optimizing and personalizing treatment for adhd canada/margaretweiss.pdf · optimizing and...
TRANSCRIPT

Optimizing and Personalizing Treatment for ADHD
Margaret Weiss MD PhDProvincial ADHD Program

Remission
• Definitions of remission are all symptom based
• Much or very much improved on the CGI-I• Mean score on the ADHD RS of < or = 1• Two score change on CGI-S• These definitions are currently used in
efficacy studies: short term, non comorbid, protocol driven studies with full compliance
Chronic Developmental Disorders
• The concept of remission derives from depression work where it predicted the likelihood of ultimate outcome
• ADHD is a developmental disorder which waxes, wanes and changes with different developmental disorders
• Does remission make sense?
Correlation of ADHD symptoms to functioning
• .2 in most studies to .68Gordon, J Attn Dis 2008
• The patient: “Does he treat what I have?”– Impairment, poor quality of life, adaptive
skills• The doctor: “Does he have what I treat?”
– Diagnoses
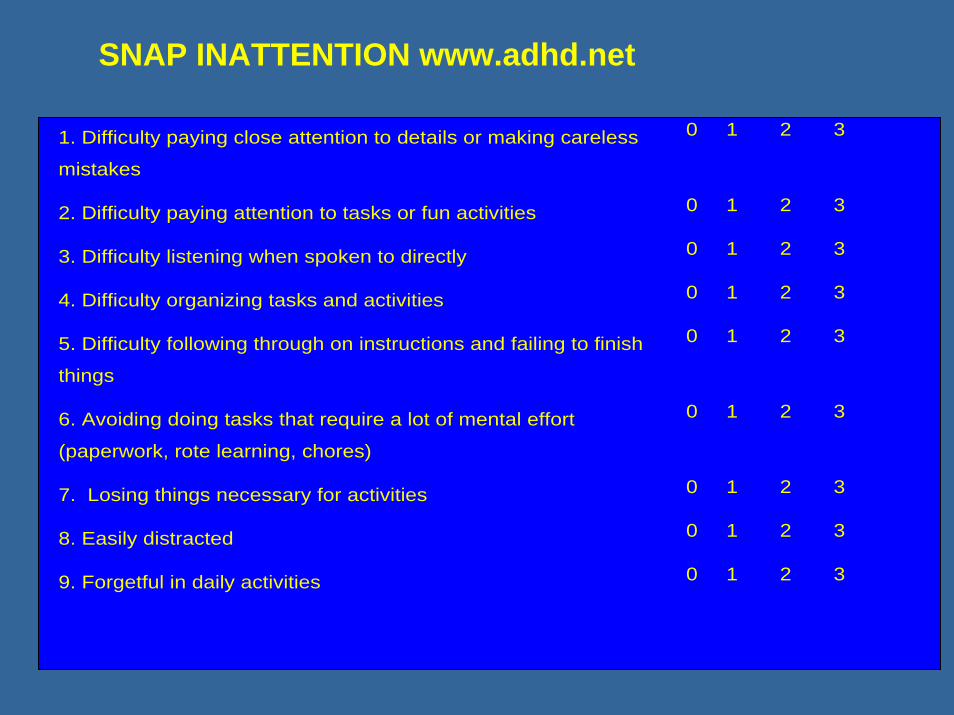
1. Difficulty paying close attention to details or making careless
mistakes
0 1 2 3
2. Difficulty paying attention to tasks or fun activities 0 1 2 3
3. Difficulty listening when spoken to directly 0 1 2 3
4. Difficulty organizing tasks and activities 0 1 2 3
5. Difficulty following through on instructions and failing to finish
things
0 1 2 3
6. Avoiding doing tasks that require a lot of mental effort
(paperwork, rote learning, chores)
0 1 2 3
7. Losing things necessary for activities 0 1 2 3
8. Easily distracted 0 1 2 3
9. Forgetful in daily activities 0 1 2 3
SNAP INATTENTION www.adhd.net
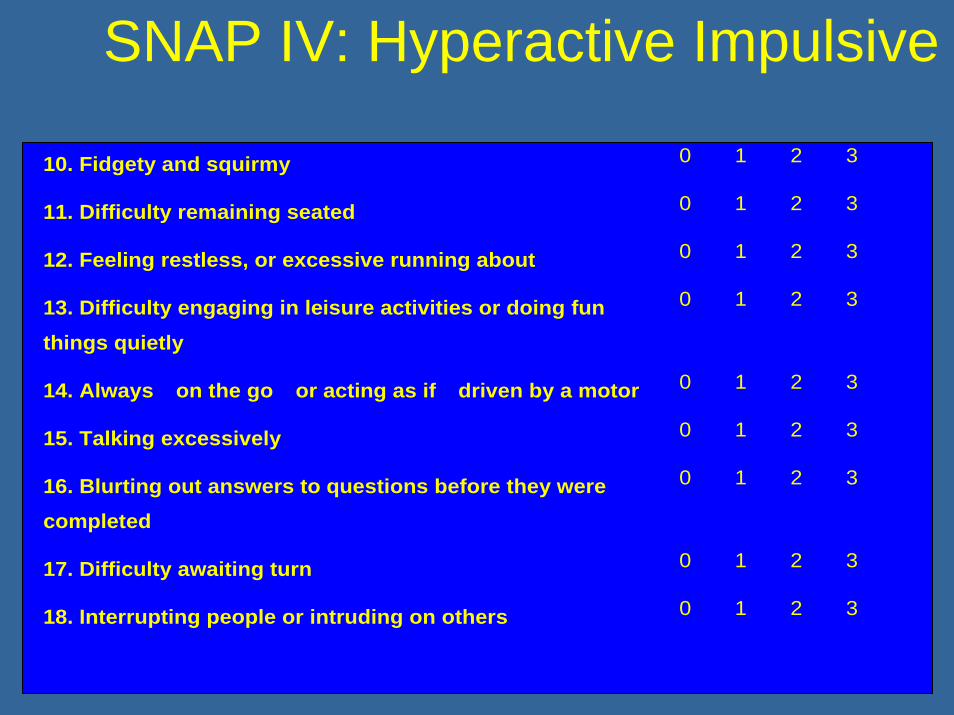
SNAP IV: Hyperactive Impulsive
10. Fidgety and squirmy 0 1 2 3
11. Difficulty remaining seated 0 1 2 3
12. Feeling restless, or excessive running about 0 1 2 3
13. Difficulty engaging in leisure activities or doing fun things quietly
0 1 2 3
14. Always �on the go� or acting as if �driven by a motor� 0 1 2 3
15. Talking excessively 0 1 2 3
16. Blurting out answers to questions before they were completed
0 1 2 3
17. Difficulty awaiting turn 0 1 2 3
18. Interrupting people or intruding on others 0 1 2 3
WEISS FUNCTIONAL IMPAIRMENT RATING
• Parent Report; Adult Self Report• No symptom items• Public Domain www.caddra.ca• Translated 18 languages• Recommended and reproduced in the Canadian Practice
guidelines www.caddra.cA• Clinician friendly• CADDRA guidelines use both sx/fxn outcomes• Internal consistency >.8, factor confirmation, high
correlation to symptoms, high sensitivity to change
Psychometric Validation WFIRS1
• Chronbach’s alpha >.9• Chronbach’s alpha domains .75 - .93• Sensitivity to change > 40%• Effect size change ATX .7 – 1.2• Factor analysis validates domain structure but
learning and school behavior are distinct• QoL, Fxn, Sx are overlapping but distinct
concepts
1AACAP 2007
Correlations of ADHD, Academic, Cognitive, and Functional Outcomes1
• 105 children 8 – 11 y who were treatment naïve
• Treated with ATX x 1 year• Measured outcome using the ADHD-RS,
WJIII, BASC, WFIRS • Analyzed correlations between outcomes
Dickson, R., Weiss, M. AACAP 2007; CACAP 2007

Improvement
1. Symptoms2. Functional Impairment3. Quality of Life4. Adaptive Skills5. Cognition6. Developmental gains
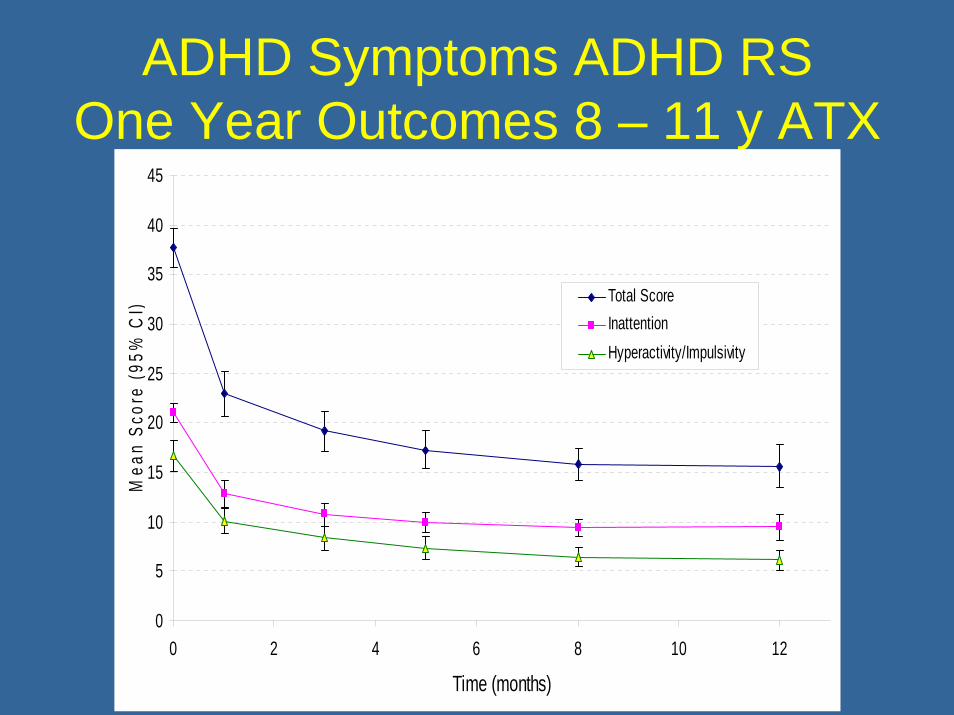
ADHD Symptoms ADHD RSOne Year Outcomes 8 – 11 y ATX
�
0
5
10
15
20
25
30
35
40
45
0 2 4 6 8 10 12
Time (months)
Mea
n Sc
ore
(95%
CI)
Total ScoreInattentionHyperactivity/Impulsivity
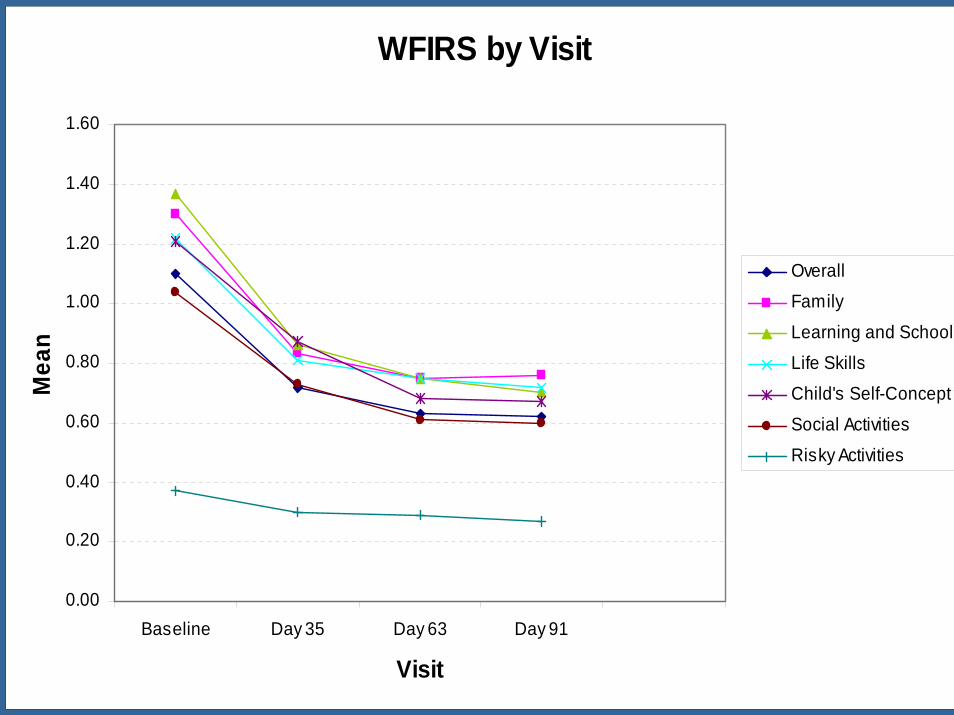
WFIRS by Visit
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
Baseline Day 35 Day 63 Day 91
Visit
Mea
n
Overall
Family
Learning and School
Life Skills
Child's Self-Concept
Social Activities
Risky Activities
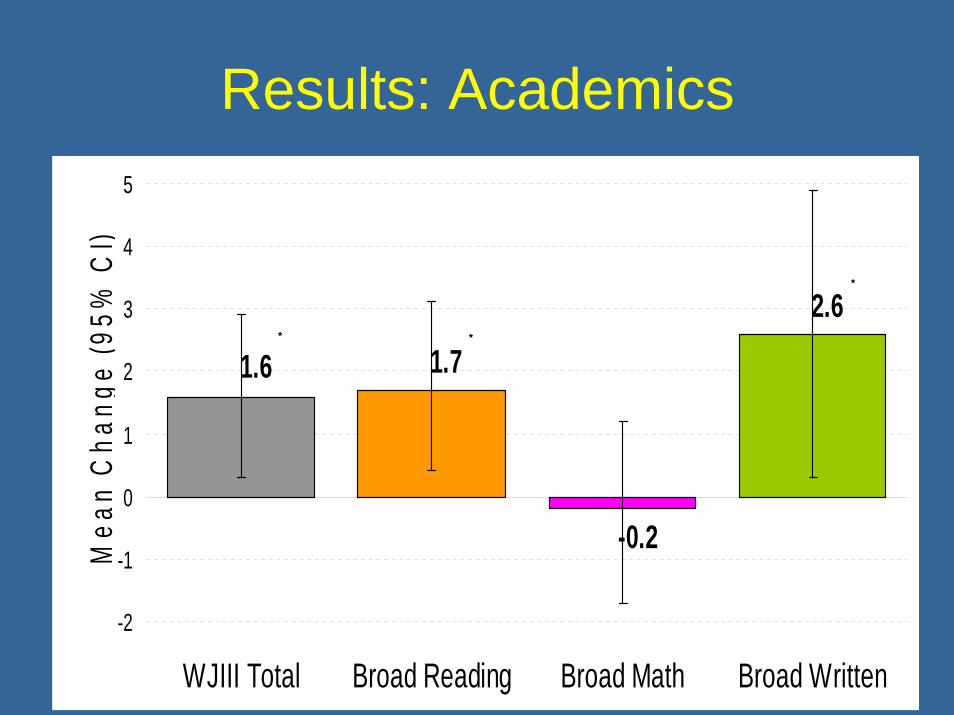
Results: Academics
2.6
-0.2
1.71.6
-2
-1
0
1
2
3
4
5
WJIII Total Broad Reading Broad Math Broad Written
Mea
n C
hang
e (9
5% C
I)
* *
*

- WJIII® Standard Scores: Change from Baseline to 1 Year
3.3*3.7
0.5
2.5*
-1.6-3.1*
0.2
1.91.7*
-6
-4
-2
0
2
4
6
8
Letter-WordIdentification
Reading Fluency PassageComprehension
Calculation Math Fluency Applied Problems Spelling Writing Fluency Writing Samples
Mea
n C
hang
e (9
5% C
I)

Executive Function: Brief
89.0
82.4
91.9
93.4
89.2
78.7
83.4
86.4
92.7
85.7
91.9
69.0
70.2
76.9
78.5
72.5
65.5
68.4
66.5
74.9
66.4
73.1
0 20 40 60 80 100
Global Executive Composite
Behavioral Regulation
Metacognition
Inhibit
Shift
Emotional Control
Initiate
Working Memory
Plan/Organize
Organization of Materials
Monitor
BRIEF Percentile Mean Score (95% CI)
Baseline (N=105) 1-Year (N=66)
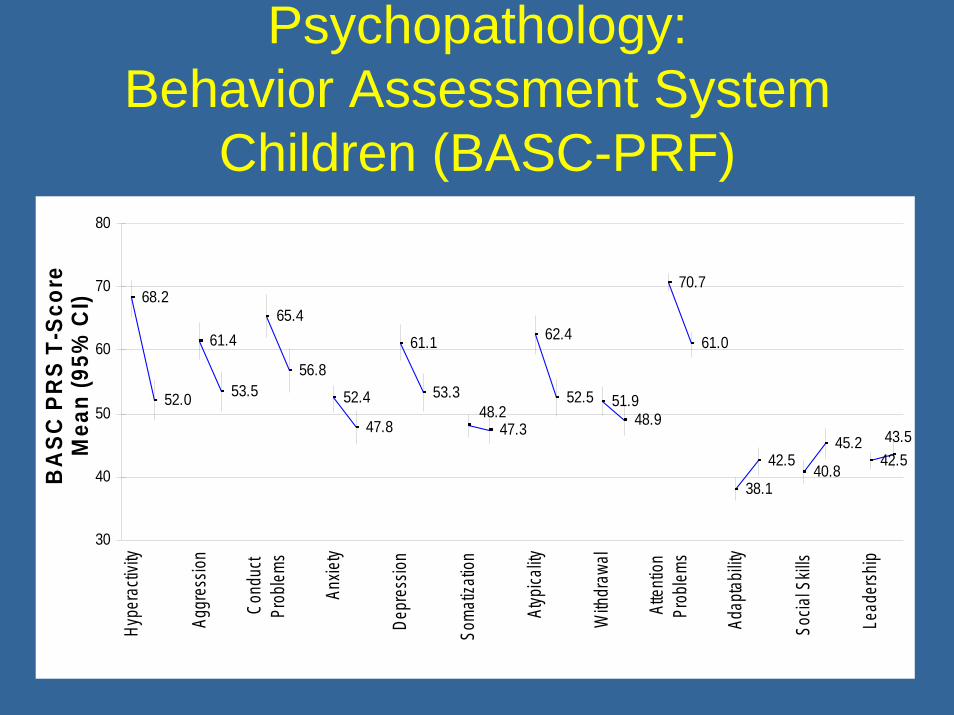
Psychopathology: Behavior Assessment System
Children (BASC-PRF)
68.2
52.0
61.4
53.5
65.4
56.8
52.4
47.8
61.1
53.3
62.4
52.5 51.948.9
70.7
61.0
38.1
42.540.8
45.247.3
48.2
42.543.5
30
40
50
60
70
80
Hype
racti
vity
Aggr
essio
n
Cond
uct
Prob
lems
Anxie
ty
Depr
essio
n
Soma
tizati
on
Atyp
icality
With
draw
al
Atten
tion
Prob
lems
Ada
ptabil
ity
Socia
l Skil
ls
Lead
ersh
ip
BA
SC P
RS
T-Sc
ore
Mea
n (9
5% C
I)

Change in ADHD symptoms mediates*
• Overall functioning, home life, school, social, activities of daily living and risky activities on the WFIRS but has minimal impact on self concept
• Executive function: total score and all subscales on the BRIEF
• All subscales and adaptive skills• on the BASC child and parent report
*p < .05
Change in ADHD symptoms does not mediate
• Improvement in the WJIII raw scores (correlation .066, p = .6)
• Improvement in the WJIII standard scores• (correlation .007, p = .96)• There are modest improvements in WJIII
reading and writing, but math fluency declines
Correlations
• There is a statistically significant correlation between improvement in ADHD and improvement in functioning, quality of life, psychopathology, and strengths
• Although children improved academically when ADHD was treated this was not statistically correlated
QUEST
• Quality of life, effectiveness, safety and tolerability study of adults with ADHD
• 735 adults; 83 sites• Outcome of 30 weeks of MAS-XR as
measured by ADHD-RS-Inv, SF-36; AIM-A; and medication satisfaction
• HRQL improved cotemporous with symptoms, with increase mainly in emotional well being
Effectiveness Outcomes
• Compliance and persistence• Real life, comorbid, clinic patients with
complex psychosocial problems and ethnic backgrounds
• Cost• Broad based outcomes• Risk/benefit ratio of improvement and
deleterious side effects
Research on Effectiveness• Evidence based medicine means we are funnels
of information to assist patients with guided choices
• This means that the research we refer to is applicable to the patients we see
• Effectiveness studies in ADHD: – NICE guidelines: none– MTA: after 3 years there is no residual effect of
treatment; 8 year follow up shows considerable impairment
– 30% persistence with stimulantsCharach 04; Miller 04; Bussing 05
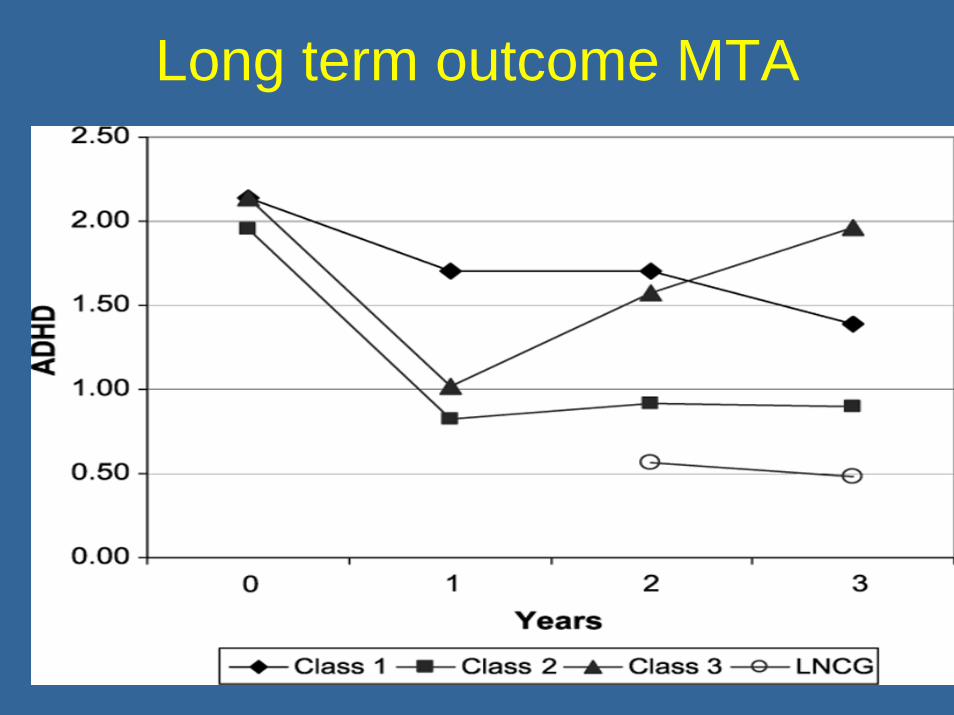
Long term outcome MTA

Effectiveness Study: Objectives• Is new and expensive really better?• Propensity analyses: who gets better?• How many drugs and why? • Safety of low dose Ris, combination Rx• Risk/benefit ratio of treatment• Individualization of treatment with comorbidity• Persistence with Rx and durability of outcome • Broad based outcomes: HRQL; Functioning;
Life skills; School and Work• Psychiatric side effects
Effectiveness Outcomes StudyMethod
1. 200 clinic patients2. No exclusions other than language3. All treatments measured naturalistically4. All direct and indirect costs measured5. Insured vs. uninsured? 6. Includes patients refusing treatment7. To what extent does improvement in
symptoms actually mediate improvement in functioning, quality of life, adaptive skills
Types of economic evaluation• Cost-Effectiveness Analysis (CEA)
– Benefits not explicitly valued - natural units used e.g. Life Years Gained (LYG) or cases detected
• Cost-Utility Analysis (CUA)– Benefits valued – typically based on LYG weighted
by an index of Quality of Life – Quality Adjusted Life Years (QALYs)
• Cost-Benefit Analysis (CBA)– Benefits valued - based on monetary valuations of
health improvements and expressed in dollars
Jumping through hoops
Safety Cost-EffectivenessQualityEfficacy
Measures• Adaptive functioning assessment system – apart from
the Vineland this is the only normed measure• Child Health Illness Profile – quality of life exclusive of
ADHD symptoms• Resource Utilization Questionnaire• Strengths and Difficulties Questionnaire• SNAP• Treatment Satisfaction Questionnaire for Medication –
Parent version• Pediatric Sleep Questionnaire• Pediatric Adverse Event Rating Scale (PAERS
www.captn.org)
Early Results
• Children who discontinue medication do not return to the clinic unless asked to do so
• Even in the face of symptom remission, mean ABAS score for self directed activity and home living < 5th percentile
• There is considerable use of multiple medication and medication switch
• There are selective medication responders
Next Year
• ICER/QALY• Propensity analysis• Weight changes: Ris; Atx; Stim• Sleep: percentage of sleep disorders and
naturalistic outcome of melatonin use• Is symptom an accurate proxy for overall
effectiveness and developmental gains?
Health• Sleep: ADHD is associated with delay in DLMO in adults
and children, RLS and PLMS• Nutrition: 44 children: majority have low Zn, Fe, Cu –
minerals which are MLT and DA cofactors and low long chain fatty acids
• Cardiac: ?risk of cardiac abnormalities in the face of developmental anomalies, associated difficulties (asthma, OM), exercise and medication
• DCD: 25% of the clinic impaired by clumsiness• Written Output: 75% of ADHD children dysgraphia• Medical Comorbidities: enuresis, asthma, otitis media• ADHD complicates PKU, neurofibromatosis, diabetes,
cystic fibrosis, congenital heart conditions
A. L. Colter, C. Cutler, and K. A. Meckling. Nutr J 7 (1):8, 2008.
Personalizing Treatment

Effect Size, What is?• The clinical relevance of the clinical trials, is analyzed
by Effect Size found, and is not related with the statistical significance.
• It’s used to understand the difference between the active drug and control.
• Represents an estimation related to a given scale in a given clinical trial
• Cohen’s recommendations are used to interpret the Effect Size1.
Effect size is not a measure of clinical significance. It is a measure of the size of the statistical difference between two conditions of points in time, and highly sensitive to accuracy of the measure used.
1Cohen J. Statistical power analyses for the behavioral sciences. 2nd ed. Mahwah, NJ: Lawrence, Erlbaum and Associates; 1988.
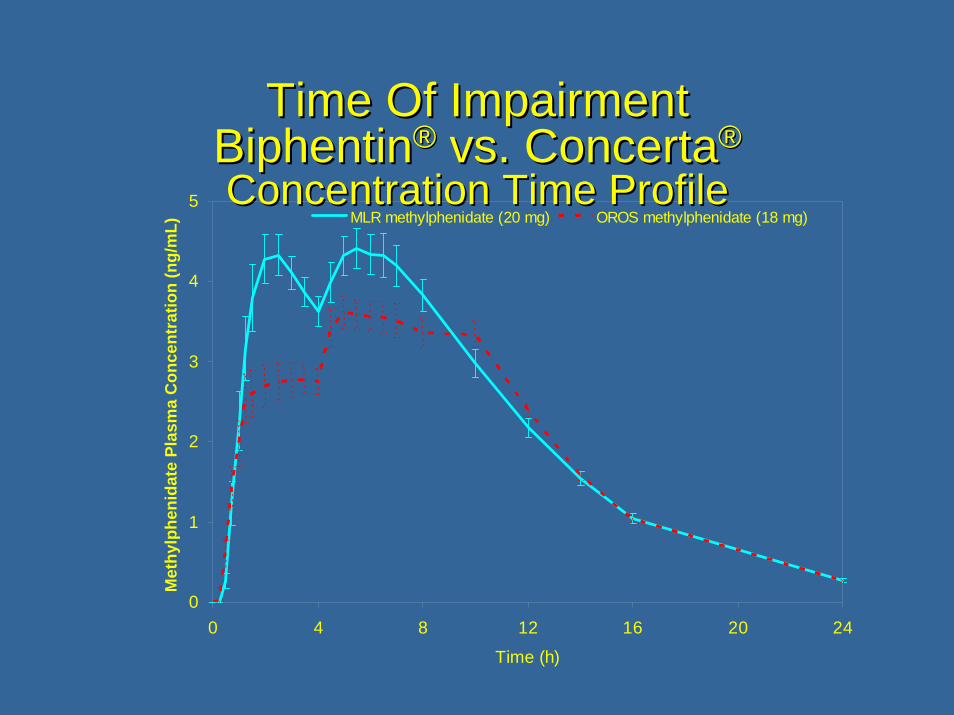
Time Of ImpairmentTime Of ImpairmentBiphentinBiphentin®® vs. vs. ConcertaConcerta®®
Concentration Time ProfileConcentration Time Profile
0
1
2
3
4
5
0 4 8 12 16 20 24
Time (h)
Met
hylp
heni
date
Pla
sma
Con
cent
ratio
n (n
g/m
L) MLR methylphenidate (20 mg) OROS methylphenidate (18 mg)
Unique Drug Response: Stim vs. Non Stim
• OROS MPH vs. Atx Newcorn Am J Psychiatry Jun 08
• N = 222 6 – 18 yo; cross over at 6 weeks• Anxiety, previous stim reaction, tics excluded• 43% of 70 patients who were stim non
responders responded to atx and of the 69 patients who did not respond to atx 42% responded to atx. 22% had no response to either
• MPH superior ES .2 for the group as a whole• No significant different in treatment naïve
population
Impact of comorbidity on Rx Selection
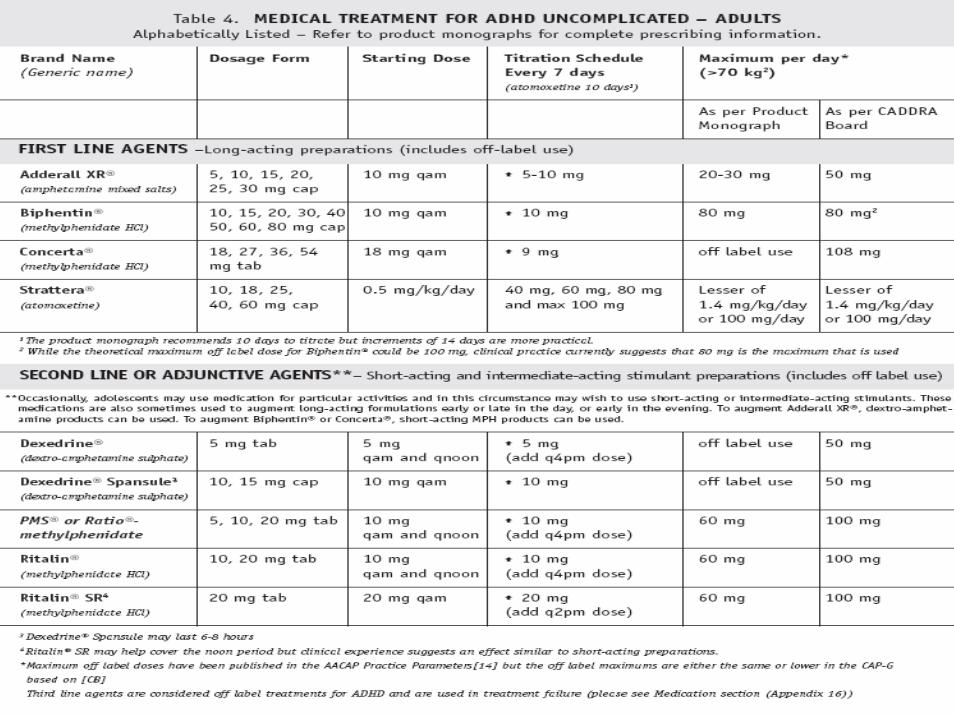
1. Time of drug must match time of impairment (i.e. Concerta a poor drug for early morning impairment)
2. Anxiety, tics, initial insomnia and possible concurrent SUD are relative indications for atomoxetine
3. Comorbid MDD requires treatment first4. Comorbid ODD and CD require concurrent
psychological management5. Explosive rage; emotional dysregulation, severe
irritability benefit from low dose SGAs6. Amphetamine as a group are more depressogenic
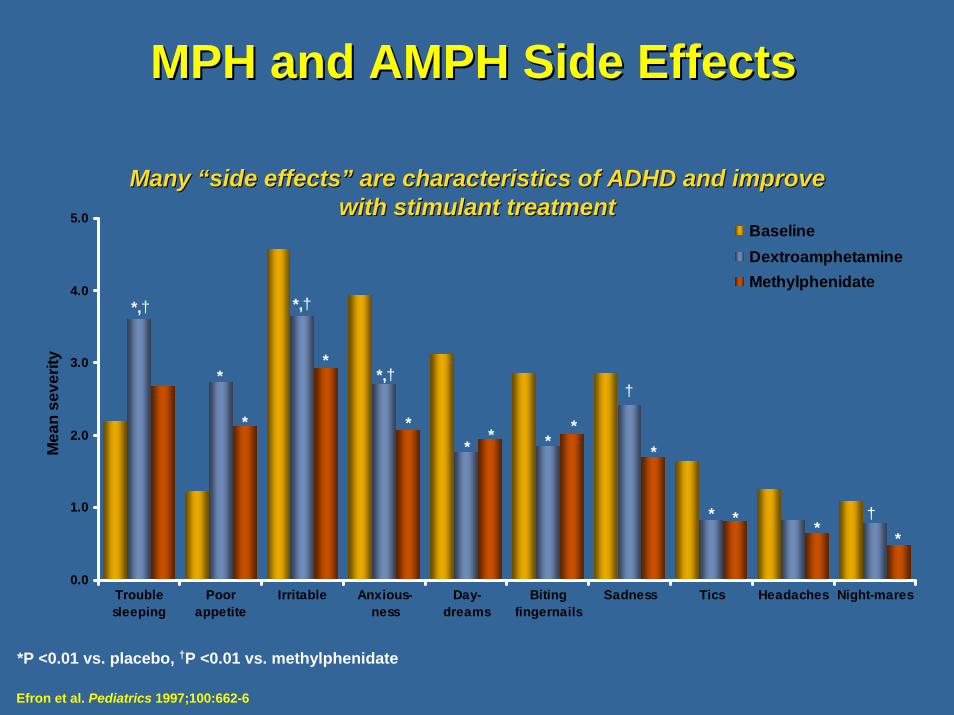
MPH and AMPH Side EffectsMPH and AMPH Side Effects
0.0
1.0
2.0
3.0
4.0
5.0
Troublesleeping
Poorappetite
Irritable Anxious-ness
Day-dreams
Bitingfingernails
Sadness Tics Headaches Night-mares
Mea
n se
verit
y
BaselineDextroamphetamineMethylphenidate
*,†
*
* *
*
*
*
** *
*
* **
*,†
*,††
†
Many Many ““side effectsside effects”” are characteristics of ADHD and improve are characteristics of ADHD and improve with stimulant treatment with stimulant treatment
Efron et al. Pediatrics 1997;100:662-6
*P <0.01 vs. placebo, †P <0.01 vs. methylphenidate

www.caddra.ca
Canadian ADD Resource Alliance1.Guidelines2.Treatment forms and scales3.Differential Diagnosis4.When to refer5.Annual conference6.Training Program
CHEAP AND EFFECTIVE: Psychological Interventions
1. Daily report card2. Psychoeducation3. Catch the good4. Skills block5. Decrease written output6. Environmental restructuring7. Minimize and structure homework8. Allocate tasks that can be done easily and well
School Based Interventions
1. Preferential seating2. Extra time on tests3. No homework4. Decreased demand for written output5. Peer buddies6. Daily report card 7. Keyboarding 8. Spare learning block at school
Treatment Implications• Externalize rewards• Chunk assignments• Use auxilliary aids such as agendas• Teach self regulation• Teach planning• Recognize that this is a disorder of performance
and not skill• Compensate for deficits in fluency with
increased time• Match environmental demands to skills• External scaffolding to provide attention
COGNITION

Executive Function Deficits• Response
disinhibition• Poor working memory• Problems sequencing• Blind to time• Blind to social
awareness• Inability to plan
• Problems with auditory processing
• Difficulty holding read material in mind
• Disorganization• Procrastination• Motivation

Working Memory
Helps the mind focus
“an attention controller”
Sluggish Cognitive Tempo or “ADD”
• Dreamy• Spacey• Sluggish – slow processing time• In their own world• Erratic performance and information
retrieval• Social Isolation• Distinct from ADHD-C and distinct from
ADHD-IA with residual hyperactivity
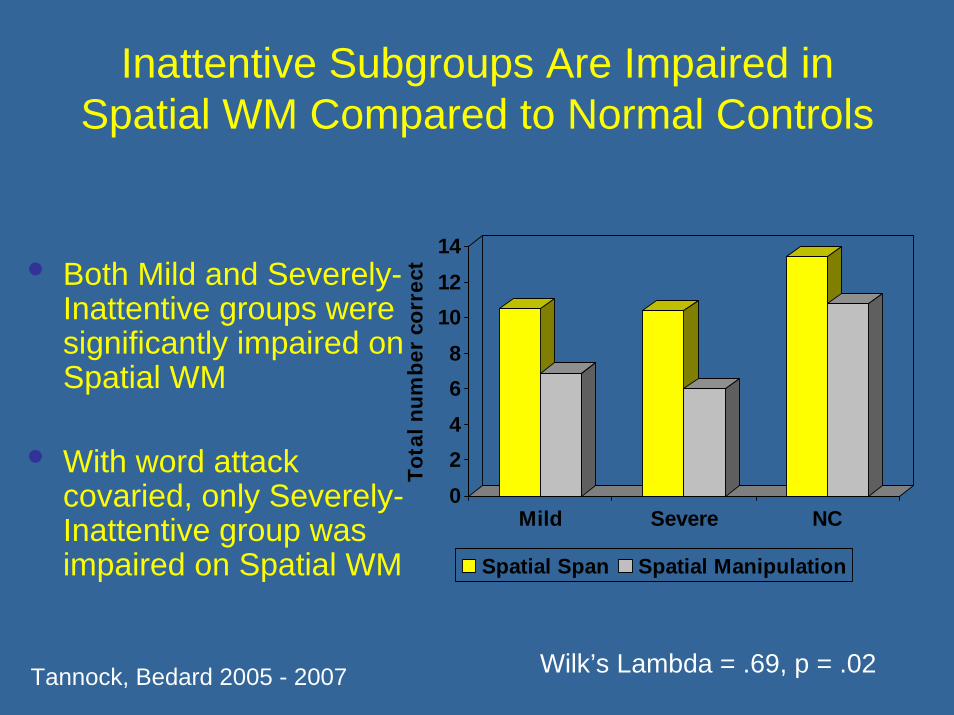
Inattentive Subgroups Are Impaired in Spatial WM Compared to Normal Controls
• Both Mild and Severely-Inattentive groups were significantly impaired on Spatial WM
• With word attack covaried, only Severely-Inattentive group was impaired on Spatial WM
02468
101214
Tota
l num
ber
corr
ect
Mild Severe NC
Spatial Span Spatial Manipulation
Wilk’s Lambda = .69, p = .02Tannock, Bedard 2005 - 2007
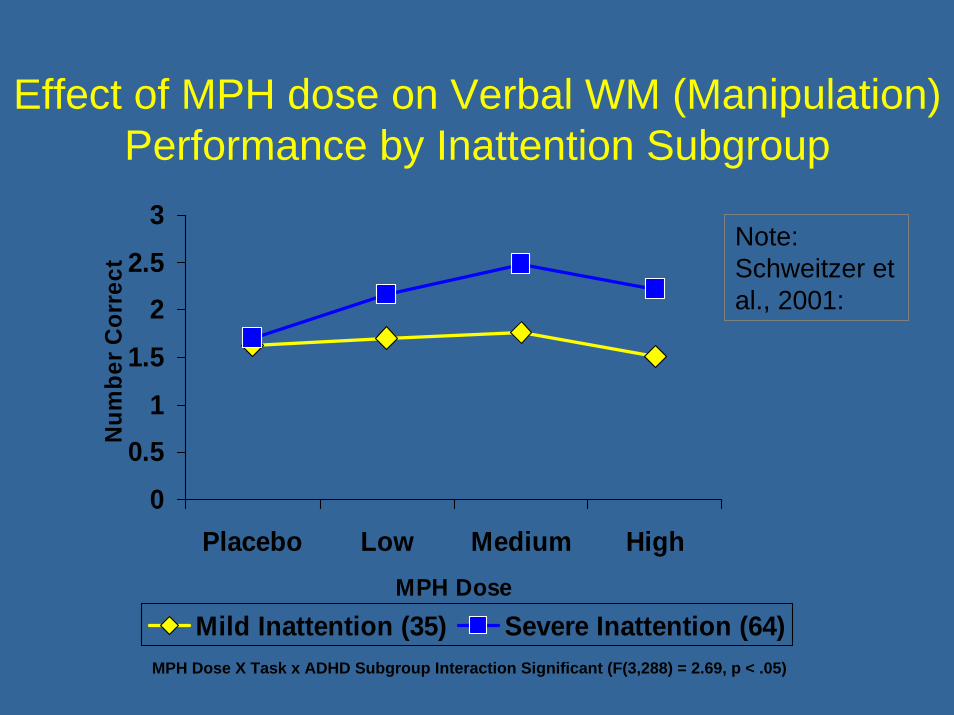
Effect of MPH dose on Verbal WM (Manipulation) Performance by Inattention Subgroup
0
0.51
1.5
22.5
3
Placebo Low Medium HighMPH Dose
Num
ber C
orre
ct
Mild Inattention (35) Severe Inattention (64)MPH Dose X Task x ADHD Subgroup Interaction Significant (F(3,288) = 2.69, p < .05)
Note: Schweitzer et al., 2001:
TO TAKE HOME• When its easy its very easy. • ADHD is mainly comorbid, severely impairing
developmental condition requiring careful assessment and follow up
• We don’t know who responds to what• Comorbidity impacts treatment outcome• In treating children we need to target their
overall health and well being as well as the disorder
• Treatment needs to be individualized to obtain remission in effectiveness outcomes