pediatrics review jennifer k. bell mhs, pa-c. topics the newborn assessment newborn problems ...
TRANSCRIPT
PEDIATRICS REVIEW
Jennifer K. Bell MHS, PA-C
TOPICS
The newborn assessmentNewborn ProblemsDevelopment ImmunizationsSpecific Pediatric problems by system
Genetic Disorders
THE NEWBORN ASSESSMENT
Apgar scoreExam•SKIN: Erythema toxicum, mongolian spots•HEENT: fontanelles•CARDIAC: PDA•ABD/GU: hypospadias, hydrocele•MS: hip dislocation•NEURO: babinski is normal
APGARS
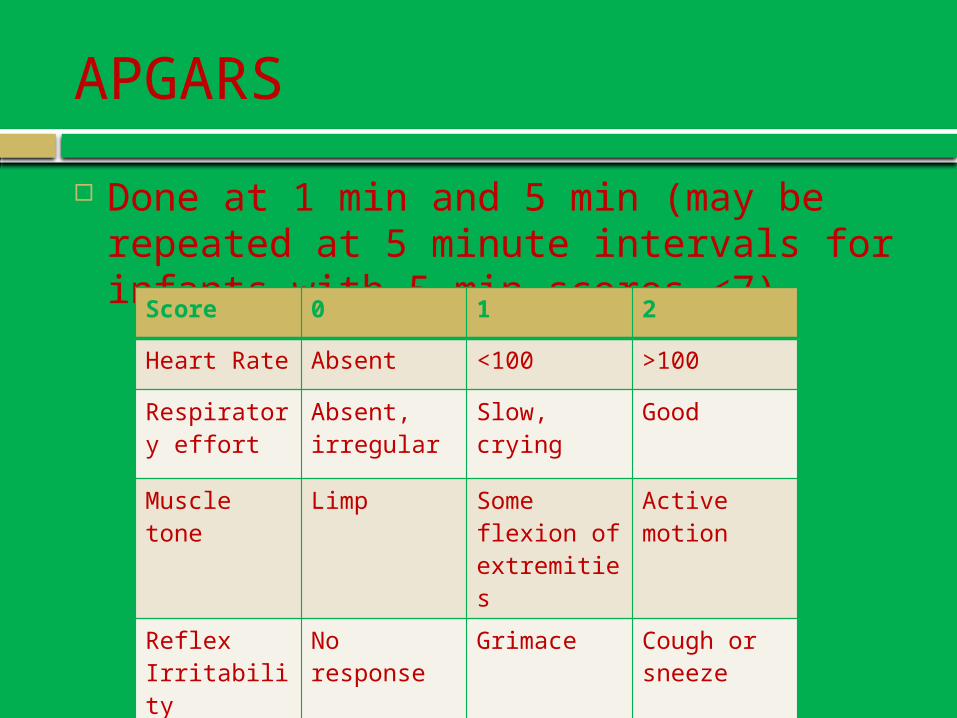
Done at 1 min and 5 min (may be repeated at 5 minute intervals for infants with 5 min scores <7)Score 0 1 2
Heart Rate Absent <100 >100
Respiratory effort
Absent, irregular
Slow, crying Good
Muscle tone Limp Some flexion of extremities
Active motion
Reflex Irritability
No response
Grimace Cough or sneeze
Color Blue, pale Acrocyanosis
Completely pink
Erythema Toxicum neonatorum (the rash of the newborn)
COMMON skin condition in newborns, BENIGN Appears in 50% of newborns Usually between day 3 or life and 2 weeks of life Rash: small, yellow to white papules surrounded
by red skin, usually on face, chest, back, upper arms, sometimes on thighs.
Palms and soles are not involved No treatment needed. Usually fade and disappear over 2 weeks or more

Erythema Toxicum neonatorum
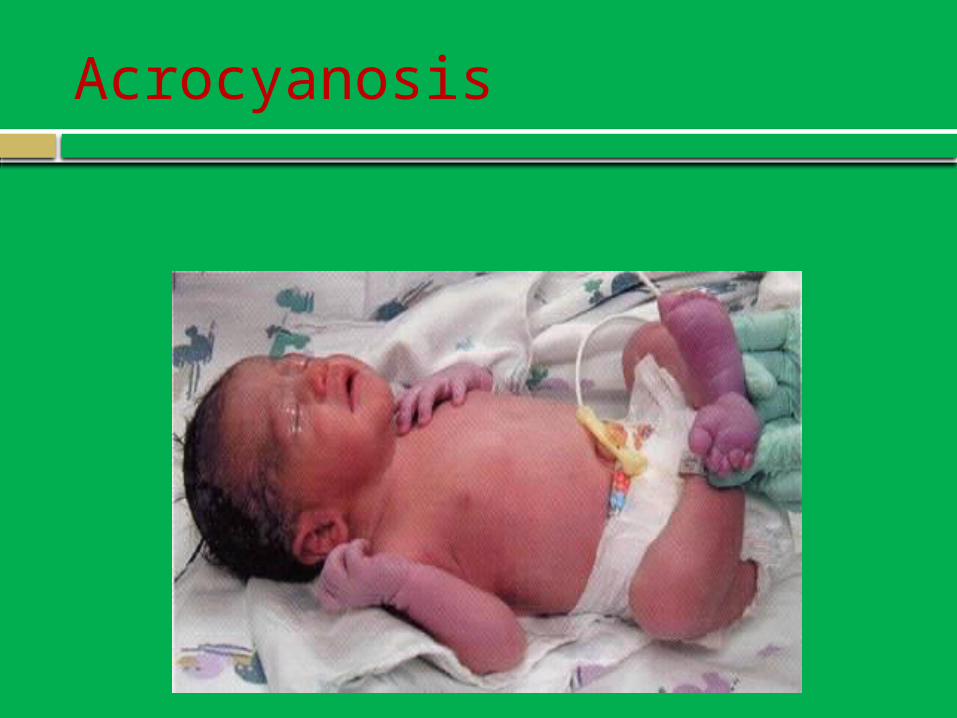
Acrocyanosis

Mongolian Spots
Benign Infantile Hemangioma
Common 3 stages: Growth, Stabilization, Disappearance Most common complication is ULCERATION Usually no treatment required and a simple BIH
resolves on its own.
Further evaluation needed for : Very large or segmented hemangiomas (>5cm) Multiple hemangiomas Located over sacral spine or at the midline Located near the eye Ulceration

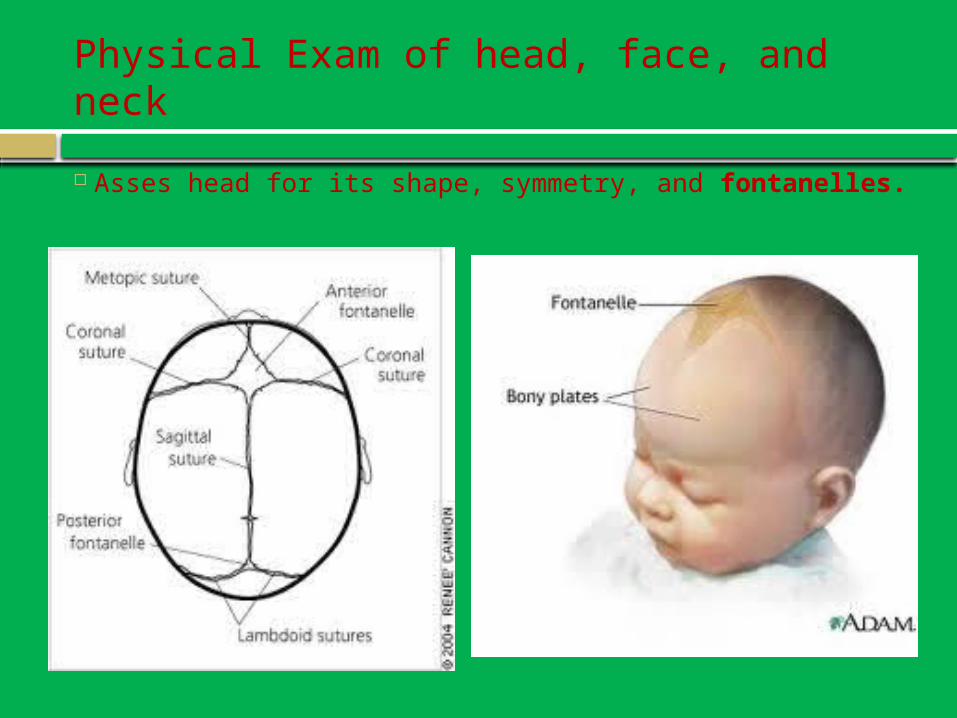
Physical Exam of head, face, and neck
Asses head for its shape, symmetry, and fontanelles.

Caput succedaneum: It is subcutaneous and does cross suture linesCephalhematoma: It is subperiosteal and does not cross suture lines
Cephalohematomas, go away over the course of a few weeks.
Caput succadaneum, goes away in a few days
CARDIAC
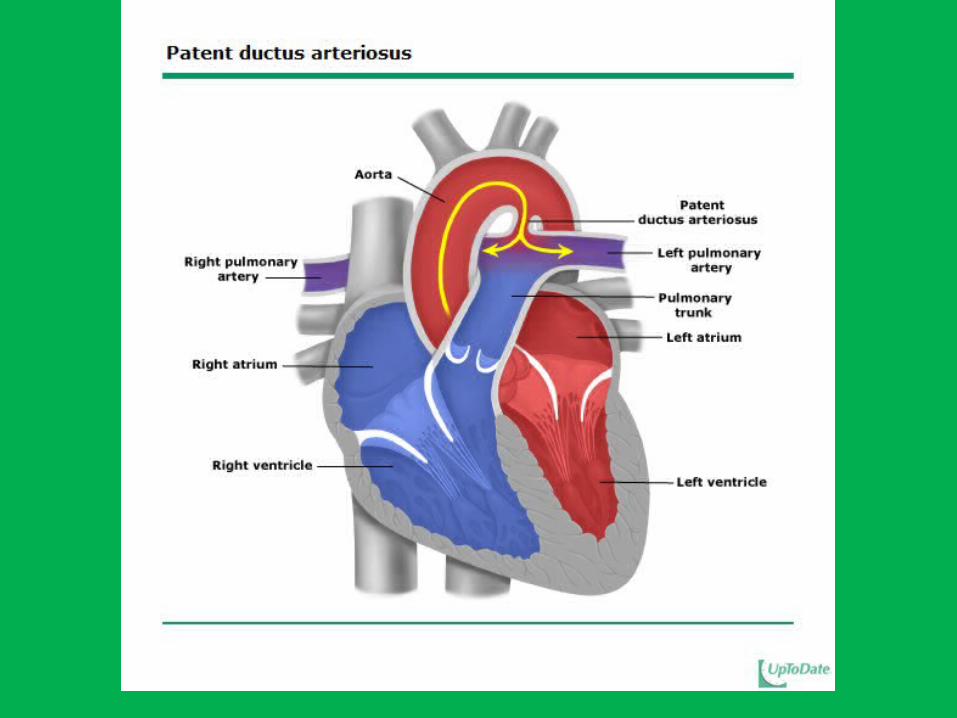
Patent Ductus Arteriosus (PDA) Failure of the ductus arteriosus to close in the first
few days of life OR reopening after functional closure.
Up to 60% in preterm infants weighing < 1500 grams
Female to male ratio= 2:1 Systolic murmur that may be continuous, and is
heard best at the upper left sternal border. MANAGEMENT:
Indomethacin: a prostaglandin synthetase inhibitor, 80% CLOSURE RATE
SURGICAL closure.
The Abdomen
Palpate the kidneys.
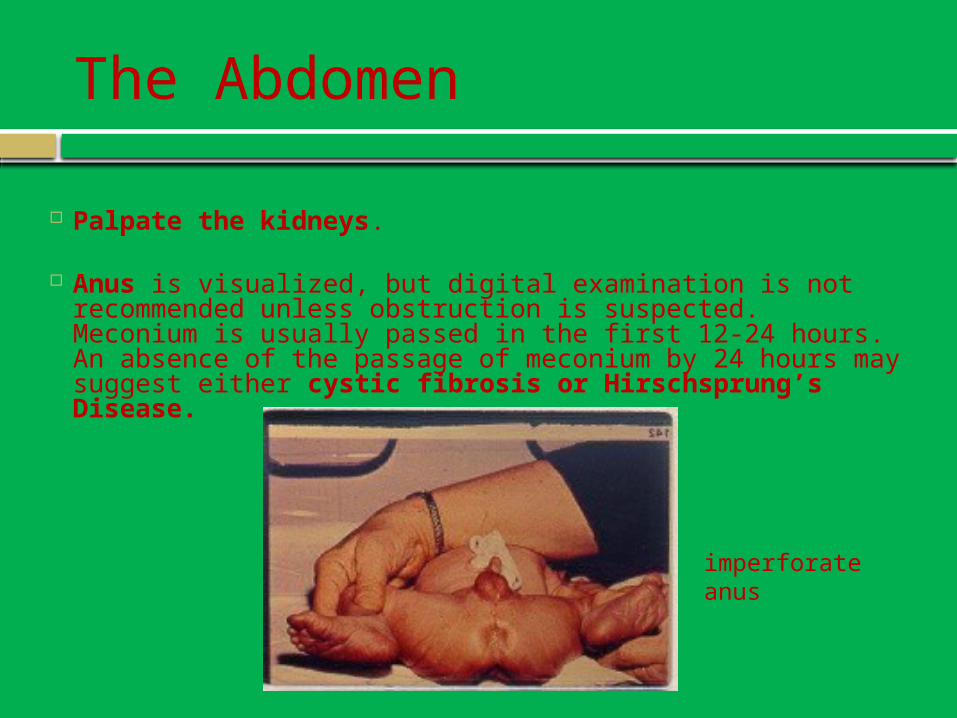
Anus is visualized, but digital examination is not recommended unless obstruction is suspected. Meconium is usually passed in the first 12-24 hours. An absence of the passage of meconium by 24 hours may suggest either cystic fibrosis or Hirschsprung’s Disease.
imperforate anus
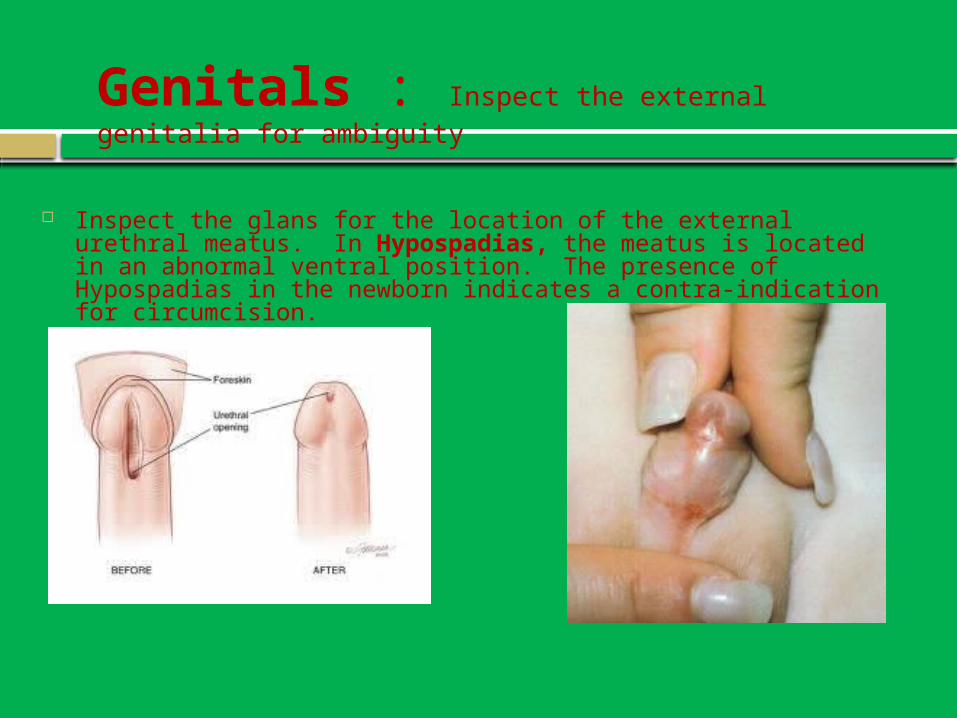
Inspect the glans for the location of the external urethral meatus. In Hypospadias, the meatus is located in an abnormal ventral position. The presence of Hypospadias in the newborn indicates a contra-indication for circumcision.
Genitals : Inspect the external genitalia for ambiguity
Genitals
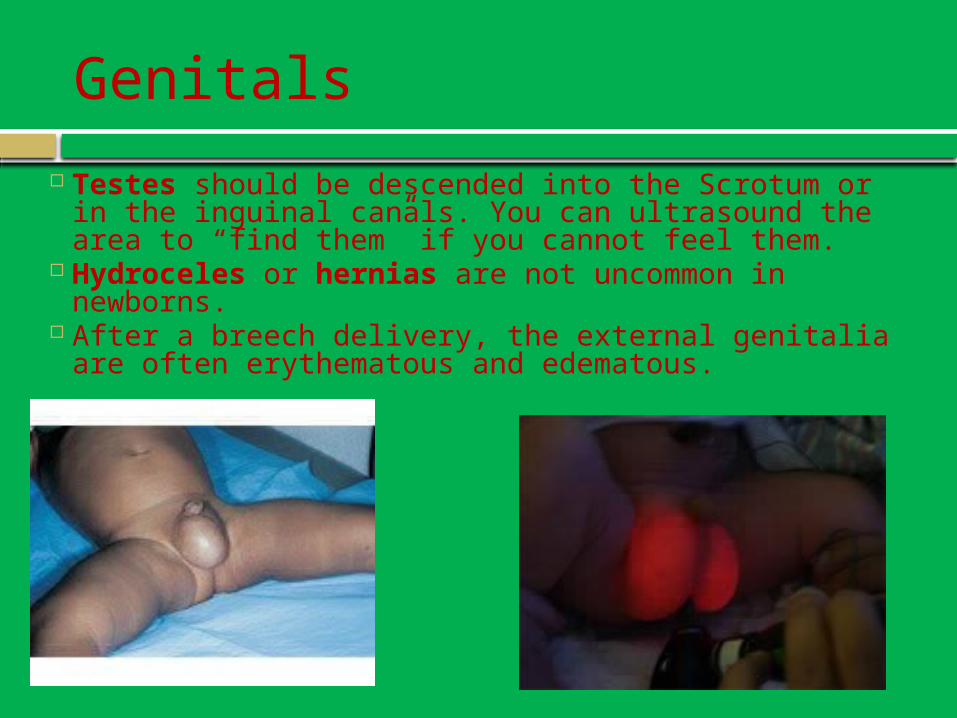
Testes should be descended into the Scrotum or in the inguinal canals. You can ultrasound the area to “find them” if you cannot feel them.
Hydroceles or hernias are not uncommon in newborns.
After a breech delivery, the external genitalia are often erythematous and edematous.
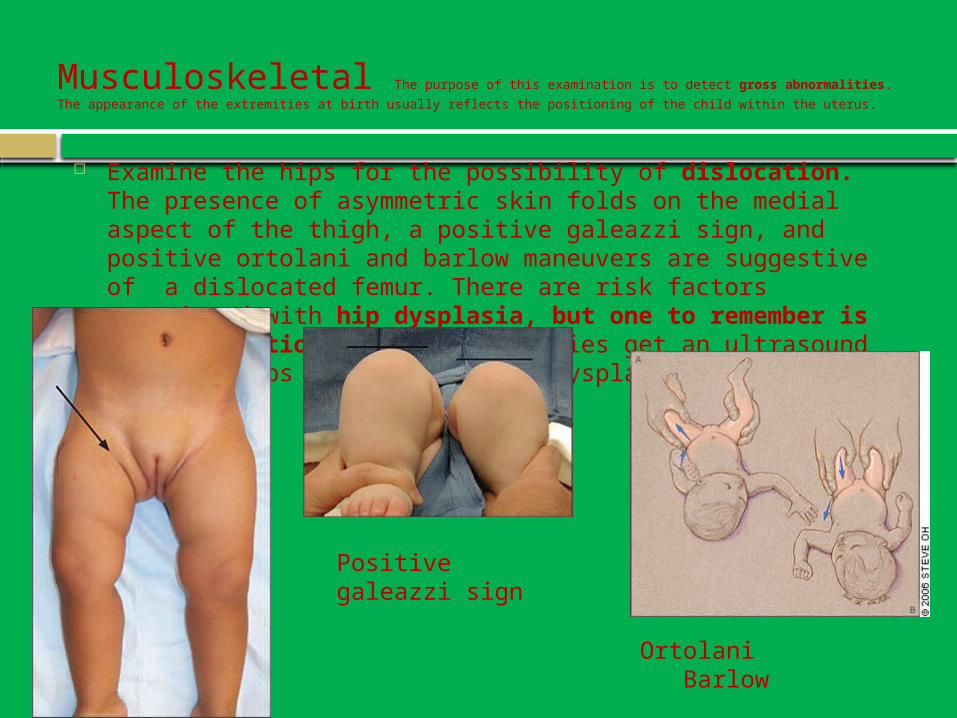
Musculoskeletal The purpose of this examination is to detect gross abnormalities. The
appearance of the extremities at birth usually reflects the positioning of the child within the uterus.
Examine the hips for the possibility of dislocation. The presence of asymmetric skin folds on the medial aspect of the thigh, a positive galeazzi sign, and positive ortolani and barlow maneuvers are suggestive of a dislocated femur. There are risk factors associated with hip dysplasia, but one to remember is breech position. (ALL breech babies get an ultrasound of their hips done to rule out dysplasia)
Positive galeazzi sign
Ortolani Barlow
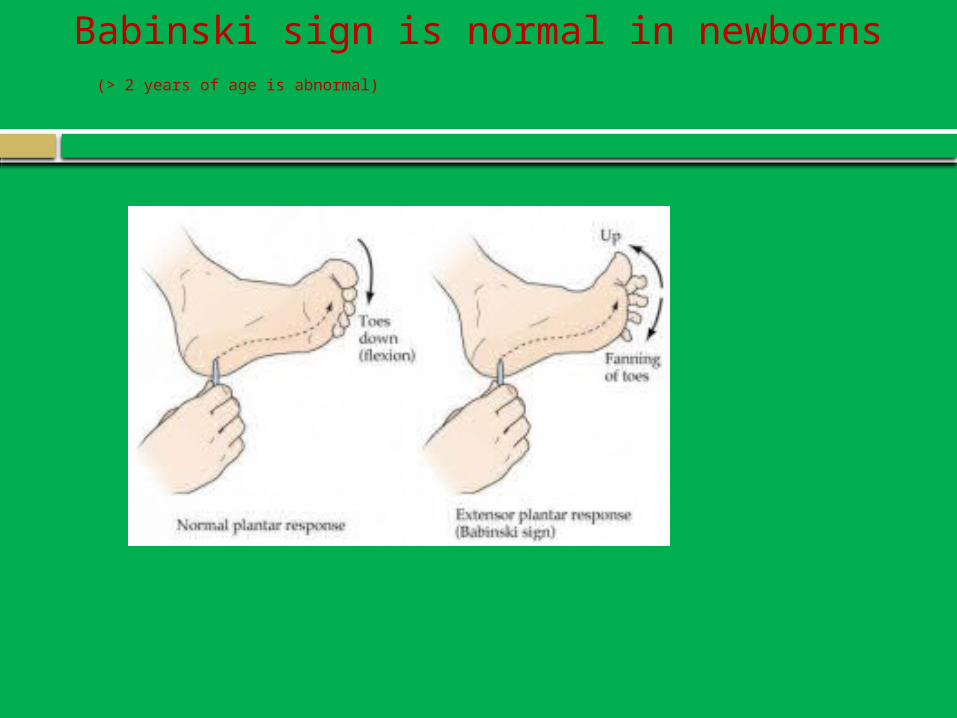
Babinski sign is normal in newborns (> 2 years of age is abnormal)
HypoglycemiaJaundiceHearing
NEWBORN ISSUES
Hypoglycemia-<40mg/dL
Differential Insufficient glucose delivery Decreased glycogen stores Increased circulating insulin (infant of a
diabetic mother, maternal drugs) Endocrine and Metabolic disorders Sepsis Hypothermia Polycythemia Asphyxia Shock
Hyperbilirubinemia
Total Serum Bilirubin Bilirubin peaks at age 5-6 days, then normally stabilizes and
drops. Low risk zone: do nothing Low intermediate risk: possibly supplement if breastfeeding, recheck in
24 hours. Encourage to put in sunlight. High intermediate risk zone: consider bili-blanket (photo therapy) or a
bili-light. Ensure not dehydrated. May need IV fluids. Physiologic jaundice: normal Breastfeeding jaundice: lack of breastmilk Breastmilk jaundice: persists in breastfed babies for 3 weeks to 4
months. Normal.
Remember Kernicterus Bilirubin >20-25 Can lead to permanent brain damage, even death.
Hearing
Routine hearing screening prior to discharge, using Auditory brainstem responses (ABR) Otoacoustic emissions (OAE) *If a child fails, further audiologic testing
needed.

Primitive ReflexesMilestones
Development
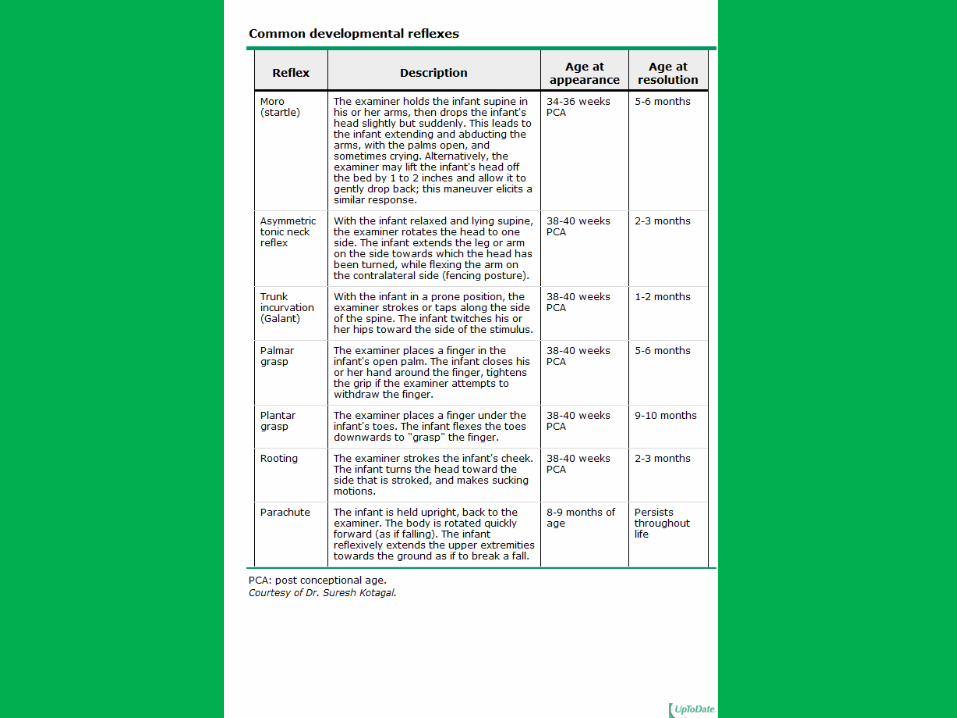
Sucking Response, Rooting Response
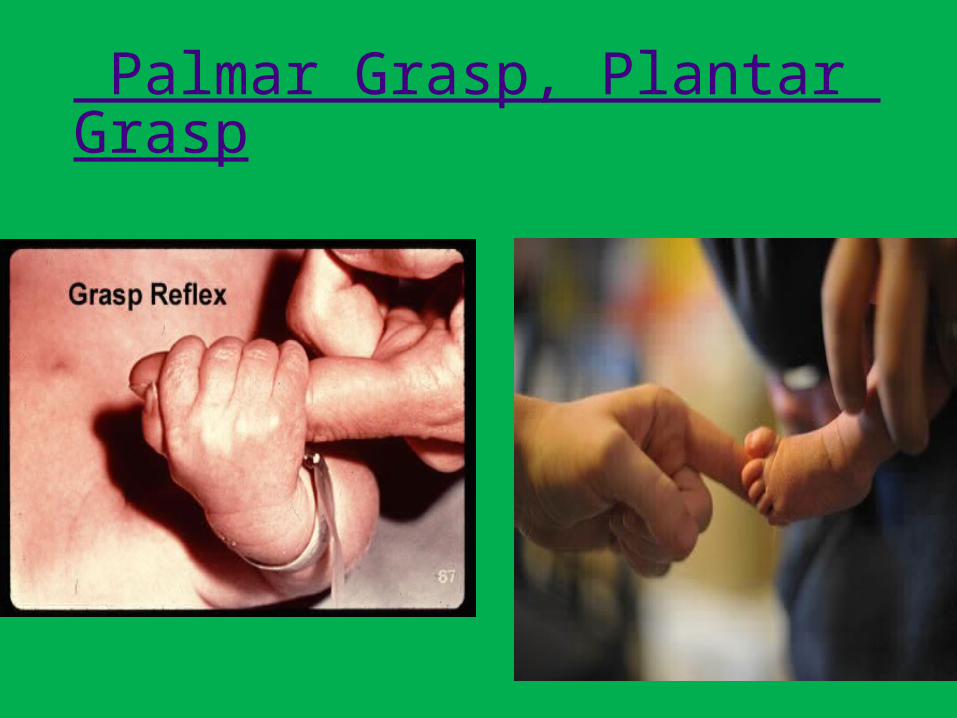
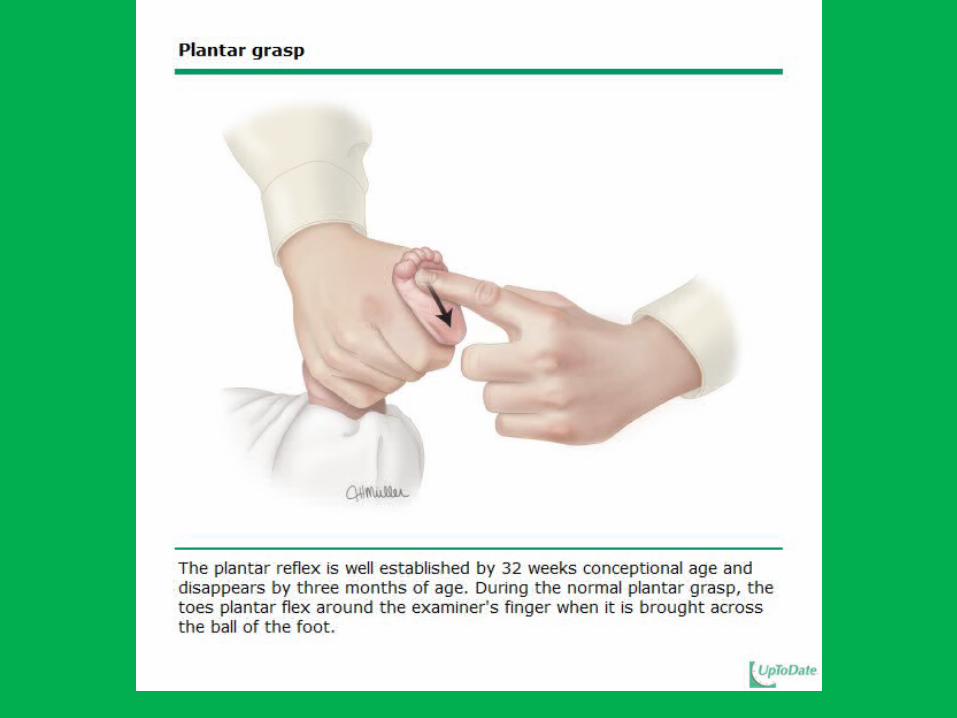
Palmar Grasp, Plantar Grasp

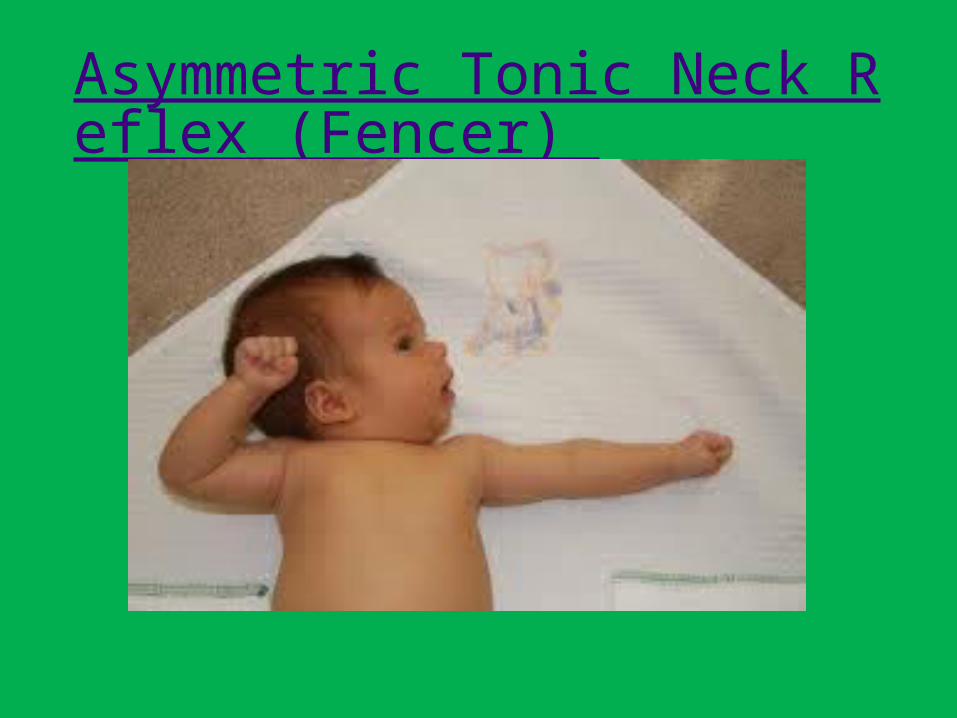
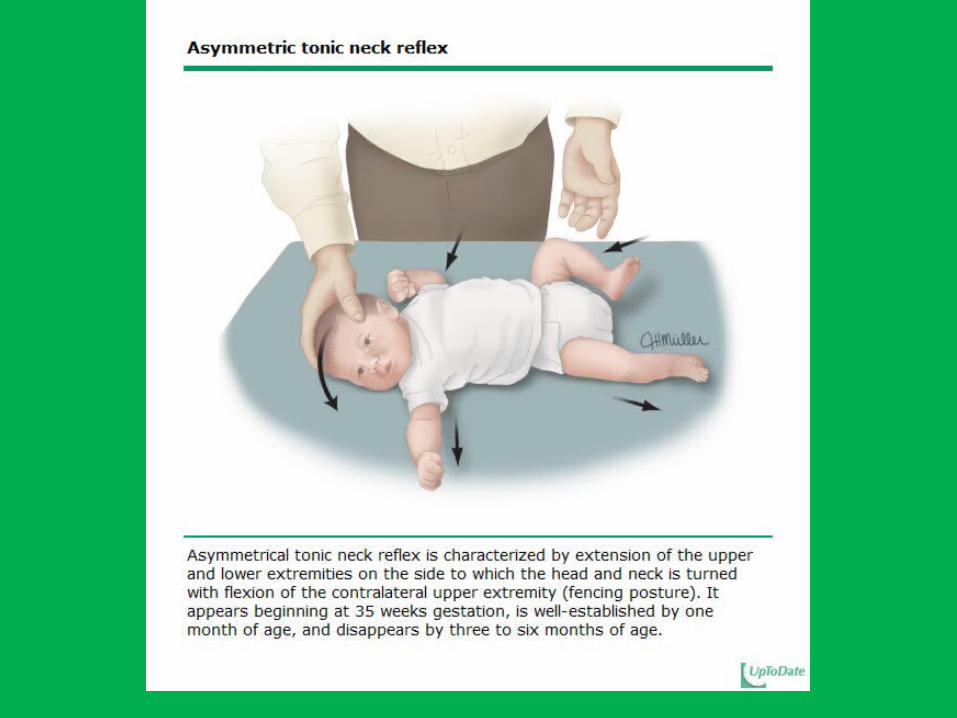
Asymmetric Tonic Neck Reflex (Fencer)
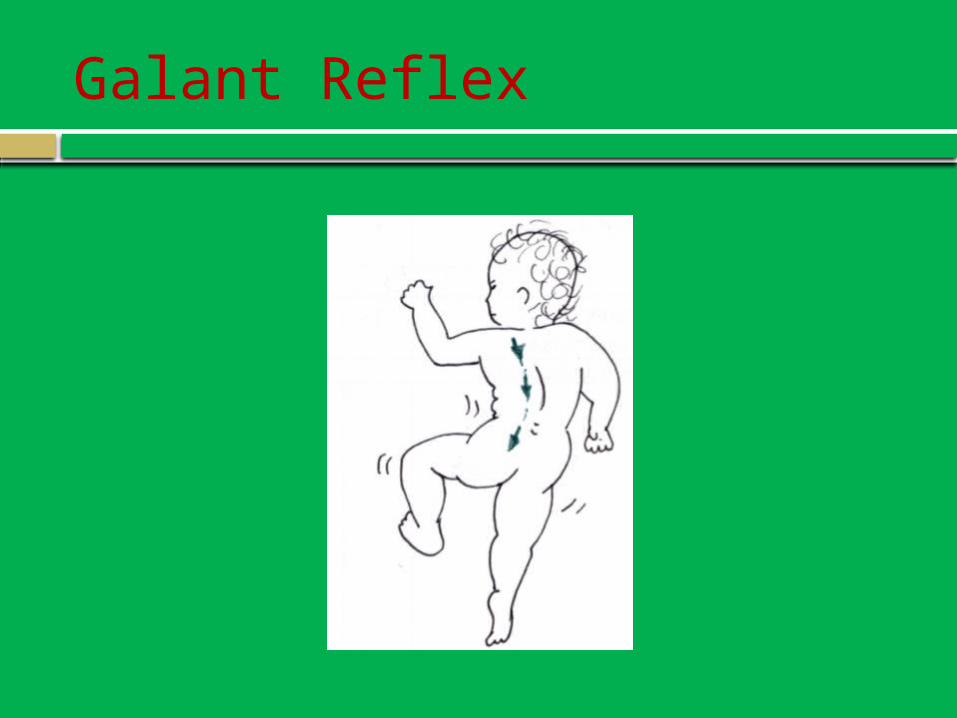
Galant Reflex
Developmental Milestones
Five Major Areas of Normal Development
1. Gross motor skills overall movements of large muscles e.g., sitting, walking, running
2. Fine motor/adaptive skills involve use of small muscles of the hands ability to manipulate small objects problem-solving skills eye-hand coordination

Five Major Areas of Normal Development
3. Language skills hearing understanding language use of language
4. Personal/social skills socialization ability to care for personal needs
5. Cognitive skills ability to use higher mental processes including
comprehension, memory, and logical reasoning
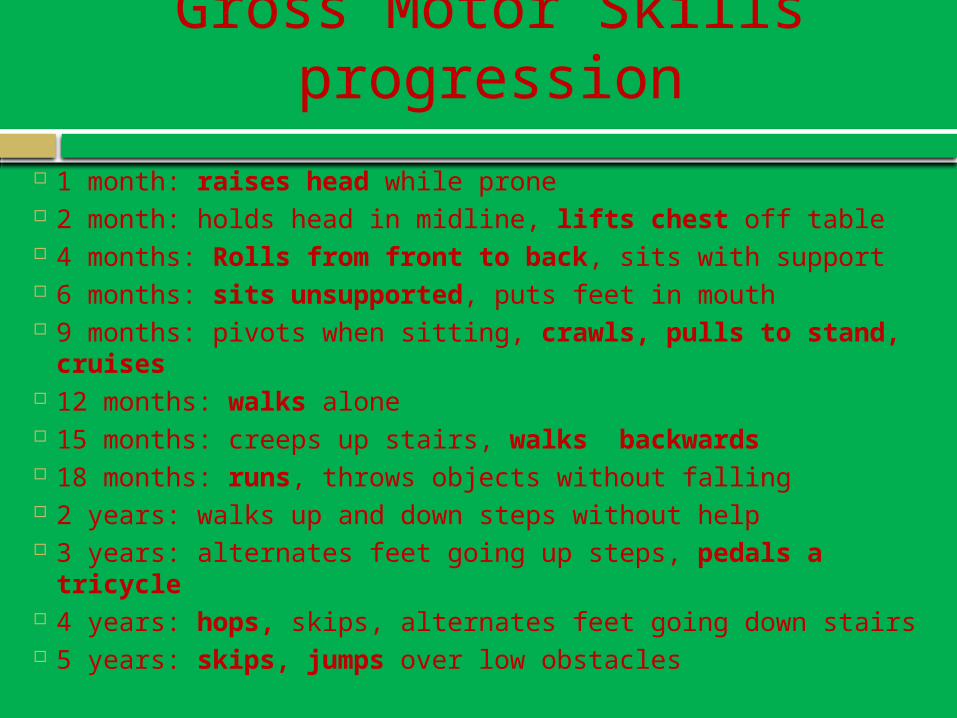
Gross Motor Skills progression
1 month: raises head while prone 2 month: holds head in midline, lifts chest off table 4 months: Rolls from front to back, sits with support 6 months: sits unsupported, puts feet in mouth 9 months: pivots when sitting, crawls, pulls to stand,
cruises 12 months: walks alone 15 months: creeps up stairs, walks backwards 18 months: runs, throws objects without falling 2 years: walks up and down steps without help 3 years: alternates feet going up steps, pedals a tricycle 4 years: hops, skips, alternates feet going down stairs 5 years: skips, jumps over low obstacles
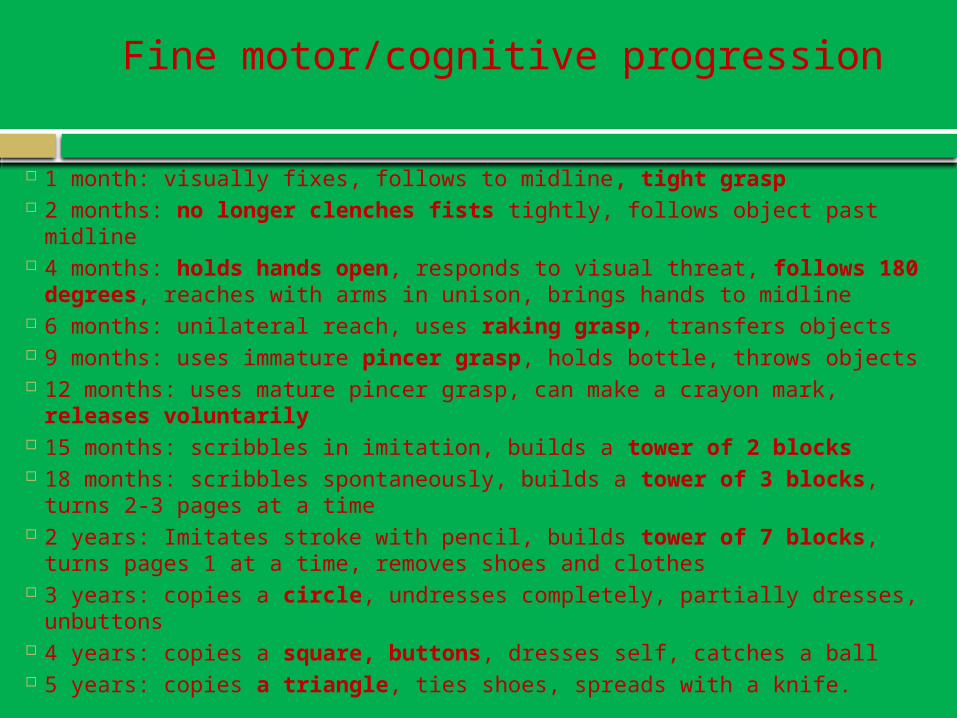
Fine motor/cognitive progression
1 month: visually fixes, follows to midline, tight grasp 2 months: no longer clenches fists tightly, follows object past midline 4 months: holds hands open, responds to visual threat, follows 180
degrees, reaches with arms in unison, brings hands to midline 6 months: unilateral reach, uses raking grasp, transfers objects 9 months: uses immature pincer grasp, holds bottle, throws objects 12 months: uses mature pincer grasp, can make a crayon mark,
releases voluntarily 15 months: scribbles in imitation, builds a tower of 2 blocks 18 months: scribbles spontaneously, builds a tower of 3 blocks, turns
2-3 pages at a time 2 years: Imitates stroke with pencil, builds tower of 7 blocks, turns
pages 1 at a time, removes shoes and clothes 3 years: copies a circle, undresses completely, partially dresses,
unbuttons 4 years: copies a square, buttons, dresses self, catches a ball 5 years: copies a triangle, ties shoes, spreads with a knife.

Language Progression
1 month: alerts to sound 2 months: smiles socially 4 months: laughs, orients to voice 6 months: babbles, lateral orientation to bell 9 months: says “mama dada” indescriminately, gestures, understands
“no” 12 months: uses 2 words besides mama and dada, follows a one step
command with a gesture, waves bye bye 15 months: uses 4-6 words, follows a one step command without a
gesture 18 months: 15 words, knows 5 body parts 2 years: uses pronouns (I, you, me) inappropriately, follows 2 step
commands, >20 word vocabulary, uses 2 word sentences 3 years: uses 250 words, 3 word sentences 4 years: knows colors, says a song or poem from memory, asks
questions 5 years: prints first name, asks what a word means, knows opposites,
counts
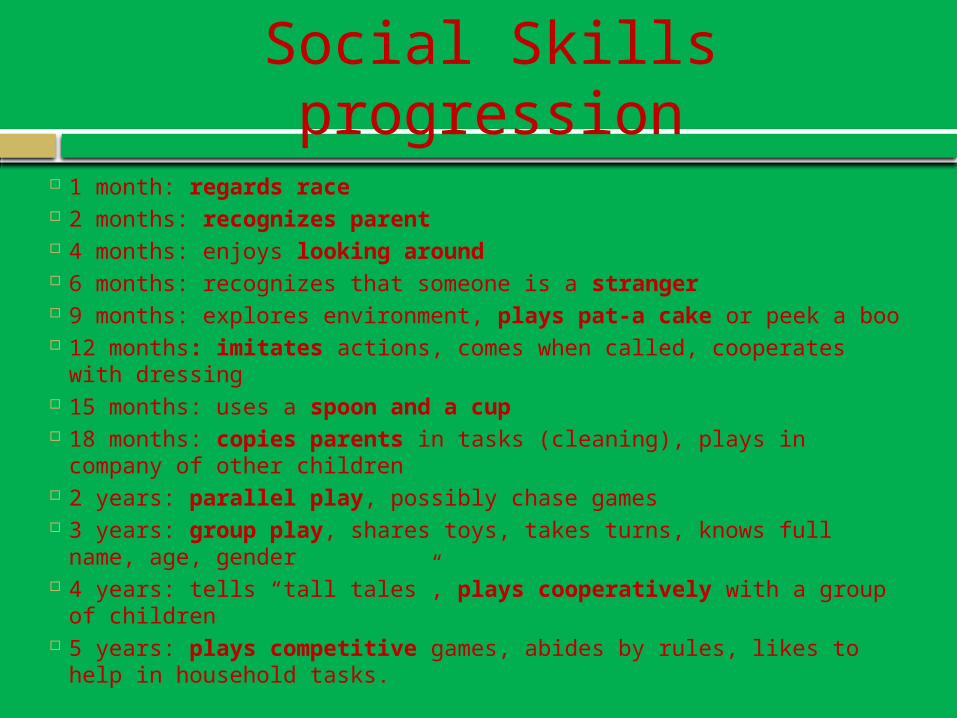
Social Skills progression
1 month: regards race 2 months: recognizes parent 4 months: enjoys looking around 6 months: recognizes that someone is a stranger 9 months: explores environment, plays pat-a cake or peek a boo 12 months: imitates actions, comes when called, cooperates with
dressing 15 months: uses a spoon and a cup 18 months: copies parents in tasks (cleaning), plays in company of
other children 2 years: parallel play, possibly chase games 3 years: group play, shares toys, takes turns, knows full name, age,
gender 4 years: tells “tall tales”, plays cooperatively with a group of
children 5 years: plays competitive games, abides by rules, likes to help in
household tasks.

Hep BRotavirusInfluenzaPneumococcalHIBPolioDtapHep AVaricellaMMRHPVMeningococcus
The schedule and also details about the conditions
Immunizations
If you memorize a typical schedule of immunizations at well child visits, you will probably have a hard time missing a vaccine question regarding timing of vaccinations.
FIRST A HINT
Hep B
Transmission: percutaneous or mucosal exposure to blood or body fluids, including contact with contaminated surfaces
Chronic HBV infection: 25% die prematurely from cirrhosis or liver cancer
Recommended: birth, 1-2 months, 6-18 months
3 dose schedule for adolescents and adults
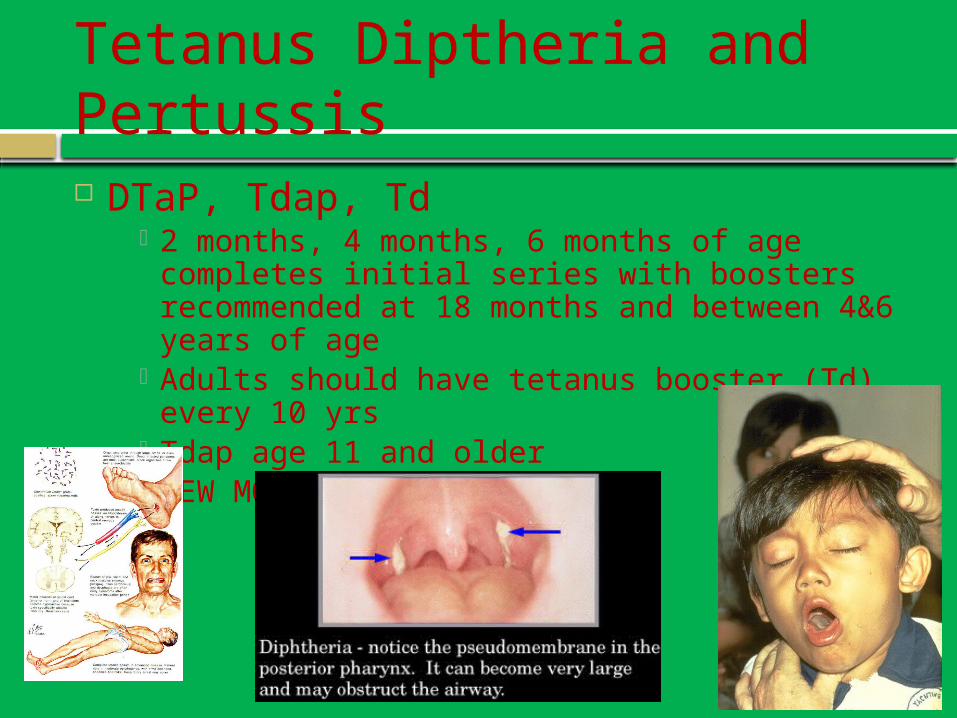
Tetanus Diptheria and Pertussis DTaP, Tdap, Td
2 months, 4 months, 6 months of age completes initial series with boosters recommended at 18 months and between 4&6 years of age
Adults should have tetanus booster (Td) every 10 yrs
Tdap age 11 and older NEW MOMS!!

Diptheria
Bacterial infection spread by respiratory droplets
Sore throat, low-grade fever Obstructive grayish membrane
Pertussis
Whooping cough Bordetella pertussis Spread by respiratory droplets Treat with Erythromycin, and treat close
contacts
Tetanus
Lockjaw Clostridium tetani (anaerobic bacteria
found in soil) Toxin proliferates in wounds Treatment with antitoxin Signs: severe muscle spasm, trismus
Rotavirus
Most common cause of severe gastroenteritis in infants and young children
Near universal infection by age 5 years U.S. – vaccine saves baby severe
dehydration, hospitalization 2-3 doses at 2/4/6 months
Influenza
Yearly dose Starts at age 6 months Avoid if allergy to eggs
Inactivated and Live are available. Do not give live vaccine to pregnant women.
Pneumococcal
All children 4 doses: 2,4,6, 12-15 months After age 2 in certain populations:
asplenics, sickle cell, complement deficiency
HIB
Prevents Meningitis, Epiglottitis, Pneumonia
HIB: bacterial infection spread by respiratory droplets
4 doses: 2, 4, 6, and 12-15 months
IPV-Poliovirus
Fecal-oral transmission Up to 95% of infections are
asymptomatic Maintain high immunization rates
Infections in Amish, 2005 29 countries reported wild poliovirus to
WHO in 2009 or 2010 (plane ride away) IPV schedule: 2, 4, 6-18 months, 4-6
years
Hep A
Fecal-oral transmission Food-borne outbreaks
PA, 2003 (Chi-Chi’s, green onions) 601 cases, 124 hospitalizations, 3 deaths
Risk factors include child or employee in day care, travel
2 doses at least 6 months apart Recommended at 12-23 months
MMR
Live vaccine First dose at 1 year, second dose at 4-6
years of age.

Measles
Begins behind the ears, and in 24-36 hours it spreads to the trunk and extremities
In 3 days it reaches its maximum intensity and fades after 5-10 days.
Koplik spots VITAMIN A
Reduce morbidity and mortality in measles
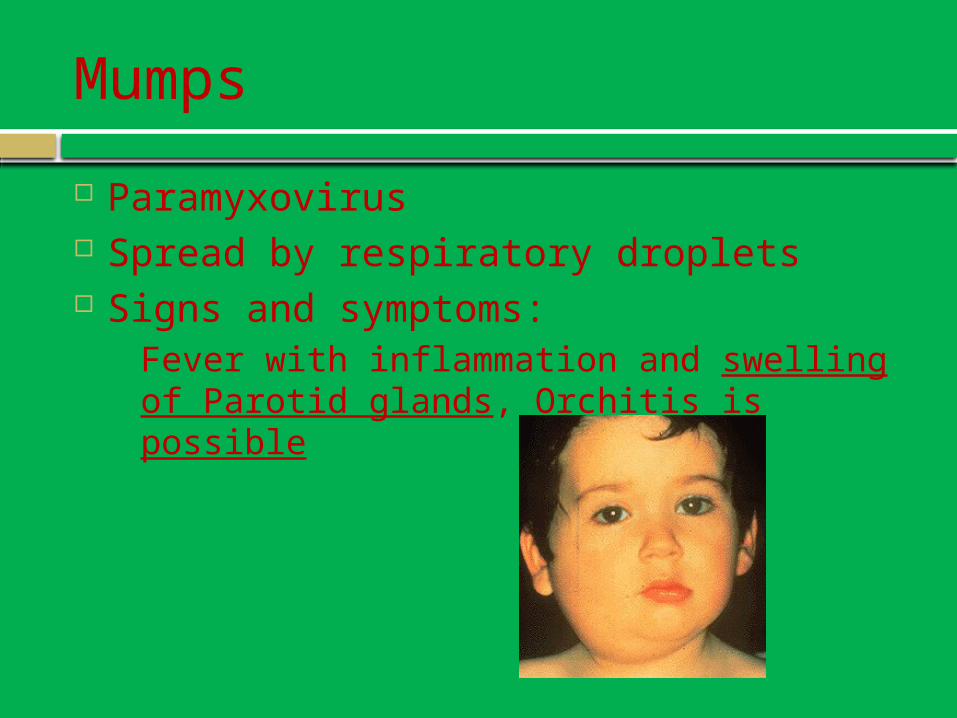
Mumps
Paramyxovirus Spread by respiratory droplets Signs and symptoms:
Fever with inflammation and swelling of Parotid glands, Orchitis is possible

Rubella
Most important consequences are to the unborn: miscarriages, stillbirths, fetal anomalies (congenital rubella syndrome).
Varivax
Varicella Zoster 2 doses: 1 year of age and a booster at 4-6
years of age
Spread by respiratory droplets Signs: fever, flue-like symptoms, blistery
itchy rash that crusts over Contagious until the rash becomes crusted Reactivations later in life are possible
(shingles)

HPV
Approved for girls and boys ages 9-26 years of age.
3 doses Dose 1 Dose 2, in 2 months Dose 3, in 6 months from first dose
Meningococcus
Protects against Neisseria meningitidis Meningitis septicemia
High risk groups Dormatory living Military
Booster dose now approved, so 1 dose at age 11, then 5 years later a booster dose.
Some Select Pediatric Problems
•Cryptorchidism•Cradle Cap•Diaper Rash•Fifths disease: Erythema Infectiosum•Roseola infantum (sixth disease)•Kawasaki’s Disease
•Nasolacrimal duct obstruction•Strep Throat•Coarctation of the Aorta•Tetrology of Fallot•Pyloric Stenosis•Intussusception
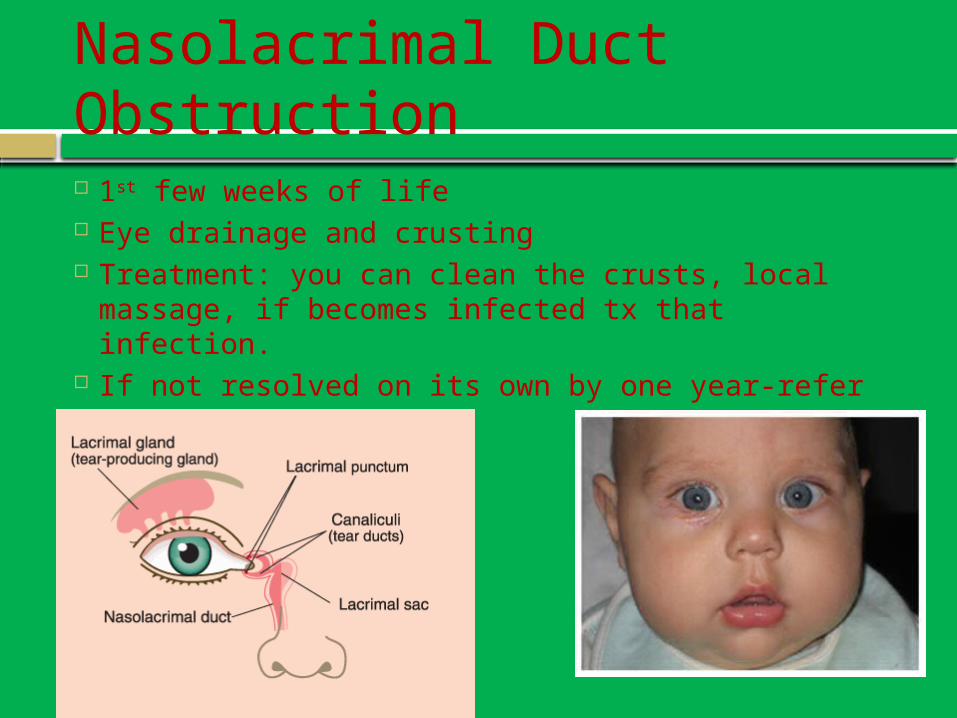
Nasolacrimal Duct Obstruction 1st few weeks of life Eye drainage and crusting Treatment: you can clean the crusts, local
massage, if becomes infected tx that infection. If not resolved on its own by one year-refer

Strep Throat: Group A (GABHS)
Strawberry tongue Scarletina rash: fine reddish sandpaper
like rash sparing the palms and soles
Symptoms: Exudative tonsilitis Ant cervical lymphadenopathy Fever > 101F Absence of URI symptoms Abdominal Symptoms
Cardiac stuff
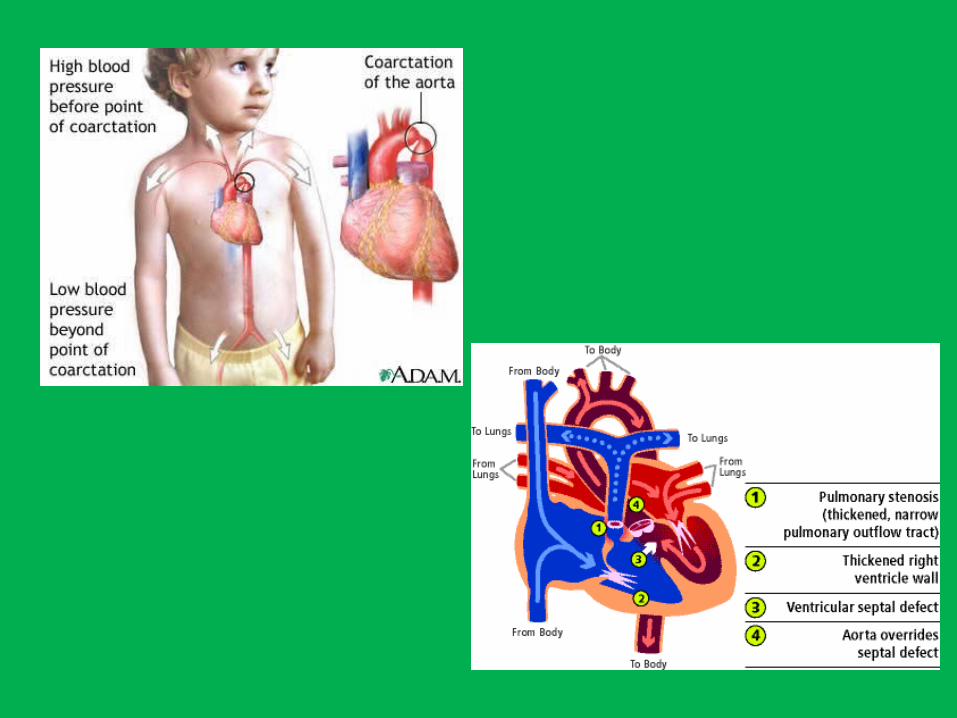
Coarctation of the aorta Narrowing of aorta causing systolic murmur
and differential in pulses in upper and lower extremities
Tx: surgery Tetralogy of Fallot
VSD, RVH, Pulmonic Stenosis, Overriding Aorta
Tx: complete surgical repair
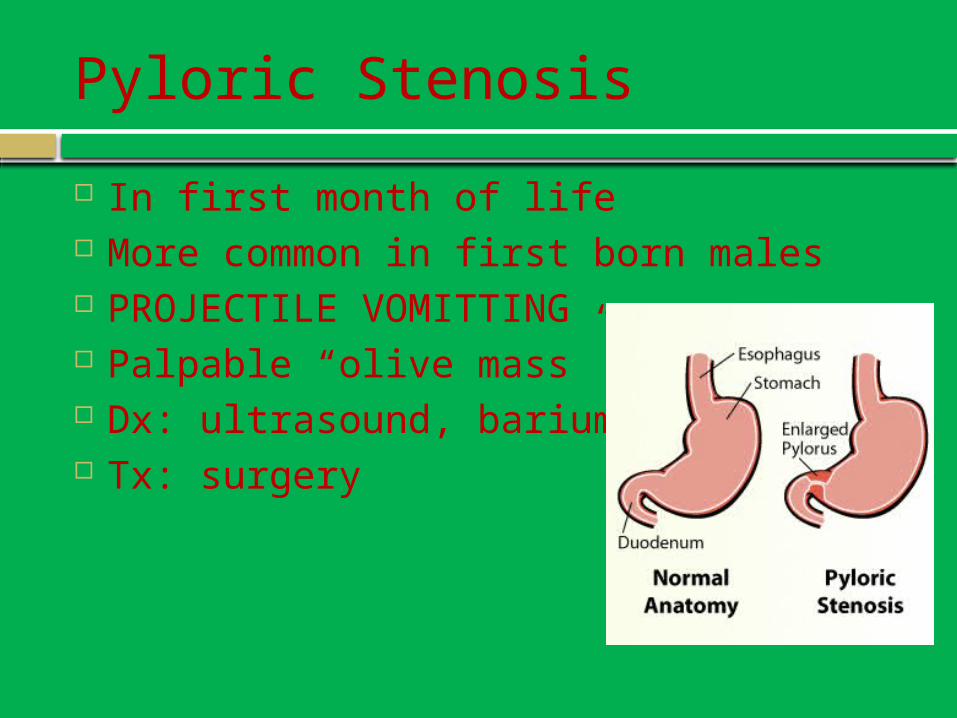
Pyloric Stenosis
In first month of life More common in first born males PROJECTILE VOMITTING Palpable “olive mass” Dx: ultrasound, barium swallow Tx: surgery
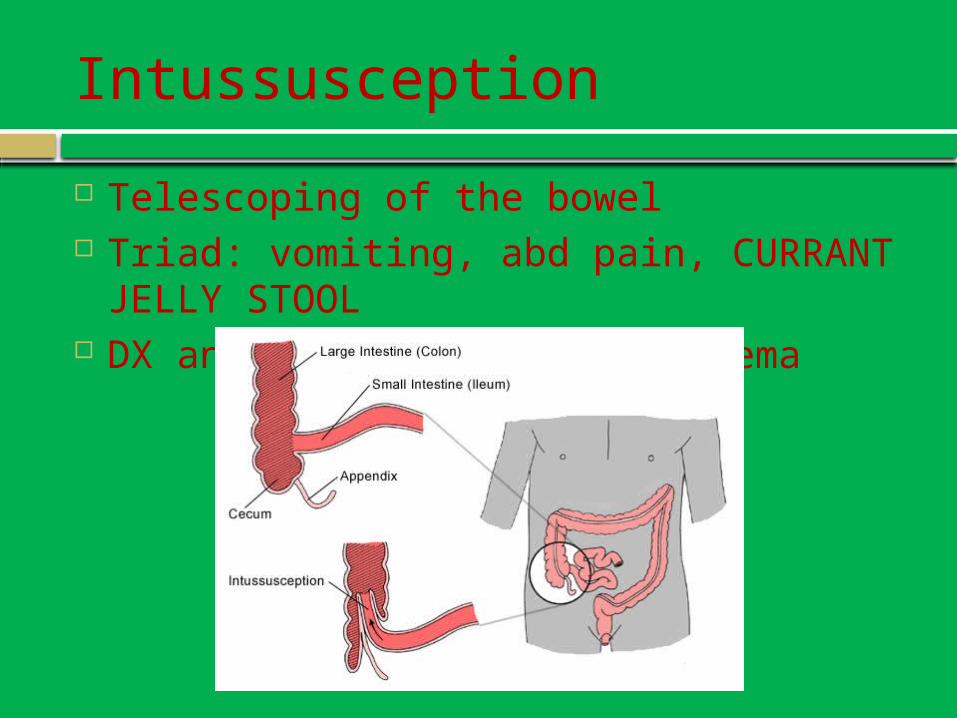
Intussusception
Telescoping of the bowel Triad: vomiting, abd pain, CURRANT JELLY
STOOL DX and TX: barium or air enema
Cryptorchidism
Increased risk of testicular cancer later in life
Undescended testes Tx: surgery

Seborrheic Dermatitis (cradle cap)
Seborrheic Dermatitis (Cradle cap) Very common rash characterized by
erythema and greasy scales Can affect the face, ears, and neck Usually self limiting, but can be treated:
White petroleum Ketoconazole Hydrocortisone cream
Diaper Dermatitis
Causes: Candida (satelite lesions)
Treatment: antifungal (lotrimin) Prolonged contact with urine or stool
causes skin breakdown Barrier (desitin otc cream)
Bacterial causes Strep B, “Perianal streptococcal infection”
(Amoxil)
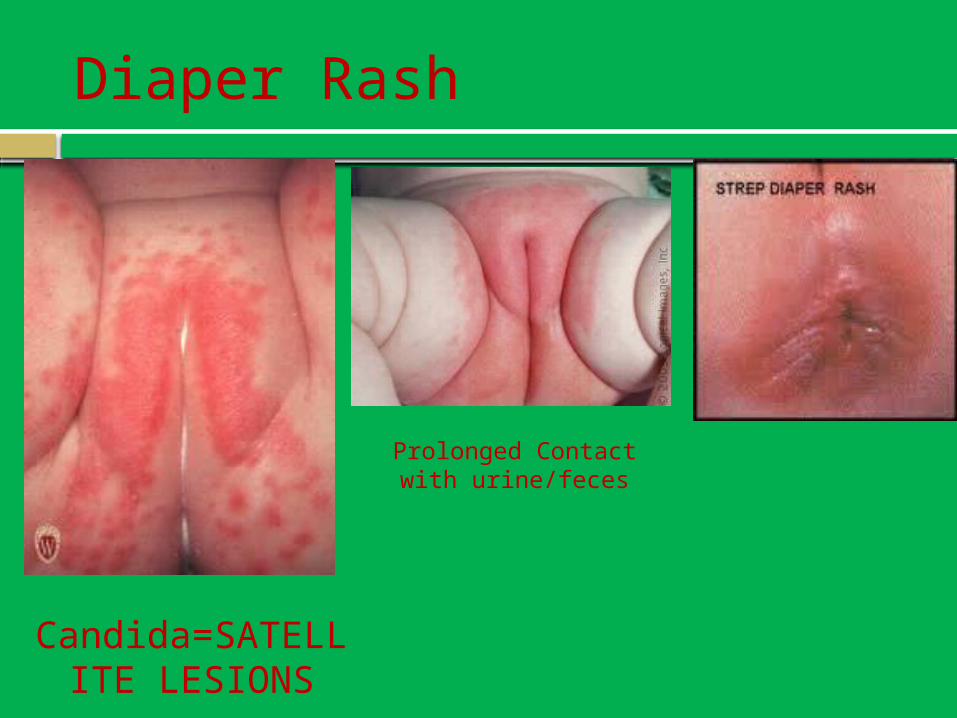
Diaper Rash
Candida=SATELLITE LESIONS
Prolonged Contact with urine/feces
Erythema Infectiosum-AKA Parvovirus B19 or Fifth disease
Common, Mildly contagious Appears in epidemics, children between
5-14 years of age Transmitted via respiratory route and
infected blood Can be asymptomatic Prodromal symptoms
Mild, pruritus, low-grade fever, malaise, sore throat (asymptomatic)
Erythema infectiosum-3 phases
Stage 1: facial erythema (slapped cheeks) Red papules coalesce forming fiery red, slightly edematous,
warm plaques that are symmetric on both cheeks and spare the nasolabial fold and circumoral region.
Fades in 4 days
Stage 2: Net pattern erythema Erythema in a fishnet-like pattern begins on the extremities 2
days after the facial erythema. Extends to the trunk and buttocks fading in 6-14 days
Stage 3: recurrent phase The eruption fades and then reappears in previously affected
sites on the face and body during the next 2-3 weeks. Triggers: emotional upsets, sunlight, temperature.

Roseola
80% of all children by age 1, 90% by age 2 Most cases are asymptomatic OR occur with a fever of
unknown origin and NO rash Most cases between 6 months and 4 years Typically: very high fever, fever subsides and the
rash appears. Febrile seizures common

Kawasaki Disease: AKA Mucocutaneous lymph node syndrome
Children: 7 weeks-12 years of age. (rare in adults)
An acute multisystem vasculitis of unknown etiology (likely infectious cause)
Cardiovascular manifestations are the main cause of morbidity
Down SyndromeKlinefelter SyndromeTurners SyndromeMarfan Syndrome
Genetic Disorders
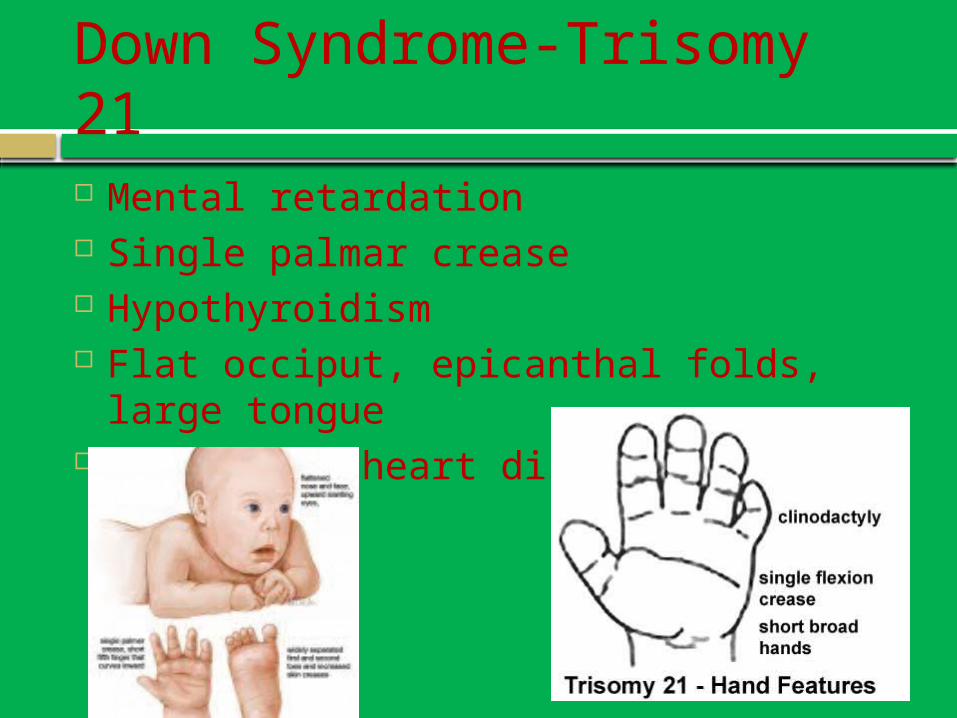
Down Syndrome-Trisomy 21
Mental retardation Single palmar crease Hypothyroidism Flat occiput, epicanthal folds, large
tongue Congenital heart disease
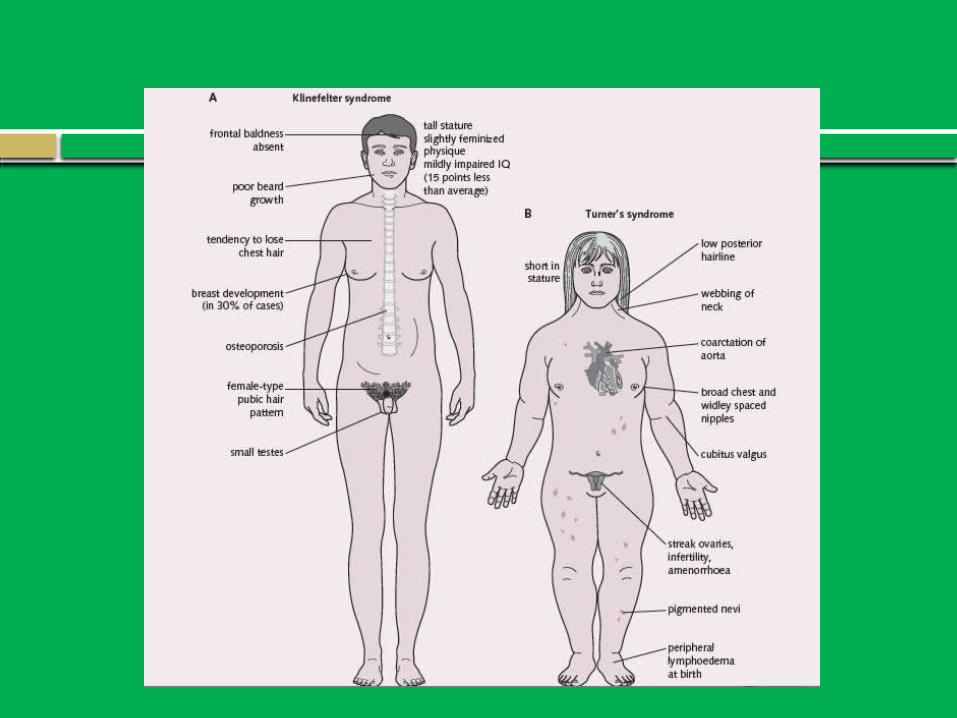
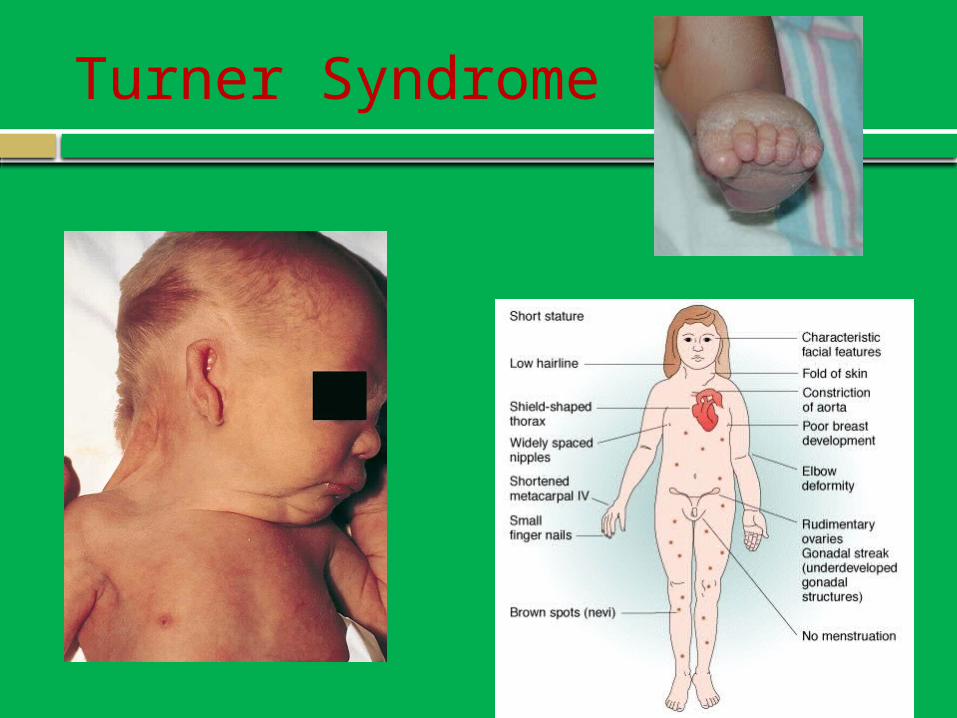
Turner Syndrome (XO)
1/2500 affected Physical characteristics
Short stature Broad chest with widely placed nipples Low hairline Low set ears Webbed neck Amenorrhea Sterility Congenital heart disease, DM, vision problems,
hypothyroidism, autoimmune diseases
Turner Syndrome
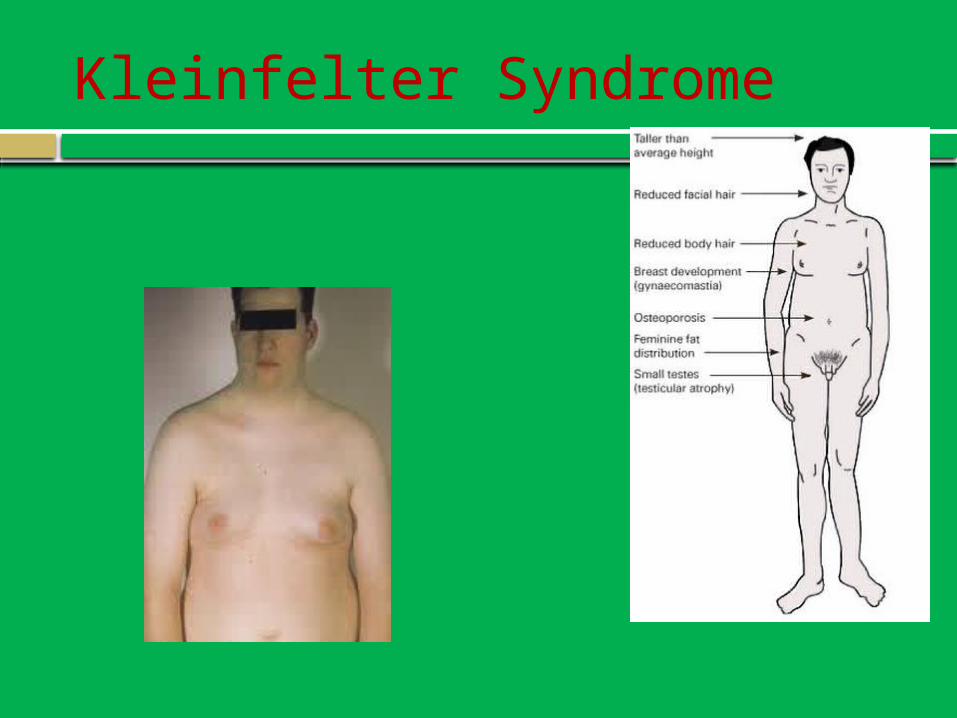
Kleinfelter Syndrome (XXY)
Most common sex chromosome disorder 1/500 Long legs small, firm testes and gynecomastia Osteoporosis Motor delay or dysfunction Language and speech problems Attention deficits Behavioral and psychosocial problems Dyslexia or reading dysfunction
Decreased fertility (thought to be the cause of 2-3% of male infertility)
Kleinfelter Syndrome
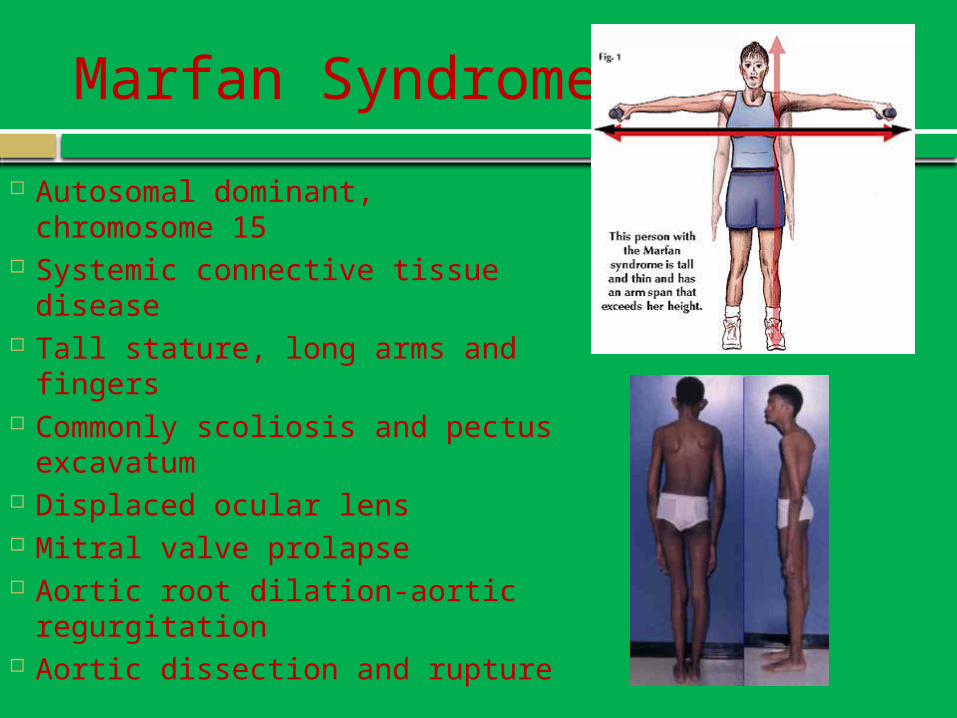
Marfan Syndrome
Autosomal dominant, chromosome 15
Systemic connective tissue disease
Tall stature, long arms and fingers Commonly scoliosis and pectus
excavatum Displaced ocular lens Mitral valve prolapse Aortic root dilation-aortic
regurgitation Aortic dissection and rupture
GOOD LUCK TO YOU ALL!!!
The Last time you will likely ever endure a lecture with me