nrha 2013 nursing home quality
TRANSCRIPT

Nurse Staffing and Quality
in Rural Nursing Homes
Peiyin Hung, MSPH, Michelle Casey, MS, Ira Moscovice, PhD
NRHA Annual Meeting | May 2013
Supported by the Office of Rural Health Policy, Health Resources and Services
Administration, PHS Grant No. U1CRH03717
Motivation for Study
• Rural and urban nursing homes are different
• Hospital-based and freestanding nursing
homes are different
• Previous studies have mixed conclusions
• Paucity of research with rural context

Study Objective
• What is the relationship between nurse
staffing levels and care quality in rural
nursing homes?

Methods: Data
• 2011 Nursing Home Compare Data
– Staffing and facility characteristics
– Quality indicators
• Minimum Dataset
– Resource Utilization Group Case Mix index for all residents
admitted to a facility
• 4,825 rural nursing homes in our sample
– 485 hospital-based (10%)
– 4,340 freestanding (90%)

Outcome Measures
• Individual quality indicators
• Composite quality indicators
• Health / Complaint inspections

Outcome Measures I
Individual Quality Indicators
Long-stay Short-stay
Pain Pain
Pressure Sores Pressure sores
Decline of Activities of Daily
Living (ADL)
Physical Restraints
Catheter
Mobility
Urinary Tract Infections
Outcome Measures II and III
Composite Quality
Scores
Average of long-stay measures
(reporting 3 or more measures)
Average of short-stay measures
(reporting any measure)
Health / Complaint
Inspections
Total deficiencies
Total actual harms
Total minimal or potentially-actual harms
Weighted total harms
Statistical Methods
• Multivariate, ordinary least-squares models
– Long-stay and short-stay quality measures
– Weighted total harms
• Negative binomial-regression models
– Health/complaint inspections
Methods: Explanatory Variables
Primary Nurse Staffing Levels
Nursing Home Structure
Secondary / Other Facility Operational Characteristics
Facility Structure Characteristics
State Fixed Effects

Limitations
• Cross-sectional study design limits the ability to
draw causal conclusions on relationships between
staffing and quality.
• Lack of individual resident-level data.
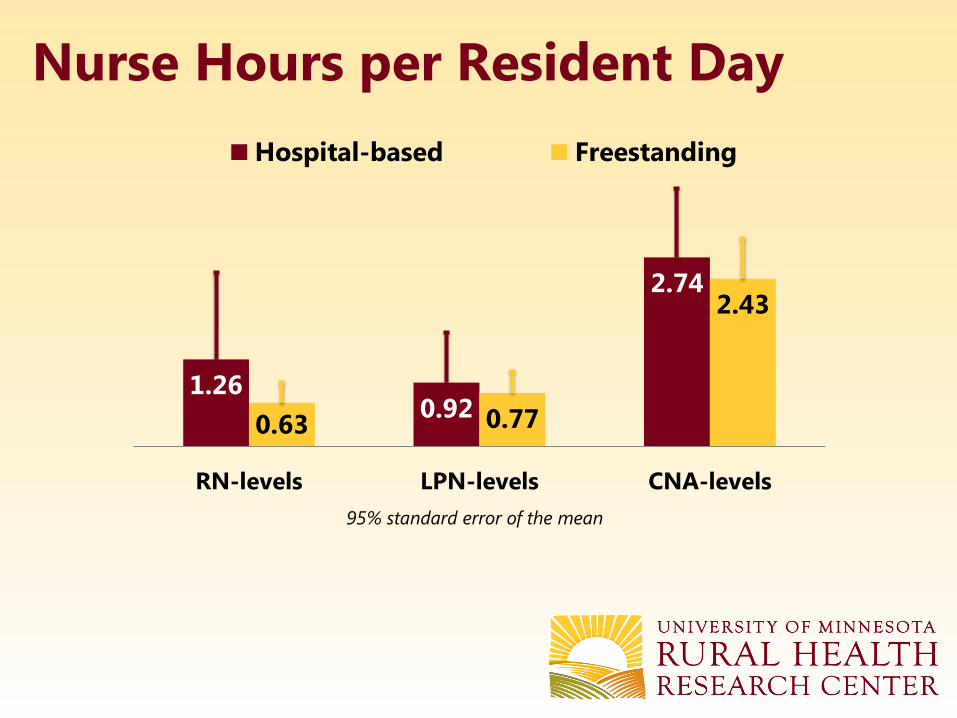
1.260.92
2.74
0.63 0.77
2.43
RN-levels LPN-levels CNA-levels
Hospital-based Freestanding
95% standard error of the mean
Nurse Hours per Resident Day

95% standard error of the mean
% of Long-Stay Residents with Outcome Measures
8.1
14.7
4.2
9.1
1.7
6.1
12.4
9.08.1
15.1
3.5
9.6
2.6
5.4
11.3
9.0
Long-stay
composite
scores
ADL
Decline
Pain Pressure
Sores
Physical
Restraints
Catheter Mobility
Decline
Urinary
Tract
Infection
Hospital-based Freestanding

24.1
2.0
21.5
27.2
2.1
24.5
Total deficiencies Total actual harms Total minimal harms or
potentially actual harms
Hospital-based Freestanding
95% standard error of the mean
Health / Complaint Inspections
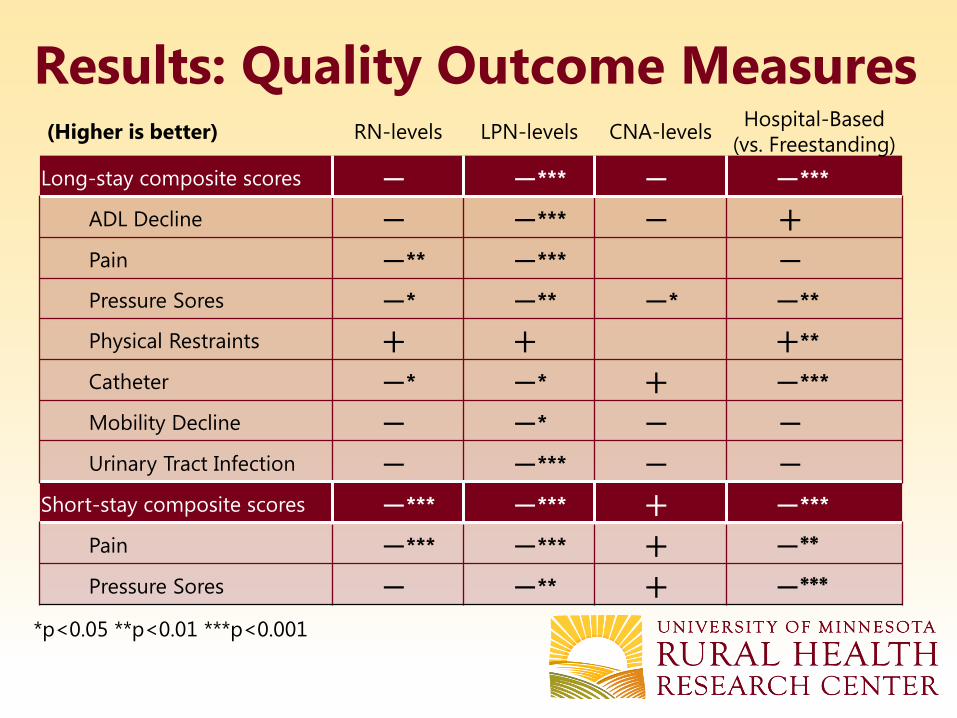
Results: Quality Outcome Measures(Higher is better) RN-levels LPN-levels CNA-levels
Hospital-Based
(vs. Freestanding)
Long-stay composite scores − −*** − −***
ADL Decline − −*** − +Pain −** −*** −Pressure Sores −* −** −* −**
Physical Restraints + + +**
Catheter −* −* + −***
Mobility Decline − −* − −Urinary Tract Infection − −*** − −
Short-stay composite scores −*** −*** + −***
Pain −*** −*** + −**
Pressure Sores − −** + −***
*p<0.05 **p<0.01 ***p<0.001
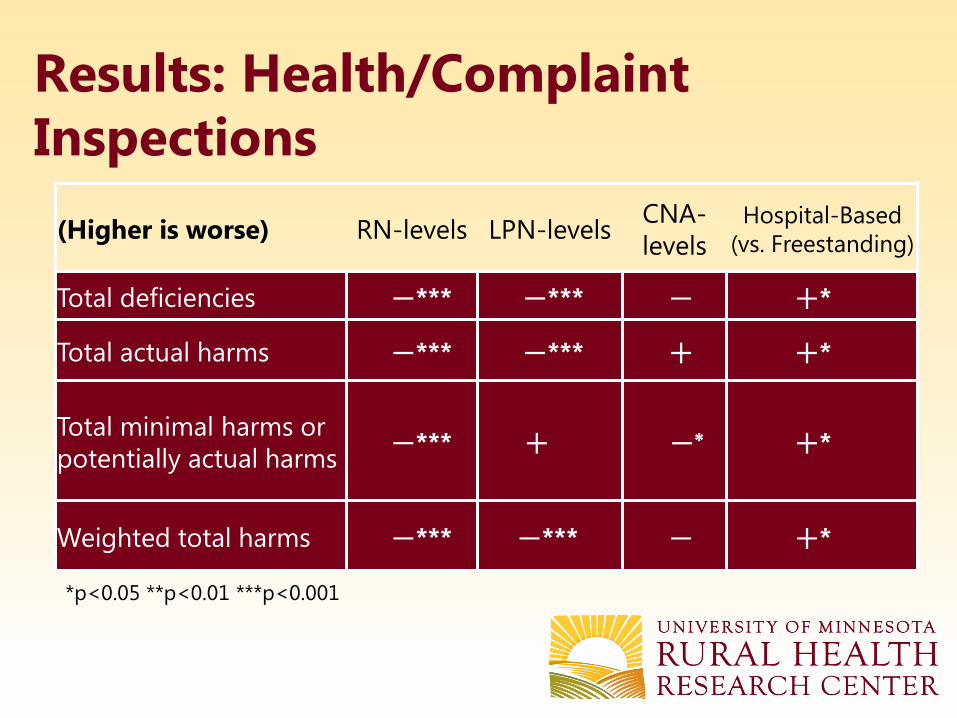
Results: Health/Complaint
Inspections
*p<0.05 **p<0.01 ***p<0.001
(Higher is worse) RN-levels LPN-levelsCNA-
levels
Hospital-Based
(vs. Freestanding)
Total deficiencies −*** −*** − +*
Total actual harms −*** −*** + +*
Total minimal harms or
potentially actual harms−*** + −* +*
Weighted total harms −*** −*** − +*

How Stratified Results Differ
• In hospital-based nursing homes:
– One unit RN-level is correlated with 3% less ADL
decline prevalence rate and 4.7 fewer
deficiencies.
– RN-levels show no associations with other
outcome measures.
How Stratified Results Differ
• In freestanding nursing homes:
– RN-levels and LPN-levels are correlated with
lower quality outcome scores.
– More CNA-levels are correlated with less
pressure sores.
– One unit increase of RN-levels is associated with
4 fewer deficiencies.
Summary
• Relationships between staffing and quality in
rural nursing homes vary by hospital-affiliation
and quality measures.
• Nurse staffing in rural nursing homes correlates
with lower quality in many measures.

Summary (cont.)
• Nurse staffing levels were associated with fewer
deficiencies in both rural hospital-based and
freestanding nursing homes.
• RN-staffing levels in rural hospital-based
facilities had stronger relationships with quality
than in freestanding facilities.

Peiyin Hung
612-623-8317
http://www.hsr.umn.edu/rhrc/