pan american health organization world health organization
TRANSCRIPT

Pan American Health Organization
World HealthOrganization

Constitution of WHO
Parties to this Constitution declare, in conformity with the Charter of the United Nations, that the following principles are basic to the happiness, harmonious relations and security of all peoples:
Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.
The enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition.
The health of all peoples is fundamental to the attainment of peace and security and is dependent upon the fullest co-operation of individuals and States.
The achievement of any State in the promotion and protection of health is of value to all.Unequal development in different countries in the promotion of health and control of disease,
especially communicable disease, is a common danger.Healthy development of the child is of basic importance; the ability to live harmoniously in a
changing total environment is essential to such development.The extension to all peoples of the benefits of medical, psychological and related knowledge is
essential to the fullest attainment of health.Informed opinion and active co-operation on the part of the public are of the utmost
importance in the improvement of the health of the people.Governments have a responsibility for the health of their peoples which can be fulfilled only by
the provision of adequate health and social measures.
Objective of WHO
The objective of the World Health Organization (hereinafter called the Organization) shall be the attainment by all peoples of the highest possible level of health.
Budget
$854,000,000
NIH Budget
$27,000,000,000
WHO Secretariat Staffing
3,200 in Geneva, and world wide
8,000 in CDC
Regional Office for Africa (AFRO) Cite du Djoue P.O.Box 06 Brazzaville, CongoTelephone: +(1-321) 95 39 100 / +242 839100 Regional Office for the Americas / Pan American Health Organization (AMRO/PAHO) 525, 23rd Street, N.W.Washington, DC 20037U.S.A.
Regional Office for the Eastern Mediterranean (EMRO) WHO Post OfficeAbdul Razzak Al Sanhouri Street, (opposite Children's Library)Nasr City, Cairo 11371 EGYPT
Regional Office for Europe (EURO) 8, ScherfigsvejDK-2100 Copenhagen 0, Denmark
Regional Office for South-East Asia (SEARO) World Health House, Indraprastha EstateMahatma Gandhi RoadNew Delhi 110002 India
Regional Office for the Western Pacific (WPRO) P.O. Box 29321000 Manila Philippines
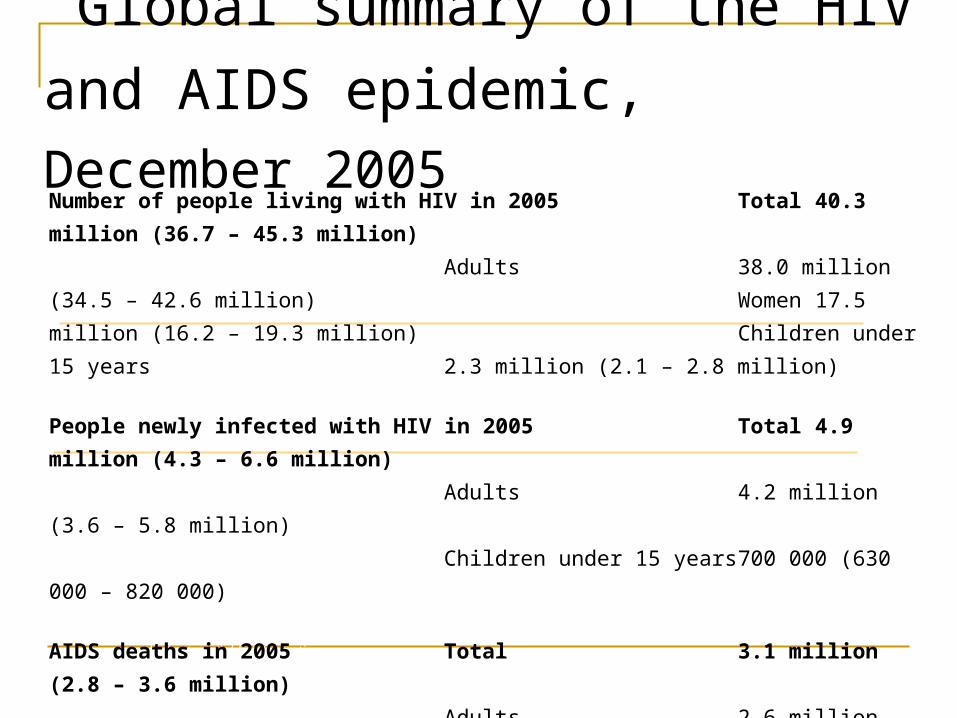
Global summary of the HIV and
AIDS epidemic, December 2005
The ranges around the estimates in this table define the boundaries within which the actual numbers lie, based on the best available information.
Number of people living with HIV in 2005 Total 40.3 million (36.7 – 45.3
million)
Adults 38.0 million (34.5 – 42.6
million) Women 17.5 million
(16.2 – 19.3 million) Children under 15 years
2.3 million (2.1 – 2.8 million)
People newly infected with HIV in 2005 Total 4.9 million (4.3 – 6.6
million)
Adults 4.2 million (3.6 – 5.8
million)
Children under 15 years 700 000 (630 000 – 820
000)
AIDS deaths in 2005 Total 3.1 million (2.8 – 3.6
million)
Adults 2.6 million (2.3 – 2.9
million)
Children under 15 years 570 000 (510 000 – 670
000)
Number of people living with HIV in 2005 Total 40.3 million (36.7 – 45.3 million)
AIDs
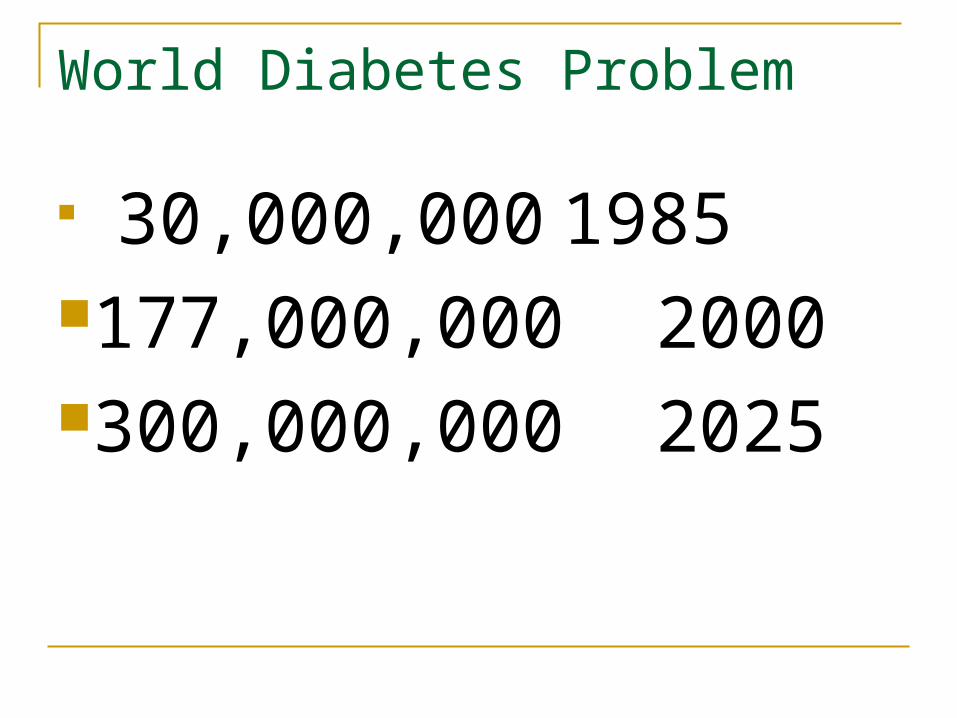
World Diabetes Problem
30,000,000 1985
177,000,000 2000300,000,000 2025
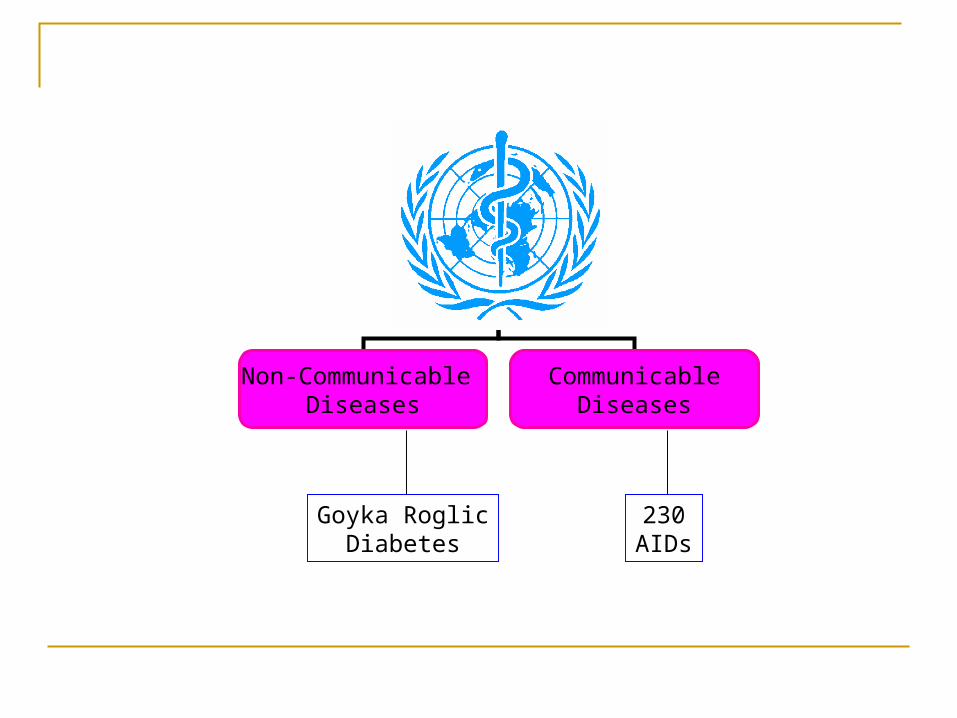
Non-Communicable Diseases
CommunicableDiseases
Goyka RoglicDiabetes
230AIDs

Smallpox, from recorded history until 1978: a lesson in cost effectiveness
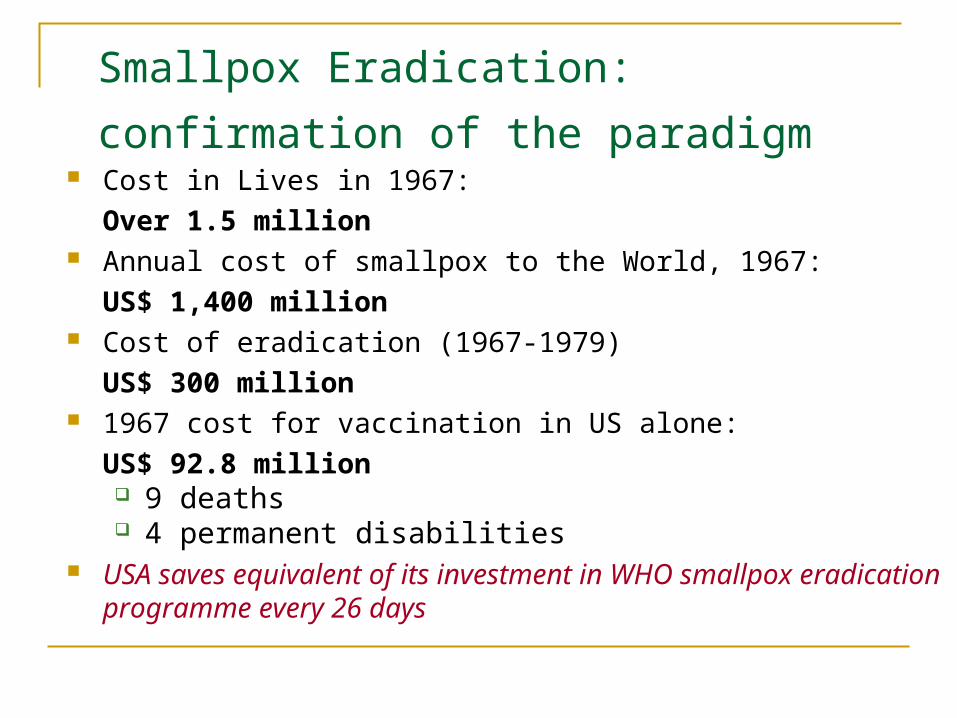
Smallpox Eradication:
confirmation of the paradigm Cost in Lives in 1967:
Over 1.5 million Annual cost of smallpox to the World, 1967:
US$ 1,400 million Cost of eradication (1967-1979)
US$ 300 million 1967 cost for vaccination in US alone:
US$ 92.8 million 9 deaths 4 permanent disabilities
USA saves equivalent of its investment in WHO smallpox eradication programme every 26 days
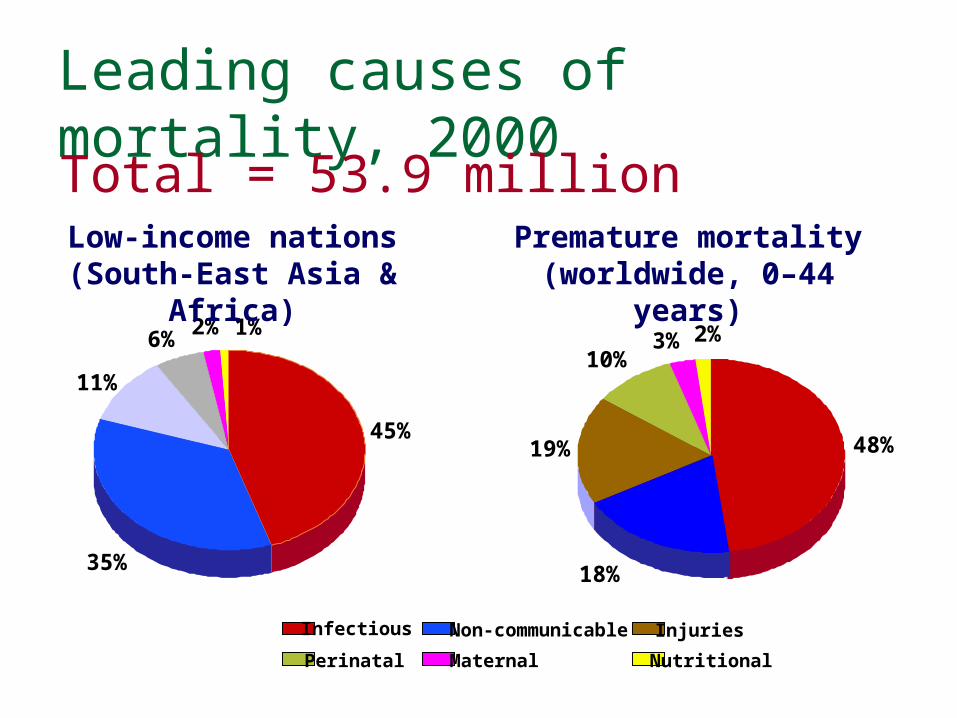
Leading causes of mortality, 2000
48%
18%
19%
10%3% 2%
InjuriesNon-communicable
Perinatal Maternal Nutritional
Infectious
11%
45%
35%
6% 1%2%
Low-income nations(South-East Asia & Africa)
Premature mortality(worldwide, 0–44 years)
Total = 53.9 million
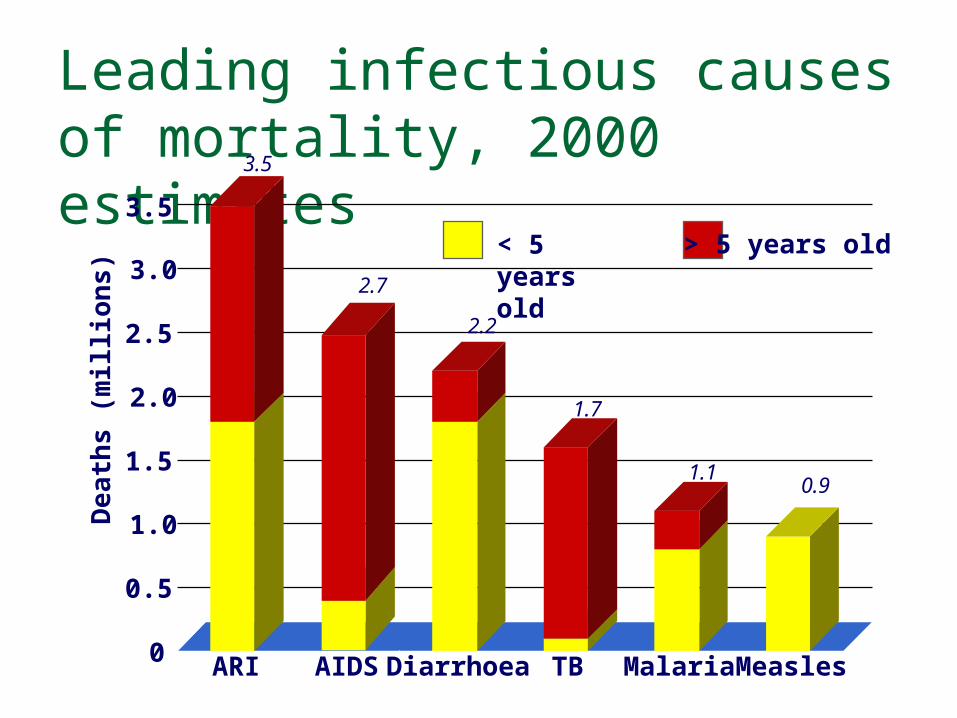
Leading infectious causes of mortality, 2000 estimates
Dea
ths
(mill
ion
s)
< 5 years old > 5 years old
0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
ARI AIDS Diarrhoea TB Malaria Measles
3.5
2.7
2.2
1.7
1.10.9
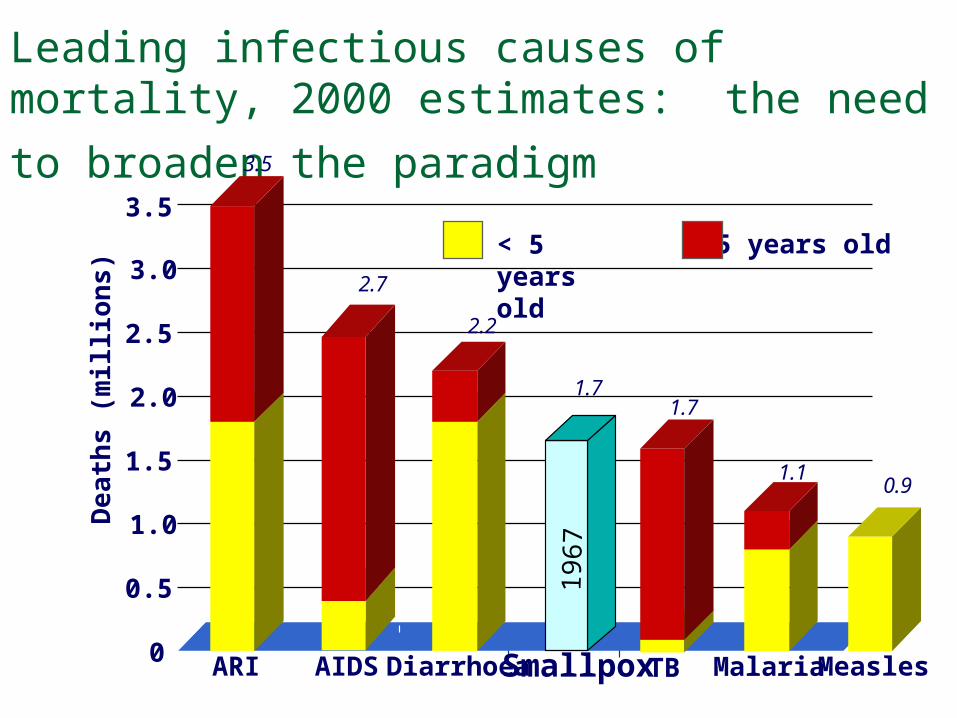
Leading infectious causes of mortality, 2000 estimates: the need to broaden the
paradigm D
ea
ths
(mill
ion
s)
ARI AIDS Diarrhoea
3.5
< 5 years old > 5 years old
0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
2.7
2.2
TB
1.7
Malaria
1.1
Measles
0.9
Smallpox
1.7
196
7
Obstacles to economic development: malaria, tuberculosis and AIDS
Malaria GDP in sub-Saharan Africa would be US$ 100 billion
greater if malaria had been eliminated 35 years ago
Tuberculosis 3–4 months lost work time with 20%–30% lost household
income; 15% greater health expenditure
HIV/AIDS GDP projected to, drop by up to 8% in sub-Saharan Africa
by 2010, and by more than 20% by 2020
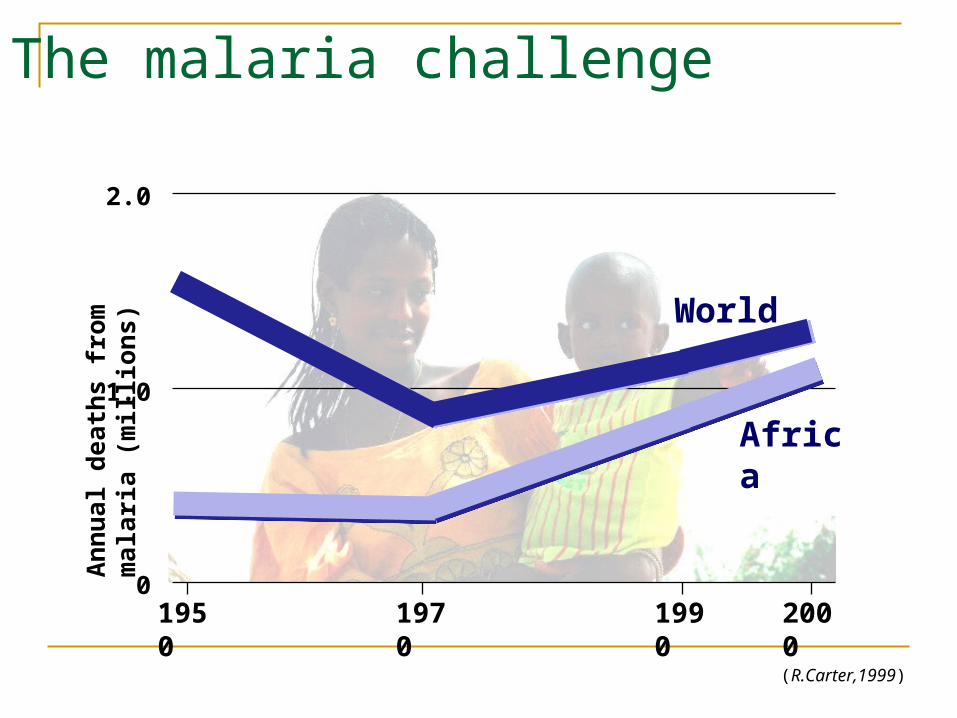
The malaria challenge
(R.Carter,1999)
Ann
ual d
eath
s fr
om m
alar
ia (m
illio
ns)
0
1.0
2.0
Africa
World
1950
1970
1990
2000
Effective evidence-based interventions:Malaria Reduce exposure to mosquitoes
insecticide-treated bednets with priority for children under five and pregnant women
vector control through spraying decrease of breeding sites in environment
Prompt diagnosis and effective treatment presumptive diagnosis in febrile children under five treatment with most appropriate therapy, switching to
combined therapy as resistance thresholds are passed
Intermittent preventive therapy (IPT) in pregnancy
Source: WHO
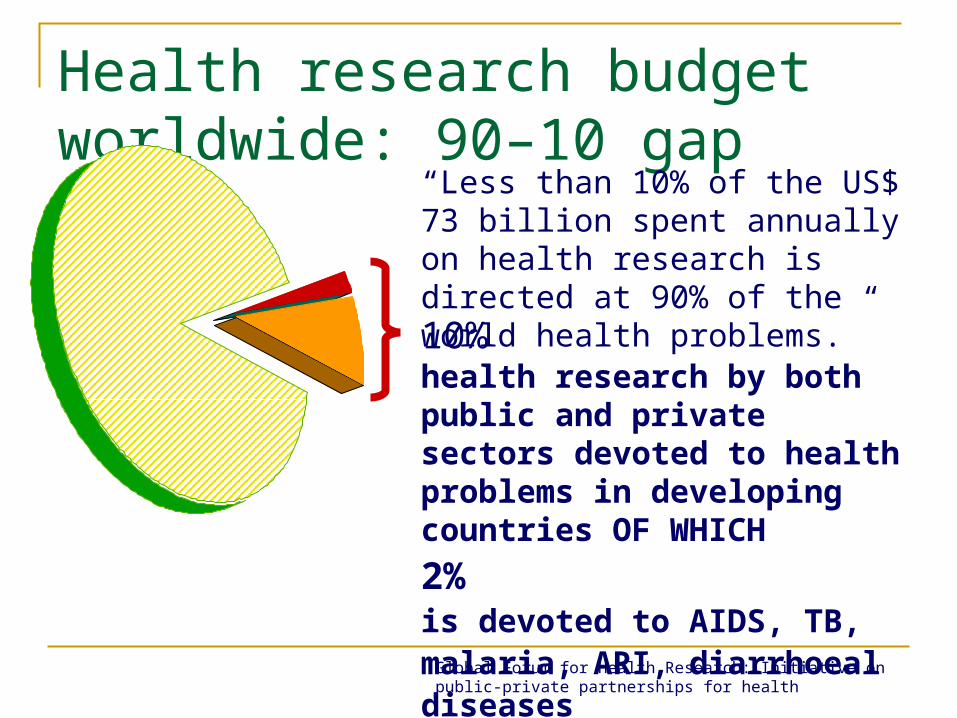
Health research budget worldwide: 90–10 gap
10%health research by both public and private sectors devoted to health problems in developing countries OF WHICH
2%is devoted to AIDS, TB, malaria, ARI, diarrhoeal diseases
“Less than 10% of the US$ 73 billion spent annually on health research is directed at 90% of the world health problems.”
Global Forum for Health Research: Initiative on public-private partnerships for health
Smallpox eradication, 1967–1978: a window of opportunity
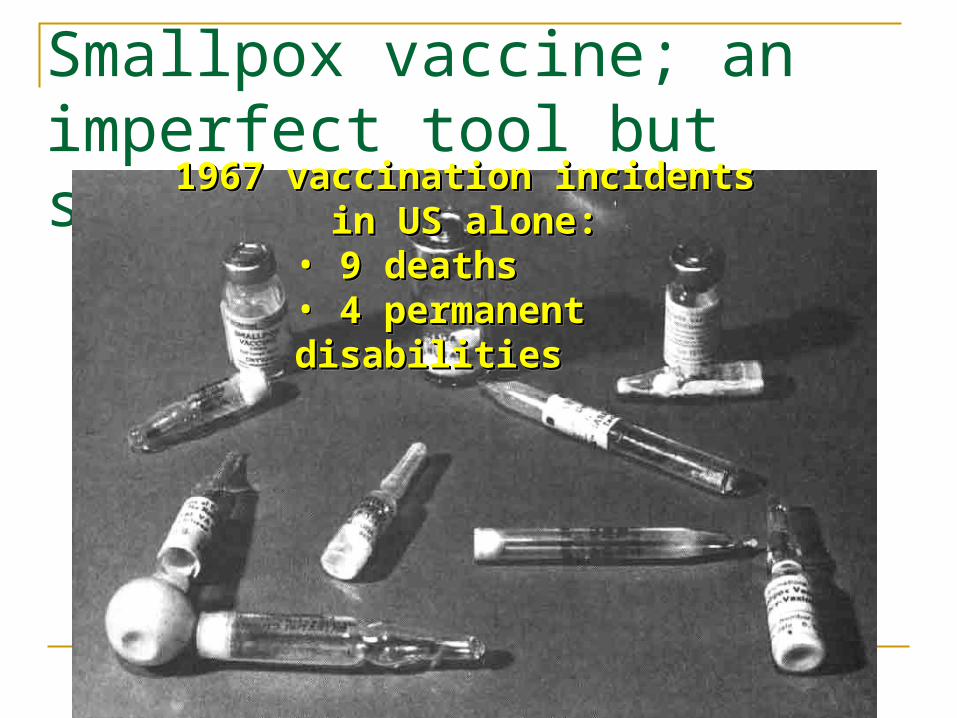
Smallpox vaccine; an imperfect tool but strong justification 1967 vaccination incidents in US 1967 vaccination incidents in US
alone:alone:• 9 deaths9 deaths• 4 permanent disabilities4 permanent disabilities
1967 vaccination incidents in US 1967 vaccination incidents in US alone:alone:
• 9 deaths9 deaths• 4 permanent disabilities4 permanent disabilities
The public health challenge in controlling AIDS, tuberculosis and malariaContinue to broaden the
resource base for infectious disease control before anti-microbial resistance closes the windows of opportunity; and rectify the 90/10 gap in research to ensure the necessary new drugs and vaccines
Dr Gro Harlem BrundtlandPrevious Director General
Bruntland Strategic Approaches for WHO
Reducing excess mortality, morbidity and disability, especially in poor and marginalized populations Promoting healthy lifestyles and reducing risk factors to human health that arise from environmental, economic, social and behavioural causes Developing health systems that equitably improve health outcomes, respond to people's legitimate demands, and are financially fair Framing an enabling policy and creating an institutional environment for the health sector, and promoting an effective health dimension to social, economic, environmental and development policy
Dr Jong-Wook LeeCurrentDirector General Elect

Dr Julio Frenk, Mexico Dr Jong Wook Lee, Republic of Korea Dr Pascoal Manuel Mocumbi, Mozambique Dr Peter Piot, Belgium Professor Ismail Sallam, Egypt
Candidates
Who are we & what do we do?
WHO Strategic DirectionsThe Corporate Strategy focuses WHO’s work on four interrelated strategic directions.Strategic Direction 1: reducing excess mortality, morbidity and disability. Strategic Direction 2: promoting healthy lifestyles and reducing risk factors to human health. Strategic Direction 3: developing health systems that equitably improve health outcomes, respond to people’s legitimate demands, and are financially fair. Strategic Direction 4: framing an enabling policy and creating an institutional environment for the health sector, and promoting an effective health dimension to social, economic, environmental and development policy.
WHO Core FunctionsIn carrying out its activities WHO focuses on the following six core functions:Articulating consistent, ethical and evidence-based policy and advocacy positions; Managing information by assessing trends and comparing performance; setting the agenda for, and stimulating, research and development; Catalysing change through technical and policy support , in ways that stimulate cooperation and action and help to build sustainable national and intercountry capacity; Negotiating and sustaining national and global partnerships; Setting, validating, monitoring and pursuing the proper implementation of norms and standards ; Stimulating the development and testing of new technologies , tools and guidelines.
What are we looking for?Recruitment at WHOThe people we are looking for should…Demonstrate a high level of technical knowledge. Be motivated and have a strong commitment to the policies and programmes of WHO. Possess good analytical skills and a keen interest in and an understanding of policy issues especially in the area of public health. Be able to work well in a multicultural team. Have working experience at national and/or international level, preferably in public health. Be proficient in at least one of the official languages of the Organization (Arabic, Chinese, English, French, Russian and Spanish) and have a working knowledge of a second. Additional languages are an asset.
Recruitment Principles"The paramount consideration in the appointment, transfer or promotion of the staff shall be the necessity of securing the highest standards of efficiency, competence and integrity. Due regard shall be paid to the importance of recruiting and maintaining the staff on as wide a geographical basis as possible." - (WHO Staff Regulation 4.2) We do not discriminate on any ground (race, creed or sex). We are committed to promoting diversity in our workforce. We aim to achieve a broad representation of member country nationals and improve gender balance. We strive to provide an environment where the contribution of each individual is valued. Selection of staff is normally made on a competitive basis.
Who are our staff?Employment Profiles at WHO
WHO recruits staff on fixed-term or temporary contracts. Staff are grouped into two broad streams – Professional or General Service staff. Professional StaffApplicants are normally required to have a university degree as well as a relevant postgraduate specialization, experience at national and/or international level in the required field of public health and development issues. Generally, we seek applications from candidates in the following fields:Health related : medical officers; epidemiologists; public health specialists; related paramedical fields; environmental health specialists; health scientists; statisticians; health economists; policy analysts. Non health-related: finance; human resources; informatics; legal; general administration. Often, the professional technical staff act as advisers in public health to Member states. Candidates should therefore normally have substantial training and experience in this field before they can be considered for an assignment. Because of WHO's particular needs and the keen competition, we are able to offer appointments only to very few applicants. Applications are carefully considered against current and projected vacancies.
What do we offer?Types of Contracts on RecruitmentFixed term AppointmentsA fixed-term appointment is a time-limited appointment for one year or more. The initial contract may be for a period of up to a maximum of two years. The first year is probationary. Any extension is subject to the continued need for the function, availability of funding and satisfactory performance.View conditions of employment for fixed-term appointments (The information provided is intended for use as a guide only.) Temporary AppointmentA temporary appointment is an appointment for a period not exceeding 11 months. Any extension of new contract is subject to the continued need for the function, availability of funding and satisfactory performance. Contracts may be offered for up to a maximum of 44 months total in 4 years. View conditions of employment for temporary appointments (The information provided is intended for use as a guide only.)
WHO Collaborating Centre
What is a WHO collaborating centre ? A WHO collaborating centre is a national institution designated by the Director-General of the World Health Organization to form part of an international collaborative network carrying out activities in support of WHO’s mandate for international health work and its programme priorities. An entire institution, or a department or laboratory within an institution, or a group of facilities for reference, research or training belonging to different institutions, may be designated as a "WHO collaborating centre". When a WHO collaborating centre comprises several departments or institutions, only one of these acts for that centre in relation to WHO. The use of the title, logo and official letterhead of "WHO collaborating centre" is strictly regulated and limited to matters directly related to WHO collaborative activities.
Role of WHO collaborating centres WHO collaborating centres play a strategic role in helping the Organization meet two major needs:
1 they contribute to implementing WHO’s programme priorities, in close coordination with the units concerned in WHO’s six Regional Offices and at headquarters;2 they strengthen institutional capacity in countries and regions.
WHO Project
WHO Multinational Project for Childhood Diabetes (WHO DIAbetes MONDiale)
WHO DiaMond Project
WHO Definition of Health
Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.
The correct bibliographic citation for the definition is: Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference, New York, 19-22 June, 1946; signed on 22 July 1946 by the representatives of 61 States (Official Records of the World Health organization, no. 2, p. 100) and entered
into force on 7 April 1948.
WHO Division of Non-Communicable Diseases
Objective: To reduce the incidence of NCDs and promote positive health
and well-being, with particular focus on developing countries.
What is the WHO global strategy on diet, physical activity and health? Member States at the May 2002 World Health Assembly mandated WHO to formulate a Global Strategy on Diet, Physical Activity and Health. World Health Assembly Resolution 55.23.The Global Strategy Process Document details the process, the timeline and the parties involved in developing the global strategy.The process for developing the strategy includes:Phase I Finalization of the expert consultation report on Diet, Nutrition and the Prevention of Chronic DiseasePhase IIProcess for stakeholder consultation on the WHO Global Strategy on Diet, Physical Activity and Health Track 1 - Regional Consultations with Member States Track 2 - UN agency consultation Track 3 - Consultation with civil society organizations Track 4 - Consultation with the private sector Track 5 - Virtual public consultation Phase IIIDrafting of the global strategy for the WHO Executive Board by February 2003, and presentation to World Health Assembly in May 2004.
http://www.who.int/chp/chronic_disease_report/part4.pdf
What is the Power of WHO?
It’s name Leveraging
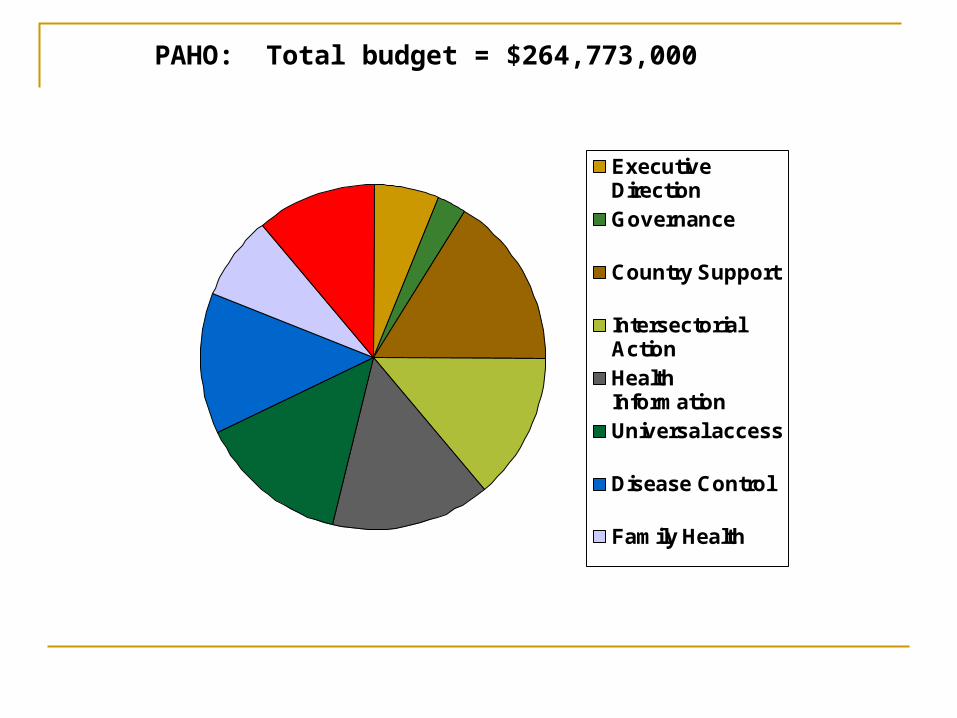
ExecutiveDirectionGovernance
Country Support
IntersectorialActionHealthInformationUniversal access
Disease Control
Family Health
Admin.
PAHO: Total budget = $264,773,000
Purposes of PAHOConstitution of the Pan American Health Organization
The fundamental purposes of the Pan American Health Organization shall be to promote and coordinate efforts of the countries of the Western Hemisphere to combat disease, lengthen life, and promote the physical and mental health of the people

Chronology of Important Events in the History of PAHO
1880- 5th International Sanitary Conference, Washington, D.C.1893-U.S. strengthens quarantine Laws1902-International Sanitary Bureau (ISB) formed by 2nd International
Conference of American States -Birth of Pan American Health Organization1923-ISB renamed Pan American Sanitary Bureau (PASB)1946-Establishment/Birth of World Health Organization (WHO)1949- PASB also becomes the Regional Office of WHO for the
Americans (AMRO)1958-Pan American Sanitary Organization of 1947 renamed
Pan American Health Organization
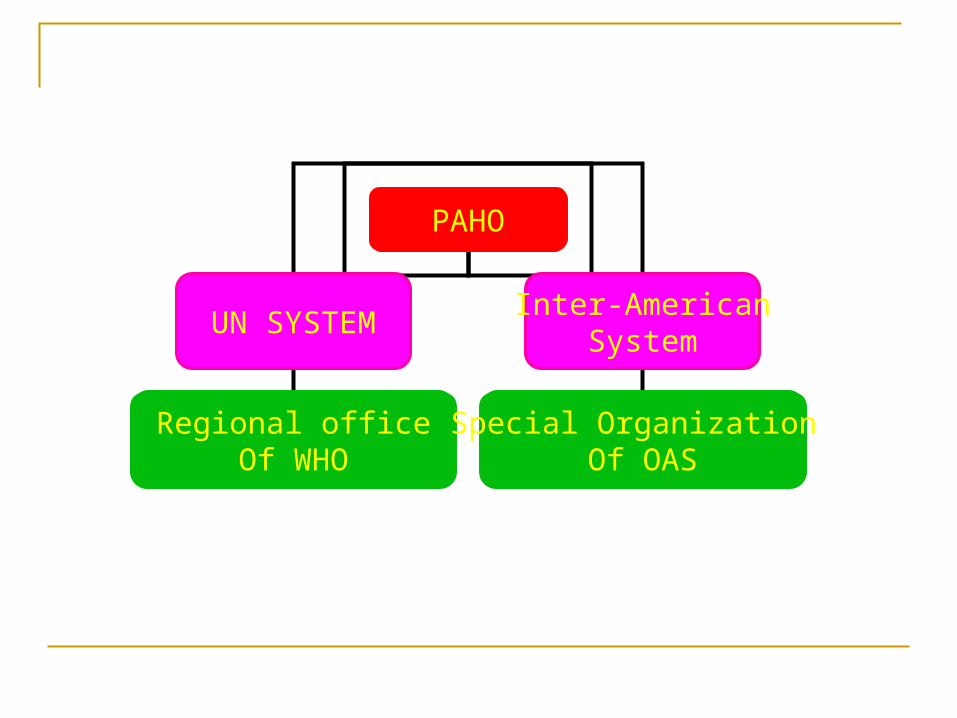
PAHO
UN SYSTEMInter-American
System
Regional officeOf WHO
Special Organization Of OAS
Origins of PAHO
Pan American Sanitary Conference The Directing Council The Executive Committee The Pan American Sanitary Bureau
Membership of Governing Bodies
Pan American Sanitary ConferenceAll Member Governments
Directing CouncilAll Member Governments
Executive CommitteeNine Member Governments
Functions of thePAHO Executive Committee
Analyze documentation for the council or the ConferencePrepare corresponding draft resolutionsPropose agendas and dates for the meetings of the Council or the ConferenceReport to the Council/Conference on its activities and those of its subcommitteesReview and approve administrative and personal policies
Subcommittees of the Executive Committee
Planning and ProgrammingWomen, Health and DevelopmentPAHO Award for AdministrationInter-American Nongovernmental Organizations
Functions of the Pan American Sanitary Conference(cont.)
Prepare periodic revisions of the Pan American Sanitary Code in accordance with the needs and policies determined by the Conference or the Receive the Quadrennial Report of the DirectorReport annually to the Council or ConferenceMaintain records and prepare final report for each accounting periodCreate organizational structure to carry out the authorization program of health activitiesPrepare provisional agenda for the Council, the Conference and the Executive CommitteeEstablish financial rules and procedures
Functions of the Director of the Pan American Health Organization
Serve as CEO of the BureauServe as Secretary ex officio of the Directing Council and Executive CommitteePrepare program and budget for consideration by the Directing Council and Executive CommitteeConvene Special meetings of the Executive Committee as necessaryAppoint technical commissions as authorized by the conference or the CouncilAccept and administer donations and requests to the Organization
Functions of the PAHO/WHO representative
Implement the PAHO/WHO Program of Technical Cooperation and supervise PAHO/WHO staff Establish and maintain close contact with the highest levels of the national administration Provide the government with information concerning PAHO/WHO polices and resolutions of the Governing Bodies of PAHO and WHOEncourage the government in implementing health-for policies and strategies Support the government in the planning and management of national health programs Collaboration with the government in identifying national programs which should receive technical cooperation
Functions of the Directing Council
Define policies, specific strategies, and program activitiesApprove the Organization’s Program Budget every two years.