pediatric respiratory medicine || sleep-disordered breathing
TRANSCRIPT
12
943
P A R T 12STRUCTURAL AND MECHANICAL ABNORMALITIES
CHAPTER65 Sleep-Disordered BreathingKaren Ann Waters
OVERVIEW
Airway collapse and hypoventilation are conditions that are potentiated during normal sleep. Pediatric sleep units under-take comprehensive diagnostic studies during sleep to evaluate these and other forms of respiratory dysfunction. Interpretation of these studies requires an understanding of the dynamics of the upper airway and of respiratory control along with their developmental interactions with sleep. Accu-rate evaluation of sleep-associated respiratory abnormalities in children, using detailed clinical and investigative proce-dures, should include an assessment of the underlying pathology.
Obstructive sleep apnea (OSA) is the most common sleep-associated breathing disorder in children. A number of syndromes and malformations are associated with particular sleep-associated diagnoses, including increased risk for OSA. The other major diagnostic group is children with congenital and acquired hypoventilation syndromes. Respiratory failure during sleep is common in association with complex airway abnormalities, chronic lung disease, neuromuscular disorders, as well as congenital or acquired neurologic conditions leading to central hypoventilation.
Treatment of these sleep-associated respiratory disorders ranges from medical therapy to invasive ventilation. Treat-ment of childhood OSA includes medical and surgical thera-pies. Perioperative assessment and management is an important component of the therapeutic intervention. Pres-sure support therapies, including nocturnal ventilation to treat hypoventilation, can now be routinely delivered by nasal
mask interfaces that are gaining wide application in pediatrics.
This chapter examines the current knowledge of OSA and sleep-associated hypoventilation in children. The normal pathology and the pathophysiology underlying sleep-related respiratory abnormalities are explored. Methods for identify-ing these disorders and their complications are discussed. The fi nal section describes treatment modalities available for these disorders, with discussion of the circumstances in which various treatments should be implemented.
PREVALENCE
OSA can occur in all age groups from infancy to adulthood. The best studies of the prevalence of childhood OSA include questionnaires that are combined with some overnight moni-toring (most commonly oximetry). The reported prevalence of habitual snoring in children varies from 3.2% to 15% of children. 1-3 Although the age groups included and the criteria for diagnosing OSA vary among studies, approximately 25% of children who snore habitually have clinically signifi cant OSA. Prevalence estimates for OSA in children range from 0.6% to 10.3%. 4,5
Hypoventilation is less common, but among children younger than 18 years, the causes of hypoventilation pub-lished from France include neuromuscular disease (34%), OSA and/or craniofacial abnormalities (30%), cystic fi brosis (17%), congenital hypoventilation (9%), scoliosis (8%), and other disorders (2%). 6 All studies that have reviewed the problem conclude that the number of patients currently ventilated is an underestimate of those who require the therapy. The best estimate of the incidence of sleep associ-ated hypoventilation is a Swedish study, showing an overall incidence of 6.6 to 9.6 per 100,000. 7 However, independent studies suggest that congenital central hypoventilation syndrome (CCHS) has an estimated incidence of 1 per 200,000. 8 Assuming that CCHS comprises 9% of all ventilated children in France, the upper incidence of children requiring ventilation should be closer to 22.2 per 100,000.
PATHOPHYSIOLOGY
Upper Airway Muscles and Mechanisms of Obstruction
The upper airway extends from the nares to the larynx. From the nasopharynx to the glottis, it is a pliable tube, with walls made up of soft tissue supported only by muscle so that the
TEACHING POINTS
● Obstructive sleep apnea is the most common sleep-associ-ated breathing disorder in children.
● Pathologies underlying obstructive sleep apnea include airway structure and obesity.
● Physiologic changes that occur during sleep contribute to the associated respiratory dysfunction.
● Other respiratory disorders often deteriorate in sleep due to loss of accessory muscle activity, especially in rapid eye movement sleep.
● Disorders of respiratory control (e.g., congenital central hypoventilation syndrome) show most serious blood gas derangements in slow wave sleep.
● Treatments for obstructive sleep apnea include medical, surgical, and noninvasive pressure support.
Ch065-A04048.indd 943Ch065-A04048.indd 943 1/18/2008 3:55:09 PM1/18/2008 3:55:09 PM

P A R T 12 ■ STRUCTURAL AND MECHANICAL ABNORMALITIES
12
944
caliber of the airway can change with simple events, such as a change in head position. 9 Most postnatal changes in the size of the airway occur during the fi rst year of life and during the pubertal growth spurt. However, during growth the airway soft tissue maintains proportionality with the facial skeleton. 10 Genioglossus activity is important in maintaining airway patency during sleep and responses vary between chil-dren with OSA compared to those without. 11-13 Upper airway refl exes protect airway patency by adjusting various muscle activities to suit the prevailing respiratory needs, and the importance of their activity in children with sleep apnea is demonstrated by changing responses after the application of topical anesthetic. 11 As refl ected by these studies of genio-glossus activity, the process of maintaining airway patency requires continuously responsive muscle function and upper airway patency is maintained by the dynamic interaction of muscle activity and airway size in both wakefulness and sleep. With sleep onset, there is relaxation of all postural muscles, including those of the upper airway. The activity of these muscles and the refl exes controlling them are blunted dra-matically by onset of sleep, although the changes are least in slow wave sleep (SWS) and greatest in rapid eye movement (REM) sleep. 14
Neural Control of the Upper Airway
Respiratory rhythm arises in the brainstem. The cells control-ling respiration have been isolated in the medulla to the region of the pre-Bötzinger complex and the associated dorsal and ventral respiratory neuronal groups. 15,16 The dorsal respi-ratory group has primary output. Output from the ventral respiratory group is modulated within the dorsal group before the fi nal integrated output. Neurons that drive the muscles of both the respiratory pump (diaphragm and accessory muscles) and the upper airway are intimately connected with those producing respiratory rhythm. 17 These respiratory centers also have intimate connections with the reticular activating system, with pontine infl uences particularly rele-vant during REM sleep. 18 The rates of development and myelination are not uniform among these neural centers, and the changing physiologic correlates during development are not well delineated.
The muscles of the upper airway are dynamically con-trolled throughout the respiratory cycle through coordination of these respiratory neuronal connections. Phasic activity of upper airway muscles can be demonstrated during normal respiration. The genioglossus is the major upper airway dilator muscle and is active during inspiration. 19 During infancy, there is active braking at the larynx during expiration. 20,21 Increased respiratory demand results in augmentation of normal respiratory activity, along with the additional recruit-ment of accessory muscles including the sternomastoid and the abdominal muscles. 22
Refl exes Protecting the Upper Airway from Obstruction
During sleep, upper airway responses to negative pressure and to hypercapnia are preserved in normal children, although infants appear to have a different pattern of upper airway activation than older children. 23 In infants, the airway is
generally stable, but the tendency to close with experimental occlusions refl ects the occurrence of spontaneous occlusions. 24
Intact brainstem refl ex pathways are vital for the preven-tion and/or rapid recovery from sleep-associated airway obstruction. These refl ex pathways involve many intercon-nections between sensory inputs from the oropharynx and chemoreceptors, the respiratory drive, the reticular activating system, and the motor neurons of the upper airway muscu-lature. 25 The afferent supply to the upper airway and larynx is mostly provided by the trigeminal, glossopharyngeal, and vagus nerves.
Arousal is an important culmination of these protective intercommunications. 26 This may be in response to chemo-receptor, mechanoreceptor, or local upper airway refl ex responses during sleep or simply due to increased ventilation whatever the primary stimulus. 27 Children with sleep apnea have increased arousals, but can also respond to airway obstruction with increased motor activity without the need for cortical arousal to occur, as they show an apparent lack of cortical arousal in response to airway obstruction. 28,29 It is possible that arousal occurs but at a level that is not seen on traditional investigative procedures, and a pattern of hierar-chical noncortical arousals has been demonstrated in infants. 30 Prior sleep defi cit, such as may occur with sleep apnea, also increases arousal thresholds, even in infants. 31
Local and brainstem refl exes act to protect upper airway patency. 19 Laryngeal receptors respond directly to increased CO2 and temperature. Rapidly adapting receptors have been identifi ed within the oropharynx that produce increases in both upper airway and diaphragm muscle activity in response to vibration with frequencies similar to snoring. 32 Local receptors in the distribution of the trigeminal nerve respond specifi cally to respiratory stimuli. 33 The laryngeal chemorefl ex and other local airway refl exes may contribute to the protective responses preventing upper airway obstruction. 34
Muscle activity from the upper airway muscles (particu-larly hypoglossal) may increase or decrease in the presence of airway obstruction, depending on the timing of the stimu-lus during inspiration. 19 Increased activity is seen during both inspiratory and expiratory phases of the respiratory cycle, although the level of response is dependent on sleep/wake state and is increased when there is increased CO2. 35 This increase in the electromyogram (EMG) signals may be used to quantify the severity of the obstruction in children and infants where recruitment of the genioglossus during airway occlusion is preserved during sleep, including REM/active sleep. 22
Developmental Aspects of Respiratory and Airway Control; Age-Related Disorders
In infants, refl ex responses to upper airway obstruction may produce apnea rather than respiratory stimulation. Laryngeal refl exes can produce life-threatening apnea in young animals, particularly in the presence of infections that damage the upper airway epithelium. 36 Infants have a predominance of inhibitory refl exes, and prolonged apnea has been docu-mented in infants in the presence of nasopharyngitis and common sedatives. 36,37 It is likely that there is associated
Ch065-A04048.indd 944Ch065-A04048.indd 944 1/18/2008 3:55:09 PM1/18/2008 3:55:09 PM
CHAPTER 65 ■ Sleep-Disordered Breathing
12
945
infl ammation or damage to sensory pathways within the epi-thelium or damage within the carotid bodies. Central apnea may also occur in response to upper airway obstruction, rather than increased respiratory effort. Hypercapnia is asso-ciated with recruitment of accessory muscles during non-REM (NREM) sleep, so ventilatory responses are less effective in REM sleep. 38 Although the initial apnea is mediated via vagal refl ex pathways, for example, following a sigh, other factors contribute to the ongoing respiratory rhythm oscillation. 39
Brainstem chemoreceptors change with development and are made more unstable by environmental changes such as altered ambient temperature. Ventilatory response testing in infants shows variability of the ventilatory response to hypoxia, although it tends to be biphasic and consistent between sleep states. 28 Ventilatory responses to changes in CO2 levels mature faster than responses to hypoxia, where inconsistent responses are frequently observed, and a large number of apparently normal infants fail to arouse during hypoxia, especially during SWS. 28,40
RELATIONSHIP OF AIRWAY OBSTRUCTION TO SLEEP
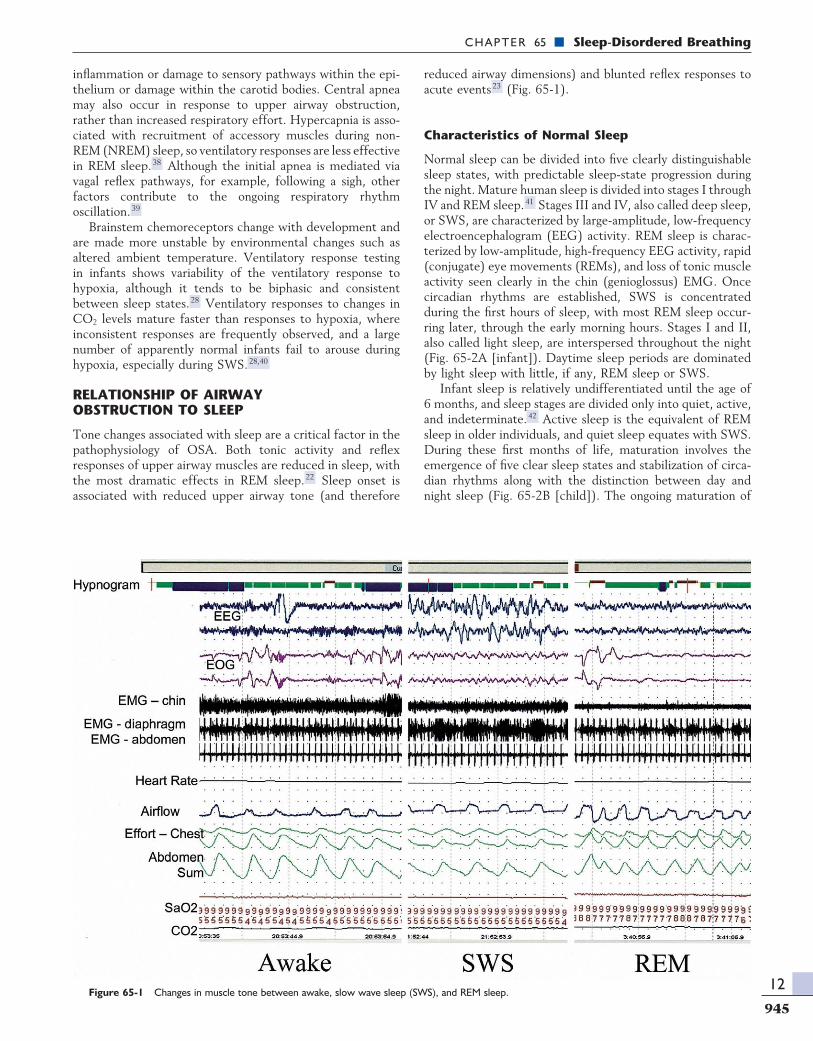
Tone changes associated with sleep are a critical factor in the pathophysiology of OSA. Both tonic activity and refl ex responses of upper airway muscles are reduced in sleep, with the most dramatic effects in REM sleep. 22 Sleep onset is associated with reduced upper airway tone (and therefore
reduced airway dimensions) and blunted refl ex responses to acute events 23 (Fig. 65-1).
Characteristics of Normal Sleep
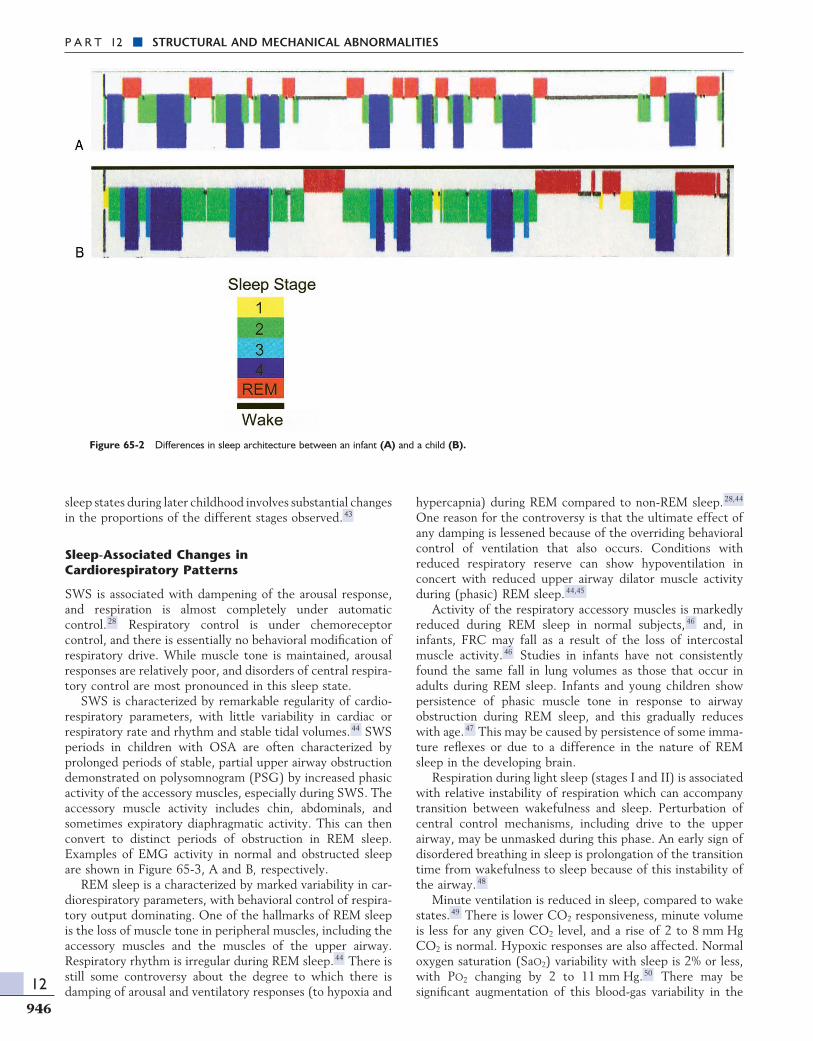
Normal sleep can be divided into fi ve clearly distinguishable sleep states, with predictable sleep-state progression during the night. Mature human sleep is divided into stages I through IV and REM sleep. 41 Stages III and IV, also called deep sleep, or SWS, are characterized by large-amplitude, low-frequency electroencephalogram (EEG) activity. REM sleep is charac-terized by low-amplitude, high-frequency EEG activity, rapid (conjugate) eye movements (REMs), and loss of tonic muscle activity seen clearly in the chin (genioglossus) EMG. Once circadian rhythms are established, SWS is concentrated during the fi rst hours of sleep, with most REM sleep occur-ring later, through the early morning hours. Stages I and II, also called light sleep, are interspersed throughout the night (Fig. 65-2A [infant]). Daytime sleep periods are dominated by light sleep with little, if any, REM sleep or SWS.
Infant sleep is relatively undifferentiated until the age of 6 months, and sleep stages are divided only into quiet, active, and indeterminate. 42 Active sleep is the equivalent of REM sleep in older individuals, and quiet sleep equates with SWS. During these fi rst months of life, maturation involves the emergence of fi ve clear sleep states and stabilization of circa-dian rhythms along with the distinction between day and night sleep (Fig. 65-2B [child]). The ongoing maturation of
Figure 65-1 Changes in muscle tone between awake, slow wave sleep (SWS), and REM sleep.
Ch065-A04048.indd 945Ch065-A04048.indd 945 1/18/2008 3:55:09 PM1/18/2008 3:55:09 PM
P A R T 12 ■ STRUCTURAL AND MECHANICAL ABNORMALITIES
12
946
Figure 65-2 Differences in sleep architecture between an infant (A) and a child (B).
sleep states during later childhood involves substantial changes in the proportions of the different stages observed. 43
Sleep-Associated Changes in Cardiorespiratory Patterns
SWS is associated with dampening of the arousal response, and respiration is almost completely under automatic control. 28 Respiratory control is under chemoreceptor control, and there is essentially no behavioral modifi cation of respiratory drive. While muscle tone is maintained, arousal responses are relatively poor, and disorders of central respira-tory control are most pronounced in this sleep state.
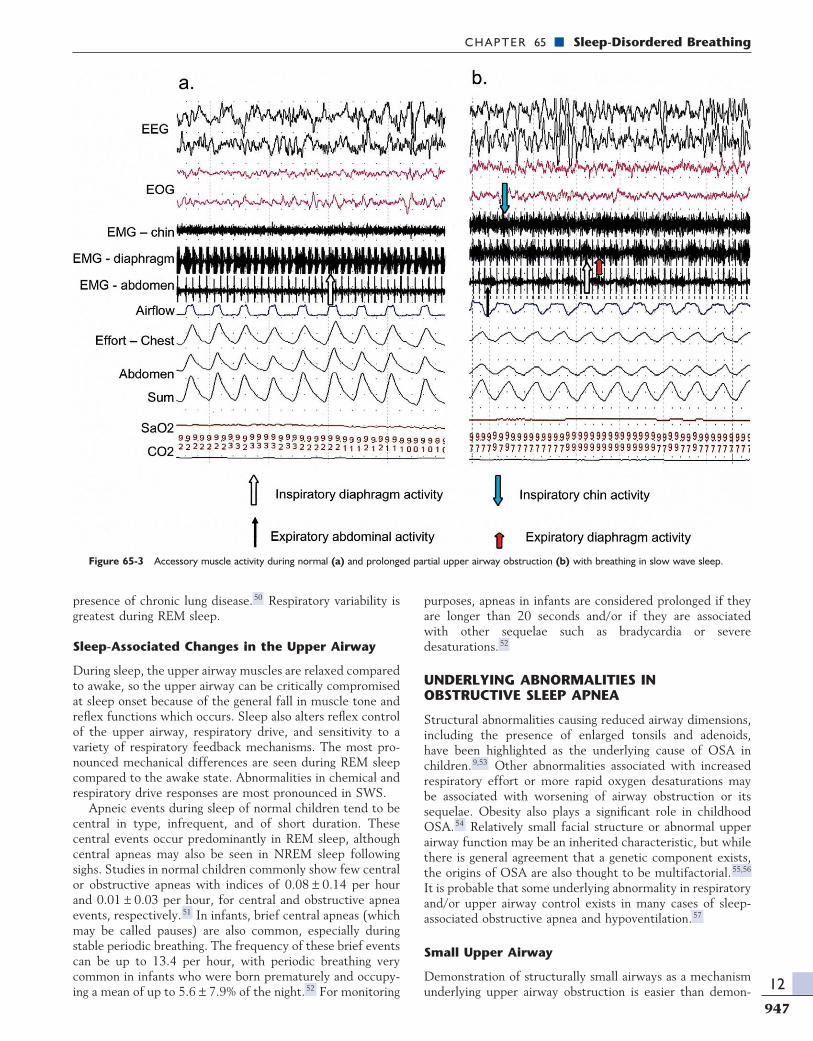
SWS is characterized by remarkable regularity of cardio-respiratory parameters, with little variability in cardiac or respiratory rate and rhythm and stable tidal volumes. 44 SWS periods in children with OSA are often characterized by prolonged periods of stable, partial upper airway obstruction demonstrated on polysomnogram (PSG) by increased phasic activity of the accessory muscles, especially during SWS. The accessory muscle activity includes chin, abdominals, and sometimes expiratory diaphragmatic activity. This can then convert to distinct periods of obstruction in REM sleep. Examples of EMG activity in normal and obstructed sleep are shown in Figure 65-3, A and B, respectively.
REM sleep is a characterized by marked variability in car-diorespiratory parameters, with behavioral control of respira-tory output dominating. One of the hallmarks of REM sleep is the loss of muscle tone in peripheral muscles, including the accessory muscles and the muscles of the upper airway. Respiratory rhythm is irregular during REM sleep. 44 There is still some controversy about the degree to which there is damping of arousal and ventilatory responses (to hypoxia and
hypercapnia) during REM compared to non-REM sleep. 28,44 One reason for the controversy is that the ultimate effect of any damping is lessened because of the overriding behavioral control of ventilation that also occurs. Conditions with reduced respiratory reserve can show hypoventilation in concert with reduced upper airway dilator muscle activity during (phasic) REM sleep. 44,45
Activity of the respiratory accessory muscles is markedly reduced during REM sleep in normal subjects, 46 and, in infants, FRC may fall as a result of the loss of intercostal muscle activity. 46 Studies in infants have not consistently found the same fall in lung volumes as those that occur in adults during REM sleep. Infants and young children show persistence of phasic muscle tone in response to airway obstruction during REM sleep, and this gradually reduces with age. 47 This may be caused by persistence of some imma-ture refl exes or due to a difference in the nature of REM sleep in the developing brain.
Respiration during light sleep (stages I and II) is associated with relative instability of respiration which can accompany transition between wakefulness and sleep. Perturbation of central control mechanisms, including drive to the upper airway, may be unmasked during this phase. An early sign of disordered breathing in sleep is prolongation of the transition time from wakefulness to sleep because of this instability of the airway. 48
Minute ventilation is reduced in sleep, compared to wake states. 49 There is lower CO2 responsiveness, minute volume is less for any given CO2 level, and a rise of 2 to 8 mm Hg CO2 is normal. Hypoxic responses are also affected. Normal oxygen saturation (SaO2) variability with sleep is 2% or less, with PO2 changing by 2 to 11 mm Hg. 50 There may be signifi cant augmentation of this blood-gas variability in the
Ch065-A04048.indd 946Ch065-A04048.indd 946 1/18/2008 3:55:11 PM1/18/2008 3:55:11 PM
CHAPTER 65 ■ Sleep-Disordered Breathing
12
947
presence of chronic lung disease. 50 Respiratory variability is greatest during REM sleep.
Sleep-Associated Changes in the Upper Airway
During sleep, the upper airway muscles are relaxed compared to awake, so the upper airway can be critically compromised at sleep onset because of the general fall in muscle tone and refl ex functions which occurs. Sleep also alters refl ex control of the upper airway, respiratory drive, and sensitivity to a variety of respiratory feedback mechanisms. The most pro-nounced mechanical differences are seen during REM sleep compared to the awake state. Abnormalities in chemical and respiratory drive responses are most pronounced in SWS.
Apneic events during sleep of normal children tend to be central in type, infrequent, and of short duration. These central events occur predominantly in REM sleep, although central apneas may also be seen in NREM sleep following sighs. Studies in normal children commonly show few central or obstructive apneas with indices of 0.08 ± 0.14 per hour and 0.01 ± 0.03 per hour, for central and obstructive apnea events, respectively. 51 In infants, brief central apneas (which may be called pauses) are also common, especially during stable periodic breathing. The frequency of these brief events can be up to 13.4 per hour, with periodic breathing very common in infants who were born prematurely and occupy-ing a mean of up to 5.6 ± 7.9% of the night. 52 For monitoring
purposes, apneas in infants are considered prolonged if they are longer than 20 seconds and/or if they are associated with other sequelae such as bradycardia or severe desaturations. 52
UNDERLYING ABNORMALITIES IN OBSTRUCTIVE SLEEP APNEA
Structural abnormalities causing reduced airway dimensions, including the presence of enlarged tonsils and adenoids, have been highlighted as the underlying cause of OSA in children. 9,53 Other abnormalities associated with increased respiratory effort or more rapid oxygen desaturations may be associated with worsening of airway obstruction or its sequelae. Obesity also plays a signifi cant role in childhood OSA. 54 Relatively small facial structure or abnormal upper airway function may be an inherited characteristic, but while there is general agreement that a genetic component exists, the origins of OSA are also thought to be multifactorial. 55,56 It is probable that some underlying abnormality in respiratory and/or upper airway control exists in many cases of sleep-associated obstructive apnea and hypoventilation. 57
Small Upper Airway
Demonstration of structurally small airways as a mechanism underlying upper airway obstruction is easier than demon-
Figure 65-3 Accessory muscle activity during normal (a) and prolonged partial upper airway obstruction (b) with breathing in slow wave sleep.
Ch065-A04048.indd 947Ch065-A04048.indd 947 1/18/2008 3:55:13 PM1/18/2008 3:55:13 PM

P A R T 12 ■ STRUCTURAL AND MECHANICAL ABNORMALITIES
12
948
strating abnormal function in children. The dynamic function of the airway is likely to play a signifi cant part in the patho-physiology of all cases of pediatric OSA. 23 Most recent studies of children’s airways use technologies such as cine-MRI. 58 These have demonstrated that children with OSA have different dynamic function of the airway as well as sig-nifi cant compromise of airway size associated with the ade-noids and tonsils. 9,58 Narrowing of the upper airway can occur at any point from the anterior nares to the larynx. This narrowing may be static or dynamic. Laryngomalacia and subglottic stenosis both increase the negative thoracic pres-sures required to generate inspiratory fl ow. Both of these types of airway narrowing predispose the affected individual to airway collapse during sleep. Children with malformations tend to have recalcitrant apnea. Persisting OSA after adeno-tonsillectomy may also be attributable to persisting airway abnormalities such as lingual tonsils. 59
Some children clearly have a structurally small upper airway, for example, in Down syndrome, or craniosynosto-ses. 60-62 A structurally small airway, no matter what the underlying cause, may also be further compromised by ade-notonsillar hypertrophy. Several studies have identifi ed abnormal facial structure associated with OSA, 63,64 but in children who are otherwise normal, chronic airway obstruc-tion has been associated with abnormal craniofacial structure that is reversible after treatment. 65 In others, with muco-polysaccharidoses or adenotonsillar hypertrophy, the airway lumen is crowded by extra soft tissue. 66 In the presence of reduced airway dimensions, upper airway muscles tend to maintain increased activity even in the awake state to main-tain a patent airway. In this situation, the loss of muscle tone that occurs with sleep onset may be the critical factor that precipitates complete or incomplete airway obstruction. 13
Abnormal Neurologic Control of Breathing
Abnormalities may occur in the central respiratory drive to the upper airway, or any site along the refl ex pathways, the neural input of the upper airway refl exes, the central neural integration of these refl exes or the motor (output) pathways. Although abnormal upper airway refl ex pathways have been postulated to cause OSA, when these refl ex pathways are disrupted in conditions such as neuromyopathies or Moebius syndrome, it is generally not an isolated defect. 67-69 The processes involved with maturation of neurologic pathways, including the pathways controlling upper airway refl exes, is proposed as a potential cause of the sudden infant death syndrome (SIDS). 34 Abnormal neurologic control of the upper airway has been implicated in OSA, but this can also result from episodic hypoxia resulting in exac-erbation of the disorder. Studies in adults with chronic snoring and OSA suggest that these patients have abnormal refl ex control of the airway lumen, although it is not clear whether these abnormalities are the cause or the effect of the disorder. 70
The pattern of abnormality in children with OSA tends to be preservation of the general architecture of sleep, 71 but their arousal responses to respiratory stimuli are dampened compared to controls. 72 Observed in its extreme form, chil-dren preserve sleep architecture at the expense of oxygen-ation and CO2 clearance. Occasionally, children also show the
converse response, of repetitive arousal in response to airway obstruction resulting in normal patterns of oxygenation and CO2, but disrupted sleep architecture. Depressed ventilatory responses have been documented in subgroups of the pedi-atric population with OSA. 73 No studies to date have con-fi rmed that arousal in response to OSA correlates with the ventilatory response activity of children, although it has been suggested that the rate of spontaneous arousals decreases as the apnea index increases. 74 These data provide some expla-nation as to why screening studies that measure only oxygen saturation (and/or CO2) do not indicate the level of sleep disturbance present in those cases with vigorous arousal in response to upper airway obstruction. 75
The congenital central hypoventilation syndrome (CCHS) occurs as a result of a genetic mutation and exemplifi es the most extreme form of abnormal neurologic respiratory control. 76 This disorder results from genetic defects in the Phox-2B pathway and is associated with varying degrees of hypoventilation; the majority of affected individuals only have sleep-associated hypoventilation, but the most severely affected have hypoventilation during wakefulness and during sleep. Now that genetic testing is available, it appears that some may only present with later onset. 77 The respiratory defect is associated with abnormal autonomic function and may also be associated with Hirschsprung’s disease. 78,79
The prototypical cause of hypoventilation is the CCHS, in which central chemoreceptor responsiveness is absent due to a genetic defect in the PHOX-2B pathway. However, acquired forms of central hypoventilation may be secondary to demonstrable anatomic lesions of the brainstem, or poste-rior fossa. 80 Abnormal central control may coexist with or may be secondary to an anatomically small airway. 73,81 Struc-tural lesions in the brainstem or other causes of respiratory failure, such as a muscular dystrophy, may also present with hypoventilation during sleep. 6 In the Arnold-Chiari malfor-mation, or syringobulbia, hypoventilation may occur second-ary to abnormal motor control of the cranial nerves or due to abnormal central control of respiration. 80,82,83
It is widely theorized that the likely underlying cause of SIDS deaths is delayed maturation or abnormalities of the neural cardiorespiratory-control pathways, causing these chil-dren to be at risk of death from an otherwise inconsequential insult. 84 Such abnormal neural control may also be expressed as, or occur secondary to OSA, and studies may be able to detect a number of those children at risk for SIDS. 85,86 The abnormality may become apparent only during an upper respiratory tract infection or other acute event. 87
Dysfunctional Upper Airway
Most children with abnormal neuromuscular control of the airway appear to have normal airway size. Palatal muscle function is abnormal in association with cleft palate, and this remains abnormal even after surgery, so that children with cleft palate appear to be at increased risk of sleep-associated airway obstruction. 88 When airway dimensions are reduced, these muscles may not be able to prevent airway obstruc-tion. 89 Presumably the local sensory perception would also be affected, although central respiratory control is not usually affected in this disorder.
Ch065-A04048.indd 948Ch065-A04048.indd 948 1/18/2008 3:55:14 PM1/18/2008 3:55:14 PM

CHAPTER 65 ■ Sleep-Disordered Breathing
12
949
Generalized motor hypotonia contributes to upper airway obstruction and is more common in younger children and in those with disorders such as Down syndrome. 90 Sleep-disordered breathing can be precipitated or exacerbated by confounders such as obesity or scoliosis. 91 Muscular dystro-phies and neuromuscular disorders are generally progressive. In Duchenne muscular dystrophy, this deterioration eventu-ally results in respiratory and cardiac failure. However, treat-ment intervention when the respiratory dysfunction is critically altered during sleep will dramatically improve the quality and prolong the lives of these patients. 92,93
OSA may occur where there is abnormal soft tissue function without demonstrable muscle weakness. In Marfan syndrome, in which the only apparent abnormality is poor connective tissue integrity, there is also a high incidence of OSA, which may then be responsible for causing or exacer-bating further abnormalities such as dilation of the aortic root. 94,95 Although it seems likely that other diagnostic groups with connective tissue disorders, such as Ehlers-Danlos syn-drome, would also have a high incidence of OSA, the groups affected with airway obstruction appear to be those with associated anatomical abnormalities such as micrognathia in rheumatoid arthritis or depositions causing airway narrowing in the mucopolysaccharidoses. 96,97 The skeletal abnormalities in achondroplasia cause a small foramen magnum. OSA in this group is thought to be on the basis of compression of the brainstem and upper cervical spinal cord at the level of the foramen magnum. 98
Mechanisms of Complications
Complications of severe OSA include failure to thrive (FTT) and pulmonary hypertension. Growth failure may be caused by disturbance of growth hormone secretion, increased energy expenditure, or more generalized metabolic responses to hypoxia. 99 Obesity is associated with OSA, and there appears to be a higher risk for metabolic complications of obesity if OSA is also present. 100,101 The neurologic and behavioral sequelae of OSA have been highlighted over recent years, although many of these appear to be reversible with treatment. 102,103
PRINCIPLES OF ASSESSMENT
To date, the diagnosis of OSA in children requires monitoring during sleep. The aim of such studies is to fi nd the abnormali-ties (sleep-associated respiratory dysfunction) and classify them by criteria which are discriminatory between studies and indicate the likelihood of detrimental effects in both the short and long term.
The gold standard for assessing sleep-related respiratory dysfunction is overnight polysomnography, and these detailed overnight studies provide the most detailed diagnostic infor-mation. It can be, however, an expensive and time-consuming procedure. Some form of screening needs to be used to determine which children should undergo such studies. Clini-cal assessment is the start of this screening process.
CLINICAL CHARACTERISTICS
Questionnaires initially looked promising, but it is now clear that history cannot distinguish OSA from primary
snoring. 104 Standardized questionnaires have been developed to assist in the process of symptom identifi cation and priori-tization. 105 The most discriminatory symptoms are breathing diffi culty during sleep, witnessed apnea, snoring, and restless sleep. 106 Witnessed apneas are typically brief. Disturbed sleep, rhinorrhea, excessive sweating during sleep, and mouth breathing in the awake state are frequent but not universal features. Other features such as enuresis are reported anec-dotally but may not be suffi ciently discriminatory to help distinguish individual children with OSA. 107,108 Upper respi-ratory tract infections appear to be an infrequent cause for the acute precipitation of obstructive apnea. 109,110 Reports are inconsistent regarding reduction in the frequency of respi-ratory tract infections after adenotonsillectomy, but overall they appear to show a slight reduction in the frequency of events. 111,112
There is consensus that even mild disease can have signifi cant negative impact on the development and behavior of infants and children, although many of these effects also appear to be reversible. 103,113 This has led to increased screening of children who are otherwise deemed to have attention defi cit-hyperactivity disorders (ADHDs). For indi-vidual cases, it is not generally possible to screen for devel-opmental or behavioral abnormalities that are specifi cally attributable to OSA, nor is it currently possible to predict the improvement an individual might achieve after surgery. 114
As children get older, their parents are less likely to witness children’s sleep, so history appears to become more unreli-able. However, factors such as a history of associated lower respiratory tract disease, secondary enuresis, or daytime sleepiness may be available. Daytime sleepiness is an infre-quent complaint among children with sleep apnea, although measures have shown that children with OSA are objectively more sleepy compared to controls. 115 Less-common presen-tations are reported anecdotally or as “associated symptoms,” such as developmental delay, night seizures, costochondritis, cyclic vomiting, hyperactivity or inattentiveness, and morning headaches. 116 OSA may also lead to exacerbation of condi-tions such as seizures, although this may not be apparent until there is improvement after treatment. 117
Past history may give an indication of the severity of obstruction. There may be a history of anesthetic diffi cul-ties. 118,119 Sedative drugs or muscle relaxants may contribute to upper airway problems, and children with OSA appear to be particularly sensitive to opiates. 120 Young infants may have symptoms of noisy breathing and sweating in sleep, and some children who present as near-miss SIDS have been demonstrated to have obstructive events on sub-sequent sleep studies. 121 Children who have subsequently died of SIDS have had obstructive apneic events demon-strated on sleep studies performed prior to death. 86 With better access to appropriate screening studies, it is possible that children who have these abnormalities can be detected and treated.
Despite recognition that history is not able to accurately identify the presence or severity of OSA in children, surveys continue to show that most ENT surgeons use only history to make the diagnosis; objective testing for OSA occurs only in 10% to 12% of cases that proceed to surgery with a diagnosis of OSA. 122
Ch065-A04048.indd 949Ch065-A04048.indd 949 1/18/2008 3:55:14 PM1/18/2008 3:55:14 PM

P A R T 12 ■ STRUCTURAL AND MECHANICAL ABNORMALITIES
12
950
Underlying Conditions
Unless there has been a clear precipitating event or specifi c questioning for a history of sleep-disordered breathing is sought, the symptoms of obstructive apnea may not be dis-tinguished from the developmental history of children where an underlying condition is associated with increased risk for airway obstruction. With research now demonstrating that some syndromes have an increased or high incidence of obstructive apnea, there is better screening of children with such disorders for this disease. Any cause of airway narrowing may contribute to sleep-associated obstruction, including rhi-nitis or nasal abnormalities. 123 Other predisposing factors include choanal stenosis, laryngeal palsy (congenital or acquired), and tracheobronchomalacia. 118,119 Infants with a history of prematurity have facial features predisposing to obstruction. 23,124 Symptoms affecting both daytime and nighttime function, including intellectual dysfunction and sleepiness, may be considered part of the inherited syndrome rather than secondary sequelae.
Studies suggest that there is a familial incidence of OSA; children with OSA often have one or more parents who are also affected. A genetic link has been proposed. 125 It is pos-sible that there is also a link with SIDS deaths. 126,127 Further studies are required to confi rm these associations.
Examination
It is increasingly rare for children with OSA to present with complications of the disease, although the link between behavioral and neurologic abnormalities has meant that chil-dren with ADHD or other behavioral disturbances may need to have a diagnosis of OSA excluded. 102 Nonetheless, vigi-lance is required among those groups at highest risk.
Careful daytime examination can potentially reveal a wide range of physical features associated with obstructive apnea in children or a variety of medical conditions that have now been associated with the disorder. 128 Increased upper airway (nasal) resistance can result in mouth breathing when awake. 129 The patency of the nasal airway should be assessed, including endoscopy if required. 129,130 Syndromes and mal-formations may be associated with other airway abnormali-ties, 131 as well as those specifi cally linked to OSA such as hypoplastic mid-face or mandible. 119 Syndromes and malfor-mations may be present in more than a quarter of children diagnosed with OSA. 132
The oropharynx must always be examined for enlarged tonsils, the extent of the tonsillar extension behind the tongue, and the presence and quantity of upper airway secre-tions. A characteristic “snorer’s throat” includes edema and petechiae in the soft tissues of the oropharynx, although petechiae can also occur with recurrent tonsillitis. 133 The palate should specifi cally be examined for clefts and other clues of submucosal clefts, such as a bifi d uvula. The presence of lymphadenopathy may support a history of recurrent tonsillitis. 133
Respiratory examination may reveal chest deformities; Harrison’s sulci are common where there is signifi cant upper airway obstruction. Restrictive chest deformities are another common cause of respiratory decompensation in sleep, although not necessarily associated with OSA. 128
Weight abnormalities are associated with OSA. Obesity is increasingly common and increases the risk for OSA even in childhood, and weight loss can be associated with improve-ment in OSA. 134 FTT occurs secondary to OSA, and may occur in up to 21% of young children (<6 years) or infants where there is also a clear growth response following effective treatment. 99 The incidence of FTT is now reported to be quite low, although it appears to be more common in infants than in older children with OSA. 121 Features of pulmonary hypertension are uncommon, except in the most severe cases and tend to be more subtle than can be observed on clinical examination. 118 Cardiologic assessment by CXR and ECG can be used, but echocardiographic examination is the most sensitive test for evaluating cardiac complications in children with severe OSA. 135,136
Clinical features of hypoventilation vary. For children with congenital central hypoventilation, the most common presen-tation is apnea or respiratory failure soon after birth, although other common features may be associated with their expo-sure to recurrent hypoxia. 137 Where hypoventilation is sec-ondary to neurologic abnormalities, the problem may be silent until the time of a sleep study, or it may present with other symptoms that relate to the neurologic abnormal-ity. 82,138 Increased awareness that children with neuromuscu-lar diseases and thoracic deformities are at risk of respiratory failure has led to increased use of anticipatory monitoring to evaluate respiratory deterioration in sleep. Although transcu-taneous and end-tidal measurements are helpful, blood gases should also be measured when there is suspicion of respira-tory failure. As arterial blood gas samples may be diffi cult to obtain in children, capillary or venous sampling and transcu-taneous monitoring are valuable aids in this assessment.
FURTHER STUDIES
Initial investigations are appropriately directed toward fi nding the underlying cause for, or complications of, OSA. Lateral airway radiographs can show airway-occluding soft-tissue (masses) including the tonsils and adenoids. They are more readily available, although not as precise as MRI for determin-ing the static size of the airway and the relative size of the tonsils and adenoids. 9,139 If linked to the respiratory cycle, dynamic differences in airway dimensions can also be deter-mined by these imaging modalities. 140 Nasendoscopy is useful for a dynamic assessment of airway size and to assess space-occupying lesions. 141 CT scan is useful for determining a three-dimensional, static image of airway size. MRI, recon-structed CT images, and acoustic refl ection can be used to determine an absolute volume for the airway. MRI is the most useful imaging technique for examining the brainstem, pos-terior fossa, and upper cervical cord.
Now that the genetic defect for CCHS has been identi-fi ed, genetic testing is appropriate if CCHS is suspected and parental testing should also be undertaken for newly diag-nosed cases. Ongoing research will clarify how the pheno-typic features of the disease relate to the genotypic expression and it is clear that genetic mosaicism can produce less severe phenotypes. 8,78 In addition, autonomic dysfunction, as previ-ously suspected and as is consistent with the pathways where the mutation has been identifi ed, does appear to coexist in the majority of cases. 142
Ch065-A04048.indd 950Ch065-A04048.indd 950 1/18/2008 3:55:15 PM1/18/2008 3:55:15 PM
CHAPTER 65 ■ Sleep-Disordered Breathing
12
951
Screening Studies
The most well-studied testing modality to screen for sleep apnea in children is oximetry. 75,143 The major diffi culty with this test is that although it is specifi c, it is not a sensitive test for sleep apnea. As with questionnaires of clinical symptoms, a signifi cant proportion of the results lead to a need for sub-sequent sleep studies, therefore limiting the cost-effective-ness of the screening.
Sleep Study Methods
Overnight sleep studies provide information about respira-tion during a period of sleep and, despite some controversies, they are still considered the gold standard for diagnosis. 5,144,145 These studies are usually performed because the history and/or examination suggest a diagnosis of OSA, but there are not enough facilities to provide full sleep studies for all children where OSA is suspected because of snoring. Therefore some form of screening is generally required in order to prioritize which children will have full sleep studies and which children should have surgery with adenotonsillectomy to treat upper airway obstruction. 143
Polysomnography is the name given to a multiple-channel, physiologic recording performed during sleep. In its complete form, more than 16 variables are measured during the normal period of nighttime sleep. The clear benefi t is the amount of information provided. The corollary in pediatrics is the highly demanding process of preparing children with all the attach-ments necessary for such a recording. Leads need to be placed accurately and fi rmly in order to provide good quality record-ings for an 8- to 10-hour study. Sleep state is recorded by a combination of EEG, eye movements, and muscle (usually genioglossus) tone. The combination of these signals is required to differentiate all sleep stages, particularly REM. To record sleep stage, a minimum of one, but usually two to four, EEG leads are used. Eye movements and EMG signals are recorded via surface electrodes. This is costly because it is both time and labor intensive, but it provides accurate diagnoses with no signifi cant detrimental effects on fi rst com-pared to subsequent studies. 146
Respiratory recordings include measures of both the effort exerted and the resulting effects. Effort can be recorded using EMG signals or chest/abdominal displacement. Ple-thysmography is the most popular measure, as the signal recorded is proportional to volume and has the potential to be calibrated. Impedance recordings are another common alternative. 147
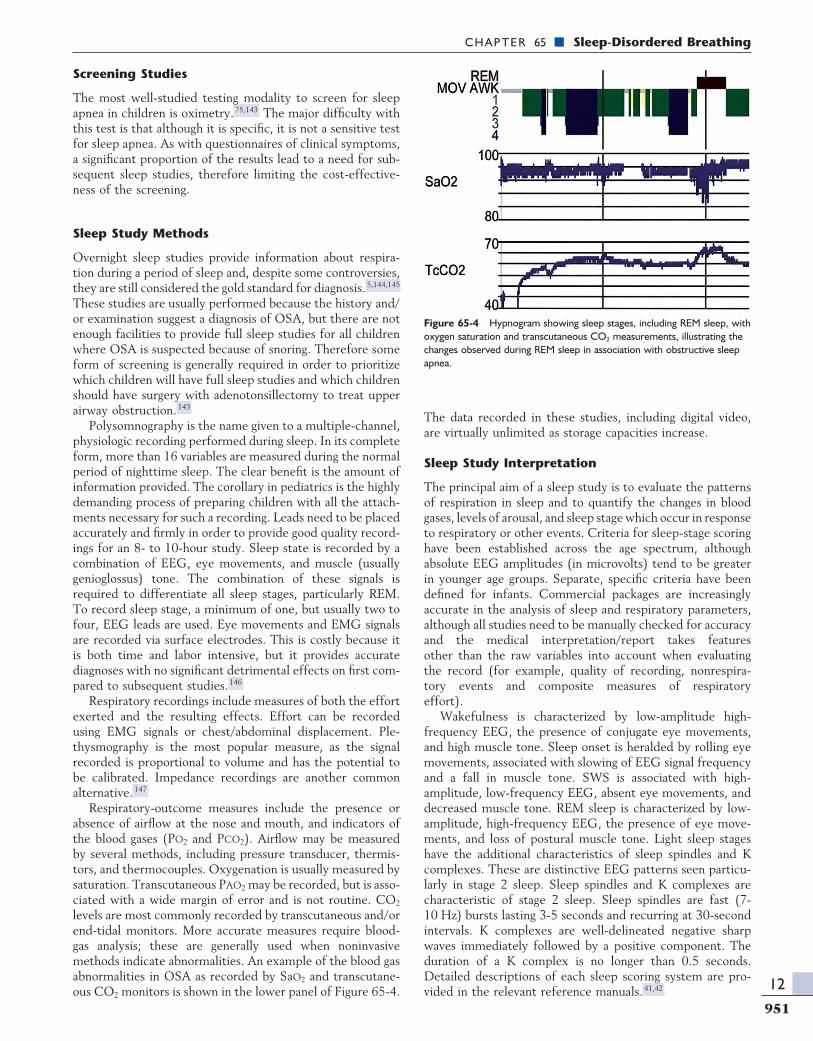
Respiratory-outcome measures include the presence or absence of airfl ow at the nose and mouth, and indicators of the blood gases (PO2 and PCO2). Airfl ow may be measured by several methods, including pressure transducer, thermis-tors, and thermocouples. Oxygenation is usually measured by saturation. Transcutaneous PAO2 may be recorded, but is asso-ciated with a wide margin of error and is not routine. CO2 levels are most commonly recorded by transcutaneous and/or end-tidal monitors. More accurate measures require blood-gas analysis; these are generally used when noninvasive methods indicate abnormalities. An example of the blood gas abnormalities in OSA as recorded by SaO2 and transcutane-ous CO2 monitors is shown in the lower panel of Figure 65-4.
The data recorded in these studies, including digital video, are virtually unlimited as storage capacities increase.
Sleep Study Interpretation
The principal aim of a sleep study is to evaluate the patterns of respiration in sleep and to quantify the changes in blood gases, levels of arousal, and sleep stage which occur in response to respiratory or other events. Criteria for sleep-stage scoring have been established across the age spectrum, although absolute EEG amplitudes (in microvolts) tend to be greater in younger age groups. Separate, specifi c criteria have been defi ned for infants. Commercial packages are increasingly accurate in the analysis of sleep and respiratory parameters, although all studies need to be manually checked for accuracy and the medical interpretation/report takes features other than the raw variables into account when evaluating the record (for example, quality of recording, nonrespira -tory events and composite measures of respiratory effort).
Wakefulness is characterized by low-amplitude high-frequency EEG, the presence of conjugate eye movements, and high muscle tone. Sleep onset is heralded by rolling eye movements, associated with slowing of EEG signal frequency and a fall in muscle tone. SWS is associated with high-amplitude, low-frequency EEG, absent eye movements, and decreased muscle tone. REM sleep is characterized by low-amplitude, high-frequency EEG, the presence of eye move-ments, and loss of postural muscle tone. Light sleep stages have the additional characteristics of sleep spindles and K complexes. These are distinctive EEG patterns seen particu-larly in stage 2 sleep. Sleep spindles and K complexes are characteristic of stage 2 sleep. Sleep spindles are fast (7-10 Hz) bursts lasting 3-5 seconds and recurring at 30-second intervals. K complexes are well-delineated negative sharp waves immediately followed by a positive component. The duration of a K complex is no longer than 0.5 seconds. Detailed descriptions of each sleep scoring system are pro-vided in the relevant reference manuals. 41,42
Figure 65-4 Hypnogram showing sleep stages, including REM sleep, with oxygen saturation and transcutaneous CO2 measurements, illustrating the changes observed during REM sleep in association with obstructive sleep apnea.
Ch065-A04048.indd 951Ch065-A04048.indd 951 1/18/2008 3:55:15 PM1/18/2008 3:55:15 PM

P A R T 12 ■ STRUCTURAL AND MECHANICAL ABNORMALITIES
12
952
Discrete respiratory events are defi ned as obstructive or central, depending on whether respiratory efforts continue during the apnea. An obstructive apnea indicates ongoing respiratory effort without airfl ow being achieved. During a central apnea there is no effort and no diaphragmatic activity. During mixed apnea airfl ow is absent, with diaphragmatic effort present for only a portion of the event. Criteria for scoring respiratory events in children need to account for the change in respiratory rate with age. In Australia, agreed criteria score respiratory events which disturb two or more consecutive respiratory cycles. The fall in oxygen saturation most commonly used to defi ne a signifi cant event is 3% to 4%. Values for normal children have now been published by several authors. 51
The frequency of arousal and the levels of oxygen desatu-ration seen during the night in children with OSA are higher than in age-matched controls, but do not approach those seen in adult patients. The tolerance in children of “stable” partial obstruction does not appear to circumvent all symptoms or sequelae of obstructive apnea. 148 Detailed studies do suggest that there is an altered duration and distribution of sleep states in these children as a group. 103,134 Not all studies show consistent changes in sleep architecture since there is a ten-dency for children to preserve sleep architecture despite OSA. 149,150 Infants appear to have signifi cant attenuation of REM sleep with respiratory disorders, including obstructive apnea. 151,152 REM sleep deprivation increases neuronal excit-ability and facilitates seizure activity, and deprivation of REM sleep during development has been shown to result in per-manent behavioral changes and brain morphologic and bio-chemical abnormalities in animals. 153
Children tend to have long periods of partial upper airway obstruction with minimal sleep disruption. Carbon dioxide retention can be marked during these periods, and some degree of hypoventilation occurs quite commonly in children with OSA. Sleep studies should include some measurement of CO2 wherever possible. 154
Studies demonstrating central hypoventilation, including central nervous system abnormalities other than CCHS, are characterized by marked blood gas disturbances in SWS. Children with CCHS fail to respond with either ventilatory or arousal responses to severe desaturations or CO2 reten-tion 155 although in our experience there does appear to be recovery of arousal in response to hypoxia after a period of treatment with adequate ventilation. Hypoventilation in response to neuromuscular or thoracic abnormalities is most marked during REM sleep when there is loss of accessory muscle activity, and a clinical history, examination, and detailed sleep study are required to distinguish this from upper airway obstruction. 156
MANAGEMENT OPTIONS
Introduction
Treatment is fi rst directed by accurate characterizations of the sleep-breathing abnormality. In the immediate sense, the signifi cance of an apnea is determined by the physiologic changes it produces. During an obstructive event, these are the consequence of reduced or absent airfl ow despite sus-tained or increased respiratory efforts. Immediate effects
include hypoxia and increased amplitude of negative intra-thoracic pressure swings as well as arousal and increased sympathetic outfl ow. 157 Hemodynamic changes include bradycardia or tachycardia and can progress to systemic and pulmonary hypertension. 158 In contrast to OSA, central hypoventilation disorders are characterized by lack of effec-tive effort in response to blood gas disturbances. 155
Public Awareness
Awareness of the syndrome of OSA appears to be increasing among the public and medical communities. 159,160 Support group networks have been one effective way of disseminating information to the public. A high percentage of children with syndromes and malformations are thought to suffer with OSA, and their families frequently belong to such support associations. Increased education of clinicians as well as the public about the symptoms and signs of the disorder has been helpful in identifying children so that they reach medical attention. Most support groups have newsletters, which are an effective means of distributing such information. Surveys reveal that the majority of children present through parental action, despite their primary physician being aware of their symptomatology.
Medical Therapies
The role of pharmacologic options for the treatment of OSA in children is still being clarifi ed. Nasal steroids are effective to reduce the severity of disease. 161 Allergic rhinitis may require topical nasal therapy whether these children have surgery or not. 162,163 Sedating agents, such as the benzodiaz-epines, may contribute to upper airway discoordination and increase upper airway secretions: 73 In some cases it may be possible to reduce these medications to minimize this com-ponent of the obstruction.
OSA is common in obese children. 101,164 The treatment of obesity is a diffi cult problem, usually involving the whole family in long-term intervention. The severity of the OSA is likely to improve after weight loss, but it is often necessary to treat the OSA acutely by other means, while commencing such a weight-control program.
Other chronic respiratory disorders may exacerbate sleep-disordered breathing. Attention should be paid to diagnosing and treating such specifi c problems as nasal polyps in cystic fi brosis, or frequent coughing, which will cause arousals and disturb sleep. 128 Maximizing lower respiratory tract function, including aggressive treatment of acute exacerbations will minimize the additional impact of sleep. Additional treat-ment, such as nocturnal nasal oxygen, CPAP, or ventilation may be necessary during sleep periods. The clinical reasons cited for commencing noninvasive mechanical ventilation (NIMV) include nocturnal hypoventilation (67%), acute exacerbations of lung disease (28%), and/or failure to thrive (21%). 6
Nasal CPAP and Nasal Mask Ventilation
Nasal mask CPAP has been used for the treatment of adult OSA since 1981, 165 with exponential increase in the number of adult patients using this therapy since that time. Major centers acquire experience with the use of nasal CPAP in
Ch065-A04048.indd 952Ch065-A04048.indd 952 1/18/2008 3:55:16 PM1/18/2008 3:55:16 PM

CHAPTER 65 ■ Sleep-Disordered Breathing
12
953
children quickly and with high success rates, confi rming that CPAP is a practical treatment alternative for those children who do not achieve relief of their obstruction by adenotonsil-lectomy. 132,166,167 Although the use of CPAP in children has been less widespread than in adults, it is now a useful alterna-tive to tracheotomy even for palliation. 168 Two important factors have been the development of a widely applicable pediatric nose mask (Fig. 65-5), and the use of a behavioral program to introduce the therapy to children. 169,170 Children often return quickly to their previous overnight sleep require-ments after the implementation of successful treatment strategies. Compliance with noninvasive treatment regimens can become diffi cult, although the predictors of noncompli-ance are not well defi ned.
Nasal masks can also be used for the delivery of nocturnal volume or pressure cycled ventilation in children who present with congenital or acquired central hypoventilation. 171 Again, this mode of treatment delivery circumvents the need for tracheotomy, and it has been successfully used in the home environment from infancy on. 93 Side effects may occur both acutely and in the long term, particularly the development of mid-face hypoplasia. 172 Overnight nursing assistance is usually required as with tracheostomized children who are ventilated in the home environment. 173
Surgical Options
The mainstay of treatment for OSA is adenotonsillectomy. The proportion of adenotonsillectomies performed to treat upper airway obstructive symptoms has shown a fairly steady increase. 174 Recent rates for tonsillectomy in Australia are 2.7% of children by the age of 5 and 8.9% by the age of 15 years. 174 Adenotonsillectomy results in signifi cant improve-ment in most children with OSA. 175 Reported results of surgery to relieve upper airway obstruction include relief of symptoms, catch-up growth in those who have been FTT, marked reduction in the work of breathing, improved neuro-cognitive function, and improved quality of life. 102,121,175,176
It is important to be aware that the complications of ade-notonsillectomy surgery are higher in children for whom the surgery is being undertaken for OSA. 177 Children with OSA
have increased anesthetic risk from sensitivity to opiates, 73,120 as well as increased risks for respiratory complications of the surgery. 143,178 Associated complications are more common in the younger age groups, with those younger than 2 to 3 years particularly affected. 179 Nonetheless, this surgery is rec-ommended as the fi rst-line treatment of OSA in children even if there are other underlying factors such as a small airway. 122,145
It is now also clear that surgery is not always curative. 180 It is estimated that around 10% to 20% of children have persisting OSA after adenotonsillectomy. 53,181 There is increased risk for persisting disease in children with an ana-tomically small or dysfunctional upper airway, obese subjects, children with a history of prematurity, and those with more severe disease before surgery. 181-183 The role for adenoidec-tomy alone, particularly when the tonsils are not large, is not clear because of the perceived increased risk for subsequent tonsillectomy. 184,185 Until further studies clarify this issue, these children should have follow-up monitoring. Particular syndromes may have a very high incidence of OSA, with those documented including children with Down syndrome, Crouzon, other craniostenoses, or skeletal dysplasias such as achondroplasia. 186,187 Airway obstruction has been reported after surgery to correct cleft palate. 88 Children with such syndromes or malformations can constitute a high proportion of those requiring ongoing treatment, indicating that they are more likely to have severe apnea than their counterparts with normal facial structure. 132 Other groups requiring ongoing supervision and intervention are those with progressive infi l-trative diseases such as mucopolysaccharidoses. 97
Other surgical procedures may be used to treat OSA including mid-face or mandibular advancement and rapid mandibular expansion. 188 These surgical procedures may be implemented on the basis of the cosmetic benefi ts expected but will also alter the character of the upper airway. Where this surgery is undertaken, there should be careful periopera-tive attention to the upper airway. 188,189
Uvulopalatopharyngoplasty (UPPP) has relatively low success rates (≈50%) and will be mentioned only to caution against its application in children. 190 UPPP has very limited application in adults, and even less in children for the treat-ment of obstructive apnea. This surgery is associated with poor long-term response and may have signifi cant complica-tions, in particular, velopharyngeal incompetence. 191
Tracheotomy remains a surgical option. This has been demonstrated to be effective in treating obstructive apnea and characteristically results in relief of sleep-associated obstruction. Catch-up growth and relief of right-heart failure have been seen in children where adenotonsillectomy alone was not successful. 188 This surgery is associated with its own morbidity and complications and is not a fi rst-line therapy.
Diaphragmatic Pacing for Hypoventilation
Electrical stimulation of the diaphragm, using a small im -plantable electrode and receiver, can successfully support ventilation in children with inadequate central respiratory drive or high quadriplegia. 192 The signal is transmitted by an antennae placed on the skin, overlying subcutaneously implanted receivers. An electrical impulse is then transmitted to the thoracic phrenic nerve, resulting in diaphragmatic
Figure 65-5 Nasal CPAP in an infant with Robin sequence (Maskmedic Concept Mask).
Ch065-A04048.indd 953Ch065-A04048.indd 953 1/18/2008 3:55:16 PM1/18/2008 3:55:16 PM

P A R T 12 ■ STRUCTURAL AND MECHANICAL ABNORMALITIES
12
954
contraction. The stimulus parameters that are most appropri-ate for children are a low stimulus frequency, short inspira-tory time, and moderate respiratory rate.
A tracheotomy is required in all young children up to school age and older in order to prevent pacing-related upper airway obstruction (the larynx does not dilate during inspira-tion). Bilateral diaphragmatic pacing is required in children in order to achieve a suffi cient level of ventilation. Due to the risk of permanent diaphragmatic and phrenic nerve injury any additional support (more than 12 to 15 hours per day) requires alternative modes of delivery. The biggest advantage of this mode of treatment is the increased mobility that it permits, although backup forms of ventilation should be available at all times. The most signifi cant complications are infection (reported rate 6%), component failure, and mechan-ical nerve injury. The disadvantages of this mode of ventila-tion (high cost, the need for a tracheotomy, and for an external transmitter) mean that, for patients who require ventilation only at night, mask ventilation is preferable. 193
CONCLUSION
Ongoing studies will determine the relationships between SIDS, the childhood syndrome of OSA, and the adult syn-
drome. With more refi ned studies, the precise implications of OSA in children will be elucidated. It is possible that some causative genetic or neurodevelopmental factor will be iso-lated in some cases of this syndrome. Current developments mean that automatically responsive pressure devices will soon be available for all age groups, making both CPAP and nasal mask ventilation more precise and therefore more comfort-able to use.
Challenges in the fi eld include development and validation of confi rmatory and discriminatory testing regimens that are more easily applied than full overnight sleep studies. For each test, there is a need to determine the cutoff levels at which treatment should be instituted as well as where special peri-operative precautions need to be introduced. This includes refi nement of treatment intervention for mild disease that may only have behavioral or developmental, rather than sig-nifi cant blood gas, respiratory, or long-term cardiac complica-tions. While recognizing the enormous practical benefi t of noninvasive interfaces for CPAP and ventilation, it is also important to defi ne the role of more defi nitive treatment options in children.
SUGGESTED READINGS
Arens R, Marcus CL: Pathophysiology of upper airway obstruction: A developmental perspective. Sleep 27:997-1019, 2004.
McNicholas WT: Impact of sleep in respiratory failure. Eur Respir J 10:920-933, 1997.
Schechter MS: Technical report: Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 109:e69, 2002.
REFERENCESThe references for this chapter can be found at www.pedrespmedtext.com.
Ch065-A04048.indd 954Ch065-A04048.indd 954 1/18/2008 3:55:17 PM1/18/2008 3:55:17 PM