online video library - seattle children's · online video library ... --mottling mottling...
TRANSCRIPT
© 2010 Seattle Children's Hospital
Outreach Education
Online Video Library 2009-2010 .........................................................................................................
Drug Affected Infants
. Jaime Ruddell, MN, ARNP, NNP-BC
February 4, 2010
.........................................................................................................
Program Handouts This information is provided as a courtesy by Children's Health Care System and its related organizations (CHCS). Persons accessing this information assume full responsibility for the use of the information and understand and agree that CHCS is not responsible or liable for any claim, loss or damage arising from the use of the information. The views and opinions of the document authors do not necessarily state or reflect those of CHCS. Neither the authors nor CHCS nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from the use of such information.
Marianne Gonterman -Outreach Education (206) 987-5318 or (800) 293-2462 ext. 2 marianne.gonterman@
seattlechildrens.org
© 2010 Seattle Children's Hospital
Slide 1
Neonatal Abstinence Syndrome: Neonatal Abstinence Syndrome:
Evaluation and ManagementEvaluation and Management
Jaime Ruddell, RNC, NNP, MSNJaime Ruddell, RNC, NNP, MSN
Seattle ChildrenSeattle Children’’s Hospitals Hospital
Slide 2
Disclosure Statement
• I do not have any conflict of interest or will be discussing any off-label product use.
• This class has no commercial support or sponsorship, nor is it co-sponsored.
Slide 3 ObjectivesObjectives
•• Discuss Drug effects in PregnancyDiscuss Drug effects in Pregnancy
•• Define Neonatal Abstinence Syndrome (NAS) Define Neonatal Abstinence Syndrome (NAS) and its common presentation.and its common presentation.
•• Describe the use of Finnegan assessment toolDescribe the use of Finnegan assessment tool
•• Discuss alternative/supportive therapy for Discuss alternative/supportive therapy for withdrawalwithdrawal
•• Discuss Pharmacological interventions; when Discuss Pharmacological interventions; when should you treatshould you treat
•• Discuss process for weaning infants of NASDiscuss process for weaning infants of NAS
•• Should mothers be allowed to breastfeed the Should mothers be allowed to breastfeed the withdrawing infant?withdrawing infant?
•• What is known about long term outcomes?What is known about long term outcomes?

© 2010 Seattle Children's Hospital
Slide 4
Presentation of Withdrawal
Slide 5
Drugs in Pregnancy: Drugs in Pregnancy: TobaccoTobacco
•• Multiple effects: Poor growth and delayed Multiple effects: Poor growth and delayed
development development
•• May be related to increased risk of SIDS?May be related to increased risk of SIDS?
•• Maternal smoking + narcotic addiction = Maternal smoking + narcotic addiction =
increased NAS effectsincreased NAS effects
Slide 6
Drugs in Pregnancy: Drugs in Pregnancy: AlcoholAlcohol
•• 10% pregnant women use alcohol10% pregnant women use alcohol
•• Damages architecture, neuronal migration, Damages architecture, neuronal migration,
synaptogenesissynaptogenesis of developing brainof developing brain
•• Fetal Alcohol Syndrome (FAS); Fetal Fetal Alcohol Syndrome (FAS); Fetal
Alcohol Effects (FAE)Alcohol Effects (FAE)
–– Growth deficiencyGrowth deficiency
–– Facial abnormalitiesFacial abnormalities
–– CNS Damage/DysfunctionCNS Damage/Dysfunction
© 2010 Seattle Children's Hospital
Slide 7
Drugs In Pregnancy: Drugs In Pregnancy: CocaineCocaine
•• Psychoactive stimulantPsychoactive stimulant
•• Pregnancy effects:Pregnancy effects:
–– Stillbirth, prematurity, placental abruption, Stillbirth, prematurity, placental abruption,
IUGR, maternal anemia & malnutritionIUGR, maternal anemia & malnutrition
–– Neonatal neurobehavioral effectsNeonatal neurobehavioral effects
–– Hypertonic, irritable, tremulous, seizuresHypertonic, irritable, tremulous, seizures
NOT NOT ――withdrawalwithdrawal‖‖
Slide 8 Drugs In Pregnancy:Drugs In Pregnancy:
MethamphetaminesMethamphetamines
•• MethamphetamineMethamphetamine
•• Psychoactive stimulant; similar to cocainePsychoactive stimulant; similar to cocaine
•• Increased incidence of preterm delivery Increased incidence of preterm delivery
and placental abruptionand placental abruption
•• More likely to be SGA; LBWMore likely to be SGA; LBW
•• ?Increased fetal and maternal blood ?Increased fetal and maternal blood
pressurepressure
Slide 9
Drugs in Pregnancy: Drugs in Pregnancy: NarcoticsNarcotics
•• Attaches to Attaches to opioidopioid receptors on neuronal cell receptors on neuronal cell
membranes to inhibit neurotransmission of membranes to inhibit neurotransmission of
excitatory pathways: excitatory pathways:
--AcetylcholineAcetylcholine
--CatecholamineCatecholamine
--SerotoninSerotonin
•• Withdrawal results in increased Withdrawal results in increased
neurotransmitter releaseneurotransmitter release-- NASNAS
© 2010 Seattle Children's Hospital
Slide 10
Neonatal Abstinence SyndromeNeonatal Abstinence Syndrome
•• A generalized disorder that arises in an A generalized disorder that arises in an infant born addicted to narcotics or other infant born addicted to narcotics or other addictive substances, marked by a group addictive substances, marked by a group of common symptoms.of common symptoms.
•• Symptoms of withdrawal may include poor Symptoms of withdrawal may include poor gastrointestinal disposition, metabolic, gastrointestinal disposition, metabolic, vasomotor, and respiratory disturbances vasomotor, and respiratory disturbances as well as central nervous system as well as central nervous system disturbances.disturbances.
Slide 11 IncidenceIncidence
•• 33--50% depending on population 50% depending on population
•• OpioidOpioid withdrawal occurs in 55withdrawal occurs in 55--94% of infants 94% of infants
born to mothers addicted to narcotics born to mothers addicted to narcotics
•• Historical TrendsHistorical Trends
•• Current TrendsCurrent Trends
•• National Household Survey on DrugsNational Household Survey on Drugs
Slide 12
Presentation of Opiate withdrawalPresentation of Opiate withdrawal
•• Neurologic ExcitabilityNeurologic Excitability--tremorstremors
--irritability irritability
--sleeplessness sleeplessness
--high pitched cryhigh pitched cry
--hypertoniahypertonia
--increased deep tendon increased deep tendon reflexesreflexes
--exaggerated Moroexaggerated Moro
--seizures seizures 66
--frequent yawning and frequent yawning and sneezingsneezing

© 2010 Seattle Children's Hospital
Slide 13
Presentation of Opiate WithdrawalPresentation of Opiate Withdrawal
•• Gastrointestinal Gastrointestinal DysfunctionDysfunction
--poor feeding poor feeding
--uncoordinated and uncoordinated and constant suckingconstant sucking
--vomitingvomiting
--Diarrhea Diarrhea
--Dehydration Dehydration
--Poor weight gainPoor weight gain
Slide 14
Presentation of Opiate withdrawalPresentation of Opiate withdrawal
•• Autonomic SignsAutonomic Signs
--Increased Sweating Increased Sweating
--nasal stuffinessnasal stuffiness
--FeverFever
--Mottling Mottling
--Temperature InstabilityTemperature Instability
Slide 15 Timing of WithdrawalTiming of Withdrawal
•• AlcoholAlcohol-- first 3first 3--12 hours after birth12 hours after birth
•• Narcotic Withdrawal (methadone Narcotic Withdrawal (methadone vsvsother)other)-- 4848--72 hours after birth??? (may be 72 hours after birth??? (may be later if BF)later if BF)
•• SedativeSedative--HypnoticsHypnotics-- 22--3 days after birth 3 days after birth (up to as late as 12(up to as late as 12--14 days)14 days)
© 2010 Seattle Children's Hospital
Slide 16
Timing of WithdrawalTiming of Withdrawal
•• BarbituratesBarbiturates-- 44--7 days of life7 days of life
•• TobaccoTobacco-- first few hours of life and can be first few hours of life and can be severesevere
•• HeroinHeroin-- usually within 24 hours usually within 24 hours
•• Buprenorphine/SubutexBuprenorphine/Subutex within 12within 12--48 48 hourshours
Slide 17
The Antepartum Interview
Slide 18 The Reality of Drug Histories:The Reality of Drug Histories:
PolydrugPolydrug UseUse
•Abuse May Be Any Combination of Drugs- worsening withdrawal symptoms
•Abuse of prescribed Drugs
•Methadone Maintenance &/or Abuse
© 2010 Seattle Children's Hospital
Slide 19 Know What Drugs are Popular in Your Town?
Slide 20
Drug History: You have to ask.
•Smoking Hx - How Many Cigarettes Do You Smoke Per Day?
•ETOH - How Many Drinks Do You Take Per Day?
•What OTC Drugs Do You Use?
•What Prescription Drugs Used?
Slide 21 Drug History Interview
•What Street/Recreational Drugs Have You Used?
•Are You in a Methadone Maintenance Program?Do You Supplement With Street Methadone?
Do you have periods of time when you feel the need for higher or supplemental dosing?
What do you do in that case?
Have You Experience Periods of Narcotic Withdrawal?
•Immediate Antepartum Drug Use:Types, Dosage, Timing and Routes
© 2010 Seattle Children's Hospital
Slide 22 The Perinatal Intake Exam
• Common symptoms of a Woman Abusing Drugs…Is She…
Disoriented?
Physically Exhausted?
Pupils Extremely Dilated Or Constricted?
Does The Appearance Of The Pregnancy Coincide With The Stated Gestational Age?
Track Marks, Abscesses, ―picking sores‖?
Sinus Inflammation, Excoriation, Or Eroded Septum?
Does The Woman Appear Honest In Her Responses?
Gum and dental health
Slide 23 Reason to consider Reason to consider
Maternal Drug ScreeningMaternal Drug Screening
•• Lack of, or unexplained, late prenatal careLack of, or unexplained, late prenatal care
•• Previous unexplained fetal demisePrevious unexplained fetal demise
•• AbruptioAbruptio placentaplacenta
•• Hypertensive episodeHypertensive episode
•• Severe mood swingsSevere mood swings
•• CerebrovascularCerebrovascular accidents, MIaccidents, MI
•• Repeated spontaneous abortionsRepeated spontaneous abortions
Slide 24 Reasons to consider Reasons to consider
Neonatal Drug ScreeningNeonatal Drug Screening
•• Unexplained prematurityUnexplained prematurity
•• SeizuresSeizures
•• Severe Vomiting/DiarrheaSevere Vomiting/Diarrhea
•• Excessive weight loss/dehydrationExcessive weight loss/dehydration
•• Unexplained intrauterine growth restrictionUnexplained intrauterine growth restriction
•• Neurobehavioral abnormality Neurobehavioral abnormality
•• Atypical vascular accidents such as CVA, Atypical vascular accidents such as CVA, MI, and NEC in otherwise healthy term MI, and NEC in otherwise healthy term infantsinfants
© 2010 Seattle Children's Hospital
Slide 25
Differential DiagnosisDifferential Diagnosis
•• Withdrawal signs may be mistaken for Withdrawal signs may be mistaken for
other common neonatal problems such asother common neonatal problems such as-- ColicColic
-- Infection/MeningitisInfection/Meningitis
-- Feeding or formula intoleranceFeeding or formula intolerance
-- Milk intoleranceMilk intolerance
-- Evidence of Hypoxic ischemic encephalopathyEvidence of Hypoxic ischemic encephalopathy
-- HypocalcaemiaHypocalcaemia
-- HyponatremiaHyponatremia
-- HypomagnesaemiaHypomagnesaemia
When in doubt, a urine and When in doubt, a urine and MeconiumMeconium drug screen drug screen maymaybe helpful, but identification of infants at risk is be helpful, but identification of infants at risk is cruciacrucial.l.
Slide 26
MeconiumMeconium and Urine Drug Testingand Urine Drug Testing
•• MeconiumMeconium-- obtain multiple samples, large quantityobtain multiple samples, large quantity
•• Reflects second half of pregnancyReflects second half of pregnancy
•• UrineUrine-- Obtain earlyObtain early
•• May result in false negativesMay result in false negatives
•• Earliest newborn urine will contain the highest Earliest newborn urine will contain the highest
concentration of substancesconcentration of substances
•• Newborn urine reflects exposure during preceding one to Newborn urine reflects exposure during preceding one to
three daysthree days
•• Cocaine metabolites may be present for 4Cocaine metabolites may be present for 4--5 days; 5 days;
marijuana for weeksmarijuana for weeks
•• Alcohol is nearly impossible to detectAlcohol is nearly impossible to detect
Slide 27
Treating Neonatal Abstinence Syndrome
© 2010 Seattle Children's Hospital
Slide 28
AAP Recommendations• The goal to NAS treatment is to:
improve feeding and weight gain
prevent seizures
reduce unnecessary hospitalization
improve family interaction/care skills
reduce incidence infant mortality and abnormal neurological development
(AAP, 1998) (Osborne et al 2005) (Kandall, 1993)
Slide 29
Tools to assess WithdrawalTools to assess Withdrawal
•• LipsitzLipsitz Tool; simple; score >4= withdrawalTool; simple; score >4= withdrawal
•• Finnegan; complex , most widely usedFinnegan; complex , most widely used(1975)(1975)
•• OstreaOstrea; numeric score; numeric score
•• Neonatal Narcotic Withdrawal Neonatal Narcotic Withdrawal IndexIndex(Grear(Grear and and SuffetSuffet, ,
1975)1975)
•• Opiate Weaning Flow SheetOpiate Weaning Flow Sheet (Frank and (Frank and ViardiViardi, 1995), 1995)
•• OpioidOpioid and Benzodiazepine withdrawal Scoreand Benzodiazepine withdrawal Score(Frank, (Frank, NaughtonNaughton and Winter, 2004)and Winter, 2004)
Slide 30
Finnegan Assessment ToolFinnegan Assessment Tool
© 2010 Seattle Children's Hospital
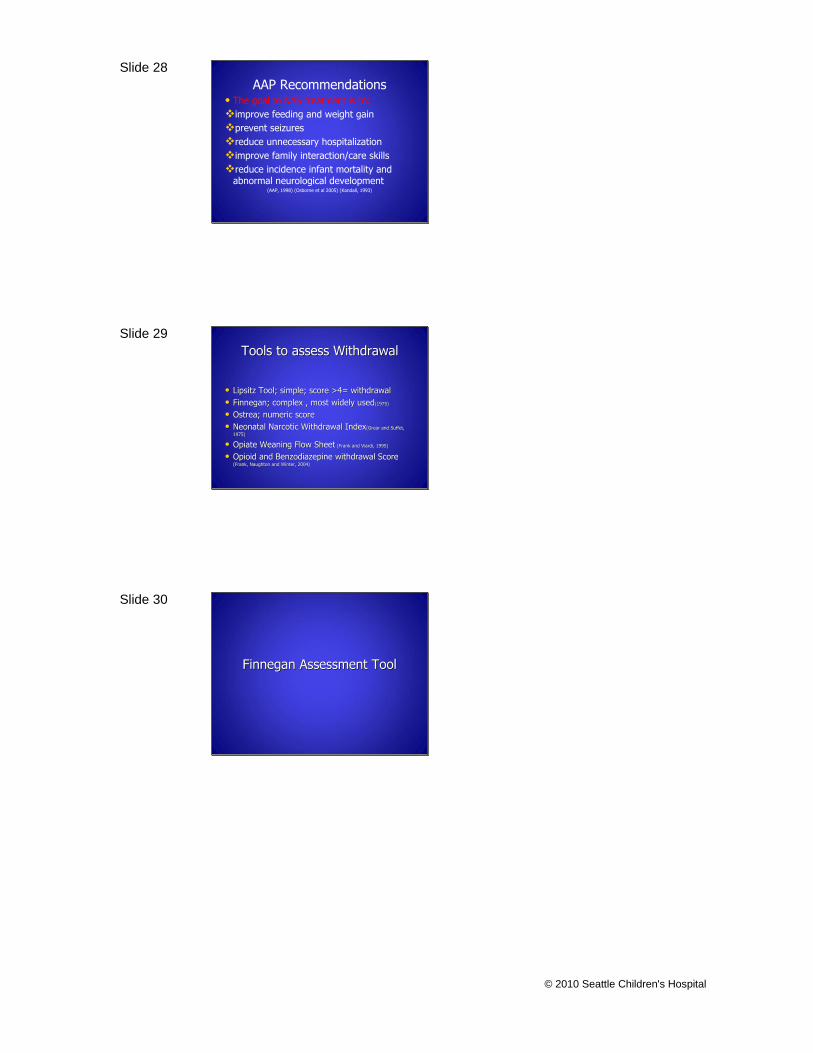
Slide 31 1 2 3
Time
Signs & Symptoms Score
High Pitched Cry 2
Continuous High Pitched
Cry
3
Sleeps <1 Hour After Feed 3
Sleeps < 2 Hours After
Feed
2
Sleeps < 3 Hours After
Feed
1
Hyperactive Moro Reflex 2
Mild Tremors When
Disturbed
1
Marked Tremors When
Disturbed
2
Mild Tremors Undisturbed 3
Marked Tremors
Undisturbed
4
Increased Muscle Tone 2
Generalized Seizures 5
Frantic Fist Sucking 1
Poor Feeding 2
Regurgitation 2
Projectile Vomiting 3
Loose Stools 2
Watery Stools 3
Dehydration 2
Frequent Yawning 1
Sneezing 1
Nasal Stuffiness 1
Sweating 1
Mottling 1
Fever < 101F (38°c) 1
Fever > 101F (38°c) 2
Resp Rate > 60 1
Resp Rate > 60 with Retrx 2
Excoriation Nose 1
Excoriation Knees 1
Excoriation Toes 1
Date
Auto
nom
ic D
istu
rban
ceN
euro
logi
cGI
Dis
turb
ance
Slide 32
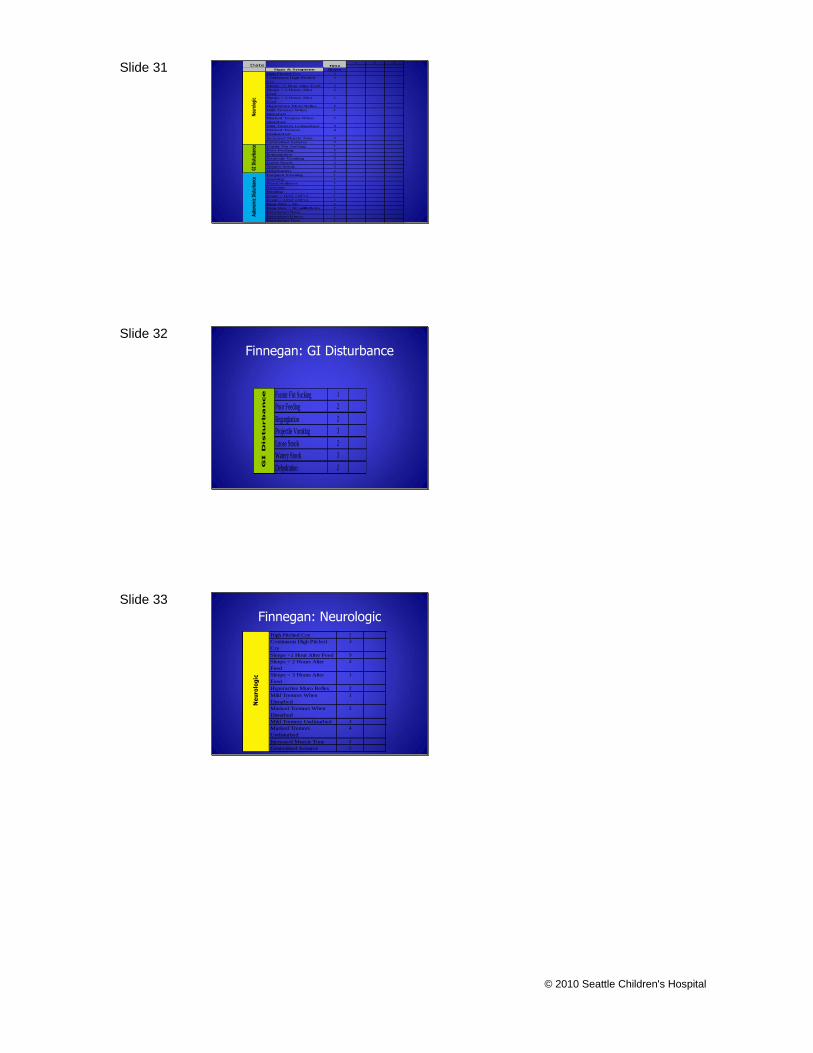
Finnegan: GI Disturbance
Frantic Fist Sucking 1
Poor Feeding 2
Regurgitation 2
Projectile Vomiting 3
Loose Stools 2
Watery Stools 3
Dehydration 2GI D
istu
rb
an
ce
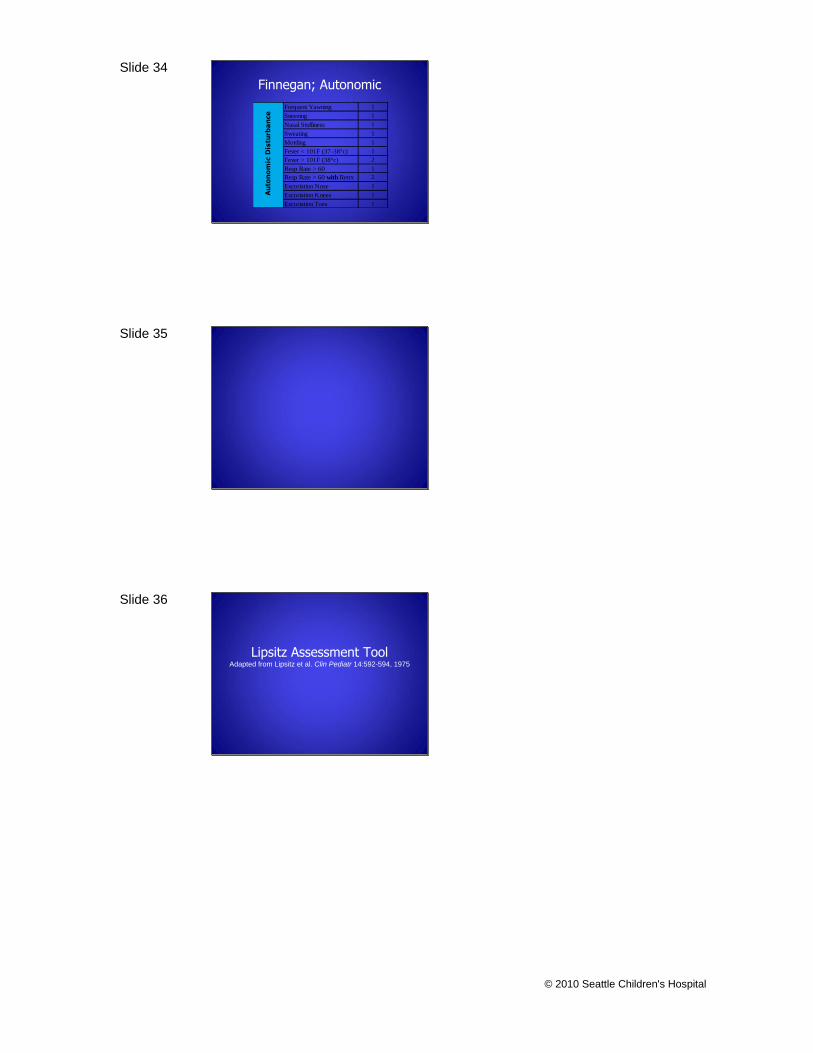
Slide 33
Finnegan: NeurologicHigh Pitched Cry 2
Continuous High Pitched
Cry
3
Sleeps <1 Hour After Feed 3
Sleeps < 2 Hours After
Feed
2
Sleeps < 3 Hours After
Feed
1
Hyperactive Moro Reflex 2
Mild Tremors When
Disturbed
1
Marked Tremors When
Disturbed
2
Mild Tremors Undisturbed 3
Marked Tremors
Undisturbed
4
Increased Muscle Tone 2
Generalized Seizures 5
Ne
uro
log
ic
© 2010 Seattle Children's Hospital
Slide 34
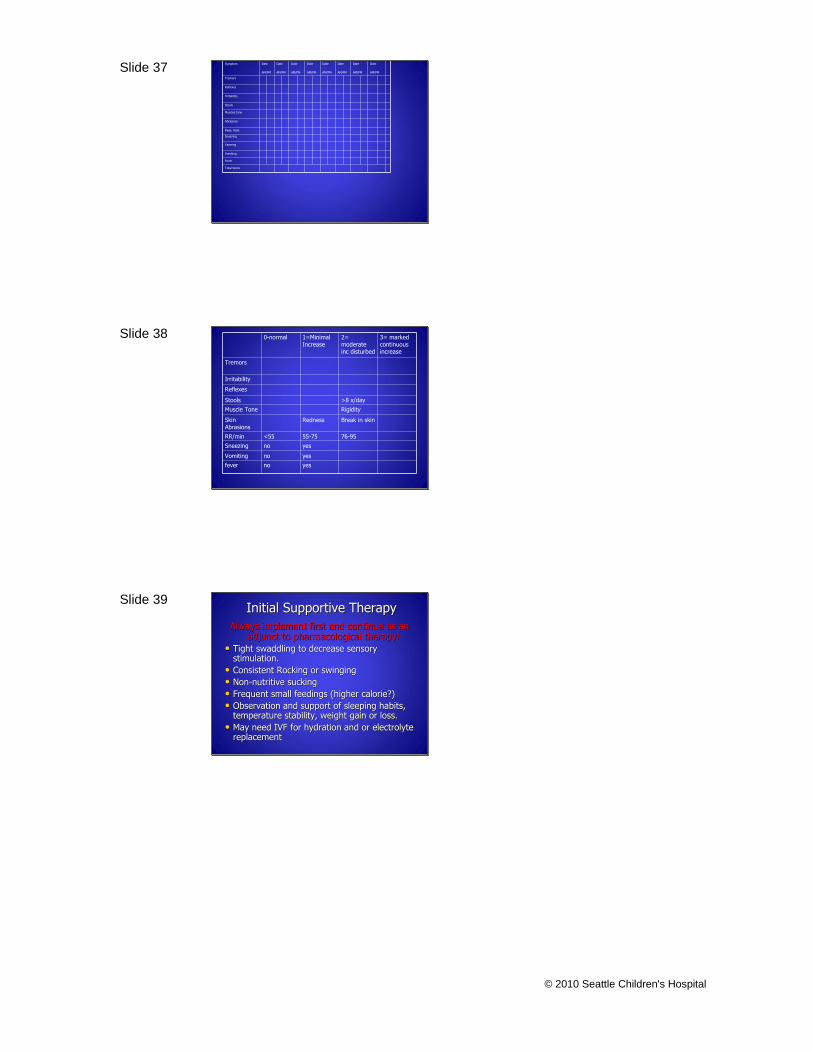
Finnegan; Autonomic
Frequent Yawning 1
Sneezing 1
Nasal Stuffiness 1
Sweating 1
Mottling 1
Fever < 101F (37-38°c) 1
Fever > 101F (38°c) 2
Resp Rate > 60 1
Resp Rate > 60 with Retrx 2
Excoriation Nose 1
Excoriation Knees 1
Excoriation Toes 1
Au
ton
om
ic D
istu
rba
nce
Slide 35
Slide 36
Lipsitz Assessment ToolAdapted from Lipsitz et al. Clin Pediatr 14:592-594, 1975
© 2010 Seattle Children's Hospital
Slide 37 Symptom Date
AM/PM
Date
AM/PM
Date
AM/PM
Date
AM/PM
Date
AM/PM
Date
AM/PM
Date
AM/PM
Date
AM/PM
Tremors
Reflexes
Irritability
Stools
Muscles tone
Abrasions
Resp. Rate
Sneezing
Yawning
Vomiting
Fever
Total Score
Slide 38 0-normal 1=Minimal Increase
2= moderate inc disturbed
3= marked continuous increase
Tremors
Irritability
Reflexes
Stools >8 x/day
Muscle Tone Rigidity
Skin Abrasions
Redness Break in skin
RR/min <55 55-75 76-95
Sneezing no yes
Vomiting no yes
fever no yes
Slide 39 Initial Supportive TherapyInitial Supportive Therapy
Always implement first and continue as an Always implement first and continue as an adjunct to pharmacological therapy!adjunct to pharmacological therapy!
•• Tight swaddling to decrease sensory Tight swaddling to decrease sensory stimulation.stimulation.
•• Consistent Rocking or swingingConsistent Rocking or swinging
•• NonNon--nutritive suckingnutritive sucking
•• Frequent small feedings (higher calorie?)Frequent small feedings (higher calorie?)
•• Observation and support of sleeping habits, Observation and support of sleeping habits, temperature stability, weight gain or loss.temperature stability, weight gain or loss.
•• May need IVF for hydration and or electrolyte May need IVF for hydration and or electrolyte replacementreplacement
© 2010 Seattle Children's Hospital
Slide 40
Treatment OptionsTreatment Options
•• Supportive CareSupportive Care
•• MorphineMorphine-- recommendedrecommended
•• PhenobarbitalPhenobarbital
•• AtivanAtivan
•• Tincture of OpiumTincture of Opium
•• Paregoric (not recommended Paregoric (not recommended d/td/t toxic toxic
effects of additives)effects of additives)
Slide 41 MorphineScore 8-10
320 micrograms/kg/daily
Scores 11-13
480 micrograms/kg/daily
Scores 14-16
640 micrograms/kg/daily
Scores 17+
800 micrograms/kg/daily
• Benefits
• Pitfalls
• Length and efficacy of therapy
Slide 42
PhenobarbitalPhenobarbital
Load with PhenobarbitalLoad with Phenobarbital
1010--20mg/kg x 1 dose20mg/kg x 1 dose
MaintenanceMaintenance
5mg/kg/day divided into two doses5mg/kg/day divided into two doses
•• BenefitsBenefits
•• DownfallsDownfalls
•• Long Term OutcomesLong Term Outcomes
© 2010 Seattle Children's Hospital
Slide 43 AtivanAtivan
Load with Load with AtivanAtivan
0.050.05--0.1mg/kg/dose q 6 hours0.1mg/kg/dose q 6 hours
Increase by 0.02mg/kg/dose to desired Increase by 0.02mg/kg/dose to desired
effect effect (increase as needed every 12 hours)(increase as needed every 12 hours)
•• BenefitsBenefits
•• DownfallsDownfalls
•• Long Term OutcomesLong Term Outcomes
Slide 44 MethadoneMethadone
Start with 0.05Start with 0.05--0.1mg/kg every 6 hours0.1mg/kg every 6 hours
Increase by 0.02mg/kg/dose to desired Increase by 0.02mg/kg/dose to desired
effecteffect(increase as often as every 12 hours)(increase as often as every 12 hours)
•• BenefitsBenefits
•• DownfallsDownfalls
•• Long Term OutcomesLong Term Outcomes
Slide 45
Weaning NAS Therapy
© 2010 Seattle Children's Hospital
Slide 46 Weaning NAS TherapyWeaning NAS Therapy
MorphineMorphine•• Target Score for Target Score for ――ControlControl‖‖
–– Consistent scores Consistent scores >12>12, consider increasing , consider increasing
pharmacologic therapypharmacologic therapy
–– Consistent scores Consistent scores 77--1111, Adequate Therapy, Adequate Therapy
–– Consistent scores Consistent scores <7<7, consider slow weaning , consider slow weaning
protocolprotocol
Slide 47 Weaning By ProtocolWeaning By Protocol
•• Stabilize With Scores < 11 for 72 HoursStabilize With Scores < 11 for 72 Hours
•• Decrease Dose by 10% of Decrease Dose by 10% of MaximumMaximum Narcotic Dose Narcotic Dose
(Do Not Adjust for Weight Gain)(Do Not Adjust for Weight Gain)
•• Wean Dose Q 48Wean Dose Q 48--72 Hours As Tolerated72 Hours As Tolerated
•• If Scores Increase After Wean Increase to Last If Scores Increase After Wean Increase to Last
Successful DoseSuccessful Dose
•• Trial DC Narcotic at 40mcg every 3 hours Trial DC Narcotic at 40mcg every 3 hours
•• ? DC Home on Narcotic, With the Family Scoring the ? DC Home on Narcotic, With the Family Scoring the
InfantInfant
Wean 20% Wean 20% maxmax dose per Week (very slow dose per Week (very slow
stable weaning pattern) (dose changes twice stable weaning pattern) (dose changes twice
weekly)weekly)
Family & PCP Score the InfantFamily & PCP Score the Infant
Slide 48 Home Weaning Schedule
Wean Date
Max dose 500 mcg Narcotic Dilution 0.4mg mg/1ml
Dose Directions
PO Q4°
Plan revised 8/22/03
8/21/03 380 mcg=0.95ml By mouth every 4 hours
8/25/03 330 mcg=0.83ml By mouth every 4 hours
8/28/03 280 mcg=0.63ml By mouth every 4 hours
9/1/03 230 mcg=0.58ml By mouth every 4 hours
9/4/03 180 mcg=0.45ml By mouth every 4 hours
9/8/03 130 mcg=0.33ml By mouth every 4 hours
9/11/03 80 mcg=0.2ml By mouth every 4 hours
9/15/03 30 mcg=0.08ml By mouth every 4 hours
9/18/03 Discontinue Narcotic -------------
© 2010 Seattle Children's Hospital
Slide 49
Weaning Strategies
•• Utilize the Family/Volunteers as much as Utilize the Family/Volunteers as much as
possiblepossible
•• SystematicSystematic
•• Dynamic and flexible related to the infants Dynamic and flexible related to the infants
response.response.
•• Concrete Administration scheduleConcrete Administration schedule
•• Consistent, Unbiased AssessmentConsistent, Unbiased Assessment
Slide 50 Obstacles to WeaningObstacles to Weaning
•• Gestational ageGestational age
•• Chronological ageChronological age
•• SensitivitySensitivity
•• Availability of Breast MilkAvailability of Breast Milk
•• Presence of the FamilyPresence of the Family
•• Differentiating between Differentiating between
irritable irritable ――newbornnewborn‖‖ activity activity
and withdrawaland withdrawal
Slide 51
Rules for WeaningRules for Weaning
•• Choose a toolChoose a tool
•• Monitor Carefully and Monitor Carefully and ConsistetnlyConsistetnly
•• Review documented responses to the doseReview documented responses to the dose
•• Be willing to adjust the dose/weaning Be willing to adjust the dose/weaning
schedule based on responseschedule based on response
•• Utilize the FamilyUtilize the Family
© 2010 Seattle Children's Hospital
Slide 52
WeaningWeaning
•• Most sources recommend 10Most sources recommend 10--20% of 20% of
original dose every other day.original dose every other day.
•• Find a pattern that works, and donFind a pattern that works, and don’’t t
change it unless necessary.change it unless necessary.
•• Choose an end pointChoose an end point
Slide 53
Slide 54
Breastfeeding the Addicted Infant
© 2010 Seattle Children's Hospital
Slide 55 Breastfeeding on MethadoneBreastfeeding on Methadone
•• 73% of Infants in New Zealand continue to 73% of Infants in New Zealand continue to
BF during wean and through discharge.BF during wean and through discharge.
•• Women on Methadone, who are eligible to Women on Methadone, who are eligible to
BF, may need increased lactation support.BF, may need increased lactation support.
•• Ensure a consistent supply of Breast milk at Ensure a consistent supply of Breast milk at
every feeding.every feeding.
•• May help the mother feel a sense of May help the mother feel a sense of ――helping helping
―― the baby.the baby.
•• May encourage more regular visits and May encourage more regular visits and
supportive measures.supportive measures.
Slide 56
Outcomes
Slide 57 Drugs in Pregnancy:Drugs in Pregnancy:
Contributors to Neonatal OutcomeContributors to Neonatal Outcome
•• Drug withdrawalDrug withdrawal
•• PolyPoly--drug usedrug use
Other contributors to outcomeOther contributors to outcome
•• PovertyPoverty
•• Maternal depressionMaternal depression
•• Poor maternal nutritionPoor maternal nutrition
•• Neglect; abuseNeglect; abuse
© 2010 Seattle Children's Hospital
Slide 58 DrugDrug--exposed infants:exposed infants:
Pediatric OutcomesPediatric Outcomes
•• Increased risk for SIDS?Increased risk for SIDS?
•• NeurobehavioralNeurobehavioral——Increased risk for Increased risk for
ADHD, learning disabilities, autism?ADHD, learning disabilities, autism?
•• Social Stigma/LabelsSocial Stigma/Labels
•• SelfSelf--fulfilling propheciesfulfilling prophecies
•• UnUn--adoptable?adoptable?
•• Increased risk for child abuse, neglectIncreased risk for child abuse, neglect
Slide 59 Research StatementsResearch Statements
•• Research shows that despite Research shows that despite
exposure to illicit drugsexposure to illicit drugs, kids have, kids have
the capability to do well if raised in athe capability to do well if raised in a
supportive nurturing environment. supportive nurturing environment.
(Marcellus, 2007)(Marcellus, 2007)
•• Illicit drug exposure is not as bad as poverty on Illicit drug exposure is not as bad as poverty on neurodevelopmentalneurodevelopmental outcomes. outcomes.
•• The greatest impediment to cognitive The greatest impediment to cognitive development in children is not drug use, but development in children is not drug use, but poverty. poverty.
Slide 60
Long Term OutcomesLong Term Outcomes
•• Behavioral Disturbances Behavioral Disturbances
•• Poor emotional state control Poor emotional state control
•• Brief attention span Brief attention span
•• Temper Outbursts Temper Outbursts
•• Leaning disabilities Leaning disabilities
•• Delayed speech Delayed speech
•• Developmental delayDevelopmental delay
© 2010 Seattle Children's Hospital
Slide 61 Discharge Plans and Follow upDischarge Plans and Follow up
•• Discharge once baby has been stabilized Discharge once baby has been stabilized medically and socially.medically and socially.
•• A plan is in place to monitor and address any A plan is in place to monitor and address any child protection issueschild protection issues
•• Referral to appropriate community support Referral to appropriate community support agenciesagencies
•• Infants of Infants of OpioidOpioid using mothers have been using mothers have been monitored for monitored for minimumminimum 48 hours48 hours
•• The infant must be monitored for adequate The infant must be monitored for adequate weight gain and intakeweight gain and intake
•• A plan is in place for long term follow up and A plan is in place for long term follow up and evaluation. evaluation.
Slide 62
References
Slide 63
ReferencesReferences
1.1. Committee on Drugs (1998) Neonatal Drug Withdrawal, Committee on Drugs (1998) Neonatal Drug Withdrawal, Pediatrics, Vol.101, no.6Pediatrics, Vol.101, no.6
2.2. HadeedHadeed, A.J., Siegel, S.R. Maternal cocaine use during pregnancy: , A.J., Siegel, S.R. Maternal cocaine use during pregnancy: effect on the newborn infant. Pediatrics.1989;84:205effect on the newborn infant. Pediatrics.1989;84:205--210.210.
3.3. Dicker, M., Leighton, E.A. 1991. Trends in diagnosed drug Dicker, M., Leighton, E.A. 1991. Trends in diagnosed drug problems among newborns. Drug and Alcohol dependency. 28: problems among newborns. Drug and Alcohol dependency. 28: 151151--165.165.
4.4. FrickerFricker, H.S., Segal, S. 1978. Narcotic , H.S., Segal, S. 1978. Narcotic adictionadiction, pregnancy, and , pregnancy, and the newborn. the newborn. The American Journal of Disabled Children. 132: The American Journal of Disabled Children. 132: 360360--366366..
5.5. Adams, E.H., Adams, E.H., GfroererGfroerer, J.C., Rouse, B.A. 1989. Epidemiology of , J.C., Rouse, B.A. 1989. Epidemiology of substance Abuse including alcohol and cigarette smoking. substance Abuse including alcohol and cigarette smoking. Annals Annals of New York Academy of Science. 562; 14of New York Academy of Science. 562; 14--20.20.
© 2010 Seattle Children's Hospital
Slide 64
ReferencesReferences6.6. DoberczakDoberczak, T.M., , T.M., KandallKandall, S.R., Friedman, P. 1993. Relationships , S.R., Friedman, P. 1993. Relationships
between maternal methadone dosage, maternalbetween maternal methadone dosage, maternal--neonatal neonatal methadone dosage, maternal methadone levels and neonatal methadone dosage, maternal methadone levels and neonatal withdrawal. Obstetrics and withdrawal. Obstetrics and GynocolgyGynocolgy. 81; 936. 81; 936--940.940.
7.7. KandallKandall, S.R., , S.R., DoberczakDoberczak, T.M., , T.M., MauerMauer, K.R., , K.R., StrashumStrashum, R.H., , R.H., KortsKorts, , D.C. 1983. Opiate D.C. 1983. Opiate vsvs CNS depressant therapy in neonatal drug CNS depressant therapy in neonatal drug abstinence syndrome. American abstinence syndrome. American JounrnalJounrnal Diseases in Children. 137; Diseases in Children. 137; 378378--382.382.
8.8. Substance Abuse and Mental Health Services Administration, OfficSubstance Abuse and Mental Health Services Administration, Office e of Applied Studies. (2004) National Survey on drug use and healtof Applied Studies. (2004) National Survey on drug use and health: h: National Findings. Washington, DC. U.S. Department of Health andNational Findings. Washington, DC. U.S. Department of Health andHuman Services. Human Services.
9.9. Blackburn, S. (2003). Maternal, fetal, and neonatal physiology: Blackburn, S. (2003). Maternal, fetal, and neonatal physiology: A A clinical perspective (2clinical perspective (2ndnd ed., pp180ed., pp180--212). St. Louis: WB Saunders.212). St. Louis: WB Saunders.
10.10.OsbourneOsbourne, D., Cole, M, Jeffry, H. (2005) Opiate treatment for , D., Cole, M, Jeffry, H. (2005) Opiate treatment for opiate withdrawal in newborn infants. Cochrane Database of opiate withdrawal in newborn infants. Cochrane Database of Systemic Reviews, 3, CD002059.Systemic Reviews, 3, CD002059.
Slide 65
ReferencesReferences
11.11.Finnegan, L.P., Finnegan, L.P., ConnaughtonConnaughton, J.F. Jr, , J.F. Jr, KronKron, R.E. & , R.E. & EmichEmich, J. (1975). , J. (1975).
Neonatal Abstinence Syndrome: Assessment and Management. Neonatal Abstinence Syndrome: Assessment and Management.
Addictive Diseases, 2, 141Addictive Diseases, 2, 141--158.158.
12.12.Lester, B., Lester, B., BoukydisBoukydis, C. and , C. and TwomeyTwomey, J. (2000). Maternal substance , J. (2000). Maternal substance
abuse and child outcome. In C. abuse and child outcome. In C. ZeanahZeanah (Ed.), Handbook of (Ed.), Handbook of infnantinfnant
mental health (2mental health (2ndnd ed., pp161ed., pp161--175) New York; Guilford Press.175) New York; Guilford Press.
13.13.Osborn, D.A., Jeffery, H.E., Cole, M.J. (2008) Sedatives for OpiOsborn, D.A., Jeffery, H.E., Cole, M.J. (2008) Sedatives for Opiate ate
withdrawal in newborn infants. Cochrane Library, Issue 3.withdrawal in newborn infants. Cochrane Library, Issue 3.
14.14.American Academy of Pediatrics, Committee on Drugs. (1998). American Academy of Pediatrics, Committee on Drugs. (1998).
Neonatal Drug Withdrawal. Pediatrics, 9, 1079Neonatal Drug Withdrawal. Pediatrics, 9, 1079--1088.1088.
15.15.Van Barr, A.L., Van Barr, A.L., FleuryFleury, P., , P., SoepatmiSoepatmi, S. , S. UlteeUltee, C.A., , C.A., WesselmanWesselman, P.J. , P.J.
1989. Neonatal behavior after drug dependent pregnancy. 1989. Neonatal behavior after drug dependent pregnancy. Archives Archives
of of DisablitiesDisablities in Children; 64: 235in Children; 64: 235--240. 240.
Slide 66
ReferencesReferences
16.16.Thompson BL Thompson BL et.alet.al. . Prenatal exposure to drugs: effects on brain Prenatal exposure to drugs: effects on brain development and implications for policy and education. development and implications for policy and education. Nature Nature Reviews 10: 303, 2009Reviews 10: 303, 2009
17.17.ShankaranShankaran S S et.alet.al. . Impact of maternal substance use during Impact of maternal substance use during pregnancy on childhood outcome. pregnancy on childhood outcome. Seminars in Fetal and Neonatal Seminars in Fetal and Neonatal Medicine 12: 143, 2007Medicine 12: 143, 2007
18.18.Stanwood GD & Levitt P. Stanwood GD & Levitt P. Drug exposure early in life: Functional Drug exposure early in life: Functional repercussionsrepercussions……CurrCurr OpinOpin PharmPharm 4: 65, 20044: 65, 2004
19.19.WA State Dept. of Health. WA State Dept. of Health. Substance abuse during pregnancy: Substance abuse during pregnancy: Guidelines for screening. 2008 Guidelines for screening. 2008 http://http://www.doh.wa.gov/cfh/mch/documents/screening_guidelines.www.doh.wa.gov/cfh/mch/documents/screening_guidelines.pdfpdf
© 2010 Seattle Children's Hospital
Slide 67
ReferencesReferences
20.20.Rogers JM. Rogers JM. Tobacco and Pregnancy: Overview of Exposures and Tobacco and Pregnancy: Overview of Exposures and Effects. Effects. Birth Def Res 84:1Birth Def Res 84:1--15, 200815, 2008
21.21.Davies J & Bledsoe J. Davies J & Bledsoe J. Prenatal Alcohol and Drug Exposures in Prenatal Alcohol and Drug Exposures in Adoption. Adoption. PedPed ClinClin NA 52:1369, 2005.NA 52:1369, 2005.
22.22.Smith LM Smith LM et.alet.al. . The Infant Development, Environment and Lifestyle The Infant Development, Environment and Lifestyle (IDEAL) Study: Effects of Prenatal Meth. Exposure, (IDEAL) Study: Effects of Prenatal Meth. Exposure, PolydrugPolydrugExposure and Poverty on Intrauterine Growth. Exposure and Poverty on Intrauterine Growth. PediatrPediatr 118: 1149, 118: 1149, 2006. 2006.
23.23.RivkinRivkin MJ MJ et.alet.al. . Volumetric MRI Study of Brain in Children with Volumetric MRI Study of Brain in Children with Intrauterine Exposure to Cocaine, Alcohol, Tobacco & Marijuana. Intrauterine Exposure to Cocaine, Alcohol, Tobacco & Marijuana. PediatrPediatr 121: 741, 2008121: 741, 2008
Slide 68 Questions…
THANK YOU