cancer screening• periodontal charting to assess
rehabilitation• assessment of patient’s plaque
management, refining techniquesand continuing motivation forthorough daily care
• microultrasonic instrumentationfor full-mouth bacterial deconta-mination
• coronal polishing• laser decontamination of unre-
solved areas• determination of recare interval.
3. Indications for TreatmentTreatment is indicated to halt theperiodontal destruction and reha-bilitate the affected tissues.Periodontal infection therapy mustinclude removal of biofilm andcalculus from the root surfacesthrough scaling. The Nd:YAG laserfurthers decontamination of thepocket by addressing the peri-odontal pocket wall. The 1,064-nmlaser wavelength is highly absorbedin melanin and hemoglobin. Both ofthese chromophores are present ininflammatory tissue. Laser-tissueinteraction reduces pathogens inthe pocket and coagulates hemor-rhaging sites, assisting the body’shealing response. This laserenhances the body’s healing processby reducing bacterial counts andachieving superficial coagulation.
4. Contraindications for Therapyand PrecautionsThere were no contraindications forthis patient to receive laser-assisted treatment of periodontaldisease with the Nd:YAG laser.Laser safety precautions werefollowed for protection of thepatient and clinician.
The energy from the Nd:YAGlaser must be directed toward thesoft tissue and away from the toothand bone.
5. Treatment Alternatives• No treatment and progression of
disease, eventual tooth loss andsystemic impact
• Conventional scaling and rootplaning
• Placement of localized antimicro-bials or antibiotics with possiblereactions
• Periodontal surgery
6. Informed ConsentAfter being educated in theprogression of untreated peri-odontal disease and treatmentoptions, the patient gave verbaland written consent to proceedwith the planned therapy. This isdocumented in the patient’s record.
T R E AT M E N TA. Restorative TreatmentObjectiveSince there were no active cariouslesions, recommendations werediscussed and treatment wasplanned in phases at the comple-tion of phase I periodontal therapy.
B. Treatment ObjectivesThe treatment objectives are tohalt the destruction of the perio -dontium due to disease processes.Laser-assisted periodontal treat-ment will reduce bacterial load inthe periodontal pocket wall, elimi-nating the related inflammatoryresponse by the body. The Nd:YAGlaser wavelength is well absorbedin pigmented and hemoglobin-richinflamed tissue. Signs of healing,such as decreased probing depths,elimination of hemorrhaging, andnormal tissue coloration andtexture, are desired. The appoint-ments are designed to allow thepatient-customized education inspecific daily plaque managementtechniques, ensuring maximumrehabilitation of the tissues.Beginning with the most infectedteeth, each appointment willaddress two to four teeth fordebridement of root surfacesthrough scaling followed by tissuedecontamination and superficialcoagulation through lasing. At thesubsequent appointment, approxi-mately 7 to 10 days later, adifferent group of teeth will bedebrided and tissues lased. Thepreviously treated area will berevisited for ultrasonic biofilmremoval from tooth surfaces andlaser decontamination of tissues.This continues the reduction ofbacterial load and enhances thebody’s healing response.Instrumentation with the ultra-sonic device is concentrated on thecervical area of tooth structure andthe fiber was calibrated to 1 mmless than the previous application.These procedures allow reinforce-ment of behavior modification indaily plaque management.
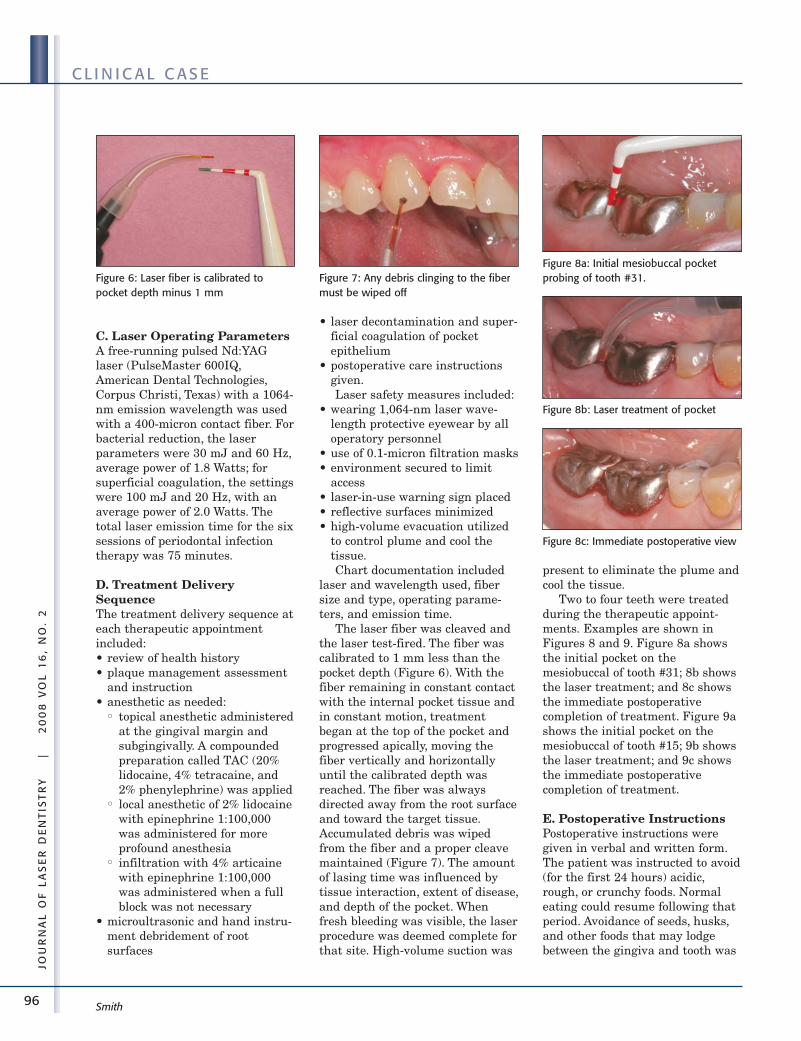
96
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Smith
C. Laser Operating ParametersA free-running pulsed Nd:YAGlaser (PulseMaster 600IQ,American Dental Technologies,Corpus Christi, Texas) with a 1064-nm emission wavelength was usedwith a 400-micron contact fiber. Forbacterial reduction, the laserparameters were 30 mJ and 60 Hz,average power of 1.8 Watts; forsuperficial coagulation, the settingswere 100 mJ and 20 Hz, with anaverage power of 2.0 Watts. Thetotal laser emission time for the sixsessions of periodontal infectiontherapy was 75 minutes.
D. Treatment DeliverySequenceThe treatment delivery sequence ateach therapeutic appointmentincluded:• review of health history• plaque management assessment
and instruction• anesthetic as needed:
•• topical anesthetic administeredat the gingival margin andsubgingivally. A compoundedpreparation called TAC (20%lidocaine, 4% tetracaine, and2% phenylephrine) was applied
•• local anesthetic of 2% lidocainewith epinephrine 1:100,000was administered for moreprofound anesthesia
•• infiltration with 4% articainewith epinephrine 1:100,000was administered when a fullblock was not necessary
• microultrasonic and hand instru-ment debridement of rootsurfaces
• laser decontamination and super-ficial coagulation of pocketepithelium
• postoperative care instructionsgiven.Laser safety measures included:
• wearing 1,064-nm laser wave-length protective eyewear by alloperatory personnel
• use of 0.1-micron filtration masks• environment secured to limit
access• laser-in-use warning sign placed• reflective surfaces minimized• high-volume evacuation utilized
to control plume and cool thetissue.Chart documentation included
laser and wavelength used, fibersize and type, operating parame-ters, and emission time.
The laser fiber was cleaved andthe laser test-fired. The fiber wascalibrated to 1 mm less than thepocket depth (Figure 6). With thefiber remaining in constant contactwith the internal pocket tissue andin constant motion, treatmentbegan at the top of the pocket andprogressed apically, moving thefiber vertically and horizontallyuntil the calibrated depth wasreached. The fiber was alwaysdirected away from the root surfaceand toward the target tissue.Accumulated debris was wipedfrom the fiber and a proper cleavemaintained (Figure 7). The amountof lasing time was influenced bytissue interaction, extent of disease,and depth of the pocket. Whenfresh bleeding was visible, the laserprocedure was deemed complete forthat site. High-volume suction was
present to eliminate the plume andcool the tissue.
Two to four teeth were treatedduring the therapeutic appoint-ments. Examples are shown inFigures 8 and 9. Figure 8a showsthe initial pocket on themesiobuccal of tooth #31; 8b showsthe laser treatment; and 8c showsthe immediate postoperativecompletion of treatment. Figure 9ashows the initial pocket on themesiobuccal of tooth #15; 9b showsthe laser treatment; and 9c showsthe immediate postoperativecompletion of treatment.
E. Postoperative InstructionsPostoperative instructions weregiven in verbal and written form.The patient was instructed to avoid(for the first 24 hours) acidic,rough, or crunchy foods. Normaleating could resume following thatperiod. Avoidance of seeds, husks,and other foods that may lodgebetween the gingiva and tooth was
Figure 6: Laser fiber is calibrated topocket depth minus 1 mm
Figure 7: Any debris clinging to the fibermust be wiped off
Figure 8a: Initial mesiobuccal pocketprobing of tooth #31.
Figure 8b: Laser treatment of pocket
Figure 8c: Immediate postoperative view
97
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Smith
recommended for a week. Thepatient opted to purchase an elec-tric toothbrush. Instructions andtechnique for use were explained.Subgingival flossing and the elec-tric toothbrush were to be avoidedfor several days. All other areaswere to be cleaned as usual. Ifdiscomfort were to occur, thepatient was instructed to use warmsalt water rinses and over-the-counter pain medication. Thepatient was informed that the mostimportant aspect of the therapywas the healing process and mini-mizing plaque at the gingivalmargin was critical in preventingre-infection.
F. ComplicationsThe patient experienced tenderness
the evening following appointmentswhere more instrumentation wasrequired, particularly in the teeth#24-25 area. He also experiencedsensitivity to temperature changesin this area. A 5% neutral sodiumfluoride varnish was applied toexposed root surfaces to preventroot caries and desensitize, and a1.1% neutral sodium fluoride denti-frice was prescribed for daily use.Adequate rest was allowed duringtherapy to minimize issues withthe TMJ and the patient toleratedtreatment well. There were noother complications during or afterthe laser treatments.
G. PrognosisPrognosis is fair to good overall aslong as he conforms to good oralhygiene and recommended intervalsfor professional supportive mainte-nance visits. Continued monitoringof teeth #24 and 25 will be neces-sary. Restorative treatment for teeth#18 and 19 is the next priority intreatment. The patient is undecidedabout an occlusal appliance.
H. Documentation All treatment and related informa-
tion was recorded in the patient’streatment record.
F O L LOW- U P C A R EA. Assessment of TreatmentOutcomesThe patient was assessed at 1week, 6 weeks, 12 weeks, and 6months following active phase-Iperiodontal infection therapy. Thepatient was educated about theimportance of his oral hygiene andencouraged to continue with a thor-ough daily routine.
The one-week examinationrevealed that the tissues werehealing. Plaque managementneeded further refinement.
The six-week post-therapy re-infection assessmentappointment:Patient has improved plaquemanagement and tissues werebecoming healthier. This appoint-ment included:• health history review• visual evaluation of tissue reha-
bilitation• assessment of patient’s plaque
management, refining techniquesand continuing motivation forthorough daily care
• intraoral photographs• microultrasonic biofilm removal
at gingival third of tooth.As mentioned previously,
probing and sulcular instrumenta-tion was avoided in order to allowundisturbed maturation of connec-tive tissue at the base of thepocket. Figures 10a and 10b showthe six-week view of teeth #31 and15, respectively.
The twelve-week post-therapyappointment:Overall, a marked improvement inperiodontal health was seen. Thepatient presented with irritationand flaking of skin at the corner ofthe mouth. Nystatin cream wasprescribed for probable fungalinfection. This appointmentincluded:• health history review
Figure 9a: Initial mesiobuccal pocketprobing of tooth #15 with exudates
Figure 9b: Laser treatment of pocket
Figure 10a: Six-week postoperative viewof tooth #31
Figure 10b: Six-week postoperative viewof tooth #15
Figure 9c: Immediate postoperative view
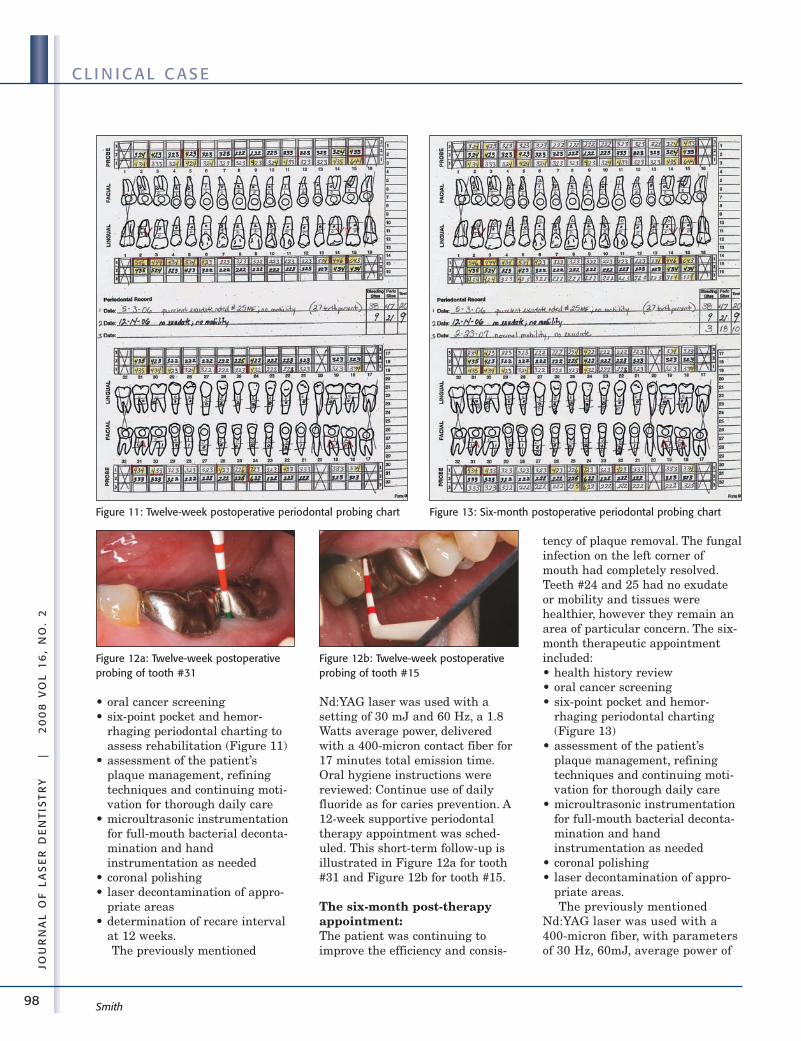
98
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Smith
• oral cancer screening• six-point pocket and hemor-
rhaging periodontal charting toassess rehabilitation (Figure 11)
• assessment of the patient’splaque management, refiningtechniques and continuing moti-vation for thorough daily care
• microultrasonic instrumentationfor full-mouth bacterial deconta-mination and handinstrumentation as needed
• coronal polishing• laser decontamination of appro-
priate areas• determination of recare interval
at 12 weeks.The previously mentioned
Nd:YAG laser was used with asetting of 30 mJ and 60 Hz, a 1.8Watts average power, deliveredwith a 400-micron contact fiber for17 minutes total emission time.Oral hygiene instructions werereviewed: Continue use of dailyfluoride as for caries prevention. A12-week supportive periodontaltherapy appointment was sched-uled. This short-term follow-up isillustrated in Figure 12a for tooth#31 and Figure 12b for tooth #15.
The six-month post-therapyappointment:The patient was continuing toimprove the efficiency and consis-
tency of plaque removal. The fungalinfection on the left corner ofmouth had completely resolved.Teeth #24 and 25 had no exudateor mobility and tissues werehealthier, however they remain anarea of particular concern. The six-month therapeutic appointmentincluded:• health history review• oral cancer screening• six-point pocket and hemor-
rhaging periodontal charting(Figure 13)
• assessment of the patient’splaque management, refiningtechniques and continuing moti-vation for thorough daily care
• microultrasonic instrumentationfor full-mouth bacterial deconta-mination and handinstrumentation as needed
• coronal polishing• laser decontamination of appro-
priate areas.The previously mentioned
Nd:YAG laser was used with a400-micron fiber, with parametersof 30 Hz, 60mJ, average power of
Figure 11: Twelve-week postoperative periodontal probing chart
Figure 12a: Twelve-week postoperativeprobing of tooth #31
Figure 12b: Twelve-week postoperativeprobing of tooth #15
Figure 13: Six-month postoperative periodontal probing chart
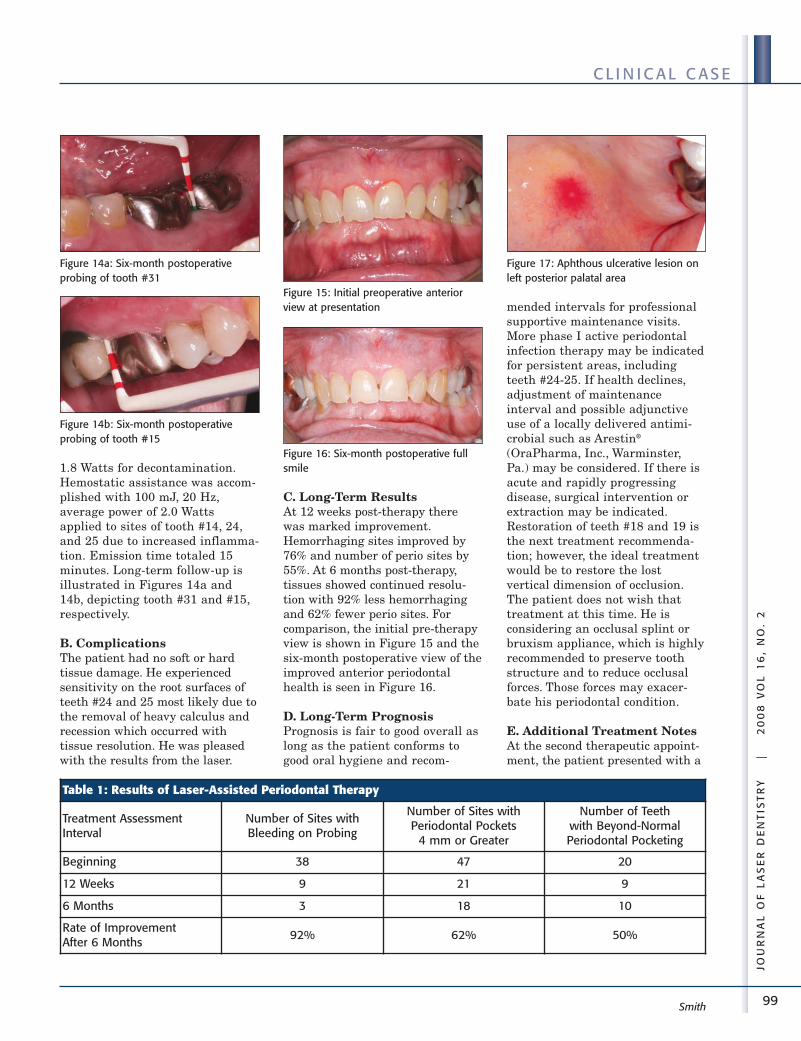
99
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Smith
1.8 Watts for decontamination.Hemostatic assistance was accom-plished with 100 mJ, 20 Hz,average power of 2.0 Wattsapplied to sites of tooth #14, 24,and 25 due to increased inflamma-tion. Emission time totaled 15minutes. Long-term follow-up isillustrated in Figures 14a and14b, depicting tooth #31 and #15,respectively.
B. ComplicationsThe patient had no soft or hardtissue damage. He experiencedsensitivity on the root surfaces ofteeth #24 and 25 most likely due tothe removal of heavy calculus andrecession which occurred withtissue resolution. He was pleasedwith the results from the laser.
C. Long-Term ResultsAt 12 weeks post-therapy therewas marked improvement.Hemorrhaging sites improved by76% and number of perio sites by55%. At 6 months post-therapy,tissues showed continued resolu-tion with 92% less hemorrhagingand 62% fewer perio sites. Forcomparison, the initial pre-therapyview is shown in Figure 15 and thesix-month postoperative view of theimproved anterior periodontalhealth is seen in Figure 16.
D. Long-Term PrognosisPrognosis is fair to good overall aslong as the patient conforms togood oral hygiene and recom-
mended intervals for professionalsupportive maintenance visits.More phase I active periodontalinfection therapy may be indicatedfor persistent areas, includingteeth #24-25. If health declines,adjustment of maintenanceinterval and possible adjunctiveuse of a locally delivered antimi-crobial such as Arestin®
(OraPharma, Inc., Warminster,Pa.) may be considered. If there isacute and rapidly progressingdisease, surgical intervention orextraction may be indicated.Restoration of teeth #18 and 19 isthe next treatment recommenda-tion; however, the ideal treatmentwould be to restore the lostvertical dimension of occlusion.The patient does not wish thattreatment at this time. He isconsidering an occlusal splint orbruxism appliance, which is highlyrecommended to preserve toothstructure and to reduce occlusalforces. Those forces may exacer-bate his periodontal condition.
E. Additional Treatment NotesAt the second therapeutic appoint-ment, the patient presented with a
Figure 14a: Six-month postoperativeprobing of tooth #31
Figure 14b: Six-month postoperativeprobing of tooth #15
Figure 15: Initial preoperative anteriorview at presentation
Figure 16: Six-month postoperative fullsmile
Figure 17: Aphthous ulcerative lesion onleft posterior palatal area
Table 1: Results of Laser-Assisted Periodontal Therapy
Treatment AssessmentInterval
Number of Sites withBleeding on Probing
Number of Sites withPeriodontal Pockets
4 mm or Greater
Number of Teeth with Beyond-NormalPeriodontal Pocketing
Beginning 38 47 20
12 Weeks 9 21 9
6 Months 3 18 10
Rate of Improvement After 6 Months
92% 62% 50%
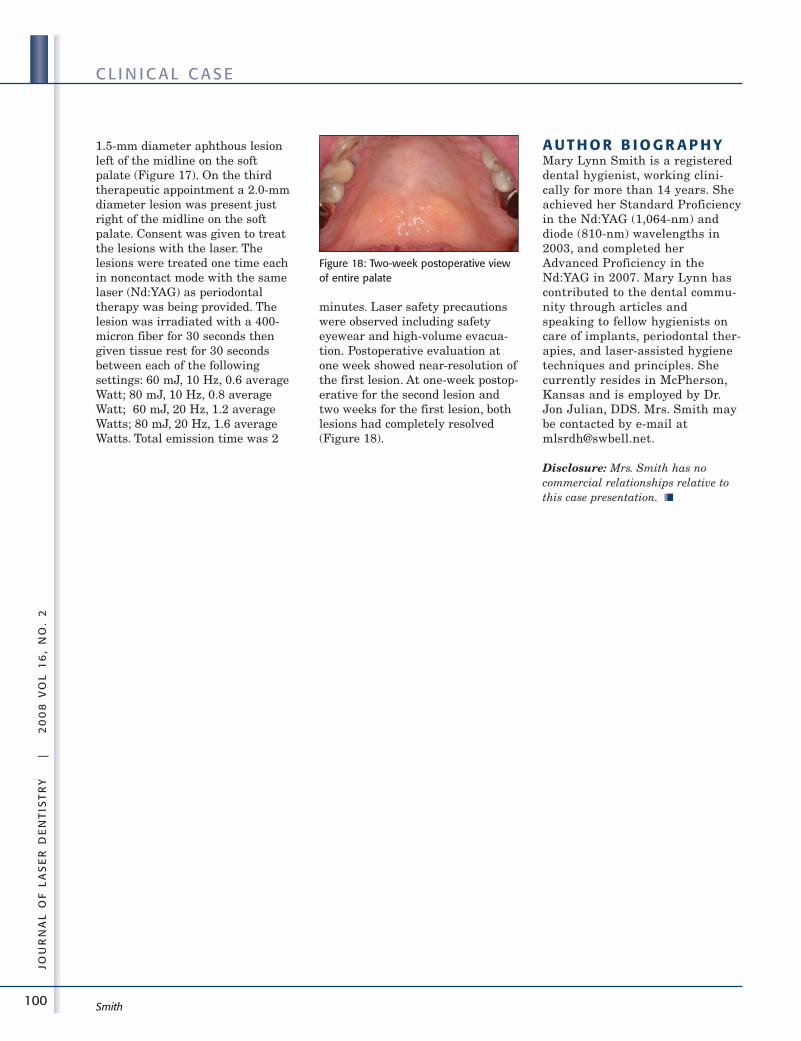
100
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
C L I N I C A L C A S E
Smith
1.5-mm diameter aphthous lesionleft of the midline on the softpalate (Figure 17). On the thirdtherapeutic appointment a 2.0-mmdiameter lesion was present justright of the midline on the softpalate. Consent was given to treatthe lesions with the laser. Thelesions were treated one time eachin noncontact mode with the samelaser (Nd:YAG) as periodontaltherapy was being provided. Thelesion was irradiated with a 400-micron fiber for 30 seconds thengiven tissue rest for 30 secondsbetween each of the followingsettings: 60 mJ, 10 Hz, 0.6 averageWatt; 80 mJ, 10 Hz, 0.8 averageWatt; 60 mJ, 20 Hz, 1.2 averageWatts; 80 mJ, 20 Hz, 1.6 averageWatts. Total emission time was 2
minutes. Laser safety precautionswere observed including safetyeyewear and high-volume evacua-tion. Postoperative evaluation atone week showed near-resolution ofthe first lesion. At one-week postop-erative for the second lesion andtwo weeks for the first lesion, bothlesions had completely resolved(Figure 18).
A U T H O R B I O G R A P H YMary Lynn Smith is a registereddental hygienist, working clini-cally for more than 14 years. Sheachieved her Standard Proficiencyin the Nd:YAG (1,064-nm) anddiode (810-nm) wavelengths in2003, and completed herAdvanced Proficiency in theNd:YAG in 2007. Mary Lynn hascontributed to the dental commu-nity through articles andspeaking to fellow hygienists oncare of implants, periodontal ther-apies, and laser-assisted hygienetechniques and principles. Shecurrently resides in McPherson,Kansas and is employed by Dr.Jon Julian, DDS. Mrs. Smith maybe contacted by e-mail [email protected].
Disclosure: Mrs. Smith has nocommercial relationships relative tothis case presentation. ■■
Figure 18: Two-week postoperative viewof entire palate
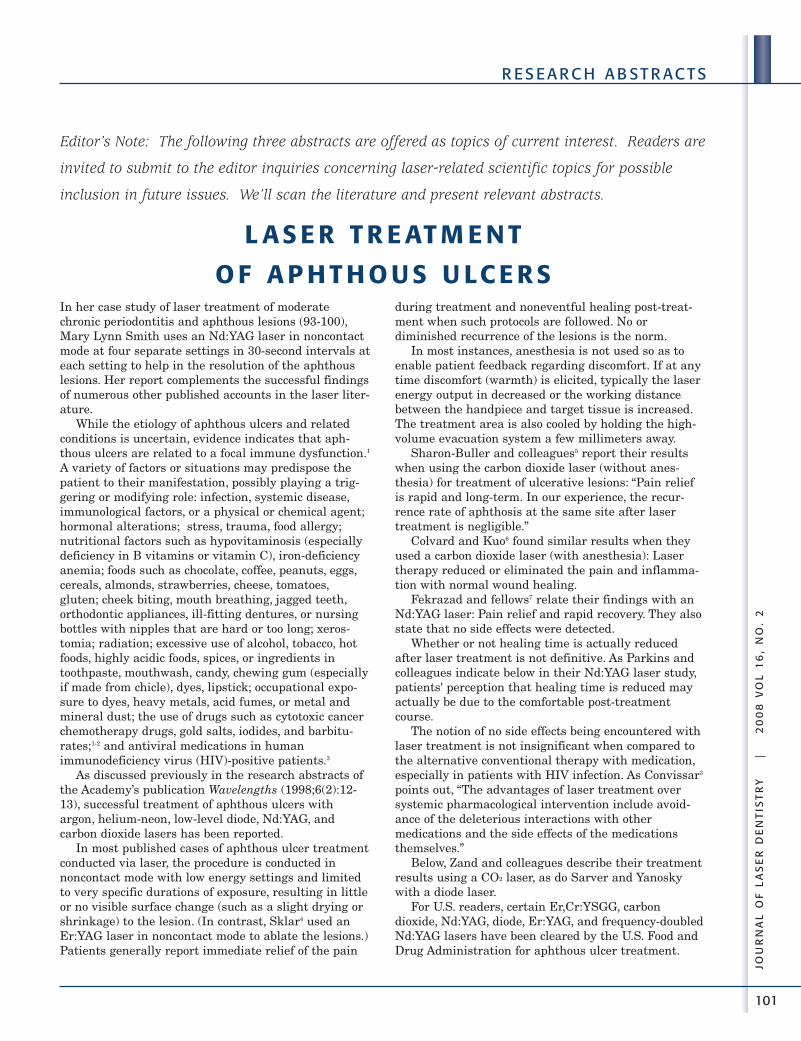
101
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
R E S E A R C H A B ST R AC T S
In her case study of laser treatment of moderatechronic periodontitis and aphthous lesions (93-100),Mary Lynn Smith uses an Nd:YAG laser in noncontactmode at four separate settings in 30-second intervals ateach setting to help in the resolution of the aphthouslesions. Her report complements the successful findingsof numerous other published accounts in the laser liter-ature.
While the etiology of aphthous ulcers and relatedconditions is uncertain, evidence indicates that aph -thous ulcers are related to a focal immune dysfunction.1
A variety of factors or situations may predispose thepatient to their manifestation, possibly playing a trig-gering or modifying role: infection, systemic disease,immunological factors, or a physical or chemical agent;hormonal alterations; stress, trauma, food allergy;nutritional factors such as hypovitaminosis (especiallydeficiency in B vitamins or vitamin C), iron-deficiencyanemia; foods such as chocolate, coffee, peanuts, eggs,cereals, almonds, strawberries, cheese, tomatoes,gluten; cheek biting, mouth breathing, jagged teeth,orthodontic appliances, ill-fitting dentures, or nursingbottles with nipples that are hard or too long; xeros-tomia; radiation; excessive use of alcohol, tobacco, hotfoods, highly acidic foods, spices, or ingredients intoothpaste, mouthwash, candy, chewing gum (especiallyif made from chicle), dyes, lipstick; occupational expo-sure to dyes, heavy metals, acid fumes, or metal andmineral dust; the use of drugs such as cytotoxic cancerchemotherapy drugs, gold salts, iodides, and barbitu-rates;1-2 and antiviral medications in humanimmunodeficiency virus (HIV)-positive patients.3
As discussed previously in the research abstracts ofthe Academy’s publication Wavelengths (1998;6(2):12-13), successful treatment of aphthous ulcers withargon, helium-neon, low-level diode, Nd:YAG, andcarbon dioxide lasers has been reported.
In most published cases of aphthous ulcer treatmentconducted via laser, the procedure is conducted innoncontact mode with low energy settings and limitedto very specific durations of exposure, resulting in littleor no visible surface change (such as a slight drying orshrinkage) to the lesion. (In contrast, Sklar4 used anEr:YAG laser in noncontact mode to ablate the lesions.)Patients generally report immediate relief of the pain
during treatment and noneventful healing post-treat-ment when such protocols are followed. No ordiminished recurrence of the lesions is the norm.
In most instances, anesthesia is not used so as toenable patient feedback regarding discomfort. If at anytime discomfort (warmth) is elicited, typically the laserenergy output in decreased or the working distancebetween the handpiece and target tissue is increased.The treatment area is also cooled by holding the high-volume evacuation system a few millimeters away.
Sharon-Buller and colleagues5 report their resultswhen using the carbon dioxide laser (without anes-thesia) for treatment of ulcerative lesions: “Pain reliefis rapid and long-term. In our experience, the recur-rence rate of aphthosis at the same site after lasertreatment is negligible.”
Colvard and Kuo6 found similar results when theyused a carbon dioxide laser (with anesthesia): Lasertherapy reduced or eliminated the pain and inflamma-tion with normal wound healing.
Fekrazad and fellows7 relate their findings with anNd:YAG laser: Pain relief and rapid recovery. They alsostate that no side effects were detected.
Whether or not healing time is actually reducedafter laser treatment is not definitive. As Parkins andcolleagues indicate below in their Nd:YAG laser study,patients' perception that healing time is reduced mayactually be due to the comfortable post-treatmentcourse.
The notion of no side effects being encountered withlaser treatment is not insignificant when compared tothe alternative conventional therapy with medication,especially in patients with HIV infection. As Convissar3
points out, “The advantages of laser treatment oversystemic pharmacological intervention include avoid-ance of the deleterious interactions with othermedications and the side effects of the medicationsthemselves.”
Below, Zand and colleagues describe their treatmentresults using a CO2 laser, as do Sarver and Yanoskywith a diode laser.
For U.S. readers, certain Er,Cr:YSGG, carbondioxide, Nd:YAG, diode, Er:YAG, and frequency-doubledNd:YAG lasers have been cleared by the U.S. Food andDrug Administration for aphthous ulcer treatment.
Editor’s Note: The following three abstracts are offered as topics of current interest. Readers are
invited to submit to the editor inquiries concerning laser-related scientific topics for possible
inclusion in future issues. We’ll scan the literature and present relevant abstracts.
L AS E R T R E AT M E N T
O F A P H T H O U S U LC E R S

102
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
R E S E A R C H A B ST R AC T S
As always, clinicians are advised to review thespecific indications for use of their lasers and to reviewtheir operator manuals for guidance on operatingparameters before attempting similar techniques ontheir patients.
R E F E R E N C ES1. Regezi JA, Sciubba JJ, Jordan RCK. Oral pathology:
Clinical pathologic correlations. 5th ed. St. Louis, Mo.:Saunders, 2008:35-39, 64.
2. Beers MH, Porter RS, Jones TV, Kaplan JL, Berkwits M,editors. The Merck manual of diagnosis and therapy. 18thed. Whitehouse Station, N.J.: Merck Research Laboratories,2006:815-818.
3. Convissar RA. Laser palliation of oral manifestations ofhuman immunodeficiency virus infection. J Am Dent Assoc2002;133(5):591-598; quiz 624-625.
4. Sklar TA. Er:YAG laser-assisted restorative dentistry andtreatment of aphthous ulcers: Case 2. J Acad Laser Dent2005;13(2):31-34.
5. Sharon-Buller A, Sela M. CO2-laser treatment of ulcerativelesions. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2004;97(3):332-334.
6. Colvard M, Kuo P. Managing aphthous ulcers: Laser treat-ment applied. J Am Dent Assoc 1991;122(6):51-53.
7. Fekrazad R, Jafari S, Kalhori K, Gholamie GA. Evaluation ofthe effects of pulsed Nd:YAG laser on RAU [RecurrentAphthous Ulcer]. Z Laser Zahnheilkd 2006;3(2):116, abstract.
Previously herpes labialis and recurrent aphthousulcers have not been successfully treated. A prelimi-nary study with a pulsed Nd:YAG laser evaluated theresults with a protocol of four-minute noncontact expo-sures for both types of lesions – 8 patients withaphthous ulcers and 14 with herpes labialis. … Mostpatients experienced relief of symptoms. Some milddiscomfort occurred during treatment. The mostnotable sensation was of warmth. The cooling action ofhigh-velocity suction was helpful in reducing thepatient’s response. Continuous motion of the laser fiberwas helpful. A momentary pause as a rotationalpattern is reversed should be avoided. Most patientstolerated the treatment well and indicated that thesensations were minor compared to the discomfort ofthe lesions. In no case was local anesthesia required.Although no visible plume was produced during lasertreatment, it could be a cause for concern. Especiallywith a herpetic lesion, viral particles could be presentwithin the plume. A mask of small size is advised at alltimes. Future research culturing the plume as it iswithdrawn in the suction stream would be informative.Since no tissue alteration is visible there may be lessliberation of the virus than would occur with an inva-sive technique. The progress of herpes lesion was
halted and aphthous lesions became desensitized.Aphthous ulcers can be treated with an Nd:YAG laserto reduce or eliminate the discomfort. Several subjectsthat were treated during the early prodromal stage didreport that the lesion was aborted. Ulcer formationusually was averted. When the lesion had progressed toan ulcerated state before treatment, the desensitizationof exposed nerve endings was probably responsible forthe dramatic improvement. The lasting duration of thepain elimination, usually until healing was complete,was judged a favorable outcome. Healing time is prob-ably not appreciably altered. Patients are morecomfortable and notice the area less. Herpes labialistreated with an Nd:YAG laser takes an altered diseasecourse. Most patients achieve initial comfort. Earlytreatment during the prodromal period usuallyreverses the development and aborts ulcer formation.Satellite vesicles and acute discomfort do not evolve.Recurrences are reduced for most patients; and duringthe experimental period a significant number did notexperience any additional herpes lesions. With thosewho eventually did have another lesion it tended to beat another location, and less severe. ■■
Copyright 1999 The Society of Photo-Optical InstrumentationEngineers
N D : YAG L AS E R T R E AT M E N T O F H E R P ES A N D A P H T H O U S U LC E R S : A P R E L I M I N A RY ST U DY
Frederick M. Parkins, Thomas J. O’Toole, John M. YanceyUniversity of Louisville, School of Dentistry, Louisville, Kentucky
Laser Florence ’99: A Window on the Laser Medicine World, October 28-31, 1999, Florence, Italy
Leonardo Longo, Alfons G. Hofstetter, Mihail-Lucian Pascu, and Wilhelm R.A. Waidelich, editors
Bellingham, Wash.: SPIE – The International Society for Optical Engineering, Proceedings of SPIE Vol. 4166, 1999:253-258

103
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
R E S E A R C H A B ST R AC T S
One of the clinical orthodontist’s biggest occupationalstress factors is the constant pressure from patients andtheir parents to finish treatment. Many predictablefactors must work together for treatment to run onschedule, including patient cooperation and timelinessof appointments. But unanticipated impediments, suchas tooth eruption problems and certain soft tissue char-acteristics, can prolong treatment. This purpose of thearticle is to describe how we use a diode soft tissue laserto solve many clinical and cosmetic problems. … One ofthe most uncomfortable experiences for orthodonticpatients is the formation of aphthous ulcers. In the past,we have offered salt water rinses, various anestheticand palliative mouth rinses, and, in particularly
persistent and painful lesions, a prescription rinse oftetracycline and topical anesthetic. Some of these solu-tions help to varying degrees, but often they only makethe situation tolerable. The diode laser offers a potentialsolution. The recommended technique involves usingthe laser on a very low-wattage setting, out of contactwith the lesion (a distance of 1-2 mm), visualizing a spotlarge enough to cover the entire lesion. The laser is acti-vated for 30 seconds, and in our experience, the patientreports an immediate elimination of pain. The aphthousulcer will generally heal and disappear approximately 1day after laser treatment, compared with 10 to 14 daysfor an untreated lesion to heal. ■■
Copyright 2005 The American Association of Orthodontists
P R I N C I P L ES O F CO S M ET I C D E N T I ST RY I N O R T H O D O N T I CS : PA R T 3 . L AS E R T R E AT M E N TS F O R TO OT H E R U P T I O N A N D SO F T T I SS U E P R O B L E M S
David M. Sarver
Mark YanoskyVestavia Hills, Alabama
Am J Orthod Dentofacial Orthop 2005;127(2):262-264
This randomized controlled clinical trial was designedto evaluate the efficacy of single-session, nonthermal,carbon dioxide (CO2) laser irradiation in relieving thepain of minor recurrent aphthous stomatitis (miRAS)as a prototype of painful oral ulcers. Fifteen patients,each with two discrete aphthous ulcers, were included.One of the ulcers was randomly allocated to be treatedwith CO2 laser (1 W of power in de-focused continuousmode) and the other one served as a placebo. Beforelaser irradiation, a layer of transparent, non-anestheticgel was placed on both the laser lesions and the placebolesions. The patients were requested to grade their pain
on a visual analog scale up to 96 h postoperatively. Thereduction in pain scores was significantly greater in thelaser group than in the placebo group. The procedureitself was not painful, so anesthesia was not required.Powermetry revealed the CO2 laser power to be 2-5 mWafter passing through the gel, which caused no signifi-cant temperature rise or any visual effect of damage tothe oral mucosa. Our results showed that a low-inten-sity, nonthermal, single-session of CO2 laser irradiationreduced pain in miRAS immediately and dramatically,with no visible side effects. ■■
Copyright 2008 Springer-Verlag London Ltd
R E L I E V I N G PA I N I N M I N O R A P H T H O U S STO M AT I T I S BY A S I N G L E S ESS I O NO F N O N -T H E R M A L C A R B O N D I OX I D E L AS E R I R R A D I AT I O N
Nasrin Zand,1 Leila Ataie-Fashtami,1 Gholamreza Esmaeeli Djavid,1 Mohsen Fateh,1
Mohammad-Reza Alinaghizadeh,2 Seyyed-Mostafa Fatemi,1 Fateme Arbarbi-Kalati3
1Iranian Center for Medial Laser (ICML), Academic Center for Education, Culture and Research (ACECR), Tehran, Iran
2Research Center of Science and Technology in Medicine (RCSTIM), Medical Sciences/University of Tehran, Tehran, Iran
3Tabriz University of Medical Sciences, Tabriz, Iran
Lasers Med Sci 2008;DOI 10.1007/s10103-008-0555-1
J O U R N A L O F L AS E R D E N T I ST RY
Continuing Education Program
The Journal of Laser Dentistry’sContinuing Dental EducationProgram offers readers an opportu-nity to earn one CE self-instructionalcredit for each of three articles inthis issue. Read the specified articlesand then select the most correctanswer to each of the questions. Ifyou correctly answer 7 of the 10questions on each test (for a score of70%), you earn one credit hour foreach test. Answer forms must becompleted as directed in the instruc-tions; otherwise, they will not beprocessed.
This program is developed byrepresentatives of the Academy ofLaser Dentistry’s Science andResearch committee and is providedas a benefit to ALD members at noadditional charge. Nonmembers are
also eligible to participate for a $20administrative fee per issue.Answers to this exercise will bepublished in a future issue.
Please photocopy andcomplete the registration formas well as the answer sheet andevaluation form on pages 108-109for each test and mail them (alongwith the $20 administrative fee if youare not an ALD member) to:
The Journal of Laser DentistryDepartment of ContinuingEducationP.O. Box 8667Coral Springs, FL 33075
Payment may be by check drawnon a U.S. bank, money order, or VISA
or MasterCard. Please keep a copy ofyour answers for your records.
Your test is graded by represen-tatives of the Academy of LaserDentistry, an ADA CERP recog-nized provider.
You will be notified by mail ofyour test score(s) and the number ofcredits awarded. You must thenforward the information to your statedental board or agency for licensurepurposes. Individuals who score lessthan 70% will receive a letter.
Answers to these tests are dueon or before December 31, 2008.
Please call the Academy of LaserDentistry (954) 346-3776 if you haveany questions about this program. ■■
104
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
CO N T I N U I N G E D U C AT I O N
105
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
CO N T I N U I N G E D U C AT I O N
Educational ObjectivesUpon successful completion of
this module, you will be able to:• Describe the fundamental char-
acteristics of the erbium lasers asused in dentistry.
• Specify 10 guidelines for maxi-mizing successful clinicalrestorative dentistry utilizing anerbium laser.
• Identify the rationale for usingerbium lasers for the effectiveablation of tooth structure.
• Describe typical treatment plansand clinical protocols involved inthe use of erbium lasers inrestorative dentistry.
• Evaluate the expected successfultreatment outcomes in clinicalcases where erbium lasers areused in restorative dentistry.
Test Questions1. The use of laser energy in the
ablation of dental hard tissue isan example of:a. photochemical interactionb. photothermal interactionc. photobiomodulationd. photogenic interaction
2. Several factors contribute to theefficient erbium laser ablation ofdental hard tissue. Among theseare the:a. laser’s delivery systemb. power density at the ablation
sitec. type of anesthesia used on
the patientd. amount of preconditioning of
the laser tip
3. The principal laser wavelengthsused in tooth preparation areEr:YAG and Er,Cr:YSGG. Theirrespective wavelengths are:a. 2,100 nm and 2,780 nmb. 2,100 nm and 2,940 nmc. 2,780 nm and 2,940 nmd. 2,940 nm and 9,600 nm
4. The erbium laser wavelengthshave a:a. high absorption by waterb. low absorption by waterc. very high absorption by
hydroxyapatited. very low absorption by
collagen
5. The surface of dentin after expo-sure to either Er:YAG orEr,Cr:YSGG laser irradiationhas the following characteristics:a. a smear layer and closed
tubulesb. a smear layer and open tubulesc. absence of a smear layerd. presence of carbonization
6. A co-axial water spray duringerbium laser preparation ofenamel and dentin is necessarybecause the spray:a. serves to aim the laser beam
at the targetb. cools the laser tipc. aids in desensitizing the
tooth structured. helps to disperse debris and
ablation products
7. Erbium laser irradiation ofenamel and dentin results in amicro-cavitated surface. Thissurface:a. should be desensitized to
avoid pulpal damageb. is ideal for bonding composite
resinc. requires additional acid-etch
techniques to minimize earlymarginal breakdown of thecomposite restoration
d. should be protected with acavity liner prior to restoration
8. Each of the following is a safetyconsideration when usingerbium laser wavelengthsEXCEPT one. Which one is thisEXCEPTION?
a. wavelength- and device-specific protection glasses forthe doctor, the assistant, andpatient to prevent eyedamage
b. appropriate face-masks toavoid plume aspiration
c. high-speed evacuation ofplume and debris to removepotentially harmful combus-tion byproducts
d. encasement of the laser tip ina wavelength-specific shieldto minimize unwanted beamdiversion
9. Which of the following state-ments is true? Erbium laserenergy:a. has greater absorption in
demineralized tooth structurethan in healthy tooth struc-ture
b. is so efficiently absorbed thatno debris accumulates in adeep preparation
c. has greater absorption inhealthy tooth structure thanin demineralized tooth struc-ture
d. does not cause any thermalrise in the target tissue
10. Studies of the pulpal tempera-ture rise when using erbiumlasers confirm the following:a. temperature rise is rapid
with each pulse and careshould be taken to avoiddamage
b. pulpal temperature rise iswithin 5 degrees Celsiusabove normal
c. pulpal temperature rise isapproximately the same aswith an air turbine
d. erbium laser wavelengthsinduce photobiomodulationwhich keeps the temperaturerise within normal limits
AC A D E MY O F L AS E R D E N T I ST RY • S E L F - I N ST R U C T I O N P R O G R A M N O . 16 21Subject Code: 250
Clinical Considerations for the Use of Er:YAG Lasers in Restorative DentistryGiuseppe Iaria, Dr. Prof. Med. Dent., Steven P.A. Parker, BDS, LDS RCS, MGGDP
106
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
CO N T I N U I N G E D U C AT I O N
Educational ObjectivesUpon successful completion of
this module, you will be able to:• State the definition and etiology
of peri-implantitis.• Describe the various alternatives
for treatment of peri-implantitis.• Identify the rationale for using
an Er:YAG laser for treatment ofperi-implantitis.
• Specify the treatment protocol forand expected successful result ofEr:YAG laser treatment of peri-implantitis.
Test Questions1. Which of the following state-
ments is true? Peri-implantitis:a. manifests as an inflammation
of the structures surroundingan implant fixture
b. is a disease of soft tissuedestruction only
c. has clinical signs similar to acarious lesion
d. cannot be treated with a laser
2. One of the major factorscontributing to peri-implantitisis the:a. design and shape of the
implant fixtureb. specific tooth that is being
replaced by the implantc. amount of bacterial exposure
to the implantd. length of time that the
implant has been allowed toosseo-integrate
3. The development of peri-implan-titis can occur because of:a. the quantity of bone
surrounding the area wherethe implant is to be placed
b. the initial depth of theosteotomy
c. the thermal trauma to theperiodontium during theosteotomy
d. a postoperative complication
4. Clinical signs of peri-implantitisinclude:a. marginal discrepancy of the
restorationb. bleeding or purulence from
the gingival tissuec. loosening of the restoration
from the abutmentd. fracture of the mechanical
connection between therestoration and the abutment
5. Which of the following is a ther-apeutic treatment ofperi-implantitis?a. removal of the implant
fixture and restorationb. occlusal adjustment of the
restorationc. removal of the granulation
tissue with plastic curettesd. supragingival prophylaxis
with pumice
6. The Er:YAG laser can be usedfor the treatment of peri-implan-titis because this device:a. is highly absorbed by the
metallic surface of theimplant fixture
b. can reshape the body of theimplant fixture
c. produces very high tempera-tures in the osseous tissue
d. can vaporize the existinginflammatory granulationtissue
7. The Er:YAG laser can be usedfor dental osseous surgicalprocedures because it:a. instantly provides coagula-
tion of the osseous tissueb. will remove only healthy
osseous tissue and not theinflammatory material
c. is effective in removingnecrotic and healthy osseoustissue
d. will regenerate neededosseous tissue
8. The Er:YAG laser can be useddirectly on the implant surfacebecause it:a. has no damaging effect on the
implant screw areas at lowenergy settings
b. can be used to remove someof the screw threads
c. will recrystallize the metallicsurface of the implant toharden it
d. will not disturb the biofilmthat adheres to the implant
9. According to the peri-implantitistreatment plan described in thearticle, the Er:YAG laser will beused for:a. carving the occlusal surface of
the implant restorationb. making a pilot hole for the
osteotomyc. preparing the donor gingival
graft sited. ablating the soft and hard
tissue in the periodontal defect
10. According to the peri-implan-titis treatment sequencedescribed in this article:a. a free gingival graft was
placed over ablated soft tissueb. a xenograft bone substitute
material was placed into thecleaned defect
c. the soft granulation tissuewas removed with handinstruments
d. the implant fixture wasremoved
AC A D E MY O F L AS E R D E N T I ST RY • S E L F - I N ST R U C T I O N P R O G R A M N O . 16 22Subject Code: 690
Peri-Implantitis Therapy with an Er:YAG LaserAvi Reyhanian, DDS, and Donald J. Coluzzi, DDS
107
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
CO N T I N U I N G E D U C AT I O N
Educational ObjectivesUpon successful completion of
this module, you will be able to:• State the definition and clinical
rationale for performing a pulpo-tomy on pediatric teeth.
• Describe the protocol for the useof an Er:YAG laser in performinga pulpotomy on pediatric teeth.
• Assess the expected long-termtreatment outcomes in clinicalcases where an Er:YAG laser isused to perform pulpotomies.
Test Questions1. Lasers are an effective alternative
for treating pulps in pediatricteeth without the need to:a. use local anestheticsb. use tooth isolationc. introduce chemicalsd. sedate the patient
2. A pulpotomy is defined as:a. the removal of the coronal
pulp of a toothb. the removal of very deep
dentinal cariesc. a root canal procedure for
pulp tissue that is irre-versibly infected or necroticdue to caries or trauma
d. placement of calciumhydroxide paste on thehealthy dentin
3. A concern when using formocre-osol for pulpotomy treatment ofprimary teeth is that:a. formocreosol may be absorbed
and distributed throughoutthe child’s body withinminutes of its use at thepulpotomy site
b. the child may have extremepain immediately after thetooth is treated
c. the child may complain of aburning sensation after thetooth is treated
d. formocreosol may get on anddiscolor the child’s skin if thechild moves
4. When a laser is utilized toperform a pulpotomy, which ofthe following statementsapplies?a. the laser should not be used
on children under the age ofone year
b. the laser should not be usedon permanent teeth
c. the laser treatment’s successis similar to that achievedwith chemical pulp therapy
d. a carbon dioxide laser is thepreferred wavelength for alaser pulp treatment
5. Which of the following is true forEr:YAG laser pulpotomy treat-ment? The laser:a. should be used with the tip
placed 5 mm from the pulpchamber
b. can be utilized for a pulpo-tomy as an alternative toelectrosurgical therapy
c. is always used to removetooth structure for access tothe pulp chamber
d. is always used without anylocal anesthetic
6. When the Er:YAG laser is usedfor pulp therapy, which of thefollowing applies?a. only the child patient
requires laser safety glassesb. everyone within the operating
area is required to use lasersafety glasses
c. no one in the operating arearequires laser safety glasses,since the Er:YAG laser isharmless to the eyes
d. only the dentist is required touse laser glasses since thechild’s mouth is so small the
laser beam stays within thechild’s oral cavity
7. A successful pulpotomy on aprimary tooth should last:a. one yearb. five yearsc. ten yearsd. until the permanent tooth
normally erupts
8. As indicated in the publishedcase study, successful pulpotomytherapy using the Er:YAG laserrequires a power setting ofapproximately:a. 4 Wattsb. 6 Wattsc. 0.75 Wattd. 1.65 Watts
9. Which of following is requiredwhen using the Er:YAG laser fora pulpotomy on a pediatricpatient?a. high-volume evacuationb. premedication for the patientc. use of loupes or a microscoped. presence of the patient’s
parent in the operatory
10. The Er:YAG laser can be usedto treat:a. only posterior primary and
permanent teethb. only anterior primary teethc. only vital teethd. both vital and nonvital
primary teeth
AC A D E MY O F L AS E R D E N T I ST RY • S E L F - I N ST R U C T I O N P R O G R A M N O . 16 23Subject Code: 430
Use of an Er:YAG Laser for Pulpotomies in Vital and Nonvital Primary TeethLawrence Kotlow, DDS
Place an X in the box correspon-ding to the answer you believe ismost correct.
A B C D
1. ❑ ❑ ❑ ❑
2. ❑ ❑ ❑ ❑
3. ❑ ❑ ❑ ❑
4. ❑ ❑ ❑ ❑
5. ❑ ❑ ❑ ❑
6. ❑ ❑ ❑ ❑
7. ❑ ❑ ❑ ❑
8. ❑ ❑ ❑ ❑
9. ❑ ❑ ❑ ❑
10. ❑ ❑ ❑ ❑
Program Evaluation — Test 1621Please evaluate this article.
Poor = 1 to Excellent = 5
Clarity of objectives _____
Usefulness of content _____
Benefit to your clinical practice _____
Quality of manuscript _____
Usefulness of references _____
Quality of illustrations _____
Relevance of illustrations _____
Clarity of questions _____
Article presented newinformation _____
Program achieved itseducational objectives _____
How many minutes did ittake you to completethe test? _____
Please list future CE topic prefer-ences:
108
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
CO N T I N U I N G E D U C AT I O N
A N S W E R S H E ET F O R T EST 16 21Clinical Considerations for the Use of Er:YAG Lasers in Restorative Dentistry
Giuseppe Iaria, Dr. Prof. Med. Dent., Steven P.A. Parker, BDS, LDS RCS, MGGDPSubject Code: 250
CO N T I N U I N G E D U C AT I O N C R E D I T R EG I ST R AT I O N F O R M
Please print or type clearly. The certificate will be issued from the information given.
First Name Initial Last Name
Degree Social Security Number
Street Address Suite
City State or Province Postal Code
Daytime Telephone Number with Area Code Fax Number with Area Code
E-mail Address
Nonmembers only: I wish to pay the $20 administrative fee by the following method:❑ Check #__________________ ❑ VISA ❑ MasterCard
Credit Card # Expiration Date
Name on Card Signature
109
JOU
RN
AL
OF
LA
SE
R D
EN
TIS
TR
Y
|
2
00
8 V
OL
16
, N
O.
2
CO N T I N U I N G E D U C AT I O N
Place an X in the box correspon-ding to the answer you believe ismost correct.
A B C D
1. ❑ ❑ ❑ ❑
2. ❑ ❑ ❑ ❑
3. ❑ ❑ ❑ ❑
4. ❑ ❑ ❑ ❑
5. ❑ ❑ ❑ ❑
6. ❑ ❑ ❑ ❑
7. ❑ ❑ ❑ ❑
8. ❑ ❑ ❑ ❑
9. ❑ ❑ ❑ ❑
10. ❑ ❑ ❑ ❑
Program Evaluation — Test 1623Please evaluate this article.
Poor = 1 to Excellent = 5
Clarity of objectives _____
Usefulness of content _____
Benefit to your clinical practice _____
Quality of manuscript _____
Usefulness of references _____
Quality of illustrations _____
Relevance of illustrations _____
Clarity of questions _____
Article presented newinformation _____
Program achieved itseducational objectives _____
How many minutes did ittake you to completethe test? _____
Please list future CE topic prefer-ences:
A N S W E R S H E ET F O R T EST 16 23Use of an Er:YAG Laser for Pulpotomies in Vital and Nonvital Primary Teeth
Lawrence Kotlow, DDSSubject Code: 430
Place an X in the box correspon-ding to the answer you believe ismost correct.
A B C D
1. ❑ ❑ ❑ ❑
2. ❑ ❑ ❑ ❑
3. ❑ ❑ ❑ ❑
4. ❑ ❑ ❑ ❑
5. ❑ ❑ ❑ ❑
6. ❑ ❑ ❑ ❑
7. ❑ ❑ ❑ ❑
8. ❑ ❑ ❑ ❑
9. ❑ ❑ ❑ ❑
10. ❑ ❑ ❑ ❑
Program Evaluation — Test 1622Please evaluate this article.
Poor = 1 to Excellent = 5
Clarity of objectives _____
Usefulness of content _____
Benefit to your clinical practice _____
Quality of manuscript _____
Usefulness of references _____
Quality of illustrations _____
Relevance of illustrations _____
Clarity of questions _____
Article presented newinformation _____
Program achieved itseducational objectives _____
How many minutes did ittake you to completethe test? _____
Please list future CE topic prefer-ences:
A N S W E R S H E ET F O R T EST 16 22Peri-Implantitis Therapy with an Er:YAG Laser
Avi Reyhanian, DDS, and Donald J. Coluzzi, DDSSubject Code: 690
