page buletin penawar - hsajb.moh.gov.myhsajb.moh.gov.my/versibaru/uploads/farmasi/bulletin... ·...
TRANSCRIPT
BULETIN PENAWAR
VOLUME 4/2018
DISEMBER 2018
EDITORIAL BOARD
ADVISOR:
PN HJH ROHAYAH BINTI ABD. GHANI
EDITORS:
PN SITI ROSNAH BT. SURADI
EN MOHD SHAFIE BIN ZABIDI
CIK ZANARIAH BT. ABU BAKAR
HOSPITAL SULTANAH AMINAH
JOHOR BAHRU
KEMENTERIAN KESIHATAN MALAYSIA
JALAN PERSIARAN ABU BAKAR SULTAN
80100 JOHOR BAHRU
TEL: 07-2257000
FAX: 07-2242694
EMAIL: [email protected]
IN THIS ISSUE Updates on Clinical Practice Guideline of
Stable Coronary Artery Disease 2018
Pulmonary Arterial Hypertension in
Adults
Methanol Toxicity
PAGE
2-3
PAGE
4-5
PAGE
6-7
PAGE
8-9
Management of Rhinosinusitis in
Adolescents and Adults
Laporan Aktiviti Bergambar Pameran
dan Ceramah Kenali Ubat Anda di SMK
Infant Jesus Convent
PAGE
10
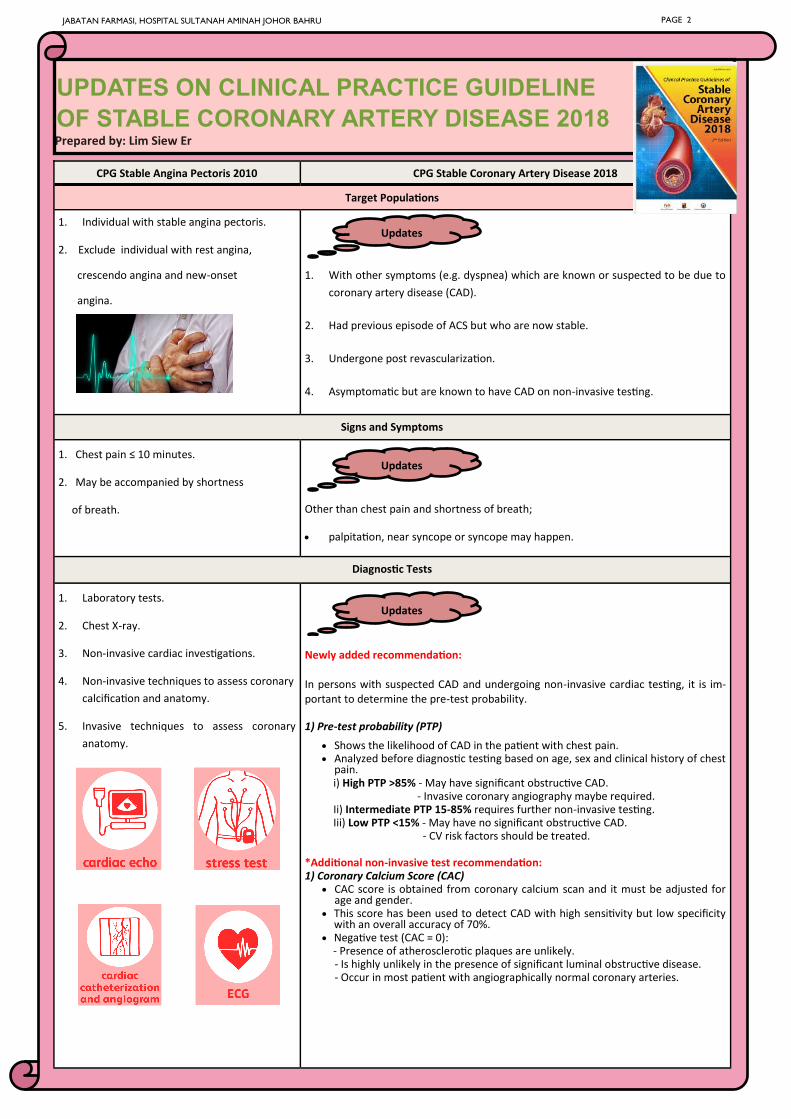
UPDATES ON CLINICAL PRACTICE GUIDELINE
OF STABLE CORONARY ARTERY DISEASE 2018 Prepared by: Lim Siew Er
JABATAN FARMASI, HOSPITAL SULTANAH AMINAH JOHOR BAHRU PAGE 2
CPG Stable Angina Pectoris 2010 CPG Stable Coronary Artery Disease 2018
Target Populations
1. Individual with stable angina pectoris.
2. Exclude individual with rest angina,
crescendo angina and new-onset
angina.
1. With other symptoms (e.g. dyspnea) which are known or suspected to be due to
coronary artery disease (CAD).
2. Had previous episode of ACS but who are now stable.
3. Undergone post revascularization.
4. Asymptomatic but are known to have CAD on non-invasive testing.
Signs and Symptoms
1. Chest pain ≤ 10 minutes.
2. May be accompanied by shortness
of breath.
Other than chest pain and shortness of breath;
• palpitation, near syncope or syncope may happen.
Diagnostic Tests
1. Laboratory tests.
2. Chest X-ray.
3. Non-invasive cardiac investigations.
4. Non-invasive techniques to assess coronary
calcification and anatomy.
5. Invasive techniques to assess coronary
anatomy.
Newly added recommendation:
In persons with suspected CAD and undergoing non-invasive cardiac testing, it is im-portant to determine the pre-test probability.
1) Pre-test probability (PTP)
• Shows the likelihood of CAD in the patient with chest pain. • Analyzed before diagnostic testing based on age, sex and clinical history of chest
pain. i) High PTP >85% - May have significant obstructive CAD. - Invasive coronary angiography maybe required. Ii) Intermediate PTP 15-85% requires further non-invasive testing. Iii) Low PTP <15% - May have no significant obstructive CAD. - CV risk factors should be treated.
*Additional non-invasive test recommendation: 1) Coronary Calcium Score (CAC)
• CAC score is obtained from coronary calcium scan and it must be adjusted for age and gender.
• This score has been used to detect CAD with high sensitivity but low specificity with an overall accuracy of 70%.
• Negative test (CAC = 0): - Presence of atherosclerotic plaques are unlikely.
- Is highly unlikely in the presence of significant luminal obstructive disease. - Occur in most patient with angiographically normal coronary arteries.
Updates
Updates
Updates
Ranolazine PR 375mg, 500mg, 750mg [Ranexa]
• Available as prolonged release formulation.
• Selectively inhibits the late inward sodium current in the
myocardium and thus reducing the intracellular calcium levels
and diastolic LV wall tension. As a result, it reduces myocardial
oxygen demand.
• Initial dose: 375mg BD then titrate to 500mg BD after 2-4
weeks. It can be further titrated to a maximum of 750mg BD.
• Adverse effects: QT interval prolongation or risk of renal fail-
ure in renal impairment patient.
Nicorandil [Adancor]
• Dual pharmacological mechanism of action with adenosine
triphosphate sensitive potassium (KATP) channel agonist and
nitrate-like properties.
• Usual starting dose is 10mg BD which can be titrated up to
20mg BD or maximum dose of 30mg BD.
• Adverse effects: Gastrointestinal ulceration or eye ulceration.
Triflusal 300mg [Grendis]
• An platelet anti-aggregant with structural similarities to
salicylates.
• Usual dose in myocardial infarction is 600mg OD within 24
hours of onset of symptoms.
• Frequency of non-haemorrhagic adverse effects (abdominal
pain, dyspepsia and peptic ulcer) is significantly higher.
• Benefit:
- Less incidence of intracranial and gastrointestinal
haemorrhage in comparison to aspirin.
Sacubitril / Valsartan 24/26mg, 49/51mg, 97/103mg [Entresto]
• Sacubitril inhibits neprilysin, a neutral endopeptidase (NEP)
which then increases levels of endogenous vasoactive
peptides including natriuretic peptides, bradykinin and
adrenomedullin.
• Starting dose: 49/51mg BD then doubling the dose every 2-4
weeks to maintenance dose of 97/103mg BD.
• Adverse reactions: angioedema, hypotension, impaired renal
function and hyperkalemia.
• Black box warnings: Discontinue as soon as possible when
pregnancy is detected as it may result in fetal injury or death.
JABATAN FARMASI, HOSPITAL SULTANAH AMINAH JOHOR BAHRU PAGE 3
Pharmacological Therapy
1) Prevention of cardiovascular events
- Aspirin (Clopidogrel or Ticlopidine for aspirin intolerant
patient).
- Statin therapy (to achieve LDL-C < 1.8mmol/l).
- ACEI / ARB, beta-blockers and mineralocorticoid
antagonists as tolerated .
• Dual antiplatelet therapy (DAPT) is recommended for 12
months post ACS.
- Aspirin and Thienopyridine (clopidogrel or
ticlopidine).
• New alternatives available:
i) Triflusal (for aspirin intolerant patient).
i) Angiotensin-receptor-neprilysin inhibitors
2) Symptomatic control/relieve
- First-line: Short acting nitrate + beta-blockers ± CCBs
to reduce angina.
- Add-on therapy: recommended in patients who
remain symptomatic.
i) Ivabradine,
ii) Trimetazidine,
iii) Long-acting nitrates
• 2 new agents can be used as add-on therapy:
i) Ranolazine
ii) Nicorandil
Updates
Updates
Updated Medications in CPG Stable CAD 2018
History, physical exam, screening
procedures, incidental findings
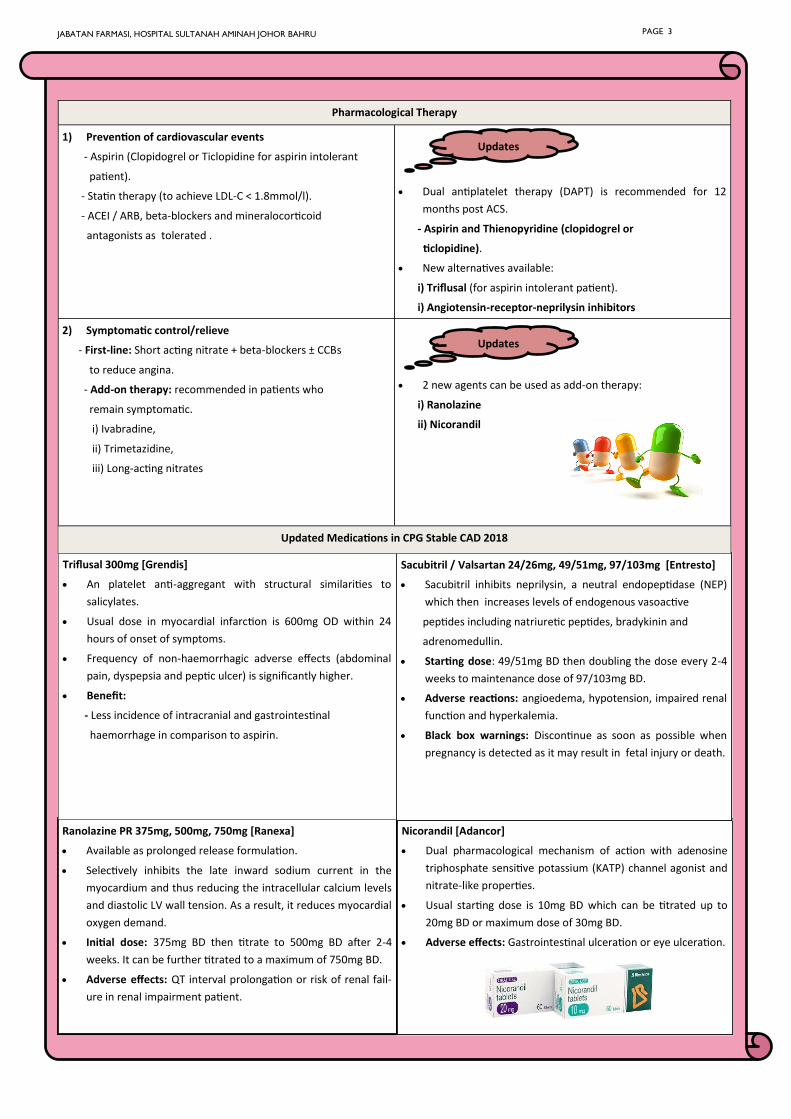
PULMONARY ARTERIAL HYPERTENSION(PAH)
PAH IN ADULTS
PAH was defined by a mean PAP (mPAP) >25mmHg at rest or >30 mmHg
with exercise.
PAH is now defined as a resting mPAP>25mmHg thereby eliminating the
diagnostic criteria associated with exercise.
The new Dana Point definition also suggests that a resting mPAP of 8 to
20mmHg should be considered as normal.
DEFINITION SYMPTOMS OF PAH
PATHOGENESIS
RISK FACTORS
UPDATES
SCREENING PAH suspicion
PAH detection ECG, CXR, Doppler echocardiography
PAH class
identification
VQ Scan, PFTs, high resolution/ spiral CT
PAH evaluation
Blood test and immunology, HIV test
6MWT
RHC with vasoreactivity
DIAGNOSIS
BY: Tan Ling Xin
JABATAN FARMASI, HOSPITAL SULTANAH AMINAH JOHOR BAHRU PAGE 4
6MWT=6-minute walk test; CT=computerized tomography,; CXR= chest X-ray; ECG=electrocardiogram; PFT=pulmonary function test; PH=pulmonary hypertension; RHC=right heart catheterisation; VQ scan=ventilation-perfusion scintigram
Doppler
echocardiography
- Patients with scleroderma.
- It is a test which very high frequency sound waves are bounced off from your heart and blood vessels. The echoes are picked up and turned into pictures to show how well the blood flow through the arteries and heart.
Genetic
testing
- Patients with more than one family member with PAH related to a mutation in Bone Morpho-genetic Protein Receptor Type II (BMPR2).
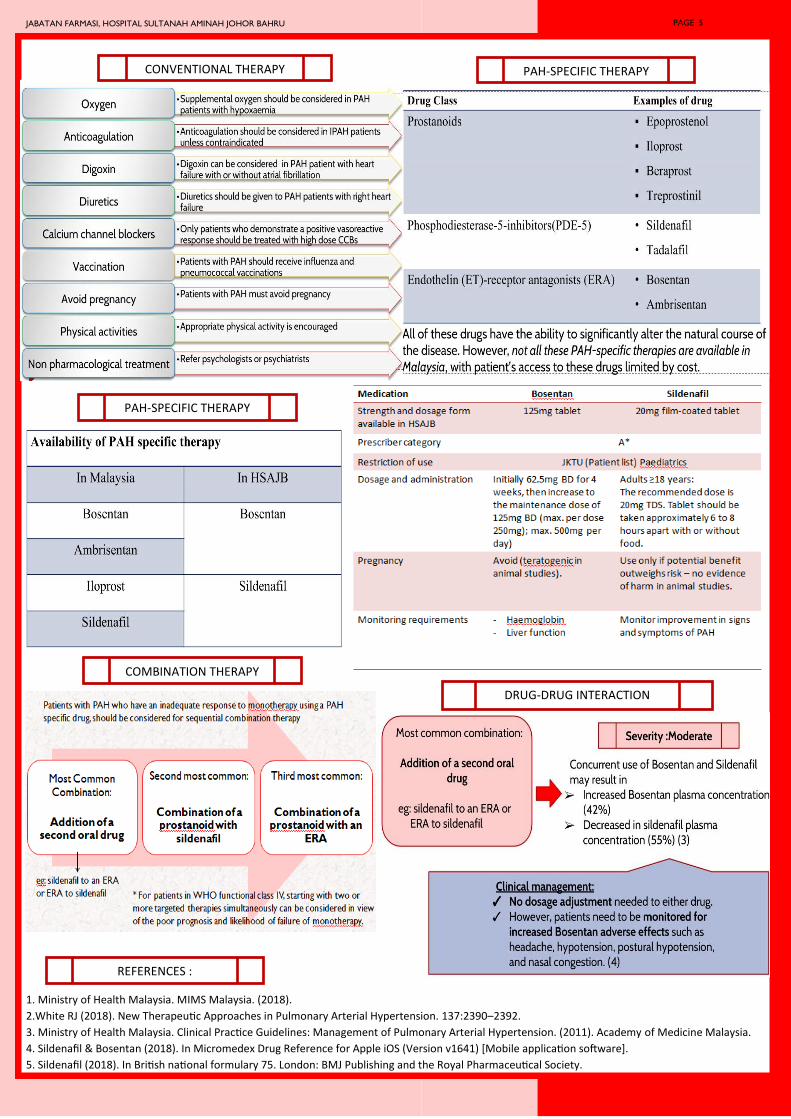
1. Ministry of Health Malaysia. MIMS Malaysia. (2018).
2.White RJ (2018). New Therapeutic Approaches in Pulmonary Arterial Hypertension. 137:2390–2392.
3. Ministry of Health Malaysia. Clinical Practice Guidelines: Management of Pulmonary Arterial Hypertension. (2011). Academy of Medicine Malaysia.
4. Sildenafil & Bosentan (2018). In Micromedex Drug Reference for Apple iOS (Version v1641) [Mobile application software].
5. Sildenafil (2018). In British national formulary 75. London: BMJ Publishing and the Royal Pharmaceutical Society.
CONVENTIONAL THERAPY PAH-SPECIFIC THERAPY
PAH-SPECIFIC THERAPY
COMBINATION THERAPY
DRUG-DRUG INTERACTION
REFERENCES :
JABATAN FARMASI, HOSPITAL SULTANAH AMINAH JOHOR BAHRU PAGE 5
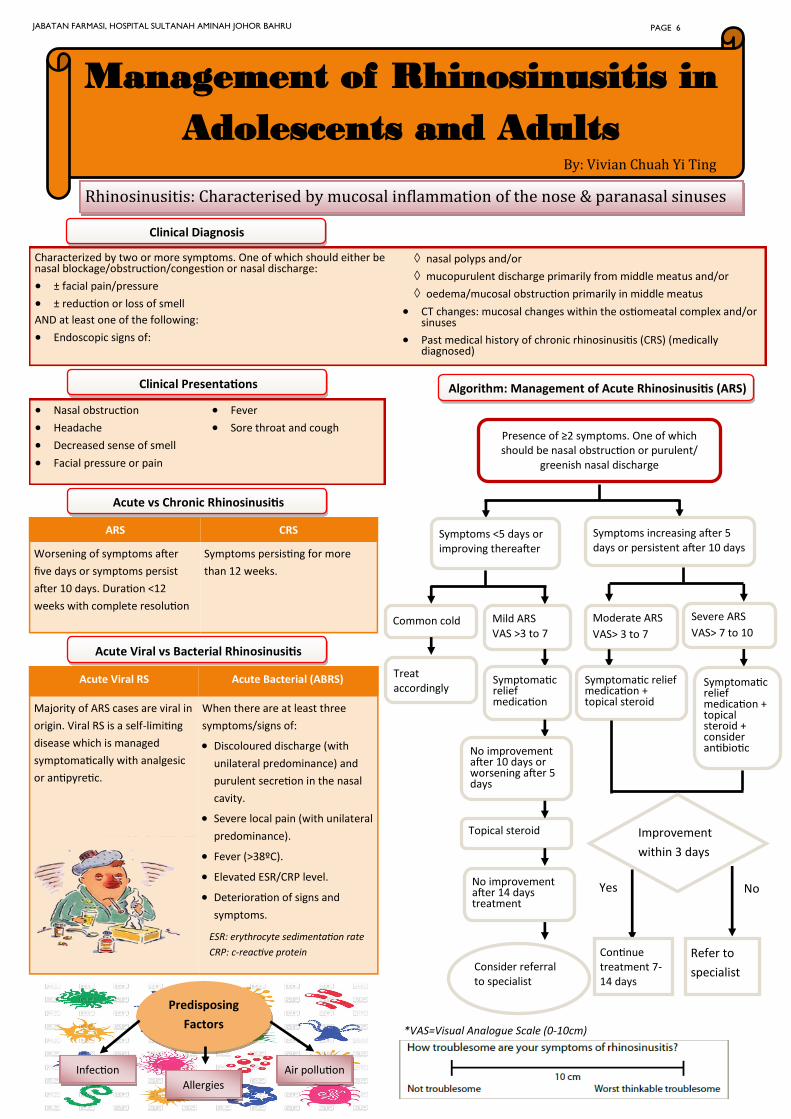
Management of Rhinosinusitis in
Adolescents and Adults By: Vivian Chuah Yi Ting
Rhinosinusitis: Characterised by mucosal inflammation of the nose & paranasal sinuses
Characterized by two or more symptoms. One of which should either be nasal blockage/obstruction/congestion or nasal discharge:
• ± facial pain/pressure
• ± reduction or loss of smell
AND at least one of the following:
• Endoscopic signs of:
nasal polyps and/or
mucopurulent discharge primarily from middle meatus and/or
oedema/mucosal obstruction primarily in middle meatus
• CT changes: mucosal changes within the ostiomeatal complex and/or sinuses
• Past medical history of chronic rhinosinusitis (CRS) (medically diagnosed)
Clinical Diagnosis
Acute vs Chronic Rhinosinusitis
ARS CRS
Worsening of symptoms after
five days or symptoms persist
after 10 days. Duration <12
weeks with complete resolution
Symptoms persisting for more
than 12 weeks.
Acute Viral vs Bacterial Rhinosinusitis
Acute Viral RS Acute Bacterial (ABRS)
Majority of ARS cases are viral in
origin. Viral RS is a self-limiting
disease which is managed
symptomatically with analgesic
or antipyretic.
When there are at least three
symptoms/signs of:
• Discoloured discharge (with
unilateral predominance) and
purulent secretion in the nasal
cavity.
• Severe local pain (with unilateral
predominance).
• Fever (>38ºC).
• Elevated ESR/CRP level.
• Deterioration of signs and
symptoms.
Algorithm: Management of Acute Rhinosinusitis (ARS)
Predisposing
Factors
Infection
Allergies
Air pollution
*VAS=Visual Analogue Scale (0-10cm)
Clinical Presentations
• Nasal obstruction
• Headache
• Decreased sense of smell
• Facial pressure or pain
• Fever
• Sore throat and cough Presence of ≥2 symptoms. One of which should be nasal obstruction or purulent/
greenish nasal discharge
Symptoms <5 days or improving thereafter
Symptoms increasing after 5 days or persistent after 10 days
Common cold
Treat accordingly
Mild ARS
VAS >3 to 7
Symptomatic relief medication
No improvement after 10 days or worsening after 5 days
Topical steroid
No improvement after 14 days treatment
Consider referral to specialist
Moderate ARS
VAS> 3 to 7
Symptomatic relief medication + topical steroid
Severe ARS
VAS> 7 to 10
Symptomatic relief medication + topical steroid + consider antibiotic
Improvement
within 3 days
Yes No
Continue treatment 7-14 days
Refer to
specialist
JABATAN FARMASI, HOSPITAL SULTANAH AMINAH JOHOR BAHRU PAGE 6
ESR: erythrocyte sedimentation rate
CRP: c-reactive protein
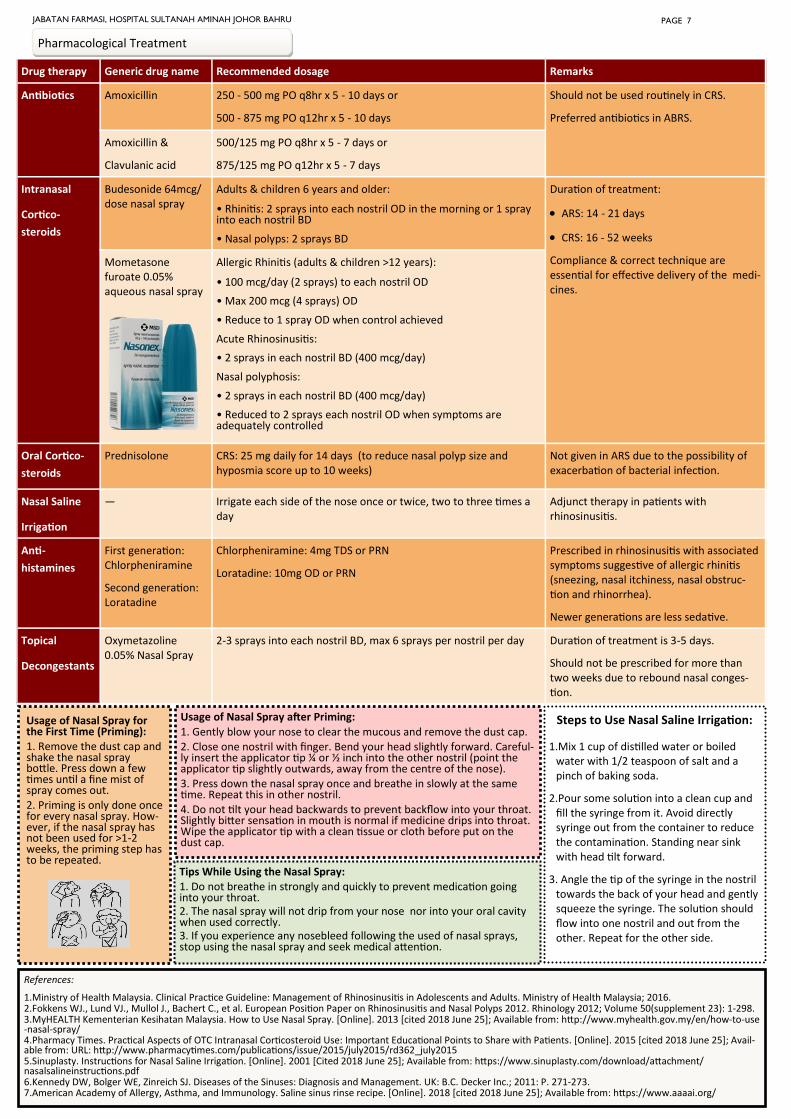
Drug therapy Generic drug name Recommended dosage Remarks
Antibiotics Amoxicillin 250 - 500 mg PO q8hr x 5 - 10 days or
500 - 875 mg PO q12hr x 5 - 10 days
Should not be used routinely in CRS.
Preferred antibiotics in ABRS.
Amoxicillin &
Clavulanic acid
500/125 mg PO q8hr x 5 - 7 days or
875/125 mg PO q12hr x 5 - 7 days
Intranasal
Cortico-
steroids
Budesonide 64mcg/ dose nasal spray
Adults & children 6 years and older:
• Rhinitis: 2 sprays into each nostril OD in the morning or 1 spray into each nostril BD
• Nasal polyps: 2 sprays BD
Duration of treatment:
• ARS: 14 - 21 days
• CRS: 16 - 52 weeks
Compliance & correct technique are essential for effective delivery of the medi-cines.
Mometasone furoate 0.05% aqueous nasal spray
Allergic Rhinitis (adults & children >12 years):
• 100 mcg/day (2 sprays) to each nostril OD
• Max 200 mcg (4 sprays) OD
• Reduce to 1 spray OD when control achieved
Acute Rhinosinusitis:
• 2 sprays in each nostril BD (400 mcg/day)
Nasal polyphosis:
• 2 sprays in each nostril BD (400 mcg/day)
• Reduced to 2 sprays each nostril OD when symptoms are adequately controlled
Oral Cortico-
steroids
Prednisolone CRS: 25 mg daily for 14 days (to reduce nasal polyp size and hyposmia score up to 10 weeks)
Not given in ARS due to the possibility of exacerbation of bacterial infection.
Nasal Saline
Irrigation
— Irrigate each side of the nose once or twice, two to three times a day
Adjunct therapy in patients with rhinosinusitis.
Anti-
histamines
First generation: Chlorpheniramine
Second generation: Loratadine
Chlorpheniramine: 4mg TDS or PRN
Loratadine: 10mg OD or PRN
Prescribed in rhinosinusitis with associated symptoms suggestive of allergic rhinitis (sneezing, nasal itchiness, nasal obstruc-tion and rhinorrhea).
Newer generations are less sedative.
Topical
Decongestants
Oxymetazoline 0.05% Nasal Spray
2-3 sprays into each nostril BD, max 6 sprays per nostril per day Duration of treatment is 3-5 days.
Should not be prescribed for more than two weeks due to rebound nasal conges-tion.
Pharmacological Treatment
References:
1.Ministry of Health Malaysia. Clinical Practice Guideline: Management of Rhinosinusitis in Adolescents and Adults. Ministry of Health Malaysia; 2016. 2.Fokkens WJ., Lund VJ., Mullol J., Bachert C., et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2012. Rhinology 2012; Volume 50(supplement 23): 1-298. 3.MyHEALTH Kementerian Kesihatan Malaysia. How to Use Nasal Spray. [Online]. 2013 [cited 2018 June 25]; Available from: http://www.myhealth.gov.my/en/how-to-use-nasal-spray/ 4.Pharmacy Times. Practical Aspects of OTC Intranasal Corticosteroid Use: Important Educational Points to Share with Patients. [Online]. 2015 [cited 2018 June 25]; Avail-able from: URL: http://www.pharmacytimes.com/publications/issue/2015/july2015/rd362_july2015 5.Sinuplasty. Instructions for Nasal Saline Irrigation. [Online]. 2001 [Cited 2018 June 25]; Available from: https://www.sinuplasty.com/download/attachment/nasalsalineinstructions.pdf 6.Kennedy DW, Bolger WE, Zinreich SJ. Diseases of the Sinuses: Diagnosis and Management. UK: B.C. Decker Inc.; 2011: P. 271-273. 7.American Academy of Allergy, Asthma, and Immunology. Saline sinus rinse recipe. [Online]. 2018 [cited 2018 June 25]; Available from: https://www.aaaai.org/
Steps to Use Nasal Saline Irrigation:
1.Mix 1 cup of distilled water or boiled water with 1/2 teaspoon of salt and a pinch of baking soda.
2.Pour some solution into a clean cup and fill the syringe from it. Avoid directly syringe out from the container to reduce the contamination. Standing near sink with head tilt forward.
3. Angle the tip of the syringe in the nostril towards the back of your head and gently squeeze the syringe. The solution should flow into one nostril and out from the other. Repeat for the other side.
JABATAN FARMASI, HOSPITAL SULTANAH AMINAH JOHOR BAHRU PAGE 7
Usage of Nasal Spray for the First Time (Priming): 1. Remove the dust cap and shake the nasal spray bottle. Press down a few times until a fine mist of spray comes out. 2. Priming is only done once for every nasal spray. How-ever, if the nasal spray has not been used for >1-2 weeks, the priming step has to be repeated.
Usage of Nasal Spray after Priming:
1. Gently blow your nose to clear the mucous and remove the dust cap. 2. Close one nostril with finger. Bend your head slightly forward. Careful-ly insert the applicator tip ¼ or ½ inch into the other nostril (point the applicator tip slightly outwards, away from the centre of the nose). 3. Press down the nasal spray once and breathe in slowly at the same time. Repeat this in other nostril. 4. Do not tilt your head backwards to prevent backflow into your throat. Slightly bitter sensation in mouth is normal if medicine drips into throat. Wipe the applicator tip with a clean tissue or cloth before put on the dust cap.
Tips While Using the Nasal Spray: 1. Do not breathe in strongly and quickly to prevent medication going into your throat. 2. The nasal spray will not drip from your nose nor into your oral cavity when used correctly. 3. If you experience any nosebleed following the used of nasal sprays, stop using the nasal spray and seek medical attention.
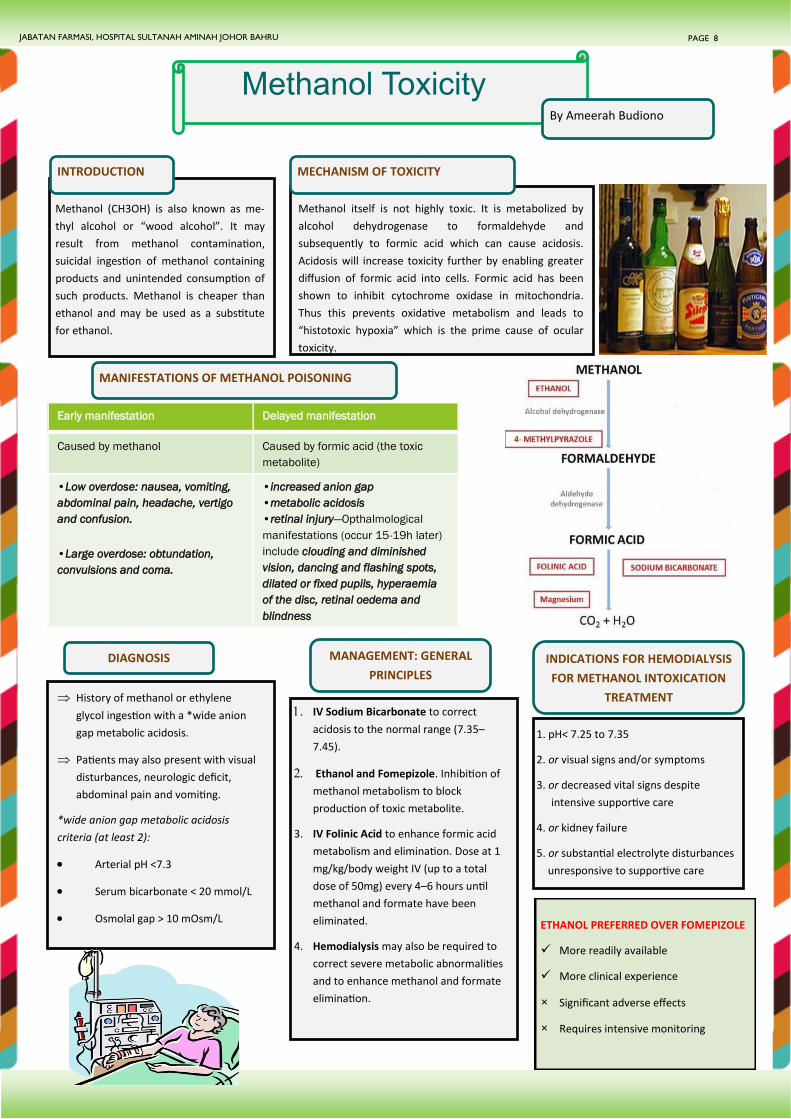
Early manifestation Delayed manifestation
Caused by methanol Caused by formic acid (the toxic
metabolite)
•Low overdose: nausea, vomiting,
abdominal pain, headache, vertigo
and confusion.
•Large overdose: obtundation,
convulsions and coma.
•increased anion gap
•metabolic acidosis
•retinal injury—Opthalmological
manifestations (occur 15-19h later)
include clouding and diminished
vision, dancing and flashing spots,
dilated or fixed pupils, hyperaemia
of the disc, retinal oedema and
blindness
ETHANOL PREFERRED OVER FOMEPIZOLE
✓ More readily available
✓ More clinical experience
× Significant adverse effects
× Requires intensive monitoring
Methanol Toxicity By Ameerah Budiono
INTRODUCTION
Methanol (CH3OH) is also known as me-
thyl alcohol or “wood alcohol”. It may
result from methanol contamination,
suicidal ingestion of methanol containing
products and unintended consumption of
such products. Methanol is cheaper than
ethanol and may be used as a substitute
for ethanol.
MECHANISM OF TOXICITY
Methanol itself is not highly toxic. It is metabolized by
alcohol dehydrogenase to formaldehyde and
subsequently to formic acid which can cause acidosis.
Acidosis will increase toxicity further by enabling greater
diffusion of formic acid into cells. Formic acid has been
shown to inhibit cytochrome oxidase in mitochondria.
Thus this prevents oxidative metabolism and leads to
“histotoxic hypoxia” which is the prime cause of ocular
toxicity.
MANIFESTATIONS OF METHANOL POISONING
DIAGNOSIS
History of methanol or ethylene
glycol ingestion with a *wide anion
gap metabolic acidosis.
Patients may also present with visual
disturbances, neurologic deficit,
abdominal pain and vomiting.
*wide anion gap metabolic acidosis
criteria (at least 2):
• Arterial pH <7.3
• Serum bicarbonate < 20 mmol/L
• Osmolal gap > 10 mOsm/L
MANAGEMENT: GENERAL
PRINCIPLES INDICATIONS FOR HEMODIALYSIS
FOR METHANOL INTOXICATION
TREATMENT
1. pH< 7.25 to 7.35
2. or visual signs and/or symptoms
3. or decreased vital signs despite
intensive supportive care
4. or kidney failure
5. or substantial electrolyte disturbances
unresponsive to supportive care
JABATAN FARMASI, HOSPITAL SULTANAH AMINAH JOHOR BAHRU PAGE 8
IV Sodium Bicarbonate to correct
acidosis to the normal range (7.35–
7.45).
Ethanol and Fomepizole. Inhibition of
methanol metabolism to block
production of toxic metabolite.
3. IV Folinic Acid to enhance formic acid
metabolism and elimination. Dose at 1
mg/kg/body weight IV (up to a total
dose of 50mg) every 4–6 hours until
methanol and formate have been
eliminated.
4. Hemodialysis may also be required to
correct severe metabolic abnormalities
and to enhance methanol and formate
elimination.

LOADING DOSE (LD) MAINTENANCE DOSE
0.8mg/kg (4ml/kg) diluted in juice
administered orally or via a nasogastric tube.
If the patient concurrently ingests ethanol,
the LD must be modified so that the blood
ethanol does not exceed 100-150mg/dL.
Non-drinker 80-130mg/kg/hr PO or via nasogastric tube.
Chronic alcoholic 150mg/kg/hr PO or via nasogastric tube.
During dialysis 250-350mg/kg/hr PO or via nasogastric tube.
ETHANOL 20% DOSING
In HSAJB, Undenatured
Ethanol 96% for Oral
Preparation is diluted to
20% for oral use.
Ethanol or fomepizole should be
administered as soon as possible after
methanol ingestion. Ethanol has
approximately 10 times greater
affinity than methanol for alcohol
dehydrogenase thus it competitively
inhibits the metabolism of methanol
to formate.
DILUTION FOR 20% ORAL
ETHANOL
Ingredients:
• Undenatured Ethanol 96% (EtOH) for oral
preparation.
• Dextrose 5% (D5%)
Procedures:
• Pour 500mL D5% in a separate container.
• Syringe out 116ml ethanol 96%.
• Mix 116ml ethanol 96% into the
container containing 500mL D5%. DURATION OF TREATMENT
Treatment should be titrated to a blood
ethanol level of 100mg/dL or patient’s
clinical condition i.e. patient starts to
show improvement without adverse
effects (if blood ethanol measurement
is not available).
Serum methanol concentration is <20
mg/dL (200 mg/L) and the patient is
asymptomatic with a normal arterial
pH.
1. Rietjens, S. J., De Lange, D. W., & Meulenbelt, J. (2014). Ethylene glycol or methanol intoxication: which antidote should be used, fomepizole or ethanol. Neth J Med, 72(2),
73-9.
2. Brent, J. (2009). Fomepizole for ethylene glycol and methanol poisoning. New England Journal of Medicine, 360(21), 2216-2223.
3. American Academy of Clinical toxicology Ad Hoc Committee on the treatment Guidelines for methanol Poisoning, Barceloux, D. G., Randall Bond, G., Krenzelok, E. P.,
Cooper, H., & Allister Vale, J. (2002). American Academy of Clinical Toxicology practice guidelines on the treatment of methanol poisoning. Journal of Toxicology: Clinical
Toxicology, 40(4), 415-446.
4. Garis Panduan Wabak Keracunan Metanol (2015), Bahagian Kawalan Penyakit, KKM.
R
E
F
E
R
E
N
C
E
S
Patient must be monitored in *ICU if IV Ethanol infusion is given due to potential adverse
effects of hypotension, tachycardia, CNS/respiratory depression, hypoglycemia,
electrolyte derangement, and gastritis.
Ethanol should be used with caution in patients:
Who have also ingested drugs that produce *CNS depression as ethanol may
enhance the depressant effect of these drugs.
Patients with hepatic disease.
Concomitant use of disulfiram, metronidazole, or chlorpropamide may cause
flushing and hypotension to occur.
History of gastrointestinal ulcers (for oral ethanol).
Avoid in pregnant patients in the first trimester due to concerns regarding the fetal
alcohol syndrome.
PRECAUTION
PAGE 9 JABATAN FARMASI, HOSPITAL SULTANAH AMINAH JOHOR BAHRU
Pameran dan ceramah KUA telah diadakan di SMK Infant Jesus Convent pada 1 November 2018.
Objektif pameran tersebut adalah untuk meningkatkan kesedaran dan pengetahuan mengenai
penggunaan ubat secara rasional di kalangan pelajar dan guru. Seramai 169 orang pelajar tingkatan 3
telah menyertai pameran tersebut.
3 orang Pegawai Farmasi dari Hospital Sultanah Aminah turut hadir untuk memberi ceramah
mengenai ubat-ubatan. Program ini diserikan lagi dengan kehadiran Pn Aynee binti Wahid, Duta
KUA . Program ini telah berjalan dengan lancar dan mendapat sambutan yang baik daripada
kalangan pelajar dan guru-guru.
PAMERAN DAN CERAMAH
KENALI UBAT ANDA (KUA)