pediatrics in review 1989 dewitt 6 12
DESCRIPTION
ooTRANSCRIPT
DOI: 10.1542/pir.11-1-61989;11;6Pediatrics in Review
Thomas G. DeWittAcute Diarrhea in Children
http://pedsinreview.aappublications.org/content/11/1/6the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/content/11/4/124.full.pdf An erratum has been published regarding this article. Please see the attached page for:
Print ISSN: 0191-9601. Village, Illinois, 60007. Copyright © 1989 by the American Academy of Pediatrics. All rights reserved.trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove
andpublication, it has been published continuously since 1979. Pediatrics in Review is owned, published, Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on July 16, 2014http://pedsinreview.aappublications.org/Downloaded from at Indonesia:AAP Sponsored on July 16, 2014http://pedsinreview.aappublications.org/Downloaded from at Indonesia:AAP Sponsored on July 16, 2014http://pedsinreview.aappublications.org/Downloaded from
The questions below should helpfocus the reading of this article.
1. What are typical laboratory find-
ings in patients with lactase malab-sorption?2. What clinical and simple labora-tory findings are useful in the differ-ential diagnosis between viral andbacterial enteritis?3. What are the roles of oral hydra-tion solutions and solid foods in themanagement of diarrhea with acutediarrheal illnesses?4. Why do soft drinks and fruit juicesnot make good oral hydration solu-tions?5. What are the characteristics ofCryptosporidlum ententis?
EDUCATIONAL OBJECTIVES
7. The pediatrician should haveknowledge to make an appropriateevaluation of a dehydrated infantwith gastroenteritis, assessingelectrolyte status and identifyingthe clinical situation in which oralrehydration is the desired methodof management rather than paren-teral fluid therapy, with specific at-tention to resources available tocorrect dehydration in a cost-effective manner (Topics, 89/90).31. The pediatrician should havean appropriate awareness of theclinical features of Campylobacterententis (Recent Advances, 88/89).91. The pediatrician should havean appropriate recognition of thevalue of the breath hydrogen testin the diagnosis of carbohydrateintolerance (Recent Advances, 88/89).99. The pediatrician should havean appropriate understanding ofthe factors involved in the decisionto start solid foods after an epi-sode of acute diarrhea in an infant(Recent Advances, 88/89).
* Associate Professor of Pediatrics, Director,
Division of General and community Pediatrics,University of Massachusetts Medical center,Worcester.
PIR 6 pediatrics in review #{149}vol. 11 no. 1 july 1989
Acute Diarrhea in ChildrenThomas G. DeWitt, MD*
Derived from the Greek dia“through”and rhien “to flow”, the termdiarrhea refers to stools that are ab-normally frequent and liquid. Themodifier “abnormal” is critical in pe-diatrics because stools can normallybe frequent and liquid in the youngpediatric patient. Acute diarrheal ill-nesses account for more than 3 mil-lion ambulatory pediatric visits, 10million sick days, and 1 00 000 hos-pital admissions per year in the UnitedStates. This review will focus primar-ily on acute pediatric diarrhea and itssequelae because chronic diarrheawarrants its own review. In this article(1) the pathophysiologic processesthat cause acute diarrhea will be ex-amined, (2) guidelines for evaluatinga child with acute diarrhea will besuggested, and (3) current manage-ment issues and approaches will beexplored.
Pathophysiology
In acute diarrhea in children, onemust consider two concepts relatedto its pathophysiology: the first is thedevelopmental aspects of the younggastrointestinal system with regard
to fluid and electrolyte transport; thesecond relates to the four principalpathophysiologic processes that cancontribute individually or collectivelyto diarrhea. These processes tend toproduce different types of diarrheawith varying fluid and electrolytelosses that have significant implica-tions for management.
The developing gastrointestinal sys-tem has an age-related variation inthe metabolism of fluid and electro-lytes. In the young infant, the intes-tinal mucosa tends to be permeableto water. As the child matures, thepermeability of the mucosa dimin-ishes. Therefore, in a young infantthe impact of the increased luminalosmolality due to diarrheal processescan result in a greater net fluid andelectrolyte loss than in an older childor adult with a similar process. Inaddition, because 80% of fluid ab-sorption occurs in the small bowel, apathologic process that predominant-ly affects the small bowel will predis-pose the young infant to more rapiddehydration.
There are four basic pathophys-iologic processes that produce diar-rheal stools in children: secretory, cy-totoxic, osmotic, and dysenteric.Diarrhea may be a combination of oneor more of these processes.
Secretory Process
Acute secretory diarrhea is due toan enterotoxin produced by an infec-tious, metabolic, or exogenous toxicagent. The enterotoxin stimulates se-cretion of fluid and electrolytes fromthe mucosal crypt cells, the principalsecretory cells of the small bowel.This process is mediated throughprostaglandins and effects cyclicadenosine monophosphate, guano-sine monophosphate, and Ca2� ionflows. The enterotoxin also mayblock absorption of fluid and electro-lytes in the villus cells, which are theprincipal absorptive cells.
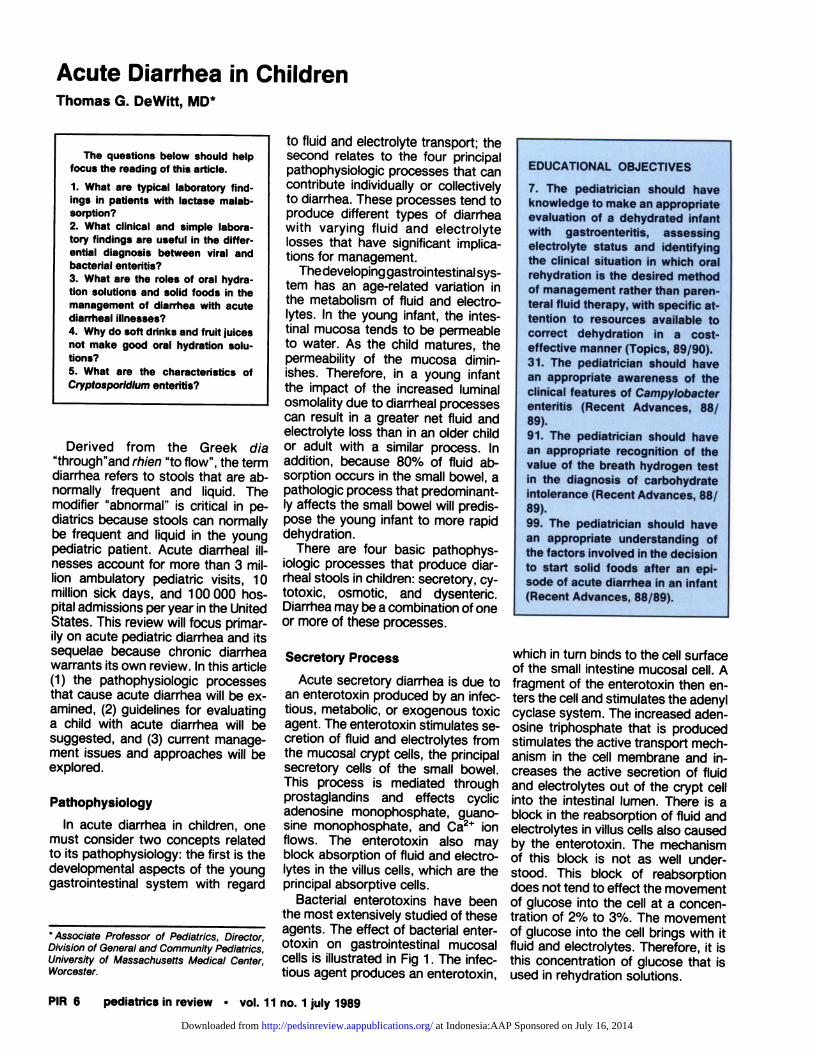
Bacterial enterotoxins have beenthe most extensively studied of theseagents. The effect of bacterial enter-otoxin on gastrointestinal mucosalcells is illustrated in Fig 1. The infec-tious agent produces an enterotoxin,
which in turn binds to the cell surfaceof the small intestine mucosal cell. Afragment of the enterotoxin then en-ters the cell and stimulates the adenylcyclase system. The increased aden-osine triphosphate that is producedstimulates the active transport mech-anism in the cell membrane and in-creases the active secretion of fluidand electrolytes out of the crypt cellinto the intestinal lumen. There is ablock in the reabsorption of fluid andelectrolytes in villus cells also causedby the enterotoxin. The mechanismof this block is not as well under-stood. This block of reabsorptiondoes not tend to effect the movementof glucose into the cell at a concen-tration of 2% to 3%. The movementof glucose into the cell brings with itfluid and electrolytes. Therefore, it isthis concentration of glucose that isused in rehydration solutions.
at Indonesia:AAP Sponsored on July 16, 2014http://pedsinreview.aappublications.org/Downloaded from
Bacterial diarrheas,particularly caused by
Campylobacter, Salmonella,and Shigella, primarily affect
the large bowel, producingfrequent, often bloody, stools
that usually containleukocytes.
Fig 1. Effect of bacteria! enterotoxin on muccsa! cells of the small intestine.
GASTROENTEROLOGY
pediatrics in review #{149}vol. 11 no. 1 july 1989 PIR 7
Cytotoxic Process
The cytotoxic process is character-ized by the destruction of the mu-cosal cells of the villi of the smallintestine, most commonly by an infec-tious viral agent. After cell lysis, thevilli shorten, and the mucosal surfacetakes on an appearance similar tothat seen in celiac disease. The func-tional effect of this process is to de-crease the surface area of the smallbowel, thereby decreasing the capa-bility of the small intestine to absorbfluid and electrolytes. In addition,most of the cells that remain are cryptcells, the principal secretory cells ofthe intestinal mucosa. In effect, thereis the same functional process as thatseen in secretory diarrhea with a pro-portional increase in the secretory
and a marked decrease in the ab-sorptive function of the small bowelmucosa.
Osmotic Process
Osmotic diarrhea is most com-monly seen in malabsorption syn-dromes, although the process func-tionally occurs with both secretoryand cytotoxic diarrheas because ofthe inability of the intestine in bothprocesses to absorb nutrients andelectrolytes normally. The most com-mon malabsorption syndrome is lac-tose intolerance due to the relativesensitivity of the lactase enzyme onthe mucosal cell brush border to anypathologic gastrointestinal process. Ifthe malabsorbed substance has a
high enough concentration to be Os-motically active, there is a net flux ofwater into the lumen resulting inloose, diarrheal stools. In many casesof osmotic diarrheal processes, thelarge bowel flora is inundated withincreased carbohydrate substratewhich is metabolized and producesgas, abdominal pain, and a de-creased stool pH.
Dysenteric Process
In dysentery there is inflammationof the mucosa and submucosa of theterminal ileum and the large bowel.The inflammation, most commonly
due to invasion by a bacterial agent,causes edema, mucosal bleeding,and leukocytic infiltration. Leuko-cytes and blood are exuded into thelumen of the intestine. Fluid absorp-tion, which is the principal activity ofthe large bowel, is decreased whichleads to liquid stools. The irritation ofthe inflammation causes increasedcolon motility and frequent stooling,often with tenesmus.
The types of diarrhea and the caus-ative agents thought to be most com-monly associated with these proc-esses are listed in Table 1 . Severalagents appear in two or more col-umns indicating that they may precip-itate several processes. Although thelongest list is in the secretory diarrheacolumn, the most common agents indeveloped countries are the patho-gens in the cytotoxic and dysentericcategories and include Rotavirus,Campylobacter, Salmonella, andShigella.
There is an alteration in the gas-trointestinal motility associated withthese processes. In secretory and cy-totoxic diarrhea, there is most oftena functional ileus, with a decrease inthe intestinal tone that slows peri-staltic movement through the intes-
at Indonesia:AAP Sponsored on July 16, 2014http://pedsinreview.aappublications.org/Downloaded from
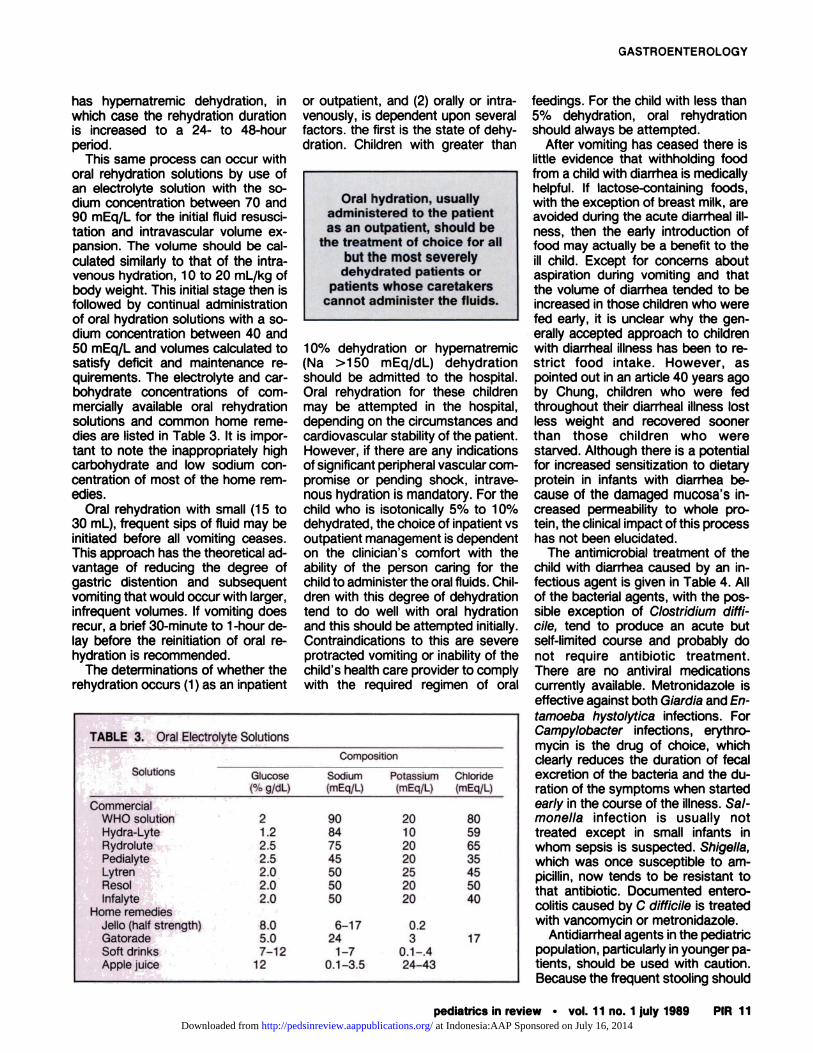
TABLE 1. Etiologic Agents inDiarrheal Processes
SecretoryEscherichia coli*Vibrio choleraeClostridium diffidileClostridium perfringensAeromonas hydrophilaStaphylococcus aureusVibrio parahaemolyticusBacillus cereusShigeilaSalmonellaYersinia enterocoilticaGiardia lambilaNeuroblastoma
CytotoxicRotavirus*Norwalk agentCryptosporidiumEscherichia coil
OsmoticLactose*Sorbitol
DysentericCampylobacter fetus*Clostridium diffidileSalmonellaShigellaYersinia enterocollticaEntamoeba histolytica
* Most common etiologic agent incategory.
�Campy Smear
+ fTreat if-Food Handler
or Incontinent
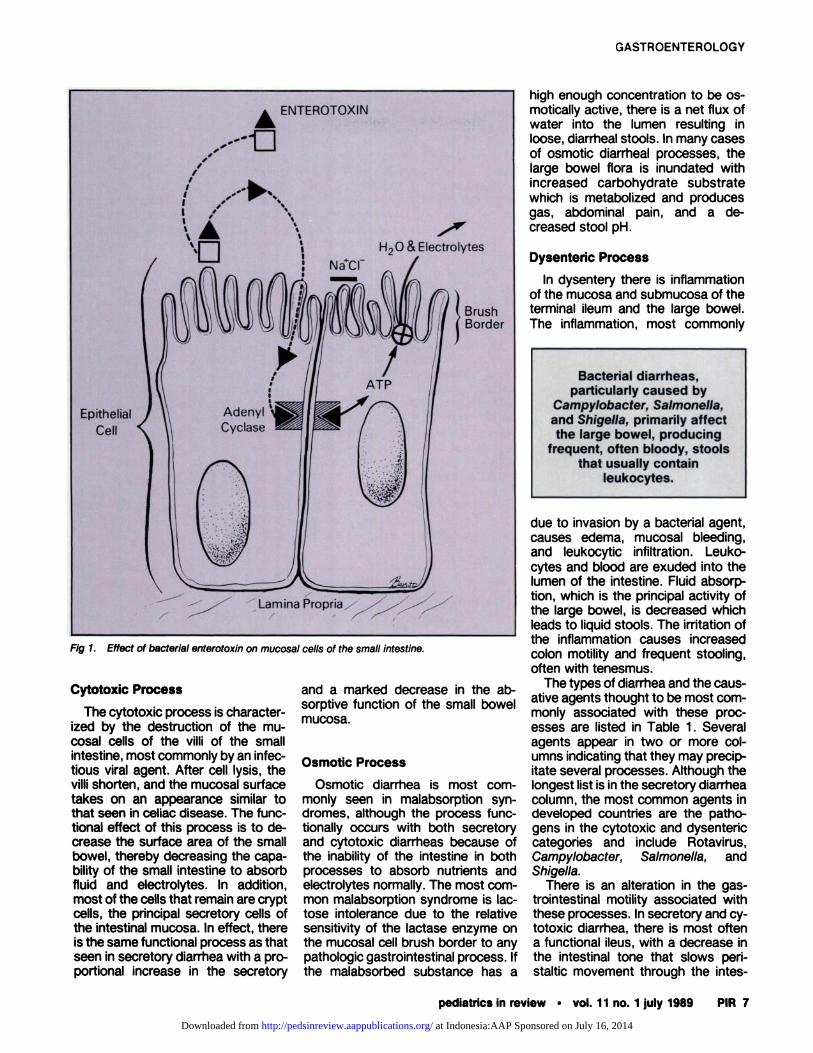
Fig 2. Algorithm for diagnostic evaluation of acute diarrhea. Adapted from Radetsky M. Labo-ratory evaluation of acute diarrhea. Pediatr Infect Dis. 1986;5:230-238 (used with permission).
Acute Diarrhea
PIR 8 pediatrics in review #{149} vol. 11 no. 1 july 1989
tines. This in turn causes (1) luminaldilation, leading to visceral abdominalpain and vomiting, (2) delayed gastricemptying, which may contribute tovomiting, and (3) rapid intestinal tran-sit time with marked peristalticrushes. In the dysenteric process,there is irritation of the colon by theinflammatory process, leading to fre-quent discharge and tenesmus. Pros-taglandins play a significant role inmediating functional ileus, althoughtheir role in the dysenteric process isnot clear.
EVALUATION
History
In diarrheal illness, the history andphysical examination serves as aninitial screen to narrow the diagnosticpossibilities. The choice of laboratorytests depends on the results of thehistory and physical examination. Be-cause most acute diarrhea in childrenis due to infectious agents, the focus
of this section will be primarily on thisetiology of acute diarrhea. Seasonalvariation is an important considera-tion because bacterial diarrheas tendto have their highest incidence inwarm seasons and the viral agentpredominates in cold seasons withRotavirus causing as much as 50%of the wintertime diarrhea in youngchildren and infants. A simple algo-rithmic approachto acute pediatricdiarrhea proposed by Radetsky andindependent of season is shown inFig 2. The initial steps are clearlyfocused on information from the his-tory and physical examination. Thespecial considerationsin this algo-rithm include malabsorption, immunecompromise, recent antibiotic use ortravel, neonatal patient, day care, andcommon outbreak.
The history, whether obtained fromthe phone conversation or during theinitial part of the office visit, needs tobe focused on assessing a child’sstate of hydration and the possiblecausative agents. Information regard-ing amount of oral intake; frequencyand volume of stool; general appear-ance of the child, especially with re-gard to hydration of lips; mental sta-
tus; and frequency of urination canhelp one assess general state of hy-dration. A history of markedly re-duced oral intake, particularly withlarge stool losses and decreased fre-quency of urination, should alert theclinician to the potential of significantdehydration. An altered mental stateis particularly worrisome, especially ifpersistent, and requires immediateevaluation. The history of dry lips is avariable sign of dehydration and maybe representative of high fever as wellas the state of hydration.
The patient or parent should beasked about fever, antibiotic therapy,exposure to day care or other chil-dren and adults with a diarrheal his-tory, ingestion of certain foods suchas raw milk and poorly prepared orstored poultry and salads, and ex-posure to other sources of potentialenterotoxin such as untreated watersources. A familial history of diarrhealillnesses, especially associated withinflammatory bowel disease of foodintolerance, should be obtained. Be-cause immuncompromised patientsrequire special consideration, infor-mation about this possibility shouldbe included.
at Indonesia:AAP Sponsored on July 16, 2014http://pedsinreview.aappublications.org/Downloaded from

Lactose intolerance is acommon side effect of many
diarrheal processes andneeds to be a consideration
in the management andfollow-up of any child with
acute diarrhea.
GASTROENTEROLOGY
pediatrics in review #{149}vol. 11 no. 1 july 1989 PIR 9
Two factors that may be particu-larly helpful in identifying the diarrhealetiology concern the history of vom-iting and the character and frequencyof the stool. The timing of the onsetof vomiting can aid in differentiating asmall vs large bowel process. Smallbowel processes, most commonlyassociated with viral agents, causedelayed gastric emptying and luminaldistention which often induces vom-iting before the onset of diarrhea.Processes involving the small boweltend to produce large volume, waterystools that are relatively infrequent.Conversely, large bowel involvement,usually due to a bacterial-induced in-flammatory process, tends to pro-duce frequent, less watery stools.
The history of bloody stools ishighly suggestive of a bacterial path-ogen, particularly in the older infantand child. Although a child withbloody diarrhea has at least a 50%chance of having a bacterial patho-gen, only one in three children withbacterial diarrhea will have bloodystools. In addition, in the infant lessthan 6 months of age, the most com-mon causes of blood in the stool arecow milk intolerance or anal fissures.
Diarrhea without concurrent fever,but with abdominal pain and greasyflatulent stools, is characteristic of a
malabsorptive process. A history ofacute diarrhea, followed by continuedor intermittently occurring episodesof loose stools, suggests malabsorp-tion. This is most commonly due tosecondary lactose intolerance, oftenexacerbated by the ingestion of milkor milk products. Excessive intake ofhigh carbohydrate fluids, such as ap-pie juice and nonabsorbable fillerssuch as sorbitol, may also lead tomalabsorptive diarrhea.
PHYSICAL EXAMINATION
The physical examination shouldbegin with a global assessment of the
child, paying particular attention tostate of hydration. Mucous mem-branes, more than the lips, should beevaluated for moistness. The appear-ance of the anterior fontanel and eyeswith regard to scaphoid presentationshould be assessed. The skin hydra-tion and turgor may give a sense ofthe degree of dehydration. The find-ing of doughy, tented skin is associ-ated with hypernatremic dehydration.Finally, the child’s mental status withregard to interaction with the exam-iner and parents can be used as ameasure of seriousness of illness anddehydration. The importance of thisglobal assessment is reflected in theYale Observation Scales for evaluat-ing critically ill children. Two of themajor components of these obser-vation scales are mental status andstate of hydration.
All children with diarrhea should becarefully weighed unclothed for corn-parison with previous weights and toprovide a baseline for monitoring sub-sequent weights during the course ofthedisease. Temperature, blood pres-sure, and pulse all may provide infor-mation concerning the degree of ill-ness. An elevated temperature in-creases insensible water loss andmay lead to more rapid dehydration.A decreased blood pressure, an ele-vated pulse, or decreased peripheralperfusion may indicate intravascularvolume loss due to dehydration. Therest of the physical examinationshould be focused on signs of con-current viral illness such as upperrespiratory tract infections that maybe associated with gastroenteritis, aswell as abdominal findings.
The abdominal examination shouldbegin with a general assessment ofwhether the abdomen is distended orscaphoid. The distended abdomenmay be associated with an ileus asseen in enteritis or gaseous dilationdue to malabsorption. The scaphoidabdomen may be associated with se-vere dehydration. Auscultation mayreveal the high pitched sounds of per-istaltic rushes found in the enteriticand secretory diarrheas. Signs of per-itonitis, which may cause diarrheadue to inflammation and local entericirritation, should be carefullyassessed. Dysenteric diarrheas tendto be associated with a more quietabdomen. A rectal examination is
often helpful in obtaining a stool sam-pIe for occult blood, culture, and ex-amination for leukocytes, pH, and re-ducing substances.
LABORATORY EVALUATION
The most crucial initial laboratoryevaluation that the clinician shouldconsider is related to the assessmentof degree of dehydration. Serum elec-trolytes, particularly sodium and bi-carbonate, should be assessed in anychild considered significantly dehy-drated. Knowing the serum sodiumconcentration is crucial when deter-mining the composition of the fluidsand rate of rehydration to be used ina child who is dehydrated. Knowingthe bicarbonaate level aids in deter-mining the degree of dehydration. Astissue perfusion decreases with in-creasing dehydration, the amount oflactic acid buildup in peripheral tissueincreases and the bicarbonate con-centration decreases. Serum ob-tamed by venipuncture and bicarbon-ate concentration measured by mul-tichannel laboratory analysis tends tobe less than serum bicarbonate cal-culated from an arterial or venousblood gas sample. If the bicarbonateconcentration seems disproportion-ately low in the context of the rest ofthe child’s assessment, a venousblood gas analysis may be helpful inclarifying this disparity. A markedlyelevated BUN concentration with arelatively normal creatinine value mayindicate recent or rapid dehydration.Serum creatinine concentrations tendto be low in infants and young chil-dren and a creatine value of 1 mg/dLin this age group may represent adoubling of the normal value. A un-nalysis for specific gravity as well asthe presence of leukocytes, ketones,and crystalline material should be ob-tamed for any child considered to bedehydrated. Because urinary tract in-fections in children may be associ-ated with diarrhea, a urine cultureshould be performed if there are leu-koyctes in the urine.
Examination of the stool may helpdetermine the differential diagnosisbut is of little use in determining de-gree of dehydration. Although occultblood in the stool may be present insmall infants with excoriated penianalareas, the appearance of gross blood
at Indonesia:AAP Sponsored on July 16, 2014http://pedsinreview.aappublications.org/Downloaded from
TABLE 2. Stool LeukocyteAssessment
1. Obtain small amount of stool,preferably with mucus.
2. Smear thinly on microscopeslide.
3. Add drop of methylene blueand apply coverslip.
4. Scan with low-power lens(lOx) and then examine underhigh power (40x).
5. Presence of a high-power fieldwith >5 leukocytes is consid-ered positive result.
Acute Diarrhea
PIR 10 pediatrics in review #{149}vol. 11 no. 1 july 1989
in the stool is diagnostically impor-tant. A distinctively abnormal stoolodor or lack thereof, as is often thecase in small bowel involvement, mayhelp differentiate the etiology, butthat diagnostic test is best left toknowledgeable noses. The presenceor absence of reducing substanceand the stool pH have not consist-ently been shown to clarify the differ-ential diagnosis of acute infectiousdiarrhea. However, the presence ofreducing substances and a low pHare indicative of malabsorption. Thepresence of mucus is commonly as-sociated with bacterial diarrheas.
The presence of stool leukocytesis helpful in identifying bacterial diar-rhea, especially those causing a dy-senteric process. Patients with leu-kocytes in their diarrheal stools haveapproximately a 70% chance of hay-ing a bacterial infection. Moreover, asmany as 90% of patients with bacte-rial dysentery have leukocytes in theirstools. Thus, presence of stool leu-kocytes has both a high-positive pre-dictive value and a high sensitivity forbacterial diarrhea. The method for as-sessing stool leukocyte content isnoted in Table 2.
Stool for culture should be ob-tained if the history and stool exami-nation strongly suggest a bacterialcause. A fresh sample of stool in aclean, if not sterile, container is pre-ferred for accurate culture results.However, a well-soaked rectal swab,two or three if possible, in transportmedia is usually sufficient. Fresh stoolfor ova and parasites should be ex-amined, especially when Giardia lam-b/ia or Cryptosporidium is suspected,as would be the case in the diarrheal
outbreak in a day-care setting. Aninitial identification of Cryptospori-dium can be done by examining aniodine-stained wet mount of centni-fuged stool for oocysts, which appearas unstained oval structures. If pre-sent, a definitive assessment with amodified acid-fast stain should beperformed. In the immunocompro-mised child, special considerationmust be given to culturing for an arrayof organisms that may becomepathogenic in such a host.
In recent years, several rapid testshave been developed to identify infec-tious agents, eg, the latex fixationtest and enzyme-linked immune as-says for Rotavirus. Of potential helpto the clinician in the near future maybe similar diagnostic tests being de-veloped for bacterial pathogens in-cluding Salmonella, Shigella andCampylobacter. Campylobacter, themost common cause of bacterial diar-rhea in young children as well asadults, may be rapidly identified bypresence of the characteristic Gram-negative vibnio, “gull wing,” orga-nisms in a gram-stained stool sample.
Although some malabsorption iscommonly associated with most diar-rheal processes, when it is the prin-cipal diagnosis being considered,there are a series of laboratory as-sessments that can be useful. Thesimplest and quickest are for stoolpH and reducing substances. A lowpH and the presence of reducing sub-stances suggest malabsorption. Inthe infrequent cases in which the diar-rhea is prolonged, more complextests can be subsequently per-formed. One of the most commonlyused tests today is the noninvasivebreath hydrogen lactose tolerancetest. In lactose intolerance, there isan increase in breath hydrogen ap-proximately 2 hours after administra-tion of a standard oral lactose doseas the malabsorbed lactose is metab-olized to hydrogen gas by the flora ofthe large intestine, transported to thelungs, and exhaled. A minimal in-crease in breath hydrogen usually in-dicates that lactose intolerance is un-likely, whereas an early increase inbreath hydrogen may suggest othersmall bowel pathologic process suchas bacterial overgrowth. Further elu-cidation of small bowel disease canbe pursued with a o-xylose absorp-
tion test by which the integrity of thesmall bowel mucosa is assessed.One hour after an oral dose of xyloseis administered, a single determina-tion of serum xylose is made. In proc-esses such as small bowel bacterialovergrowth, celiac disease, and re-gional entenitis, the damaged mucosais unable to absorb xylose normallyand the 1-hour serum level is low. Ifthe D-xylOse test result is positive,additional evaluation, including bi-opsy and diagnostic imaging studies,should be considered. However,most tests for the evaluation of smallintestinal integrity and functionshould be reserved for the work-upof chronic or recurring diarrhea.
MANAGEMENT
The use of oral hydration solutionsrepresents the greatest advance inthe treatment of diarrhea in the past15 years. Prior to the introduction anddemonstrated efficacy of the WorldHealth Organization oral rehydrationsolution, intravenous hydration wasthe only accepted treatment for sig-nificantly dehydrated children. Pa-tients were hospitalized, given noth-ing by mouth, resuscitated with intra-venous fluid, and then gradually givenincreased amounts of oral fluids. Ifdiarrhea recurred, as it almost inevit-ably did, the oral intake was reducedand intravenous hydration was con-tinued. An understanding of thepathophysiologic process mentionedpreviously has dramatically changedthis approach. Use of oral rehydrationsolutions with appropriate concentra-tions of glucose (approximately 2%)and varying concentrations of elec-trolytes as appropriate for the stageof rehydration has significantly de-creased the need for inpatient, intra-venous hydration.
The first stage of intravenous re-hydration classically consists of arapid infusion of an isotonic solutionto expand the intravascular volumeusually given at a rate of 1 0 to 20mL/kg of body weight throughout a1- to 2-hour period. Subsequent in-travenous hydration is a combinationof replacement of the estimated fluidloss based on the degree of dehydra-tion added to the regular mainte-nance needs. This should occurthroughout 16 hours, unless the child
at Indonesia:AAP Sponsored on July 16, 2014http://pedsinreview.aappublications.org/Downloaded from
Oral hydration, usuallyadministered to the patientas an outpatient, should be
the treatment of choice for allbut the most severely
dehydrated patients orpatients whose caretakers
cannot administer the fluids.
�Commerdal-!WHO solulHydra-Lb -� =
RydrolutePediaIyte�!Lytren�ResolInfalyte
Home remedJello (half �GatoradeSoft drinkSAp�
GASTROENTEROLOGY
pediatrics in review #{149}vol. 11 no. 1 july 1989 PIR 11
has hypematremic dehydration, inwhich case the rehydration durationis increased to a 24- to 48-hourperiod.
This same process can occur withoral rehydration solutions by use ofan electrolyte solution with the so-dium concentration between 70 and90 mEq/L for the initial fluid resusci-tation and intravascular volume ex-pansion. The volume should be cal-culated similarly to that of the intra-venous hydration, 10 to 20 mL/kg ofbody weight. This initial stage then isfollowed by continual administrationof oral hydration solutions with a so-diurn concentration between 40 and50 mEq/L and volumes calculated tosatisfy deficit and maintenance re-quirements. The electrolyte and car-bohydrate concentrations of corn-mercially available oral rehydrationsolutions and common home reme-dies are listed in Table 3. It is impor-tant to note the inappropriately highcarbohydrate and low sodium con-centration of most of the home rem-edies.
Oral rehydration with small (15 to30 mL), frequent sips of fluid may beinitiated before all vomiting ceases.This approach has the theoretical ad-vantage of reducing the degree ofgastric distention and subsequentvomiting that would occur with larger,infrequent volumes, If vomiting doesrecur, a brief 30-minute to 1-hour de-lay before the reinitiation of oral re-hydration is recommended.
The determinations of whether therehydration occurs (1) as an inpatient
or outpatient, and (2) orally or intra-venously, is dependent upon severalfactors. the first is the state of dehy-dration. Children with greater than
10% dehydration or hypematremic(Na >150 mEq/dL) dehydrationshould be admitted to the hospital.Oral rehydration for these childrenmay be attempted in the hospital,depending on the circumstances andcardiovascular stability of the patient.However, if there are any indicationsof significant peripheral vascular corn-promise or pending shock, intrave-nous hydration is mandatory. For thechild who is isotonically 5% to 10%dehydrated, the choice of inpatient vsoutpatient management is dependenton the clinician’s comfort with theability of the person caring for thechild to administer the oral fluids. Chil-dren with this degree of dehydrationtend to do well with oral hydrationand this should be attempted initially.Contraindications to this are severeprotracted vomiting or inability of thechild’s health care provider to complywith the required regimen of oral
feedings. For the child with less than5% dehydration, oral rehydrationshould always be attempted.
After vomiting has ceased there islittle evidence that withholding food
- from a child with diarrhea is medicallyhelpful. If lactose-containing foods,with the exception of breast milk, are
� avoided during the acute diarrheal ill-ness, then the early introduction offood may actually be a benefit to theill child. Except for concerns aboutaspiration during vomiting and thatthe volume of diarrhea tended to beincreased in those children who werefed early, it is unclear why the gen-erally accepted approach to childrenwith diarrheal illness has been to re-strict food intake. However, aspointed out in an article 40 years agoby Chung, children who were fedthroughout their diarrheal illness lostless weight and recovered soonerthan those children who werestarved. Although there is a potentialfor increased sensitization to dietaryprotein in infants with diarrhea be-cause of the damaged mucosa’s in-creased permeability to whole pro-tein, the clinical impact of this processhas not been elucidated.
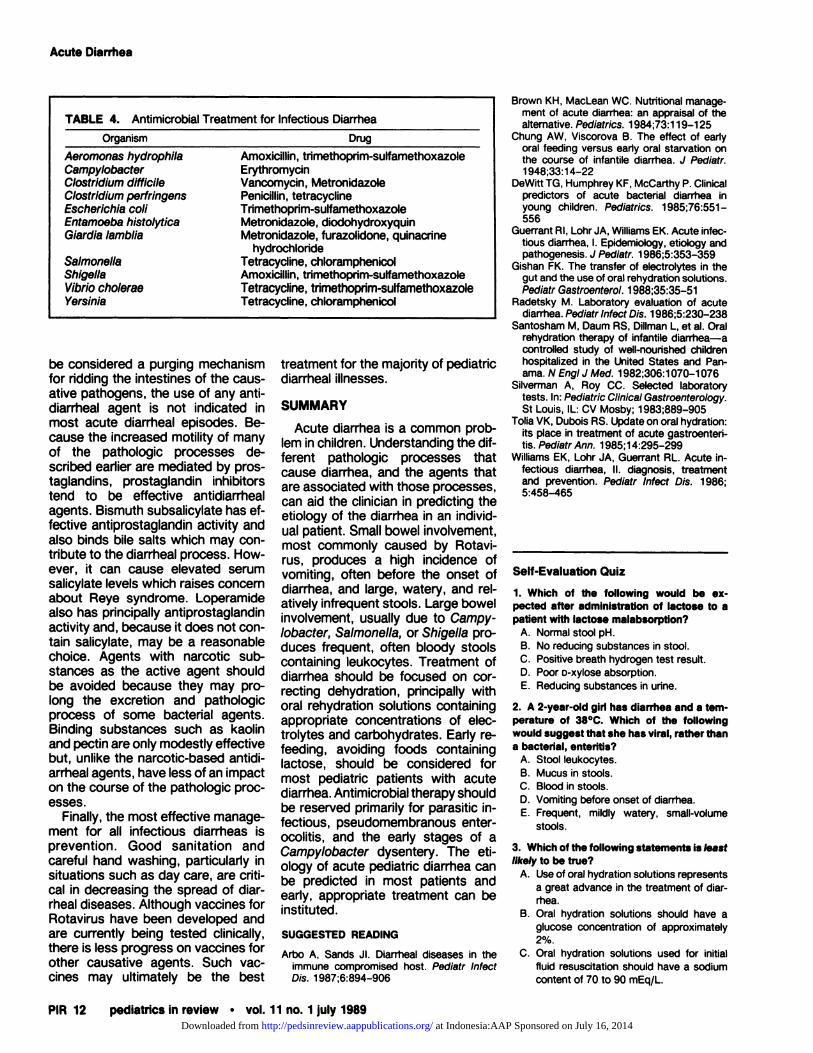
The antimicrobial treatment of thechild with diarrhea caused by an in-factious agent is given in Table 4. Allof the bacterial agents, with the pos-sible exception of Clostridium diffi-dile, tend to produce an acute butself-limited course and probably donot require antibiotic treatment.There are no antiviral medicationscurrently available. Metronidazole iseffective against both Giardia and En-tamoeba hystolytica infections. ForCampylobacter infections, erythro-mycin is the drug of choice, whichclearly reduces the duration of fecalexcretion of the bacteria and the du-ration of the symptoms when startedearly in the course of the illness. Sal-monella infection is usually nottreated except in small infants inwhom sepsis is suspected. Shigella,which was once susceptible to am-picillin, now tends to be resistant tothat antibiotic. Documented entero-colitis caused by C diffidile is treatedwith vancomycin or metronidazole.
Antidiarrheal agents in the pediatricpopulation, particularly in younger pa-tients, should be used with caution.Because the frequent stooling should
at Indonesia:AAP Sponsored on July 16, 2014http://pedsinreview.aappublications.org/Downloaded from
Organism
TABLE 4. Antimicrobial Treatment for Infectious Diarrhea
Aeromonas hydrophilaCampylobacterClostridium diffidileClostridium perfringensEscherichia coilEntamoeba histolyticaGiardia lambila
Drug
SalmonellaShigellaVibrio cho/eraeYersinia
Amoxicillin, trimethopnm-sulfamethoxazoleErythromycinVancomycin, MetronidazolePenicillin, tetracyclineTrimethoprim-sulfamethoxazoleMetronidazole, diodohydroxyquinMetronidazole, furazolidone, quinacrine
hydrochlorideTetracydine, chloramphenicolAmoxicillin, trimethoprim-sulfamethoxazoleTetracycline, tnmethoprim-sulfamethoxazoleTetracycline, chioramphenicol
Acute Diarrhea
PIR 12 pediatrics in review #{149}vol. 11 no. 1 july 1989
be considered a purging mechanismfor ridding the intestines of the caus-ative pathogens, the use of any anti-diarrheal agent is not indicated inmost acute diarrheal episodes. Be-cause the increased motility of manyof the pathologic processes de-scnibed earlier are mediated by pros-taglandins, prostaglandin inhibitorstend to be effective antidiarrhealagents. Bismuth subsalicylate has ef-fective antiprostaglandin activity andalso binds bile salts which may con-tribute to the diarrheal process. How-ever, it can cause elevated serumsalicylate levels which raises concernabout Reye syndrome. Loperamidealso has principally antiprostaglandinactivity and, because it does not con-tam salicylate, may be a reasonablechoice. Agents with narcotic sub-stances as the active agent shouldbe avoided because they may pro-long the excretion and pathologicprocess of some bacterial agents.Binding substances such as kaolinand pectin are only modestly effectivebut, unlike the narcotic-based antidi-arrheal agents, have less of an impacton the course of the pathologic proc-esses.
Finally, the most effective manage-ment for all infectious diarrheas isprevention. Good sanitation andcareful hand washing, particularly insituations such as day care, are criti-cal in decreasing the spread of diar-rheal diseases. Although vaccines forRotavirus have been developed andare currently being tested clinically,there is less progress on vaccines forother causative agents. Such vac-cines may ultimately be the best
treatment for the majority of pediatric
diarrheal illnesses.
SUMMARY
Acute diarrhea is a common prob-lem in children. Understanding the dif-ferent pathologic processes thatcause diarrhea, and the agents thatare associated with those processes,can aid the clinician in predicting theetiology of the diarrhea in an individ-ual patient. Small bowel involvement,most commonly caused by Rotavi-rus, produces a high incidence ofvomiting, often before the onset ofdiarrhea, and large, watery, and rel-atively infrequent stools. Large bowelinvolvement, usually due to Campy-/obacter, Salmonella, or Shigella pro-duces frequent, often bloody stoolscontaining leukocytes. Treatment ofdiarrhea should be focused on con-recting dehydration, principally withoral rehydration solutions containingappropriate concentrations of elec-trolytes and carbohydrates. Early re-feeding, avoiding foods containinglactose, should be considered formost pediatric patients with acutediarrhea. Antimicrobial therapy shouldbe reserved primarily for parasitic in-fectious, pseudomembranous enter-ocolitis, and the early stages of aCampylobacter dysentery. The eti-ology of acute pediatric diarrhea canbe predicted in most patients andearly, appropriate treatment can beinstituted.
SUGGESTED READING
Arbo A, Sands JI. Diarrheal diseases in theimmune compromised host. Pediatr InfectDis. 1987;6:894-906
Brown KH, MacLean WC. Nutritional manage-ment of acute diarrhea: an appraisal of thealternative. Pediatrics. 1984;73:1 19-125
Chung AW, Viscorova B. The effect of earlyoral feeding versus early oral starvation onthe course of infantile diarrhea. J Pediatr.1948;33:1 4-22
DeWitt TG, Humphrey KF, Mccarthy P. clinicalpredictors of acute bacterial diarrhea inyoung children. Pediatrics. 1985;76:551 -
556Guerrant RI, Lohr JA, Williams EK. Acute infec-
tious diarrhea, I. Epidemiology, etiology andpathogenesis. J Pediatr. 1986;5:353-359
Gishan FK. The transfer of electrolytes in thegut and the use of oral rehydration solutions.Pediatr Gastroenterol. 1988;35:35-51
Radetsky M. Laboratory evaluation of acutediarrhea. Pediatr Infect Dis. 1986;5:230-238
Santosham M, Daum AS, Dillman L, et al. Oralrehydration therapy of infantile diarrhea-acontrolled study of well-nourished childrenhospitalized in the United States and Pan-ama. N EngI J Med. 1982;306:1 070-1 076
Silverman A, Roy cc. Selected laboratorytests. In: Pediatric CllnicalGastroenterology.St Louis, IL: CV Mosby; 1983;889-905
Tolia VK, Dubois AS. Update on oral hydration:its place in treatment of acute gastroenteri-tis. Pediatr Ann. 1985;14:295-299
Williams EK, Lohr JA, Guerrant AL. Acute in-fectious diarrhea, II. diagnosis, treatmentand prevention. Pediatr Infect Dis. 1986;5:458-465
Self-Evaluation Quiz
1. Which of the following would be cx-pected after administration of lactose to apatient with lactose malabsorption?
A. Normal stool pH.B. No reducing substances in stool.C. Positive breath hydrogen test result.
D. Poor D-xylOSe absorption.E. Reducing substances in urine.
2. A 2-year-old girl has diarrhea and a tem-perature of 38#{176}C.Which of the followingwould suggest that she has viral, rather thana bacterial, enteritis?
A. Stool leukocytes.B. Mucus in stools.C. Blood in stools.
0. Vomiting before onset of diarrhea.E. Frequent, mildly watery, small-volume
stools.
3. Which of the following statements is leastlikely to be true?
A. Use of oral hydration solutions representsa great advance in the treatment of diar-rhea.
B. Oral hydration solutions should have aglucose concentration of approximately2%.
C. Oral hydration solutions used for initial
fluid resuscitation should have a sodiumcontent of 70 to 90 mEq/L.
at Indonesia:AAP Sponsored on July 16, 2014http://pedsinreview.aappublications.org/Downloaded from

DOI: 10.1542/pir.11-1-61989;11;6Pediatrics in Review
Thomas G. DeWittAcute Diarrhea in Children
ServicesUpdated Information &
http://pedsinreview.aappublications.org/content/11/1/6including high resolution figures, can be found at:
Permissions & Licensing
http://pedsinreview.aappublications.org/site/misc/Permissions.xhtmlentirety can be found online at: Information about reproducing this article in parts (figures, tables) or in its
Reprintshttp://pedsinreview.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
at Indonesia:AAP Sponsored on July 16, 2014http://pedsinreview.aappublications.org/Downloaded from
Hypoglycemia
PIR 124 pediatrics in review #{149} vol. 11 no.4 october 1989
REFERENCES
1 . Chaussain JL. Glycemic response to 24hour fast in normal children and childrenwith ketotic hypoglycemia. J Pediatr.1973;82:438-443
2. Gutberlet AL, Comblath M. Neonatal hy-poglycemia revisited, 1975. Pediatrics.1976;58:1 0-17
3. Stanley CA, Baker L. Hyperinsulinism ininfancy: diagnosis by demonstration of ab-normal response to fasting hypoglycemia.Pediatrics. 1976;57:702-71 1
4. Phillip M, Bashan N, Smith CP, Moses SW.An algorithmic approach to diagnosis ofhypoglycemia. J Pediatr. 1987;1 10:387-390
5. Witte DP, Greider MH, DeSchryver-Kec-skemeti K, Kissane JM, White NH. Thejuvenile human endocrine pancreas: nor-mal v idiopathic hypennsulinemic hypogly-cemia. Semin Diag Pathol. 1984;1 :30-42
6. Chaussain J-L, Georges P, Gendrel D,Donnadieu M, Job J-C. Serum branched-chain amino acids in the diagnosis of hy-perinsulinism in infancy. J Pediatr.1980;96:923-926
7. Finegold DN, Stanley CA, Baker L. Gly-cemic response to glucagon during fastinghypoglycemia: an aid in the diagnosis ofhyperinsulinism. J pediatr. 1980;96:257-259
8. Kramer JL, Bell MJ, DeSchryver K, BowerRJ, Temberg JL, White NH. Clinical andhistologic indications for extensive pan-creatic resection in nesidioblastosis. Am J
Surg. 1982;143:1 16-1199. Lee PA, Mazur T, Danish A, et al. Micro-
penis, I. criteria, etiologies and classifica-tion. Johns Hopkins Med J. 1980;146:156-164
10. Chen Y-T, Comblath M, Sidbury JB. Corn-starch therapy in type I glycogen storagedisease. N EngI J Med. 1984;310:171-175
SUGGESTED READING
Aynsley-Green A, Soltesz G. Hypoglycaemiain Infancy and Childhood. London, England:Churchill-Livingstone; 1985
Comblath M, Schwartz A, eds. Disorders ofCarbohydrate Metabolism in Infancy. Phila-delphia, PA: WB Saunders; 1976
Self-Evaluation Quiz
10. In the evaluation of hypoglycemia in ayoung child, the least likely helpful diagnos-tic test among the following would be:
A. Oral glucose tolerance test.B. Serum ketones level.C. Serum lacticacad level.D. Plasma insulin level.E. Plasma level of growth hormone.
11. In an infant with hypoglycemia, simul-taneous measurement of serum glucoseand growth hormone levels 4 hours after a
feeding, at a time when the infant wassymptmatic, found both levels to be abner-mally low. These findings suggest that theprimary defect is most likely to be:
A. Hyperinsullnism.B. Hypopituitansm.C. Glycogen storage disease, type I (von
Gierke).D. Accelerated fasting.E. Phosphoenolpyruvate carboxykinase de-
ficiency.
12. In an infant or child with postprandlalhypoglycemia, among the following findingsthe least likely is:A. Weakness.B. Tremor.
C. Pallor.0. Bradycardia.E. Cold sweat.
13. An infant with hypoglycemia has appar-ently suppressed serum levels of insulin andappropriately elevated levels of ketones ata time when she is symptomatic as a resuftof hypoglycemia. These findings suggestthat among the following her primary con-dition is most likely to be:
A. A disorder of fatty acid metabolism.B. Camitine deficiency.C. Glycogen storage disease, type I.D. Hypennsulinism.E. Hypopituitarism.
Department of Corrections
In the article by Dewitt in the July 1989 issue of Pediatrics in Review, “AcuteDiarrhea in Children,” itisunfortunatethatinTable 3 on page lithe spelling of therehydration solution “Rehydralyte” was printed as “Rydrolute.” In addition, Hydra-Lyteand Infalyte are no longer marketed.