overweight, obesity and physical inactivity guideline · overweight, obesity and physical...
TRANSCRIPT

BRITISHCOLUMBIA
MEDICALASSOCIATION
Ministry of Health
Overweight, Obesity and Physical Inactivity
Scope
The prevalence of overweight, obesity and physical inactivity has been increasing in all ages and is a major contributor to chronic diseases, including diabetes, hypertension, cardiovascular disease (CVD) and kidney disease.
Family physicians are encouraged to discuss and provide brief advice to all patients regarding the importance of a healthy active lifestyle (when an opportunity is available and appropriate). Learning new behaviour around eating and exercise is like learning a new language-it takes time (up to 4 years or more), practice, and requires ongoing support and encouragement from a hopeful, empathetic and informed care provider.
RECOMMENDATION 1 Physicians are encouraged to measure and document health indicators
Height, weight, body-mass index (BMI), waist circumference, physical activity level, and eating behaviour should be measured and documented in people of all ages, as appropriate, when they are seen by the physician for other reasons.
RECOMMENDATION 2 Determine and record body mass index (BMI), using tools attached to this guideline. (see Appendix 1, 3, 4,5,6)
Children/Youth
• Normal - BMI < 85th percentile • Overweight- BMI > 85th percentile • Obese > 95th percentile
Adults
• BMI ≥25 overweight• BMI >27 overweight and increased risk of hypertension, diabetes and CVD• BMI ≥ 30 obese, higher risk of complications
Adult Waist Circumference
Increased risk: female: ≥ 80 cm male ≥ 94 cmHigh risk: female: ≥ 88 cm male ≥ 102 cm
A rapid increase in BMI over a short period of time should prompt review of the nutritional and physical activity situation of the subject.
RECOMMENDATION 3 Activity level – determine and record Children/youth Adults
Inactive <30 min/day <30 min/day
Moderately active 30-90 min/day 30-60 min/day
Very active >90 min/day >60 min/day
Inactive: no appreciable exercise Moderately increased heart rate active: e.g.: walking. Very active: e.g.: Running, cycling, swimming lengths
2
2
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
3
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
RECOMMENDATION 4 Using the questions below, determine and record diet quality/dietary habits
1. Do you usually eat breakfast?2. Do you usually* eat 5 or more servings of fruit and vegetables/day3. Do you usually* choose whole grain products?4. Do you usually* choose low fat or reduced fat alternatives at home and when eating out?5. How many boxes, cups or cans of fruit juice or pop do you usually drink per day? What do you drink when you are thirsty? More than one “no” answer and more than one serving of sweetened beverage per day indicates the need for nutritional advice from the physician or referral to a registered dietitian or Dial-A-Dietitian (1 800 667-3438)
*indicate to the patient that “usually” means 5 or more days of the week, most weeks.
RECOMMENDATION 5 Assess factors that may infl uence weight, activity level and risk levels
1. Ask about family history of overweight, diabetes, high cholesterol, heart disease, hypertension and kidney disease
2. Consider associated health conditions:
Children/youth AdultDepression HypertensionAsthma Type 2 diabetesBeing bullied ArthritisLearning diffi culties DepressionType 2 diabetes
3. Assess social conditions
• poverty• unemployment/employment issues• education level• workplace and home stresses• current or previous abuse
4. Further diagnostic assessment should be individualized based on risk factors and family history. Extensive laboratory assessment of overweight, obese and physically inactive patients in the
absence of obvious risk factors or physical fi ndings is rarely fruitful.
RECOMMENDATION 6 Adults: Assess each individual’s readiness for change. Tailor interventions and support to their current situation (See Appendix 2)
1. Educate adults about the risks of excess weight and the benefi ts of moderate weight loss and increased activity. Reinforce the message that even modest weight loss and increased activity can confer signifi cant health benefi ts. Increases in physical activity in a stable, overweight person likely confer greater health advantages than diet in a physically inactive person.
2
2
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
3
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
2. Assess readiness to change: Ask the following questions:• Are you considering trying to lose weight or increase activity?• Are you currently trying to lose weight or increase activity?• Would you like some information to help you?
3. Help the patient who is ready to change to set realistic goals:• Emphasize gradual change in lifestyle over time• Recommend increased physical activity (e.g. walking 30 minutes/day)• Recommend some level of caloric restriction• Provide self-help materials• Praise success
See Appendix 2 for detailed explanation of stages of change
Physicians are encouraged to provide brief lifestyle advice during the management of other conditions whenever an opportunity is available and appropriate.
RECOMMENDATION 7 Children and youth-assessment and management
Assessment and management will require: • the involvement of parents or care-givers where possible and may require formal nutritional
counseling by a registered dietitian and or pediatric referral • an understanding and sensitive approach to assessment of potential eating disorders
With growing children and youth, the goals may be weight maintenance and increased activity while normal linear growth occurs.
RECOMMENDATION 8 Drugs/popular diets/surgical treatment (adults)
1. Pharmacological treatments are of limited benefi t and have frequent side effects. The long term benefi ts are unknown. There may be limited use of one agent in adolescence.2. Popular diets are becoming extremely prevalent and controversial. Evidence shows that over the long term, their effi cacy is due to caloric defi cit (energy in and out) and duration. Diets that are restrictive in particular food groups offer no long-term benefi t and impose considerable risk of micronutrient defi ciencies.3. The surgical treatment of obesity involves risks and complications. Patients should only consider surgery if their BMI is greater than 40 or if it is greater than 35 and there is a related condition such as hypertension, type 2 diabetes or cardiovascular disease.4. Very frequent “weigh-in” sessions (for example, weekly visits) have shown no long term benefi ts.
Rationale
Obesity in adults is indicated by a body-mass index (BMI) of 30 or more. About 33% of adult Canadians had a BMI greater than 25 (overweight) and 14.9% had a BMI of >30 in 20031. The Brit-ish Columbia Nutrition Survey showed that 56% of British Columbians are overweight or obese2. The prevalence of obesity in both children and adults has been increasing in BC and throughout Canada in children, adolescents and adults 2,3,4. Obesity is a major risk factor for hypertension, type 2 diabetes, dyslipidemia, gallbladder disease, cancer and cardiovascular disease 5.
Physicians and patients have requested a coherent reproducible approach to medical assistance in the management of obesity and inactivity. Recommendations for screening and intervention for obesity have recently been developed by the American College of Family Physicians5. The recommendations
4
4
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
5
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
focus on using BMI as an indicator of obesity and advice regarding weight loss, increased physical activity and the risk of more serious diseases. Efforts to reduce calorie and fat intake have been shown to cause weight loss, particularly if they are applied together with a physical exercise program.
The American Academy of Pediatrics has provided some recommendations for the prevention of pediatric overweight and obesity6 . The Canadian Pediatric Society, the College of Family Physicians, Dietitians of Canada and the Community Health Nurses Association have prepared a summary regard-ing the use of growth charts in Canadian infants and children 7. Although therapeutic options remain to be optimized, behavioural approaches that involve the child and family have demonstrated success. The recommendations suggest as a guideline that children and adolescents should be considered overweight if they are between the 85th and 95th percentiles using Centers for Disease Control (CDC) growth charts8,9. Obesity in children and youth is a BMI for age of greater than the 95th percentile. Physicians can use clinical judgment to address overweight and obesity in children and adolescents and to advise them about the benefi ts of weight loss, increased physical activity and increased risk of complications.
Recent evidence indicates that adult BMI of between 25 and 30 is not associated with increased mortality. Attempts at intervention should focus on more overweight ≥ 27 with comorbidities such as hypertension or diabetes and obese patients, particularly those with comorbidities10.
References
1. Statistics Canada Health Indicators. June 2004.2. British Columbia Ministry of Health Services. British Columbia Nutrition Survey. Report on Physical
Activity and Body Weight. March 2004. 3. Katzmaryk PT. The Canadian obesity epidemic, 1985-1998. CMAJ 2002;166:1039-1040.4. Tremblay MS and Willms JD 2000. Secular trends in the body mass index of Canadian children
CMAJ 2000;163:1429-33.5. McTigue KM, Harris R, Hemphill B et al. Screening and intervention for obesity in adults: Summary
of the evidence for the US Preventive Services Task Force. Ann Intern Med 2003;139:933-949.6. American Academy of Pediatrics. prevention of pediatric overweight and obesity.
Pediatrics 2003;112: 424-430.7. Canadian Paediatric Society. Use of growth charts for assessing and monitoring growth in
Canadian infants and children: Executive summary. Paediatr Child Health 2004;9:171-173.8. Centres for Disease Control 2005. http://www.cdc.gov/nchs/about/major/nhanes/
growthcharts/charts.htm9. Cole TJ, Bellizzi MC, Flegal KM and WH Dietz. Establishing a standard defi nition for child over-
weight and obesity worldwide: international survey. BMJ 2000;320:1-6.10. Flegal KM, Graubard BI, Williamson DF and MH Gail. Excess deaths associated with underweight,
overweight and obesity. JAMA 2005;293:1861-67.

4
4
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
5
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
SponsorsThis guideline was developed by the Guidelines and Protocols Advisory Committee, approved by the British Columbia Medical Association and adopted by the Medical Services Commission. Partial fund-ing for this guideline was provided by the Health Canada Primary Health Care Transition Fund.
Effective Date: September 1, 2005
This guideline is based on the scientifi c evidence at the time of the effective date.
The principles of the Guidelines and Protocols Advisory Committee are:
• to encourage appropriate responses to common medical situations• to recommend actions that are suffi cient and effi cient, neither excessive nor defi cient • to permit exceptions when justifi ed by clinical circumstances.
Guidelines and Protocols Advisory Committee 1515 Blanshard Street 2-3 Victoria BC V8W 3C8
Phone: (250) 952-1347 E-mail: [email protected] Fax: (250) 952-1417 Web site: www.healthservices.gov.bc.ca/msp/protoguides
G&P2005-098
6
6
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
7
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
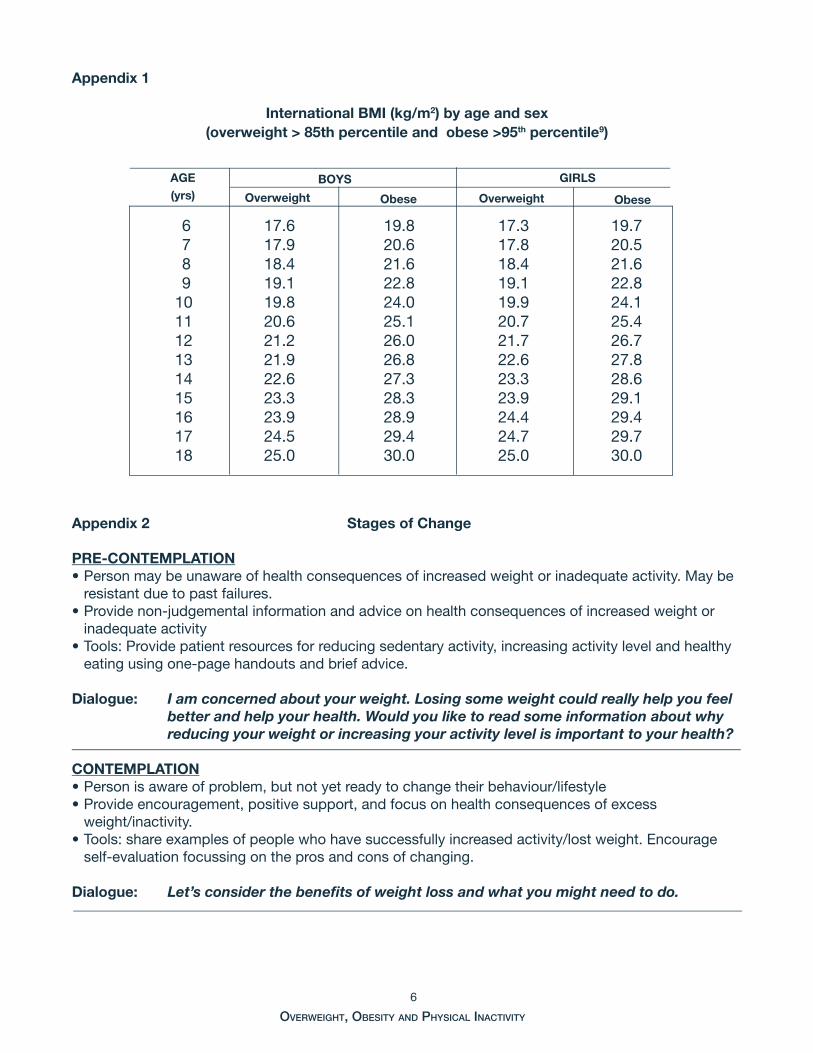
Appendix 1
International BMI (kg/m2) by age and sex (overweight > 85th percentile and obese >95th percentile9)
Appendix 2 Stages of Change
PRE-CONTEMPLATION• Person may be unaware of health consequences of increased weight or inadequate activity. May be
resistant due to past failures.• Provide non-judgemental information and advice on health consequences of increased weight or
inadequate activity• Tools: Provide patient resources for reducing sedentary activity, increasing activity level and healthy
eating using one-page handouts and brief advice.
Dialogue: I am concerned about your weight. Losing some weight could really help you feel better and help your health. Would you like to read some information about why reducing your weight or increasing your activity level is important to your health?
CONTEMPLATION• Person is aware of problem, but not yet ready to change their behaviour/lifestyle• Provide encouragement, positive support, and focus on health consequences of excess weight/inactivity. • Tools: share examples of people who have successfully increased activity/lost weight. Encourage
self-evaluation focussing on the pros and cons of changing.
Dialogue: Let’s consider the benefi ts of weight loss and what you might need to do.
6 17.6 19.8 17.3 19.7 7 17.9 20.6 17.8 20.5 8 18.4 21.6 18.4 21.6 9 19.1 22.8 19.1 22.810 19.8 24.0 19.9 24.111 20.6 25.1 20.7 25.412 21.2 26.0 21.7 26.713 21.9 26.8 22.6 27.814 22.6 27.3 23.3 28.615 23.3 28.3 23.9 29.116 23.9 28.9 24.4 29.417 24.5 29.4 24.7 29.718 25.0 30.0 25.0 30.0
BOYS GIRLS
Overweight Obese Overweight Obese
AGE (yrs)
6
6
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
7
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
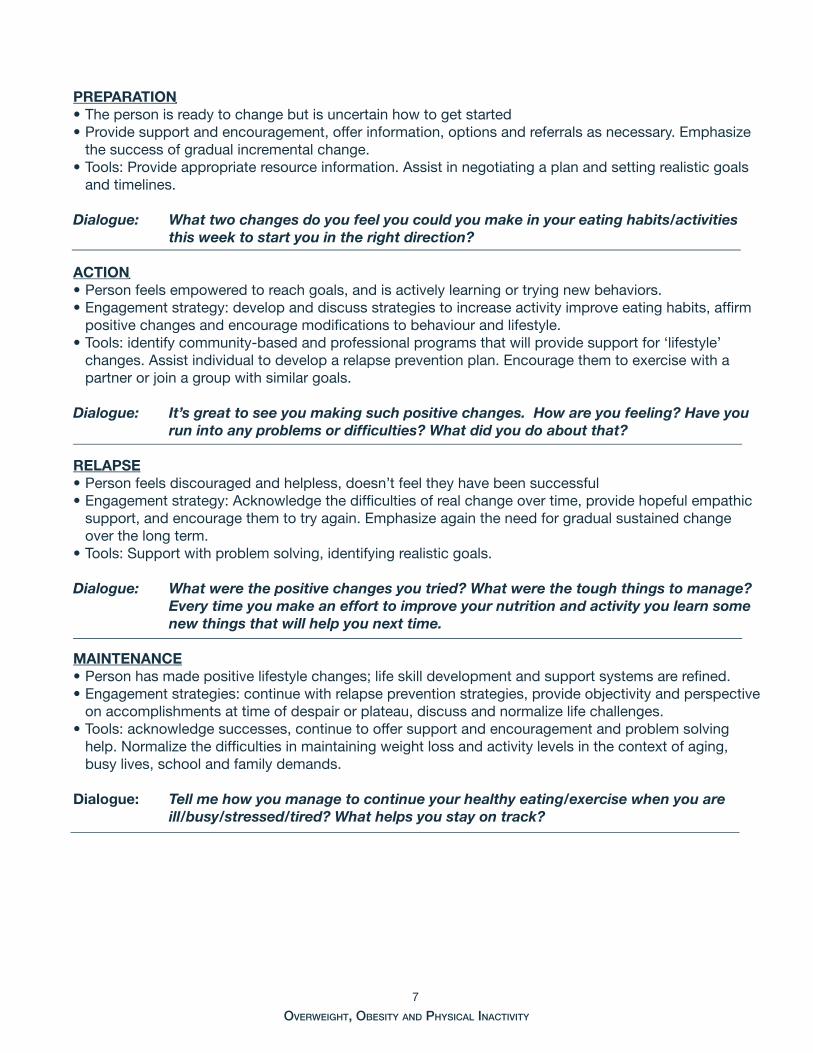
PREPARATION• The person is ready to change but is uncertain how to get started • Provide support and encouragement, offer information, options and referrals as necessary. Emphasize
the success of gradual incremental change.• Tools: Provide appropriate resource information. Assist in negotiating a plan and setting realistic goals
and timelines.
Dialogue: What two changes do you feel you could you make in your eating habits/activities this week to start you in the right direction?
ACTION• Person feels empowered to reach goals, and is actively learning or trying new behaviors.• Engagement strategy: develop and discuss strategies to increase activity improve eating habits, affi rm
positive changes and encourage modifi cations to behaviour and lifestyle. • Tools: identify community-based and professional programs that will provide support for ‘lifestyle’
changes. Assist individual to develop a relapse prevention plan. Encourage them to exercise with a partner or join a group with similar goals.
Dialogue: It’s great to see you making such positive changes. How are you feeling? Have you run into any problems or diffi culties? What did you do about that?
RELAPSE• Person feels discouraged and helpless, doesn’t feel they have been successful • Engagement strategy: Acknowledge the diffi culties of real change over time, provide hopeful empathic
support, and encourage them to try again. Emphasize again the need for gradual sustained change over the long term.
• Tools: Support with problem solving, identifying realistic goals.
Dialogue: What were the positive changes you tried? What were the tough things to manage? Every time you make an effort to improve your nutrition and activity you learn some new things that will help you next time.
MAINTENANCE• Person has made positive lifestyle changes; life skill development and support systems are refi ned. • Engagement strategies: continue with relapse prevention strategies, provide objectivity and perspective
on accomplishments at time of despair or plateau, discuss and normalize life challenges. • Tools: acknowledge successes, continue to offer support and encouragement and problem solving
help. Normalize the diffi culties in maintaining weight loss and activity levels in the context of aging, busy lives, school and family demands.
Dialogue: Tell me how you manage to continue your healthy eating/exercise when you are ill/busy/stressed/tired? What helps you stay on track?

8
8
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
9
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
152
155
157
160
163
165
168
170
173
175
178
180
183
185
188
191
193
Kg Lbs
Heig
ht(c
m)
Heig
ht(ft
/in)
Wei
ght
5’0”
5’1”
5’2”
5’3”
5’4”
5’5”
5’6”
5’7”
5’8”
5’9”
5’10
”5’
11”
6’0”
1414
1516
1617
1818
1920
2021
2222
2324
2425
2626
2728
2829
30
6’1”
1314
1515
1616
1718
1819
2020
2122
2223
24 2
425
2626
27
2828
29
6’2”
1313
1415
1516
1717
1819
1920
2121
2222
2324
24
2526
2627
28
28
6’3”
1213
1414
1516
1617
1718
1919
2021
2122
2223
24
24
2526
2627
27
6’4”
1213
1314
1515
1616
1718
1819
1920
2121
2223
2324
2425
26 2
627
BMI <
18
= u
nder
wei
ght
18
.5 to
24
= h
ealth
y w
eigh
t
≥25
= o
verw
eigh
t
≥ 27
= in
crea
sing
risk
of h
yper
tens
ion,
type
2 d
iabe
tes
≥ 3
0 ob
ese
1920
2122
23
2425
2627
2829
3031
3233
34
35
36
3
7
38
39
40
4
1
42
43
1819
2021
22
2324
2526
2727
2829
3031
3233
3334
3637
3839
4042
1819
1920
21
2223
2425
2627
2728
2930
3132
3334
3535
3637
3839
1718
1920
21
2122
2324
2526
2727
2829
3031
3233
3334
3536
3738
1717
1819
20
2122
2223
2425
2627
2728
2930
3132
3233
3435
3637
1617
1819
19
2021
2223
2324
2526
2727
2829
3132
3233
3435
3637
1616
1718
19
2020
2122
2323
2425
2627
2728
2930
3131
3233
3434
1516
17
17 1
819
2021
2122
2324
2425
2627
2728
2930
3031
3233
3315
1616
17
1818
1920
2121
2223
2424
2526
2727
2829
3030
3132
3214
15
1617
17
1819
1920
2122
2223
2424
2526
2727
2829
2930
3132
14 1
515
16
1717
1819
2020
2122
2223
2424
2526
2627
2829
2930
31
100
105
110
115
12
012
513
013
514
014
515
015
516
016
5
170
1
7518
0
185
1
90
195
2
00
205
2
10
21
5
220
Bo
dy
Mas
s In
dex
(BM
I) C
hart
1920
21
22
2
324
2526
2627
2829
3031
3232
34
3
5
36
3738
39
40
41
42
45
48
5052
55
5759
6164
6668
7073
75
77
8082
84
8
6
89
91
93
95
98
1
00
Appendix 3
Not
e: C
onsi
der
mus
cle
mas
s w
hen
eval
uatin
g B
MI
(Ad
ults
)
8
8
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
9
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
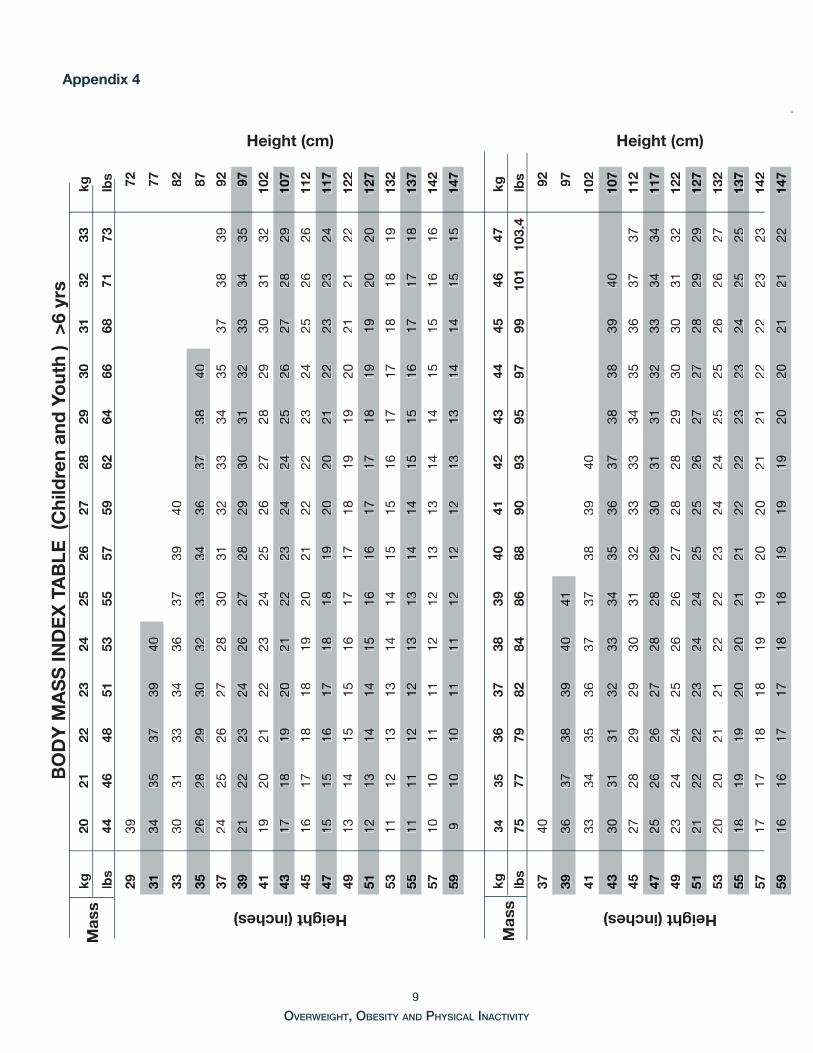
Appendix 4B
OD
Y M
AS
S IN
DE
X T
AB
LE (
Chi
ldre
n an
d Y
out
h )
>6
yrs
kg20
2122
2324
2526
2728
2930
3132
33
kg
lbs
4446
4851
5355
5759
6264
6668
7173
lb
s
Height (inches)29
3972
Height (cm)31
3435
3739
4077
3330
3133
3436
3739
4082
3526
2829
3032
3334
3637
3840
87
3724
2526
2728
3031
3233
3435
3738
3992
3921
2223
2426
2728
2930
3132
3334
3597
4119
2021
2223
2425
2627
2829
3031
3210
2
4317
1819
2021
2223
2424
2526
2728
2910
7
4516
1718
1819
2021
2222
2324
2526
2611
2
4715
1516
1718
1819
2020
2122
2323
2411
7
4913
1415
1516
1717
1819
1920
2121
2212
2
5112
1314
1415
1616
1717
1819
1920
2012
7
5311
1213
1314
1415
1516
1717
1818
1913
2
5511
1112
1213
1314
1415
1516
1717
1813
7
5710
1011
1112
1213
1314
1415
1516
1614
2
599
1010
1111
1212
1213
1314
1415
1514
7
Mas
skg
3435
3637
3839
4041
4243
4445
4647
k
g
lbs
7577
7982
8486
8890
9395
9799
101
103.
4
lbs
Height (inches)
3740
92
Height (cm)
3936
3738
3940
4197
4133
3435
3637
3738
3940
102
4330
3131
3233
3435
3637
3838
3940
107
4527
2829
2930
3132
3333
3435
3637
3711
2
4725
2626
2728
2829
3031
3132
3334
3411
7
4923
2424
2526
2627
2828
2930
3031
3212
2
5121
2222
2324
2425
2526
2727
2829
2912
7
5320
2021
2122
2223
2424
2525
2626
2713
2
5518
1919
2020
2121
2222
2323
2425
2513
7
5717
1718
1819
1920
2021
2122
2223
2314
2
5916
1617
1718
1819
1919
2020
2121
2214
7
Mas
s
10
10
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
11
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
� ��� � � � � �� �� �� �� �� �� �� �� �� �� ��
��
��
��
��
��
��
��
��
�����
��
��
��
��
��
��
��
��
��
�����
��
��
��
���
���
��� �������
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
�
��
� �� �� ������ ����
���� ���� ������������� ���������������
������ �
������� ��������� �
�������
� ��� �������� ������ ��� ������ ���������� �� ������������� ����
��� �������� ������ ��� ������� ������� ���������� ��� ������ ���������
�������������������������������
���� ��� ������ ������� ���� ��������
��������� ��� ��� ���� ��������� ����������
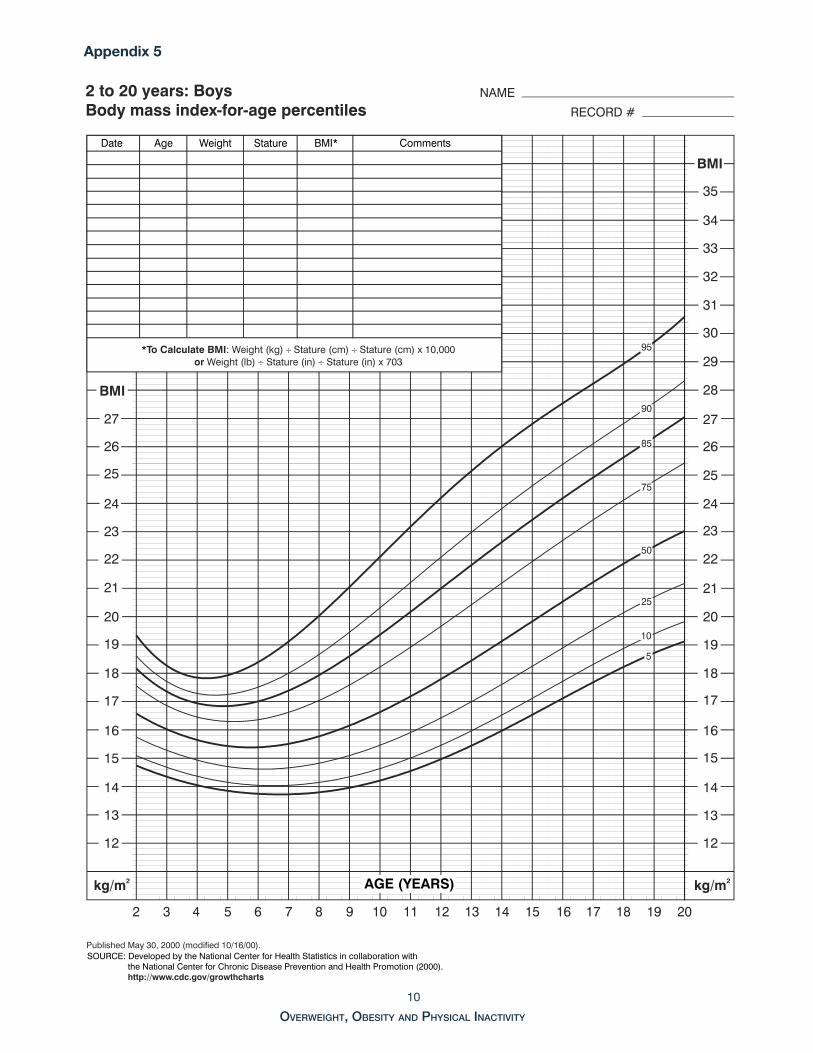
Appendix 5
10
10
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
11
OVERWEIGHT, OBESITY AND PHYSICAL INACTIVITY
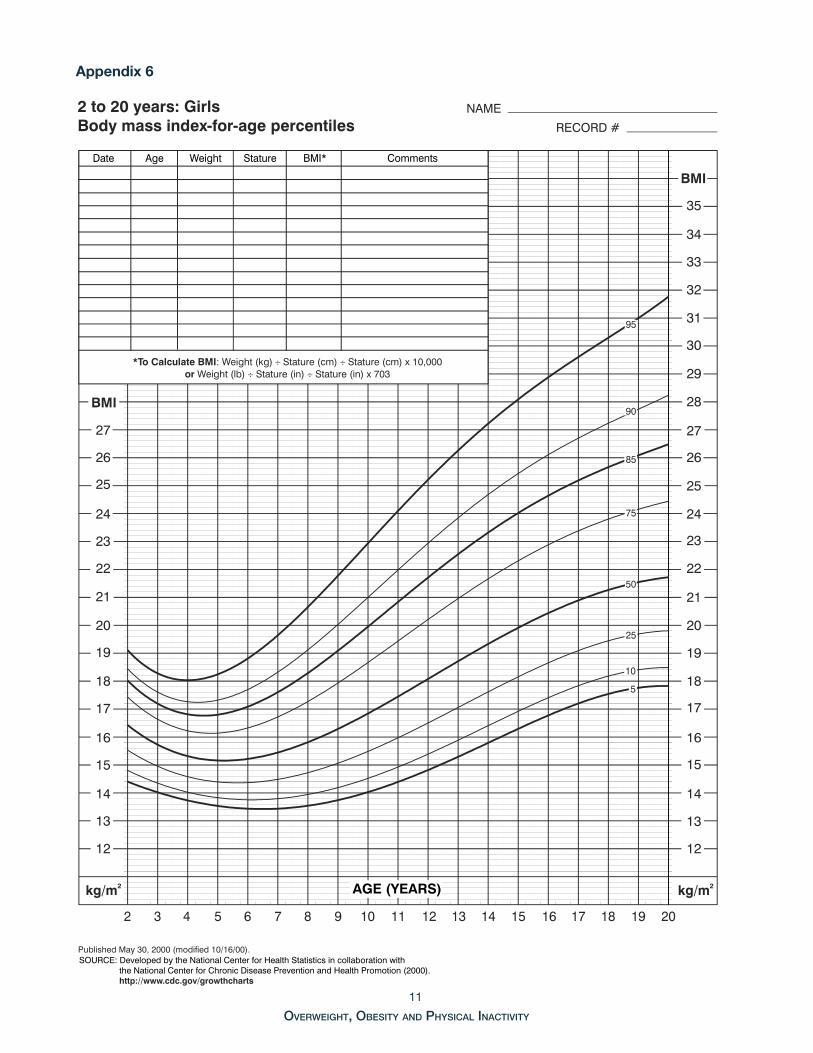
Appendix 6
� �� �� ������ �����
���� ���� ������������� ���������������
������ �
������� ��������� �
�������
� ��� �������� ������ ��� ������ ���������� �� ������������� ����
��� �������� ������ ��� ������� ������� ���������� ��� ������ ���������
�������������������������������
� ��� � � � � �� �� �� �� �� �� �� �� �� �� ��
��
��
��
��
��
��
��
��
�����
��
��
��
��
��
��
��
��
��
�����
��
��
��
���
���
��� �������
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
���� ��� ������ ������� ���� ��������
��
��
��
��
��
��
��
�
��������� ��� ��� ���� ��������� ����������
Healthy Active LivingA GUIDE FOR PATIENTS
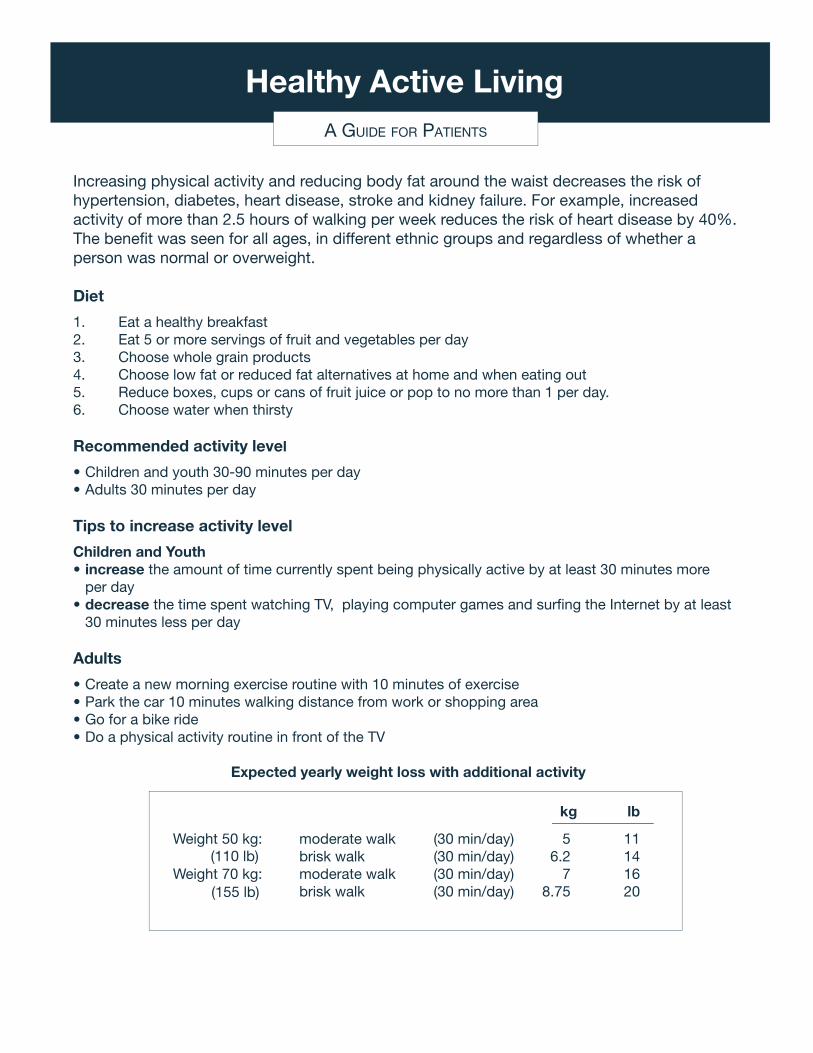
Increasing physical activity and reducing body fat around the waist decreases the risk of hypertension, diabetes, heart disease, stroke and kidney failure. For example, increased activity of more than 2.5 hours of walking per week reduces the risk of heart disease by 40%. The benefi t was seen for all ages, in different ethnic groups and regardless of whether a person was normal or overweight.
Diet
1. Eat a healthy breakfast2. Eat 5 or more servings of fruit and vegetables per day3. Choose whole grain products4. Choose low fat or reduced fat alternatives at home and when eating out5. Reduce boxes, cups or cans of fruit juice or pop to no more than 1 per day.6. Choose water when thirsty
Recommended activity level
• Children and youth 30-90 minutes per day• Adults 30 minutes per day
Tips to increase activity level
Children and Youth• increase the amount of time currently spent being physically active by at least 30 minutes more per day • decrease the time spent watching TV, playing computer games and surfi ng the Internet by at least 30 minutes less per day
Adults
• Create a new morning exercise routine with 10 minutes of exercise• Park the car 10 minutes walking distance from work or shopping area• Go for a bike ride• Do a physical activity routine in front of the TV
Expected yearly weight loss with additional activity
kg lb
Weight 50 kg: moderate walk (30 min/day) 5 11 brisk walk (30 min/day) 6.2 14
Weight 70 kg: moderate walk (30 min/day) 7 16 brisk walk (30 min/day) 8.75 20
(110 lb)
(155 lb)
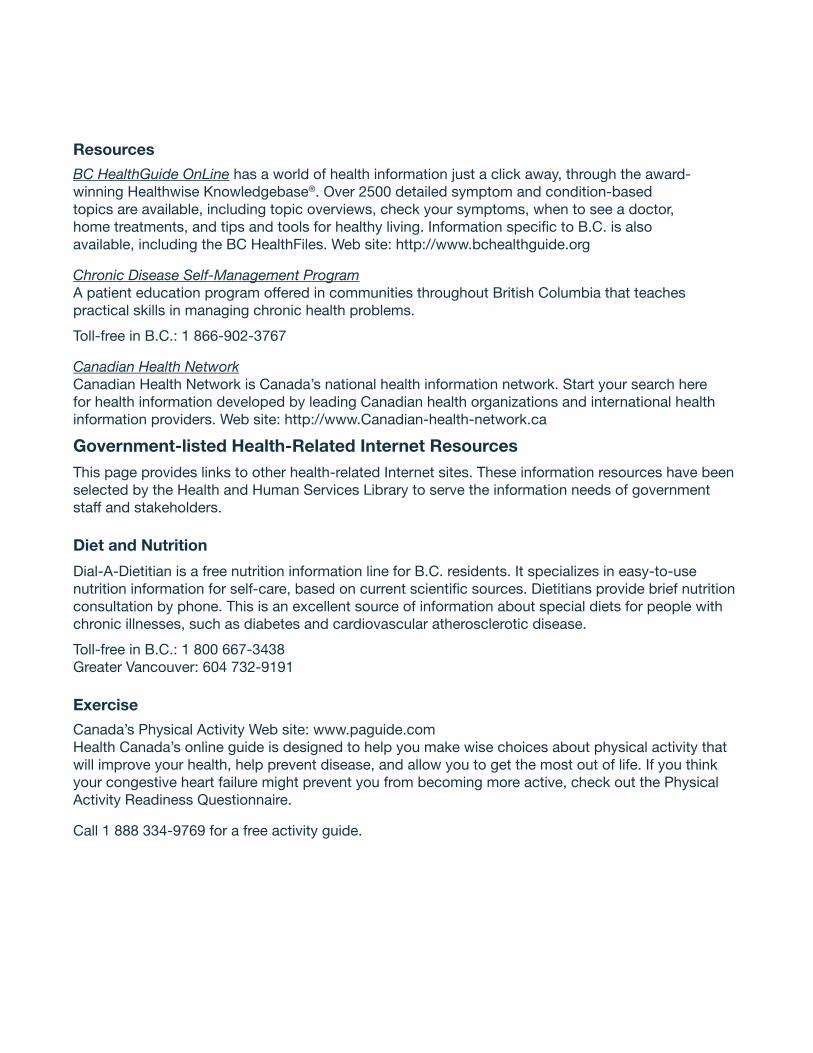
Resources
BC HealthGuide OnLine has a world of health information just a click away, through the award-winning Healthwise Knowledgebase®. Over 2500 detailed symptom and condition-based topics are available, including topic overviews, check your symptoms, when to see a doctor, home treatments, and tips and tools for healthy living. Information specifi c to B.C. is also available, including the BC HealthFiles. Web site: http://www.bchealthguide.org
Chronic Disease Self-Management ProgramA patient education program offered in communities throughout British Columbia that teaches practical skills in managing chronic health problems.
Toll-free in B.C.: 1 866-902-3767
Canadian Health NetworkCanadian Health Network is Canada’s national health information network. Start your search here for health information developed by leading Canadian health organizations and international health information providers. Web site: http://www.Canadian-health-network.ca
Government-listed Health-Related Internet ResourcesThis page provides links to other health-related Internet sites. These information resources have been selected by the Health and Human Services Library to serve the information needs of government staff and stakeholders.
Diet and Nutrition
Dial-A-Dietitian is a free nutrition information line for B.C. residents. It specializes in easy-to-use nutrition information for self-care, based on current scientifi c sources. Dietitians provide brief nutrition consultation by phone. This is an excellent source of information about special diets for people with chronic illnesses, such as diabetes and cardiovascular atherosclerotic disease.
Toll-free in B.C.: 1 800 667-3438Greater Vancouver: 604 732-9191
Exercise
Canada’s Physical Activity Web site: www.paguide.comHealth Canada’s online guide is designed to help you make wise choices about physical activity that will improve your health, help prevent disease, and allow you to get the most out of life. If you think your congestive heart failure might prevent you from becoming more active, check out the Physical Activity Readiness Questionnaire.
Call 1 888 334-9769 for a free activity guide.