older drivers and risk to other road users
TRANSCRIPT

Accid. Anal. and Prev., Vol. 29, No. 5, pp. 573–582, 1997© 1997 Elsevier Science Ltd
All rights reserved. Printed in Great Britain0001-4575/97 $17.00 + 0.00
PII: S0001-4575(97)00010-9
OLDER DRIVERS AND RISK TO OTHER ROAD USERS
B D
SmithKline Beecham Pharmaceuticals, Collegeville, PA 19426-0989, U.S.A.
(Received 8 July 1996; in revised form 20 January 1997)
Abstract—This paper examines the degree to which older drivers impose an ‘‘excess’’ risk of death or injuryserious enough to require hospitalization on other road users; that is, the amount of risk older drivers imposeon others above and beyond the amount imposed by drivers who are not yet old. A data set linking crashinformation from police accident reports to hospital discharge data in Wisconsin, 1991, was used to analyzeexcess risk associated with older drivers in two ways. First, the difference in the rate of serious injuries to otherroad users per 100 million driver age-group miles was used to estimate the total number of serious injuriesresulting from the excess risk imposed on others by older drivers. Second, statistical models were used to inferthe association between driver age and crash severity while conditioning on a variety of crash-specificinformation. Drivers aged 65–74 did not appear to impose excess risk of either deaths or injuries requiringhospitalization in either the aggregate or individual level analyses. Drivers aged 75 and over are associated withincreased injuries to others, although the actual number is very small; the individual crash-level analysis suggeststhat a non-trivial part of the excess risk found in the aggregate analysis is a product of confounding. © 1997Elsevier Science Ltd.
INTR ODU CTION drive safely is undiminished’’ (emphasis added;Transportation Research Board, 1994). Despite the
Over the coming decades, the demographics of thegrowing relevance of this issue, research on risks to
driving population will change dramatically because other road users is at best rare. Evans (1991) analyzedof the aging of the baby-boom generation. It has Fatal Accident Reporting System (FARS) data onbeen estimated that by the year 2000, one-third of all the age of drivers involved in fatal motor vehicle–drivers will be aged 55 or over (American Association pedestrian crashes; a literature search found no otherof Retired Persons, 1992); by the year 2030, older work on risks to other road users. Older-driverdrivers are expected to increase by two-thirds over research has tended to focus on areas such as thetheir current level (Transportation Research Board, total or personal risk associated with age groups (see,1994). These demographic shifts might be expected e.g., Insurance Institute for Highway Safety, 1992;to result in a fundamental change in the riskiness Stutts and Martell, 1992); medical interventions (see,associated with driving: it is well known that the e.g., Leveille et al., 1994; Ray et al., 1992); medicalnumber of motor vehicle crashes per unit of distance conditions (see, e.g., Gresset and Meyer, 1994;driven is ‘‘U’’-shaped, with crash risk increasing Koepsell et al., 1994); and subjective awareness ofslightly between the ages of 55 and 60, but greater risk (see, e.g., Holland, 1993; Guppy, 1993).increases in risk with each successive five-year interval While the total level of risk faced by older drivers( Insurance Institute for Highway Safety, 1992). (and their passengers) is an interesting issue in itsSimilarly, the risk of involvement in crashes resulting own right, it is not the critical issue in assessing thein a fatality is also ‘‘U’’-shaped relative to driver age likely change in risk to road users in general from an(Insurance Institute for Highway Safety, 1992). increase in the number of older drivers over the
The prospect of more older drivers on the road coming decades. The central issue in assessing thehas generated concern among traffic safety experts effect of more older drivers on road safety in generaland policy-makers alike. One result was that the is the degree to which older drivers impose a higherTransportation Research Board of the National level of risk on other road users. For example, ifResearch Council convened a meeting in 1993 to older drivers were, say, ten times as likely to be‘‘address the means by which licensing agencies involved in a crash as other drivers, but all oldercan discharge their obligation to protect the public driver crashes were single-vehicle crashes, an increasefrom those elderly drivers who cannot operate safely in the number of older drivers would not affect the
risk associated with road use by non-older drivers,while assuring the mobility of those whose ability to
573

574 B. D
even though the number of crashes involving older 7–10%. Karlson et al. (1994) also report that 23% ofrelevant discharge records failed to match with andrivers would increase. If an increase in the number
of older drivers is to result in an increased level of accident report; of these, 10% were estimated to notmatch because of missing data, and another 30%risk to road users in general, it must be the case that
older drivers impose a greater risk on other road failed to match because an accident report did notexist (e.g., crashes occurring outside of Wisconsin,users than not-yet-older drivers do.
This paper uses two methods to examine the transfers between hospitals, readmissions, etc.). Theremaining 60% of ‘‘failed matches’’ are a consequencequestion of whether older drivers impose more risk
on other road users than do drivers under age 65. of the stringency of match criteria: relaxing thecriteria would result in more matches, but also inThe first approach focusses on the difference in risk
to others per unit of distance driven by an age group. more false matches. Under the criteria chosen by theWisconsin CODES group, approximately two-thirdsThe resulting estimate of risk differences is then used
to calculate the actual number of injuries attributable of all records were successfully matched, and approxi-mately three-quarters of all records which were capa-to the ‘extra’ risk older drivers impose on other road
users over and above the level imposed by drivers ble of being matched were successfully matched.There is no reason to believe that the failed matchesunder 65. By focussing on age groups in the aggregate,
this approach ignores the details of specific crashes. were the product of a selection process, althoughobviously there is no feasible way of checking.The second approach analyzes crash-level data to
take account of available information relevant to The data used here are a subset of the CODESdata. Because our interest is in the injury risk driverscrash outcomes, such as the types of vehicles involved
in a crash. This approach results in estimates of the impose on other road users, single-unit (a unit beinga motor vehicle, bike or pedestrian) collisions aredegree to which driver age is associated with crash
severity (as defined by crash outcomes). excluded; such collisions comprise about 20–25% ofall crashes. Collisions involving three or more unitsare also excluded, because there is no way of telling
DATAwhich component of a collision involving three ormore units was responsible for a given injury (i.e. ifThe data used in this paper are from the
Wisconsin Crash Outcomes Data Evaluation System a person in unit A was injured in a three-vehiclecollision, we cannot tell if the injury resulted from(CODES) for the year 1991. These data are the result
of a matching process linking police accident reports the collision of vehicles A and B, or the collisionbetween vehicles A and C ); these crashes account forfrom the Wisconsin Department of Transportation
to inpatient discharge records for acute-care hospitals less than 10% of all crashes. Thus, the data hereconsist of all 77,458 reported collisions in Wisconsinfrom the Office of the Commissioner of Insurance.1
Because personal identifiers are not available, the involving two units during 1991, or approximatelytwo-thirds of all crashes in the CODES data.data are linked through a probabilistic matching
process. Briefly, the process uses a number of primarydata items (e.g., date of crash/admission to hospital,
ME THOD S AND RESU LTSbirth date, sex, and zip code of residence) to establishlikely matches; if necessary, a secondary group of This section analyzes the Wisconsin CODES
data to estimate the level of risk older drivers imposevariables (e.g., county of the event, health servicearea of the event, etc.) is used (Karlson and Quade, on other road users, and whether this level of risk
differs from that imposed by other drivers, i.e. those1994). A more complete description is in Karlsonet al. (1994). who are not yet old. Other road users are defined as
persons outside the driver’s vehicle; while not aBecause the matching process is probabilistic,errors occur. These take two forms: false matches, in perfect measure, this definition distinguishes between
persons with some choice about whether to acceptwhich the crash information of one individual ismatched to the hospital discharge information of the risks associated with a particular person’s driving
behaviors (i.e., persons voluntarily entering a caranother person; and non-matches, where records ofa crash resulting in injuries fails to link with a driven by person X ), and those persons with no
choice in the matter (i.e., persons with whom a cardischarge report. Karlson et al. (1994) report onthree different methods of estimating the proportion driven by person X collides). The age of 65 is used
as a threshold for inclusion in the ‘‘older driver’’of false matches, and estimate a false-match rate ofcategory, and the risk to others is measured againstall drivers below age 65. Although this approach is1Wisconsin requires any crash resulting in $500 property
damage or any injury be reported. uninformative about the risks of older drivers relative
575Older drivers and risk to other road users
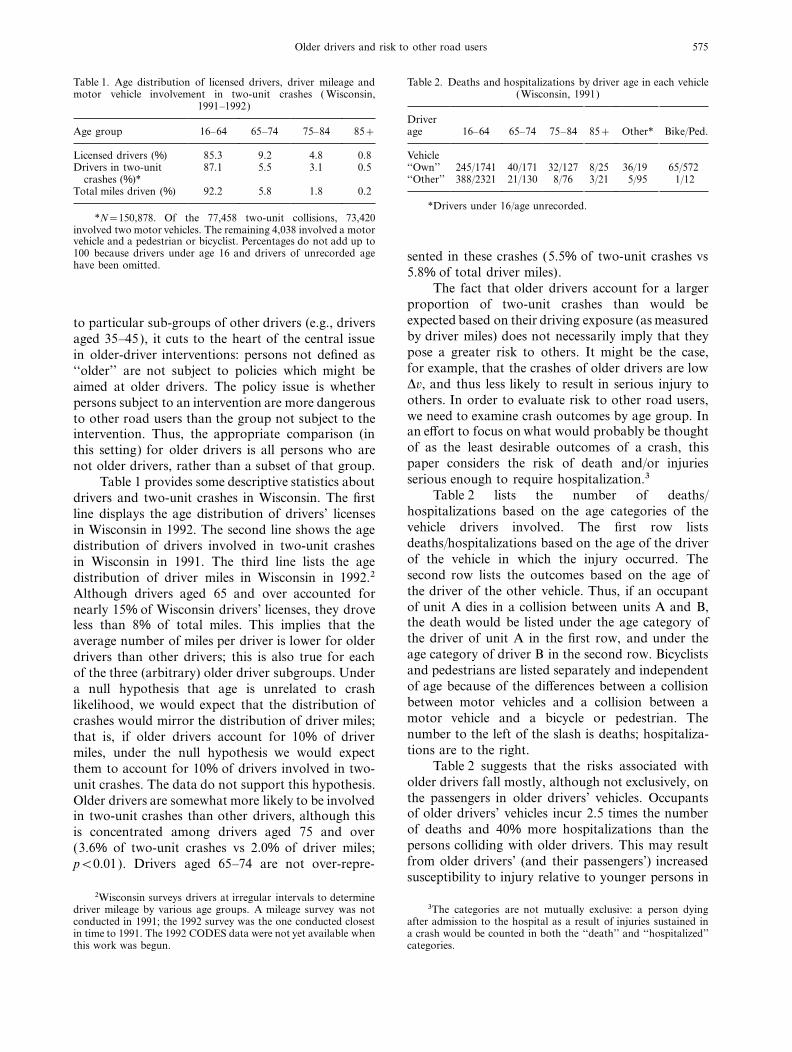
Table 1. Age distribution of licensed drivers, driver mileage and Table 2. Deaths and hospitalizations by driver age in each vehicle(Wisconsin, 1991)motor vehicle involvement in two-unit crashes ( Wisconsin,
1991–1992)Driverage 16–64 65–74 75–84 85+ Other* Bike/Ped.Age group 16–64 65–74 75–84 85+
Licensed drivers (%) 85.3 9.2 4.8 0.8 Vehicle‘‘Own’’ 245/1741 40/171 32/127 8/25 36/19 65/572Drivers in two-unit 87.1 5.5 3.1 0.5
crashes (%)* ‘‘Other’’ 388/2321 21/130 8/76 3/21 5/95 1/12Total miles driven (%) 92.2 5.8 1.8 0.2
*Drivers under 16/age unrecorded.*N=150,878. Of the 77,458 two-unit collisions, 73,420
involved two motor vehicles. The remaining 4,038 involved a motorvehicle and a pedestrian or bicyclist. Percentages do not add up to100 because drivers under age 16 and drivers of unrecorded age sented in these crashes (5.5% of two-unit crashes vshave been omitted.
5.8% of total driver miles).The fact that older drivers account for a larger
proportion of two-unit crashes than would beexpected based on their driving exposure (as measuredto particular sub-groups of other drivers (e.g., driversby driver miles) does not necessarily imply that theyaged 35–45), it cuts to the heart of the central issuepose a greater risk to others. It might be the case,in older-driver interventions: persons not defined asfor example, that the crashes of older drivers are low‘‘older’’ are not subject to policies which might beDv, and thus less likely to result in serious injury toaimed at older drivers. The policy issue is whetherothers. In order to evaluate risk to other road users,persons subject to an intervention are more dangerouswe need to examine crash outcomes by age group. Into other road users than the group not subject to thean effort to focus on what would probably be thoughtintervention. Thus, the appropriate comparison (inof as the least desirable outcomes of a crash, thisthis setting) for older drivers is all persons who arepaper considers the risk of death and/or injuriesnot older drivers, rather than a subset of that group.serious enough to require hospitalization.3Table 1 provides some descriptive statistics about
Table 2 lists the number of deaths/drivers and two-unit crashes in Wisconsin. The firsthospitalizations based on the age categories of theline displays the age distribution of drivers’ licensesvehicle drivers involved. The first row listsin Wisconsin in 1992. The second line shows the agedeaths/hospitalizations based on the age of the driverdistribution of drivers involved in two-unit crashesof the vehicle in which the injury occurred. Thein Wisconsin in 1991. The third line lists the agesecond row lists the outcomes based on the age ofdistribution of driver miles in Wisconsin in 1992.2the driver of the other vehicle. Thus, if an occupantAlthough drivers aged 65 and over accounted forof unit A dies in a collision between units A and B,nearly 15% of Wisconsin drivers’ licenses, they drovethe death would be listed under the age category ofless than 8% of total miles. This implies that thethe driver of unit A in the first row, and under theaverage number of miles per driver is lower for olderage category of driver B in the second row. Bicyclistsdrivers than other drivers; this is also true for eachand pedestrians are listed separately and independentof the three (arbitrary) older driver subgroups. Underof age because of the differences between a collisiona null hypothesis that age is unrelated to crashbetween motor vehicles and a collision between alikelihood, we would expect that the distribution ofmotor vehicle and a bicycle or pedestrian. Thecrashes would mirror the distribution of driver miles;number to the left of the slash is deaths; hospitaliza-that is, if older drivers account for 10% of drivertions are to the right.miles, under the null hypothesis we would expect
Table 2 suggests that the risks associated withthem to account for 10% of drivers involved in two-older drivers fall mostly, although not exclusively, onunit crashes. The data do not support this hypothesis.the passengers in older drivers’ vehicles. OccupantsOlder drivers are somewhat more likely to be involvedof older drivers’ vehicles incur 2.5 times the numberin two-unit crashes than other drivers, although thisof deaths and 40% more hospitalizations than theis concentrated among drivers aged 75 and overpersons colliding with older drivers. This may result(3.6% of two-unit crashes vs 2.0% of driver miles;from older drivers’ (and their passengers’) increasedp<0.01). Drivers aged 65–74 are not over-repre-susceptibility to injury relative to younger persons in
2Wisconsin surveys drivers at irregular intervals to determinedriver mileage by various age groups. A mileage survey was not 3The categories are not mutually exclusive: a person dying
after admission to the hospital as a result of injuries sustained inconducted in 1991; the 1992 survey was the one conducted closestin time to 1991. The 1992 CODES data were not yet available when a crash would be counted in both the ‘‘death’’ and ‘‘hospitalized’’
categories.this work was begun.
576 B. D
a crash of a given level of severity (see, e.g., Evans, drivers under 65), and multiplying by the number ofmiles driven by the age group.4 This is an estimate1988).
Although Table 2 tells us how many deaths of the number of deaths and hospitalizations attribut-able to the risk older drivers impose on other roadand/or hospitalizations resulted from collisions
involving older drivers, it does not address our central users over and above the ‘‘baseline’’ level of the riskdrivers under age 65 impose on other road users.concern, i.e., how risk to other road users varies with
driver age. One important issue is evident from Tables 3 and 4 indicate that drivers aged 65–74imposed a negative excess risk on other road users;Table 1: older drivers average fewer miles per year
than other drivers, and so have fewer ‘‘opportunities’’ that is, the two-unit collisions drivers aged 65–74were involved in resulted in fewer deaths and hospital-to injure other road users. This, together with the
fact that there are many more drivers under age 65 izations per 100 million miles of driving by the groupthan did the two-unit collisions of drivers under 65.than there are older drivers, suggests that we would
expect to observe more total serious injuries among Drivers aged 75–84 were associated with slightlymore deaths per 100 million driver miles than driverspersons colliding with drivers under 65 than among
persons colliding with older drivers, even if crashes under 65 (0.032 deaths per 100 million miles). Theslight excess risk combined with the relatively lowinvolving older drivers were on average more severe
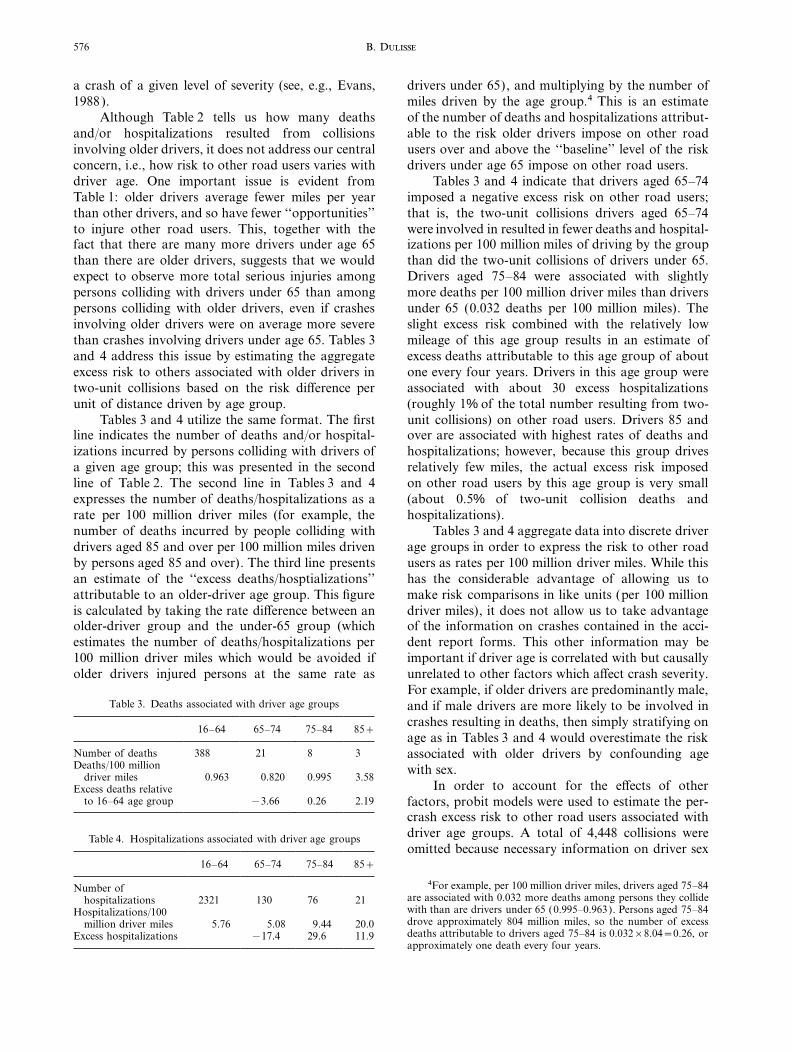
than crashes involving drivers under age 65. Tables 3 mileage of this age group results in an estimate ofexcess deaths attributable to this age group of aboutand 4 address this issue by estimating the aggregate
excess risk to others associated with older drivers in one every four years. Drivers in this age group wereassociated with about 30 excess hospitalizationstwo-unit collisions based on the risk difference per
unit of distance driven by age group. (roughly 1% of the total number resulting from two-unit collisions) on other road users. Drivers 85 andTables 3 and 4 utilize the same format. The first
line indicates the number of deaths and/or hospital- over are associated with highest rates of deaths andhospitalizations; however, because this group drivesizations incurred by persons colliding with drivers of
a given age group; this was presented in the second relatively few miles, the actual excess risk imposedon other road users by this age group is very smallline of Table 2. The second line in Tables 3 and 4
expresses the number of deaths/hospitalizations as a (about 0.5% of two-unit collision deaths andhospitalizations).rate per 100 million driver miles (for example, the
number of deaths incurred by people colliding with Tables 3 and 4 aggregate data into discrete driverage groups in order to express the risk to other roaddrivers aged 85 and over per 100 million miles driven
by persons aged 85 and over). The third line presents users as rates per 100 million driver miles. While thishas the considerable advantage of allowing us toan estimate of the ‘‘excess deaths/hosptializations’’
attributable to an older-driver age group. This figure make risk comparisons in like units (per 100 milliondriver miles), it does not allow us to take advantageis calculated by taking the rate difference between an
older-driver group and the under-65 group (which of the information on crashes contained in the acci-dent report forms. This other information may beestimates the number of deaths/hospitalizations per
100 million driver miles which would be avoided if important if driver age is correlated with but causallyunrelated to other factors which affect crash severity.older drivers injured persons at the same rate asFor example, if older drivers are predominantly male,
Table 3. Deaths associated with driver age groups and if male drivers are more likely to be involved incrashes resulting in deaths, then simply stratifying on
16–64 65–74 75–84 85+age as in Tables 3 and 4 would overestimate the risk
Number of deaths 388 21 8 3 associated with older drivers by confounding ageDeaths/100 million with sex.
driver miles 0.963 0.820 0.995 3.58In order to account for the effects of otherExcess deaths relative
to 16–64 age group −3.66 0.26 2.19 factors, probit models were used to estimate the per-crash excess risk to other road users associated withdriver age groups. A total of 4,448 collisions wereTable 4. Hospitalizations associated with driver age groupsomitted because necessary information on driver sex
16–64 65–74 75–84 85+4For example, per 100 million driver miles, drivers aged 75–84Number of
are associated with 0.032 more deaths among persons they collidehospitalizations 2321 130 76 21with than are drivers under 65 (0.995–0.963). Persons aged 75–84Hospitalizations/100drove approximately 804 million miles, so the number of excessmillion driver miles 5.76 5.08 9.44 20.0deaths attributable to drivers aged 75–84 is 0.032×8.04=0.26, orExcess hospitalizations −17.4 29.6 11.9approximately one death every four years.
577Older drivers and risk to other road users
Table 5. Deaths
Model 1 Model 2
Unit number 1 2
Specification A B A B A B
Driver age65–74 0.236 0.268 0.201 0.244 0.281 0.295
(0.068) (0.094) (0.100) (0.106) (0.101) (0.110)0.22% 0.27% 0.20% 0.26% 0.25% 0.27%
75–84 0.377 0.426 0.354 0.418 0.404 0.436(0.076) (0.084) (0.102) (0.110) (0.119) (0.130)0.44% 0.54% 0.45% 0.58% 0.43% 0.49%
85+ 0.432 0.427 0.430 0.402 0.431 0.472(0.167) (0.192) (0.212) (0.252) (0.280) (0.295)0.55% 0.54% 0.61% 0.55% 0.48% 0.56%
Other driver age65–74 0.023 0.023 0.113 0.121 −0.117 −0.132
(0.084) (0.094) (0.108) (0.117) (0.149) (0.163)0.02% 0.02% 0.10% 0.11% 0.06% 0.06%
75–84 −0.139 −0.212 −0.044 −0.095 −0.240 −0.351(0.143) (0.162) (0.195) (0.210) (0.244) (0.258)0.08% 0.11% 0.03% 0.06% 0.10% 0.13%
85+ −0.042 −0.122 * * 0.159 0.090(0.306) (0.357) (0.311) (0.372)0.03% 0.07% 0.12% 0.06%
−2×log likelihood 3912.9 3328.6 2181.2 1850.3 1720.0 1458.2
*No deaths occurred in unit 1 vehicles colliding with drivers aged 85+.
was missing for one or both drivers. Additionally, differential risk older drivers impose on other roadusers. In order to do so, it is important to avoidbecause one of the models discussed below utilizes
the data as crash pairs, the 4,038 collisions involving including variables which are a consequence ofchoices which are a function of driver age. If suchpedestrians or bicyclists were deleted from the data:
not deleting these crashes would result in a statistical variables are included, the coefficient of the agevariables cannot be interpreted as the contributionmodel assuming that the likelihood of sustaining a
serious injury is the same when colliding with a bike of age to the likelihood of a given outcome. A simpleexample illustrates the point. Suppose that there areor pedestrian as when colliding with a car. Thus, the
data analyzed in this section consists of 137,944 two types of collisions (A and B), and that type Acrashes are more likely to result in a death. Supposevehicles/drivers involved in 68,972 collisions.
Two models were estimated. The models differ further that older drivers are twice as likely as otherdrivers to be involved in type A crashes (i.e., crashsolely on whether the order in which the vehicles
were entered on the accident report form is assumed type is a function of age). Including crash type as anexplanatory variable in a model with death as theto contribute meaningful information as to the likeli-
hood of injuries resulting from the crash. For exam- dependent variable would mean that the age-relatedeffect on crash type (and therefore the likelihood ofple, it could be the case that the vehicle held to be
‘‘at fault’’ in the crash is more likely to be entered death(s) as a consequence of the crash) would not bereflected in the coefficient of the age variable, resultingon the accident report form first, and that persons in
the ‘‘at fault’’ vehicle are less likely to be injured in an underestimate of the age-related effect on thelikelihood of a death.seriously in the crash. If this were the case, then we
would wish to obtain separate estimates for the effects In order to avoid this problem, we want to useexplanatory variables which do not reflect choicesof characteristics of the drivers of vehicles 1 (the
vehicle entered on the accident report form first) and made by drivers that might be related to their age.Determining which variables meet that criterion is2. Thus, the estimates from the first model are
obtained by including all 137,944 vehicles involved ultimately arbitrary, in that one can make argumentsfor and against including particular variables.in crashes involving two motor vehicles in a single
estimation equation. The estimates from the second Consequently, each of the models was estimatedunder two specifications. The first specificationmodel utilize separate equations for vehicles 1 and 2,
each of which contains data on 68,972 vehicles. included only the age category of each driver, the sexof each driver, and the type of vehicles involved inThe interest here is to obtain an estimate of the
578 B. D
Table 6. Hospitalizations
Model 1 Model 2
Unit number 1 2
Specification A B A B A B
Driver age65–74 0.211 0.232 0.217 0.245 0.205 0.222
(0.035) (0.037) (0.050) (0.053) (0.045) (0.052)0.35% 0.40% 0.92% 1.07% 0.90% 1.00%
75–84 0.350 0.358 0.356 0.366 0.345 0.359(0.041) (0.043) (0.056) (0.059) (0.060) (0.063)0.70% 0.73% 1.76% 1.84% 1.77% 1.87%
85+ 0.446 0.462 0.525 0.530 0.344 0.378(0.091) (0.095) (0.119) (0.125) (0.143) (0.148)1.02% 1.08% 3.13% 3.18% 1.77% 2.01%
Other driver age65–74 −0.068 −0.073 −0.045 −0.056 −0.091 −0.089
(0.043) (0.046) (0.061) (0.064) (0.062) (0.064)0.08% 0.08% 0.14% 0.18% 0.29% 0.28%
75–84 0.042 0.017 0.034 0.018 0.047 0.013(0.052) (0.055) (0.079) (0.083) (0.070) (0.074)0.06% 0.02% 0.12% 0.06% 0.17% 0.05%
85+ 0.083 0.070 0.150 0.190 0.022 −0.043(0.120) (0.126) (0.170) (0.176) (0.168) (0.182)0.12% 0.10% 0.59% 0.78% 0.08% 0.14%
−2×log likelihood 18,265.6 16,992.8 8,867.2 8,243.7 9,388.4 8,728.1
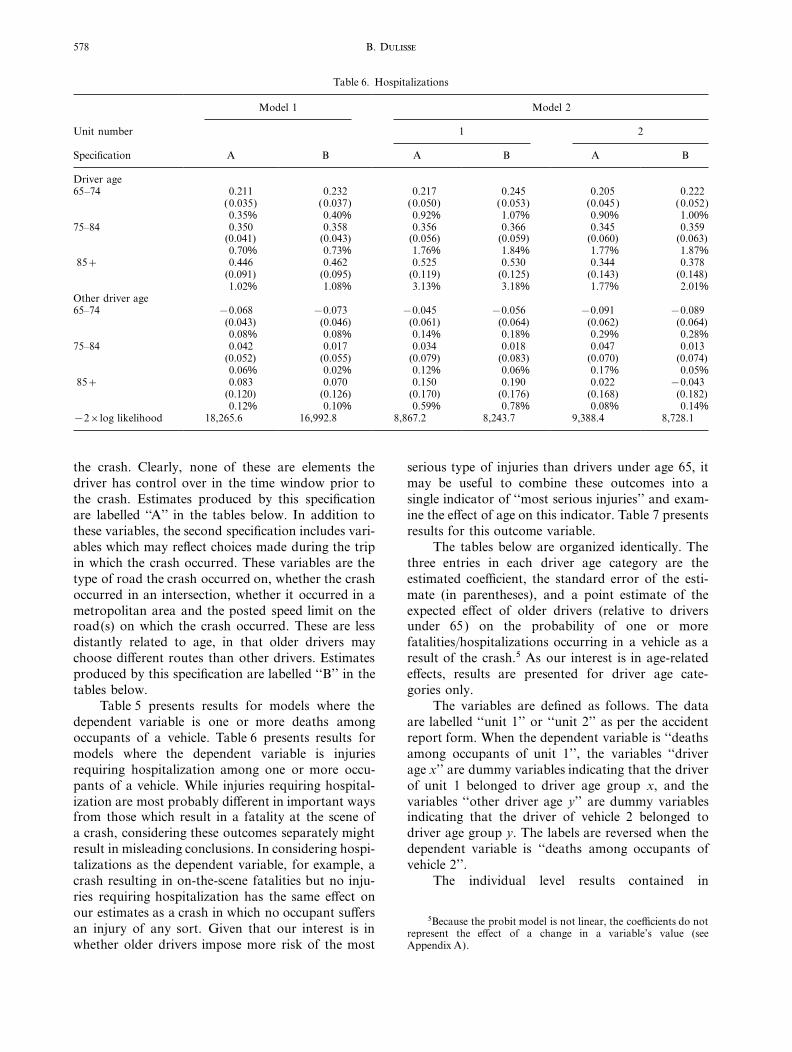
the crash. Clearly, none of these are elements the serious type of injuries than drivers under age 65, itmay be useful to combine these outcomes into adriver has control over in the time window prior to
the crash. Estimates produced by this specification single indicator of ‘‘most serious injuries’’ and exam-ine the effect of age on this indicator. Table 7 presentsare labelled ‘‘A’’ in the tables below. In addition to
these variables, the second specification includes vari- results for this outcome variable.The tables below are organized identically. Theables which may reflect choices made during the trip
in which the crash occurred. These variables are the three entries in each driver age category are theestimated coefficient, the standard error of the esti-type of road the crash occurred on, whether the crash
occurred in an intersection, whether it occurred in a mate (in parentheses), and a point estimate of theexpected effect of older drivers (relative to driversmetropolitan area and the posted speed limit on the
road(s) on which the crash occurred. These are less under 65) on the probability of one or morefatalities/hospitalizations occurring in a vehicle as adistantly related to age, in that older drivers may
choose different routes than other drivers. Estimates result of the crash.5 As our interest is in age-relatedeffects, results are presented for driver age cate-produced by this specification are labelled ‘‘B’’ in the
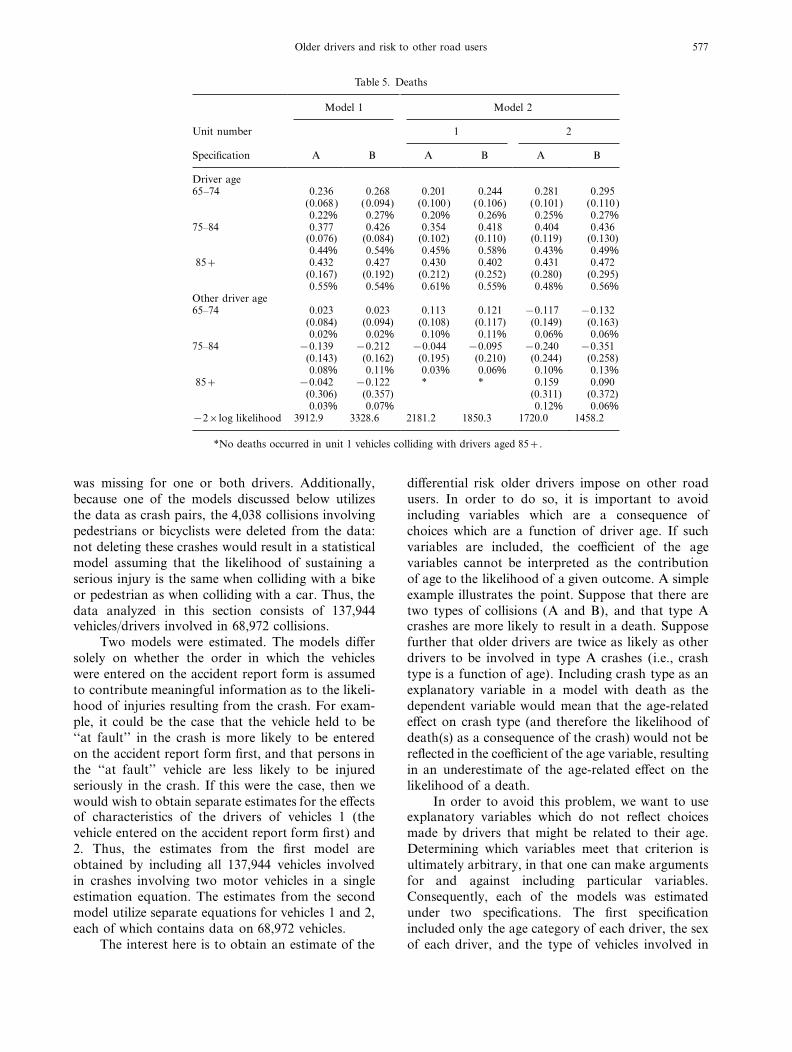
tables below. gories only.The variables are defined as follows. The dataTable 5 presents results for models where the
dependent variable is one or more deaths among are labelled ‘‘unit 1’’ or ‘‘unit 2’’ as per the accidentreport form. When the dependent variable is ‘‘deathsoccupants of a vehicle. Table 6 presents results for
models where the dependent variable is injuries among occupants of unit 1’’, the variables ‘‘driverage x’’ are dummy variables indicating that the driverrequiring hospitalization among one or more occu-
pants of a vehicle. While injuries requiring hospital- of unit 1 belonged to driver age group x, and thevariables ‘‘other driver age y’’ are dummy variablesization are most probably different in important ways
from those which result in a fatality at the scene of indicating that the driver of vehicle 2 belonged todriver age group y. The labels are reversed when thea crash, considering these outcomes separately might
result in misleading conclusions. In considering hospi- dependent variable is ‘‘deaths among occupants ofvehicle 2’’.talizations as the dependent variable, for example, a
crash resulting in on-the-scene fatalities but no inju- The individual level results contained inries requiring hospitalization has the same effect onour estimates as a crash in which no occupant suffers
5Because the probit model is not linear, the coefficients do notan injury of any sort. Given that our interest is in represent the effect of a change in a variable’s value (see
Appendix A).whether older drivers impose more risk of the most

579Older drivers and risk to other road users
Table 7. Deaths and/or hospitalizations
Model 1 Model 2
Unit number 1 2
Specification A B A B A B
Driver age65–74 0.212 0.236 0.200 0.233 0.226 0.243
(0.034) (0.036) (0.049) (0.052) (0.048) (0.050)1.00% 1.13% 0.91% 1.10% 1.09% 1.20%
75–84 0.353 0.365 0.360 0.377 0.347 0.361(0.040) (0.042) (0.055) (0.058) (0.058) (0.062)1.93% 2.02% 1.96% 2.09% 1.91% 2.02%
85+ 0.477 0.494 0.538 0.542 0.397 0.434(0.087) (0.092) (0.114) (0.121) (0.134) (0.140)2.98% 3.14% 3.54% 3.58% 2.31% 2.63
Other driver age65–74 −0.069 −0.075 −0.036 −0.048 −0.102 −0.101
(0.042) (0.044) (0.058) (0.062) (0.060) (0.064)0.24% 0.26% 0.13% 0.17% 0.34% 0.34%
75–84 0.026 −0.000 0.016 −0.000 0.033 −0.003(0.051) (0.055) (0.078) (0.083) (0.069) (0.073)0.14% 0.00% 0.06% 0.00% 0.13% 0.01%
85+ 0.050 0.036 0.118 0.161 −0.012 −0.083(0.120) (0.127) (0.170) (0.177) (0.169) (0.183)0.20% 0.14% 0.49% 0.70% 0.04% 0.29%
−2×log likelihood 19,728.8 18,117.5 9,680.4 8,872.3 10,037.0 9,221.9
Tables 5–7 provide no meaningful support for a of serious injury (e.g., death or injury requiringhospitalization) than persons colliding with not-yet-hypothesis that older drivers impose excess risks ofolder drivers. These data largely fail to identify suchserious injuries on other road users. Many of theincreases in risk associated with older drivers.individual coefficients, particularly in Table 7 (any
The results presented in Section 3 provide noserious injury), are negative (although none are statis-support for the hypothesis that drivers aged 65–74tically significant at meaningful levels). Of the esti-impose an excess risk on other road users relative tomated positive coefficients (suggesting increased risk)drivers under 65. The analysis of the aggregated dataresulting from model 1 in any of the three tables,indicate that per 100 million driver miles, driversnone has an associated test statistic that rejects theaged 65–74 are associated with fewer deaths andnull hypothesis of b=0 (i.e., no difference betweeninjuries requiring hospitalization to other road usersthe older driver group and drivers under 65) at thethan drivers under age 65. The analysis of the indivi-p=0.42 level; none of the estimated positive coeffi-dual-level data suggests that the excess risk of seriouscients from model 2 have an associated test statisticinjury to others from drivers in this age group iswhich rejects the null hypothesis of b=0 at the p=sufficiently small that it cannot be distinguished from0.28 level. It is reasonable to conclude that these datathe background ‘‘noise’’.suggest that crashes involving older drivers are not
For drivers aged 75 and over, the mode ofmore probable than crashes involving drivers under analysis has some effect on the estimate of excess riskage 65 to result in serious injuries to other road users. to others associated with older drivers. The aggregate
analysis suggests that drivers 75–84 impose excessrisk of injuries requiring hospitalization on otherD ISC USSIONroad users, and that drivers aged 85 and over impose
Physical skills used while driving (e.g., vision, excess risk of death and injuries requiring hospitaliza-hearing, reflexes, etc.) generally erode with age. If the tion on other road users. The level of excess risk toerosion of these skills reduces the ability of older others imputed by the aggregate analysis is, however,persons to drive safely, we would expect not only fairly small in the context of total serious injuriesthat they would incur more crashes, but also that as (1% or smaller). The individual level analysis findsa consequence of these crashes, we would observe no meaningful excess risk of death or injuries requir-more serious injuries. In particular, if the erosion of ing hospitalization associated with drivers aged 75skills among older drivers makes them more danger- and over, and suggests that part of the excess riskous to other road users, we would expect that persons found in the aggregate analysis is probably due to
confounding with other crash factors.colliding with older drivers would face a higher risk

580 B. D
The strengths and weaknesses of these two meth- hood of the same specification in model 1. Again,likelihood ratio tests reject this null hypothesis forods are complementary. The strength of the aggregate
analysis is that the risk is denominated in terms of each specification in Tables 5–7. However, as ourinterest is in estimating the excess risk of older driversexposure (i.e., miles driven by age group). The weak-
ness of this approach is that due to the aggregation, rather than providing the best possible ‘‘fit’’ to thedata, the likelihood ratio test’s rejection of the nullindividual crash information is ignored. The presence
of the individual crash-level information is the hypothesis does not indicate that specification B is tobe preferred to that of specification A. The decisionstrength of the second approach. Unfortunately,
because the data are crash-based and do not contain as to which estimates are ‘‘best’’ is not in this casean issue of statistical inference, but rather an ulti-information on miles driven by each driver, we cannot
control for an important indicator of exposure. While mately arbitrary choice based on the researcher’s(and reader’s) assessment of which specification isthese data limitations prevent us from estimating the
total risk to others of death or hospitalization associ- more appropriate given the concerns about theestimates.ated with driver age, they do not affect our ability to
draw inferences about risk to others conditioning on A related issue of interest involves the choice ofmodel. The choice of model depends on whether thea crash.
It is important to recognize that despite the process by which drivers are entered onto the accidentreport form is random, or conveys meaningful infor-complimentary strengths and weaknesses, the two
approaches offer consistent implications as to whether mation. In Tables 5–7, the log likelihood test rejectsthe null hypothesis of ‘‘no difference’’. Once again,older drivers are more dangerous than the not yet
old. The aggregate analysis, accounting for exposure however, we should not choose the ‘‘best’’ estimatesbased on statistical testing, but rather on whether webut ignoring crash-specific details, suggests that the
excess risk to others of serious injuries is confined to believe that the process resulting in the order of entryin the accident report form conveys meaning.drivers aged 75 and over, and that this excess risk
is relatively small. The individual level analyses, Fortunately, the choice of model 1 vs model 2, orspecification A vs specification B, is not a majoralthough not accounting for exposure (or crash risk
per unit of exposure), suggest that controlling for issue: the conclusion that older drivers are not impos-ing meaningful excess risk on other road users iscrash-specific information reduces the association
between driver age and risk to others to a level robust across the choices of model and specification.The above analyses have ignored the issue ofindistinguishable from background noise. It is interes-
ting to note, however, that the associations between fault in crashes. It is intuitive to think that ignoringfault is problematic. Consider, for example, a collisiondriver age and risk to occupants in the driver’s vehicle
(as opposed to risk to others) were large and statistic- resulting when driver A runs through a stop sign andcollides with driver B. We might think that the injuriesally significant. The estimated coefficients and mean
levels of excess risk associated with a driver’s age in to persons in vehicle B say much more about the riskimposed on other road users by driver A than injuriesrelation to serious injuries in his own vehicle are
generally an order of magnitude larger than the to persons in vehicle A says about driver B. Thiswould suggest that we focus our attention on injuriescorresponding values on the likelihood of serious
injuries in the colliding vehicle. This suggests that the incurred by persons who were not at fault in acollision, i.e., those caused by the ‘‘guilty’’ party, asresults on risk to others are not simply due to large
standard errors driven by small cell sizes. a means of assessing the risks drivers impose on otherroad users in a more meaningful way.A few comments on methodological issues are
appropriate. The first is that specification B provides There are two reasons why such an approach isless useful than it might appear. First, as counter-a better fit to the data (as indicated by the smaller
log likelihood values) than specification A. Likelihood intuitive as it might seem, driver B in our example isresponsible for some of the risk associated with theratio tests for each model in each table reject the null
hypothesis that specification B provides no better fit crash. In order to see this point, consider the samesituation (driver A running through a stop sign)than specification A. Second, it is also clear that the
process determining the order in which drivers are under the circumstance that all other drivers wereprohibited from using the road. In that case, noentered on the accident report form conveys informa-
tion which improves the fit (as indicated by a compari- collision with another vehicle is possible. Thus, itmust be the case that all drivers impose risks on otherson of the log likelihoods) to the data. Under the
null hypothesis that driver order does not improve road users simply by their very presence on the road.Focussing on injuries incurred by the ‘‘innocent vic-the fit, the sum of the log likelihoods for a given
specification in model 2 should equal the log likeli- tims’’ while excluding injuries incurred by the ‘‘guilty

581Older drivers and risk to other road users
and Prevention, Atlanta, GA. Thanks are gratefully extended toparties’’ removes some part of the risk we want toTrudy Karlson and Chip Quade of the Center for Health Systems
consider. Further, if there was an age-related differ- Research and Analysis at the University of Wisconsin for providingthe CODES data and general helpfulness. Jeff Sacks and Janeence in the likelihood of being the ‘‘innocent victim’’Stutts provided helpful comments on early drafts of this paper.in a crash, focussing on injuries caused by ‘‘at fault’’
drivers could seriously bias our results.6A second reason why we might not wish to focus APPEND IX A
exclusively on at-fault drivers is that relatively fewIn linear models, the interpretation of coefficients of variablesserious crashes result in a ticket, the most obvious is straightforward: the coefficient value is the expected change in
indicator of culpability. Only 15% of crashes resulting the value of the dependent variable resulting from a unit changein the value of the associated right-hand side variable. In non-in a fatality produce a traffic citation for one or bothlinear models such as the logit or probit, however, such andrivers; less than half of crashes resulting in a hospi- interpretation of the coefficient is invalid. Consider the following
talization produce a ticket. Thus, as a practical simple example. Suppose that the probability of an event yoccurring is a function of a single variable x, such that E [prob( y=matter, by focussing on crashes in which culpability1)]=F(xb), where E […] denotes the expected value operator, andhas been assigned (in the form of a ticket) we F(z) is the relevant distribution function evaluated at the value z.
eliminate 85% of crashes resulting in fatalities, and The expected change in the probability of observing the event y asa result of a small increase in the value of x would be:over half of the crashes resulting in hospitalizations.
∂E [prob(y=1)]/∂x=∂F(xb)/∂(xb) ∂(xb)/∂xThese are the crashes we are most interested in fromthe viewpoint of risk imposed on others, and conse- =f (xb )bquently it makes little sense to ignore them. This where f(z) is the relevant probability density function evaluated atimplicitly suggests that non-ticket crashes resulting in z. Clearly, the expected increase in the probability of observing
y=1 is not b, but rather a function of b which depends on theserious injuries are no different from non-ticketinitial value of x (through f(xb)). Roughly speaking, the closercrashes in which no one is injured. This seems the value of xb is to 0, the larger the marginal effect of a change
unlikely. in x on the probability of observing y=1.The same conclusion holds for the coefficient of a categorical
variable, as is the case of interest here. Suppose that the probabilityof observing y=1 was a function of a continuous variable x asCON CLU SIO Nabove, and a categorical variable w which takes the value 1 if anindividual belongs to a given group and 0 otherwise, i.e.,Data linking police accident reports to hospitalE[prob( y=1)]=F(xb+wc). The expected difference in the prob-discharge data covering all reported crashes in ability of observing y=1 between persons for whom w=1 and
Wisconsin in 1991 were used to analyze the excess w=0 for a given value of x is F(xb+c)−F(xb)≠c. Again, theeffect on the expected value of observing y=1 depends on therisk of deaths and injuries requiring hospitalizationvalue of xb.imposed by older drivers on other road users. For both the continuous and categorical variable cases, inter-
Analyses were conducted on aggregated data using preting the value of a coefficient depends critically on the scalevalue xb chosen. Any number of alternative methods have beenage-group level exposure data, and on individual-proposed for evaluating the marginal effect associated with a givenlevel data without measures of exposure but richer coefficient. For example, some researchers choose to average the
information about the circumstances of individual estimated marginal effect across all individuals; others set the valueof each variable in x to its mean value. The values given in thecrashes. Both approaches indicate that drivers agedthird lines of Tables 5–7 were calculated by setting the scale vector65–74 do not impose an excess risk of deaths or non- xb to the value such that W(xb) equalled the mean probability of
fatal serious injuries on other road users. In the the relevant event. For example, occupants of 1,840 of the 137,944vehicles involved in crashes incurred injuries requiring a hospitalaggregate analyses, drivers aged 75–84 were found toadmission, a proportion of 0.013338746. If W(z) is the standardimpose a small excess risk of injuries requiring hospi- normal distribution function evaluated at the point z, then
talization on other road users, and drivers aged 85 W(−2.2162046)=0.013338746. Thus, the coefficients of model 1in Table 6 were evaluated at the point −2.2162046; e.g., for theand over were found to impose a small excess risk ofcategory ‘‘other driver age 75–84’’ we have:death and hospitalization on other road users.
W(−2.2162046+0.042)−W(−2.2162046)=0.0148Individual-level analyses, however, failed to find evi-−0.0133=0.0015dence that any older-driver group imposed a non-
trivial level of excess risk on other road users. which is the value reported in the third line.
Acknowledgements—This research was conducted while the authorRE FERE NCE Swas an Epidemic Intelligence Service Fellow at the National Center
for Injury Prevention and Control, Centers for Disease ControlAmerican Association of Retired Persons (AARP) (1992)
Graduated Driver Licensing: Creating Mobility Choices.American Assocoation of Retired Persons, Washing-6Consider, for example, the possibility that older driverston, DC.engage in behaviors which make them more likely to be struck by
Evans, L. (1988) Older driver involvement in fatal andother vehicles, but not be held at fault in a crash. These behaviorssevere traffic crashes. Journal of Gerontology 43,result in age-related differences in the risk to other road users, and
therefore should be included in our assessment of risk. 186–193.

582 B. D
Evans, L. (1991) Traffic Safety and the Driver. Van Model Results. Center for Health Systems Research andAnalysis, Madison, WI.Nostrand Reinhold, New York, NY.
Gresset, J. and Meyer, F. (1994) Risk of automobile acci- Koepsell, T., Wolf, M., McCloskey, L., Buchener, D.,Louie, D., Wagner, E. and Thompson, R. (1994) Medi-dents among elderly drivers with impairments or chronic
diseases. Canadian Journal of Public Health 85, 282–285. cal conditions and motor vehicle collision injuries inolder adults. Journal of the American Geriatric SocietyGuppy, A. (1993) Subjective probability of accident and
apprehension in relation to self–other bias, age, and 42, 695–700.Leveille, S., Buchner, D., Koepsell, T., McCloskey, L.,reported behavior. Accident Analysis and Prevention
25, 375–382. Wolf, M. and Wagner, E. (1994) Psychoactive medic-ations and injurious motor vehicle collisions involvingHolland, C. (1993) Self-bias in older drivers’ judgements of
accident likelihood. Accident Analysis and Prevention older drivers. Epidemiology 5, 591–598.Ray, W., Fought, R. and Decker, M. (1992) Psychoactive25, 431–441.
Insurance Institute for Highway Safety (IIHS) (1992) drugs and the risk of injurious motor vehicle crashes inelderly drivers. American Journal of Epidemiology 136,Status Report Special Issue: Crashes, Fatal Crashes per
Mile. Insurance Institute for Highway Safety, Washing- 873–883.Stutts, J. and Martell, C. (1992) Older driver populationton, DC.
Karlson, T. and Quade, C. (1994) Head injuries associated and crash involvement trends. Accident Analysis and Pre-vention 24, 317–327.with motorcycle use—Wisconsin, 1991. MMWR 43,
423–431. Transportation Research Board (1994) TransportationResearch Circular No. 429: The Licensing of OlderKarlson, T., Quade, C., Wickeham, D., Sumi, M., Karon,
S. and Bigelow, W. (1994) Crash Outcome Data Drivers. Transportation Research Board, Washington,DC.Evaluation Systems (CODES) Mandated Research