orthopaedic surgery - · pdf file24 complex case: pelvic osteosarcoma 26 academic activities...
TRANSCRIPT
NYU LANGONE MEDICAL CENTER 550 First Avenue, New York, NY 10016
NYULANGONE.ORG
Orthopaedic Surgery
LARGESTRESIDENCY PROGRAM
IN THE COUNTRY
TOP 5IN U.S. NEWS &
WORLD REPORT
REDEFININGQUALITY AND
PATIENT SAFETY
2016 / YEAR IN REVIEW

1 MESSAGE FROM THE CHAIR
2 FACTS & FIGURES
4 NEW & NOTEWORTHY
8 CLINICAL CARE & RESEARCH
9 Personalized Approach to Joint Replacement
11 Ultra-Low Dose CT Reduces Risk
13 Complex Case: Scheuermann’s Kyphosis
14 Regenerative Medicine
16 New Momentum For Wide-Awake Hand Surgery
18 Robot and Computer-Assisted Surgery
20 Quality and Safety Initiatives
22 Bone and Cartilage Regeneration Research
24 Complex Case: Pelvic Osteosarcoma
26 ACADEMIC ACTIVITIES
34 LOCATIONS
36 FACULTY & LEADERSHIP
Contents
Produced by the Office of Communications and Marketing,NYU Langone Medical Center Photography: Karsten Moran Writer: Bryn Nelson Creative Direction: Ideas on Purpose, www.ideasonpurpose.com Design: Craig Williams, www.thecraigwilliams.com
On the cover: Human bone, osteoporosis
Message from the Chair
ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 1
JOSEPH D. ZUCKERMAN, MD
Walter A.L. Thompson Professor of Orthopaedic Surgery
Chair, Department of Orthopaedic Surgery
Dear Colleagues and Friends:
From simple to complex cases, NYU Langone Medical Center’s Department of Orthopaedic Surgery aims to provide each patient we see with the very best in individualized care.
In 2016, I’m proud to report considerable headway toward that goal with exciting growth in our educational, clinical, and research capabilities. Among the most significant steps forward, the five-year Orthopaedic Surgery Residency Program’s expansion to 70 residents now makes this program—one of the country’s most diverse—the largest of its kind. Likewise, we expanded the department’s fellowship program to include 21 post-graduate clinical fellows. As you’ll read in the pages of this update, our highly skilled surgeons continue to blaze new trails and solve complex cases in collaboration with Neurosurgery, Plastic Surgery, and other departments. An exciting partnership with the Department of Radiology has demonstrated the mettle of low-dose CT scans in diagnosing joint fractures, and we’ve presented promising results on using shockwave therapy to treat refractory tendinitis. Meanwhile, our bench-to-bedside approach is embodied in several additional clinical care advances. We’re among the first medical centers in the United States to provide dedicated space and resources for wide-awake hand surgery, and we’ve expanded our same-day joint replacement options to include hip, knee, and shoulder arthroplasty. After leading the way in robotic and sensor-assisted partial knee and total hip replacements, our expanded suite of surgical options now includes total knee replacements. In the Joint Preservation and Arthritis Center, an impressive roster of personalized options, including less-invasive surgical alternatives, help patients retain their joints for as long as possible. Our synovial fluid repository and new Joint Preservation Registry II also are providing a rich vein of potential biomarkers that may help us measure osteoarthritis risk, disease progression, and therapeutic response. Finally, our vibrant research portfolio continues to pay big dividends. Multiple collaborative projects are pointing the way toward promising bone and cartilage regeneration options that may help patients recover from fractures, joint injuries, and other tissue-damaging conditions more quickly. The new Center for Regenerative Medicine is rigorously testing the merits of injectable biologics, such as stem cells derived from platelet-rich plasma to delay, or even avoid, the need for knee replacement surgery. Our safety and quality research projects are suggesting how to improve patient outcomes while boosting efficiency—complementary goals as medicine moves toward bundled payments. We are clarifying how to reduce the danger of pre- and post-surgical risk factors, using simulations to improve how surgeons communicate with patients, and sharing information with other medical centers to help reduce care disparities. Some of our studies are underscoring how simple changes might significantly influence the operating room turnover time for hand surgery, enable discharges to patients’ own homes, and enhance tissue repair after shoulder surgery. Together, these insights will enable us to allocate our resources where they can do the most good. With this flurry of activity, we are laying the groundwork for an ever-stronger push toward innovative explorations at the bench, interventions at the bedside, and improvements in the daily lives of our patients.

2 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
797SHOULDER AND ELBOW
2,269SPINE
4,343SPORTS
797TRAUMA
142TUMOR
Patient Volume: By Division
5,775ADULT RECONSTRUCTIVE
2,711HAND
709FOOT AND ANKLE
523PEDIATRICS
2,269SPINE
Department of Orthopaedic Surgery
Faculty and Students
Patient Volume: Top Procedures
227FACULTY
21FELLOWS
61RESIDENTS
1,901TOTAL HIP REPLACEMENTS
1,725TOTAL KNEE REPLACEMENTS
4,263KNEE ARTHROSCOPIES
Facts & Figures
TOP 5in the country for orthopedics in U.S. News & World Report’s “Best Hospitals” for four consecutive years.
Numbers represent FY16 (Sept 2015–Aug 2016)
ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 3
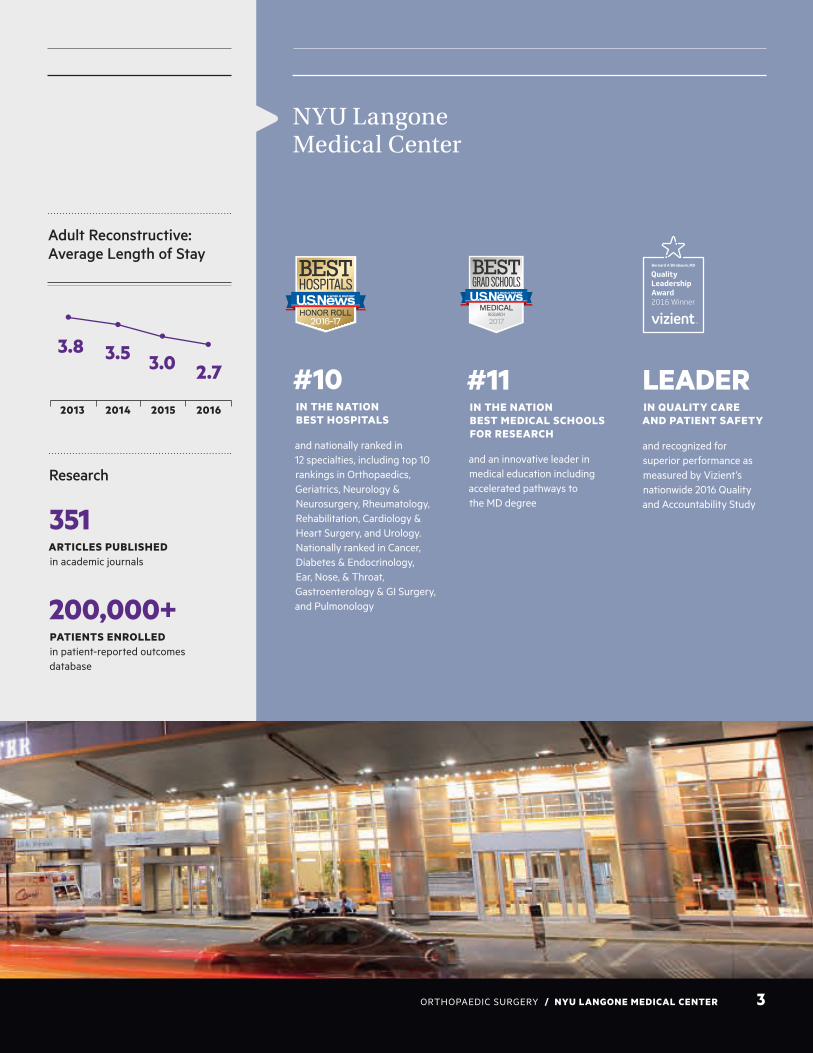
NYU Langone Medical Center
#10IN THE NATION BEST HOSPITALS
and nationally ranked in 12 specialties, including top 10 rankings in Orthopaedics, Geriatrics, Neurology & Neurosurgery, Rheumatology, Rehabilitation, Cardiology & Heart Surgery, and Urology. Nationally ranked in Cancer, Diabetes & Endocrinology, Ear, Nose, & Throat, Gastroenterology & GI Surgery, and Pulmonology
#11IN THE NATION BEST MEDICAL SCHOOLS FOR RESEARCH
and an innovative leader in medical education including accelerated pathways to the MD degree
LEADERIN QUALITY CARE AND PATIENT SAFETY
and recognized for superior performance as measured by Vizient’s nationwide 2016 Quality and Accountability Study
351ARTICLES PUBLISHED in academic journals
200,000+PATIENTS ENROLLED in patient-reported outcomes database
Research
3.8 3.5 3.0 2.7
2013 2014 2015 2016
Adult Reconstructive: Average Length of Stay

4 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
New & Noteworthy
Assessing the Impacts of Intra-Wound Antibiotics and Antiseptics on Wound and Tissue Healing
The application of intra-wound antibiotics and dilute antiseptics in the surgical wound is emerging as a clinical practice that may decrease the postoperative infection rate.
“The efficacy of these strategies has been shown clinically in nonrandomized clinical studies,” says Mandeep S. Virk, MD, assistant professor of orthopaedic surgery. “However, the effect of these agents on host cells
participating in tissue repair is not known. It’s possible that these agents might have a toxic effect on cells participating in tissue healing—including bone, tendon, ligament, and skin.” To help understand the potential effects of intra-wound application of these antibiotics and antimicrobial agents on the host cells, Dr. Virk and colleagues are studying the process in vitro. The researchers apply
different concentrations of antibiotic and antiseptic solutions to fibroblast, myoblast, and osteoblast, assessing the impact on proliferation, migration, and survival of these cells. “Our hope is to pick up a concentration that would be least toxic to host cells, but would still be efficacious against the bacteria,” says Dr. Virk.
A Year of Expansion in Education and Training
LARGEST RESIDENCY IN THE NATION.The department’s educational and training programs experienced notable growth in 2016. Among the highlights: The ACGME recognized the history of excellence in the Orthopaedic Surgery Residency Program by allowing it to expand from 60 to 70 residents per year. The five-year program, already highly ranked in the nation, is now also the largest with 14 residents accepted every year.
NEW FELLOWSHIPS IN HAND SURGERY AND ARTHROPLASTY. With expansions in hand surgery and arthroplasty, the department broadened its fellowship programs to include 20 postgraduate clinical fellows across six divisions. As leaders in educational innovation, the residency and fellowship programs both continued their novel use of direct observation to evaluate the clinical skills of trainees.
HEALTH POLICY CERTIFICATE FOR RESIDENTS. In 2016, the department also established a unique one-year certificate program with the Robert F. Wagner Graduate School of Public Service that allows one resident per year to receive a health policy
certificate. Based on coursework and involvement in both state and national health lobbying organizations, the certificate program offers special training in leadership and policy development—skills increasingly in demand among orthopaedic surgeons.
Transformation through Growth and Innovation
Orthopaedic Surgery residents

ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 5
New Shockwave Therapy Unit Takes Aim at Intractable Tendinitis
Shockwave therapy has long been used as an effective treatment to fragment kidney stones and gallstones. Over the past few years, evidence has mounted that the therapy’s directed pulses of mechanical energy also can help treat chronic tendinopathy cases that haven’t responded well to other therapeutic options. The therapy is showing early promise in treating patients with refractory tendinitis since debuting at NYU Langone in September 2016. “It’s a safe intervention with the potential for excellent results,” says Dennis A. Cardone, DO, associate professor of orthopaedic
surgery and chief of Primary Care Sports Medicine. The division’s new shockwave therapy unit is still a relative rarity at academic medical centers in the United States. With its arrival, however, Dr. Cardone says the cutting-edge technique will help him and his colleagues initiate new studies, collect valuable long-term data, and potentially expand its use to treat a range of painful conditions, including rotator cuff and hamstring injuries, frozen shoulder, Achilles tendinitis, calcific tendinopathy, and plantar fasciitis. Insufficient blood flow, Dr. Cardone says,
may be a major reason why some chronic tendinopathies are extremely difficult to heal. Although the physiological mechanisms underlying shockwave therapy aren’t fully understood, studies have suggested that its success may stem from its ability to promote revascularization of the affected tendons. Patients at NYU Langone typically receive the treatment once a week for three weeks. Data on long-term outcomes are still pending; in the interim, however, Dr. Cardone is encouraged by early signs that the repeated treatments are bringing enduring relief.
Dennis Cardone, DO

6 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
New & Noteworthy
Improving Outcomes and Efficiency Through Better Blood Management
As part of an institution-wide initiative, NYU Langone’s Value-Based Management team partnered with the Department of Orthopaedic Surgery to reduce the high rate of blood transfusions performed beyond the scope of medical indications. Unnecessary or inappropriate blood transfusions have been associated with higher inpatient mortality and excess costs. Thanks to a rigorous effort to change practice, faculty members increased the percentage of blood transfusion orders that complied with national guidelines from 57 percent to more than 90 percent throughout the institution, and the Department of Orthopaedic Surgery improved more than any other department. “We’re still doing well after the initial push. That’s the real test of any major change like this,” says Claudette M. Lajam, MD,
assistant professor of orthopaedic surgery, and departmental representative for the Medical Center-wide initiative. From national guidelines based on hemoglobin concentration and other medical factors, the team, led by hospitalist Frank M. Volpicelli, MD, assistant professor of medicine, constructed a dashboard that linked each transfusion indication with the associated blood counts, and helped surgeons compare their progress to that of their peers. A computerized order entry system also helped the doctors think about a transfusion’s necessity while avoiding “alarm fatigue.” The success also relied on regular communications with the physicians and reinforcement of positive trends to help them change their habits. A similar approach has helped reduce the unnecessary use of cell saver machines to
salvage a patient’s blood during surgery. After reviewing the frequency of use and examining the outcomes, the department adopted new guidelines about when the technique should and shouldn’t be used.
“We’ve brought our wasteful cell saver usage nearly down to zero,” Dr. Lajam says. A third project, led by James D. Slover, MD, associate professor of orthopaedic surgery, has assessed the preoperative use of tranexamic acid, or TXA, to prevent major bleeding associated with hip and knee arthroplasty. For institutions with baseline transfusion rates below 25 percent, the research suggested that TXA is not cost-effective. The potential for savings, however, increases above the 25 percent threshold due to TXA’s rising potential to help reduce transfusion rates.
Claudette Lajam, MD
ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 7
New Leadership and Growth in Pediatrics
NYU Langone added three new faculty members to its Pediatric Orthopaedic Division this year, including a new chief, Pablo Castañeda, MD.
Dr. Castañeda comes to New York from Mexico City, where he has specialized in treating hip disorders in children and adolescents. His practice focuses on improving outcomes for children with developmental dysplasia of the hip, Legg-Calvé-Perthes disease, and slipped capital femoral epiphysis. He currently serves on the medical advisory board of the International Hip Dysplasia Institute and serves on the board of
the Mexican College of Orthopaedics and Traumatology, and is past president of the Mexican Society of Pediatric Orthopaedics.
Also joining the Pediatric Orthopaedic Division are Mara Karamitopoulos, MD, clinical assistant professor of orthopaedic surgery, who previously was the co-director of pediatric orthopaedics at Maimonides Medical Center, and Jody Litrenta, MD, clinical assistant professor of orthopaedic surgery, who joins NYU Langone following a pediatric orthopaedic fellowship at Children's National Medical Center.
Pablo Castañeda, MD
NYU LANGONE AFFILIATION WITH WINTHROP-UNIVERSITY HOSPITAL BRINGS EXPANDED AND ENHANCED HEALTHCARE NETWORKS TO LONG ISLAND
NYU Langone Medical Center and Winthrop-University Hospital on Long Island have reached an agreement to affiliate the institutions’ extensive healthcare networks. NYU Langone, with more than 150 ambulatory sites throughout the region, will complement Winthrop-University Hospital’s main campus, multiple ambulatory sites, and network of 66 faculty and community-based practices in more
than 140 locations extending from eastern Long Island to Upper Manhattan. The affiliation will further expand NYU Langone’s presence on Long Island, while enhancing Winthrop’s inpatient and outpatient services with improved access to NYU Langone’s wide range of medical and surgical specialties.
“This agreement publicly confirms our confidence that an affiliation will allow both of our institutions to collaborate and share best practices to better meet the healthcare needs of the communities we serve,” says Robert I. Grossman, MD, the Saul J. Farber Dean and CEO of NYU Langone. Pending regulatory approval, the institutions are aiming to complete their affiliation in spring 2017.

8 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
Research-driven Innovations in Care
COMBINING EXPERTISE, NOVEL RESEARCH FINDINGS, AND THE LATEST TECHNIQUES, TECHNOLOGY, AND FACILITIES,
THE ORTHOPAEDIC TEAM AT NYU LANGONE PROVIDES INDIVIDUALIZED CARE FOR PATIENTS WITH COMMON CONDITIONS
OR THE MOST COMPLEX CLINICAL NEEDS.
James D. Slover, MD
Clinical Care and Research
ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 9
“We want the right operation or intervention for the right patient at the right time,” says Richard Iorio, MD, the Dr. William and Susan Jaffe Professor of Orthopaedic Surgery and chief of the department’s Adult Reconstructive Division. Solutions may eventually need to be as individualized as the “arthritis fingerprints” that determine a patient’s risk, progression, and therapeutic response, Dr. Iorio says. A host of recent departmental initiatives are helping to make that personalized approach a reality.
BIOMARKERS ENHANCE RISK PREDICTION
As they sort through the many factors that may determine disease risk and therapeutic success, the department’s researchers are increasingly looking to biomarkers. “Part of our mission is to avoid joint replacements and big surgeries in people who don’t need them, and biomarkers may help us identify who those patients are,” Dr. Iorio says. The department’s well-curated synovial fluid repository is already enabling researchers to test biomarkers that may predict which young athletes who sustain knee injuries are likely to subsequently develop osteoarthritis (OA), and when older patients with OA are likely to require a joint replacement. From roughly three dozen potential biomarkers initially isolated from the repository, researchers are extensively analyzing a set of 10, according to Thorsten Kirsch, PhD, professor of orthopaedic surgery and cell biology and vice chair of research. In addition, department faculty are partnering with NYU Langone radiologists to develop new imaging methods that can detect early OA changes and other methods that could complement biomarkers in predicting surgical outcomes and disease progression.
The newly launched Joint Preservation Registry II is supporting these efforts with an ambitious plan to collect knee, hip, and shoulder joint synovial fluid from 1,000 OA patients, as well as matched blood and urine samples and patient-reported outcome scores. Ultimately, Dr. Iorio says, validated biomarker profiles may help doctors and patients determine whether replacement surgery or joint preservation procedures are likely to meet their needs. “It’s going to be an important decision tool,” he says.
AVERTING HIP REPLACEMENTS FOR AVASCULAR NECROSIS
Most patients diagnosed with avascular necrosis or osteonecrosis of the hip are relatively young, which means that any therapies doctors recommend to help them avoid a hip replacement procedure—with a likely later revision—carries considerable long-term benefits. To that end, Thomas A. Einhorn, MD, professor of orthopaedic surgery, director of clinical and translational research and co-director of the Osteonecrosis Center, has helped to formalize a program that uses mesenchymal stem cells to treat early osteonecrosis. “The idea is that in avascular necrosis of the hip, or osteonecrosis, there’s dead bone in the head of the femur,” Dr. Einhorn says, “and when that bone dies it will eventually collapse and the patient would need a hip replacement.” Bone marrow stem cells injected directly into the femoral head through a minimally invasive method can interrupt this process, helping to regenerate, rejuvenate, and restore living bone to prevent a collapse of the joint and subsequent OA. The bone marrow aspirate concentrate (BMAC) procedure has drawn patients to NYU Langone from
Personalized Solutions Preserve and Replace Joints Based on Patient Profile
For some patients with joint-related problems, a total knee or hip replacement may restore mobility and relieve pain, while others may achieve reduced symptoms and restored function through less-invasive alternatives. Stratifying these patients by risk and likelihood of improvement is a major aim of NYU Langone.

10 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
Clinical Care and Research
around the country. Dr. Einhorn estimates that it has been successful in roughly two-thirds of cases so far, with clinical success based on a diminution or eradication of painful symptoms and an averted hip replacement.
NEW PROGRAMS STRATIFY RISK IN ARTHRITIS MANAGEMENT
NYU Langone also is personalizing treatment options for total knee or hip arthroplasty with a new model that stratifies candidates based on their preexisting surgical risk factors and provides options to mitigate those factors, which may lead to poor outcomes. Dubbed Perioperative Orthopaedic Surgical Home, or POSH, the model is aimed at identifying and reducing risk in eight main categories. POSH, a collaboration with NYU Langone’s Rusk Rehabilitation and Department of Population Health, matches patients with the programs that will best meet their risk-reduction needs. Those who smoke or are morbidly obese, for example, can be enrolled in smoking cessation or weight loss programs. “Patients could even avoid a joint replacement if they modify these risk factors sufficiently,” Dr. Iorio says. The department also is incorporating the POSH model into a broader commercial effort known as the Lifetime Initiative for the Management of Arthritis, or LIMA. This unique website provides comprehensive information, peer support from other patients, advice from an arthritis coach, and evidence-based self-evaluations to help patients determine their risk of progression and the best course of action. If patients find out they’re in a very low-risk category, for example, conservative measures such as arthritis-friendly exercises and over-the-counter pain medications might be enough to help them manage their condition.
SAME-DAY JOINT REPLACEMENT PROGRAM EXPANDS
For the right patients, same-day discharge following joint replacement can lead to better outcomes and higher satisfaction. Since Roy I. Davidovitch, MD, assistant professor of orthopaedic surgery, performed the first same-day hip replacement in New York City in 2015, NYU Langone has worked to bring the benefits of the approach to more patients.
The same-day hip replacement program has expanded to include knee and shoulder replacements; a same-day discharge group with faculty from both the Adult Reconstructive and Shoulder and Elbow divisions collaborate to apply same-day hip replacement protocols and best practices to the other procedures. Surgeons decide which patients are good candidates and how their pain and therapy needs will be safely and efficiently met in the hours, days, and weeks after the surgery. Regional nerve blocks and medication cocktails, for example, can help provide smooth transitions for patients in the first 24 postoperative hours. “Our foremost priority is to ensure that this strategy is safe and that patients will have adequate pain control at home,” says Mandeep S. Virk, MD, assistant professor of orthopaedic surgery. “They should have a responsible adult with them, and all of the necessary resources so that they can go home and sleep in their own bed without being deprived of necessary, immediate postsurgical care.”
Roy I. Davidovitch, MD
ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 11
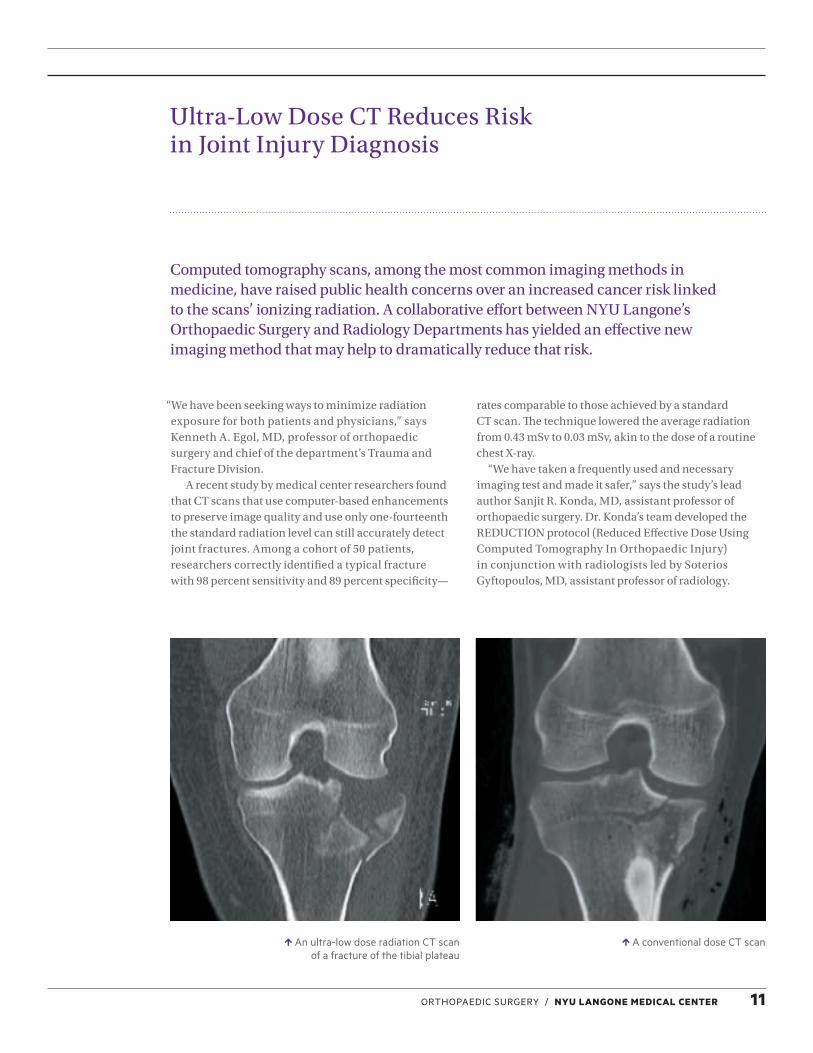
An ultra-low dose radiation CT scan of a fracture of the tibial plateau
A conventional dose CT scan
Ultra-Low Dose CT Reduces Risk in Joint Injury Diagnosis
“We have been seeking ways to minimize radiation exposure for both patients and physicians,” says Kenneth A. Egol, MD, professor of orthopaedic surgery and chief of the department’s Trauma and Fracture Division.
A recent study by medical center researchers found that CT scans that use computer-based enhancements to preserve image quality and use only one-fourteenth the standard radiation level can still accurately detect joint fractures. Among a cohort of 50 patients, researchers correctly identified a typical fracture with 98 percent sensitivity and 89 percent specificity—
rates comparable to those achieved by a standard CT scan. The technique lowered the average radiation from 0.43 mSv to 0.03 mSv, akin to the dose of a routine chest X-ray.
“We have taken a frequently used and necessary imaging test and made it safer,” says the study’s lead author Sanjit R. Konda, MD, assistant professor of orthopaedic surgery. Dr. Konda’s team developed the REDUCTION protocol (Reduced Effective Dose Using Computed Tomography In Orthopaedic Injury) in conjunction with radiologists led by Soterios Gyftopoulos, MD, assistant professor of radiology.
Computed tomography scans, among the most common imaging methods in medicine, have raised public health concerns over an increased cancer risk linked to the scans’ ionizing radiation. A collaborative effort between NYU Langone’s Orthopaedic Surgery and Radiology Departments has yielded an effective new imaging method that may help to dramatically reduce that risk.

12 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
Clinical Care and Research
EARLY SIGNS OF IMAGING SUCCESS
The collaborative effort began when Dr. Konda introduced the idea of using CT scans to diagnose traumatic arthrotomies of the knee. The telltale detection of air in the knee joint had previously relied on the saline load test, which requires injections of an intra-articular saline solution. “You could imagine that it is likely an invasive, painful procedure for a patient. It also takes time,” Dr. Egol says.
Dr. Konda, however, noticed that CT scans of open fractures around the knee commonly revealed air within the joint, and follow-up research confirmed that the method could diagnose traumatic arthrotomies as well. The promise of the approach, however, came with a new challenge: how to reduce the patients’ radiation exposure. “We worked with our radiology colleagues on cadavers to see if we could develop an imaging protocol that would help us detect the air in the joint and minimize the radiation,” Dr. Egol says.
Based on their success in assessing open knee wounds with the low-dose CT strategy, the researchers asked whether the method also could help diagnose extremity fractures. “We applied this low-dose technology to all the different areas of the body that would normally get CT scans, comparing it to standard-dose radiation CT scans, and found that we really didn’t lose any accuracy in diagnosis,” Dr. Egol says.
Subsequent research confirmed that the team’s strategy didn’t adversely impact patient outcomes. The results are now prompting a multidepartmental collaboration between the Departments of Radiology and Emergency Medicine to reduce radiation exposure for patients with orthopaedic trauma and for the physicians involved in their care. “Patients who undergo a traumatic injury or suspected fracture have enough to worry about,” Dr. Egol says. “Our research makes radiation exposure among the least of their concerns.”
TAPPING NYU LUTHERAN’S DIVERSE PATIENT POPULATION FOR RESEARCH INITIATIVES
Researchers are tapping NYU Lutheran’s diverse patient population for two research projects. In one, investigators are studying the incidence of lateral compression type 1 pelvic ring fractures, which have a mortality rate of 5.1% to 8.6%. In another, NYU Lutheran has contributed more than 100 patients to a study about a new geriatric trauma triage score developed by NYU Langone researchers that has shown good ability to predict inpatient mortality and complication. The Score for Trauma Triage in the Geriatric and Middle-Aged (STTGMA) distinguishes between high-energy and low-energy injury patients. In early results, the STTGMA has shown superior predictive value when the score is calculated at initial patient presentation as opposed to retrospective application. Researchers hope this predictive score can be used to help guide efficient and appropriate patient care in the future.
Complex Case: Scheuermann’s Kyphosis
Postoperative X-ray
Collaboration in Atypical Case of Scheuermann’s Kyphosis and Spinal Cord Herniation
The strong collaboration between the orthopaedic surgeons and neurosurgeons at NYU Langone’s Spine Center recently enabled a complex corrective spine surgery following a rare diagnosis.
ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 13
with an operating microscope, released adhesions of the cord to the anterior dura, and repositioned it in the center of the canal by dividing the dentate ligaments.
Dr. Errico took over and performed radical facetectomies to decompress the spinal nerves and harvest bone material for subsequent grafting. He then corrected White’s spinal curvature and stabilized the spine by fusing 12 of the patient’s vertebrae, from T2 to L1, with 24 pedicle screws and two-foot-long titanium rods.
Finally, Dr. Perin completed the thoracic laminoplasty and screwed miniplates to the vertebral laminae and adjacent lateral mass to prevent a recurrence of the hernia. The surgeons then carefully placed the allografts over the posterior elements of White’s decorticated vertebrae, to aid bone regeneration.
RESULTS
Following the surgery, the patient felt immediate relief upon waking in the post-anesthesia care unit. “No numbness, no pain—just like that,” White recalls. After recovering from the surgery, he remained pain-free, returning to golf and other favorite activities.
Traditionally, the realm of orthopaedic spine surgeons was mainly bone issues, while spinal neurosurgeons dealt with neural structures. “But over the last 20 years or so, these two specialties have become less distinct and more collaborative,” says Thomas J. Errico, MD, professor of orthopaedic surgery and neurosurgery and co-director of NYU Langone’s Spine Center.
PRESENTATION
The benefits of such collaboration were in full view when Adam White, 20, a former lineman on his Pennsylvania high school football team, requested a surgical evaluation in May 2015 to address intense pain between his shoulder blades that had worsened progressively over an eight-month period. In addition, he experienced numbness and tingling that radiated from his fingers to his biceps and from his toes to his knees. Sudden movements, especially sneezing, caused severe and shooting pain that was nearly unbearable, even with medication.
With an MRI, Noel I. Perin, MD, associate professor of neurosurgery, discovered that White was suffering from a rare T5 through T7 spinal cord herniation. It was an interesting intersection with another uncommon diagnosis the young man had received previously at NYU Langone: a pronounced curvature of his thoracic spine due to Scheuermann’s kyphosis, found by radiologists on scoliosis X-rays. “I’ve never before seen both in a single patient,” Dr. Perin says.
SURGICAL PLAN
Dr. Perin developed a comprehensive surgical plan in consultation with Dr. Errico. Each specialty “brings a little extra to the table,” says Dr. Errico, and that additive effect has been highly beneficial for complex cases such as White’s.
During the 13-hour surgery that followed, Dr. Perin first addressed his patient’s spinal-cord hernia and myelopathy with a laminectomy, laminoplasty, and cord decompression. Following a durotomy, he explored the intradural spinal cord
14 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
Clinical Care and Research
Tailoring and Testing New Treatment Options through Regenerative Medicine
Over the past few years, sports medicine has benefitted enormously from the use of injectable biologics to delay or even avoid the need for knee replacement surgery. Among the growing list of promising therapeutic options, NYU Langone is using growth factors derived from platelet-rich plasma and stem cells from bone marrow aspirate to treat osteoarthritis (OA) and testing the treatments on a range of other conditions.
“Biologics will certainly play a major role in the future in the management of patients with musculoskeletal disease,” says Laith M. Jazrawi, MD, associate professor of orthopaedic surgery and chief of the Division of Sports Medicine. Dr. Jazrawi is leading plans for the department’s Center for Regenerative Medicine that would include a dedicated procedure room for injectable therapeutics.
NYU Langone researchers are conducting multiple projects to help determine which biologics may have the brightest future. For one multicenter randomized controlled trial, investigators are comparing the effectiveness of platelet-rich plasma to dry needling for treating patellar tendinopathy. Other researchers are pursuing a randomized controlled trial in collaboration with Birmingham, Alabama-based NuTech Medical, Inc., to compare the effectiveness of the company’s ReNu™ amniotic stem cell allograft to a hyaluronic acid injection or saline control for treating knee OA. A third study is examining whether hyaluronic acid injections improve the symptoms of patients with the earliest stages of OA, compared with physical therapy alone.
Although preliminary, Dr. Jazrawi says the clinical trials’ results have been encouraging so far. Pending FDA approval, he and his colleagues also hope to investigate the OA-treating potential of adipose tissue-derived stem cells, which could be harvested from liposuctions in collaboration with the Plastic Surgery Department. The cells, Dr. Jazrawi says, might even help reestablish cartilage in an OA-afflicted knee.
RESEARCH SYNERGY WITH SYNOVIAL FLUID REGISTRY
The current and upcoming clinical research projects, he says, fit well with the work of the department’s Joint Preservation and Arthritis Center. Synovial fluid samples collected as part of the Joint Preservation Registry, for instance, are helping to match patients’ therapeutic responses to unique biomarkers. “We’re beginning to tailor our medical care toward a specific patient profile,” Dr. Jazrawi says. In this case, he notes, the biomarker-based profile can help determine which patients will respond best to which cellular therapy.
“There may be a specific cohort of patients that has better regenerative potential,” he says. Asking why they improve with stem cell injections while others do not can lead to a better alignment of treatments based on patients’ molecular characteristics identified via blood, urine or joint fluid samples. “Getting that information, it will help us determine if a patient will benefit more from an
350SYNOVIAL FLUID SAMPLES
COLLECTED FROM PATIENTS INDICATED FOR ARTHROSCOPIC KNEE SURGERY.

ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 15
injection, from physical therapy, or by going right to total knee replacement,” he says.
Departmental researchers led by Eric Strauss, MD, associate professor of orthopaedic surgery, accurately predicted OA severity based on levels of the synovial fluid biomarkers MCP-1 and IL-6. A separate line of collaborative research led by Philip Band, PhD, research professor of orthopaedic surgery and biochemistry and molecular pharmacology, found that higher levels of a proprietary protein marker called TSG-6 may reflect a more urgent need for knee replacement.
Finally, researchers are collecting fluid from patients undergoing knee arthroscopy to likewise help determine who is more likely to do well or poorly. The decision-aiding information, in turn, can prevent treatment delays and streamline patient care. “They’re getting the best treatment possible for them, not for all patients in general,” Dr. Strauss says. “So we’re looking for this tailored, personal medicine concept based on the data from this registry to help us answer some of these questions.”
SUPERIOR RESULTS WITH SUPERIOR CAPSULAR RECONSTRUCTION
NYU Langone’s expanding use of a new procedure called superior capsular reconstruction is helping patients with a deficient and non-repairable rotator cuff injury avoid a traditional reverse shoulder replacement and its complications.
“The concept of a superior capsular reconstruction—using a dermal allograft, anchoring it into the glenoid and then re-attaching it to the humeral head at the rotator cuff insertion—has provided significant pain relief to select patients with irreparable rotator cuff tears and has improved shoulder function,” says Andrew S. Rokito, MD, associate professor of orthopaedic surgery and chief of the Shoulder and Elbow Division. This procedure, which offers an alternative to shoulder replacement, represents an “exciting” change in the field of orthopaedics, especially within sports medicine.
Eric Strauss, MD
16 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
Clinical Care and Research
Wide-awake hand surgery with only local anesthesia—first championed by Canadian surgeons—has been implemented by a few U.S. institutions, and is becoming a growing topic of discussion among hand surgeons. NYU Langone will became one of the first centers in the country to formalize a wide-awake hand surgery program, with a dedicated check-in area and surgery room at its Outpatient Surgery Center opening in January 2017. “One key advantage of the technique is the ability to dispense with general anesthesia and sedation that can lead to negative side effects and complications for the patient,” says S. Steven Yang, MD, MPH, clinical associate professor of orthopaedic surgery, who led the launch of the center.
REMOVING THE EPINEPHRINE SAFETY BARRIER
Anesthesia is currently administered routinely to counteract the intense discomfort of sustained tourniquet pressure—up to 200 to 250 mm Hg—used to provide a bloodless field for hand and arm surgery. As a vasoconstrictor, epinephrine limits bleeding and prolongs the anesthetic effect by delaying its dissipation through the blood stream, but was thought to be hazardous. “We were always taught that we shouldn’t use epinephrine,” Dr. Yang says, based on the mistaken belief that an overwhelming vasoconstrictive effect in the fingers’ small vessels could lead to ischemia and necrosis. But recent studies now suggest that the true culprit of epinephrine-related complications was likely impurities in the anesthesia formulations, lending the concept of wide-awake hand surgery a major boost by eliminating the tourniquet.
Based on this new insight, doctors are using a large dose of local anesthetic such as lidocaine, mixed with epinephrine, to numb the surgical site and constrict the blood vessels. The high volume of incoming medication offers a secondary benefit by reducing bleeding via the tamponade effect. “Almost like inflating a balloon inside the arm or the hand, it pinches off the blood vessels,”
Dr. Yang says. “The combination of those features enables us to do the surgery without a tourniquet. And if we don’t use the tourniquet, we don’t need to give the sedation or general anesthesia drugs."
“If you don’t need to give the drugs, you don’t have to have patients doing all of this preoperative testing, which is costly and inconvenient for patients,” adds Dr. Yang.
CONFIRMING SURGICAL EFFICACY IN REAL TIME
Although a wide variety of surgeries may prove amendable to the surgical technique, the department is beginning by offering the approach for smaller procedures, such as releases of carpal tunnel, trigger finger, De Quervain’s, and wrist tendinitis, as well as excisions of ganglions and cysts around the wrist.
Beyond improved safety, efficiency, and cost savings, patients who remain awake during the procedures can provide constructive feedback to their surgeons, Dr. Yang says. After surgery to release a patient’s trigger finger, for example, he can ask the patient to make a fist and slowly straighten out the affected finger to determine whether the tendon is still catching.
Likewise, for patients who have had tendon lacerations repaired, surgeons can ask them to move their hands and fingers to assess the strength and quality of the repairs and determine whether more work is required. “We can actually check patients’ movements while they’re on the operating table, where the hand is still open,” Dr. Yang adds. “There is obviously a significant advantage there.”
In conjunction with the surgical program’s official launch, Dr. Yang and colleagues are initiating several prospective studies to assess patient satisfaction, clinical outcomes, and potential cost savings of wide-awake hand surgery. For patients, he says, the eventual payoff could be a safe and effective procedure that makes hand surgery akin to going to the dentist for a filling.
A Dedicated Space and New Momentum for Wide-Awake Hand Surgery
Hand surgery without tourniquets, sedation, or general anesthesia—once unthinkable—is in the midst of a remarkable renaissance thanks to a burst of recent research demonstrating the safety, efficacy, and benefits of a technique once limited by misconceptions.

ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 17
S. Steven Yang, MD, MPH
18 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
Clinical Care and Research
The evolution of such robot-assisted orthopaedic surgeries has been spurred by a combination of cutting-edge tools, technical expertise, evidence-based pain management, and rapid recovery protocols. As a result, surgeons can employ minimally invasive techniques, reduce errors, prevent complications, and increase their precision in ways that preserve more bone and tissue. Indeed, the new option for total knee replacement is poised to boost the accuracy, outcome, and patient satisfaction of an increasingly in-demand surgery that already accounts for about 85 percent of all knee arthroplasties. Patrick A. Meere, MD, clinical associate professor of orthopaedic surgery, says the advances have actually benefitted each of the main approaches for total knee arthroplasty. “Within the last five years, two things have happened: Robots have become the champions of the measured resection-alignment school of thought, and sensors have come into play in the balancing school,” Dr. Meere says.
ROBOTICS MEET RESECTION
The measured resection approach, which places greater emphasis on precise anatomical cutting of bone and less on soft tissue alignment, has benefitted from MAKOplasty®, a robot-assisted technique that uses CT scans to create three-dimensional preoperative templates. NYU Langone surgeons have successfully used MAKOplasty for partial knee and unicompartmental knee replacements over the past five years, and for total hip replacements over the past three years. With MAKOplasty, surgeons can match landmarks in a patient’s body to those in the 3D model; a 1:1 registration match then allows the robot to create a virtual space that guides each surgical cut. “Once you have that, you can achieve a level of accuracy that has been unsurpassed to
date, both for partial knee replacements and for hip replacements,” Dr. Meere says. The MAKO system, which offers preoperative imaging capabilities and the highest levels of accuracy, is one of two robotics-assisted systems used at NYU Langone. The other is NAVIO, an image-less, handheld computer wand that follows the contours of a patient’s bones and creates accurate cut guides based on mathematical models.
“Because it doesn’t depend on a preoperative CT scan, the NAVIO alternative is more nimble and less expensive, and reduces the patient’s radiation exposure,” says Jonathan Vigdorchik, MD, assistant professor of orthopaedic surgery. In addition to his research using robotics in total knee replacement, Dr. Vigdorchik is exploring how robotic-assisted surgery can be used to help customize the total hip replacement. By using the department’s EOS full-body low-dose X-ray machine to take images of patients in various functional positions, surgeons can help guide a personalized and optimized position for the components in a hip replacement to decrease the risk of complications such as dislocation and improve wear and longevity.
FINDING A BETTER BALANCE
The balancing approach to knee arthroplasty, which places more emphasis on balancing the ligaments and soft tissue of the knees, initially benefitted from computer navigation tools that improved the consistency in knee alignment when it came online more than a decade ago. Yet patient satisfaction scores following those surgeries still lagged behind those of total hip replacement patients. Now, newer sensors in the tibia liners, in regular use at NYU Langone, offers greater balancing guidance by measuring pressure rather than alignment. “They have sensors embedded in the trial components, so surgeons
In Joint Replacement Surgeries, Robots and Sensors Lend a Critical Hand
Recent advances in robotic and sensor technology have expanded their application in joint replacement surgeries, from partial knee to total hip, and NYU Langone is one of the first medical centers to offer a robot-assisted surgical option for total knee replacements.

ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 19
can verify the equal distribution of pressure on the inside and outside of the knee,” says Dr. Meere. The sensors also leave an imprint on the point of contact to the tibia, to help surgeons see patterns associated with excessive laxity or tightness.
EXPANDING APPLICATIONS, ENHANCING OUTCOMES
The Medical Center is concurrently focused on using robotics to assist in surgeon training and to reduce variability in outcomes—ultimately raising patient satisfaction scores for knee replacement surgery. Because the knee joint is so complex and subjected to such unpredictable forces, Dr. Meere says, knee arthroplasty was a challenging skill to teach in the absence of technology. “It’s a fantastic learning tool for the residents because it provides a live picture of your action instead of a theoretical one—you do a surgical correction and see the immediate results,” he says.
To further integrate the robotics technology with balancing sensors in clinical practice, NYU Langone’s Advanced Arthroplasty Research Lab is conducting both bench-top and clinical research. “The integration and
use of robotics will be tracked with our very efficient tools of patient-reported outcomes before and after surgery so we can clearly validate the superiority of robotic surgery versus conventional surgery,” says Dr. Vigdorchik. Although this type of research takes many years to complete, early clinical results are already showing promising success.
Likewise, patient-reported measures can help demonstrate whether the robotics-sensor combination offers the best possible outcome. “That’s the future,” he says. “The natural evolution is to merge the two together.”
Jonathan Vigdorchik, MD
NYU LANGONE IS
1 of 8WORLDWIDE REFERENCE CLINICS THAT
ARE PART OF THE INTERNATIONAL SOCIETY FOR COMPUTER-ASSISTED
ORTHOPAEDIC SURGERY FELLOWSHIP.
20 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
Clinical Care and Research
Before every joint or spine procedure over a nearly 10-year period, the department’s doctors swabbed each patient’s nose for pathogens and applied topical antibiotics to the nares to eradicate Staphylococcus species. Roughly one-third of patients carry the bacterium and an estimated two to three percent carry MRSA. “Our research has shown that those patients are at increased risk of developing infection after surgery, so we screen and eradicate it,” says Joseph A. Bosco, MD, professor of orthopaedic surgery and vice chair for clinical affairs.
The new study found that the preoperative procedure decreased the infection rate in a cost-effective manner, though it did not drive the risk to baseline levels. Now the researchers are collaborating with infectious disease
and epidemiology experts at NYU Langone to identify the remaining risk factors and eliminate them if possible. In the meantime, Dr. Bosco says, surgeons can discuss the infection risk with patients prior to surgery to help them make a more informed decision about whether to proceed with the surgery.
The department also is using physician-specific HCAPS scores to identify opportunities for improvement, and is developing a comprehensive educational program for physicians who may need more help. One key element of the program is a peer-to-peer simulation, developed in conjunction with the New York Simulation Center for the Health Sciences (NYSIM), which uses simulated patient encounters to help physicians prepare for difficult situations.
Quality and Safety Initiatives Aid Outcomes While Boosting Value
Multiple studies examining orthopaedic quality and patient safety have highlighted the many improvements that NYU Langone has made to clinical practice. One major study, recently published in the Journal of the American Academy of Orthopaedic Surgeons and based on data from more than 16,000 patients, found that a bacterial screening and prophylaxis eliminated much of the post-surgical infection risk.
Richard Iorio, MD

ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 21
NEW INSIGHTS ON MITIGATING SURGICAL RISK AND IMPROVING ACCESS
In another quality and safety initiative, the department is tapping large national databases to examine how depression, substance abuse, smoking, and other risk factors affect patient outcomes after joint arthroplasty. One emerging point is that such risks are best addressed preoperatively. Dr. Bosco and colleagues also have found that patients with a lower socioeconomic status have worse outcomes. “They tend to have fewer resources available to them and less access to care,” he says. “And they tend to come to the process later, so they’re sicker.”
Although high-volume medical centers like NYU Langone yield better outcomes, Dr. Bosco says, poorer individuals have reduced access to such centers. Even relatively small increases in a patient’s distance to a major center, he notes, can be prohibitive to those who don’t own a car and whose lack of mobility makes public transportation difficult.
The department’s research suggests that as joint replacement surgeries have increased at high-volume centers over the past decade, they have decreased at low-volume centers. To address the growing gap in access, the department is sharing lessons learned, clinical pathways, and specific protocols—such as antibiotic prophylaxis—with lower-volume medical centers. “We have to be cognizant of the fact that high-volume centers increase health care disparities by attracting greater numbers of patients, and share our knowledge with low- volume centers to decrease that disparity,” Dr. Bosco says.
BUNDLED PAYMENTS YIELD MULTIPLE BENEFITS IN JOINT REPLACEMENT SURGERY
In January 2013, NYU Langone became an early entrant in Medicare’s Bundled Payments for Care Improvement initiative, which sets a fixed reimbursement price for a hospitalization and the 90-day period after discharge, known as an “episode of care.” Four years later, the Medical Center is boosting patient outcomes after joint replacement surgery at significant cost savings through the bundled payments program, and developing infrastructure and expertise that could similarly aid a host of other procedures.
Upon their discharge, joint replacement patients are typically transferred to relatively costly inpatient facilities such as skilled nursing facilities or
rehabilitation centers. NYU Langone researchers found that patients who were sent home instead, however, fared better and at a lower average cost of care. “The readmission rate was less, the infection rate was less, and the patient satisfaction was greater,” says Dr. Bosco. “Not only did discharge home save money, but it also improved outcomes—and that came as a surprise.”
In a recent Journal of the American Academy of Orthopaedic Surgeons study, Dr. Bosco and colleagues documented 16 percent savings on bundled payments for lower extremity joint replacement. Most of the savings, they found, came in the post-acute phase. “It’s all about making sure that there’s a smooth transition between the hospital and home, that they have the resources at home to be successful, and that we keep a close eye on them,” he says.
Prior to all joint replacement surgeries, clinical care coordinators help patients understand what to expect following discharge. They also use a newly developed tool called RRAT, or the Readmission Risk Assessment Tool, to identify those at greatest risk for readmission or discharge to a nursing home. The risk stratification, Dr. Bosco says, helps the care team identify and allocate the resources necessary to reduce readmissions.
After discharge, coordinators and other staff closely monitor the patients, employing telemedicine, visiting nurses, and therapists to smooth the transitions. Dr. Bosco and colleagues are sharing their lessons learned with other departments and institutions as the bundled payment methodology becomes mandatory in multiple areas of medicine. The added knowledge and tools are driving efficiencies in non-bundled conditions as well. “We were fortunate to develop an infrastructure and expertise for our institution through our voluntary participation, which will help us apply these practices to other areas in the future,” Dr. Bosco says.
BUNDLED PAYMENTS PROGRAM A SUCCESS AT NYU LUTHERAN
The Bundled Payments for Improved Care initiative also has been successful at NYU Lutheran, where 206 patients are enrolled, with 31% discharged home, 68% to NYU Lutheran Augustana Center, a subacute rehabilitation facility, and just 1% to inpatient rehabilitation.
22 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
Clinical Care and Research
ENHANCING BONE HEALING FUNCTION IN OLDER PATIENTS
One line of NIH-funded research is focusing on the Wnt signaling pathways, which induce the differentiation of bone-forming cells from osteoprogenitor cells. The number and potency of skeletal stem cells decreases significantly with aging; boosting endogenous Wnt signals, then, may be one way to reclaim the lost function and help older patients more quickly recover from bone fractures.
Dr. Leucht and colleagues are optimizing an approach—tested in mice, rabbits, and human cells—that delivers the Wnt 3A protein via liposomes to help boost a patient’s bone-healing potential. “If we use it in a young animal, we’re able to increase bone formation by about 350 percent,” he says. In older animals or those with major defects, the strategy can restore the osteogenic potential back to that of a healthy young animal.
RE-CODING SKELETAL STEM CELLS
A second study is examining whether removing an embryonic signal called the Hox code can enable the body’s skeletal stem cells to be more adaptable when introduced to new locations. Bones above the neck’s hyoid lack a Hox code, whereas all other bones include it. “The code basically imprints a function onto the cell, and the cells are limited by that,” Dr. Leucht says. “If you put them into a different environment, they recognize that it’s not their home, are confused by that and don’t do the right thing.”
As Dr. Leucht has found, the Hox code may have critical clinical implications because stem cells derived from code-lacking craniofacial bones are far better at regenerating broken or injured bones in mice than are cells from code-constrained bones such as the tibia.
Surgeons cannot use facial bones for bone grafts, so Dr. Leucht and his team hope to introduce the same plasticity into stem cells isolated from the pelvis or other long bones. Based on RNA sequencing, his team has
New Advances in Bone and Cartilage Regeneration Research
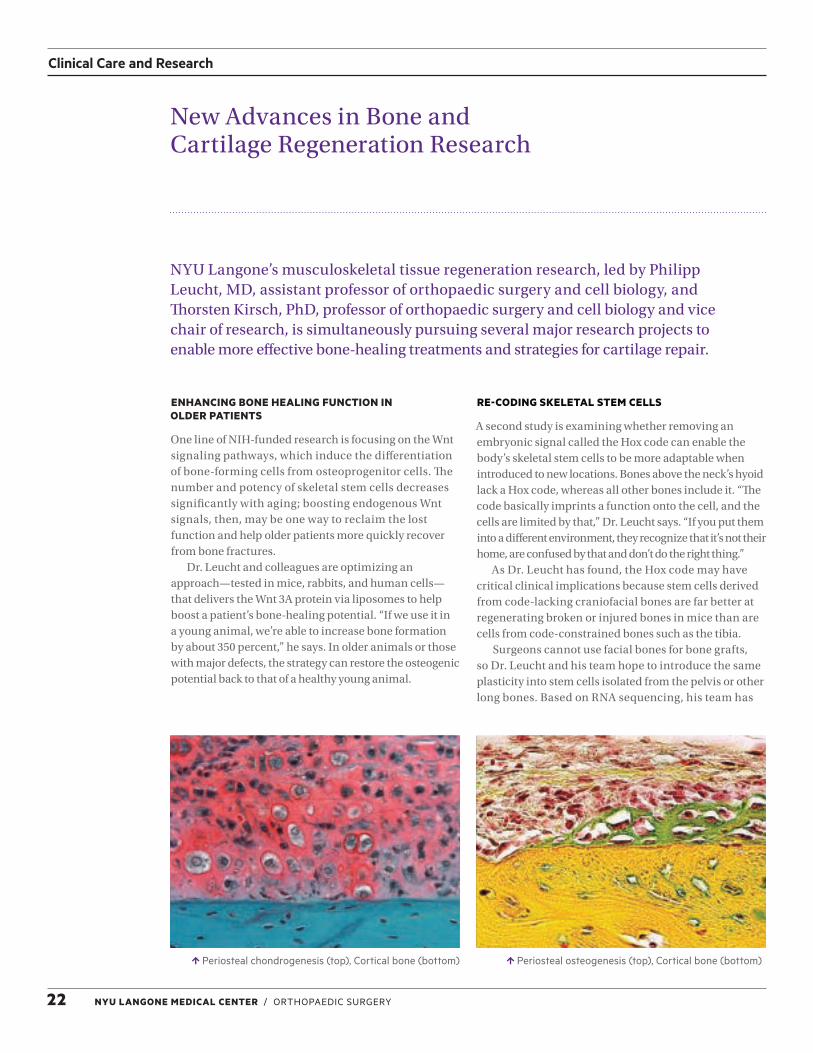
Periosteal chondrogenesis (top), Cortical bone (bottom) Periosteal osteogenesis (top), Cortical bone (bottom)
NYU Langone’s musculoskeletal tissue regeneration research, led by Philipp Leucht, MD, assistant professor of orthopaedic surgery and cell biology, and Thorsten Kirsch, PhD, professor of orthopaedic surgery and cell biology and vice chair of research, is simultaneously pursuing several major research projects to enable more effective bone-healing treatments and strategies for cartilage repair.

ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 23
found more than 2,000 gene expression differences in Hox-positive versus Hox-negative cells. Follow-up studies now underway may help identify the true drivers of the latter cells’ regenerative powers.
Another project is looking at the role of chronic low-level inflammation on skeletal stem cells. This chronic inflammation slowly increases with age, raising the risk of cancer and Alzheimer’s disease and potentially interfering with bone healing due to its negative impact on the number and osteogenic potential of the remaining pool of bone marrow stem cells.
Dr. Leucht found that one-year-old mice—equivalent to 55 to 65-year-old humans—showed elevated signs of inflammation associated with aging, or “inflammaging.” Remarkably, however, his team suppressed such inflammation and restored the skeletal stem cells’ bone-healing potential with low doses of nonsteroidal anti-inflammatory drugs. In essence, the treatment seemed to reverse the aging process and restore the cells’ osteogenic potential.
“By reducing the inflammation, these cells can recognize and recover from a senescence pathway and turn back into an active progenitor cell pool that can be used if there’s an injury in these animals,” he says. Dr. Leucht and colleagues are now trying to clarify the underlying pathway.
STUDYING THE ROLE OF ANTIDEPRESSANTS IN FRACTURE HEALING
For a fourth project, the lab is conducting bench-to-bedside research to better understand whether commonly prescribed selective serotonin reuptake inhibitor antidepressants such as fluoxetine might interfere with fracture healing. The project began when Dr. Leucht noticed that roughly 25 to 30 percent of his patients with nonunions were on SSRIs, compared to about 10 percent of the general population.
In mice, his team showed that chronic antidepressant users were indeed impaired in their fracture healing: their osteoblasts survived and proliferated normally, but could not differentiate properly. The researchers are now planning to look prospectively at patients with fractures, document those who are taking SSRIs, and determine which develop nonunions. “This may be something
that’s very clinically relevant and may be actually translatable within a year or two if we can finish the clinical trials,” Dr. Leucht says.
NEW PEPTIDE GREATLY ENHANCES CARTILAGE REPAIR
Other NYU Langone researchers led by Dr. Kirsch have made strides in cartilage regeneration, including the recent identification of a peptide that seems to stimulate cartilage repair. The peptide, which binds to hyaluronan in the cartilage matrix, has proven effective when combined with high molecular weight hyaluronan. Although the mechanism remains unclear, “it is possible that the peptide together with high molecular hyaluronan might provide a stem cell niche where the cells can attach and build new cartilage,” says Dr. Kirsch. The researchers have filed for a patent on their discovery and are actively investigating the peptide’s potential role in recruiting stem cells to repair musculoskeletal tissues.
Philipp Leucht, MD
COLLABORATION WITH ENGINEERS
The Department of Orthopaedic Surgery is expanding its collaboration with the NYU Tandon School of Engineering, moving two labs to the school’s facilities with the aim of further stimulating interactions between engineers and orthopaedic surgeons.
Complex Case: Pelvic Osteosarcoma
resolution the team needed to map the surgical site. Dr. Rapp and Dr. Saadeh turned to BioDigital Human®, an augmented reality program, to create a highly detailed interactive map.
In collaboration with a 3D virtual surgery engineer at 3D Systems in Colorado, the team created custom 3D-printed jigs that they could temporarily secure to the pelvic and fibula bones to precisely guide a surgical saw. “The pelvis is a curved bone,” Dr. Rapp says, “so it’s much more difficult to anticipate the angles of the cuts, even if you have the best anatomical mind in the world.”
The virtual surgical plan converted CT scans into exact copies of Morales’s bone anatomy, permitting the surgeons to practice the surgical procedure beforehand. “This would be the first time part of a fibula would be inserted into a pelvis with the aid of 3D technology, but using the models, we felt confident that it could work,” Dr. Rapp says.
The strategy sounded so futuristic, Morales recalls. “But these men had saved my life before, and I’d seen what they were capable of. I trusted them,” she says.
RESULTS
After a carefully devised chemotherapy regimen to shrink the tumor, Dr. Rapp and Dr. Saadeh led a seven-hour surgery at Tisch Hospital in February 2015. Dr. Rapp excised Morales’s tumor while Dr. Saadeh removed the matched fibula fragment. They slotted in the replacement bone, performed microsurgery to attach the veins and arteries, and inserted titanium plates at both sites to stabilize the bone while it healed.
Six months later, a cancer-free Morales was able to put weight on her left leg and stand up unassisted. A year after the surgery, she began walking on her own—and reclaiming her future.
“There’s so much I want to do now,” she says. “I want to get my life started.”
PRESENTATION
In 2013, Sara Morales, 32, had been treated at NYU Langone for an osteosarcoma above her right shin that had required resection and a knee replacement. When she returned in 2014 with increasingly intense pain in her left hip, an MRI revealed a new tumor growing in her pelvic bone near the sacroiliac joint.
Morales faced a new round of chemotherapy and removal of the diseased bone, but the osteosarcoma’s hard-to-reach location deep in the pelvis, along with the need to maintain pelvic integrity to allow for weight-bearing, complicated the procedure. Full excision might require removing up to half of her pelvis and permanently confining her to a wheelchair.
SURGICAL PLAN
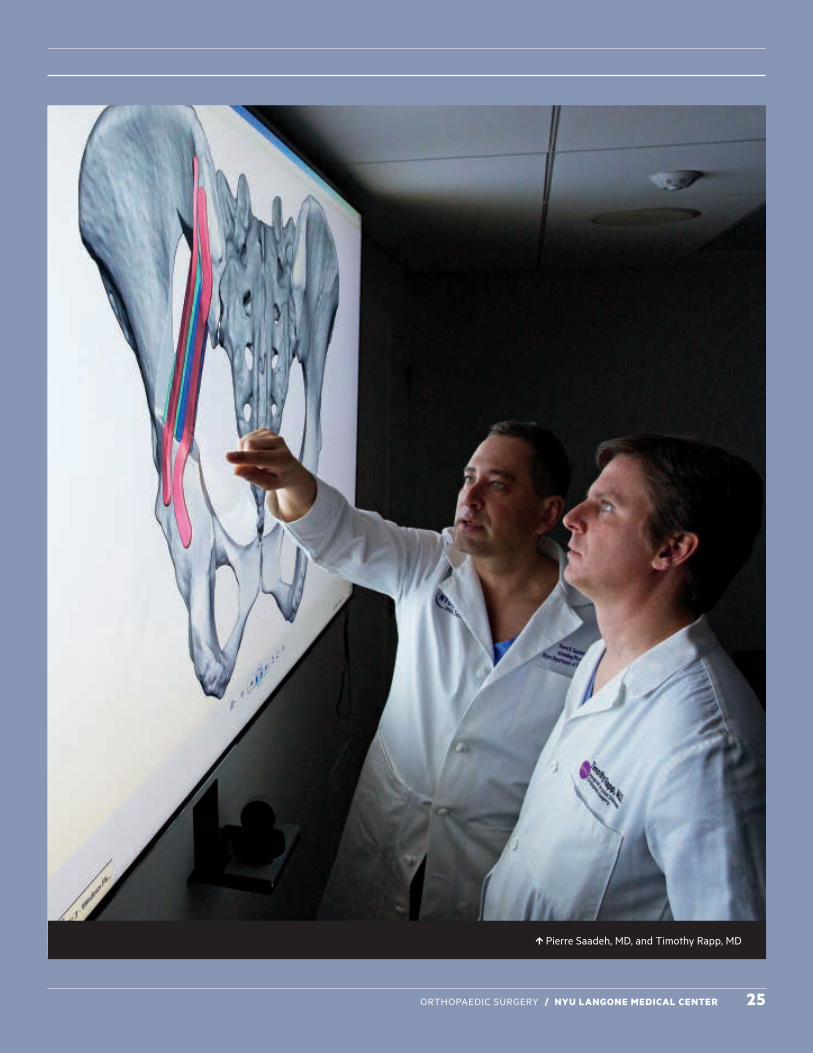
To preserve her ability to walk, the surgeons devised an alternate strategy, employing sophisticated 3D tools more commonly associated with head and neck surgery. Timothy R. Rapp, MD, associate professor of orthopaedic surgery and chief of the Division of Orthopaedic Oncology, had previously removed Morales’s initial tumor above her shin. He developed the new tumor resection plan in partnership with plastic surgeon Pierre B. Saadeh, MD, associate professor and chief of plastic surgery at Bellevue Hospital Center. Instead of reaching the pelvis through her abdomen and performing an internal amputation, the surgeons concluded that accessing and resecting her tumor from the back would cause less damage and allow for a more accurate resection. Equally important, this approach also would provide the exposure needed for reconstruction. To stabilize the pelvis after cutting out a nearly three-inch segment of bone, they opted to use part of her left fibula to bridge the gap. In order to keep the fibula alive during and after surgery, the fibula’s blood supply was brought with the bone and reconnected to local vessels in the pelvis using an operating microscope.
The complex operation would have to be extensively planned, and standard anatomy diagrams failed to provide the sufficient
3D Imaging Finds New Application in Resection of Complex Pelvic Osteosarcoma
Every year, doctors in the United States diagnose about 800 people with osteosarcoma—many of them adolescents or young adults who contract the cancer for unknown reasons during growth spurts.
24 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 25
Pierre Saadeh, MD, and Timothy Rapp, MD
ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 25
26 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
SELECTED PUBLICATIONS
Agten CA, Kaplan DJ, Jazrawi LM, Burke CJ. Subchondroplasty: what the radiologist needs to know. AJR Am J Roentgenol. 2016; 207: 1257–1262.
Arno S, Bell CP, Alaia MJ, Singh BC, Jazrawi LM, Walker PS, Bansal A, Garofolo G, Sherman OH. Does anteromedial portal drilling improve footprint placement in anterior cruciate ligament reconstruction? Clin Orthop Relat Res. 2016; 474: 1679–1689.
Ayalon O, Marcano A, Paksima N, Egol K. Concomitant ulnar styloid fracture and distal radius fracture portend poorer outcome. Am J Orthop (Belle Mead NJ). 2016; 45: 34–37.
Behery OA, Kester BS, Williams J, Bosco JA, Slover JD, Iorio R, Schwarzkopf R. Patterns of ninety-day readmissions following total joint replacement in a bundled payment initiative. J Arthroplasty. 2016 Nov 1.
Buchalter DB, Mahure SA, Mollon B, Yu S, Kwon YW, Zuckerman JD. Two-stage revision for infected shoulder arthroplasty. J Shoulder Elbow Surg. 2016 Nov 22.
Buza JA 3rd, Jancuska JM, Slover JD, Iorio R, Bosco JA 3rd. Variation in diagnoses for hip arthroplasty among New York State hospitals: implications for the Comprehensive Care for Joint Replacement Model. J Arthroplasty. 2016 Nov 15.
Capo J, Kaplan DJ, Fralinger DJ, Adler RS, Campbell KA, Jazrawi LM, Alaia MJ. Ultrasonographic visualization and assessment of the anterolateral ligament. Knee Surg Sports Traumatol Arthrosc. 2016 Jun 25.
Capo J, Kaplan DJ, Fralinger DJ, Gyftopolous S, Strauss EJ, Jazrawi LM, Alaia MJ. Femoral screw divergence via the anteromedial portal using an outside-in retrograde drill in bone-patella tendon-bone anterior cruciate ligament reconstruction: a cadaveric study. Arthroscopy. 2016 Sep 10.
Capo J, Shamah SD, Jazrawi L, Strauss E. Clinical outcomes of ACL reconstruction with tibialis anterior allograft using an anteromedial portal approach. Knee. 2016; 23: 1089–1092.
Capogna B, Ryan WE, McGee AW, Jazrawi LM. Coracoid fracture following Latarjet failure a case report. Bull Hosp Jt Dis (2013). 2016; 74: 318–322.
Capogna B, Strauss E, Konda S, Dayan A, Alaia M. Distal patellar tendon avulsion in association with high-energy knee trauma: a case series and review of the literature. Knee. 2016 Dec 1.
Capogna BM, Egol KA. Treatment of nonunions after malleolar fractures. Foot Ankle Clin. 2016; 21: 49–62.
Capriccioso CE, Zuckerman JD, Egol KA. Initial varus displacement of proximal humerus fractures results in similar function but higher complication rates. Injury. 2016; 47: 909–913.
Christiano AV, Pean CA, Konda SR, Egol KA. Predictors of patient reported pain after lower extremity nonunion surgery: the nicotine effect. Iowa Orthop J. 2016; 36: 53–58.
Clair AJ, Evangelista PJ, Lajam CM, Slover JD, Bosco JA, Iorio R. Cost analysis of total joint arthroplasty readmissions in a bundled payment care improvement initiative. J Arthroplasty. 2016; 31: 1862–1865.
Cuéllar VG, Cuéllar JM, Kirsch T, Strauss EJ. Correlation of synovial fluid biomarkers with cartilage pathology and associated outcomes in knee arthroscopy. Arthroscopy. 2016; 32: 475–485.
Davidovitch RI, DelSole EM, Vigdorchik JM. Subspine impingement: 2 case reports of a previously unreported cause of instability in total hip arthroplasty. Hip Int. 2016; 26: e24–29.
DelSole EM, Egol KA, Tejwani NC. Construct choice for the treatment of displaced, comminuted olecranon fractures: are locked plates cost effective? Iowa Orthop J. 2016; 36: 59–63.
Ding DY, Kanevsky R, Strauss EJ, Jazrawi LM. Anteromedialisation tibial tubercle osteotomy for recurrent patellar instability in young active patients: a retrospective case series. Injury. 2016; 47: 737–741.
Ding DY, Ryan WE, Strauss EJ, Jazrawi LM. Chronic distal biceps repair with an Achilles allograft. Arthrosc Tech. 2016; 5: e525–529.
Dundon JM, Bosco J, Slover J, Yu S, Sayeed Y, Iorio R. Improvement in total joint replacement quality metrics: year one versus year three of the Bundled Payments for Care Improvement Initiative. J Bone Joint Surg Am. 2016; 98: 1949–1953.
Elbuluk A, Deshmukh A, Inneh I, Iorio R. The present and future of genomics in adult reconstructive orthopaedic surgery. JBJS Rev. 2016; 4: e61–66.
Fralinger DJ, Kaplan DJ, Weinberg ME, Strauss EJ, Jazrawi LM. Biological treatments for tendon and ligament abnormalities: a critical analysis review. JBJS Rev. 2016; 4(6).
Frankel VH, Kaplan DJ, Egol KA. Biomechanics of fractures. Orthop Trauma. 2016; 30 (Suppl 2): S2–56.
Galos DK, Konda SR, Kaplan DJ, Ryan WE, Alaia MJ. Transosseous-equivalent repair for distal patellar tendon avulsion. Arthrosc Tech. 2016; 5: e385–389.
Gold HT, Slover JD, Joo L, Bosco J, Iorio R, Oh C. Association of depression with 90-day hospital readmission after total joint arthroplasty. J Arthroplasty. 2016; 31: 2385–2388.
Gross SC, Galos DK, Taormina DP, Crespo A, Egol KA, Tejwani NC. Can tibial shaft fractures bear weight after intramedullary nailing? A randomized controlled trial. J Orthop Trauma. 2016; 30: 370–375.
Hinds RM, Gottschalk MB, Strauss EJ, Capo JT. Trends in arthroscopic procedures performed during orthopaedic residency: an analysis of Accreditation Council for Graduate Medical Education case log data. Arthroscopy. 2016; 32: 645–650.
Hinds RM, Phillips D, Egol KA, Capo JT. Variation in pediatric orthopedic case volume among residents: an assessment of Accreditation Council for Graduate Medical Education case logs. J Pediatr Orthop B. 2016 Oct 27.
Inneh IA, Clair AJ, Slover JD, Iorio R. Disparities in discharge destination after lower extremity joint arthroplasty: analysis of 7924 patients in an urban setting. J Arthroplasty. 2016; 31: 2700–2704.
Iorio R. The future is here: bundled payments and International Statistical Classification of Diseases, 10th Revision. J Arthroplasty. 2016; 31: 931.
Jones RB, Wright TW, Zuckerman JD. Reverse total shoulder arthroplasty with structural bone grafting of large glenoid defects. J Shoulder Elbow Surg. 2016; 25: 1425–1432.
Kester BS, Williams J, Bosco JA, Slover JD, Iorio R, Schwarzkopf R. The association between hospital length of stay and 90-day readmission risk for femoral neck fracture patients: within a total joint arthroplasty bundled payment initiative. J Arthroplasty. 2016; 31: 2741–2745.
Khurana S, Davidovitch RI, Kwon YK, Zuckerman JD, Egol KA. Similar function and improved range of shoulder motion is achieved following repair of three- and four-part proximal humerus fractures compared with hemiarthroplasty. Bull Hosp Jt Dis (2013). 2016; 74: 212–218.
Konda SR, Davidovitch RI, Egol KA. Initial surgical treatment of humeral shaft fracture predicts difficulty healing when humeral shaft nonunion occurs. HSS J. 2016; 12: 13–17.
Konda SR, Goch AM, Leucht P, Christiano A, Gyftopoulos S, Yoeli G, Egol KA. The use of ultra-low-dose CT scans for the evaluation of limb fractures: is the reduced effective dose using ct in orthopaedic injury (REDUCTION) protocol effective? Bone Joint J. 2016; 98-B: 1668–1673.
Academic Activities
ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 27
Mahure SA, Mollon B, Shamah SD, Zuckerman JD, Kwon YW, Rokito AS. The incidence of subsequent surgery after outpatient arthroscopic rotator cuff repair. Arthroscopy. 2016; 32: 1531–1541.
Mahure SA, Mollon B, Yu S, Kwon YW, Zuckerman JD. Definitive treatment of infected shoulder arthroplasty with a cement spacer. Orthopedics. 2016; 39: e924–930.
Manoli A, Capriccioso CE, Konda SR, Egol KA. Total shoulder arthroplasty for proximal humerus fracture is associated with increased hospital charges despite a shorter length of stay. Orthop Traumatol Surg Res. 2016; 102: 19–24.
Mercuri JJ, Okey NE, Karia RJ, Gross RH, Zuckerman JD. Resident physician duty-hour requirements: what does the public think? J Am Acad Orthop Surg. 2016; 24: 789–795.
Mollon B, Mahure SA, Ding DY, Zuckerman JD, Kwon YW. The influence of a history of clinical depression on peri-operative outcomes in elective total shoulder arthroplasty: a ten-year national analysis. Bone Joint J. 2016; 98-B: 818–824.
Mollon B, Mahure SA, Ensor KL, Zuckerman JD, Kwon YW, Rokito AS. Subsequent shoulder surgery after isolated arthroscopic SLAP repair. Arthroscopy. 2016; 32: 1954–1962.
Mollon B, Mahure SA, Roche CP, Zuckerman JD. Impact of glenosphere size on clinical outcomes after reverse total shoulder arthroplasty: an analysis of 297 shoulders. J Shoulder Elbow Surg. 2016; 25: 763–771.
Naik AA, Hinds RM, Paksima N, Capo JT. Risk of injury to the dorsal sensory branch of the ulnar nerve with percutaneous pinning of ulnar-sided structures. J Hand Surg Am. 2016; 41: e159–163.
Odeh K, Doran J, Yu S, Bolz N, Bosco J, Iorio R. Risk-stratified venous thromboembolism prophylaxis after total joint arthroplasty: aspirin and sequential pneumatic compression devices vs aggressive chemoprophylaxis. J Arthroplasty. 2016; 31 (9 Suppl): 78–82.
Phillips DP, Zuckerman JD, Kalet A, Egol KA. Direct observation: assessing orthopaedic trainee competence in the ambulatory setting. J Am Acad Orthop Surg. 2016; 24: 591–599.
Ramme AJ, Gales J, Stevens N, Verma V, Egol K. Rumpel-Leede phenomenon in a patient with laboratory markers positive for Sjögren disease. A A Case Rep. 2016; 6: 352–354.
Ramme AJ, Iorio R, Smiaronksi J, Wronka A, Rodriguez G, Specht L, Chang G, Egol KA. Organizational and technical considerations for the implementation of a digital orthopaedic templating system. Bull Hosp Jt Dis (2013). 2016; 74: 254–261.
Regan DK, Gould S, Manoli A 3rd, Egol KA. Outcomes over a decade after surgery for unstable ankle fracture: functional recovery seen 1 year postoperatively does not decay with time. J Orthop Trauma. 2016; 30: e236–241.
Shue J, Karia RJ, Cardone D, Samuels J, Shah M, Slover JD. A randomized controlled trial of two distinct shared decision-making aids for hip and knee osteoarthritis in an ethnically diverse patient population. Value Health. 2016; 19: 487–493.
Shulman BS, Marcano AI, Davidovitch RI, Karia R, Egol KA. Nature's wrath-the effect of weather on pain following orthopaedic trauma. Injury. 2016; 47: 1841–1846.
Slover JD, Mullaly KA, Payne A, Iorio R, Bosco J. What is the best strategy to minimize after-care costs for total joint arthroplasty in a bundled payment environment? J Arthroplasty. 2016; 31: 2710–2713.
Strauss EJ, Day MS, Ryan M, Jazrawi L. Evaluation, treatment, and outcomes of meniscal root tears: a critical analysis review. JBJS Rev. 2016; 4(8).
Uquillas CA, Ward JP, Zuckerman JD. Total hip arthroplasty after proximal femoral osteotomy: a technique that can be used to address presence of a retained intracortical plate. Am J Orthop (Belle Mead NJ). 2016; 45: E224–226.
Wasserman BR, Singh BC, Kaplan DJ, Weinberg M, Meislin R, Jazrawi LM, Strauss EJ. Braking reaction time after right-knee anterior cruciate ligament reconstruction: a comparison of 3 grafts. Arthroscopy. 2016 Aug 25.
Williams J, Kester BS, Bosco JA, Slover JD, Iorio R, Schwarzkopf R. The association between hospital length of stay and 90-day readmission risk within a total joint arthroplasty bundled payment initiative. J Arthroplasty. 2016 Sep 28.
Yu S, Mahure SA, Branch N, Mollon B, Zuckerman JD. Impact of race and gender on utilization rate of total shoulder arthroplasty. Orthopedics. 2016; 39: e538–544.
Yu SW, Szulc AL, Walton SL, Davidovitch RI, Bosco JA, Iorio R. Liposomal bupivacaine as an adjunct to postoperative pain control in total hip arthroplasty. J Arthroplasty. 2016; 31: 1510–1515.
AMERICAN ACADEMY OF ORTHOPAEDIC SURGEONS (AAOS) ANNUAL MEETING 2016
Podium Presentations, Instructional Course Lectures, and Symposia
Diabetes as a Predictor for Extended Hospital Stay and Complications in Surgical CSM Patients—Nancy Worley, Cyrus Jalai, BA, Shaleen Vira, MD, Shenglin Wang, MD, Thomas J. Errico, MD, Michael C. Gerling, MD, Peter G. Passias, MD
Focal and Dynamic Cervical Alignment Correlates with Health-Related Quality of Life in Cervical Deformity Patients—Renaud Lafage,Virginie Lafage, PhD, Themistocles S. Protopsaltis, MD, Robert A. Hart, MD, Eric O. Klineberg, MD, Justin S. Smith, MD, Brian J. Neuman, MD, Christopher Ames, MD
A Novel Index for Quantifying the Surgical Risk for Patients with Cervical Spine Disorders—Peter G. Passias, MD, Bryan J. Marascalchi, MD, Bassel Diebo, MD, Nancy Worley, Cyrus Jalai, BA, Virginie Lafage, PhD
Prospective Multicenter Assessment of Early Complication Rates Associated with ACD Surgery in 78 Patients—Justin S. Smith, MD, Virginie Lafage, PhD, Christopher I. Shaffrey, MD, Themistocles S. Protopsaltis, MD, Peter G. Passias, MD, Eric O. Klineberg, MD, K D. Riew, MD, Christopher Ames, MD
Length of Stay and 30-Day Readmission Predictors in CSM Patients: Analysis of 3,057 ACS-NSQIP Patients—Peter G. Passias, MD, Cyrus Jalai, BA, Nancy Worley, Shaleen Vira, MD, Michael C. Gerling, MD, Virginie Lafage, PhD, Thomas J. Errico, MD
Predictors of Upper Body Post-Operative Pain/Disability in Surgical Cervical Radiculopathic Patients—Peter G. Passias, MD, Kristen E. Radcliff, MD, Robert E. Isaacs, MD, Kristina Bianco, Cyrus Jalai, BA, Paul M. Arnold, MD, Patrick C. Hsieh, MD, MSc, Alexander Vaccaro, MD, PhD
How to Reverse Reversomania: Arthroscopic Repair of Massive Cuff Tears— Laith Jazrawi, MD
How bundled payment works in my practice—Richard Iorio MD
Principles of Orthopaedic Leadership: Local, Regional, National—Joseph Zuckerman, MD
Cervical Spine Smackdown: Ask the Experts—Themistocles Protopsaltis MD
Elbow Arthritis in the Young Athlete—Laith Jazrawi, MD, Mandeep Virk, MD
Periarticular Fractures of the Tibia: The Case for Going Prone—Kenneth A. Egol, MD
Dynamometer Strength Testing Following Subpectoral Proximal Biceps Tenodesis with Cortical Button Fixation—Adam Lipman, MD, Steven Shamah, Alan W. McGee, MD, Maxwell Weinberg, MD, Eric J. Strauss, MD, Orrin H. Sherman, MD, Andrew J. Feldman, MD, Laith M. Jazrawi, MD
Fractures of the Proximal Femur: A Case-based Approach—Kenneth A. Egol, Roy Davidovitch, MD, Sanjit Konda, MD, Phillip Leucht, MD
Tibial Plateau Functional Outcome Score Identifies Patients at Risk of Diminished Functional Outcome—Sanjit R. Konda, MD, Arthur Manoli III, MD, Roy Davidovitch, MD , Kenneth A. Egol, MD
Low Intensity Pulsed Ultrasound in Acute Tibial Shaft Fractures Treated with IM Nails: The Results of the TRUST Trial—Thomas A. Einhorn, MD
The Effect of Knee Flexion Contracture on Outcomes of Distal Femur Fractures—Kenneth A. Egol, MD
Differences in Cost and Length of Stay for Hip, Distal Femoral, and Pelvic Fractures—Kenneth A. Egol, MD, Sanjit Konda, MD
Relationship Status Affects the Discharge Location for Trauma Patients—Kenneth A. Egol, MD, Sanjit Konda, MD
The Relationship Between Hospital Payer Mix and Volume Growth in Total Joint Arthroplasty—Anthony A. Catanzano, MD, Raj Karia, MPH, Joseph A. Bosco III, MD
Pitfalls in the Operative Management of Common Shoulder Problems: How to Avoid and What To Do When They Occur—Joseph Zuckerman, MD, Andrew Rokito, MD
Preventing Hospital Readmissions and Limiting the Complications Associated with Total Hip Arthroplasty--Optimizing Patient Health Perioperatively and Preventing Readmission—Richard Iorio, MD
Practical Tips for Implementing Bundled Payments in Your Practice-- Strategies and Tactics for Successful Implementation of Bundled Payments Richard Iorio, MD
From the Glenoid to the Radial Tuberosity - Management of Biceps Pathology— To understand open and arthroscopic approaches to long head of the biceps tendon

28 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
tenodesis, with an emphasis on outcomes, value, and complications in 2016—Eric Strauss, MD, Laith Jazrawi MD
Reverse Total Shoulder Arthroplasty Outcomes With and Without Repair of the Subscapularis—Richard J. Friedman, MD, Pierre-Henri Flurin, MD, Thomas W. Wright, MD, Joseph D. Zuckerman, MD, Christopher Roche, MBA
Comparison of Outcomes with Reverse Total Shoulder Arthroplasty in Patients With and Without Scapular Notching—Joseph D. Zuckerman, MD, Lynn A. Crosby, MD, Pierre-Henri Flurin, MD, Thomas W. Wright, MD, Christopher Roche, MS, MBA
Reverse Shoulder Outcomes with Scapular Deformities: Augmented Glenoid Baseplates vs. Bone Grafting—Thomas W. Wright, MD, Richard B. Jones, MD, Pierre-Henri Flurin, MD, Joseph D. Zuckerman, MD, Christopher Roche, MD
Incidence of Unplanned Admission from an Outpatient Orthopaedic Surgery Center—Michael S. Day, MD, Germaine Cuff, PhD, RN, Hersh Shroff, MD, Lorraine Hutzler, BA, Samir Kendale, MD, Jeanna D. Blitz, MD
Comparison of Perioperative Times at an Ambulatory Surgery Center and an Outpatient Facility Andrew D. Rosenberg, MD, Joseph A. Bosco III, MD
Improvement in TJA Quality Metrics: Year One vs. Year Three of the Bundled Payment for Care Initiative—Richard Iorio, MD, Joseph D. Zuckerman, MD, Joseph A. Bosco III, MD, James D. Slover, MD, Stephen Yu, MD, John M. Dundon, MD, Yousuf Sayeed SR, MS
Joint Replacement Surgical Home: Impact of Patient Characteristics and Comorbidities on Length of Stay—Ran Schwarzkopf, MD, Kyle S. Ahn, MD, Joseph B. Rinehart, MD, Maxime Cannesson, Zeev Kain, MD, MBA
Ultra Low Dose Computed Tomography Scanning: A Reliable Modality with an Improved Patient Safety Profile—Sanjit R. Konda, Abraham M. Goch, Philipp Leucht, MD, Anthony V. Christiano, Soterios Gyftopoulos, Kenneth A. Egol, MD
Inpatient Rehabilitation Following Hip Fracture: Recent Trends and Implications for Post-Acute Care Reform—Arthur Manoli III, MD, Sanjit R. Konda, MD, Christian A. Pean, MS, Kenneth A. Egol, MD
The Effect of Severity of Illness on Spine Surgery Costs Across New York State Hospitals—Ian Kaye, MD, Lorraine Hutzler, BA, Joseph A. Bosco III, MD
Risk Factors for Subsequent Surgery after ACL Reconstruction: A Population-Based Study—Siddharth A. Mahure, MD, Brian Capogna, MD, Brent Mollon, MD, FRCSC, Orillia, Ontario, Canada, Andrew S. Rokito, MD
Discrepancies in Planned Sagittal Alignment and Age-Adjusted Ideals: Implications of Over- or Under-Correction—Jensen Henry, BA, Matthew A. Spiegel, BA, Jonathan H. Oren, MD, Isaac Gammal, BA, Cyrus Jalai, BA, Themistocles S. Protopsaltis, MD, Thomas J. Errico, MD, Virginie Lafage, PhD
Chain of Relaxation: How Sagittal Correction Affects Spino-Pelvic, Lower Limb, and Global Alignment—Jonathan H. Oren, MD, Shaleen Vira, MD, Barthelemy Liabaud, MD, Bassel Diebo, MD, Matthew A. Spiegel, BA, Renaud Lafage, Thomas J. Errico, MD, Frank J. Schwab, MD, Virginie Lafage, PhD
Age-Adjusted Alignment Goals Have the Potential to Reduce Proximal Junction Kyphosis—Frank J. Schwab, MD, Renaud Lafage, Steven D. Glassman, MD, Robert S. Bess, MD, Robert A. Hart, MD, Douglas C. Burton, MD, Han Jo Kim, MD, Virginie Lafage, PhD
Defining the Role of Lower Limbs in Compensating for Sagittal Malalignment—Renaud Lafage, Barthelemy Liabaud, MD, Bassel Diebo, MD, Jonathan H. Oren, MD, Shaleen Vira, MD, Themistocles S. Protopsaltis, MD, Thomas J. Errico, MD, Frank J. Schwab, MD, Virginie Lafage, PhD
Unlocking T1 Pelvic Angle’s Clinical and Sagittal Significance by Analyzing Its Relation to Pelvic Tilt— Barthelemy Liabaud, MD, Renaud Lafage, Jonathan H. Oren, MD, Shaleen Vira, MD, Bassel Diebo, MD, Themistocles S. Protopsaltis, MD, Thomas J. Errico, MD, Frank J. Schwab, MD, Virginie Lafage, PhD
Reliability of Intraoperative Prone Lateral Radiographs in Predicting Postoperative Standing Sagittal Alignment—Wesley Bronson, MD, Themistocles S. Protopsaltis, MD, Barthelemy Liabaud, MD, Gregory M. Mundis, MD, Jeffrey Gum, MD, Douglas C. Burton, MD, Frank J. Schwab, MD, Virginie Lafage, PhD
Brushing Up on Your Test-Taking Skills—Joseph Bosco
Adult Spinal Deformity: Surgical Planning and Complications—Thomas Errico, MD, Themistocles Protopsaltis, MD, Robert Bess, MD
Hospital Specific Hip Arthroplasty Surgical Site Infection Rates do Not Correlate with Other Procedure SSI Rates—Ravi Vaswani, BS, Raj Karia, MPH, Lorraine Hutzler, BA, Joseph A. Bosco III, MD
Regional Anesthesia Only for Clavicle Fracture Open Reduction Internal Fixation is Safe and Effective—Devon J. Ryan, BA, Kenneth A. Egol, MD
Total Shoulder Arthroplasty for Proximal Humerus Fracture is Associated with Increased Hospital Charges—Arthur Manoli III, MD, Sanjit R. Konda, MD, Christina Capriccioso, BS, Kenneth A. Egol, MD
Development of a Preoperative ASD Frailty Index that Correlates to Common Quality and Value Metrics—Amit Jain, MD, Daniel Sciubba, MD, Baltimore, Maryland, Khaled Kebaish, MD, Brian J. Neuman, MD, Robert S. Bess, MD, Christopher Ames, MD
When Does Compensation for Lumbar Stenosis Become a Clinical Sagittal Plane Deformity?—Aaron Buckland, FRACS, MD, Shaleen Vira, MD, Jonathan H. Oren, MD, Renaud Lafage, Bassel Diebo, MD, Themistocles S. Protopsaltis, MD, Frank J. Schwab, MD, Virginie Lafage, PhD, John A. Bendo, MD
Center Variability in Surgical Technique and Outcomes in Adult Spinal Deformity—Thomas Cheriyan, Munish C. Gupta, MD, Renaud Lafage, Justin S. Smith, MD, Robert S. Bess, MD, Robert A. Hart, MD, Richard A. Hostin, MD, Virginie Lafage, PhD
Clinical Outcomes of Hip Arthroscopy in Patients Over 60—Brian Capogna, MD, John Begly, MD, Michael Ryan, MD, Kristofer E. Chenard, MD, Rajkishen Narayanan, MS, Thomas Youm, MD
Adult Lumbar Scoliosis: State-of-the-Art Treatment (Operative and Nonoperative) —Themistocles Protopsaltis
The Management of Meniscal Pathology: From Partial Meniscectomy to Transplantation—Eric Strauss, MD, Laith Jazrawi, MD
Adult Lumbar Disc Herniation: Treatment, Complications, Outcomes, and Evidence-Based Data for Patient and Health Professional Counseling—Peter Passias MD
Realignment Planning in Adult Spinal Deformity: The Newest Tools, Formulas, and Techniques to Get it Right—Robert S. Bess, MD, Themistocles Protopsaltis, MD
Preoperative Optimization of Total Joint Arthroplasty Surgical Risk—Richard Iorio, MD, Moderator
Cardiovascular Disease and Stroke Prevention—James D. Slover, MD
Joint Preservation Techniques for the Knee in 2016--Technical pearls for performing combined cartilage restoration, meniscus transplantation, ligament reconstruction, and/or realigning osteotomies—Eric Strauss, MD
Is it the Back or the Hip? Differentiating Lumbar Spine from Hip Pathologies: Key Points of Evaluation and Treatment—Afshin Razi, MD, Moderator
Degenerative hip disorders or painful total hip replacement with back pain— James D. Slover, MD
Challenges in spinal deformity and hip arthritis—Aaron Buckland, FRACS
Ask An Expert: Shoulder and Elbow—Joseph Zuckerman, MD
Fitness Tracking Devices: Applications in Orthopaedics—Dalibel M. Bravo, MD, Stephanie Swensen, MD, Claudette M. Lajam, MD
Knee Society/AAHKS: Minimizing TKA Complications—Richard Iorio, MD
Hip Society/AAHKS: Complex Primary THA: Case-Based Discussion on the State of the Art—Richard Iorio, MD
International Society for the Advancement of Spine Surgery: Hype and Marketing— Jeffrey Goldstein, MD
Knee Society/AAHKS Session V: Highlights—W.N. Scott, MD
Posters/Video/ Multimedia Presentations
3D-MRI versus 3D-CT in the Evaluation of Osseous Anatomy in Femoroacetabular Impingement and Hip Dysplasia—Jonathan Vigdorchik, MD, Nima Eftekhary, MD, Avner Yemin, MD, Roy Davidovitch, MD, Michael C. Bloom, MD, Soterios Gyftopoulos, MD
Establishing a Pragmatic Knee Preservation Registry to Follow Patients with Degenerative Joint Disease—Stephen Yu, MD, Alessandra Szulc, MA, Elisha Lee, Xiang Zhou, PhD, Raj Karia, MPH, Eric J. Strauss, MD, Laith M. Jazrawi, MD, Richard Iorio, MD, Philip Band, PhD
Knee Arthroscopy in the Setting of Degenerative Arthritis—Jason P. Hochfelder, MD, Jiho Han, W N. Scott, MD, William J. Long, MD
Biomechanical Evaluation of Four Internal Fixation Constructs for Scaphoid Fractures—Bryan Beutel, MD, Eitan Melamed, MD, Richard M. Hinds, MD, Michael B. Gottschalk, MD, John T. Capo, MD
End Tidal Carbon Dioxide (ETCO2) Predicts Pulmonary Embolism in Postoperative Orthopaedic Patients—Austin Ramme, MD, PhD, Alana E. Sigmund, MD, Eduardo Iturrate, MD, Lorraine Hutzler, BA, Ezra E. Dweck, David J. Steiger, MD, Joseph A. Bosco III, MD
Psychiatric Conditions Impact 90-Day Hospital Readmission Rates Following Total Joint

ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 29
Replacement—Heather Gold, James D. Slover, MD, Lijin Joo, MA,Joseph A. Bosco III, MD, Richard Iorio, MD, Cheongeun Oh, PhD
Socioeconomic Status Independently Affects HCAHPS Scores—Brandon Shulman, MD, Brooks Crowe, BA, Lorraine Hutzler, BA, Joseph A. Bosco III, MD
Predictors for Hospital Readmission Within Two Years Following Adult Spinal Deformity Surgery—Peter G. Passias, MD, Eric O. Klineberg, MD, Cyrus Jalai, BA, Nancy Worley, MS, Alexandra Soroceanu, MD, Themistocles S. Protopsaltis, MD, Virginie Lafage, PhD
Unilateral versus Bilateral Instrumentation in Transforaminal Lumbar Interbody Fusion: A Meta-Analysis—Thomas Cheriyan, Virginie Lafage, PhD, Sonali Narang, BA, Steven Samrock, BA, Bradley Y. Harris, JD, Jeffrey A. Goldstein, MD, John A. Bendo, MD, Frank J. Schwab, MD, Thomas J. Errico, MD
Predicting Extended Length of Hospital Stay in an Adult Spinal Deformity Surgical Population—Eric O. Klineberg, MD, Peter G. Passias, MD, Cyrus Jalai, BA, Nancy Worley, MS, Robert A. Hart, MD, Daniel Sciubba, MD, Douglas C. Burton, MD
Development of New Onset Cervical Deformity in Non-Operative ASD Patients With Three-Year Follow Up—Peter G. Passias, MD, Cyrus Jalai, BA, Nancy Worley, MS, Renaud Lafage, Virginie Lafage, PhD, Christopher Ames, MD, Eric O. Klineberg, MD
CSM Surgery Complication Rates, Predictors of Their Development, and Effect on Outcomes at Two Years—Michael C. Gerling, MD, Peter G. Passias, MD, Shaleen Vira, MD, Kristina Bianco, Nancy Worley, MS, Cyrus Jalai, BA, Cheongeun Oh, PhD, Alexander Vaccaro, MD, PhD
Chronic Conditions Associated with Reoperation After Adult Lumbar Fusion Surgery—Justin Paul, MD
Predicting Cervical Curvature Required for Horizontal Gaze; Implication for Cervical and Thoracolumbar Surgeons—Bassel Diebo, MD, Shaleen Vira, MD, Jonathan H. Oren, MD, Barthelemy Liabaud, MD, Renaud Lafage,Themistocles S. Protopsaltis, MD, Thomas J. Errico, MD, Frank J. Schwab, MD, Virginie Lafage, PhD, Lonner, MD, Thomas J. Errico, MD
Predictive Model for Cervical Alignment Following Surgical Correction of Adult Spinal Deformity—Peter G. Passias, MD, Cheongeun Oh, PhD, Cyrus Jalai, BA, Nancy Worley, MS, Renaud LafageVirginie Lafage, PhD, Christopher Ames, MD
Adult Spinal Deformity: National Trends in the Treatment and Perioperative Outcomes from 2003-2010—Peter G. Passias, Cyrus Jalai, BA, Nancy Worley, MS, Shaleen Vira, MD, Bryan J. Marascalchi, MD, Virginie Lafage, PhD, Thomas J. Errico, MD
Novel Index to Quantify the Surgical Risk in Adult Spinal Deformity: 10,912 Patients from National Inpatient Sample—Bassel Diebo, MD, Vincent Challier, MD, Bryan J. Marascalchi, MD, Cyrus Jalai, BA, Nancy Worley, MS, Virginie Lafage, PhD,Peter G. Passias, MD
Performance Outcomes After Metacarpal Fractures in National Basketball Association Players—Michael S. Guss, MD, John Begly, MD, Austin Ramme, MD, Richard M. Hinds, MD, Raj Karia, MPH, John T. Capo, MD
Fracture Repair in Hemodialysis Patients is Associated with Higher Complication Rate and Worse Quality Measures—Ravi Vaswani, BS, Arthur Manoli III, MD, Kenneth A. Egol, MD
Microdialysis Detects Ischemic Change Early in the Evolution of Acute Compartment Syndrome—Alexander Crespo, MD, Sanjit R. Konda, MD, Abraham M. Goch, Kenneth A. Egol, MD
Hip Fracture Treatment at Orthopaedic Teaching Hospitals: Better Care at a Lower Cost—Sanjit R. Konda, MD, Arthur Manoli III, MD, Karan S. Patel, Kenneth A. Egol, MD
Advanced Arthroplasty Techniques for Acetabular Component Placement in Dysplastic Hips—Amy Wasterlain, MD, Nicole Wake, MS, Maxwell Weinberg, MD, Jonathan Vigdorchik, MD
LIMA: Lifetime Initiative for the Management of Arthritis (LIMA): Understanding Arthritis as a Disease State—Richard Iorio, MD, Alessandra Szulc, MD, Philip Band, PhD, Thomas A. Einhorn, MD, Joseph A. Bosco III, MD, Laith M. Jazrawi, MD, James D. Slover, MD, Raj Karia, Joseph D. Zuckerman, MD
Distal Radius Fractures: Tips to Prevent Complications and Management if They Occur—Christopher Klifto, MD, Michael S. Guss, MD, Anthony Sapienza, MD, Syngil S. Yang, MD, John T. Capo, MD, Nader Paksima, DO, Kevin M. Klifto, MD
3D Printing: The Latest Innovations and Applications in Orthopaedic Surgery—Stephen Yu, MD, Hamadi Murphy, Austin Ramme, MD, PhD, Richard Iorio, MD, Peter S. Walker, PhD, Jonathan Vigdorchik, MD
Osteoporosis and the Orthopaedic Surgeon's Role—Arthur Manoli III, MD, Roy Davidovitch, MD, Nirmal C. Tejwani, MD, Frank A. Liporace, MD, Sanjit R. Konda, MD, Kenneth A. Egol, MD
Occupational Hazards of Orthopaedic Surgery: What's Known, What's Not, and How
to Protect Ourselves—Rachel S. Rohde, MD, Claudette M. Lajam, MD, Julie E. Adams, MD, Jennifer M. Wolf, MD
Total Disc Arthroplasty: The Current and Future Use of an Evolving Technology in Spine Surgery—Saqib Hasan, MD, Karan S. Patel, MD, Wesley Bronson, MD, William Ryan, BS, Themistocles S. Protopsaltis, MD, Jeffrey A. Goldstein, MD, Thomas J. Errico, MD
MRI Physics: What Every Orthopaedic Surgeon Should Know—Stephanie Swensen, MD, Michael S. Day, MD, Maxwell Weinberg, MD, Michael J. Alaia, MD, Gregory Chang, MD, Michael Recht, MD, Eric J. Strauss, MD, Laith M Jazrawi, MD
The Weak Link in ACL Reconstruction: A Guide to Graft Fixation Device Selection. —Maxwell Weinberg, MD, Christopher Looze, MD, Steven Shamah, Michael J. Alaia, MD, Guillem Gonzalez-Lomas, Eric J. Strauss, MD, Laith M. Jazrawi, MD
Update on Fracture Nonunion: State of the Art 2016—Anthony V. Christiano, Abraham M. Goch, Philipp Leucht, MD, Sanjit R. Konda, MD, Kenneth A. Egol, MD
Scapular Fractures: From Bankart to Body—Michael S. Day, MD, William Ryan, BS, Maxwell Weinberg, MD, Michael J. Alaia, MD, Eric J. Strauss, MD, Kenneth A. Egol, MD, Laith M. Jazrawi, MD
Evaluation and Management of Pediatric Bone Lesions—Alan T. Blank, MD, MS, Daniel M. Lerman, Norman Y. Otsuka, MD, Timothy Rapp, MD
Rectus Femoris Repair with Anterior-Inferior Iliac Spine Debridement—Guillem Gonzalez-Lomas, MD, Daniel J. Kaplan, BA, Natalie Danna, MD, David Fralinger, MD, Michael J. Alaia, MD, Roy Davidovitch, MD, Laith M. Jazrawi, MD
Chronic Quadriceps Tendon Reconstruction—Michael J. Alaia, MD, Daniel J. Kaplan, BA, William Ryan, BS, Maxwell Weinberg, MD, Guillem Gonzalez-Lomas, MD, Eric J. Strauss, MD, Robert J. Meislin, MD, Laith M. Jazrawi, MD
Chronic Patellar Tendon Reconstruction—Michael J. Alaia, MD, Jason Capo, MD, Brian Capogna, MD, Daniel J. Kaplan, BA, William Ryan, BS, David Fralinger, MD, Eric J. Strauss, MD, Laith M. Jazrawi, MD
Repair of a Patellar Chondral Lesion in the Setting of an Increased TT-TG—Jason Capo, MD, Daniel J. Kaplan, BA, William Ryan, BS, David Fralinger, MD, Thomas Youm, MD
Chronic Patellar Instability with Large Chondral Defect—Guillem Gonzalez-Lomas, MD, Daniel J. Kaplan, BA, Sergio A. Glait, MD, William Ryan, BS, David Fralinger, MD, Robert J. Meislin, MD, Eric J. Strauss, MD, Laith M. Jazrawi, MD
Extra-Articular Augmentation for the Failed ACL:ALL Reconstruction Sergio A. Glait, MD, Daniel J. Kaplan, BA, William Ryan, BS, Amy Kaplan, BS, Michael J. Alaia, MD, Eric J. Strauss, MD, Laith M. Jazrawi, MD
Lateral Collateral Ligament Reconstruction Using Docking Technique—Sergio A. Glait, MD, Daniel J. Kaplan, BA, William Ryan, BS, David Fralinger, MD, Guillem Gonzalez-Lomas, MD, Eric J. Strauss, MD Laith M. Jazrawi, MD
Biomechanics of Fractures—Victor H. Frankel, MD, Daniel J. Kaplan, BA, Kenneth A. Egol, MD
Pectoralis Major Tendon Repair: Brief Review and Surgical Technique—Jason Capo, MD, Brent Mollon, MD, Sergio A. Glait, MD, Daniel J. Kaplan, BA, William Ryan, BS, Andrew S. Rokito, MD
Arthroscopically Assisted Acromioclavicular/Coracoclavicular Joint Reconstruction of the Shoulder—Jason Capo, MD, John Begly, MD, Daniel J. Kaplan, BA, William Ryan, BS, Amy Kaplan, BS, Laith M. Jazrawi, MD, Robert J. Meislin, MD
Rotator Cuff Repair Using Collagen Based Bioinductive Implant—Jason Capo, MD, John Begly, MD, Daniel J. Kaplan, BA,William Ryan, BS, David Fralinger, MD, Eric J. Strauss, MD, Robert J. Meislin, MD,
Ulnar Collateral Ligament Reconstruction - Modified Jobe Approach using Docking Technique—Sergio A. Glait, MD, Daniel J. Kaplan, BA, William Ryan, BS, Maxwell Weinberg, MD, Michael J. Alaia, MD, Guillem Gonzalez-Lomas, MD, Laith M. Jazrawi, MD
Management of Glenoid Bone Loss in Shoulder Arthroplasty—Michael S. Guss, MD, William Ryan, BS, Daniel J. Kaplan, BA, Brent Mollon, MD, Kirk A. Campbell, MD, Young W. Kwon, MD, PhD, Joseph D. Zuckerman, MD
Open Shoulder Stabilization using Humeral and Distal Tibial Allografts—Jason Capo, MD Michael Ryan, MD, Daniel J. Kaplan, BA, William Ryan, BS, David Fralinger, MD, Andrew S. Rokito, MD
French-Door (Double-Door) Laminoplasty—Daniel J. Kaplan, BA, Christine Choi, BS, MS, Themistocles S. Protopsaltis, MD
30 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
Edward M. Adler, MD New York Metro Area’s Top Doctors, Castle Connolly
O. Alton Barron, MD New York Metro Area’s Top Doctors, Castle Connolly
John A. Bendo, MD New York Metro Area’s Top Doctors, Castle Connolly
Joseph A. Bosco, MD New York Metro Area’s Top Doctors, Castle Connolly
Louis W. Catalano, MD New York Metro Area’s Top Doctors, Castle Connolly
Cary B. Chapman, MD New York Metro Area’s Top Doctors, Castle Connolly
Roy I. Davidovitch, MD New York Metro Area’s Top Doctors, Castle Connolly
Kenneth A. Egol, MD New York Metro Area’s Top Doctors, Castle Connolly
Thomas J. Errico, MD America’s Top Doctors, Castle Connolly
Steven Z. Glickel, MD America’s Top Doctors, Castle Connolly
David H. Godfried, MD New York Metro Area’s Top Doctors, Castle Connolly
Jeffrey A. Goldstein, MD America’s Top Doctors, Castle Connolly
Salil Gupta, MD New York Metro Area’s Top Doctors, Castle Connolly
Richard Iorio, MD Frank Stinchfield Research Award, The Hip Society • Richard Kilfoyle Award, Winning Manuscript, New England Orthopaedic Society • Chairman, Advanced APM Development Committee, American Association of Hip and Knee Surgeons • Chairman, Advocacy Committee, American Association of Hip and Knee Surgeons • New York Metro Area’s Top Doctors, Castle Connolly
Laith M. Jazrawi, MD New York Metro Area’s Top Doctors, Castle Connolly
Patrick A. Meere, MD
Awards & Recognition

ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 31
Thomas Errico, MD, and Anthony Frempong-Boadu, MD
Yong H. Kim, MD New York Metro Area’s Top Doctors, Castle Connolly
William L. King, MD New York Metro Area’s Top Doctors, Castle Connolly
Vijay John Mani, MD New York Metro Area’s Top Doctors, Castle Connolly
Patrick A. Meere, MD America’s Top Doctors, Castle Connolly • Best Podium Presentation, Conference for Computer Assisted Orthopaedic Surgery International
Robert J. Meislin, MD New York Metro Area’s Top Doctors, Castle Connolly
Nader Paksima, DO, MPH New York Metro Area’s Top Doctors, Castle Connolly
Martin Posner, MD Lifetime Achievement Award, New York Society for Surgery of the Hand (NYSSH)
Andrew E. Price, MD New York Metro Area’s Top Doctors, Castle Connolly
Craig S. Radnay, MD New York Metro Area’s Top Doctors, Castle Connolly
Timothy B. Rapp , MD New York Metro Area’s Top Doctors, Castle Connolly
Keith B. Raskin, MD America’s Top Doctors, Castle Connolly
Michael E. Rettig, MD New York Metro Area’s Top Doctors, Castle Connolly
Donald J. Rose, MD New York Metro Area’s Top Doctors, Castle Connolly
Anthony Sapienza , MD Member, ER Committee, American Society for Surgery of the Hand (ASSH)
Ran Schwarzkopf, MD The Lawrence D. Dorr Surgical Techniques & Technologies Award, American Association of Hip and Knee Surgeons
W. Norman Scott, MD Lifetime Achievement Award, Arthritis Foundation
Steve Sheskier, MD New York Metro Area’s Top Doctors, Castle Connolly
Jeffrey M. Spivak, MD Leon L. Wiltse Research Award, International Society for the Advancement of Spine Surgery • America’s Top Doctors, Castle Connolly
Jonathan R. Stieber, MD New York Metro Area’s Top Doctors, Castle Connolly
Eric J. Strauss, MD Traveling Fellow, American Orthopaedic Association’s American-British- Canadian (ABC)
Steven A. Stuchin, MD America’s Top Doctors, Castle Connolly
Nirmal C. Tejwani, MD Board member, Orthopaedic Trauma Association (OTA)
Jonathan Vigdorchik, MD Insall Knee Traveling Fellowship
Peter S. Walker, PhD Best Podium Presentation, Conference for Computer Assisted Orthopaedic Surgery International
S. Steven Yang, MD, MPH New York Metro Area’s Top Doctors, Castle Connolly
Thomas Youm, MD New York Metro Area’s Top Doctors, Castle Connolly
Joseph D. Zuckerman, MD America’s Top Doctors, Castle Connolly Most Impactful Chairs of Last 20 Years, Academic Orthopaedic Consortium

32 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
As of December 2016
Located in the heart of Manhattan, with additional facilities throughout the New York City area, NYU Langone Medical Center consists of five hospitals and a growing outpatient network that brings our world-class medical services directly to the communities where our patients live and work.
NYU Langone’s Department of Orthopaedic Surgery cares for patients throughout the NYU Langone campus, including five flagship facilities:
Hospital for Joint Diseases, New York, NY This 190-bed hospital is the premier inpatient facility of the Department of Orthopaedic Surgery and the cornerstone of its patient safety and quality initiatives.
NYU Langone Medical Center, New York, NY A variety of inpatient and outpatient orthopaedic services are provided at NYU Langone’s 705-bed, flagship acute care hospital, including emergency orthopaedic services in the Ronald O. Perelman Center for Emergency Services.
Center for Musculoskeletal Care, New York, NY With 110,000 square feet of state-of-the-art space, NYU Langone’s premier facility for outpatient musculoskeletal care encompasses orthopaedics, rheumatology, rehabilitation, musculoskeletal radiology, and pain management.
Outpatient Surgery Center, New York, NY NYU Langone’s 22,000-square-foot cutting- edge facility focuses on ambulatory orthopaedic procedures, including shoulder, elbow, wrist, and hand surgeries, knee and ankle arthroscopies, ACL reconstruction, rotator cuff repair, and fracture fixation, among others.
NYU Lutheran Medical Center, Brooklyn, NY Affiliated with NYU Langone since April 2015 and merged as of January 2016, NYU Lutheran offers Brooklyn residents convenient access to high-quality healthcare.
Locations
For more information about our locations, visit, nyulangone.org/locations
MANHATTAN
BRONX
NJ
STATENISLAND
QUEENS
WESTCHESTER
CT
BROOKLYN
Long Island
8 additional locations in Westchester
2 additional locations in New Jersey
6 additional locations in Staten Island
8 additional locations in
Department of Orthopaedic Surgery
NYU Langone Medical Center

ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 33
Faculty & Leadership
Joseph A. Bosco, MD, and Joseph D. Zuckerman, MD
Department Leadership
Joseph D. Zuckerman, MD
Walter A.L. Thompson Professor of Orthopaedic Surgery; Chair of the Department of Orthopaedic Surgery
Phone: 212.598.6674
Email: [email protected]
Joseph A. Bosco, MD
Vice Chair of Clinical Affairs
Phone: 646.501.7042
Email: [email protected]
Gail S. Chorney, MD
Vice Chair for Professional Practice
Director, Center for Musculoskeletal Care; Director, Hospital for Joint Diseases Ambulatory Care Services
Phone: 646.501.7171
Email: [email protected]
Kenneth A. Egol, MD
Vice Chair of Education and Chief of the Division of Trauma & Fracture
Phone: 212.598.3889
Email: [email protected]
William L. Jaffe, MD
Vice Chair
Phone: 212.598.6796
Email: [email protected]
Thorsten Kirsch, PhD
Vice Chair of Research
Phone: 212.598.6589
Email: [email protected]
Thomas R. Lyon, MD
Vice Chair, NYU Lutheran
Phone: 718.630.7000
Email: [email protected]
Dennis A. Cardone, DO
Chief, Primary Care Sports Medicine Division
Pablo Castañeda, MD
Chief, Pediatric Orthopaedic Division
Thomas J. Errico, MD
Chief, Spine Division
Richard Iorio, MD
Chief, Joint Replacement and Adult Reconstructive Division
Laith M. Jazrawi, MD
Chief, Sports Medicine Division
Toni M. Mclaurin, MD
Clinical Site Chief, Bellevue Hospital Center
Kenneth J. Mroczek, MD
Chief, Foot and Ankle Division
Paul J. Ort, MD
Clinical Site Chief, Manhattan Veterans Affairs (VA) Medical Center
Nader Paksima, DO, MPH
Clinical Site Chief, Jamaica Hospital Medical Center
Martin Posner, MD
Chief, Hand Division
Timothy B. Rapp, MD
Chief, Oncology Division
Andrew S. Rokito, MD
Chief, Shoulder and Elbow Division
James D. Slover, MD
Clinical Site Chief, Hospital for Joint Diseases
Nirmal C. Tejwani, MD
Clinical Site Chief, Tisch Hospital
34 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
Full Faculty List
Adult Reconstructive
Richard Iorio Chief
Edward AdlerAlan J. DayanAjit J. DeshmukhThomas A. Einhorn Joseph FelicciaIvan Fernandez-MadridPhilip A. FontanettaRobert S. GoldsteinJames GurtowskiWilliam L. JaffeMichael N. KangClaudette M. LajamJustin G. LamontPeter R. LanganNachum LevinJohn C. L’insalataWilliam J. LongVijay J. ManiScott E. MarwinPatrick A. MeereRobert L. MichaelsGregory MontalbanoPaul J. OrtMukund R. PatelParthiv RathodSteven J. RavichHank RossRan SchwarzkopfW. Norman ScottErnesto D. SeldmanJeffrey ShapiroJames D. Sloverthaddeus SpakSteven StruhlSteven A. StuchinVladimir TressJonathan VigdorchikRaymond B. WalshOskar WegLori G. WeiserArnold B. WilsonThomas YoumJoseph D. Zuckerman
Pediatric Orthopaedic Surgery
Pablo Castañeda Chief
David H. Godfried Director, Center for Children
Gail S. ChorneyAlice ChuDavid S. FeldmanJenny M. FrancesSamara FriedmanMara KaramitopoulisDavid Y. Lin
Vivek NatarajanDonna P. PhillipsAndrew E. PriceJoshua Strassberg
Spine
Thomas J. Errico Chief
Roger AntoineJohn A. BendoAaron J. BucklandAlexandre B. De MouraJoseph W. DryerLeon K. EisenJason M. GallinaMichael C. GerlingJeffrey A. GoldsteinYong H. KimJeffrey D. KleinAngel E. MacagnoRonald MoskovichJonathan H. OrenPeter G. PassiasCarl B. PaulinoJeffrey PerryAnthony M. PetrizzoThemistocles ProtopsaltisJoseph S. PyunMartin QuirnoAfshin E. RaziMark A. RiegerJeffrey M. SpivakJonathan R. Stieber
Sports Medicine
Laith M. Jazrawi Chief
Michael J. AlaiaJoseph A. BoscoKirk A. CampbellCraig M. CapeciAdam B. CohenAndrew J. FeldmanJoshua B. FrankCalogero GambinoRamesh H. GidumalGuillem Gonzalez-LomasStuart J. HershonJames M. KipnisJerry LublinerRobert J. MeislinDavid S. MencheDavid S. PereiraAndrew S. RokitoDonald J. RoseMehul R. ShahOrrin H. ShermanJonathan J. SilverMarc SilvermanStuart SpringerDrew A. SteinEric J. StraussBradley R. WassermanDavid S. Weiss
Alice Chu, MD
ORTHOPAEDIC SURGERY / NYU LANGONE MEDICAL CENTER 35
Primary Care Sports Medicine
Dennis A. Cardone Chief
Bret C. JacobsWarren K. Young
Shoulder And Elbow
Andrew S. Rokito Chief
Laith M. JazrawiYoung W. KwonRobert J. MeislinTimothy G. ReishMandeep S. VirkJean S. YunJoseph D. Zuckerman
Trauma And Fracture
Kenneth A. Egol Chief
Roy I. DavidovitchSanjit R. KondaPhilipp LeuchtFrank A. LiporaceThomas R. LyonToni M. MclaurinNirmal C. TejwaniAldo Vitale
Orthopaedic Oncology
Timothy B. Rapp Chief
Foot And Ankle
Kenneth J. Mroczek Chief
Cary ChapmanCraig S. RadnaySteven Sheskier
Hand
Martin Posner Chief
Steven Green Assoc. Chief
Nader Paksima Assoc. Chief
Omri B. AyalonAlton O. BarronJohn T. CapoLouis W. CatalanoStuart ElkowitzSteven Z. GlickelSteven M. GreenSalil GuptaJacques H. HacquebordWilliam L. KingSalvatore LenzoEitan MelamedMukund R. PatelVipul P. PatelFrancis R. PelhamKeith B. RaskinMichael E. RettigAnthony SapienzaSteven A. StuchinS. Steven Yang
Research
Thorsten Kirsch Chief
Philip BandMarco CampelloAlesha CastilloMary CowmanSally R. FrenkelManny HalpernRaj J. KariaOran KennedyPhilipp LeuchtChuanju LiuSmita RaoAli SheikhzadehPeter S. WalkerShira WeinerSherri Weiser-HorwitzXiang Zhou
Academic Appointments
Marc H. AppelDan AtarAndrew N. BazosAdam BernsteinAlvin M. Bregman
Joel S. BuchalterWilliam BurmanWinshih ChangJack ChouekaDouglas J. FauserColleen M. FayLawrence G. FosterAlfred GarofaloMark A. GurlandJames GurtowskiRonald H. IsraelskiKevin KaplanVictor KhabieSteven KleinFrank J. LiggioRaphael S.f. LongobardiStephen G. MaurerMorteza MeftahSeth MillerRoy M. NuzzoAndrew M. PeretzJeffrey RichmondPhilip RobbinsJeffrey E. RosenRoy W. SandersVictor SassonPhilip SchrankSusan C. ScottJordan A. SimonMichael G. SoojianAdam D. SoyerStuart T. StylesBradley D. WienerJamie WisserJohn Zeller
Emeritus
Arnold T. BermanL. Paul BriefEnrique ErgasVictor FrankelVladimir GolyakhovskyAlfred D. GreismanJohn E. HandelsmanWallace B. LehmanLester LiebermanMargareta C. NordinJacques Serge ParisienMark PitmanPaul PostLawrence SchulmanKenneth E. SesloweJoseph A. SuarezN. Noel Testa
36 NYU LANGONE MEDICAL CENTER / ORTHOPAEDIC SURGERY
Leadership
New York University
William R. BerkleyChair, Board of Trustees
Andrew Hamilton, PhDPresident
Robert Berne, MBA, PhDExecutive Vice President for Health
NYU Langone Medical Center
Kenneth G. LangoneChair, Board of Trustees
Robert I. Grossman, MDSaul J. Farber Dean and Chief Executive Officer
Steven B. Abramson, MDSenior Vice President and Vice Dean for Education, Faculty, and Academic Affairs
Dafna Bar-Sagi, PhDSenior Vice President and Vice Dean for Science, Chief Scientific Officer
Andrew W. Brotman, MDSenior Vice President and Vice Dean for Clinical Affairs and Strategy, Chief Clinical Officer
Michael T. BurkeSenior Vice President and Vice Dean, Corporate Chief Financial Officer
Richard Donoghue Senior Vice President for Strategy, Planning, and Business Development
Annette Johnson, JD, PhDSenior Vice President and Vice Dean, General Counsel
Grace Y. KoSenior Vice President for Development and Alumni Affairs
Kathy LewisSenior Vice President for Communications and Marketing
Joseph LhotaSenior Vice President and Vice Dean, Chief of Staff
Vicki Match Suna, AIASenior Vice President and Vice Dean for Real Estate Development and Facilities
Nader MherabiSenior Vice President and Vice Dean, Chief Information Officer
Robert A. Press, MD, PhDSenior Vice President and Vice Dean, Chief of Hospital Operations
Nancy SanchezSenior Vice President and Vice Dean for Human Resources and Organizational Development and Learning
NYU Langone By the Numbers*
4,381Original Research Papers**
550,500Square Feet of Research Space
$334MNIH Funding
$328MTotal Grant Revenue
1,519Beds
100Operating Rooms
145,907Emergency Room Visits
68,602Patient Discharges
3,850,000Outpatient Faculty Practice Visits
9,649Births
3,584Physicians
4,899Nurses
574MD Candidates
80MD/PhD Candidates
233PhD Candidates
397Postdoctoral Fellows
1,472Residents and Fellows
*Numbers represent FY16 (Sept 2015–Aug 2016) and include NYU Lutheran **Calendar year 2015
1 MESSAGE FROM THE CHAIR
2 FACTS & FIGURES
4 NEW & NOTEWORTHY
8 CLINICAL CARE & RESEARCH
9 Personalized Approach to Joint Replacement
11 Ultra-Low Dose CT Reduces Risk
13 Complex Case: Scheuermann’s Kyphosis
14 Regenerative Medicine
16 New Momentum For Wide-Awake Hand Surgery
18 Robot and Computer-Assisted Surgery
20 Quality and Safety Initiatives
22 Bone and Cartilage Regeneration Research
24 Complex Case: Pelvic Osteosarcoma
26 ACADEMIC ACTIVITIES
34 LOCATIONS
36 FACULTY & LEADERSHIP
Contents
Produced by the Office of Communications and Marketing,NYU Langone Medical Center Photography: Karsten Moran Writer: Bryn Nelson Creative Direction: Ideas on Purpose, www.ideasonpurpose.com Design: Craig Williams, www.thecraigwilliams.com
On the cover: Human bone, osteoporosis

NYU LANGONE MEDICAL CENTER 550 First Avenue, New York, NY 10016
NYULANGONE.ORG
Orthopaedic Surgery
LARGESTRESIDENCY PROGRAM
IN THE COUNTRY
TOP 5IN U.S. NEWS &
WORLD REPORT
REDEFININGQUALITY AND
PATIENT SAFETY
2016 / YEAR IN REVIEW