paroxysmal ventricular tachycardia: astudy one -...
TRANSCRIPT
Paroxysmal Ventricular Tachycardia: A Study ofOne Hundred and Seven Cases
By CHARLEs A. ARMBRUST, JR., M.D., AND SAMUEL A. LEVINE, M.D.
A review is presented of 107 cases of paroxysmal ventricular tachycardia. In the majority it was
associated with acute coronary thrombosis or coronary sclerosis, in some with rheumatic valvulardisease, and in others with no organic heart disease. It is generally critical and demands carefulattention. Occasional cases are overlooked because only one heart sound is present for each cardiaccycle and the heart rate is misjudged to be one-half the actual rate. The outlook often is serious ifthe condition is not effectively treated. Therapy generally is successful in controlling the arrhyth-mia. The most valuable drug is quinidine. Other medications are magnesium sulfate, atropine,potassium salts, and possibly morphine.
P AROXYSMAL ventricular tachycardiais one of the less common types of par-oxysmal rapid heart action. In spite of
its rarity, prompt diagnosis and treatment aremost important because often the patient's lifeis at stake and with proper therapy the resultsmay be excellent. The arrhythmia occurs pre-dominantly in patients with serious organicheart disease and this, in addition to the effectof the rapid ventricular rate, makes it impera-tive that the attack be terminated as soon aspossible if a fatal outcome is to be averted.
Lewis1 reported the first case of ventriculartachycardia. His patient was a seaman who hadrepeated premature ventricular contractions oc-curring singly and in runs of as many as 11beats. Shortly after Lewis' publication in 1909,reports2-4 of isolated instances of this arrhyth-mia appeared which were followed by reportsof larger series and more complete reviews. -8Lewis9 produced ventricular tachycardia indogs by ligating the coronary arteries andRobinson and Herrmann"O called attention tothe relationship of paroxysmal ventriculartachycardia to coronary occlusion in man.Scott,1" in 1921, was successful in controllingthis arrhythmia by the use of quinidine admin-istered orally. There was 1:1 retrograde con-duction to the auricles and no evidence oforganic heart disease. The present study of 107cases is reported with the hope of clarifyingsome of the problems of diagnosis, prognosis,and treatment encountered in patients with thisdisorder.
From the Medical Clinic of the Peter Bent Brig-ham Hospital and the Department of Medicine,Harvard Medical School, Boston, M1ass.
IMATERIAL
All cases of paroxysmal ventricular tachycardiaoccurring in the Peter Bent Brigham Hospital andthe private practice of one of us (S. A. L.) from 1915to 1948, inclusive, have been studied. Sixteen of
NaCASES
40
30
20
10
0-9 10-49 20-29 30-39 40-49 50-59 60-69 70-79 80-8s 90-99
AGE IN DECADES
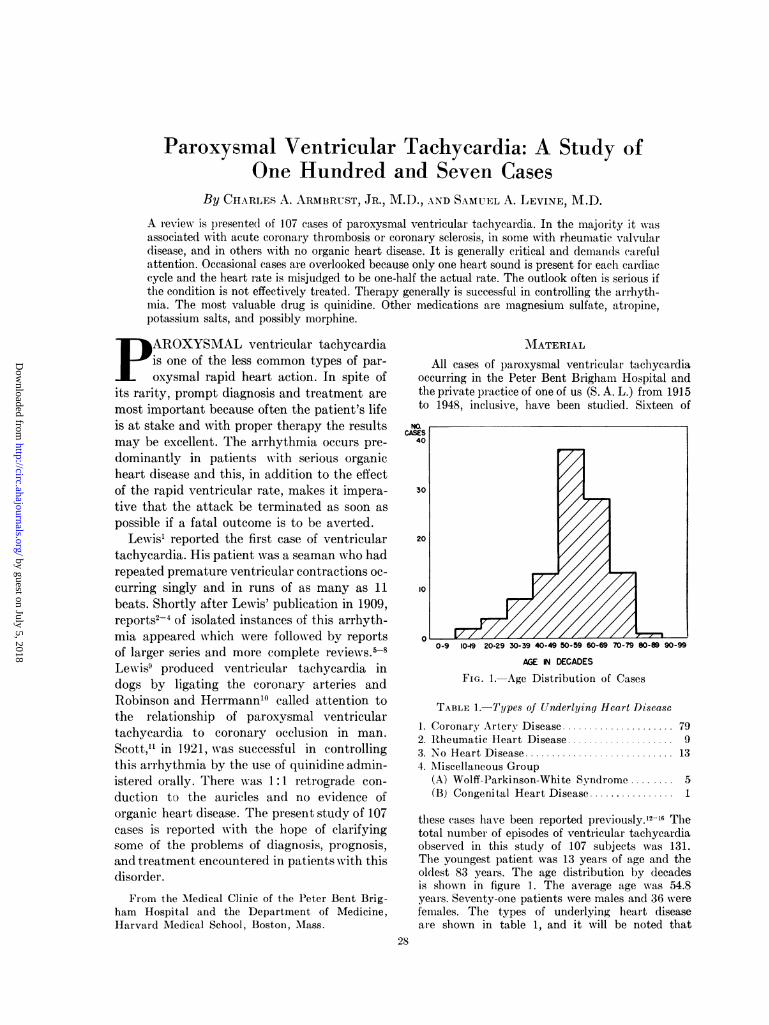
FIG. 1.-Age Distribution of Cases
TABLE 1.-Types of Underlying Heart Disease
1. Coronary Artery Disease ..................... 792. Rheumatic Heart Disease .................... 93.NoH eart D isease 134. Miscellaneous Group
(A) Wolff-Parkinson-White Syndrome ........ 5(B) Congenital Heart Disease ................ 1
these cases have been reported previously."2-16 Thetotal number of episodes of ventricular tachycardiaobserved in this study of 107 subjects was 131.The youngest patient was 13 years of age and theoldest 83 years. The age distribution by decadesis shown in figure 1. The average age was 54.8years. Seventy-one patients were males and 36 werefemales. The types of underlying heart diseaseare shown in table 1, and it will be noted that
28
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

CHARLES A. ARMBRUST, JR. AND SAMUEL A. LEVINE
coronary artery disease was present in 74 percent of the patients. The duration of the attacksvaried from a few seconds to twenty-three days.Eighty-two patients had persistent attacks (hoursto days) and 25 had intermittent attacks (secondsto a few minutes). The ventricular rate during theepisodes varied from 138 to 292 with one exception;in one patient the rate was 115.
CLINICAL DIAGNOSIS
The bedside findings which suggest the clini-cal diagnosis of paroxysmal ventricular tachy-cardia have been described by Levine17',9and Strong and Levine.18 These consist of achanging intensity of the first heart sound at theapex, a slight irregularity of the ventricularcycle length, and the failure of vagal stimula-tion to produce any effect on the tachycardia.A changing intensity of the first sound was
noted in forty-three episodes. This sign will bedetected only on careful auscultation and isnot present in patients who have concomitantauricular fibrillation or in those in whom thereis 1:1 retrograde conduction. In the rare in-stance in which 2:1 retrograde conduction tothe auricles takes place one might expect tofind alternation in the intensity of the firstsound. The mechanism of production of thechanging first sound is thought to be dependenton the changing relationship between auricularand ventricular contraction, similar to thatwhich occurs in conjunction with completeheartblock.19 Excluding the patients with auric-ular fibrillation, a changing intensity of thefirst sound was noted in approximately 50 percent of the patients in this series.
In the common type of paroxysmal auricu-lar tachycardia the cycle length is perfectlyconstant, whereas in ventricular tachycardiaslight but detectable irregularities in the cyclelength may be observed in an appreciable num-ber of instances. The slight irregularities inrhythm in ventricular tachycardia can easilybe overlooked unless auscultation is carried outcarefully. Cooke and White7 on the other handfound thirteen of fifteen tracings of definite andprolonged paroxysms of ventricular tachycar-dia to be perfectly regular. Cooke and White7also found that irregular rhythm was mostlikely to occur during short paroxysms and inpatients with auricular fibrillation. Williams
and Ellis8 found only 4 of 24 patients with thepersistent type of tachycardia to have an ob-vious irregularity of the rhythm. In the 107episodes of the persistent type of tachycardiain this series, in 32 per cent the rhythm wasslightly irregular, while in 76 per cent of theintermittent type a similar type of slight ir-regularity was manifest. In considering theslight irregularity that is seen in paroxysmalventricular tachycardia it must be clear thatthe actual heart rate can be quite constantover long periods of time. It is the length ofcontiguous cycles that may change. The dif-ference may not be more than 0.03 secondthough occasionally it is much greater and maynot occur but once in many cycles. The ear isable to appreciate these slight variations incycle length. In contrast, the contiguous cyclesin the common type of paroxysmal auriculartachycardia rarely vary more than 0.01 secondin length.Paroxysmal ventricular tachycardia does not
respond to vagal stimulation. This finding ishelpful in the differentiation of ventricular fromparoxysmal auricular tachycardia, auricularflutter, and sinus tachycardia.
Gallarvardin20 described changes in the jug-ular pulse wave in patients with ventriculartachycardia. Further observations of the jugu-lar pulse during the arrhythmia have been re-ported by Prinzmetal and Kelley.2' In ventric-ular tachycardia the auricular rate is generallyslower than the ventricular rate and the pulsa-tions of the auricles at this slower rate may bevisible in the jugular vein. In addition, occa-sional prominent jugular waves will appear dur-ing cycles when the auricles are contractingwhile the ventricles are in systole. Such find-ings may be particularly helpful in those pa-tients in whom P waves are not visible in theelectrocardiogram. The abnormal jugular pul-sations will be absent in subjects in whom thereis no change in the intensity of the first heartsound, that is, in those with auricular fibrilla-tion and 1:1 retrograde conduction.There is one additional unusual auscultatory
phenomenon that merits discussion, particu-larly since it has not been hitherto described.There were three instances in this series inwhich only one heart sound could be heard
29
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

PAROXYSMAL VENTRICULAR TACHYCARDIA
with each cycle. In 2 patients this resulted inthe heart rate being misinterpreted by someobservers as being one-half the actual rate. Inone of these patients, the sounds alternated inintensity so that they closely resembled thenormal sounds. It was difficult at the bedsideto tell whether the rate was 115awith two soundsto a beat or 230 with only one sound. This couldnot be determined from the radial pulse sincethe patient was pulseless and the blood pres-sure was not obtainable. The electrocardiogramquickly revealed the fact that the ventricleswere beating at a rate of 230. It is of interestthat in this case two physicians who had beenseeing the patient for some hours had over-looked the tachycardia and thought the heartrate was "about one hundred." Such expe-riences must be more frequent than has beenrealized as we have seen other instances ofparoxysmal rapid heart action in which onlyone heart sound could be heard with eachcardiac cycle.
In summary, one may state that there arebedside methods available which will enablethe physician to suspect the diagnosis of par-oxysmal ventricular tachycardia in most casesand even to make a fairly definite diagnosis inmany instances without the aid of the elec-trocardiograph.
ELECTROCARDIOGRAPHIC DIAGNOSIS
The criteria for the electrocardiographic diag-nosis of ventricular tachycardia were first pro-posed by Robinson and Herrmann.11 They em-phasized three features. The first is the detectionof auricular complexes (P waves) occurring in-dependently and at a slower rate than the ven-tricular rate. The second is the presence ofventricular complexes that are abnormal inform and different from those observed in thesame patient when the paroxysm is not present.The third is the finding of isolated ectopic ven-tricular complexes before or after a paroxysmthat have the same form as the ventricularcomplex during the paroxysm.The presence of P waves may be difficult to
detect in the standard limb leads and thereforespecial auricular leads may be of value in theirdemonstration. If the condition of the patient
is not too serious, esophageal leads taken in theauricular region may be helpful.The abnormal ventricular complexes in them-
selves are not sufficient to make the diagnosis,as there may be aberration of the ventricularcomplexes due to the rapid rate alone.'0 Alsoauricular tachycardia, auricular fibrillation, au-ricular flutter, and nodal tachycardia with aber-rant ventricular conduction or with permanentbundle branch block may simulate ventriculartachycardia.22 The concomitant presence of au-ricular fibrillation and paroxysmal ventriculartachycardia which occurred in 20 of the casesadds further difficulties in diagnosis.Cooke and White7 noted that ectopic ven-
tricular beats exactly similar in type to thoseof the paroxysm may be very difficult to findand that complexes almost alike are adequateto aid in the diagnosis. It is of interest thatthese authors have reported other cases inwhich auricular premature beats preceded andfollowed the paroxysms of ventricular tachy-cardia. They have also observed that the oc-currence of paroxysms of abnormal ventricularcomplexes, regular and more rapid than theprevious rate during auricular fibrillation, isdiagnositic of ventricular tachycardia.
PATIENTS WITH CORONARY ARTERY DISEASE
In our series, in 79 cases (74 per cent) coro-nary artery disease was the cause of the under-lying heart disease. The diagnosis of coronaryartery disease was restricted to those patientswho had angina pectoris or myocardial infarc-tion, either acute or old. A number of thepatients in this group had, in addition, hyper-tensive cardiovascular disease, but no distinc-tion has been made here between the hyper-tensive and nonhypertensive. In 44 patients theattacks occurred following an acute myocardialinfarction. The youngest patient was 31 yearsof age and the oldest 83 years. There were 55men and 24 women. The attacks of tachycardiawere of two types, persistent or intermittent.The latter were short paroxysms of tachycardialasting seconds or minutes which ceased spon-taneously or were controlled readily in mostcases by therapy. There were 18 patients of thegroup with coronary artery disease who hadintermittent paroxysms. The persistent type of
30o
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

CHARLES A. ARMBRUST, JR. AND SAMUEL A. LEVINE
attack, of which there were seventy-sixinstances presents the more difficult therapeu-tic problem. The episodes, as can be seen infigure 2, tend to occur most frequently with theonset of acute myocardial infarction or duringthe first two weeks after the acute infarction.The attacks of tachycardia were regarded asoccurring with the onset of an acute myocardialinfarction when they were noted during the firstsix hours after the first evidence of coronarypain. It is not possible to determine how manysubjects if any, developed the rapid heart ratedirectly with or a few seconds after the first
to CS
0-1 1-4 5-9 1044 IS-I9 2024 25.2930-D 4 35-39 40.44
DAYS
FIG. 2.-Onset of Paroxysmal Ventricular Tachy-cardia after Acute Infarction.
evidence of heart pain. If the attack of tachy-cardia occurs at the same time as the acuteinfarction there may be some difficulty in eitherconfirming or excluding the diagnosis of theunderlying infarct. It is quite well known thatparoxysmal rapid heart action of any type can
result in chest pain, fever, leukocytosis, fall inblood pressure, and even subsequent electro-cardiographic changes without any myocardialinfarction.23'24 An added difficulty is that theshock state resulting from the tachycardia maybe followed by a myocardial infarction, such as
occurs in association with shock following hem-orrhage or surgical operation.
Patients may have single or multiple attacksof ventricular tachycardia. The control of mul-tiple attacks depends on the use of varyingdoses of quinidine prophylactically. There were
10 patients with coronary artery disease whohad multiple attacks of ventricular tachycardiawhile under observation and 17 additional pa-tients who gave a history of multiple episodes.The attacks in 3 of these patients were particu-larly interesting.
One patient had his first attack of paroxysmalventricular tachycardia on the twenty-sixth dayafter an acute myocardial infarction. In the ensuingsixteen days he had twelve recurrent episodes.Following each attack reversion to normal rhythmoccurred after a single dose of quinidine sulfate,either 0.6 Gm. given intravenously or 1.0 Gm.orally. This patient then had an uneventful recoveryand is alive and working at the present time,two and one-half years following the last episode.The second patient, a 55 year old Negro, had an
acute myocardial infarction complicated by ven-tricular tachycardia in 1939. From 1939 to March1949 he had 111 episodes of paroxysmal rapidheart action. In five observed attacks the arrhyth-mia was identified as ventricular tachycardia andeach episode was arrested by quinidine therapy.It is reasonable, therefore, to assume that all theother attacks were of similar origin. These attackshave recurred in spite of the prophylactic use ofquinidine and potassium salts but the patient hascontinued his work as a janitor.The third patient, a 58 year old white man, had
an acute myocardial infarction in 1943 complicatedby ventricular tachycardia. From December 1943to the present time he has been treated in thehospital for eight episodes of ventricular tachy-cardia and has controlled many attacks at homeby taking quinidine orally. He is working at thepresent time.
These 3 cases are exceptional but they bringout the fact that a patient with serious under-lying organic heart disease may have multipleattacks of ventricular tachycardia and stillcarry on relatively normal activity for manyyears. They also indicate that repeated attacksof ventricular tachycardia may occur in a pa-tient who once had a myocardial infarction,purely as a neurogenic upset without any addi-tional injury to the coronary arteries or theheart muscle. In that sense the attack thenbehaves as paroxysmal auricular tachycardiadoes in an otherwise healthy individual.The duration of the attacks varied from a
few seconds to twenty-four days. There wereseventeen instances in which the attack lastedone to five hours; eleven, six to twelve hours;nine, twelve to twenty-four hours; eighteen, one
31
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

PAROXYSMAL VENTRICULAR TACHYCARDIA
to five days; and fourteen, five to twenty-fourdays. The longest case on record persisted forseventy-one days while the patient was underobservation in the hospital and a probable sixadditional days prior to admission to the hos-pital.25 The patient expired with uncontrolledventricular tachycardia. The duration of theattack is largely dependent on the promptnesswith which the diagnosis is made and effectivetherapy instituted.The presence of auricular fibrillation during
ventricular tachycardia is rather difficult todetermine with accuracy. It was assumed to bepresent if found directly after the ventriculartachycardia disappeared. Accepting this as-sumption, auricular fibrillation was present in14 patients of the coronary group. When theventricular tachycardia was effectively treatedwith quinidine, the concomitant auricular fibril-lation did not generally revert to normal sinusrhythm and even resisted reversion on largedoses of quinidine.The production of -ventricular tachycardia by
the use of quinidine has been previously re-pvrted8'6, 27 and was observed in 2 patients inthis group. Both had auricular fibrillation andhad received large doses of digitalis in an un-successful effort to slow the ventricular rate.Quinidine was administered and both patientspromptly developed paroxysms of ventriculartachycardia which ceased when the quinidinewas discontinued.
PATIEINTS WITH RHEUMATIC1 HEART DISEASE
There were 9 patients (8.4 per cent) in ourseries who had rheumatic valvular disease. Thiswas present in 15 per cent of the subjects ofone reported series28 and 3 per cent of another.8The age of our parents with rheumatic valvulardisease ranged from 21 to 62 years; 8 were over40 years of age. Seven had persistent attacks oftachycardia and 2 intermittent attacks. Allthe patients with rheumatic valvular diseasewere in severe congestive failure before theattacks of ventricular tachycardia occurred. Onepatient was in extremis. Five had coexistentauricular fibrillation. Digitalis had been givento 8 prior to the onset of the tachycardia. In4 of these 8 the doses were in all likelihood toosmall to have produced any toxic effects but
in the other 4 one might readily suspect thatdigitalis was in some way responsible for thetachycardia.
SUBJECTS WITH NORMAL HEARTS
Thirteen patients (12 per cent) had no evi-dence of organic heart disease. In other reportedseries, 17 per cent,5 14 per cent, and 10 percent-8 showed no evidence of organic heartdisease. The youngest in the present series was20 years of age and the oldest 53 years. Five hadintermittent and 8 persistent attacks. Theintermittent attacks were short paroxysms oftachycardia, with the patient usually complain-ing of palpitation and occasionally of dyspnea.Some of these episodes occurred With greatfrequency and were so distressing that medicaladvice was sought. These attacks were pre-cipitated by exercise, emotion, and smoking.In the majority of instances the episodes wereof no great significance.
In this group there were 4 patients with per-sistent tachycardia in whom the clinical fea-tures are worthy of comment.
A 20 year old medical student had had recurrentattacks of ventricular tachycardia bleginning in hismiddle teens. All the attacks were related directlyto exercise. During eight months of 1945 lhe hadeleven episodes of tachycardia, all of several hours'duration. These either ceased spontaneously or re-version to normal rhythm was effected by theoral administration of quinidine.A 23 year old dental student had recurrent
attacks of palpitation and dyspnea with ventriculartachycardia beginning at the age of 13 years. Thispatient had from one to nine paroxysms a month,varying in duration from several minutes to thirteenhours. The longest period during which lhe wasfree from attacks was two years.
The third patient was a 34 year old woman,whose first attack of ventricular tachycardia lastedtwenty days and was refractory to large oral dosesof quinidine. Her condition was desperate. Reversionto normal rhythm occurred after a large oral doseof quinidine followed by 1 mg. of atropine. Follow-ing this the patient had two more short episodeswhile receiving prophylactic quinidine, 0.2 Gm.four times a day. She then had no more attacksuntil nine and ten years later, when she had twoepisodes. At the present time she is alive andfairly well.The fourth patient, a 42 year old man, developed
auricular fibrillation, paroxysmal ventricular tachy-cardia, and congestive failure. He had at least
32
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

CHARLES A. ARMBRUST, JR. AND SAMUEL A. LEVINE
three episodes of ventricular tachycardia duringa six weeks' stay in the hospital. Following recovery,he has been working every day; he is symptomlessand has no findings suggestive of heart diseaseat the present time, three years later.
It can be seen that patients without anyevidence of organic heart disease may haveepisodes of ventricular tachycardia and in somecases present the same difficult therapeuticproblems and dangers as those with underlyingorganic heart disease. However, after reversionto normal rhythm the prognosis is excellent.
MISCELLANEOuTS GROUP
Five patients with the Wolff-Parkinson-White syndrome, with peculiar ventricular com-plexes, have been included in this study. Onordinary inspection the electrocardiographicpattern resembled that of paroxysmal ventric-ular tachycardia. Three of these cases havepreviously been reported." The interpretationof the exact mechanism can be disputed. It iswell known that the customary disturbances inrhythm associated with the Wolff-Parkinson-White syndrome are auricular in type, usuallyparoxysmal auricular tachycardia or fibrilla-tion. Therefore, it is quite likely that these 5cases showing rapid broad ventricular com-plexes were instances of conduction throughthe anomalous bundle rather than cases ofparoxysmal ventricular tachycardia.29 The onlymethod of identifying a true ventricular tachy-cardia, in the presence of the Wolff-Parkinson-White syndrome, would be to detect auricularcomplexes coming regularly, independently, andmore slowly than the ventricular beats. Thishas not as yet been demonstrated.
Despite the difficulty in interpretation, thesefive cases are included because they respondedin general just as the more classic instances ofventricular tachycardia. None of these patientsshowed any other evidence of organic heartdisease. As a group they were young patients,the ages being 13, 30, 36, 37, and 52 years. Twoof these 5 died suddenly, the other 3 remainingquite well. One young boy presented a picturethat was confused with and misdiagnosed as anacute myocardial infarction. In one case thetachycardia stopped spontaneously and in an-other reversion took place after a moderate
amount of digitalis was given. However, therole played by digitalis in producing the rever-sion is doubtful. In the other 3, reversionresulted from quinidine administration. In onecase there was a gradual but rapid slowing ofthe ventricular rate from around 300, beforethe normal rhythm was established. This iswhat one might expect from quinidine therapyif the abnormal mechanism was ventricular inorigin, for if auricular fibrillation was presentit is much more customary to observe an ac-celeration of the ventricular rate following quin-idine, before regularization occurs, than a de-celeration.The important inference to be drawn from
these experiences is that although the Wolff-Parkinson-White syndrome with paroxysmalarrhythmias may be unassociated with anyother detectable organic heart disease, suddendeath is not a very rare eventuality.The last patient in this group was a young
man, 30 years of age, who had Eisemenger'scomplex. The diagnosis was confirmed by in-tracardiac catheterization studies. His primarycomplaints were palpitation and attacks of syn-cope. When the spells of unconsciousness be-came frequent, he had to discontinue his workwhich otherwise he would have been able toperform. It was found that his difficulty wasdue to ventricular extrasystoles, which occa-sionally developed into short runs of paroxysmalventricular tachycardia and were followed bysyncopal attacks. He seemed to be helped by abilateral upper dorsal sympathectomy and qui-nidine therapy.
PART PLAYED BY DIGITALIS
Forty-seven patients received digitalis invarying amounts prior to the onset of ventric-ular tachycardia. Twenty-six were on whatwas considered maintenance doses or less atthe time the tachycardia developed. In thesepatients it was doubtful if digitalis played anypart in the precipitation of the episodes. Thir-teen received what was considered as probablyexcessive doses. In these digitalis may havebeen important in the production of the parox-ysms. In 6 there was definite evidence ofdigitalis intoxication, such as nausea, vomiting,premature ventricular contractions, and bigem-
33
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

PAROXYSMAL VENTRICULAR TACHYCARDIA
inal and trigeminal rhythm. In these casesdigitalis may have precipitated the arrhyth-mia but conclusive evidence of this is notavailable. Two patients with definite digitalisintoxication had bidirectional ventricular tachy-cardia and one with probable intoxication hadalternation of the ventricular complexes.
Digitalis has long been considered as oneof the more common precipitating factors inthe development of ventricular tachycardia.Lundy and McLellan6 in their review in 1934stated that digitalis was responsible for 100per cent of the cases in which alternating bi-directional complexes were observed. Marvin30reported 5 cases of ventricular tachycardia withalternation of the complexes and postulatedthat factors other than digitalis alone mustplay a part as 3 patients had no headache,nausea, or vomiting and only one had yellowvision. Scherf and Kisch3' in a study of 18 pa-tients showing bidirectional ventricular tachy-cardia found that all but 4 were receivingdigitalis at the time the tachycardia developed.They also noted that there was no definite rela-tionship between the amount of digitalis andthe development of ventricular tachycardia.They believed that there must be in addition tothe digitalis factor an injured myocardium.
Digitalis cannot be looked upon as an im-portant or frequent cause of ventriculartachycardia when it is appreciated that inthis very clinic from which the cases are beinganalyzed, thousands of different individualshave received full doses of digitalis and yetonly a very few have ever showed this arrhyth-mia. In one patient with valvular heartdisease who had had previous attacks ofparoxysmal ventricular tachycardia an attackappeared for the first time directly after afull dose of digitalis had been given. Therewas little doubt about the relationship be-tween cause and effect in this instance. Inanother patient it was clearly establishedthat the ventricular rate during the ventric-ular tachycardia accelerated under digitalistherapy. It is therefore very difficult toevaluate, with any degree of exactness, whatpart digitalis had in evoking the attacks oftachycardia, though we are of the opinion
that it does play a role in a small number ofcases.
CLINICAL FEATURESThe clinical features that characterize the
episodes of ventricular tachycardia have beenstudied in seventy-seven attacks in whichadequate data were available. The onset ofparoxysmal ventricular tachycardia may beentirely unnoticed by the patients. In suchcases the diagnosis is made only when theexamining physician or nurse notices that thepatient has a rapid heart rate, and the phy-sician investigates the rapid rhythm morethoroughly. There are, however, certain clinicalfeatures that make one suspect that the patientis having a bout of paroxysmal rapid heartaction. The sudden onset of palpitation andslight to moderate dyspnea were the mostcommon subjective symptoms noticed by thepatients in this study. Dizziness and syncopalattacks with loss of consciousness may usherin the episodes. These symptoms may occurregardless of whether or not organic heartdisease is present. Cerebral manifestationssuch as these were present in 13 patientsand have been described previously as occur-ring in association with paroxysmal tachy-cardia.32 There is another type of syncopethat may occur, for some patients with com-plete heart block may have a short paroxysmof ventricular tachycardia or fibrillation whichis then followed by ventricular arrest of suffi-cient length to cause unconsciousness andconvulsions. Such a mechanism producingAdams-Stokes episodes in persons with com-plete heart block is well known.26' 33-3 Therewere 5 patients in this series who exhibitedthese findings. One patient, a 46 year oldwoman, had had complete heart block withAdam-Stokes attacks for a period of threeyears, the latter always being preceded byparoxysms of ventricular tachycardia or ven-tricular fibrillation. The patient failed to re-spond to any type of therapy and finallyexpired suddenly during an episode. Atpostmortem examination the heart weighed360 grams, there was no evidence of coronaryatherosclerosis, the interventricular septumshowed no abnormalities, nor were there
34
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from
CHARLES A. ARMBRUST. JR. AND SAMUEL A. LEVINE3
any other structural abnormalities of theheart. Therefore, judged by postmortem ex-amination, this patient had a normal heart.
Eighteen patients noticed substernal andprecordial pain with the onset of the attackof tachycardia. The pain may be identicalwith that of angina pectoris23 or of an acutemyocardial infarction. In patients who havehad previous episodes of angina pectoris ora previous myocardial infarction the painwas usually not as severe as that due to theangina or infarction. The majority of patientsdescribed the pain as a dull ache, a heavyfeeling, or a choking sensation.
In any patient, especially in one with anacute myocardial infarction, in whom suddencollapse occurs, ventricular tachycardia shouldbe suspected. With the onset of the rapidrate there may be a marked fall in bloodpressure; the skin becomes cold and clammyand profuse sweating occurs. The conditionchanges in a matter of minutes from satis-factory to critical. There were 44 patientsin shock during the episode of ventriculartachycardia. The shock varied from mild,in which the systolic blood pressure wasslightly less than 100 mm., to profound inwhich the blood pressure was unobtainable.In sixty-two instances congestive heart failurewas present. The congestive failure wasmanifested by moist rales at the lung basesor throughout the chest and varying degreesof right-sided failure. These variations de-pended on the type of underlying heart diseaseand the duration of the rapid rate.
It may be said in summary that a patientwith ventricular tachycardia may be asympto-matic during the attack or may have syncopalepisodes, dizziness, or sudden collapse withthe onset or during the paroxysm. Chestpain similar in all respects to that of anginapectoris may occur.
PROGNOSIS
Strauss5 reported that in 50 patients withventricular tachycardia with underlying or-
ganic heart disease, 40 were dead within threehours to six months of the onset, with an
average duration of life of twenty-four days.Cooke and White7 noted that 17 of 21 patients
with coronary artery disease expired in froma few hours to eighteen months. Follow-upinformation was available on 84 patients inthis group of 107. In 42 patients in whomventricular tachycardia complicated an acutemyocardial infarction, 28, or 64 per cent,were dead within one month after the attackof tachycardia. Ten lived two years or longer;the longest period of survival was elevenyears. Of 24 patients with coronary sclerosisand attacks of ventricular tachycardia, 10were dead within six months after the firstattack. The remainder lived for periods vary-ing from one to ten years. The outlook, ascan be seen, is particularly grave in those inwhom the tachycardia complicates an acutemyocardial infarction. Patients, however, maylive for many years if there is recovery fromthe acute attack, and in addition these yearsmay be useful and productive ones.There was follow-up information available
on 6 patients with rheumatic valvular diseaseand ventricular tachycardia. Three were deadwithin one month after the episode. Two diedwithin eighteen months and one is alive atthe end of five years.The patients with no underlying heart
disease have a very favorable prognosis ashas been previously mentioned.5 There were13 such patients in this group. In one patient,death was due to Adams-Stokes attacks whichhad recurred for three years; in another it wasdue to a neoplasm. Eight were alive and wellfor periods of from nine to twenty-one yearsafter the attacks. In some of the patientsthe paroxysms ceased spontaneously. Theprognosis in these patients was not affectedby their having multiple attacks.
In general it may be said that althoughparoxysmal ventricular tachycardia is aserious complication of coronary artery disease,there are enough instances in which a satis-factory and useful recovery takes place tomake one hopeful. It appears to be an especiallyominous complication when occurring in asso-ciation with rheumatic valvular heart diseasebut the outlook may be very favorable whenthe arrhythmia is unassociated with anystructural disease of the heart.
35
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from
PAROXYSMAL VENTRICULAR TACHYCARDIA
TREATMENT
Several drugs have been used in the treat-ment of this arrhythmia. In 1921, Scott"successfully used quinidine orally to controlrecurrent episodes of ventricular tachycardia.In 1927, Levine and Stevens12 tried intra-venous quinidine therapy in an effort to effectreversion of ventricular tachycardia compli-cating an acute myocardial infarction. Thisattempt was unsuccessful with the smallintravenous dose used but the arrhythmiawas reverted to normal sinus rhythm withmuch larger oral doses of quinidine. In 1937,Hepburn and Rykert27 successfully treated 8patients having paroxysmal ventricular tachy-cardia with quinidine administered intra-venously. These authors advocated the useof quinidine intravenously only in patients whowere moribund or in shock.
Zwillinger36 first reported the value of mag-nesium sulfate in patients with ventriculartachycardia. Boyd and Scherf37 treated 2patients with this drug; the treatment waseffective in one. In 1932, Sampson and Ander-son38 used potassium salts in an effort to con-trol auricular and ventricular ectopic beatsand auricular and ventricular tachycardia.One patient with ventricular tachycardiawas treated successfully but in another aparadoxical effect occurred and ventriculartachycardia was produced. Stempien andKatz39 used potassium chloride with successin a case that was refractory to all other formsof therapy. Salley14 described the use of atro-pine with quinidine after the ventricularrate has been slowed by the latter. Sabathie40noted that morphine given intravenouslywas of value in 9 of 10 patients.
In some instances, both the persistentform (of hours' or days' duration) of thetachycardia and the intermittent type ceasedspontaneously without any form of therapy.There were 6 patients with persistent tachy-cardia in whom reversion was effected withouttreatment and 12 with intermittent episodeswho required no therapy. There were 4 patientswho expired before any type of treatmentcould be given.
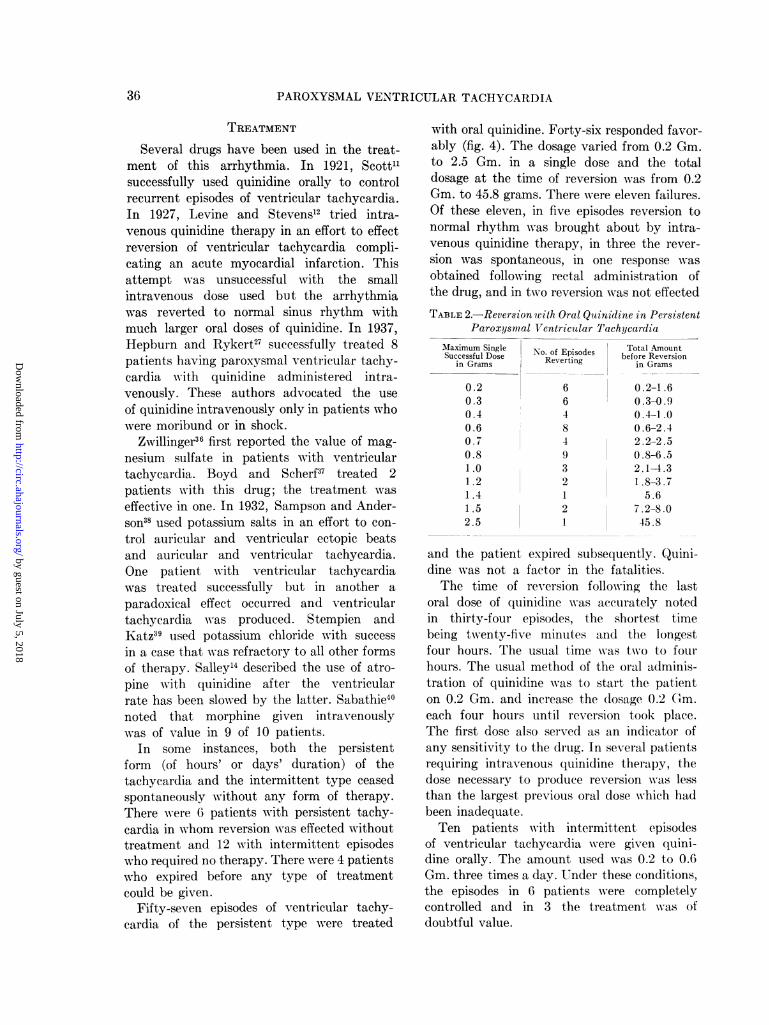
Fifty-seven episodes of ventricular tachy-cardia of the persistent type were treated
with oral quinidine. Forty-six responded favor-ably (fig. 4). The dosage varied from 0.2 Gm.to 2.5 Gm. in a single dose and the totaldosage at the time of reversion was from 0.2Gm. to 45.8 grams. There were eleven failures.Of these eleven, in five episodes reversion tonormal rhythm was brought about by intra-venous quinidine therapy, in three the rever-sion was spontaneous, in one response wasobtained following rectal administration ofthe drug, and in two reversion was not effected
TABLE 2.-Reversion with Oral Quinidine in PersistentParoxysmal Ventricular Tachycardia
Maximum Single No. of Episodes Total AmountSuccessful Dose Reverting before Reversion
in Grams Rvrigin Grams
0.20.30.40.60.70.81.01.21.41.52.5
66484932121
0.2-1.60.3-0.90.4-1.00.6-2.42.2-2.50.8-6.52.1-4.31 .8-3.7
5.67.2-8.045.8
and the patient expired subsequently. Quini-dine was not a factor in the fatalities.The time of reversion following the last
oral dose of quinidine was accurately notedin thirty-four episodes, the shortest timebeing twenty-five minutes and the longestfour hours. The usual time was twio to fourhours. The usual method of the oral adminis-tration of quinidine was to start the patienton 0.2 Gm. and increase the dosage 0.2 (G)m.each four hours until reversion took place.The first dose also served as an indicator ofany sensitivity to the drug. In several patientsrequiring intravenous quinidine therapy, thedose necessary to produce reversion was lessthan the largest previous oral dose which hadbeen inadequate.Ten patients with intermittent episodes
of ventricular tachycardia were given quini-dine orally. The amount used was 0.2 to 0.6Gm. three times a day. Under these conditions,the episodes in 6 patients were completelycontrolled and in 3 the treatment was ofdoubtful value.
36
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from
CHARLES A. ARMBRUST, JR. AND SAMUEL A. LEVINE
In thirty-one persistent episodes of ventric-ular tachycardia, quinidine was administeredintravenously. The treatment was successfulin 20 cases. The single intravenous dosesvaried from 0.2 to 1.5 grams. In six of thetwenty episodes, reversion was not effectedon the first intravenous dose but was accom-plished on the second. The second intravenousdose varied greatly in amount. There wereeleven failures with this method. In 2 of these11 patients, reversion to normal sinus rhythmfollowed a larger single oral dose of quinidine,in one it followed the administration ofmagnesium sulfate, in one, failure followedthree injections of quinidine in fifteen hours(total 3.4 Gm.) and reversion took placespontaneously the next day. In one patientthe therapy was stopped after 0.3 Gm., in 2patients death was the result of ventriculartachycardia, and in 4 death was due to quini-dine toxicity. The first of the four fatalitiesdue to quinidine occurred in a 55 year oldwoman, with mitral stenosis and mitralinsufficiency, who was in a moribund statewith pulmonary edema and shock. She diedafter 0.6 Gm. quinidine been given in 100 cc.
of 5.0 per cent glucose solution in twentyminutes. The second patient was a man, 63years of age, with hypertension, aortic steno-sis, aortic insufficiency, and an acute myo-
cardial infarction. He was in uremic coma
and had congestive heart failure. He was
given 0.3 Gm. quinidine in a few minutes, whenrespirations suddenly ceased. The third, a
woman, 58 years old, with an acute myocardialinfarction, in extreme shock, was given 0.6 Gm.quinidine in 200 cc. of solution in twenty-fiveminutes. The heart rate fell from 137 to 100beats per minute. She then received 0.6 Gm.quinidine in one to two minutes and respira-tions ceased two minutes later. The fourth,a woman 51 years old, with mitral stenosis,mitral insufficiency, auricular fibrillation, andmarked congestive failure, was in extremiswith a blood pressure of 80/60. After 0.1Gm. quinidine in 30 cc. of solution had beengiven slowly, she expired. It is clear from these4 cases that all fatalities occurred in patientswho were in extremis. In each instance it didnot appear that they would have survivedfor many minutes or more than a few hours.
Thirteen patients were treated with mag-nesium sulfate given intravenously in dosesvarying from 2 to 5 grams. One patient receivedonly 1 gram. Nine received two or more in-jections, usually within thirty minutes ofeach other. In 2 cases, reversion to normalsinus rhythm took place and in one casethe ventricular tachycardia w-as convertedto 2:1 flutter. The side effects noted weresimilar to those described by Boyd and Scherf,37namely, a feeling of intense heat, flushing,and nausea. The value of magnesium sulfateis not great but the drug is relatively safeand therefore can be tried early. It provedeffective rarely when quinidine failed.
In 7 patients, atropine sulfate was giveneither intravenously or intramuscularly indoses of 1 or 2 milligrams. The atropine wasusually given after maximum slowing of theventricular rate had been brought about byquinidine. The most dramatic effect occurredin the patient previously described by Salley,'4in whom the ventricular rate was slowed from160 to 112 following 2.0 Gm. quinidine givenby mouth; then 2 mg. of atropine were givenintramuscularly and almost immediately com-plete heart block with a ventricular rate of30 developed. There were 2 other patientsin whom atropine may have been instrumentalin causing reversion of the tachycardia tonormal sinus rhythm. One patient had hadventricular tachycardia for twenty-one daysand had failed to respond to magnesiumsulfate, quinidine either orally or intravenously,and potassium salts. Finally 1 Gm. of quinidinewas given intravenously and the rate fellfrom 180 to 110; 2 mg. of atropine were givenand normal sinus rhythm occurred almostat once. The second patient had had ventric-ular tachycardia for twenty days and hadnot responded to any form of therapy. Shewas given 2.5 Gm. of quinidine by mouth ina single dose. After the heart rate slowed,1 mg. of atropine was given and reversiontook place in about two hours. The atropinemay not have played any part in the reversionin this case. In the remaining cases atropinewas of no value. Salley14 suggested that atropinebreaks up the circus of ventricular tachycardiaby paralysing the vagus and that this effectlengthens the refractory period of the ven-
37
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from
PAROXYSMAL VENTRICULAR TACHYCARDIA
tricles. Wilburne and collaborators4l producedventricular tachycardia in animals by theintravenous injection of epinephrine and foundthat the arrhythmia could be prevented bythe use of atropine prior to the administrationof epinephrine.
Potassium salts were used only in 2patients and proved to be of no value. Mlor-phine (30 mg.) was given intravenously toone patient and failed to cause reversion.The drug of choice in the treatment of ven-
tricular tachycardia, in our opinion, is quini-dine. The route of administration of thequinidine depends on the clinical conditionof the patient. If the condition is critical,the drug should be given by the intravenousroute. This is a matter of individual judge-ment and difficult to express in very definitiveterms. In general, if it appears that the patientis likely to succumb in minutes or hoursthe intravenous route is preferable, whereasif he is likely to survive for days the oralmethod might be employed. Quinidine hydro-chloride, diluted (0.6 Gm. with 200 cc. of 5per cent glucose in distilled water), may begiven by slow drip over a period of about onehour.* Electrocardiograms, made continuouslyor frequently during the injection, are helpfulin that the procedure can be stopped instantlyif reversion takes place or if any threateningdisturbance in the cardiac mechanism occurs.If the first intravenous injection fails, a similaror larger amount may be given within severalhours.
There are many difficulties in appraisingand predicting the effect of oral quinidinedosage. One common error in general practiceis to continue the same oral dosage day afterday. This applies not only to the treatmentof paroxysmal ventricular tachycardia butto auricular fibrillation and other arrhythmias.If a certain program, such as 0.2 to 0.3 Gm.three times a day, is not effective in a day ortwo it is not likely to be any more effectiveif continued indefinitely.42 The maximumeffective blood level of the drug is reachedabout an hour or two after oral administrationand there is practically none left in the bloodstream twenty-four hours later.4' 4 On the
*Quinidine hydrochloride supplied through thecourtesy of Brewer & Company, Worcester, Mass.
other hand, the blood level need not be thedetermining factor in causing an effect onthe heart or reversion to normal sinus rhythm.This is well illustrated by the experienceswe have had in which auricular fibrillationhas reverted to normal rhythm six hours ormore after the last dose had been given. Insuch cases the blood level must have passedits peak when sudden regularization took place.
In general it is of little importance toestimate the total amount of the drug em-ployed. The significant factor is the largestsingle dose that is required to effect reversion.Many patients have had 10 or 20 Gm. ofquinidine given as a total dose over manydays without any beneficial effect on theirarrhythmia, while a total of 1 or 2 Gm. whengiven in increasing doses over the courseof one or two days was effective. In administer-ing quinidine either orally or intravenouslyit is helpful to observe a slowing of the ventriclewhich occurs quite frequently. This indicatesa partial effect in the right direction andmakes one think that further dosage mightproduce the desired regularization.Another value of quinidine is that even if
the drug does not cause reversion of theventricular tachycardia, it may keep the ven-tricular rate at a slower rate and improvethe general state of the patient.45 Such aneffect has been noted in many of the patientsin this series. Quinidine has also been reportedas being valuable in controlling bidirectionalventricular tachycardia.46Much has been said and written about the
toxic effects of quinidine. In the treatmentof ventricular tachycardia these matters areof very little importance as the conditionunder consideration is already critical andoften fatal if uncontrolled. Excessive quinidinemay produce shock but these patients arenot infrequently already in shock. In manycases marked distortion of the electrocardio-grams resulted from the large doses of quini-dine. Had such abnormalities been used as acriterion for cessation of therapy the attackswould not have been controlled. It is difficultto define the exact indication for discontinuingthe drug. It is reasonable to regard suddensyncope or some other obviously desperateuntoward complication such as convulsions
38
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from
CHARLES A. ARMBRUST, JR. AND SAMUEL A. LEVINE
as sufficient reason to discontinue the treat-ment. The fact that the patient becomesnauseated, dizzy, weak, or develops diarrheaor ringing of the ears should not discouragethe physician from persisting with this therapy,when the alternative is likely to be a fataltermination.
SUMMARY1. The following observations were made
from a study of 107 patients with paroxysmalventricular tachycardia, varying in age from13 to 83 years, with the majority between50 and 70 years.
2. The diagnosis can often be suspectedby simple bedside examination but is betterconfirmed by electrocardiographic studies. Onclinical examination an occasional case canbe overlooked because only one heart soundmay be present to each cardiac cycle so thatthe physician estimates the rate at one-halfits actual value.
3. In 79 patients (74 per cent) the under-lying cause of the heart disease was coronaryartery disease, generally with recent or oldmyocardial infarction. Nine patients hadrheumatic heart disease, 13 no heart disease,and 6 miscellaneous conditions.
4. There were 27 patients who had re-currences of prolonged attacks over the courseof months or years.
5. The duration of the prolonged attacksvaried from hours to twenty-four days.
6. It seemed that digitalis played a role inthe precipitation of the paroxysmal ventriculartachycardia in only a small number of in-stances.
7. Although the attack of tachycardia maybe symptomless, it is frequently accompaniedby substernal pain, sudden collapse, shock,dyspnea, or syncope.
8. The immediate prognosis of the attackof tachycardia is very good, since in all buta few subjects normal rhythm was resumedfollowing appropriate therapy. The ultimateprognosis is grave in those who have under-lying coronary or valvular disease; however,a fair number of these were able to carry ona useful occupation for years.
9. In the group of subjects with no organicheart disease the prognosis is generally excel-
lent. Even in this group the threat of suddendeath is present; death during a paroxysmoccurred in one patient who had a structurallynormal heart post mortem.
10. In this study, magnesium sulfate ad-ministered intravenously was occasionally ofvalue, potassium salts given orally were ofno value in the few instances in which theywere employed, and morphine given intra-venously failed on the one occasion it wastried. The treatment of choice was quinidinetherapy. The oral administration was success-ful in forty-six of fifty-seven episodes. Theintravenous route, used in the more desperatecases, was successful in twenty out of thirty-one attacks.
11. The intelligent use of quinidine wasfound to be of great value in this conditionand not infrequently life saving.
REFERENCESLEWIS, T.: Single and successive extrasystoles.
Lancet 1: 382, 1909.2 HART, T. S.: Paroxysmal tachycardia. Heart 4:
128, 1912.VAUGHAN, W. T.: A stu(ly of paroxysmal tachy-
cardia with especial reference to tachycardia ofventricular origin. Arch. Int. Med. 21: 381, 1918.
4 WILLIUS, F. A.: Paroxysmal tachycardia of ven-tricular origin. Boston M. & S. J. 178: 40, 1918.
STRAUSS, M. B.: Paroxysmal ventricular tachy-cardia. Am. J. M. Sc. 179: 337, 1930.
6 LUNDY, C. J. , AND MICLELLAN, L. L.: Paroxys-mal ventricular tachycardia: An etiologicalstudy with special reference to the type. Ann.Int. Med. 7: 812, 1934.
7 COOKE, W. T., AND WHITE, P. D.: Paroxysmalventricular tachycardia. Brit. Heart J. 5: 33,1943.
8 WILLIAMS, C. , AND ELLIS, L.: Ventricular tachy-cardia, an analysis of 36 cases. Arch. Int. MIed.71: 137, 1943.
9 LEWIS, T.: The experimental production of parox-ysmal tachycardia and the effects of ligation ofthe coronary arteries. Heart 1: 98, 1909-10.
10 POBINSON, G. C., AND HERRMANN, G. R.: Parox-ysmal tachycardia of ventricular origin, and itsrelation to coronary occlusion. Heart 8: 59,1921.
1 SCOTT, R. W.: Observations on a case of ventricu-lar tachycardia with retrograde conduction.Heart 9: 297, 1921-22.
12 LEVINE, S. A., AND STEVENS, W. B.: The thera-peutic value of quinidine in coronary thrombo-sis complicated by ventricular tachycardia. Am.Heart J. 3: 253, 1928.
39
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from
PAROXYSMAL VENTRICULAR TACHYCARDIA
13 , AND FULTON, M. N.: The effect of quinidinesulfate on ventricular tachycardia. J.A.M.A.92: 1162, 1929.
14 SALLEY, S. M.: An unusual atropine effect on
ventricular tachycardia. Am. J. M. Sc. 183:456, 1932.
15 LEVINE, S. A., AND BEESON, P. B.: The Wolff-Parkinson-White syndrome with paroxysms ofventricular tachycardia. Am. Heart J. 22: 401,1941.
16 , AND CURTIS, A. N.: A case of ventricular
tachycardia and auricular fibrillation: An un-
usual problem in therapy. Am. Heart J. 1: 413,1926.
17 : The clinical recognition of the various types
of paroxysmal rapid heart action. Boston M.& S. J. 184: 53, 1921.
18 STRONG, G. F. , AND LEVINE, S. A.: The irregu-larity of the ventricular rate in paroxysmalventricular tachycardia. Heart 10: 125, 1923.
19 LEVINE, S. A.: The clinical recognition of parox-
ysmal ventricular tachycardia. Am. Heart J.3: 177, 1927.
20 GALLAVARDIN, L.: Tachycardia paroxystique ven-triculaire. Arch. d. mal. du. cceur 13: 121, 1920.
21 PRINZMETAL, M., AND KELLEY, F.: On the sig-nificance of the jugular pulse in the clinicaldiagnosis of ventricular tachycardia. Am. HeartJ. 9: 370, 1934.
22 MARVIN, H. M., AND WHITE, P. D.: Observationson paroxysms of tachycardia. Arch. Int. Med.29: 403, 1922.
23 BARNES, A. R., AND WILLIUS, F. A.: Cardiac painin paroxysmal tachycardia. Am. Heart J. 2:490, 1926.
24 LEVINE, S. A. , AND GOLDEN, R.: Some observa-tions on paroxysmal rapid heart action withspecial reference to roentgen-ray measurementsof the heart in and out of attacks. Arch. Int.Med. 29: 836, 1922.
25 MAYS, A. T.: Ventricular tachycardia of unusu-
ally long duration (seventy-seven days). Am.Heart J. 23: 119, 1942.
26 KERR, W. J. , AND BENDER, W. L.: Paroxysmalventricular fibrillation with cardiac recovery ina case of auricular fibrillation and completeheart-block while under quinidine sulphate ther-apy. Heart 9: 269, 1921.
27 HEPBURN, J. H., AND RYKERT, H. E.: The use ofquinidine sulfate intravenously in ventriculartachycardia. Am. Heart J. 14: 620, 1937.
28 HERRMANN, G. R., AND HEJTMANCIK, M. R.: A
clinical and electrocardiographic study of parox-ysmal ventricular tachycardia and its manage-ment. Ann. Int. Med. 28: 989, 1948.
29 LANGENDORF, R.: Auricular fibrillation withanomalous A-V conduction (WPW syndrome)imitating ventricular paroxysmal tachycardia.Am. Heart J. 37: 645, 1949.
° MARVIN, H. M.: Paroxysmal ventricular tachy-
cardia with alternating complexes due to digi-talis intoxication. Am. Heart J. 4: 21, 1928.
31 SHERF, D., AND KISCH, F.: Ventricular tachy-cardias with variform complexes. Bull. NewYork M. Coll., Flower & Fifth Ave. Hosps.2: 73, 1939.
32 BARNES, A. R.: Cerebral manifestations of parox-ysmal tachycardia. Am. J. M. Sc. 171: 489,1926.
33 DAVIS, D., AND SPRAGUE, H. B.: Ventricularfibrillation. Its relation to heart block; Reportof a case in which syncopal attacks and deathoccurred in the course of quinidine therapy.Am. Heart J. 4: 559, 1929.
34 SCHWARTZ, S. P., AND JEZER, A.: Transient ven-tricular fibrillation. The clinical and electro-cardiographic manifestations of the syncopalseizures in a patient with auriculoventriculardissociation. Arch. Int. Med. 50: 450, 1932.
35 PARKINSON, J., PAPP, C., AND EVANS, W.: Theelectrocardiogram of the Stokes-Adams attack.Brit. Heart J. 3: 171, 1941.
36 ZWILLINGER, L.: Uber Die Magnesiumwirkungauf das Herz. Klin. Wchnschr. 14: 1429, 1935.
31 BOYD, L. J., AND SCHERF, D.: Magnesium sulfatein paroxysmal tachycardia. Am. J. M. Sc. 206:43, 1943.
38 SAMPSON, J. L., AND ANDERSON, E. M.: The treat-ment of certain cardiac arrhythmias with po-tassium salts. J.A.M.A. 99: 2257, 1932.
STEMPIEN, S., AND KATZ, K. H.: Quinidine andpotassium in the treatment of refractory parox-ysmal ventricular tachycardia. Am. Heart J.24: 555, 1942.
41 GONZALEZ SABATHIE, L.: On the intravenous useof morphine in the treatment of paroxysmalventricular tachycardia. Am. Heart J. 33: 719,1947.
41 WILBURNE, M., SURTSHIN, A., RODBARD, S., ANDKATZ, L. N.: Inhibition of paroxysmal ventricu-lar tachycardia by atropine. Am. Heart J. 34:860, 1947.
42 GOLD, H.: Pharmacologic basis of cardiac therapy.J.A.M.A. 132: 547, 1946.
43 WEISMAN, S. A.: Studies on the time required forthe elimination of quinidine from the heart andother organs. Am. Heart J. 20: 21, 1940.
44 LINENTHAL, A. J., ULICK, S., AND PATTERSON,L. A.: Fluorometric measurement of plasmaquinidine and its correlation with cardiac ef-fects in man. J. Clin. Investigation 26: 1188,1947.
41 RISEMAN, J. E. F., AND LINENTHAL, H. F.: Par-oxysmal ventricular tachycardia; Its favorableprognosis in the absence of acute cardiac dam-age and its treatment with parenterally ad-ministered quinine dihydrochloride. Am. HeartJ. 22: 219, 1941.
46 SCHWAB, E. H.: Observations on the etiology andtreatment of paroxysmal ventricular tachy-cardia. Am. Heart J. 6: 404, 1931.
40
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

CHARLES A. ARMBRUST, JR. and SAMUEL A. LEVINEParoxysmal Ventricular Tachycardia: A Study of One Hundred and Seven Cases
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1950 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.1.1.28
1950;1:28-40Circulation.
http://circ.ahajournals.org/content/1/1/28the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
is located, click Request Permissions in the middle column of the Web page under Services. Furtherthe Editorial Office. Once the online version of the published article for which permission is being requested
can be obtained via RightsLink, a service of the Copyright Clearance Center, notCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from