pathways, power & pitfalls - virologyresearch.unsw.edu.au · molecular diagnostics • major...
TRANSCRIPT
Viral PCRPathways, Power & Pitfalls
Neisha Jeoffreys

Molecular Diagnostics
• Major advances in recent years• Discovered in 1983 - specialist only, extremely
expensive• Over last 25 years
– Cheaper– Faster– Commercial kits & reagents
• NAA has moved from specialist only to a routine diagnostic tool

Why use NAAT?
• Sensitive • Specific• Versatile• Poor quality specimens – FFPE• Faster
– How fast is it really? – batch testing common– Not POC

• RNA – reverse transcriptase• Traditionally block thermocycler & gel analysis• Approx 4-5 hours, size discrimination - confirmation for specificity
Polymerase Chain Reaction (PCR)Double stranded DNA Denaturation
Annealing Primers
ExtensionTaq polymerase
ACGTTAG
GCCAGTGCACT dNTPs
2 strands of Double stranded DNA

Real Time PCR• Fluorescent probes or dyes• During amplification, an increase in fluorescence
which correlates with the amount of DNA produced• Detected in real time• Very fast - 1 hour• Reduced contamination

How does RT PCR work? SYBR green
Intercalating dye
Non specific binding to any double stranded DNA

Melt Curves

Real Time PCR Hydrolysis Probes
Specific, no further confirmation required
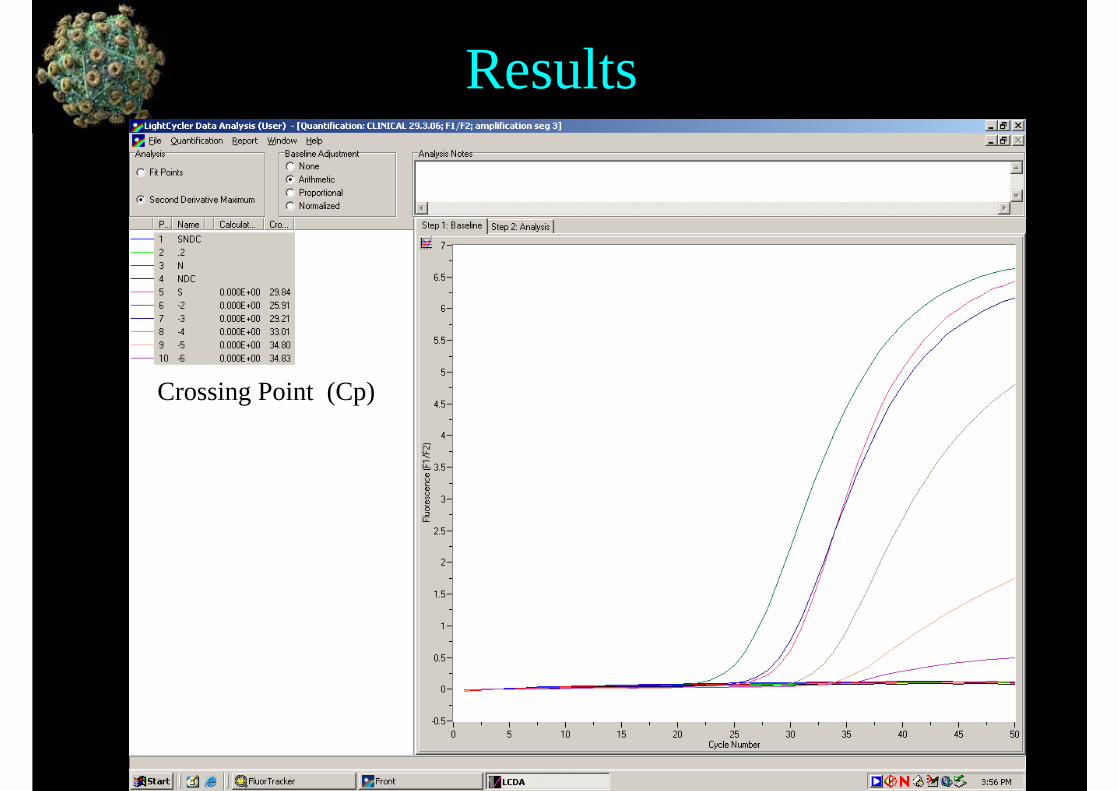
Results
Crossing Point (Cp)

Where does PCR fit in the Clinical Laboratory?
• Detection–Single Target–Multiple Targets
• Quantitation• Resistance testing• Subtyping

PCR for Detection of Herpes Simplex Virus (HSV)?
– Culture • Acute infection, correct transport conditions• Excellent sensitivity• Result in 2-3 days
– Direct Fluorescent Antibody (DFA)• Result in 2 hours • acute infection & specific sample types• Sensitivity dependant on collection & expertise (up to 80%)
– Serology• Poor sensitivity and specificity• Paired sera• Congenital & latent infections

PCR for Detection of Herpes Simplex Virus (HSV)?
• PCR– Excellent sensitivity (90 –95%)– Specific - differentiate HSV 1 & 2– Same day result – Acute infection, all sample types– Not reliant on specimen transport conditions
• But…..– Too expensive for one-off testing – Resistance testing requires culture

PCR for detection of all viruses?• Arbovirus
– Serology test of choice– Humans are an accidental host– Period of viraemia too short
• Hepatitis C– Serology used routinely– PCR
• Resolve equivocal serology• Detect early infections in window period• Identify active infection in HCV antibody + pregnant women• Monitoring while on antiviral therapy

Where does PCR fit in the Clinical Laboratory?
• Detection–Single Target–Multiple Targets
• Quantitation• Resistance testing• Subtyping
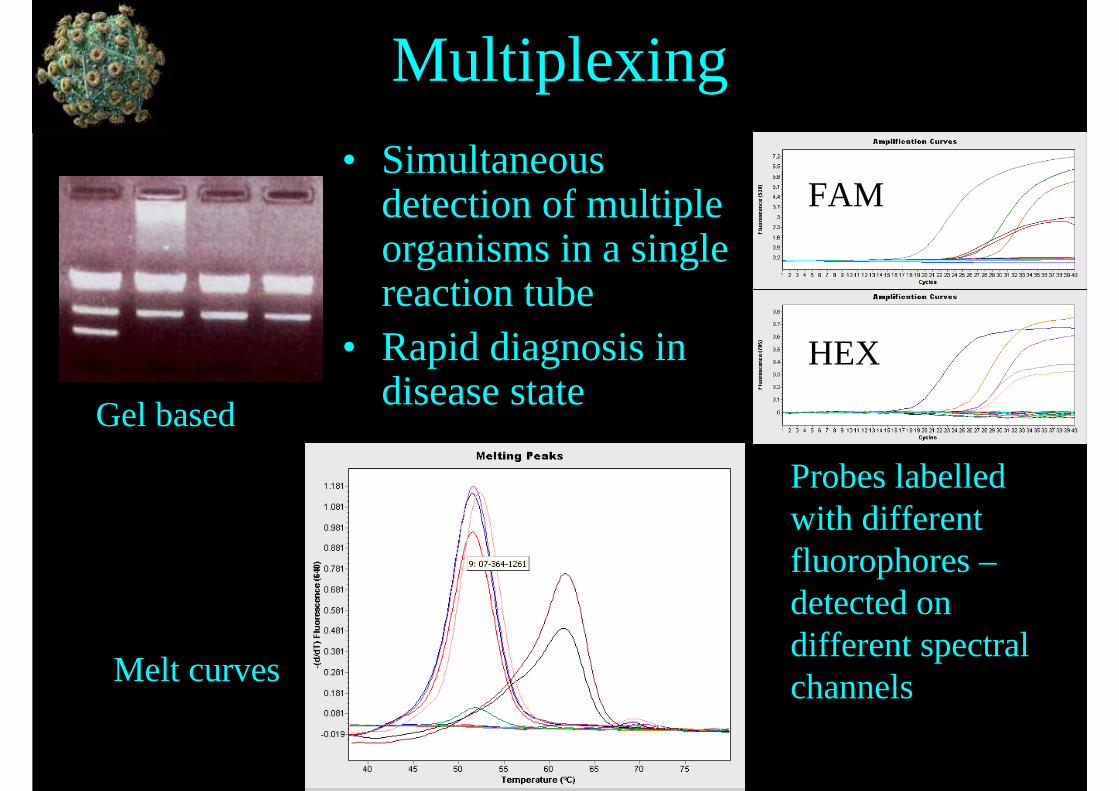
Multiplexing• Simultaneous
detection of multiple organisms in a single reaction tube
• Rapid diagnosis in disease stateGel based
Probes labelledwith different fluorophores –detected on different spectral channelsMelt curves
FAM
HEX

RSV / Flu A / Flu B Multiplex
•Technically difficult–Cross reaction between fluorescent channels–3 – 4 targets maximum–Competition between targets common
Significant impact when dual infections present
–H5N1 PCR single target
RSV
Flu A
Flu B

Multiplex Tandem PCR (MT-PCR)
• Commercial systems – AusDiagnostics1st amplification
– Up to 72 primer pairs multiplexed– Very short – enrichment
2nd amplification– Product diluted into single primer/probe reactions– Detected using same channel and recorded as positive
or negative for that target
• Increased sensitivity and specificity• Avoid problems of competition and cross reaction• Increased risk of contamination

Influenza Profile 1
9
8
7
6
5
4
3
2
1No.
Artificial sequence for assay control SPIKE
"non-POU domain containing, octamer-binding"
NONO
5' UTR of Rhinovirus RV
Respiratory Syncytial Virus L geneRSV
NP segment of influenza B consensus Pan-INF-B
NP segment of influenzaPan-INF-A
Hemagglutinin H5 HA-H5
Hemagglutinin HA-H3
Influenza H1HA-H1DescriptionGenes72 well gene Disc with 9 genes x 8 samples
NONO, human gene contol
SPIKE, Assay control, inhibition control and as a normalized genes against gene of interest
Kiran Thapa

Viral Respiratory Infection Validation
99%100 %100 %100%100 %100 %100 %Specificity
86%100 %100 %92%100 %100 %94 %Sensitivity
691760750403700720233-
1*601020340705051+MT-PCR Result
-+-+-+-+-+-+-+
RVRSVFlu BH5H3H1Flu ACell Culture
• Discordant results– 3 H5 (Irradiated specimen, negative by other
PCR)– 1 RV negative– Picornavirus by culture and RV by MT-PCR
77 clinical isolate tested by Influenza Profile Disc 1 & cell culture
Kiran Thapa
Where does PCR fit in the Clinical Laboratory?
• Detection–Single Target–Multiple Targets
• Quantitation• Resistance testing• Subtyping

Quantitation of Viral Load

Uses of Quantitation• Monitor disease progression
– HIV plasma viral load• Monitor treatment efficacy
– HIV – RNA as a surrogate marker– HCV – test pre treatment and at 12 weeks
• Monitor immunosuppression – BK in renal transplant patients– Immunosuppression BK – nephropathy– Immunosuppression BK - rejection
When to treat?• CMV infection prevalent in solid organ,
BM transplant & immunosuppressed• Asymptomatic or symptomatic• Not all patients require pre-emptive therapyBut….• Appropriate cut off?• PP65 antigenemia – always treat• Depends on patient type, specimen type,
test performed• Standardisation difficult

Where does PCR fit in the Clinical Laboratory?
• Detection–Single Target–Multiple Targets
• Quantitation• Resistance testing• Subtyping

Resistance Testing• HIV, Influenza, HSV, CMV, VZV, HBV, HCV• Genotypic – point mutations, specific target
HIV – major mutations at drug contact sites– minor mutations restore viral fitness– Signature mutations– Amplify regions spanning protease and reverse
transcriptase genes– Sequencing & analysis– Resistance panel

Resistance Panel

Detection of drug hypersensitivity• HLA-B 5701 allele• Life threatening hypersensitivity to
Abacavir• 7-9 % population carries gene• All HIV patients tested prior to treatment
Housekeeping gene 439 bp
B57 allele 197bp
B5701 allele 117bp

Where does PCR fit in the Clinical Laboratory?
• Detection–Single Target–Multiple Targets
• Quantitation• Resistance testing• Subtyping

Molecular Subtyping• HSV 1 encephalitis / HSV 2 aseptic meningitis
• Human Papillomavirus (HPV)– High risk types & cervical cancer– Epidemiological studies – vaccine trials– Medico-legal cases
• Influenza– H3 & H1 subtyping– Vaccine development– H1 resistance to TamiFlu

High Resolution Melt analysis(HRM)
• Explore genetic variation in PCR products based on melting temperature
• SNPs easily identified• VZV
Heterozygous mutation
Homozygous mutation
Wild type curves

Pitfalls of Viral Molecular Diagnostics
• Contamination & Inhibition– Good Molecular Biology practice– Correct use of effective controls
• NDC, spike or house-keeping genes (inhibition and amp efficiency)
• Extraction of RNA viruses – easily degraded & quality essential– Specimen transport affects results– Extraction control
Genetic Diversity• Assay design for large viral families
– Enterovirus – over 100 subtypes– Identification of conserved regions– Are all subtypes detected equally?
• Genetic Drift– High replication, poor proof reading of reverse transcriptase– Periodic target review– Yearly changes to assays for Influenza
• Genetic Re-assortment– Influenza – H5N1– Identification of circulating strains

RSV Genetic Drift
Genetic Drift / Low viral load / Dual Infection ?

In house vs Commercial• Commercial
– Easy to use but expensive– Require expert analysis & trained personnel as subject to same
pitfalls– Well validated - consistent performance?– Built in controls– No further laboratory QC requirements – Only available for common organisms
• In-house– Unique primer/probe or literature adaptation– Easily changed to suit genetic drift– Cost effective– Variable validation & quality control– Wide range of efficacy– New legislation & regulation (NPAAC & TGA)

NPAAC & TGA• Regulation of In-house IVD devices
– Introduce quality into the system– Historically NPAAC standards for good laboratory
practice – NATA - Quality control documentation– External QAP assessed performance
• New NPAAC Standards inc TGA Guidelines– Standards for Good Manufacturing Practices– Quality control assessed at every step of the process,
from initial literature review to end result– Requires review of quality of product– May see a lot of labs move to commercial assays– Will provide standardised level of performance

Conclusion• PCR come along way in the last 25 years• Readily available to most laboratories• Not always the most appropriate test• Real time PCR enhanced capabilities• Detection of single & multiple targets,
Quantitation, Resistance Detection & Subtyping• Powerful tool in clinical diagnostic lab• But pitfalls common • Our responsibility to ensure we have a quality
detection system – commercial or in house.

With great power, comes great responsibility….
Acknowledgements
• Greg James• Dominic Dwyer• Mala Ratnamohan• Ken McPhie• David Dickeson• Evelyn Crewe• Sophie Branch
• Kiran Thapa• Linda Donovan• Terry Flood• Julia Warning• Rady Kim• Mary Faragalla