parenteral and enteral nutrition - angelfire · parenteral and enteral nutrition audis bethea, ......
TRANSCRIPT
1
Parenteral and Enteral Nutrition
Audis Bethea, Pharm.D.Assistant Professor
Therapeutics IDecember 5 & 9, 2003
Parenteral Nutrition
Definition process of supplying nutrients via the intravenous route Synonyms
I. total parenteral nutrition (TPN) , peripheral parenteral nutrition (PPN)
IndicationsI. NPO for 5 – 7 daysII. Patients who cannot or will not
receive nutrition by the enteral/oral route for 5-7 days
Mattox Tw. Pharmacotherapy;. 1999;128: 2231-2236.
2
Parenteral Nutrition
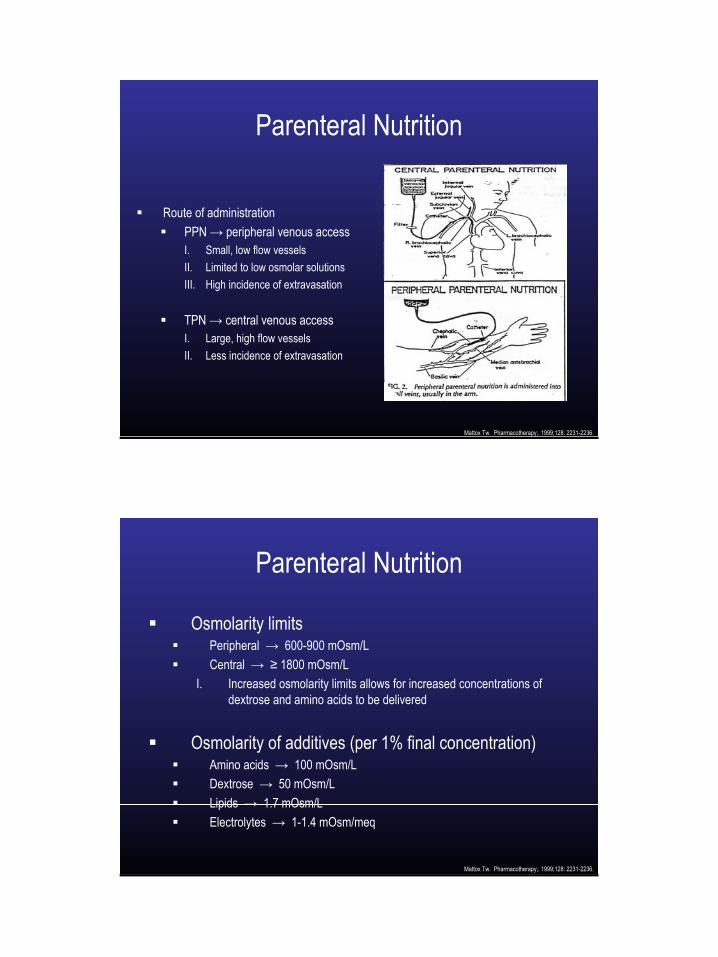
Route of administrationPPN → peripheral venous accessI. Small, low flow vessels II. Limited to low osmolar solutionsIII. High incidence of extravasation
TPN → central venous accessI. Large, high flow vessels II. Less incidence of extravasation
Mattox Tw. Pharmacotherapy;. 1999;128: 2231-2236.
Parenteral Nutrition
Osmolarity limitsPeripheral → 600-900 mOsm/LCentral → ≥ 1800 mOsm/L
I. Increased osmolarity limits allows for increased concentrations of dextrose and amino acids to be delivered
Osmolarity of additives (per 1% final concentration)Amino acids → 100 mOsm/LDextrose → 50 mOsm/LLipids → 1.7 mOsm/LElectrolytes → 1-1.4 mOsm/meq
Mattox Tw. Pharmacotherapy;. 1999;128: 2231-2236.
3
Parenteral Nutrition
Modes of deliveryI. 2 in 1 → (Dextrose, AA,
electrolytes) with fat emulsion administered separately
II. 3 in 1 → all parenteral nutrients in one bag
Mattox Tw. Pharmacotherapy;. 1999;128: 2231-2236.
Parenteral NutritionRoute of administration
PPN → peripheral venous accessI. Small, low flow vessels II. Limited to low osmolar solutions due to high incidence of
thrombophlebitis and extravasation
TPN → central venous accessI. Large, high flow vessels such as inferior, superior vena cava, internal
jugular (vessels close to the heart)II. Less incidence of thrombophlebitis and extravasation with high
osmolar solutions
Mattox Tw. Pharmacotherapy;. 1999;128: 2231-2236.

4
Parenteral Nutrition3 in 1 → all parenteral nutrients in one bag
AdvantagesI. Decreased infection rate due to less venous line manipulation II. Fewer intravenous lines required for administrationIII. Decreased preparation timeIV. Ease of administration for home useV. Better delivery of fat soluble vitaminsVI. Decreased incidence of bacterial growth in preparation
DisadvantagesI. Lipids may occlude central venous cathetersII. Addition of lipids creates compatibility concernsIII. Stability of the solution is decreased by the addition of lipidsIV. Addition of lipids impairs visual inspection of precipitates
Mattox Tw. Pharmacotherapy;. 1999;128: 2231-2236.
Designing Parenteral Nutrition
Carbohydrates (CHO)Dextrose monohydrate → primary energy source (3.4 kcal/g)
Stock (manufactured) concentrations of dextrose range from 5-70% I. Dextrose 70% (D70W) most commonly used to prepare PN solutions
Amount of CHO in a PN solution is dependant uponI. Caloric requirementsII. Optimal balance of CHO and fat for non-protein calories (NPCs)
Mattox Tw. Pharmacotherapy;. 1999;128: 2231-2236.
5
Designing Parenteral NutritionAmino acids (AA)
Highest source of energy in PN solutions (4 kcal/g)**NOT USED AS A ENERGY SOURCE**
Standard solutions provide essential, semi-essential, and non-essential AAI. Essential AA → unable to be produced by your body; must be ingested
from dietII. Semi-essential → body cannot produce in stressed states III. Non-essential AA → can be produced with adequate nutritional intake
“Specialty” formulas are available for patients with renal and hepatic dysfunction
AA solutions have high osmolarity which limits there use in PPN solutions
Mattox Tw. Pharmacotherapy;. 1999;128: 2231-2236.
Designing Parenteral NutritionIntravenous fat emulsions (Lipids)
Concentrated source of calories I. 10% solution provides 1 kcal/mLII. 20% solutions provides 2 kcal/mL
Provide essential fatty acids (Linoleic and linolenic acid)I. < 10% of daily caloric intake consisting of lipids may lead to depletion of
essential fatty acids
Optimal lipid intake/supplementation is 20-40% of total daily calories
Lipids infused via PPN may provide protection from phlebitis
Mattox Tw. Pharmacotherapy;. 1999;128: 2231-2236.

6
Practice CalculationYou are now ready to order a TPN that will provide your patient with 2600 kcal/day, 150 g of protein/day, and 2500 mL/day. You have decided to decrease the fluid supplementation provided via TPN to account for the extra fluids the patient is receiving through other IV medications. Your hospital only prepares 3-in-1 TPNs so you will need to prepare an order that includes the % of dextrose, protein, and the amount of lipids that you need to provide.
1. Determine what NPC:N ratio you would like to use.Stressed patient → 90 - 120:1 = 150 g protein / 6.25 = 24 g N
= 2600 kcal / 24 g N = 108.3 kcal (NPC):N
2. You decide to provide the NPC as 70% CHO and 30% lipids. How many calories will now be given in the form of CHO and fat?
CHO = 2600 kcal (0.7) = 1820 kcal Lipids = 2600 - 1820 = 780 kcal (rounded to 750 mL)
Practice CalculationNow you need to determine the percentages of dextrose, protein, and the amount of lipids (mL) you need to put into the TPN to provide the calculated parameters.
1. % Dextrose **Hint = % means # of grams per 100mL**
**This TPN will provide 25, 100s (2500/100 = 25)**
= 1820 kcal ÷ 3.4 kcal/g = 535.3 g CHO = 535.3 g CHO ÷ 25 = 21% (round to D 20%)
2. % AA= 150 g AA ÷ 25 = 6% AA
3. Lipids **Ordered as # of calories or mL** ***Can use 10 or 20% lipids***
10% (1 kcal/mL) = 750mL or 20% (2 kcal/mL) = 375 mL
7
Designing Parenteral Nutrition
ElectrolytesElectrolyte supplementation is tailored to individual patient requirements
Supplementation may be affected by sensible losses and complications of illness (diarrhea, ostomy drainage, diaphoresis, refeeding, etc.)
Chloride vs. acetate intake is depends on acid-base balanceI. Generally use equal amounts to maintain balance (1:1 ratio)
a. Metabolic acidosis → maximize acetateb. Metabolic alkalosis → maximize chloride
Calcium and phosphorus are conditionally incompatible!!
Mattox Tw. Pharmacotherapy;. 1999;128: 2231-2236.
Designing Parenteral NutritionIntravenous vitamins
Designed to provide daily allowancesDisease states may alter vitamin requirements
Intravenous trace elementsDesigned to provide daily allowancesStandard preparations contain Mn, Cu, Zn, and Se
InsulinAdded to PN solution to prevent hyperglycemia induced by high (CHO) loadUp to 10% of insulin added to PN solution may adsorb to the IV bag
I. Advantagesa. Tight control of blood glucose improves outcomes and reduces infection b. Prevents consumption of protein as energy source
Mattox Tw. Pharmacotherapy;. 1999;128: 2231-2236.

8
Practice CalculationCW’s TPN order for D20% w/ 6% AA and 375mL 20% lipids is nearing completion. Based on the following basic metabolic panel finalize the order by adding the necessary electrolyte supplementation. CW has been receiving IVF of ½ NS (77meq NaCl/ L)w/ 20 meq KCL @ 75mL/hr.
Sodium 130 meq/L (136-146)
Potassium 3.2 meq/L (3.4-5.3)
Chloride 96 meq/L (101-111)
Bicarbonate 35 meq/L (21-31)
Glucose 130 mg/dL (60-110)
BUN 20 mg/dL (5-18)
Creatinine 0.9 mg/dL (0.5-1.2)
**As ordered in the TPN**
Sodium 100 meq/L
Potassium 25 meq/L
Chloride:Acetate ratio → 2:1
Add MVI, trace elements
**Remember Ca-Phos product for precipitation**
Consider adding insulin if BG increases
***IVF have provided 1800mL of fluid/d, 36 meq of KCl, and 138.6 meq of NaCl
Practice CalculationCW’s TPN has been is now being infused. You are ready to go home for the day, but need to first order labs for monitoring CW’sTPN. What do you order?
1. Daily → BMP w/ Ca, Phos, Mg, CBC, FSBG, physical exam, intake/output
2. Weekly → PREALBUMIN, LFTs, trace elements +/- transferrin, +/- indirect calorimetry
9
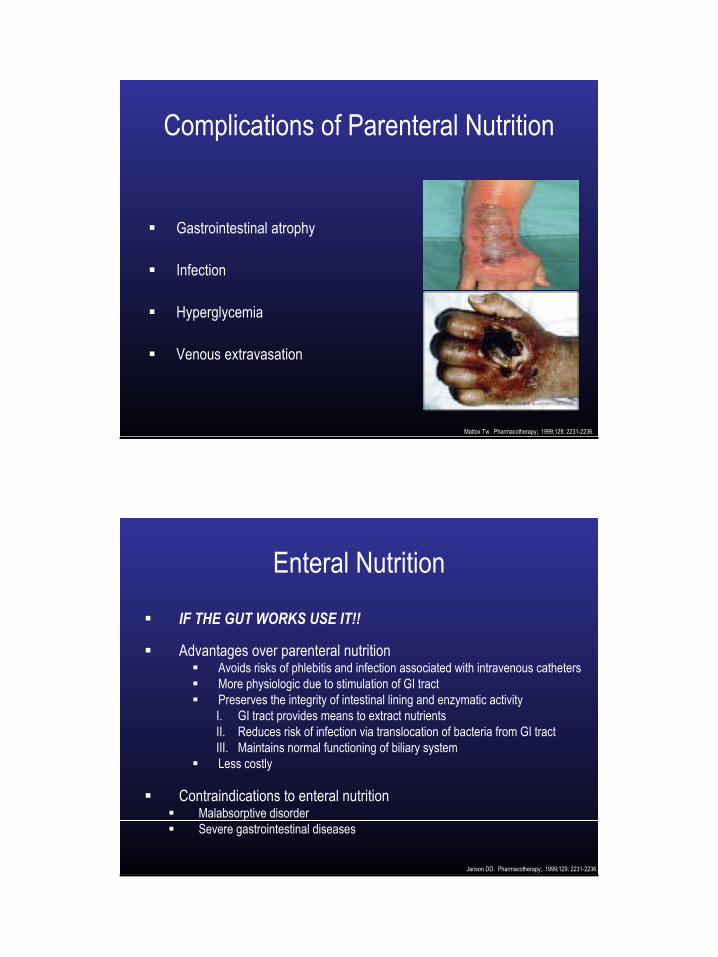
Complications of Parenteral Nutrition
Gastrointestinal atrophy
Infection
Hyperglycemia
Venous extravasation
Mattox Tw. Pharmacotherapy;. 1999;128: 2231-2236.
Enteral Nutrition
IF THE GUT WORKS USE IT!!
Advantages over parenteral nutritionAvoids risks of phlebitis and infection associated with intravenous catheters More physiologic due to stimulation of GI tract Preserves the integrity of intestinal lining and enzymatic activityI. GI tract provides means to extract nutrientsII. Reduces risk of infection via translocation of bacteria from GI tract III. Maintains normal functioning of biliary systemLess costly
Contraindications to enteral nutritionMalabsorptive disorder Severe gastrointestinal diseases
Janson DD. Pharmacotherapy;. 1999;129: 2231-2236.

10
Enteral Nutrition
Administration of enteral nutritionOral Feeding tubes
NG / OG / NJPEG / PEJ
Janson DD. Pharmacotherapy;. 1999;129: 2231-2236.
Enteral NutritionChoosing a feeding tube
StomachI. Most physiologic II. Sensation of being fullIII. Allows use of numerous
feeding formulasIV. Must have intact gag reflex
IntestineI. Patients with gastroparesisII. Delayed gastric emptyingIII. High risk of aspiration
Janson DD. Pharmacotherapy;. 1999;129: 2231-2236.
11
Enteral NutritionAdministration technique
BolusI. More physiologic II. Not administered via tubes in
duodenum or jejunumIII. Administer < 400 mL per
bolus
Continuous I. High nutritional requirementsII. Tubes in the duodenum or
jejunum
Janson DD. Pharmacotherapy;. 1999;129: 2231-2236.
Classification of Enteral Formulas
Monomeric formulas (Peptamen, Vivonex)Pre-digested amino acids to improve absorption
Recommended for patients with altered GI functionI. Peptide-based → partially digested (Peptamen)II. Elemental → most pre-digested form with proteins as free AA
Polymeric formulas (Osmolite, Complete modified, IsoSource) Contains intact macronutrients → triglycerides, protein, and CHO polymers
Highly concentrated and fiber enhanced feeding formulas
Formulas require normally functioning GI tract and absorptive capacity
Janson DD. Pharmacotherapy;. 1999;129: 2231-2236.
12
Classification of Enteral Formulas
Specialized, disease specific formulas (Pulmocare, Nutrihep)Modified for pulmonary, renal, hepatic, and endocrine failureComposition and nutrients vary with indication (modified to a specific disorder)Allows maintenance of nitrogen balance without exacerbating underlying diseaseSpecialized formulas are extremely expensive
Feeding modules/Caloric additivesCHO (carbohydrate polymers) → Moducal®, Polycose®
Protein (casein, whey) → ProMod®, Casec®
Fat → MCT oil®, Microlipid®, corn oilFiber → Unifiber®
Janson DD. Pharmacotherapy;. 1999;129: 2231-2236.
Characteristics of Enteral FormulasOsmolality
↑ osmolality may decrease gastric emptying leading to diarrhea and dehydration
Estimated “free water” Usually dependent upon the formula’s concentration
I. < 1.5 kcal/mL → 80% free waterII. > 1.5 kcal/mL → 70% free water
Percentages account for the amount of water available to meet daily fluid requirements after the product is absorbed
Fiber content Fiber supplementation may help to maintain normal bowel function
Janson DD. Pharmacotherapy;. 1999;129: 2231-2236.
13
Administration of Enteral Nutrition
Intermittent (bolus) administrationNutritional supplementation administered as 4-8 bolusesSimulates normal physiologic eating patternsLess likely to promote drug-food interactionsHigher risk of aspiration
Continuous administrationBeneficial in patients with high nutritional requirementsUseful in patients with malabsorption due to rapid GI transit or impaired digestionLower risk of aspirationMore likely to promote drug-food interactions
Janson DD. Pharmacotherapy;. 1999;129: 2231-2236.
Administration of Enteral Nutrition
Residuals Amount of enteral formula and GI secretions left in the stomach or intestine
High residuals I. Poor gastric or intestinal transit/emptyingII. Increased risk for aspirationIII. Hold feeds
a. Bolus feeding → > 100mLb. Continuous feeding → > 1/2 of rate administered
Therapy for high residualsI. Hold enteral feedings II. Initiate drug therapy with promotility agents
a. Metaclopramideb. Erythromycin
Janson DD. Pharmacotherapy;. 1999;129: 2231-2236.

14
Practice CalculationThe physician thanks you for your excellent work in providing nutritional support for CW (prealbumin is 29 mg/dL). In fact CW is doing so well that we are ready to transition him from parenteral to enteral nutrition. The surgeons would prefer to feed CW via nasogastric tube to prevent introduction of a foreign body into his resected intestine. Please prepare a EN regimen for CW that includes parameters for transitioning from PN.
**You have decided to use a concentrated formula (1.5 kcal/mL) in order to meet CW’s caloric needs.
1. How many mL of formula will CW require?2100 mL (to provide 3200 kcal) —this formula will provide 1470-1680 mL of water
2. Bolus vs. continuous administration?Bolus → goal rate of 350 mL q4 hours
Practice CalculationPlease provide parameters for transitioning CW from TPN to EN and identify any monitoring parameters that may be different from those used with TPN.
1. Initiate EN at 50 mL q4 hours and increase bolus by 50 mL with every feed to a goal rate of 350 mL. Flush tube with 150 mL water q4 hours
2. Decrease TPN to 1 liter and discontinue tomorrow if patient is at EN goal.
3. Monitor residuals q4 x three boluses. Hold boluses and initiatepromotility agent residuals are greater than > 100mL
4. Monitor tube placement every shift
15
Nutritional Supplementation