patterns of discontinuation of atypical antipsychotics in the province of québec: a retrospective...
TRANSCRIPT

Clinical Therapeutics/Volume 32, Supplement A, 2010
2010 S21
Accepted for publication August 3, 2009.
Express Track online publication January 20, 2010.doi: 10.1016/j.clinthera.2010.01.0030149-2918/$ - see front matter
© 2010 Excerpta Medica Inc. All rights reserved.
ABSTRACTBackground: Patterns of discontinuation of atypical
antipsychotic drugs, including the return to therapy after an interruption, have not been examined longitudinally.
Objective: This study was conducted to describe discontinuation patterns of atypical antipsychotic drugs across a spectrum of outpatients in the province of Québec.
Methods: This retrospective, inception cohort study employed data from the Québec health insurance board databases and the Québec hospitalization registry on Québec Drug Plan beneficiaries between the ages of 20 and 64 years who first filled a prescription for any antipsychotic drug between January 1, 2000, and December 31, 2007. Five subcohorts were constructed according to the initial antipsychotic received: either 1 of the 4 atypical antipsychotics covered by the Québec drug plan at the time of the study—olanzapine, que-tiapine, risperidone, and clozapine—or polytherapy (>1 atypical antipsychotic, or 1 atypical and 1 typical antipsychotic). Discontinuation was defined as a fail-ure to refill the initial prescription within 2 times the days’ supply of the preceding claim. In individuals who discontinued initial drug treatment, a new course of treatment was defined as initiation of treatment with any antipsychotic drug after a first treatment discontinuation. Discontinuation of a second course of treatment was defined as failure to refill a prescrip-tion for the second drug within 2 times the days’ sup-ply of the preceding claim. Patients were followed from initiation to December 31, 2004, ineligibility for the drug plan, or death, whichever came first. Kaplan-Meier curves and Cox regression models were used to compare discontinuations and new courses of treat-ment by initial atypical antipsychotic.
Results: The overall cohort consisted of 46,074 drug plan beneficiaries who had initiated antipsychotic treatment during the specified period. The majority of
individuals were female (54.6%) and lived in urban areas (79.2%); the median age ranged from 40 to 44 years. The mean (SD) duration of follow-up was 2.67 (1.91) years. Compared with individuals whose initial therapy was olanzapine, those whose initial therapy was quetiapine had a significantly higher like-lihood of discontinuing initial treatment (adjusted hazard ratio [AHR] = 1.06; 95% CI, 1.04–1.09; P < 0.001). The likelihood of discontinuing initial treat-ment was significantly lower among those whose ini-tial therapy was risperidone (AHR = 0.93; 95% CI, 0.90–0.95; P < 0.001), clozapine (AHR = 0.56; 95% CI, 0.46–0.68; P < 0.001), or polytherapy (AHR = 0.69; 95% CI, 0.64–0.74; P < 0.001). Those whose initial therapy was quetiapine were significantly less likely than those whose initial therapy was olanzapine to begin a second course of treatment (AHR = 0.95; 95% CI, 0.90–0.99; P = 0.02). Compared with indi-viduals who initiated a second course of treatment with olanzapine, those who initiated a second course with quetiapine were more likely to discontinue again (AHR = 1.09; 95% CI, 1.04–1.14; P < 0.001), where-as those who initiated a second course with risperi-done were less likely to discontinue again (AHR = 0.95; 95% CI, 0.90–1.00; P = 0.04).
Conclusions: This study population had a high risk of discontinuing initial atypical antipsychotic therapy within 1 year. Those who discontinued had a low like-lihood of returning to treatment, and those who did return to treatment had a high likelihood of discon-tinuing again. These patterns of use may have serious consequences for patients’ health and for the utiliza-
Patterns of Discontinuation of Atypical Antipsychotics in the Province of Québec: A Retrospective Prescription Claims Database Analysis
Jocelyne Moisan, PhD1,2; and Jean-Pierre Grégoire, MPH, PhD, FISPE1,2
1Faculty of Pharmacy, Université Laval, Québec, Canada; and 2URESP, Centre de recherche FRSQ du CHA universitaire de Québec, Québec, Canada

S22 Volume 32 Supplement A
Clinical Therapeutics
cian services (date and diagnosis), and dispensed drugs (drug identification number, dispensing date, number of days’ supply, and prescriber specialty). The drug plan database has been recognized as accurate for prescription claims.6
Med-Écho is the acute-care hospital discharge regis- try for Québec. It provides data on length of hospital stay and diagnoses (dates, primary diagnosis, and sec-ondary diagnoses).
Study PopulationThe RAMQ database was used to identify all drug
plan beneficiaries between the ages of 20 and 64 years who filled ≥1 prescription for any antipsychotic drug (Anatomical-Therapeutic-Chemical [ATC] code N05A, excluding N05AN [lithium]) between January 1, 2000, and December 31, 2007, excluding those who were not eligible for the plan during the entire 365-day period before the first antipsychotic dispensing on or after January 1, 2000. For each identified individual, data were obtained for the period from 365 days before the date of the first dispensing of an antipsychotic on or after January 1, 2000, through December 31, 2007.
The following individuals were excluded: benefi-ciaries whose first antipsychotic drug claim occurred after March 31, 2007 (because hospitalization data were not available after this date); those aged <20 years or >64 years on the date of the first dispensing; and those with a record of ≥1 antipsychotic drug dispens-ing in the 365-day period before this date. The reason for the age restriction was to create a relatively homo-geneous group of individuals with a higher likelihood of being prescribed antipsychotic drugs for the treat-ment of schizophrenia or bipolar disorders. In the el-derly, these drugs are mainly prescribed to control behavioral symptoms of dementia, whereas children and teenagers are more likely to receive parental help in managing their medication use.
Only individuals whose first claim included an atypi-cal antipsychotic (ATC codes N05AH02, N05AH03, N05AH04, and N05AX08) were retained. All selected individuals were followed from the date of their first claim for an atypical antipsychotic (date of treatment initiation) until death, end of eligibility for the drug plan, or the end of follow-up, whichever came first.
The study was approved by the Commission d’accès à l’information du Québec and by the research ethics committee of the Centre de recherche du CHA universitaire de Québec.
tion of health services. (Clin Ther. 2010;32[Suppl A]: S21–S31) © 2010 Excerpta Medica Inc.
Key words: discontinuation, persistence, adherence, atypical antipsychotics.
INTRODUCTIONIn Canada, atypical antipsychotics are indicated for the treatment of schizophrenia and bipolar disorders; in addition, they are frequently used off-label to treat behavioral disturbances associated with dementia and other mental disorders.1 Atypical antipsychotic drugs have differing pharmacologic properties that are likely to translate into differences in outcomes and tolerabili- ty. Thus, treatment discontinuation, a major negative outcome, is likely to vary from one atypical antipsy-chotic drug to another.
Patterns of use of atypical antipsychotic drugs in clinical practice have yet to be fully described. Al-though differences in patterns of drug discontinuation have been studied as a function of the atypical anti- psychotic initially prescribed,2–5 patterns of return to therapy and discontinuation after initiation of a sec-ond course of treatment have not been examined.
The objective of the present study was to character-ize patterns of discontinuation of atypical antipsy-chotic drugs in the province of Québec among outpa-tients who were prescribed an atypical antipsychotic for the first time.
METHODSStudy Design and Data Sources
This retrospective, inception cohort study em-ployed information obtained from the Québec health insurance board (Régie de l’assurance maladie du Québec [RAMQ]) databases and the Québec hospital-ization registry (Med-Écho). The RAMQ health insur-ance plan covers medical services and hospitalizations for all permanent residents in the Canadian province of Québec. The RAMQ Public Prescription Drug In-surance Plan covers all residents aged ≥65 years (re-ceiving or not guaranteed income supplement), wel-fare recipients, and persons who are ineligible for a private plan. In 2006, 3.2 million of the population of 7.5 million were RAMQ beneficiaries.
The RAMQ databases include information on pa-tients’ age, sex, residency area (rural or urban, as de-fined by Canada Post based on national postal code), drug plan beneficiary type, drug plan eligibility, physi-

2010 S23
J. Moisan and J.-P. Grégoire
ing a second course of treatment for each antipsychotic drug relative to olanzapine.7 The models were con-trolled for age, beneficiary type, and residency area at treatment initiation; sex; calendar year of first treat-ment initiation; initial prescriber’s specialty; and the following (all in the year before the start of initial treatment): hospital or ambulatory diagnosis of men-tal disorder (schizophrenia [International Classifica-tion of Diseases, Ninth Revision (ICD-9) code 295], bipolar disorder [ICD-9 code 296], other psychoses [ICD-9 codes 290–294 and 297–299], or other mental disorders [ICD-9 codes 300–319]) and mental disorder– related hospitalization (ICD-9 codes 290–319); use of other psychotropic drugs (ATC codes N03, N04, N05AN, N06, and N07); number of different thera-peutic classes; and number of medical visits.
Hazard ratios (HRs) and 95% CIs were calculated. Analyses were performed using SAS version 9.1 (SAS Institute Inc., Cary, North Carolina).
RESULTSStudy Population
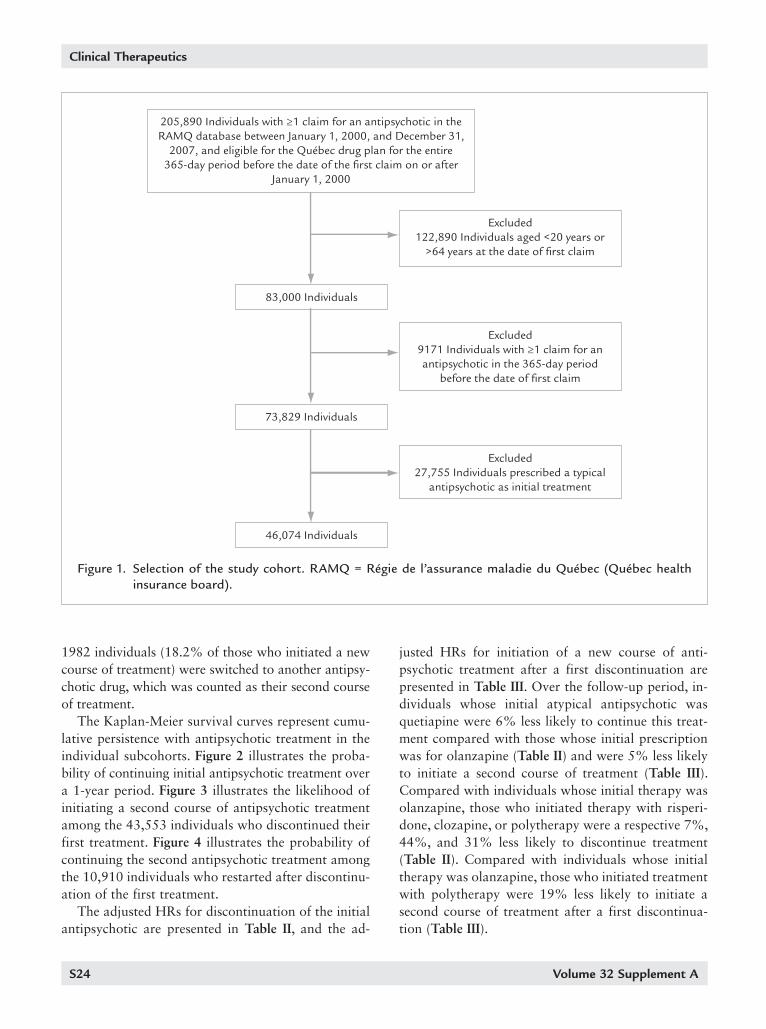
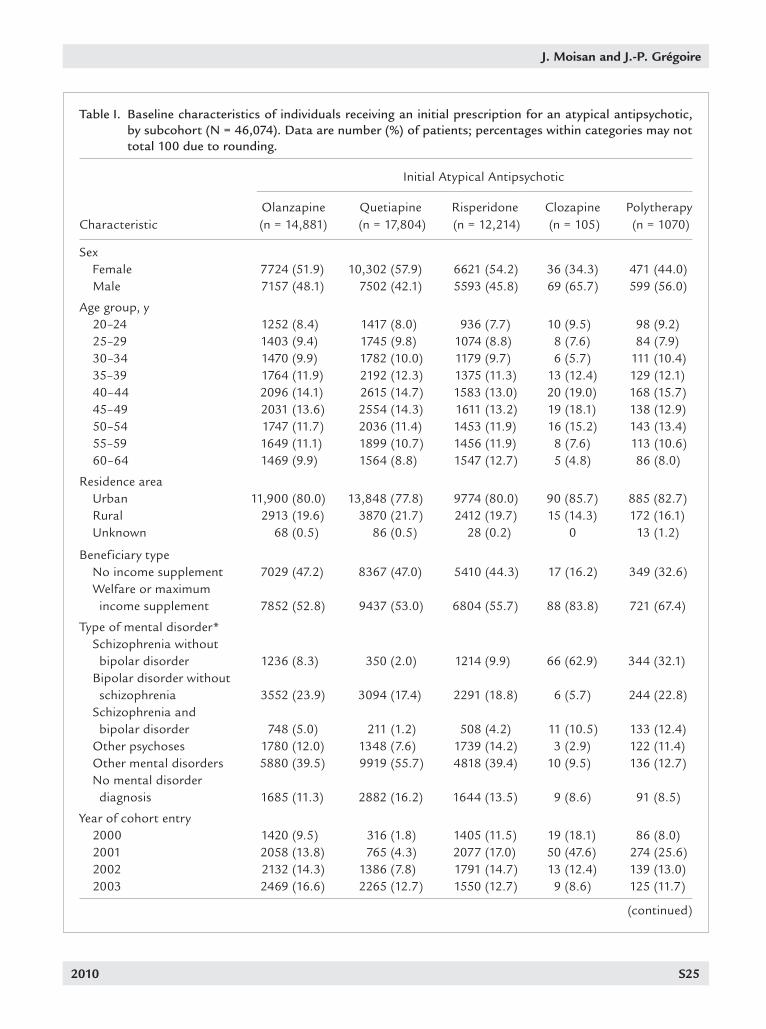
A total of 46,074 individuals were included in the analysis (Figure 1). Characteristics of the study popu-lation are summarized in Table I. The majority of these individuals were female (54.6%) and lived in ur-ban areas (79.2%); the median age ranged from 40 to 44 years. The initial antipsychotic was prescribed pre-dominantly by general practitioners (55.9%). The mean (SD) duration of follow-up was 2.67 (1.91) years. During the study period, 14% of cohort members lost their eligibility for the drug plan and 4% died.
Quetiapine was the initial atypical antipsychotic prescribed for 17,804 individuals (38.6%), followed by olanzapine, risperidone, and clozapine (14,881 [32.3%], 12,214 [26.5%], and 105 [0.2%]), respec-tively. Treatment was initiated with >1 antipsychotic drug in 1070 (2.3%) individuals.
Treatment DiscontinuationA total of 43,553 individuals discontinued their
initial treatment. Among the 10,910 individuals who returned to therapy after a first discontinuation, 4409 (40.4%), 3164 (29.0%), 2512 (23.0%), 19 (0.2%), and 543 (5.0%) initiated a second course of treatment with quetiapine, olanzapine, risperidone, clozapine, and typical antipsychotics, respectively, and 263 (2.4%) received polytherapy as the second course of treat-ment. Before discontinuation of the initial treatment,
Discontinuation AnalysisFive subcohorts were constructed according to the
initial antipsychotic received: either 1 of the 4 atypical antipsychotics covered by the Québec drug plan at the time of the study—olanzapine, quetiapine, risperi-done, and clozapine—or polytherapy (>1 atypical an-tipsychotic, or 1 atypical and 1 typical antipsychotic). Discontinuation of the initial treatment was defined as failure to refill the initial prescription (initial mono-therapy or all initial polytherapy drugs) within 2 times the days’ supply of the previous claim. The discon-tinuation date was calculated as the date of the last refill plus the days’ supply. For individuals who had a claim for another antipsychotic drug (switch) before the date of discontinuation of the initial treatment, the initial treatment was considered to be discontinued on the date of the first claim for the new antipsychotic.
For individuals who discontinued their initial drug treatment, a new course of treatment was defined as initiation of treatment with any antipsychotic drug after discontinuation of the first treatment. Discon-tinuation of the second course of treatment was de-fined as failure to refill a prescription for a second drug treatment within 2 times the days’ supply of the preceding claim.
The number of days from treatment initiation to discontinuation was computed for each of the 5 sub-cohorts, as was the number of days from a first dis-continuation to initiation of a new course of therapy. The time from initiation to discontinuation of a sec-ond course of treatment was assessed according to the antipsychotic drug dispensed at initiation of the sec-ond course.
Days of hospitalization were excluded from the analy-sis, as no information is available in the Med-Écho da-tabase regarding the drugs used during hospitalization.
Statistical AnalysisFrequency distributions were used to describe indi-
vidual characteristics at the time of initiation of atypi-cal antipsychotic treatment. Discontinuation and re-turn to therapy data for each subcohort were assessed longitudinally using Kaplan-Meier curves.
The statistical significance (a priori α level of 0.05) of the differences between Kaplan-Meier curves was analyzed using the log-rank test.7 Cox regression models were used to assess the likelihoods of discon-tinuing treatment, of initiating a second course of treat-ment after a first discontinuation, and of discontinu-
S24 Volume 32 Supplement A
Clinical Therapeutics
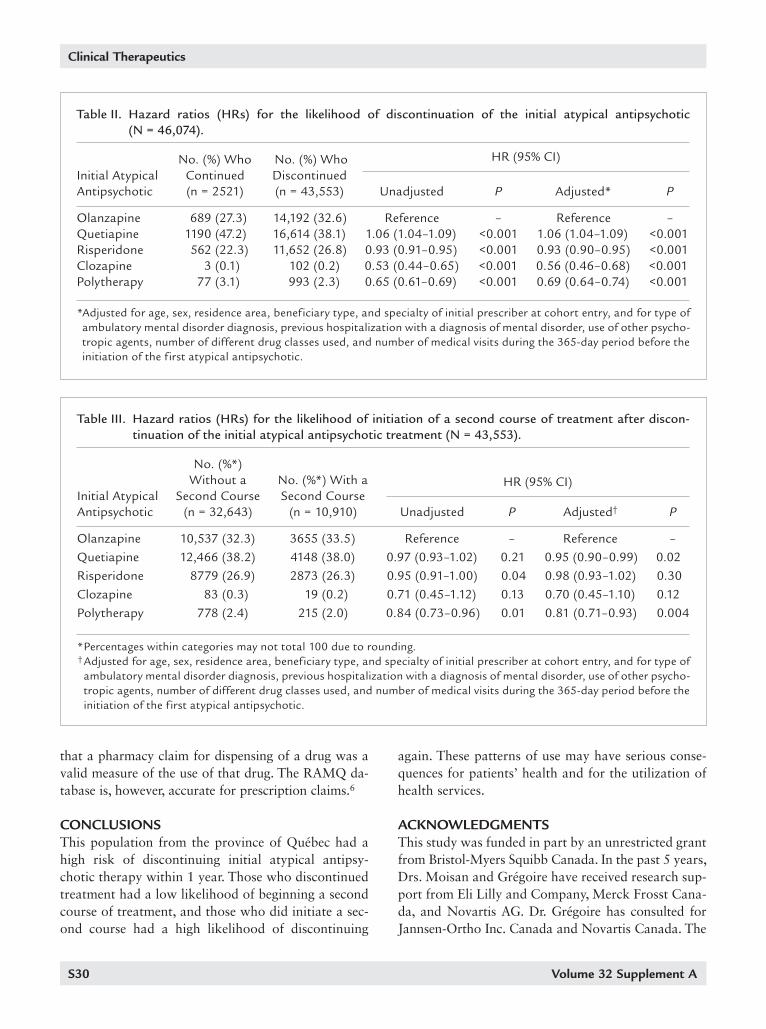
justed HRs for initiation of a new course of anti- psychotic treatment after a first discontinuation are presented in Table III. Over the follow-up period, in-dividuals whose initial atypical antipsychotic was quetiapine were 6% less likely to continue this treat-ment compared with those whose initial prescription was for olanzapine (Table II) and were 5% less likely to initiate a second course of treatment (Table III). Compared with individuals whose initial therapy was olanzapine, those who initiated therapy with risperi-done, clozapine, or polytherapy were a respective 7%, 44%, and 31% less likely to discontinue treatment (Table II). Compared with individuals whose initial therapy was olanzapine, those who initiated treatment with polytherapy were 19% less likely to initiate a second course of treatment after a first discontinua-tion (Table III).
1982 individuals (18.2% of those who initiated a new course of treatment) were switched to another antipsy-chotic drug, which was counted as their second course of treatment.
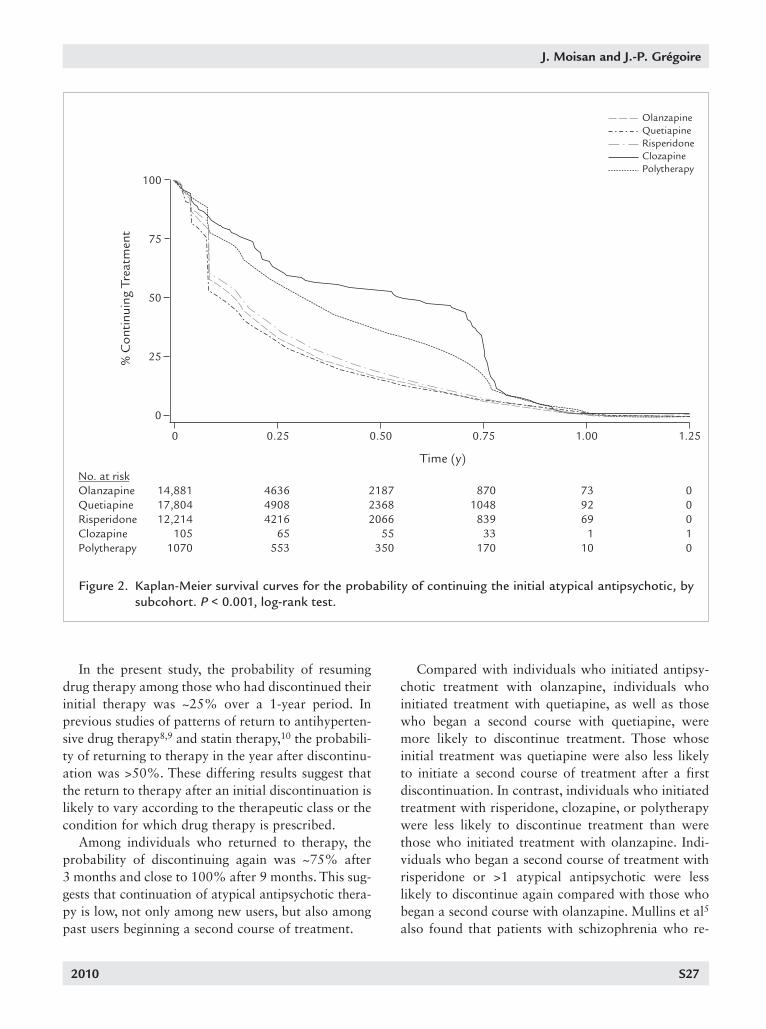
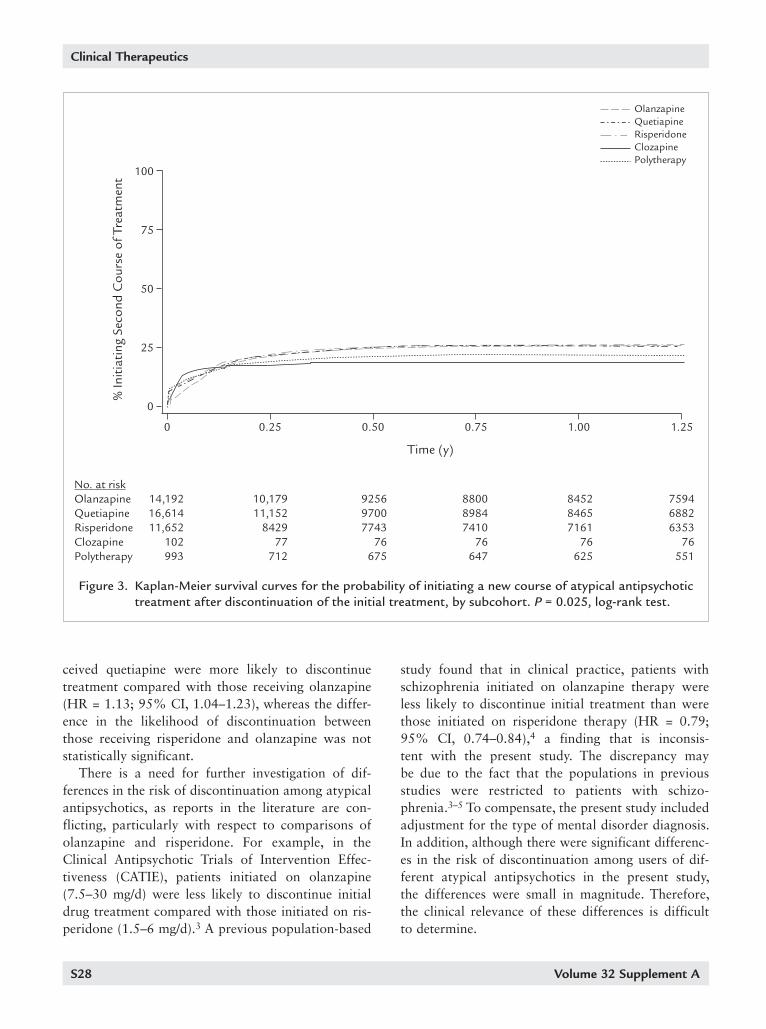
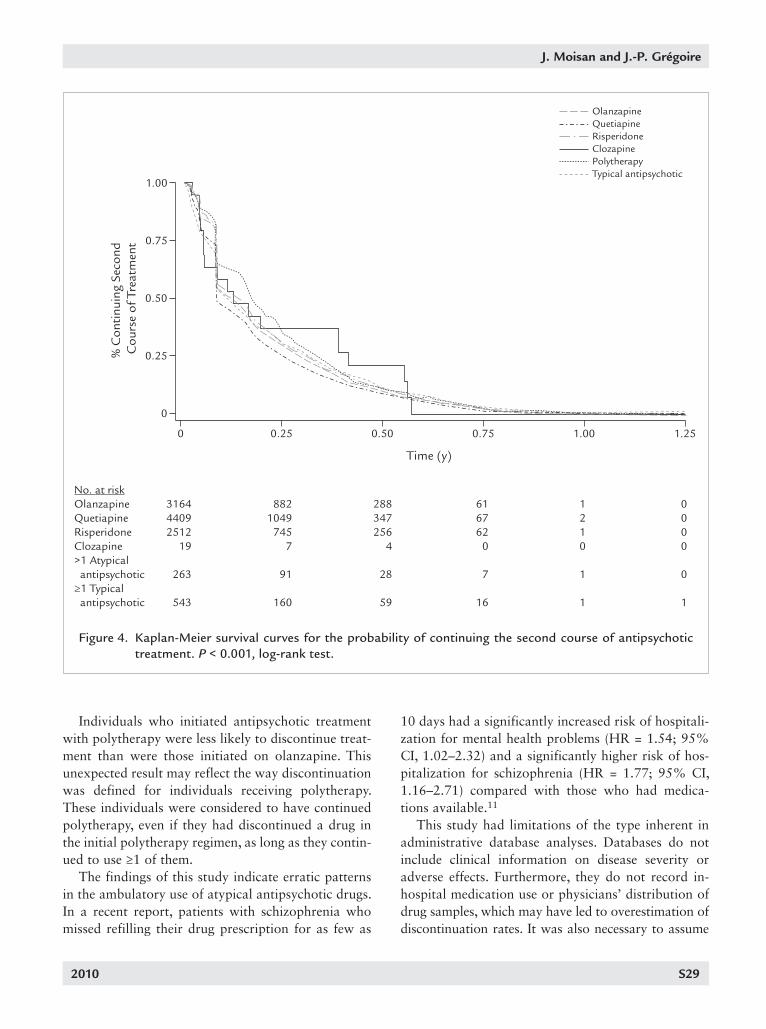
The Kaplan-Meier survival curves represent cumu-lative persistence with antipsychotic treatment in the individual subcohorts. Figure 2 illustrates the proba-bility of continuing initial antipsychotic treatment over a 1-year period. Figure 3 illustrates the likelihood of initiating a second course of antipsychotic treatment among the 43,553 individuals who discontinued their first treatment. Figure 4 illustrates the probability of continuing the second antipsychotic treatment among the 10,910 individuals who restarted after discontinu-ation of the first treatment.
The adjusted HRs for discontinuation of the initial antipsychotic are presented in Table II, and the ad-
Figure 1. Selection of the study cohort. RAMQ = Régie de l’assurance maladie du Québec (Québec health insurance board).
2010 S25
J. Moisan and J.-P. Grégoire
Table I. Baseline characteristics of individuals receiving an initial prescription for an atypical antipsychotic, by subcohort (N = 46,074). Data are number (%) of patients; percentages within categories may not total 100 due to rounding.
Initial Atypical Antipsychotic
Olanzapine Quetiapine Risperidone Clozapine Polytherapy Characteristic (n = 14,881) (n = 17,804) (n = 12,214) (n = 105) (n = 1070)
Sex Female 7724 (51.9) 10,302 (57.9) 6621 (54.2) 36 (34.3) 471 (44.0) Male 7157 (48.1) 7502 (42.1) 5593 (45.8) 69 (65.7) 599 (56.0)
Age group, y 20–24 1252 (8.4) 1417 (8.0) 936 (7.7) 10 (9.5) 98 (9.2) 25–29 1403 (9.4) 1745 (9.8) 1074 (8.8) 8 (7.6) 84 (7.9) 30–34 1470 (9.9) 1782 (10.0) 1179 (9.7) 6 (5.7) 111 (10.4) 35–39 1764 (11.9) 2192 (12.3) 1375 (11.3) 13 (12.4) 129 (12.1) 40–44 2096 (14.1) 2615 (14.7) 1583 (13.0) 20 (19.0) 168 (15.7) 45–49 2031 (13.6) 2554 (14.3) 1611 (13.2) 19 (18.1) 138 (12.9) 50–54 1747 (11.7) 2036 (11.4) 1453 (11.9) 16 (15.2) 143 (13.4) 55–59 1649 (11.1) 1899 (10.7) 1456 (11.9) 8 (7.6) 113 (10.6) 60–64 1469 (9.9) 1564 (8.8) 1547 (12.7) 5 (4.8) 86 (8.0)
Residence area Urban 11,900 (80.0) 13,848 (77.8) 9774 (80.0) 90 (85.7) 885 (82.7) Rural 2913 (19.6) 3870 (21.7) 2412 (19.7) 15 (14.3) 172 (16.1) Unknown 68 (0.5) 86 (0.5) 28 (0.2) 0 13 (1.2)
Beneficiary type No income supplement 7029 (47.2) 8367 (47.0) 5410 (44.3) 17 (16.2) 349 (32.6) Welfare or maximum income supplement 7852 (52.8) 9437 (53.0) 6804 (55.7) 88 (83.8) 721 (67.4)
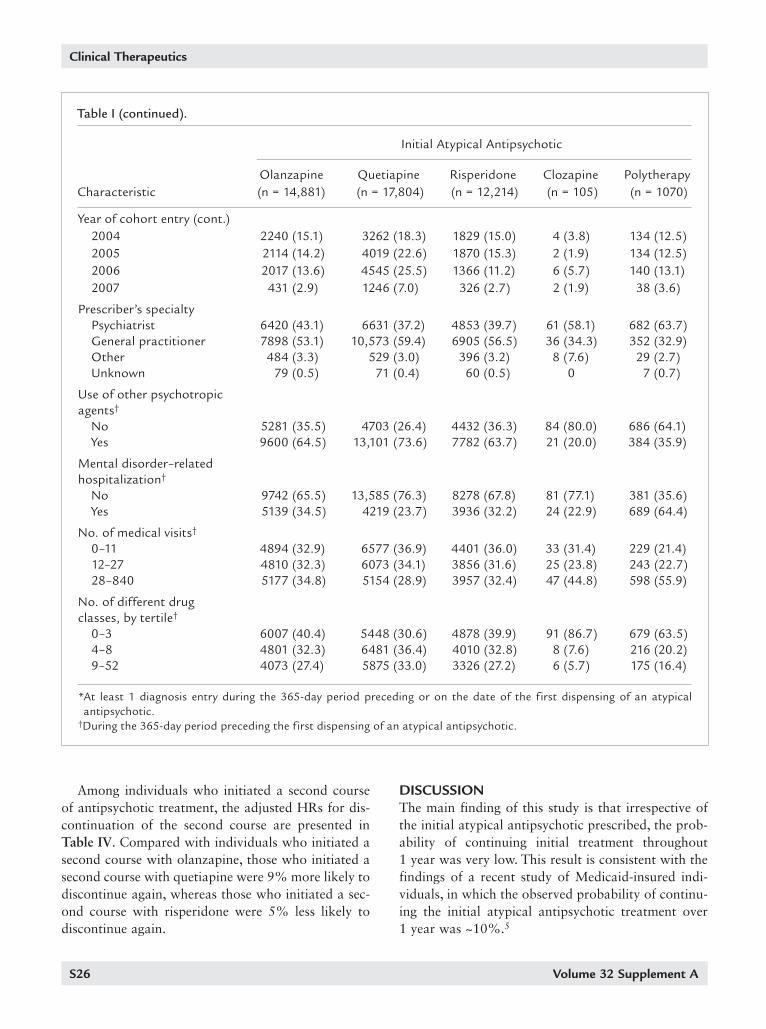
Type of mental disorder* Schizophrenia without bipolar disorder 1236 (8.3) 350 (2.0) 1214 (9.9) 66 (62.9) 344 (32.1) Bipolar disorder without schizophrenia 3552 (23.9) 3094 (17.4) 2291 (18.8) 6 (5.7) 244 (22.8) Schizophrenia and bipolar disorder 748 (5.0) 211 (1.2) 508 (4.2) 11 (10.5) 133 (12.4) Other psychoses 1780 (12.0) 1348 (7.6) 1739 (14.2) 3 (2.9) 122 (11.4) Other mental disorders 5880 (39.5) 9919 (55.7) 4818 (39.4) 10 (9.5) 136 (12.7) No mental disorder diagnosis 1685 (11.3) 2882 (16.2) 1644 (13.5) 9 (8.6) 91 (8.5)
Year of cohort entry 2000 1420 (9.5) 316 (1.8) 1405 (11.5) 19 (18.1) 86 (8.0) 2001 2058 (13.8) 765 (4.3) 2077 (17.0) 50 (47.6) 274 (25.6) 2002 2132 (14.3) 1386 (7.8) 1791 (14.7) 13 (12.4) 139 (13.0) 2003 2469 (16.6) 2265 (12.7) 1550 (12.7) 9 (8.6) 125 (11.7)
(continued)
S26 Volume 32 Supplement A
Clinical Therapeutics
DISCUSSIONThe main finding of this study is that irrespective of the initial atypical antipsychotic prescribed, the prob-ability of continuing initial treatment throughout 1 year was very low. This result is consistent with the findings of a recent study of Medicaid-insured indi-viduals, in which the observed probability of continu-ing the initial atypical antipsychotic treatment over 1 year was ~10%.5
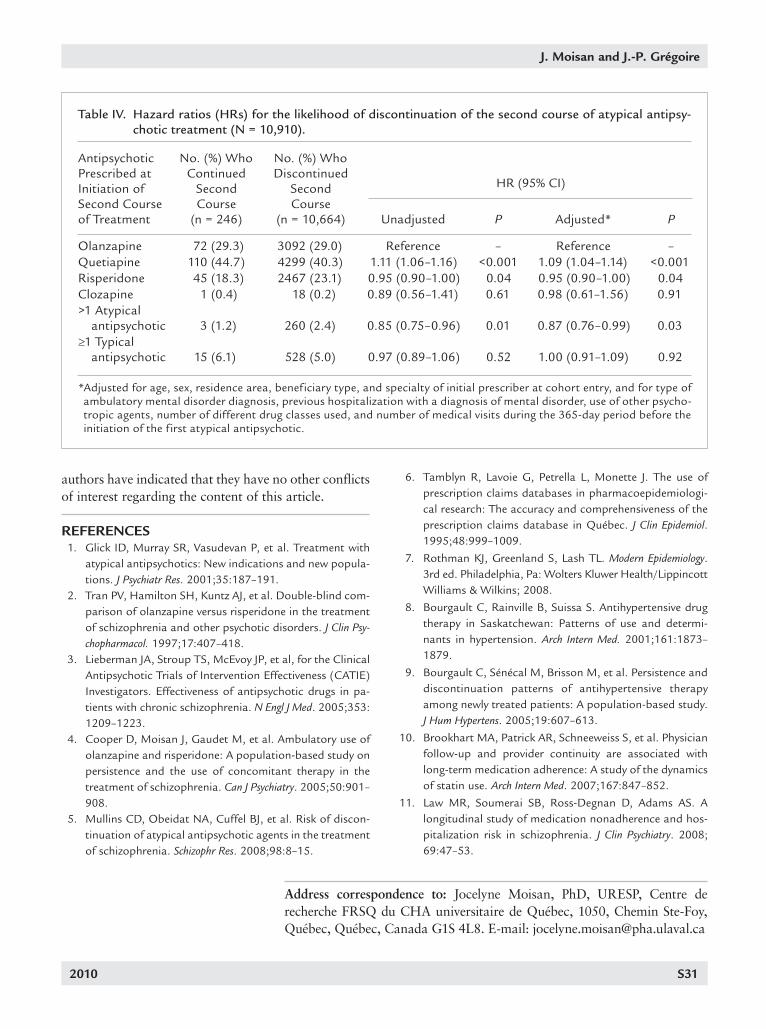
Among individuals who initiated a second course of antipsychotic treatment, the adjusted HRs for dis-continuation of the second course are presented in Table IV. Compared with individuals who initiated a second course with olanzapine, those who initiated a second course with quetiapine were 9% more likely to discontinue again, whereas those who initiated a sec-ond course with risperidone were 5% less likely to discontinue again.
Year of cohort entry (cont.) 2004 2240 (15.1) 3262 (18.3) 1829 (15.0) 4 (3.8) 134 (12.5) 2005 2114 (14.2) 4019 (22.6) 1870 (15.3) 2 (1.9) 134 (12.5) 2006 2017 (13.6) 4545 (25.5) 1366 (11.2) 6 (5.7) 140 (13.1) 2007 431 (2.9) 1246 (7.0) 326 (2.7) 2 (1.9) 38 (3.6)
Prescriber’s specialty Psychiatrist 6420 (43.1) 6631 (37.2) 4853 (39.7) 61 (58.1) 682 (63.7) General practitioner 7898 (53.1) 10,573 (59.4) 6905 (56.5) 36 (34.3) 352 (32.9) Other 484 (3.3) 529 (3.0) 396 (3.2) 8 (7.6) 29 (2.7) Unknown 79 (0.5) 71 (0.4) 60 (0.5) 0 7 (0.7)
Use of other psychotropic agents†
No 5281 (35.5) 4703 (26.4) 4432 (36.3) 84 (80.0) 686 (64.1) Yes 9600 (64.5) 13,101 (73.6) 7782 (63.7) 21 (20.0) 384 (35.9)
Mental disorder–related hospitalization†
No 9742 (65.5) 13,585 (76.3) 8278 (67.8) 81 (77.1) 381 (35.6) Yes 5139 (34.5) 4219 (23.7) 3936 (32.2) 24 (22.9) 689 (64.4)
No. of medical visits†
0–11 4894 (32.9) 6577 (36.9) 4401 (36.0) 33 (31.4) 229 (21.4) 12–27 4810 (32.3) 6073 (34.1) 3856 (31.6) 25 (23.8) 243 (22.7) 28–840 5177 (34.8) 5154 (28.9) 3957 (32.4) 47 (44.8) 598 (55.9)
No. of different drug classes, by tertile†
0–3 6007 (40.4) 5448 (30.6) 4878 (39.9) 91 (86.7) 679 (63.5) 4–8 4801 (32.3) 6481 (36.4) 4010 (32.8) 8 (7.6) 216 (20.2) 9–52 4073 (27.4) 5875 (33.0) 3326 (27.2) 6 (5.7) 175 (16.4)
* At least 1 diagnosis entry during the 365-day period preceding or on the date of the f irst dispensing of an atypical antipsychotic.
†During the 365-day period preceding the f irst dispensing of an atypical antipsychotic.
Table I (continued).
Initial Atypical Antipsychotic
Olanzapine Quetiapine Risperidone Clozapine Polytherapy Characteristic (n = 14,881) (n = 17,804) (n = 12,214) (n = 105) (n = 1070)
2010 S27
J. Moisan and J.-P. Grégoire
Compared with individuals who initiated antipsy-chotic treatment with olanzapine, individuals who initiated treatment with quetiapine, as well as those who began a second course with quetiapine, were more likely to discontinue treatment. Those whose initial treatment was quetiapine were also less likely to initiate a second course of treatment after a first discontinuation. In contrast, individuals who initiated treatment with risperidone, clozapine, or polytherapy were less likely to discontinue treatment than were those who initiated treatment with olanzapine. Indi-viduals who began a second course of treatment with risperidone or >1 atypical antipsychotic were less likely to discontinue again compared with those who began a second course with olanzapine. Mullins et al5 also found that patients with schizophrenia who re-
In the present study, the probability of resuming drug therapy among those who had discontinued their initial therapy was ~25% over a 1-year period. In previous studies of patterns of return to antihyperten-sive drug therapy8,9 and statin therapy,10 the probabili- ty of returning to therapy in the year after discontinu-ation was >50%. These differing results suggest that the return to therapy after an initial discontinuation is likely to vary according to the therapeutic class or the condition for which drug therapy is prescribed.
Among individuals who returned to therapy, the probability of discontinuing again was ~75% after 3 months and close to 100% after 9 months. This sug-gests that continuation of atypical antipsychotic thera- py is low, not only among new users, but also among past users beginning a second course of treatment.
Time (y)No. at riskOlanzapine 14,881 4636 2187 870 73 0Quetiapine 17,804 4908 2368 1048 92 0Risperidone 12,214 4216 2066 839 69 0Clozapine 105 65 55 33 1 1Polytherapy 1070 553 350 170 10 0
% C
ontin
uing
Tre
atm
ent
0.750.500.25 1.000 1.25
OlanzapineQuetiapineRisperidoneClozapinePolytherapy
100
25
0
50
75
Figure 2. Kaplan-Meier survival curves for the probability of continuing the initial atypical antipsychotic, by subcohort. P < 0.001, log-rank test.
S28 Volume 32 Supplement A
Clinical Therapeutics
study found that in clinical practice, patients with schizophrenia initiated on olanzapine therapy were less likely to discontinue initial treatment than were those initiated on risperidone therapy (HR = 0.79; 95% CI, 0.74–0.84),4 a finding that is inconsis- tent with the present study. The discrepancy may be due to the fact that the populations in previous studies were restricted to patients with schizo- phrenia.3–5 To compensate, the present study included adjustment for the type of mental disorder diagnosis. In addition, although there were significant differenc-es in the risk of discontinuation among users of dif- ferent atypical antipsychotics in the present study, the differences were small in magnitude. Therefore, the clinical relevance of these differences is difficult to determine.
ceived quetiapine were more likely to discontinue treatment compared with those receiving olanzapine (HR = 1.13; 95% CI, 1.04–1.23), whereas the differ-ence in the likelihood of discontinuation between those receiving risperidone and olanzapine was not statistically significant.
There is a need for further investigation of dif- ferences in the risk of discontinuation among atypical antipsychotics, as reports in the literature are con- flicting, particularly with respect to comparisons of olanzapine and risperidone. For example, in the Clinical Antipsychotic Trials of Intervention Effec- tiveness (CATIE), patients initiated on olanzapine (7.5–30 mg/d) were less likely to discontinue initial drug treatment compared with those initiated on ris-peridone (1.5–6 mg/d).3 A previous population-based
Time (y)
No. at riskOlanzapine 14,192 10,179 9256 8800 8452 7594Quetiapine 16,614 11,152 9700 8984 8465 6882Risperidone 11,652 8429 7743 7410 7161 6353Clozapine 102 77 76 76 76 76Polytherapy 993 712 675 647 625 551
% In
itiat
ing
Seco
nd C
ours
e of
Tre
atm
ent
0.750.500.25 1.000 1.25
OlanzapineQuetiapineRisperidoneClozapinePolytherapy
100
25
0
50
75
Figure 3. Kaplan-Meier survival curves for the probability of initiating a new course of atypical antipsychotic treatment after discontinuation of the initial treatment, by subcohort. P = 0.025, log-rank test.
2010 S29
J. Moisan and J.-P. Grégoire
10 days had a significantly increased risk of hospitali- zation for mental health problems (HR = 1.54; 95% CI, 1.02–2.32) and a significantly higher risk of hos-pitalization for schizophrenia (HR = 1.77; 95% CI, 1.16–2.71) compared with those who had medica-tions available.11
This study had limitations of the type inherent in administrative database analyses. Databases do not include clinical information on disease severity or adverse effects. Furthermore, they do not record in-hospital medication use or physicians’ distribution of drug samples, which may have led to overestimation of discontinuation rates. It was also necessary to assume
Individuals who initiated antipsychotic treatment with polytherapy were less likely to discontinue treat-ment than were those initiated on olanzapine. This unexpected result may reflect the way discontinuation was defined for individuals receiving polytherapy. These individuals were considered to have continued polytherapy, even if they had discontinued a drug in the initial polytherapy regimen, as long as they contin-ued to use ≥1 of them.
The findings of this study indicate erratic patterns in the ambulatory use of atypical antipsychotic drugs. In a recent report, patients with schizophrenia who missed refilling their drug prescription for as few as
No. at riskOlanzapine 3164 882 288 61 1 0Quetiapine 4409 1049 347 67 2 0Risperidone 2512 745 256 62 1 0Clozapine 19 7 4 0 0 0>1 Atypical antipsychotic 263 91 28 7 1 0≥1 Typical antipsychotic 543 160 59 16 1 1
% C
ontin
uing
Sec
ond
Cou
rse
of T
reat
men
t
0.750.500.25 1.000 1.25
Time (y)
OlanzapineQuetiapineRisperidoneClozapinePolytherapyTypical antipsychotic
1.00
0.25
0
0.50
0.75
Figure 4. Kaplan-Meier survival curves for the probability of continuing the second course of antipsychotic treatment. P < 0.001, log-rank test.
S30 Volume 32 Supplement A
Clinical Therapeutics
again. These patterns of use may have serious conse-quences for patients’ health and for the utilization of health services.
ACKNOWLEDGMENTSThis study was funded in part by an unrestricted grant from Bristol-Myers Squibb Canada. In the past 5 years, Drs. Moisan and Grégoire have received research sup-port from Eli Lilly and Company, Merck Frosst Cana- da, and Novartis AG. Dr. Grégoire has consulted for Jannsen-Ortho Inc. Canada and Novartis Canada. The
that a pharmacy claim for dispensing of a drug was a valid measure of the use of that drug. The RAMQ da-tabase is, however, accurate for prescription claims.6
CONCLUSIONSThis population from the province of Québec had a high risk of discontinuing initial atypical antipsy-chotic therapy within 1 year. Those who discontinued treatment had a low likelihood of beginning a second course of treatment, and those who did initiate a sec-ond course had a high likelihood of discontinuing
Table III. Hazard ratios (HRs) for the likelihood of initiation of a second course of treatment after discon-tinuation of the initial atypical antipsychotic treatment (N = 43,553).
No. (%*) Without a No. (%*) With a Initial Atypical Second Course Second Course Antipsychotic (n = 32,643) (n = 10,910) Unadjusted P Adjusted† P
Olanzapine 10,537 (32.3) 3655 (33.5) Reference – Reference –Quetiapine 12,466 (38.2) 4148 (38.0) 0.97 (0.93–1.02) 0.21 0.95 (0.90–0.99) 0.02Risperidone 8779 (26.9) 2873 (26.3) 0.95 (0.91–1.00) 0.04 0.98 (0.93–1.02) 0.30Clozapine 83 (0.3) 19 (0.2) 0.71 (0.45–1.12) 0.13 0.70 (0.45–1.10) 0.12Polytherapy 778 (2.4) 215 (2.0) 0.84 (0.73–0.96) 0.01 0.81 (0.71–0.93) 0.004
* Percentages within categories may not total 100 due to rounding. † Adjusted for age, sex, residence area, beneficiary type, and specialty of initial prescriber at cohort entry, and for type of
ambulatory mental disorder diagnosis, previous hospitalization with a diagnosis of mental disorder, use of other psycho-tropic agents, number of different drug classes used, and number of medical visits during the 365-day period before the initiation of the f irst atypical antipsychotic.
HR (95% CI)
Table II. Hazard ratios (HRs) for the likelihood of discontinuation of the initial atypical antipsychotic (N = 46,074).
No. (%) Who No. (%) Who Initial Atypical Continued Discontinued Antipsychotic (n = 2521) (n = 43,553) Unadjusted P Adjusted* P
Olanzapine 689 (27.3) 14,192 (32.6) Reference – Reference –Quetiapine 1190 (47.2) 16,614 (38.1) 1.06 (1.04–1.09) <0.001 1.06 (1.04–1.09) <0.001Risperidone 562 (22.3) 11,652 (26.8) 0.93 (0.91–0.95) <0.001 0.93 (0.90–0.95) <0.001Clozapine 3 (0.1) 102 (0.2) 0.53 (0.44–0.65) <0.001 0.56 (0.46–0.68) <0.001Polytherapy 77 (3.1) 993 (2.3) 0.65 (0.61–0.69) <0.001 0.69 (0.64–0.74) <0.001
* Adjusted for age, sex, residence area, beneficiary type, and specialty of initial prescriber at cohort entry, and for type of ambulatory mental disorder diagnosis, previous hospitalization with a diagnosis of mental disorder, use of other psycho-tropic agents, number of different drug classes used, and number of medical visits during the 365-day period before the initiation of the f irst atypical antipsychotic.
HR (95% CI)
2010 S31
J. Moisan and J.-P. Grégoire
6. Tamblyn R, Lavoie G, Petrella L, Monette J. The use of prescription claims databases in pharmacoepidemiologi-cal research: The accuracy and comprehensiveness of the prescription claims database in Québec. J Clin Epidemiol. 1995;48:999–1009.
7. Rothman KJ, Greenland S, Lash TL. Modern Epidemiology. 3rd ed. Philadelphia, Pa: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008.
8. Bourgault C, Rainville B, Suissa S. Antihypertensive drug therapy in Saskatchewan: Patterns of use and determi-nants in hypertension. Arch Intern Med. 2001;161:1873– 1879.
9. Bourgault C, Sénécal M, Brisson M, et al. Persistence and discontinuation patterns of antihypertensive therapy among newly treated patients: A population-based study. J Hum Hypertens. 2005;19:607–613.
10. Brookhart MA, Patrick AR, Schneeweiss S, et al. Physician follow-up and provider continuity are associated with long-term medication adherence: A study of the dynamics of statin use. Arch Intern Med. 2007;167:847–852.
11. Law MR, Soumerai SB, Ross-Degnan D, Adams AS. A longitudinal study of medication nonadherence and hos-pitalization risk in schizophrenia. J Clin Psychiatry. 2008; 69:47–53.
authors have indicated that they have no other conflicts of interest regarding the content of this article.
REFERENCES 1. Glick ID, Murray SR, Vasudevan P, et al. Treatment with
atypical antipsychotics: New indications and new popula-tions. J Psychiatr Res. 2001;35:187–191.
2. Tran PV, Hamilton SH, Kuntz AJ, et al. Double-blind com-parison of olanzapine versus risperidone in the treatment of schizophrenia and other psychotic disorders. J Clin Psy-chopharmacol. 1997;17:407–418.
3. Lieberman JA, Stroup TS, McEvoy JP, et al, for the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Investigators. Effectiveness of antipsychotic drugs in pa-tients with chronic schizophrenia. N Engl J Med. 2005;353: 1209–1223.
4. Cooper D, Moisan J, Gaudet M, et al. Ambulatory use of olanzapine and risperidone: A population-based study on persistence and the use of concomitant therapy in the treatment of schizophrenia. Can J Psychiatry. 2005;50:901– 908.
5. Mullins CD, Obeidat NA, Cuffel BJ, et al. Risk of discon-tinuation of atypical antipsychotic agents in the treatment of schizophrenia. Schizophr Res. 2008;98:8–15.
Table IV. Hazard ratios (HRs) for the likelihood of discontinuation of the second course of atypical antipsy-chotic treatment (N = 10,910).
Antipsychotic No. (%) Who No. (%) Who Prescribed at Continued Discontinued Initiation of Second Second Second Course Course Course of Treatment (n = 246) (n = 10,664) Unadjusted P Adjusted* P
Olanzapine 72 (29.3) 3092 (29.0) Reference – Reference –Quetiapine 110 (44.7) 4299 (40.3) 1.11 (1.06–1.16) <0.001 1.09 (1.04–1.14) <0.001Risperidone 45 (18.3) 2467 (23.1) 0.95 (0.90–1.00) 0.04 0.95 (0.90–1.00) 0.04Clozapine 1 (0.4) 18 (0.2) 0.89 (0.56–1.41) 0.61 0.98 (0.61–1.56) 0.91>1 Atypical antipsychotic 3 (1.2) 260 (2.4) 0.85 (0.75–0.96) 0.01 0.87 (0.76–0.99) 0.03≥1 Typical antipsychotic 15 (6.1) 528 (5.0) 0.97 (0.89–1.06) 0.52 1.00 (0.91–1.09) 0.92
* Adjusted for age, sex, residence area, beneficiary type, and specialty of initial prescriber at cohort entry, and for type of ambulatory mental disorder diagnosis, previous hospitalization with a diagnosis of mental disorder, use of other psycho-tropic agents, number of different drug classes used, and number of medical visits during the 365-day period before the initiation of the f irst atypical antipsychotic.
HR (95% CI)
Address correspondence to: Jocelyne Moisan, PhD, URESP, Centre de recherche FRSQ du CHA universitaire de Québec, 1050, Chemin Ste-Foy, Québec, Québec, Canada G1S 4L8. E-mail: [email protected]