pathophysiological basis of adjustment of glomerulotubular balance in crf and pathophysiology of crf
TRANSCRIPT
PATHOPHYSIOLOGICAL BASIS OF ADJUSTMENT OF GLOMERULOTUBULAR BALANCE IN CRF AND PATHOPHYSIOLOGY OF CRF
CHAIR PERSONDR. B. KUMARSPEAKERKOUSHIK MUKHERJEE
CONTENTS• GLOMERULO TUBULAR BALANCE(GTB)• PATHOLOGICAL CONSIDERATION IN CRF• ADJUSTMENT OF GTB IN CRF• TREATMENT TARGETS
GLOMERULO TUBULAR BALANCE• Glomerulotubular Balance refers to the phenomenon
whereby a constant fraction of the filtered load of the nephron is resorbed across a range of Glomerular Filtration Rates (GFR).
• In other words, if the GFR spontaneously increases, the rate of water and solute resorption in the tubule proportionally increases, thus maintaining the same fraction the filtered load being resorbed.
MECHANISM OF GTB• Operates in PCT where 67% of filtered load reabsorbed
regardless the value of GFR.• Precise mechanism unknown.• Appears to act completely independently of
neuroendocrine regulatory mechanisms.• Changes in GFR result in modification of the Starling
forces in the peritubular capillaries resulting in proportionally increased or decreased total nephronic resorption.
• Recently, a luminal mechanism has also been identified in which shear strain on the proximal tubule brush border activates apical co-transporters.
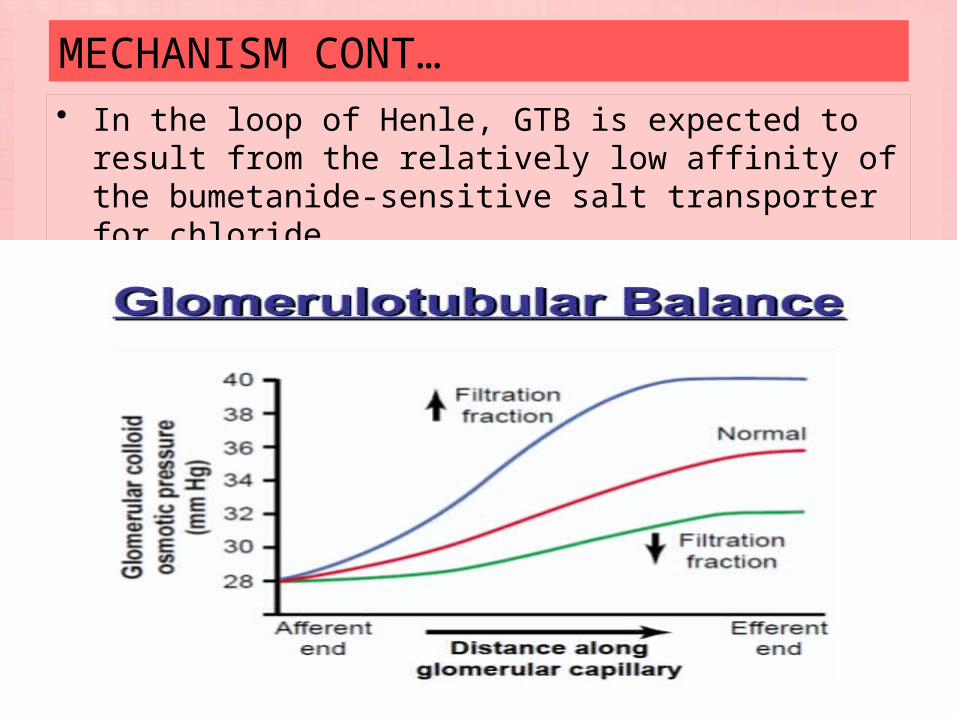
MECHANISM CONT…• In the loop of Henle, GTB is expected to result from the
relatively low affinity of the bumetanide-sensitive salt transporter for chloride.
SIGNIFICANCE OF GTB• A critical mechanism which protects distal segments of
the nephron from being overloaded in contexts of short-term increases in GFR.
• can be thought of as an additional layer of protection if mechanisms of tubuloglomerular feedback, that normalize rates of GFR, momentarily fail or are slow to be triggered.
• Avoid disruption of distal tubular regulation.• Maintain the volume & composition of final urine.
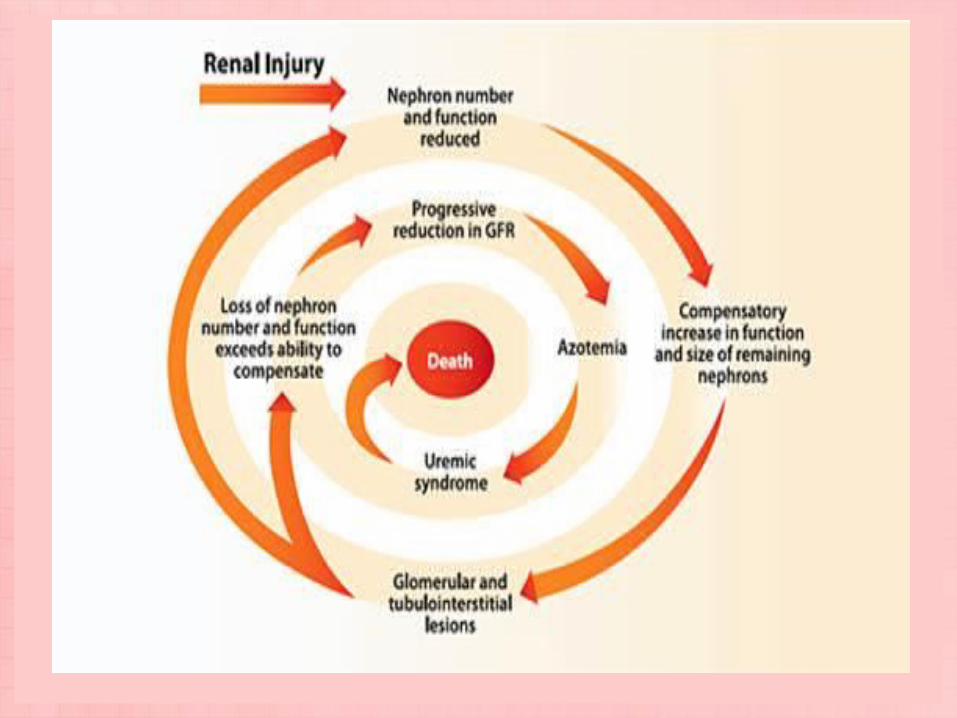
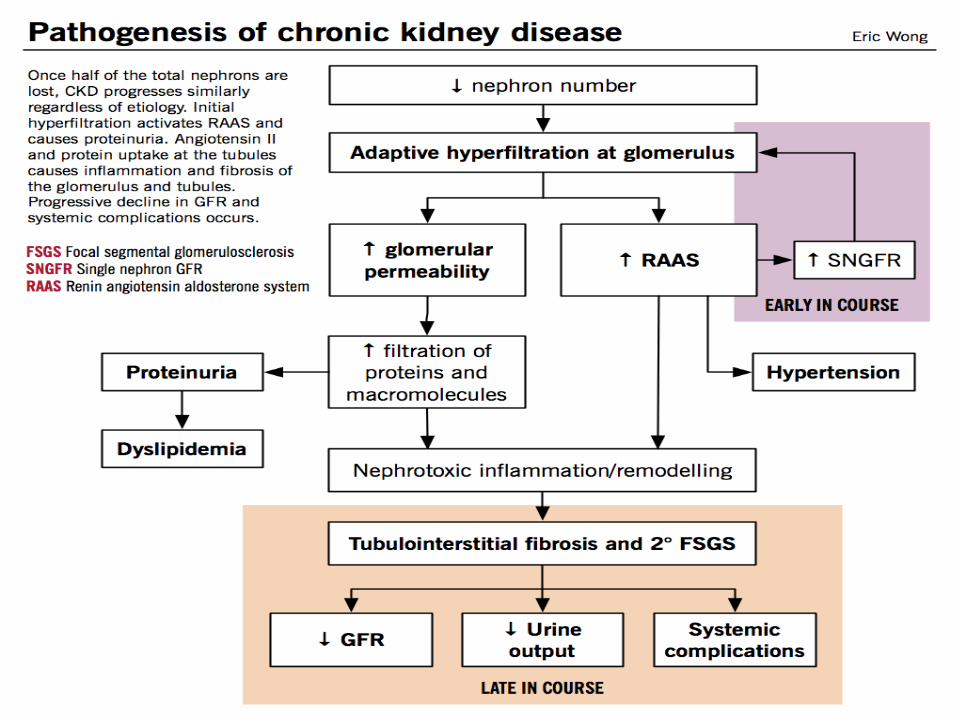
CHRONIC RENAL FAILURE• The term chronic renal failure applies to the process of
continuing significant irreversible reduction in nephron number and typically corresponds to CKD stages 3–5.
• Short term adaptations of hypertrophy and hyperfiltration of viable nephrons in case of nephron loss in chronic kidney disease.
• Adaptive mechanisms become maladaptive as the increased pressure and flow within the nephron predisposes to disruption of the filtration barrier leading to sclerosis and dropout of the remaining nephrons.
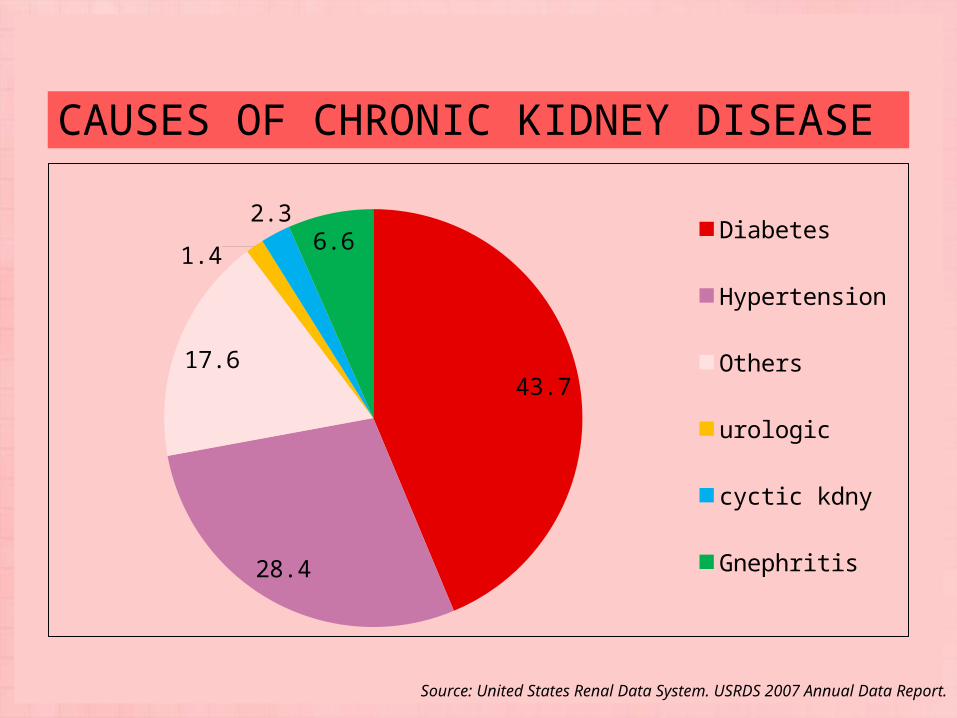
CAUSES OF CHRONIC KIDNEY DISEASE
43.7
28.4
17.6
1.42.36.6 Diabetes
Hypertension
Others
urologic
cyctic kdny
Gnephritis
Source: United States Renal Data System. USRDS 2007 Annual Data Report.
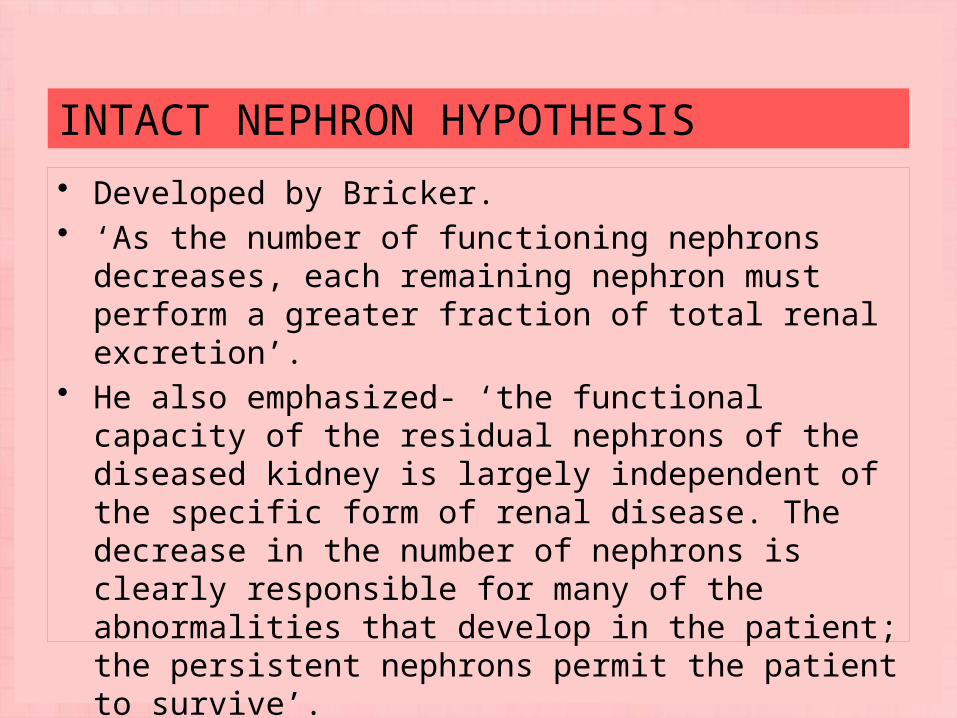
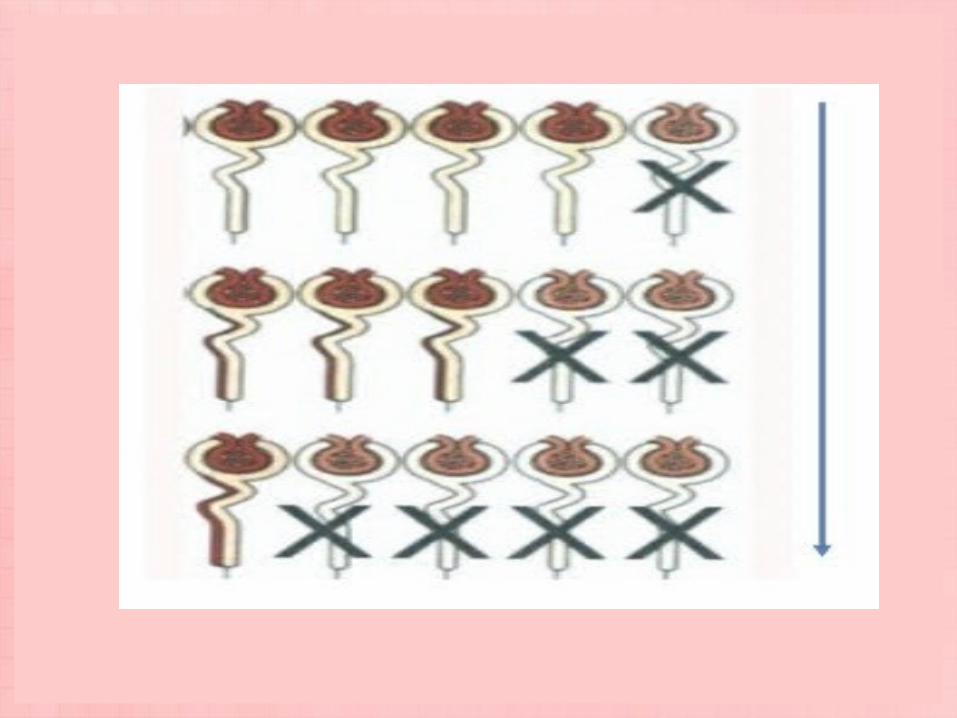
INTACT NEPHRON HYPOTHESIS• Developed by Bricker.• ‘As the number of functioning nephrons decreases, each
remaining nephron must perform a greater fraction of total renal excretion’.
• He also emphasized- ‘the functional capacity of the residual nephrons of the diseased kidney is largely independent of the specific form of renal disease. The decrease in the number of nephrons is clearly responsible for many of the abnormalities that develop in the patient; the persistent nephrons permit the patient to survive’.
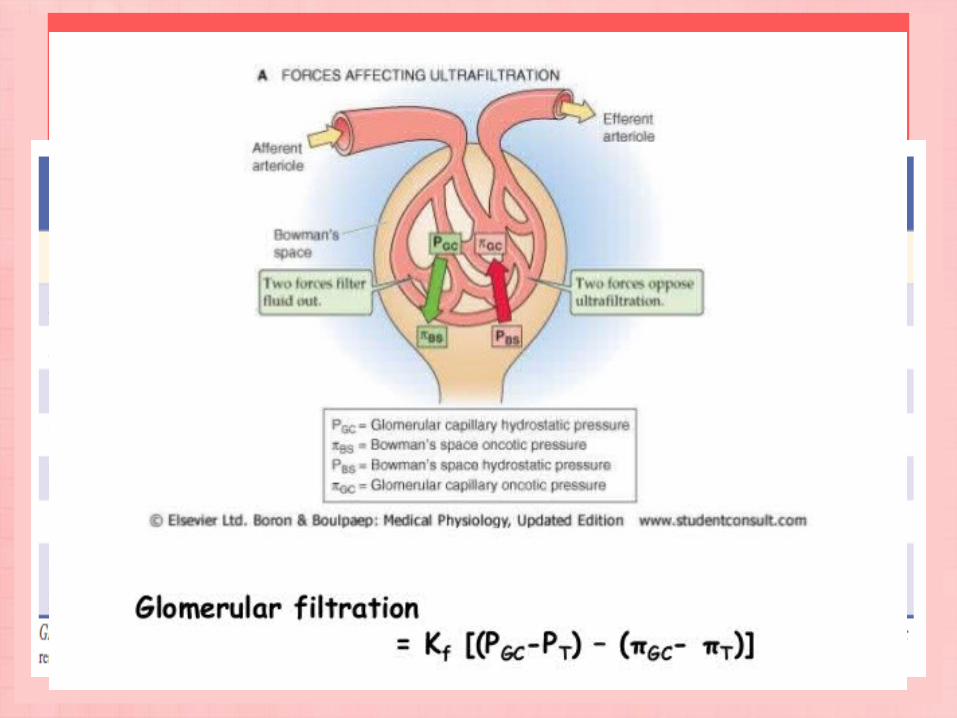
ALTERATIONS IN GLOMERULAR PHYSIOLOGY IN NEPHRON LOSS• The rise in SNGFR associated with renal mass ablation
referred to as glomerular hyperfiltration and the elevated glomerular capillary hydrostatic pressure is termed glomerular hypertension.
• Studies imply that single-kidney GFR (and therefore also the average SNGFR) increases by 30% to 40% after uninephrectomy in humans.
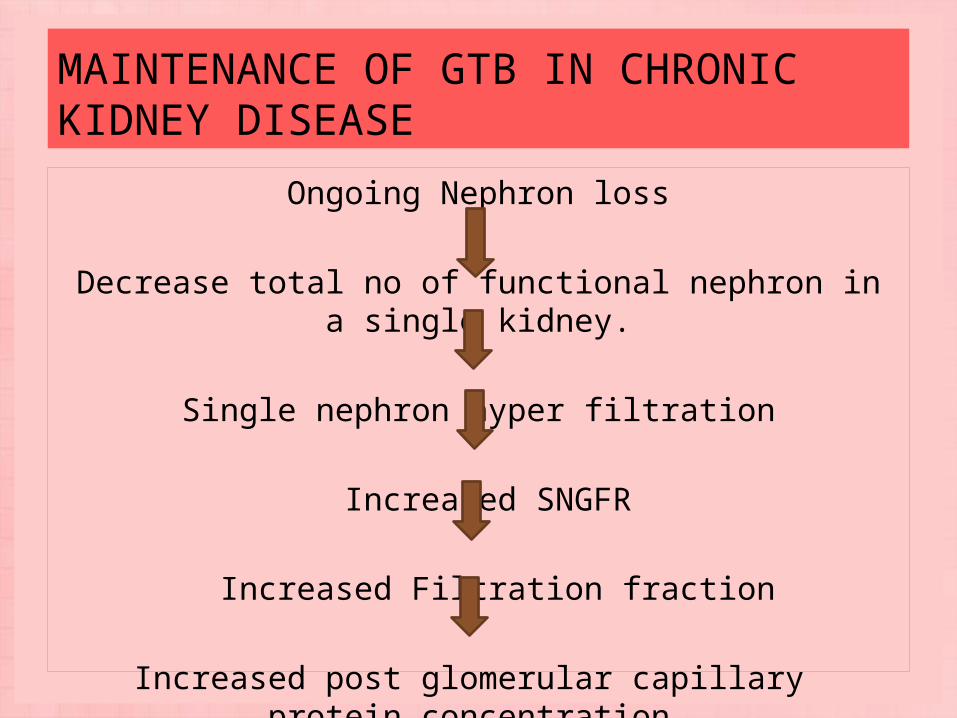
MAINTENANCE OF GTB IN CHRONIC KIDNEY DISEASE
Ongoing Nephron loss
Decrease total no of functional nephron in a single kidney.
Single nephron hyper filtration
Increased SNGFR
Increased Filtration fraction
Increased post glomerular capillary protein concentration.
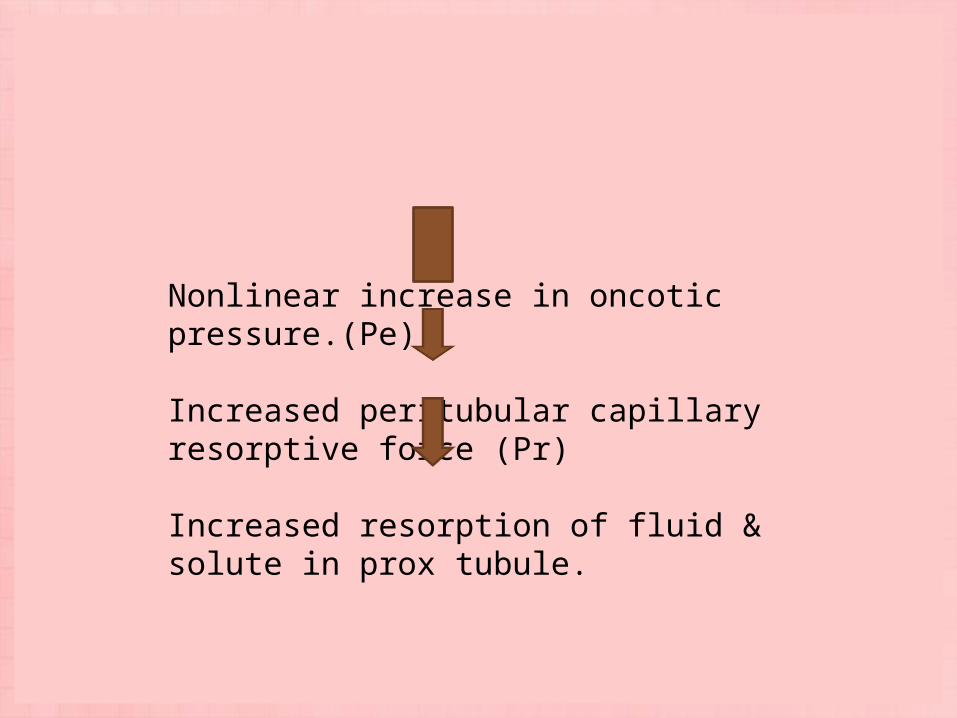
Nonlinear increase in oncotic pressure.(Pe)
Increased peritubular capillary resorptive force (Pr)
Increased resorption of fluid & solute in prox tubule.
MEDIATORS OF GLOMERULAR HEMODYNAMIC RESPONSE TO NEPHRON LOSS
Renin-Angiotensin-Aldosterone System Endothelins Natriuretic Peptides Eicosanoids Nitric Oxide Bradykinin Urotensin II
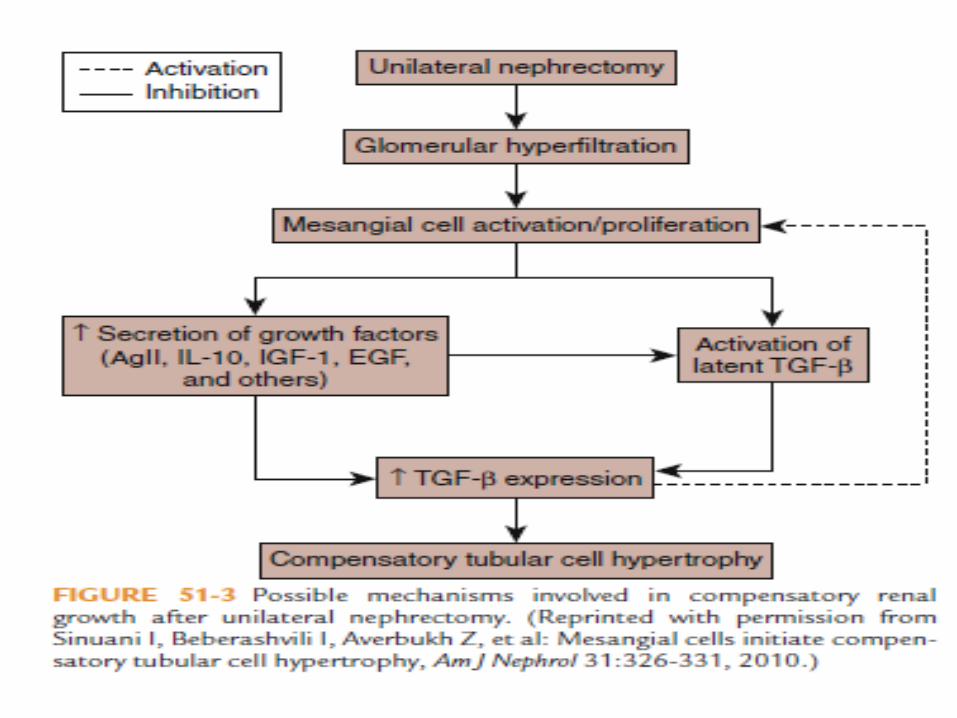
RENAL HYPERTROPHIC RESPONSES TO NEPHRON LOSS• Among the earliest responses to unilateral nephrectomy
are biochemical changes that precede cell growth.• These are-i) Increased activity of choline kinase and ornithine
decarboxylaseii) Increased ribosomal RNA, protein and poly(A)-deficient
mRNA synthesisiii) Increased DNA synthesis• Renal mass continues to rise for 1 to 2 months until a 40%
to 50% increase is achieved. The degree of compensatory growth is a function of the extent of renal ablation.
MECHANISMS OF RENAL HYPERTROPHY IN RESPONSE TO NEPHRON LOSS
• Solute load• Renotropic factors• Endocrine effects• Growth factors• Mesangial cell response• Tubule cell responses
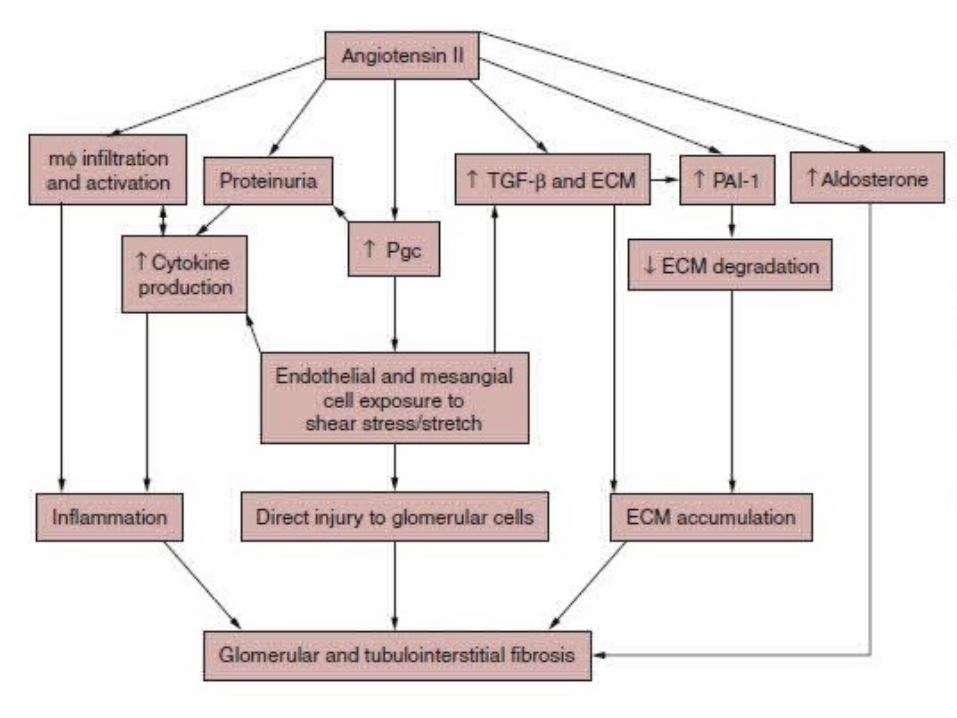
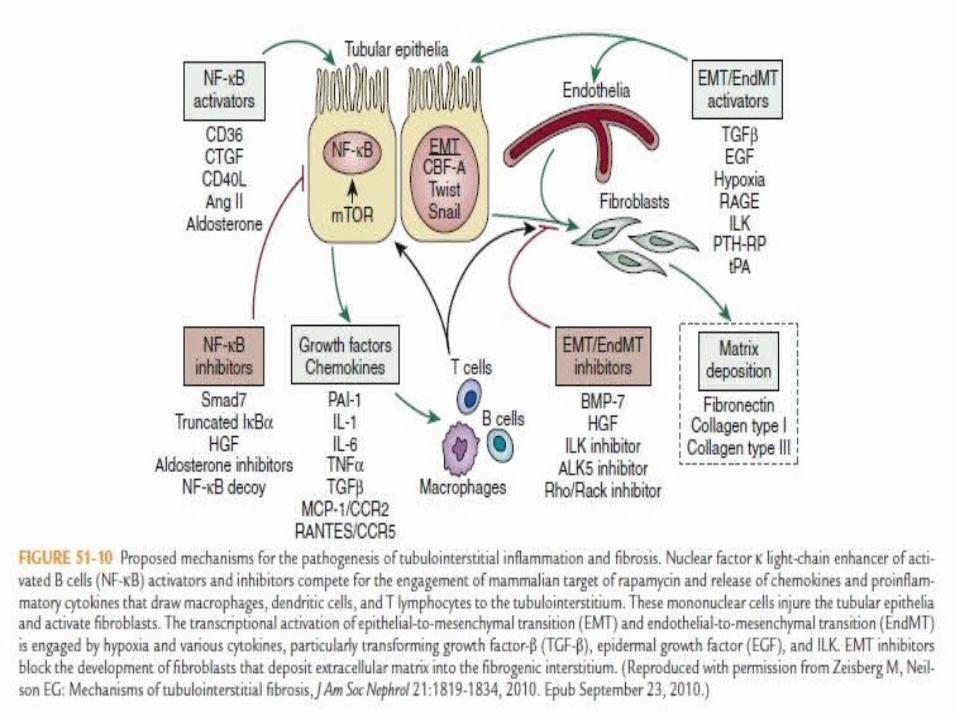
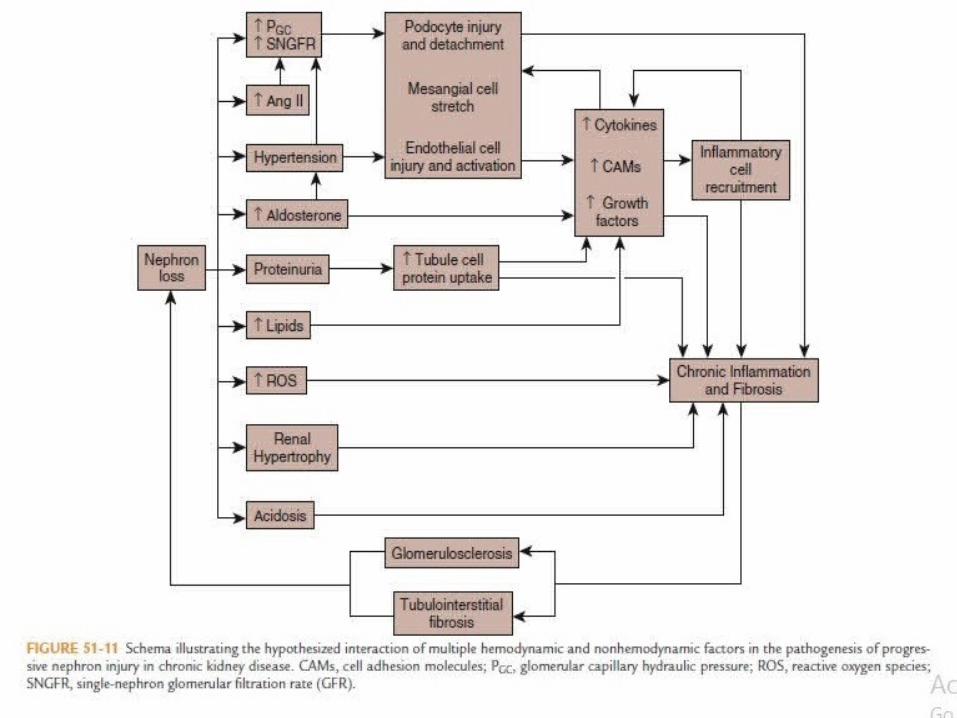
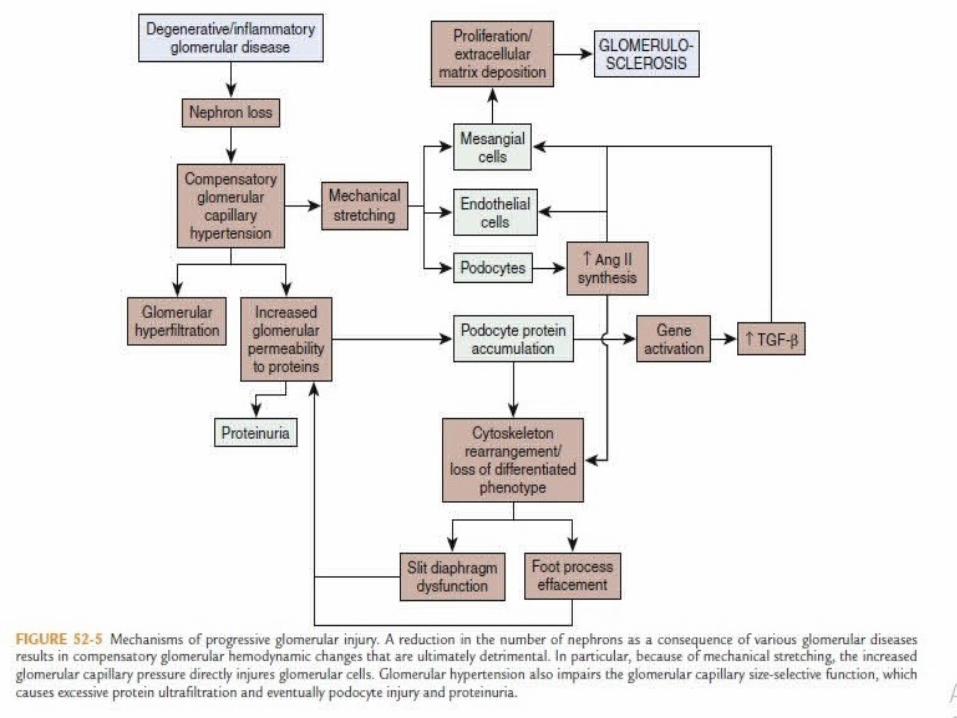
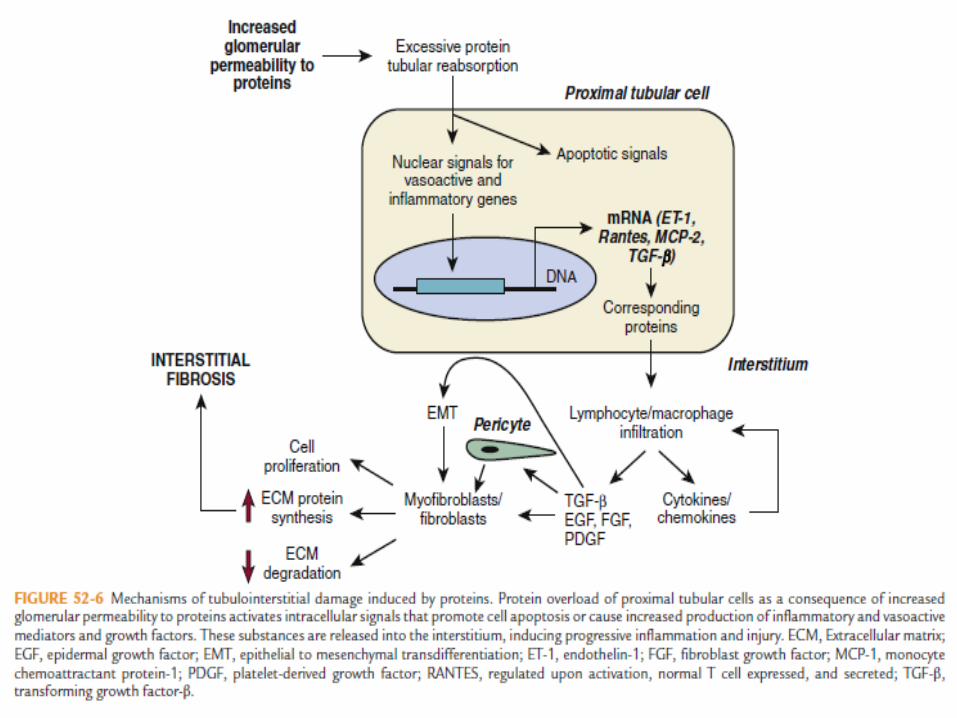
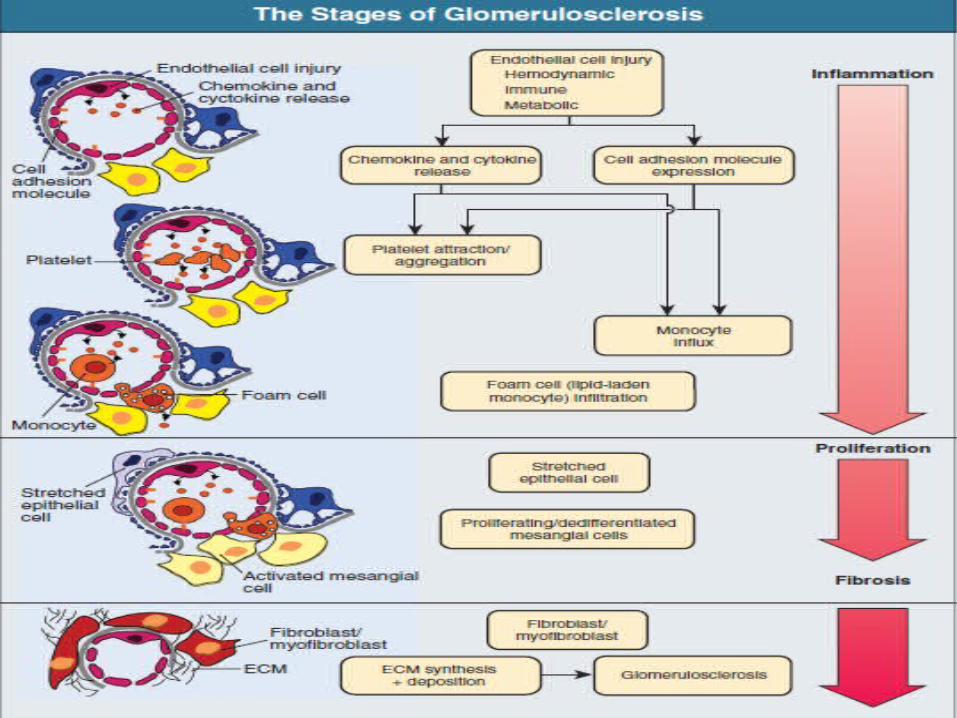
LONG TERM CONSEQUENCES OF ADAPTATION
Non hemodynamic factors:• TGF-B• Angiotensin• Aldosterone• HGF• BMP-7• Oxidative stress• Acidosis • Loss of glomerular permselectivity
Hemodynamically induced injury:
Endothelial cellsMesangial cellsPodocytesCellular infiltration
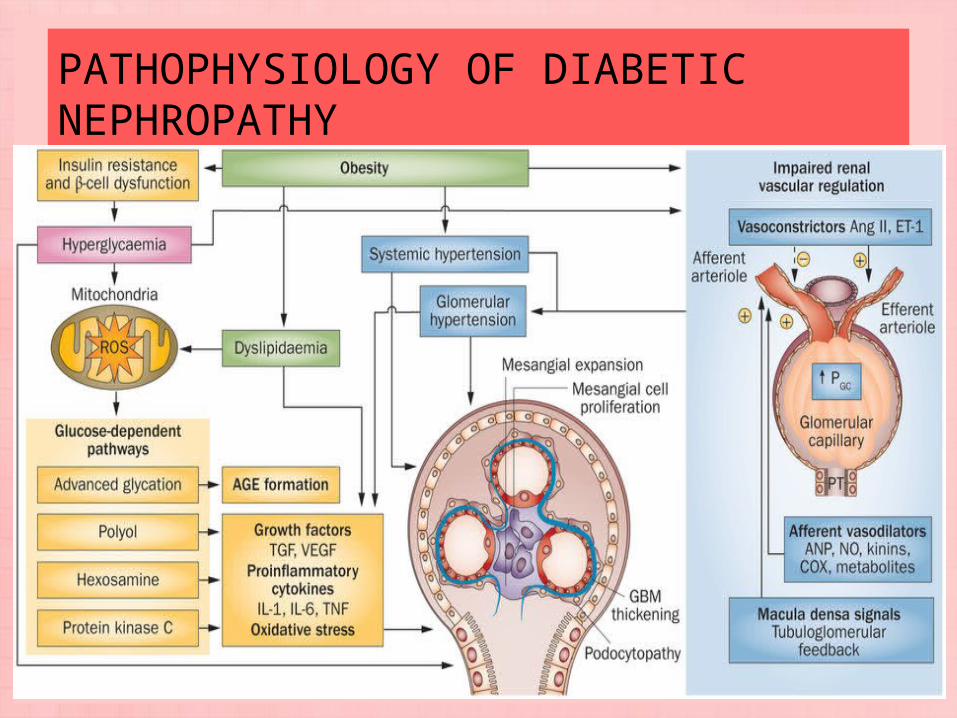
PATHOPHYSIOLOGY OF DIABETIC NEPHROPATHY
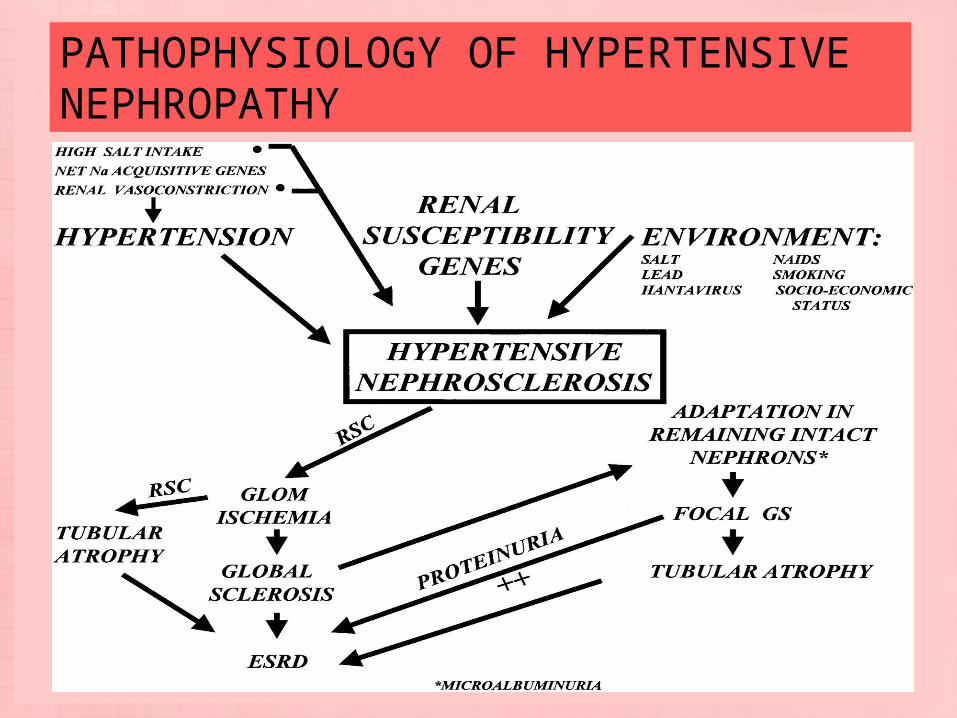
PATHOPHYSIOLOGY OF HYPERTENSIVE NEPHROPATHY
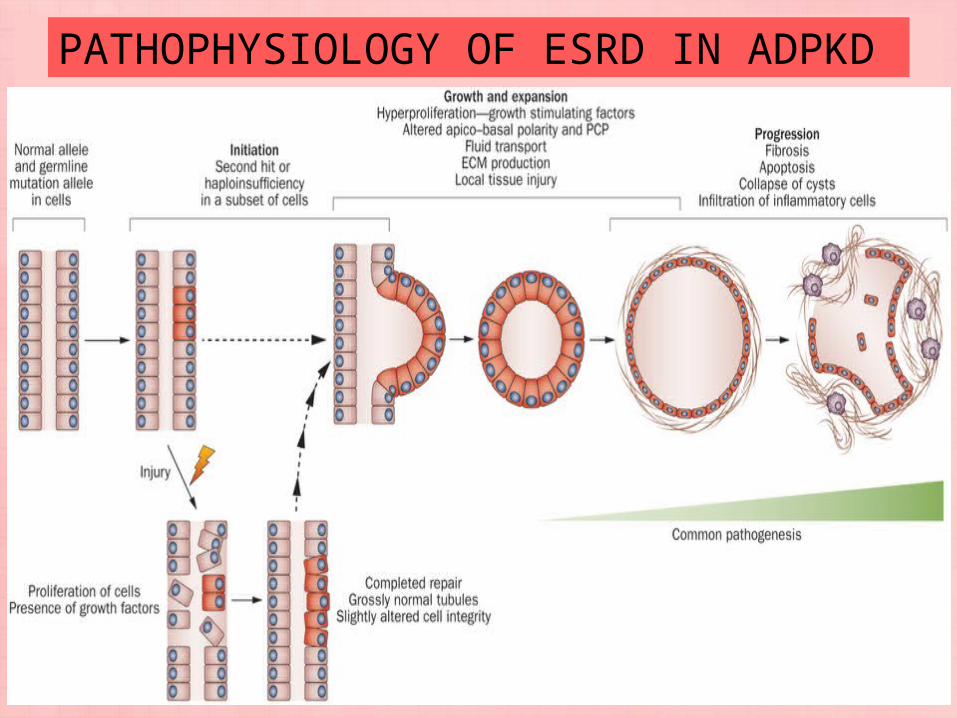
PATHOPHYSIOLOGY OF ESRD IN ADPKD
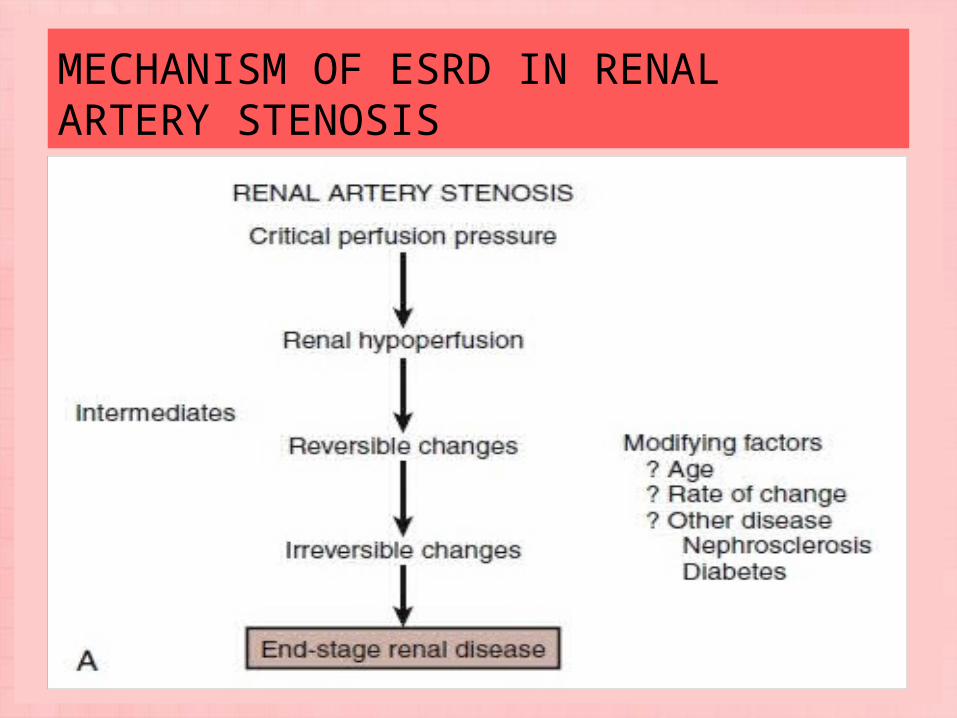
MECHANISM OF ESRD IN RENAL ARTERY STENOSIS
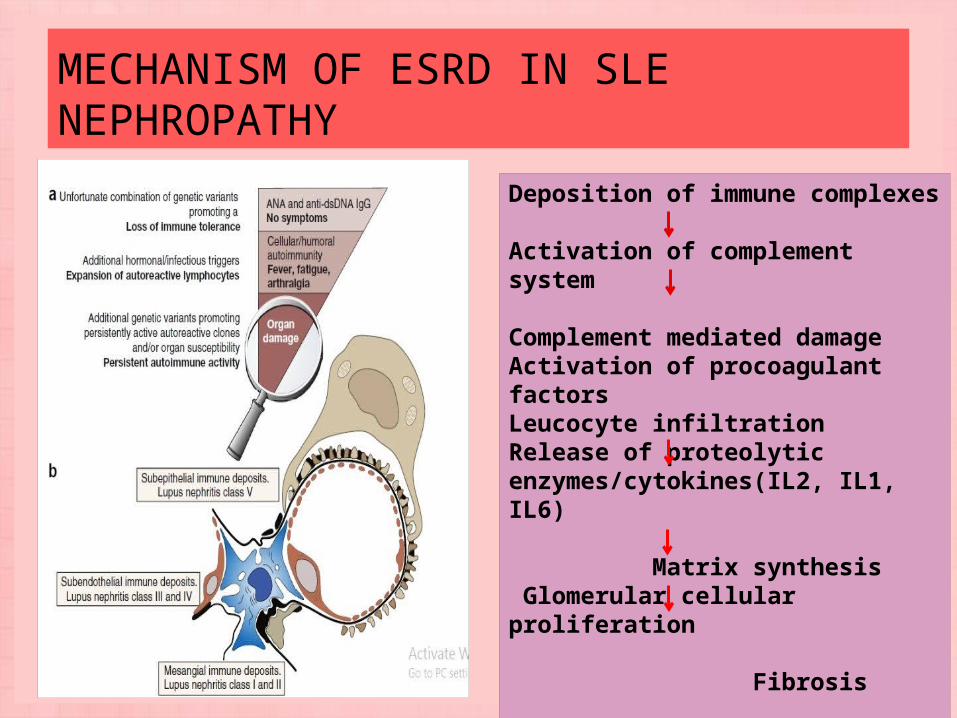
MECHANISM OF ESRD IN SLE NEPHROPATHY
Deposition of immune complexes
Activation of complement system
Complement mediated damageActivation of procoagulant factorsLeucocyte infiltrationRelease of proteolytic enzymes/cytokines(IL2, IL1, IL6)
Matrix synthesis Glomerular cellular proliferation
Fibrosis
ESRD
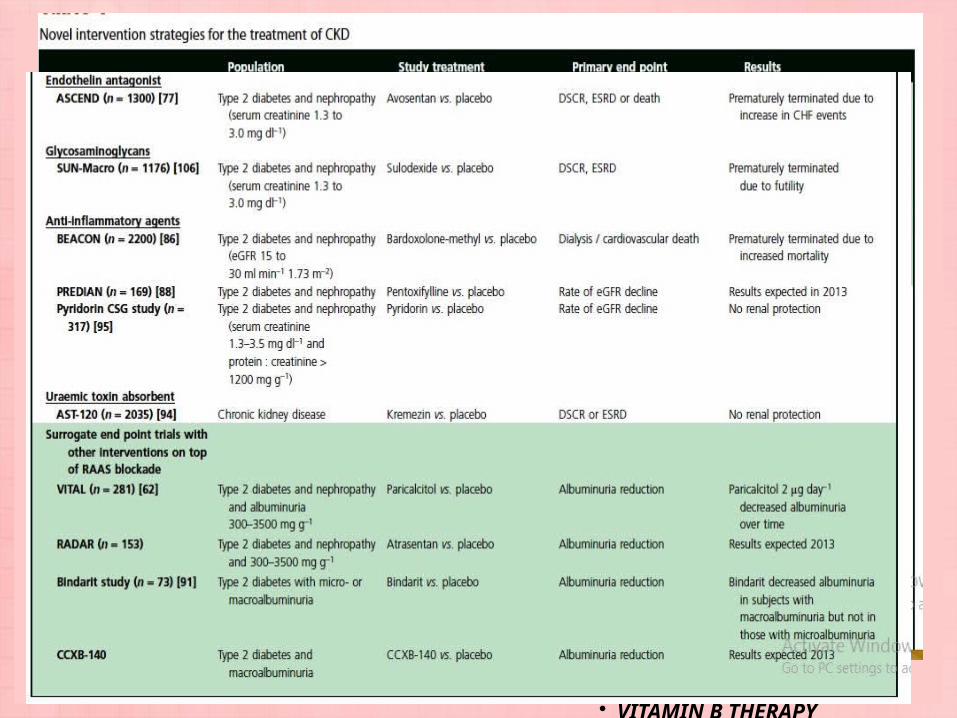
TREATMENT TARGETS- TRADITIONAL AND NOVEL
Traditional targets
• RAAS BLOCKADE• GLYCEMIC CONTROL• VITAMIN D• URIC ACID LOWERING• PHOSPHATE
LOWERING
Novel targets
• ENDOTHELIN ANTAGONISTS
• ANTI-INFLAMMATORY AGENTS
• BARDOXOLONE• PENTOXYFYLLINE• CTP-499• MONOCYTE
CHEMOATTRACTANT PROTEIN-1 INHIBITION
• URAEMIC TOXIN ABSORBANTS KREMEZIN (AST-120)
• VITAMIN B THERAPY
THANK YOU…..