notes for contributors - lksnorth.nhs.uk · apply some creativity neil foley 9 salford and...
TRANSCRIPT
Items not submitted in time for thepublication deadline will be publishedin the following edition.
Guidelines for contributors are alsoavailable on the Lihnn website.
contributions shouldbe submitted to:Kathy Turtle, Librarian, Lancashire Teaching Hospitals NHS Trust,Postgraduate Education Centre,Chorley Hospital, Preston Road,Chorley PR7 1PP
Tel: 01257 245607Fax: 01257 245623Email: [email protected]
Lihnn is on the web via Aditus at www.aditus.nhs.uk.Click on Communities, then By Profession, to the Lihnn link.
notes for contributors1. Articles and news items are
welcome from all members of Lihnn,including support staff and staff inhigher education institutions.
Lihnn members are activelyencouraged to write up accountsof events and courses attended.Articles on new developments andprojects successfully managed arealso welcome.
2. News items and short pieces,which can range from factual toamusing, are also welcome.
3. All items can be submitted in printor electronic format.
please abide by the following points:Don’t forget your name, location, titleof article and date of article.
All acronyms should be written out infull for the first occasion they are usedin the text. Please give full details ofevents, courses and conferencesattended. This should include:
■ The name of event and location
■ Date of event
■ Name of organizing or sponsor-ing body
■ Details of how support materialscan be obtained (where necessary)
■ Full references to any publishedreports, articles, etc.
LIBRARY AND INFORMATION HEALTH NETWORK NORTHWESTNEWSLETTER
EDITORIAL BOARD
Kathy Turtle (Chair)Lancashire Teaching Hospitals NHS Trust
Rachel BuryUniversity Hospital Aintree
Suzanne KellyHealth Care Libraries Unit
Hannah GrayMersey Care NHS Trust
Kieran LambFade, Liverpool
12
Design & Print by Heaton Press Ltd Stockport Tel: 0161 442 1771
LIHNNK*13 spring'04 v2 9/6/04 2:40 pm Page 1
by Health Libraries, For Health Libraries ISSUE 13 SPRING 2004
IN THIS ISSUEBetter Information, Better Communication in Healthcare Alice Taylor 2
Health Minister John Hutton visits Salford PCT Library 3Jacqui Muskett
Writing for Publication: How to get started 3Melanie Hinde
Managing Knowledge for Health and Social Care ARCConference 26-28th April 2004Linda Riley & Mandy Beaunont 4
Opening of Child & Family Information Centre 4Sheelaugh Greenslade
Report on the Study Day at theKing’s Fund Library on QualityInformation for Social CareNorma Blackburn & Liz Stitt 6
Coffee and a chat?DL Net course on networkingDebra Thornton 7
NeLH Workshop for Primary Care Librarians Birmingham Rosalind McNally 8
You got a problem?... You gota problem?... Apply some creativityNeil Foley 9
Salford and Trafford’s graduate trainee James Allen 11
Now that all the editorial boardmembers have had an opportunity towrite the editorial, the task onceagain falls to me. It’s been good tobe able to share this task, and Ihope you’ve all appreciated thedifferent styles and approaches.Apologies are due to Hannah Graywho wrote the last editorial, butwhose name I forgot to include atthe end of the page.
I’ve probably said this to some of youbefore, but there are times in an editor’sworking life, when it all gets a bit biblical.What do I mean by this? Well, first thedesert, then the flood! After an editionhas been published I start to think aboutthe next one. There’s a time when I’m desperately hoping that material is goingto be written, and it can feel a bit likebeing in a desert. When contributionsstart to appear especially near to a dead-line, it seems like the great relief of aflood on parched land! I’m sure that any-one who has edited a newsletter knowshow it feels, and I am always eternallygrateful to contributors who submit earlyand respond to deadlines.
Well I’m pleased to say that this issue is averitable “fatted calf”! Alice Taylorwrites about a conference on informationfor patients and mentions an especiallyuseful talk by the Plain EnglishCampaign. Melanie Hinde takes upthe theme of writing, with good tips ongetting published, gleaned from a work-shop at Aston. For those of you interestedin patient information, SheelaughGreenslade describes the setting up ofan information unit at Alder Hey to provide
resources for patients, their families andcarers. Another style of communication,but just as important, is networking.Debra Thornton reports on a NeLHresidential on how to make best use ofgetting together with colleagues.
Just to confirm that our professional horizonsare always being widened, the issues ofknowledge management, and informationfor social care are the subjects of twoconference reports. Linda Riley andMandy Beaumont give accounts ofthe “Managing Knowledge for Healthand Social Care” conference held inLondon, and Norma Blackburn andLiz Stitt explain the issues concerningthe literature of social care and providingresources to social workers. I know thatsome of you, like myself, embarked onthe SCHARR Folio course on informationfor social care, and will find this articlevery interesting reading.
On familiar territory, Ros McNally,summarises a NeLH workshop on information in primary care.
For anyone who’s feeling jaded, and Iwon’t say if that includes me, turn to NeilFoley’s account of the residential courseon creative thinking and problem solving.Having been in the profession for moreyears than I’d care to admit to, it wasrefreshing to read about James Allen’syear as a graduate trainee with Salfordand Trafford. It’s heartening to know that enthusiastic recruits are enteringthe profession.
Kathy Turtle
B R O A D E N Y O U R H O R I Z O N S
LIHNNK*13 spring'04 v2 9/6/04 2:40 pm Page 2
On the 4th and 5th February 2004 Iattended a conference in Londoncalled ‘Better Information, BetterCommunication in Healthcare’. Theaim of the conference was to discussissues and share good practicearound delivering high quality information to patients, their familiesand the public.
Speakers included Claire Rayner (journalist,novelist, broadcaster and president of thePatients’ Association) who spoke about herexperiences both as a nurse and a patient,Bruce Hain (Head of Science at AldermanQuinney Secondary School) who talked aboutcommunicating health messages to children,and the lessons we can learn from teachers,and Rosie Winterton MP (Minister of State forHealth) who, rather than giving a presentation,used her allotted half hour to take questionsfrom the floor.
Bob Gann, the Director of NHS Direct Online,gave a presentation on the future of NHS DirectOnline. The website, www.nhsdirect.nhs.uk,includes an encyclopaedia, a self help guide,information on local NHS services and anonline enquiry service, and receives an averageof 500,000 hits a month. However, as noteveryone has access to the Internet or knowshow to use computers, some of the informationon NHS Direct Online is also available via NHSDirect Information Points. These informationpoints can be found in easily accessible publicplaces such as supermarkets, pharmacies andlibraries, and use a touch-screen system rather than a keyboard. So far there are 180 information points across the UK, with an average of 16,000 users a month, and theNHS Plan commits to having 500 informationpoints by the end of 2004. It is also plannedthat in the future, NHS Direct content willappear on existing high street kiosks.
Dr Geoff Royston, Head of OperationalResearch at the DoH gave a presentation onaccessing health information via digital TV. Justbefore Christmas the DoH agreed a £15m contract with the interactive TV company MMTVto launch NHS Direct Digital TV in summer 2004.The advantages of digital TV (DTV) are thatbesides being a fast and convenient mass
medium, it is also socially inclusive, for the percentage of people with access to DTV variesvery little across social classes. NHS Direct DTVis an information service, and will not bebroadcasting programmes, but it will have ‘redbutton’ hot links from popular TV shows – forexample, a person watching a TV programmefeaturing teenage pregnancy would be able topress the ‘red button’ on their remote control tolink through to information on pregnancy onNHS Direct DTV. The service will provide information on local NHS services, and willinclude an encyclopaedia, a self help guide,and healthy living advice. It will also includevideo clips. We were shown a sample videoclip in which patients who had undergonecataract surgery talked about their experiences,plus some footage of the cataract surgery takingplace. Subject to successful piloting, the scopeof NHS Direct DTV will be expanded in thefuture to offer services such as ordering repeatprescriptions.
I also attended a presentation by John Wildfrom the Plain English Campaign, an independentgroup fighting for public information to be written in plain English, as opposed to ‘gobbledygook’ or jargon. He gave severalexamples of confusing language, such as USSecretary of Defence Donald Rumsfeld’s mysterious comment that
as we know, there are known knowns; there arethings we know we know. We also know thereare known unknowns; that is to say we knowthere are some things we do not know. Butthere are also unknown unknowns - the oneswe don't know we don't know (Rumsfeld, 12February 2002, Department of Defence briefing).
Similar examples include the following newspaper headlines:
■ Record numbers of inmates killed themselves for the second year running last year
■ Nato rapid response unit to be ready by 2006
■ New study on obesity looks for larger test group.
The Plain English Campaign suggests avoidinglegalistic language such as ‘notwithstanding’,‘aforementioned’ and ‘herewith’, and Latinphrases such as ‘quid pro quo’ and ‘ad hoc’.They recommend using short sentences, activeverbs and simple language. For example, thePlain English Campaign translated the follow-ing sentence from:
‘if there are any points on which you requireexplanation or further particulars we shall beglad to furnish such additional details as maybe required by telephone’to‘if you have any questions, please ring’.
Plain English is not about ‘dumbing down’ language, abolishing jargon and new words,or curbing writers of literature. Plain English issimply information that conveys its messageclearly and concisely to its intended audience. Over the two days of the conference, we heardmany different presentations from a wide variety of speakers on delivering high qualitypatient information, but I felt the presentationfrom the Plain English Campaign offered themost practical and useful advice. We need toensure that patient information is suitable foreveryone, including those with a lower level ofliteracy, or those who do not speak English asa first language. Using plain English will ensurethat patient information can be understood byas many people as possible, thus empoweringpeople to make informed decisions about theirhealthcare.
Alice TaylorIntelligence OfficerPatient InformationManchester NHS Agency
2
Better Information, Better Communication in Healthcare
LIHNNK*13 spring'04 v2 9/6/04 2:40 pm Page 3
3
Health Minister John Hutton visits Salford PCT Library on 23 January 2004
I recently attended this half dayworkshop at Aston UniversityLibrary. The workshop aim was tohelp us make the first steps in get-ting an article published.
There were two speakers, Katy Jordan,Faculty Librarian, University of Bath andChristopher Cipkin, Music Librarian, ReadingUniversity. The following is a joint synopsis oftheir presentations.
Why don’t we writeThe main reasons or excuses given for notwriting are time and lack of subject. It is easyto give precedent to other priorities. Theremay also be the fear factor, thinking we areno good at writing or our opinions are toohumble.
Why should we write We are all working on similar areas of development and we need practical examplesof good practice. Writing for publicationenables us to share good practice, highlight
our library’s achievements and contributes toour personal development. No one else cantalk as authoritatively about what we do, noone else has our combination of skills andexperience, what we have to offer is a uniqueperspective.
How to get started – choosing your subject.Could be a project you have worked on, anopinion or idea you want to discuss, informationyou have gathered or reporting on a courseor conference. Think about what sort of articleyou are writing (long/short/practical/-analytical), who the audience will be, who willpublish it.
What makes a good article?A good article will be current, relevant, offersolutions, be practical, may be controversial,refers to previous literature and contains evidence to back up what it is saying.
Who will publish itChoose a publication you enjoy reading anddecide if you can write the sort of article they
publish, this will also give you an idea oflength, style, and approach. Editors alwayswant material and may even approach you.
Good writingGood writing is clear, easy to read, enjoyableto read, enthusiastic. Write using PlainEnglish, www.plainenglish.co.uk. PlainEnglish is clear, easy to read, with straightforwardvocabulary, straightforward grammar and adirect and open style. Try saying aloud whatyou want to say, as if you are explaining it tosomeone, ensure what you write is grammaticallycorrect, then leave it alone!
Final thoughtsGetting in to print is not as daunting or as difficult as you may think. Editors are hungryfor material, practical articles are well received.
Remember you can speak, therefore youcan write!
Melanie Hinde, LIS Project ManagerKnowledge Management and Information forthe Public, Manchester NHS Agency
Extract from Salford PCT's 'FrontLINE' magazine Issue 6 - Spring 2004
Health Minister John Huttongave PCT staff a huge pat onthe back after paying a flyingvisit to Salford in January.
Mr. Hutton spent six hours travelling fromLondon and back - just to take a few hours findingout about healthcare services in Salford after
being invited to open the library and e-learningsuite at St. James's House.
He spent time with staff - including district nurses,GPs and allied health professionals - at thelibrary before sitting down with children fromSalford primary schools, who told him aboutthe five a day fruit scheme.
As he cut the ribbon to officially open thelibrary facilities, Mr. Hutton said: "We have to
close the gap between the richest and the poorest in terms of health and what better placeto start than Salford. I can't give enough praiseto the staff here - you are leading the way forother PCTs to follow. You are doing a fantasticjob."
Submitted by Jacqui Muskett
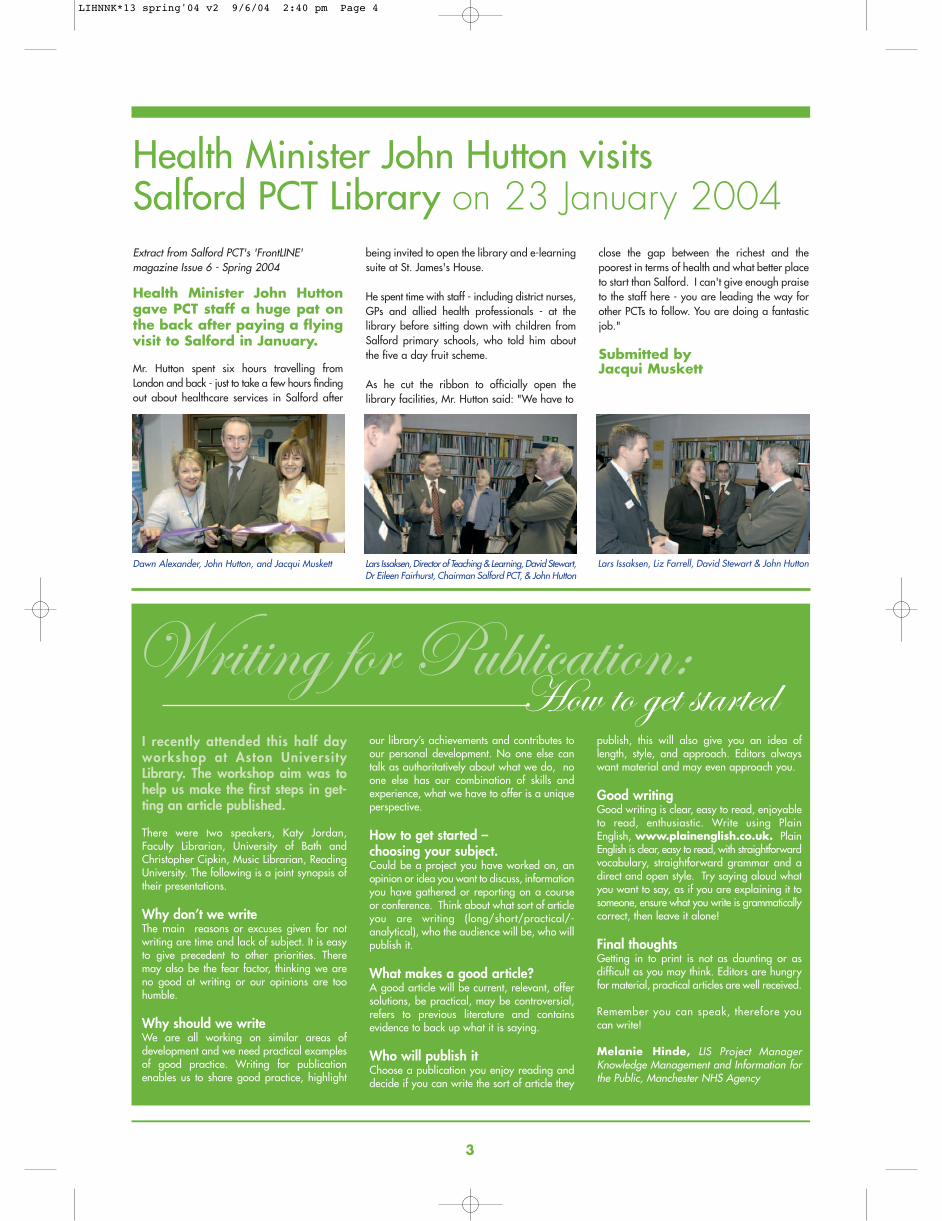
Dawn Alexander, John Hutton, and Jacqui Muskett Lars Issaksen, Director of Teaching & Learning, David Stewart,Dr Eileen Fairhurst, Chairman Salford PCT, & John Hutton
Lars Issaksen, Liz Farrell, David Stewart & John Hutton
LIHNNK*13 spring'04 v2 9/6/04 2:40 pm Page 4
OK here’s a poser for you. What doa stolen magazine, a lost party offrench school children and a taxi driver’s wife going into labour allhave in common? Answers on apostcard to Linda please!
I have just given you some seemingly randompieces of information, without the added ingredient of the tacit ‘knowledge’ that joins it allup, so presumably it’s meaningless to most of you.
Thus we have the difference between informationand knowledge, though closely related they arenot the same.
The first day of the conference was a broadoverview of the topic, useful for anyone whodidn’t know anything at all about knowledgemanagement (KM). The best speaker by farwas David Cavanagh from BP, who told us inthe most casual way that by instilling into theorganisation a knowledge management culturethey had saved the company $30 million onone oil well alone. Multiply that world-wideand the team had definitely justified their existence! The message from this talk was thatthe KM team were greatly valued because theydemonstrated the outcomes of their work interms of the money that was saved by theorganisation .Last year alone $500 million.
The second day contained the more authoritativespeakers who were also given longer slots, sothat they could go into their topics in moredepth. There were the usual suspects of BruceMadge, Veronica Fraser and Andrew Booth, allof whom always give good value for money. Inaddition I think Linda Wishart who spoke aboutimplementing the DOH’s knowledge managementstrategy and Joy Ellery’s Securing buy-in fromyour service users to senior management,deserve particular mentions. Their enthusiasmand love of the topic shone through.
We also attended the additional day three,which were two workshops. The first of whichwas ‘The Knowledge Management SWAP-SHOP’ where there was a lively exchange ofreflections and experiences. The second work-shop covered the topic of knowledge audits.This was less useful, as, though interesting, thework had been conducted more on the lines ofa ‘quick and dirty study’ than an authoritativepiece of research and best practice which couldbe emulated.
Altogether we spent an intense three days looking at knowledge management and cameaway ‘richer’ for the experience. My thanks toDavid Stewart and the unit who sponsored myplace allowing me to share this event with someof my other North West colleagues.
Oh, and just before I leave you, the answer tomy original poser was that they were all part ofmy (very interesting!) journey on the way downto London to attend the conference. I can’t tell
you, the no doubt happy, outcome for the taxidriver as I don’t have the knowledge of whereto contact him to ask…………
Linda RileyKnowledge & Libraries Manager for East Lancs Hospital Trust.
4
Managing Knowledge for Health
Opening of Child & Family
Information Centre
THE INSTALLATION OF THE UNIT
Patient information can empower patients, parentsand carers to have a genuine partnership intheir care. Improving access to quality informationwill strengthen partnerships between cliniciansand patients, their families and carers and alsounderpin the informed consent process.
On 29th January 2004, The Child & FamilyInformation Centre was launched at the RoyalLiverpool Children's NHS Trust. The centre wasofficially opened by a member of the Parentsand Carers Forum and by members of theChildren's Council. The centre is sited along
the main corridor of Alder Hey and is aimed atproviding a welcoming environment wherepatients, parents and carers can find informationon health and health related matters. There area range of resources and services that arefreely available to patients of the Trust and theirparents and carers including; access to theInternet, a database of 300 local support groupsand the services of information professional.
Funding for the collection and facilities camefrom a range of sources and the Trust is gratefulfor the support provided by Health Care
November 2003: The ground was prepared for the installation of the unit
At the end of November the Unit was dropped into place
Managing Knowledge for Health 26-28th A
KM
LIHNNK*13 spring'04 v2 9/6/04 2:40 pm Page 5
5
The three-day conference was veryenjoyable and provided me with anopportunity to network and discussideas around the first steps thatwould be required in developingand delivering the knowledge management agenda for my Trust.
The first day of seminars provided the opportunityto re-enforce my understanding of knowledgemanagement, with the second day building onmy existing knowledge and providing an environment which enabled me to begin generating ideas on how to this agenda forward.One of the main benefits of attending the conference has been that it has provided mewith a number of key messages that needed tobe considered if knowledge management is tobe implemented successfully and a definition ofknowledge management that appeals to me.
What is Knowledge Management?“The capabilities by which communities withinan organisation capture the knowledge that iscritical to them, constantly improve it, andmake it available in the most effective mannerto those people who need it, so that they canexploit it creatively to add value as a normalpart of their work”
(A guide to good practice in KM by BritishStandards Institute, 2001.)
The Four keys aspects of KM■ Creating the knowledge base■ Ensuring availability■ Giving people skills to use
knowledge effectively■ Developing a knowledge sharing culture
Barriers to Knowledge Management■ Organizational culture■ Lack of ownership■ Information and communications technology■ Non-standardised procedures■ Organizational structures■ Top management commitment■ Rewards and recognition■ Staff turnover
Success factors■ Highlighting the need that people in the
organisation People and their understandingof their business processes are critical.
■ Think big but plan and deliver small manageable pieces that contribute to andbuild on wider vision i.e. bit size.
■ Senior level customer buy-in and visible leadership is crucial.
■ Gather a team of talented and committedstaff sharing a common vision. It is important that the organisation does notsee the KM agenda as one person butdevelop a strategy that links in existingsteering groups within the organisation toprovide the framework to deliver the agenda.
■ Use the risk management agenda to getbuy in into projects and changes to working practice.
■ Emphasize that the benefits resulting fromthe implementation of KM will be greaterthan the effort needed to start this process.
■ Use Induction as a tool ton devolve KMthroughout the organisation with respect ofhow information is managed and disseminated within the Trust.
Steps to Implementing KM1. Conduct a knowledge audit - map the
organizations information resources2. Identifying tacit and explicit knowledge3. Names of people and their roles4. Documentation current systems
and procedures5. Reality check on what really happens, not
what is supposed to happen6. Identify problems and common complaints7. Identify key stakeholders8. The draft mission statement needs to be
clear about what you are trying to achieveand why (what is the vision, which are thesponsors, who will benefit?).
If anyone would like any further information,contact me on 01772 522763 or e-mail me at:[email protected]
Mandy BeaumontLibrary Services Manager, Lancashire Teaching Hospitals NHS Trust
h and Social Care ARC Conference
Library Unit. I was responsible for translatingthe Trust Patient Information Group vision ofan information centre into reality and I also man-age the centre as well as patient informationservices for the Trust.
Access to the centre was a high priority whenplanning the layout of and a number of issueswere identified for example the centre is singlelevel unit without steps or stairs, considerationwas given to the site of fixtures and fittings , ahearing loop system has been installed andthe P.C's are available on height adjustable
work stations. The resources and services willbe demand led and patients; parents and carersviews are actively encouraged to shape theservice delivery. Working with stakeholders(both in the Trust and the community) is a veryimportant aspect of the strategic developmentof the centre and relationships and partnershipsare being formed with a range of organisations.Helen Blackburn, Trust Librarian and I meetregularly to exploit opportunities to developcohesive and services to Trust staff.
The centre is open Monday to Friday 9.30
a.m. to 5.00 p.m.; there is an answerphoneand post box for out of hour’s enquiries. Thecentre also acts as a resource for educationalpurposes and also as a meeting place. In thefirst 2 months since opening, this multi purposefacility had been visited by almost 650 people,with enquiries ranging from condition andprocedure information to the location of thenearest cash machine. The AssistantInformation Officer, Andrew Willan and I arelooking for to developing and expanding theservices in the coming year.
Sheelaugh Greenslade
January 2004: Fixtures and Fittings were installed
End of January: Ready and waiting!
h and Social Care ARC Conference April 2004
LIHNNK*13 spring'04 v2 9/6/04 2:40 pm Page 6
6
Report on the Study Day at the King’s Fund Library on Quality Information for Social CareOn the 23rd February 2004,the King’s Fund Library hosteda study day on “QualityInformation for Social Care”.The aims of the day were toprovide an overview of socialcare policy, give an insight intoissues affecting the quality ofsocial care information andhighlight resources availablein social care information.
The day lived up to all our expectationsand met the aims it set out to meet.Finding resources available foraccessing information in socialcare is something that as theboundaries between health andsocial care provision begins to bluris of interest to us all.
The study day was of particularinterest to the authors who, fromApril 2003 to March 2004, workedon a Lancashire-wide clinicalenquiry service project in mentalhealth and learning disability. Theproject findings illustrated the closeinteraction between health andsocial care professionals in thesedisciplines, and the need to provideboth groups with information relevantto their common field and to theirspecific professions. Speakers anddelegates at the study day high-lighted the barriers to accessinginformation, namely lack of ITequipment, lack of basic IT andinformation retrieval skills, and thesparsity of social care resources.This was confirmed locally by thefindings from the Lancashire project.
Information Systems to be interoperable
Roger Lund from the NationalKnowledge Service highlighted thelack of coordination of knowledgeand the need to pull knowledgesources together nationally as theDepartment of Health is now lookingat health and social care as awhole. By doing so the access anddelivery systems used to provideinformation would be improved.Roger discussed the concept ofcommon knowledge cores providingone set of information but presentedin different ways to different recipients.The elements of the NationalKnowledge Service would have theaim of information systems beinginteroperable.
Roger summarised what progress hadbeen made in the last financial year:
In terms of technology, interoperabilitystandards had been developedwith the National Knowledge infrastructure. Athens access management was now standard forall staff across the NHS. NHSDirect Online, nhs.uk, and theModerisation Agency were nowco-hosted by one provider.
In terms of content, 5 NSF specialistlibraries and 3 new knowledgeservices (depression, public healthand ante-natal screening) hadbeen deve loped. The DrugInformation Zone for the MedicinesInformation Service had been fundedin an attempt to mobilise knowledge
He set out what could be achievedin the forthcoming year: namely toinvestigate the feasibility of integrating NeLH and eLSC, and tofacilitate searching across both systems.
It was acknowledged that a singletaxonomy system for social carewould need to be developed.
AgeInfo freely accessible
Diane Gwynne-Smith from theSocial Care Institute for Excellence(SCIE) focused on the developmentof the electronic Library for SocialCare (eLSC).
The electronic Library for SocialCare is going forward in separatephases:
Phase 1 is a review of the infrastructure,looking at making the resourcemore user friendly, particularly inview of its wide client group i.e.researchers, practitioners and serviceusers. Diane agreed with Roger ofthe need to make the body ofknowledge accessible with a commontaxonomy using a topic approach.
Phase 2 would look at establishinga definitive gateway to social careby identifying other contentproviders and commissioning newcontent. She proposed a widerpartnership working, with thoseNeLH specialist libraries whichhave a social care element.
SCIE are to make AgeInfo freely
accessible in the near future, and itis planned to integrate this withCareData.
Diane reiterated the need for Internetand Research skills to be developedand as a consequence of these skillsgaps, a skills building area wouldbe provided on their website.
SCIE will be funded by theDepartment of Health for a furtherthree years.
Use ChildData not just ERIC and PsycInfo
Alan Gomersal from the Centre forEvidence Based Policy and Practicespoke on finding the evidence inthe social sciences. Alan spoke of the information contained on the organisation’s website –www.evidencenetwork.org
Alan described its contents, whichincluded 44 – 45 databases andgateways to information. He urgeddelegates to use a variety of data-bases when searching social careliterature, not just ERIC andPsycInfo. He listed the Web ofKnowledge, and Sociological andPsychological Abstracts as Researchdatabases. He reminded people ofthe relevance of Practice databasessuch as CareData, Planex, Accompliceand CommunityWise. He listedResearch and Practice databasessuch as AgeInfo, ChildData, Sigle,Assia, Criminal Justice Abstractsand Inside Web. Unfortunately, theBritish Library have now pulled outof Sigle (Selective Information ofGrey Literature in Europe).
The website also has an Associateslist of 500 members. He invitedlibrarians to join. As one of the roles of the Centre isto provide training seminars andworkshops, Alan described theattributes of the various databases& literature searching in some detail.
He compared systematic reviewswith narrative reviews, and althoughhe admitted that systematic reviewswere seen as the ‘gold standard’, inhis experience he felt they were notread by practitioners. He felt thatnarrative reviews were more accessible, quicker to produce, andmore relevant to the practitioner, +
although not always accepted bymany academics. This comparisonprompted some challenges from thedelegates!
He concluded by stating that hisaim would be to encourage databasesuppliers to merge their content, tofacilitate improved coverage whensearching the social care literature.
Be Evidence Based in Social Care
Following Alan was Alice Moselyfrom the Centre for EvidenceBased Social Services whospoke on increasingaccess to social careresearch.
Alice listed whatshe felt were pract i t ionerf r i e n d l ysocial carew e b s i t e sand thesewere www.whatworksfo rch i ld ren.org.uk plustwo researchsites, Research i n P r a c t i c ew w w. r i p . o r g . u k& Research Mindednesswww.resmind.swap.as.uk.She also included the occupationaltherapy trials site www.otseeker.com.
She i l lus trated their own “BeEv i d e n c e B a s e d ” s i t e a twww.Be-Evidence-Based.com asthis presented original pieces ofprimary research. The site haspractice relevant topics andincludes training tutorials in theskills section.
The Centre’s main functions are todisseminate activities and to trainstaff in locating and appraisingresearch, so that staff understandthe material they retrieve. A numberof reports, all of which are down-loadable, are made available onthe site. The reports include twolarge scale studies on access to ITprovision for social care staff.
Alice felt that access to Athens wasessential for social care staff.Athens is currently available tosocial care staff in Scotland.
LIHNNK*13 spring'04 v2 9/6/04 2:41 pm Page 7
7
10 Social Care “Briefings”
Following lunch and a chance tohave a guided tour of the King’sFund library, Andrew Booth andHelen Bouchier from Scharr spokeon meeting the information andtraining needs of the social careworkforce.
Andrew described three initiativesfrom Scharr which sought toachieve this.
The Social Care InformationOutreach Project set out to identifythe information skills training neededfor social care practitioners acrossTrent. Results demonstrated thatbudgets and politics dictated servicesprovided rather than research evidence. Social care was perceivedas a difficult area to apply research,given the practical nature of thework. Less than 20% of the sample
surveyed took a literature –based approach to evidence
based practice.
The SCISTER project(Soc ia l CareI n f o r m a t i o nSkills & Trainingin ElectronicR e s o u r c e )developed athree prongedapproach toe v i d e n c ebased practice
courses. Threecourses offered
training: for socialcare practitioners; for
NHS librarians; and aweb-based course for
NHS librarians. The projectfindings identified both the need toprovide information for practitioners,and information for management.
The third initiative was to provideoutputs in the form of a series ofsocial care ‘Briefings’, funded bySCIE. Ten ‘briefings’ have so farbeen produced. Briefings are compiled by an equal ratio of academics and practitioners,acknowledged as ‘experts’ in thefield, and these briefings are fundedto continue for a further 12 months.
Workshops
The second part of the afternoonconsisted of 2 workshops, Findingthe Ev idence led by AlanGomersal, and Appraising theEvidence led by Alice Mossley andAnnie Ellis.
Whilst Finding the Evidence builton the excellent presentation given
by Alan Gomersal it was weightedmore heavily on the poor resourcesand would perhaps have beenmore bene f i c ia l i f i t had concentrated on quality resources.
Although Appraising the Evidencewas described as a workshop session, it was in practice, a furtherpresentation, with little time for delegate participation. It was aver y succ inc t summar y o f qualitative versus quantitativeresearch methods, using scenariosin social care. This was followedby highlighting the points to notewhen deciding which papers torequest from a literature search i.e.relevance; quality of the abstract;appropriateness of the researchdesign; and the trustworthiness ofthe research. Each of these pointswere explored further. Followingthis critical appraisal component,the remainder of the presentationcovered a variety of researchissues such as a reminder of thehierarchy of evidence, and bias.
A developing knowledgebase in Social Care
Overall, the message of the daywas that information provision andretrieval in the social care field isseveral steps behind the healthinformation field in producing,finding and using information toinform practice. Social carepractitioners are hampered by alack of IT infrastructure and both alack of basic IT and informationretrieval skills.
However, what was heartening tolearn from this study day was thatquality information in social care isbeing produced and is becomingmore widely available. Issues suchas a common taxonomy, a commonknowledge core, and the provisionof information skills training are allbe ing addressed and th i s i s something which we, as librarians,will benefit from.
Presentations from this study day are available on theInformation for the Management o f Hea l t h ca r e web s i t e a twww.ifmh.org.uk/studydays.html
Liz StittLibrary Services Manager,Calderstones NHS Trust
Norma Blackburn Library Services Manager,Blackpool, Fylde & WyreHospitals NHS Trust
Many of us know that networkingis an important part of our joband sometimes feel that we aresales people rather than librarians.Day one of the NeLH’s recentDLnet residential (3-4 March2004) helped us put that conceptinto perspective and gave ushints and tips on how to ‘do’ net-working effectively, based on ourown personal styles.Mick Cope gave us an insight into how to build and sustainprofessional relationshipswhich will benefit uspersonally, professionallyand as a service. Thefollowing is a summaryof the day with extractsfrom his book, ‘PersonalNetworking.’1
Managing investmentswisely to optimize return.
‘Social capital’ is all aboutdeveloping mutually beneficialprofessional relationships to promote co-operation. Some tips in building social capital:
■ Ensure that you get the bestfrom the relationship
■ Don’t create connections withnegative people
■ Recognise that some relation-ships will need time to grow
■ Identify those people whohave a clear sense of purposeand try to connect with them
‘If you want to grow social capitalthat has value and will achieve
success you cannotkeep drinking coffeewith people for fun.’
This all sounds a bitmerciless but there aresome valuable tipsthat can help us all in our professionallives to build usefulre la t ionsh ips wi th colleagues.
Mick identified four social stylesand we were invited to find outwhich one was our own. Knowingyour own personal style andlearning how to interpret the personal style of others in yournetwork gives you a useful strategyfor dealing with new situations,making decisions or resolvingconflicts.
Of course, you’re not going towalk into a room and find thatpeople are wearing large colour-coded badges stating that theyare a ‘star’ or a ‘rock’ (as wedid), but it does help to knowwhat characteristics to look for inpeople – and how to get the bestout of the situation by using thisknowledge. Try it next time you
want to ask for a favour – or apay rise (and let me know if itworks!)
Debra Thornton
REFERENCES1 Mick Cope (2003), Personal Networking,Edinburgh: Pearson Education
Coffee and a chat?
PERSONAL CHARACTERISTICS WHAT TO DO IF STYLE YOU MEET ONE
ROCK
STAR
SAGE
JUDGE
Pleasant, steadfast, strongpersonal values, willingnessto help others. Slow toadapt to change, may be perceived as stubborn.
Optimistic, friendly, possibly extrovert, good atselling their ideas. May beinconsistent, lacking inobjectivity, disorganised.
Value their enthusiasm, givethem lots of information,“accept that what they saydoesn’t make sense – butunderstand that it is theright thing for them.”
Precise, conscientious, ability to appraise thingsand draw strong conclusions,objective. Can be seen ascold or aloof, may not trustthe views of others, may beslow to accept change.
Very effective at gettingthings done. Can be verypersuasive through the useof logical energy, solid factsand powerful argument.
Be precise in your principles and objectives.Explain your decision andthe rationale behind it. Beaware they may talk firstand think later.
Be factual and objective,give them time to expresstheir views, let themappraise the situation andcome to a decision basedon the facts.
Be flexible, respect theirvalues, give them theopportunity to talk abouttheir views. Show interestby asking questions.
LIHNNK*13 spring'04 v2 9/6/04 2:41 pm Page 8
8
National Electronic Library for Health (NELH)Workshop for Primary Care Librarians
22nd-23rd January 2004, Birmingham
This workshop brought togetherlibrarians with a remit to provideservices for primary care staff togetherwith those interested in improvingservices to primary care.
It was organised and led by staff from theNELH. They have identified primary carelibrarians as key change agents in promotinguptake and use of NELH. The purpose of theworkshop was to developunderstanding and apprecia-tion of what NELH needs fromlibrarians, what primary carelibrarians need from NELHand what NELH can do torespond.
The workshop began with SueLacey-Bryant presenting thefindings of a survey of primarycare librarians which waspart of the NELH OutreachL ibrar ian Suppor t andDevelopment Project. Thisrevealed a current picture of fragmented and diverse jobroles and models of servicedelivery together with profes-sional isolation experiencedby some librarians working inor for primary care. There are also several barriers todeveloping the teaching/-training role of librarians inprimary care:
■ Lack of recurrently funded posts to providestability for developing teaching programmes
■ Poor connectivity of PCs to the internet inprimary care settings
■ Low priority/lack of time given to IT andinformation skills among primary care staff
However, there is a great deal of commitmentand enthusiasm among participants and primary care librarians towards overcomingthese barriers.
This presentation provided the basis for smallgroup discussions of what participants felt werethe key barriers to the successful implementationof innovative developments like NELH and therole of outreach librarians. Currently the structure of outreach librarian posts, whetherbased in PCT, Secondary Care Trust or WDCare around short-term contracts. It is unlikely
that the role will be effective in the long termwithout more recurrent funding for posts to provide an effective organisational structure.
Particular problems with promoting NELH wereconnectivity in general practices and the needto improve the search engine. Work to rectifythis is on-going. Muir Grey outlined the widerplans for integrating NELH with NKS (NationalKnowledge Service) to offer improved decisionsupport for patients and staff. Decision support
systems integrate evidence with clinical conditions within the consultation. The aim isfor all “knowledge products” to conform tocommon standards of quality and documentmanagement. NELH will be transformed intoNLH (National Library for Health) in the nearfuture to integrate with National Core Content,Electronic Library for Social Care and theNational Knowledge Service.
The workshop included several informative presentations from practicing outreach librariansdescribing their experiences of setting up anddelivering services to primary care staff. Thekey messages from this were:
■ the importance of having strong professionalnetworks and back-up from a library andinformation service (LIS), either PCT, Trust orUniversity based
■ the need for people in this role to have a wide range of skills both professional and managerial, including the ability to influence others
The second day involved a review of currentNELH marketing activity together with a sessionworking through a variety of scenarios ingroups around overcoming barriers in primarycare. Important themes which emerged werethe need to identify all primary care staff, not
just GPs (health servicemanagers, health visitors,practice nurses, community-based PAMS, practicemanagers) and to investtime getting to know theirneeds and ways of working.Find “champions” whohave influence over thoseyou wish to influenceeither by virtue of theirauthority or charisma andtarget them.
The workshop was verywe l l d e l i v e r ed and stimulated a great deal ofnetworking. For thosewho wou ld l i ke morein fo rma t i on a l l t h ep r e s e n t a t i o n s a n d information on how to ne twork f u r t h e r a r e available at:
www.nelh.nhs.uk/dlnet/primarycare/default.asp
The development and expansion of LIS inprimary care is overdue as primary care haslong been the poor relation in the NHS in termsof access to high quality support services.However, the success of NELH and other electronic services reflective of the re-modellingof LIS on the basis of electronic access ultimatelydepends on building relationships and continuityof access with support from skilled professionalswho can provide back-up in the shape of specialist subject knowledge, training, adviceand support to facilitate and enable the embedding of NELH.
Rosalind McNally
LIHNNK*13 spring'04 v2 9/6/04 2:41 pm Page 9
9
You got a problem?... You got a problem?...
Apply some creativityApply some creativityOn the 2nd and 3rd March, theLIHNN/HCLU Residential event tookplace at The Ramada Hotel,Blackrod, Bolton. Blackrod, not to beconfused with Blackrod, the func-tionary of the Palace of Westminster.Hardly compatible, illogical even,you might say – town and a person– but therein are the opportunitiesfor exercising creativity. Neil Foleywrites about the proceedings of thisyear’s course, Problem-solving andCreative Thinking.
This two-day residential, led by DeborahDalley, sought to convey the message that creativity can be applied to problem-solving. Atevery turn there are opportunities to solveproblems - and thereby contribute to the economy, health economy or otherwise - identifyusers’ information needs; setting up new information services; developing marketingstrategies; designing document templates;reviewing policies and procedures; or devisingtraining workshops. The list could go on, as I’msure you appreciate.
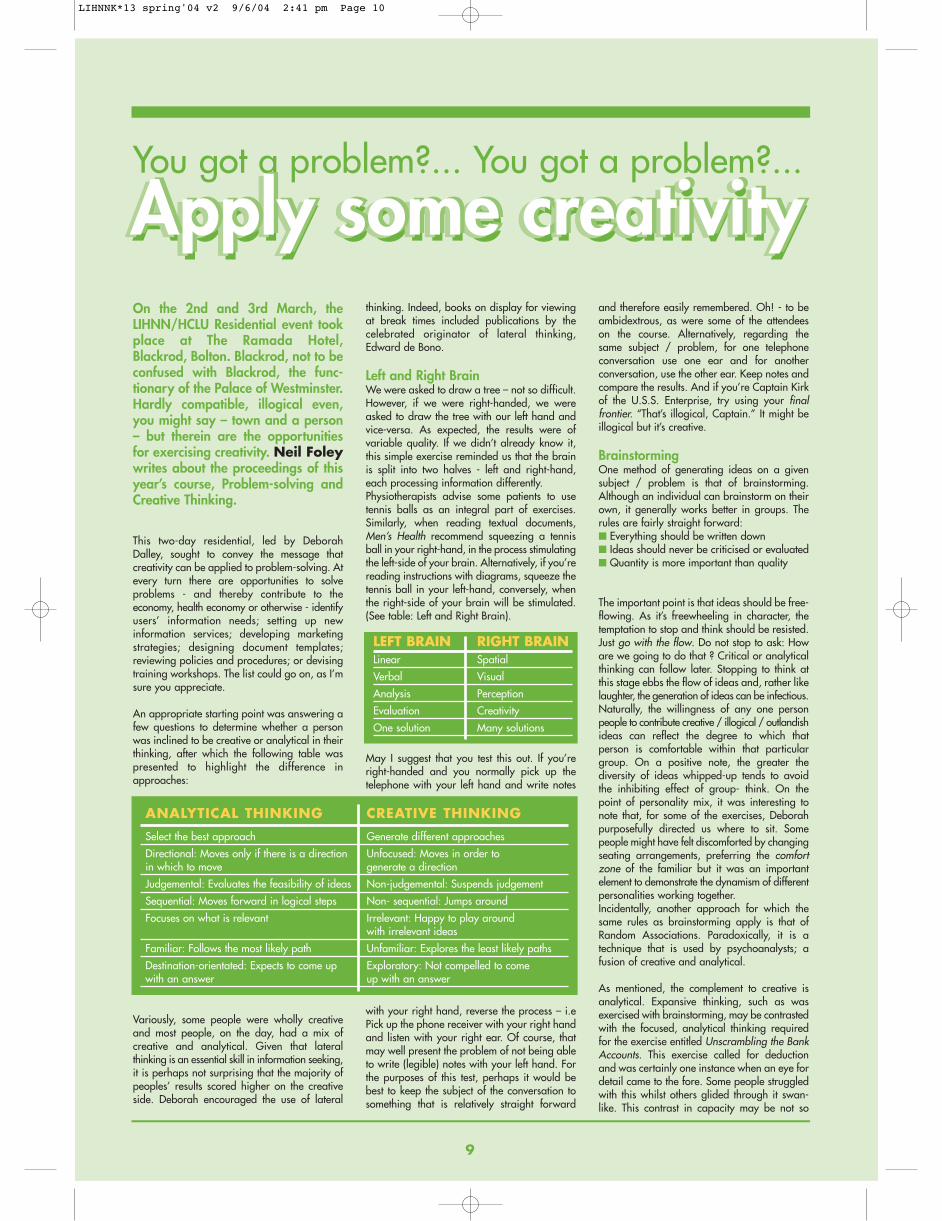
An appropriate starting point was answering afew questions to determine whether a personwas inclined to be creative or analytical in theirthinking, after which the following table waspresented to highlight the difference inapproaches:
Variously, some people were wholly creativeand most people, on the day, had a mix of creative and analytical. Given that lateral thinking is an essential skill in information seeking,it is perhaps not surprising that the majority ofpeoples’ results scored higher on the creativeside. Deborah encouraged the use of lateral
thinking. Indeed, books on display for viewingat break times included publications by the celebrated originator of lateral thinking,Edward de Bono.
Left and Right BrainWe were asked to draw a tree – not so difficult.However, if we were right-handed, we wereasked to draw the tree with our left hand andvice-versa. As expected, the results were ofvariable quality. If we didn’t already know it,this simple exercise reminded us that the brainis split into two halves - left and right-hand,each processing information differently.Physiotherapists advise some patients to usetennis balls as an integral part of exercises.Similarly, when reading textual documents,Men’s Health recommend squeezing a tennisball in your right-hand, in the process stimulatingthe left-side of your brain. Alternatively, if you’rereading instructions with diagrams, squeeze thetennis ball in your left-hand, conversely, whenthe right-side of your brain will be stimulated.(See table: Left and Right Brain).
LEFT BRAIN RIGHT BRAINLinear Spatial
Verbal Visual
Analysis Perception
Evaluation Creativity
One solution Many solutions
May I suggest that you test this out. If you’reright-handed and you normally pick up thetelephone with your left hand and write notes
with your right hand, reverse the process – i.ePick up the phone receiver with your right handand listen with your right ear. Of course, thatmay well present the problem of not being ableto write (legible) notes with your left hand. Forthe purposes of this test, perhaps it would bebest to keep the subject of the conversation tosomething that is relatively straight forward
and therefore easily remembered. Oh! - to beambidextrous, as were some of the attendeeson the course. Alternatively, regarding thesame subject / problem, for one telephone conversation use one ear and for another conversation, use the other ear. Keep notes andcompare the results. And if you’re Captain Kirkof the U.S.S. Enterprise, try using your finalfrontier. “That’s illogical, Captain.” It might beillogical but it’s creative.
Brainstorming One method of generating ideas on a givensubject / problem is that of brainstorming.Although an individual can brainstorm on theirown, it generally works better in groups. Therules are fairly straight forward:■ Everything should be written down■ Ideas should never be criticised or evaluated■ Quantity is more important than quality
The important point is that ideas should be free-flowing. As it’s freewheeling in character, thetemptation to stop and think should be resisted.Just go with the flow. Do not stop to ask: Howare we going to do that ? Critical or analyticalthinking can follow later. Stopping to think atthis stage ebbs the flow of ideas and, rather likelaughter, the generation of ideas can be infectious.Naturally, the willingness of any one personpeople to contribute creative / illogical / outlandishideas can reflect the degree to which that person is comfortable within that particulargroup. On a positive note, the greater thediversity of ideas whipped-up tends to avoidthe inhibiting effect of group- think. On thepoint of personality mix, it was interesting tonote that, for some of the exercises, Deborahpurposefully directed us where to sit. Somepeople might have felt discomforted by changingseating arrangements, preferring the comfortzone of the familiar but it was an important element to demonstrate the dynamism of differentpersonalities working together.Incidentally, another approach for which thesame rules as brainstorming apply is that ofRandom Associations. Paradoxically, it is atechnique that is used by psychoanalysts; afusion of creative and analytical.
As mentioned, the complement to creative isanalytical. Expansive thinking, such as wasexercised with brainstorming, may be contrastedwith the focused, analytical thinking requiredfor the exercise entitled Unscrambling the BankAccounts. This exercise called for deductionand was certainly one instance when an eye fordetail came to the fore. Some people struggledwith this whilst others glided through it swan-like. This contrast in capacity may be not so
ANALYTICAL THINKING CREATIVE THINKING
Select the best approach Generate different approaches
Directional: Moves only if there is a direction Unfocused: Moves in order to in which to move generate a direction
Judgemental: Evaluates the feasibility of ideas Non-judgemental: Suspends judgement
Sequential: Moves forward in logical steps Non- sequential: Jumps around
Focuses on what is relevant Irrelevant: Happy to play around with irrelevant ideas
Familiar: Follows the most likely path Unfamiliar: Explores the least likely paths
Destination-orientated: Expects to come up Exploratory: Not compelled to come with an answer up with an answer
Apply some creativityApply some creativity
LIHNNK*13 spring'04 v2 9/6/04 2:41 pm Page 10
much a reflection of intelligence, rather, it perhapshighlights differences in preferred learningstyles. Those wishing to develop their analyticalthinking skills were encouraged to seek outlogic puzzle books.
Sensory StimulationCreativity may be stimulated by heighteningALL FIVE senses – hearing, sight, touch, tasteand smell. For example, eat food you’ve nevereaten before, visit a country you’ve never visitedbefore, change your perfume / aftershave,wear clothes of different cloth, decorate yourhome in a radically different colour scheme,strike up a conversation with a stranger or reada newspaper you’ve never read, join an organisation as a volunteer, try a different TV/radio station or learn to play a musical instrument.There’s a whole world out there! One step couldbe the beginning of a progressive series ofsteps. As they say, The journey of a thousandmiles begins with the first step. Incidentally,journeying and finding new physical routesdevelops new neural pathways in the brain,avoiding auto-pilot mode.
On the specific point of sight, Deborah dreweverybody’s attention to pithy words promotedby the Department of Trade & Industry: Look where everyone else is lookingSee what no one else is seeingDo what no one else is doing
Regarding hearing, some people stimulate creativity by having music playing in the back-ground whilst thinking. But that doesn’t suiteverybody.
Problem ChecklistNotwithstanding the benefits of venturingbeyond the comfort zone, at other points duringthe two days, relative stability within establishedgroups supported the development of a rapport,facilitating the discussion of a personal problemarea. In this context, each group was asked toaddress a problem presented by one memberof the group, applying the structure providedby the Problem Checklist. (See ProblemChecklist).
Problem Diagnosis One method discussed relating to problemdiagnosis was that of Force Field Analysis(FFA). In terms of attempting to affect a change,Deborah explained FFA in terms of two sets offorces – those which drive the change andthose which restrain it. The stronger of the twowill determine the outcome.Essentially, in applying FFA, there a few stages:■ Decide upon the situation that you wish to
change and describe the current situation.
■ Looking to the future, describe how the futureappears to you and how you would like it tobe. In other words, apply visualisation.
■ Having performed the descriptive element,you then have to identify the separate driv-ing forces which will encourage and thosewhich will restrain the change.
■ Systematically, assess the character of eachof the forces, taking into account their rela-tive strength / weakness. Do you have anycontrol over any of the factors? Alternatively,are you able to influence any of the factors?
Reviewing the picture to date, in transit betweenthe current situation and your visualised condition,you will now need either to add more drivingforces / remove restraining forces, or possiblyperform both. The stronger likelihood of success,apparently, comes with focusing attention onthe restraining factors. Therefore, developaction plans to remove those factors. Implementthe action plans and evaluate.
In terms of evaluation, Deborah suggested thefollowing method:
■ Listing possible solutions
■ Ranking solutions according to importance –(i.e. numbered scale: 5= Extremely important,4 = very important and so on). If working ina group, total up the number of points allocated per person to each idea. Theidea(s) with the highest score should be considered worthy of implementation.
ConclusionAlthough this two-day residential, entitledProblem-solving and Creative Thinking, wastargeted at Assistant / Deputy Librarians, most,if not all, of the content could be applied by anymember of the library staff – and should be.Indeed, the methods could be applied to anysituations which present problems, whether inyour library, in your personal life – or wherev-er. In a recent edition of Men’s Health it wasreported that a survey of more than 1000 man-agers had found that innovation and creativi-ty… the most important qualities for survivingin the working world.
To lift an innovative thought from the level of acreative idea into a practical reality, subjectingthe idea to critical analysis, is generally a goodidea. For optimum performance therefore, notleast in terms of time, hybridity is the key word.Being able to switch from analytical to creativemode as different types of problems presentthemselves is the ideal situation. Deborah saidthat it is “…a matter of recognising the differences (between creative thinking and analytical thinking) in order to be able to useboth effectively.” As Meryl Streep once said inan interview with Barry Norman, One musthave bread and one must have wine.
If a person experiences a relative imbalancebetween the two approaches – creative andanalytical – Deborah suggested that effortshould be concentrated on applying appropriatemethods to raise the performance of the weakerof the two, with a view to achieving the twoworking in concert. Perhaps the same could be said in developingbeyond one’s preferred learning styles.
Certainly, variety is the spice of life.Purposefullyexposing oneself to new experiences increasesthe likelihood of being to relate to a broaderrange of people, from all walks of life.Essentially, preparation for enhanced networking – particularly applicable if you findyourself in a rut. Anyone for tennis?......Remember that you are limited only by yourimagination and that creative thoughts don’thave to be logical. My apologies to any aficionados of Star Trek.
Labelling Creative as C and Analytical as A, tomaximise thinking, ideally, it is not so much Cor A but rather C and A - or maybe even C&A– which reminds me, I need to do some clothesshopping. Yet another example of creative /lateral / illogical connections.
The event was facilitated by Training Consultant, Deborah Dalley.Tel: 01706 826054 Mobile: 07949 497730E-mail: [email protected]
ReferencesMen’s Health. Have your best year ever, Jan2004, pp.82-87.
10
PROBLEM CHECKLISTSelect one member of your team to own theproblem and then use the following checklistto better understand their problem.
1. DEFINE THE PROBLEMWrite a one sentence headline defining the problem.
2. BACKGROUNDDescribe:■ What the present situation is■ How the problem has occurred
3. WHY IS THERE A PROBLEMDescribe:■ Why it is a problem to you■ Why it should be solved
4. HISTORYExplain:What has been tried to solve the problem in the past
Why did this not work
What else has been thought of
Why it has not been tried
Why it would not work
Who else is in a similar situation
What have they done to address the problem
LIHNNK*13 spring'04 v2 9/6/04 2:41 pm Page 11

As Salford and Trafford’s graduatetrainee librarian, I have had a fascinatingyear so far. I started in this role lastSeptember with only brief libraryexperience at the Manchester Schoolof Physiotherapy, which along withmy background as a geographerand historian, had whet my appetitefor more work in the field oflibraries, archives and information.
Without really knowing what to expect, I jumped at the chance of this graduate traineerole: a job I wanted to do, with prospects forfurther study and career development, andwithout hours of commuting everyday. So farI’ve worked in three of the five library andinformation services I’m covering in the year,but already I have seen, learnt and experienceda huge range of work – far more, I expect, thanI could have in a university or public library,even as a graduate trainee. In addition to theusual library tasks of classifying, cataloguing,covering, labelling, shelving, tidying, straight-ening and loaning books, I have become anexpert in literature searching, and a whole hostof other aspects of modern library work. I havedeveloped and arranged material for libraryintranet pages, and been involved in the publicityand marketing of library services, by producingposters, newsletters, and flyers, undertaking auser survey, and promoting the ADITUS websiteand services. I have represented the Libraryservices at Trust meetings, and at Salford PCTwelcomed John Hutton, Minister of State forHealth, to officially open the Library andResource Service. In addition to the usuallibrary environments, I have worked for thehealth promotion unit, based within the libraryat Salford PCT, which introduced new types ofuser, information and services, and I will alsobe spending time at the Medicines Informationunit at Hope Hospital.
So what have I learnt from all this work? Therole of the library and librarian in the NHS isto ensure that everyone involved in health andsocial care has convenient access to informationto ensure they can deliver care efficiently andeffectively. With the huge number of journalsavailable online, clinical databases and electronicTables of Contents, it should be easier than everfor people to keep up to date with the enormousvolume of new information that is constantlyproduced – the job of the Library service is toencourage this to happen. It’s not all aboutjournals and e-resources of course, but this bestdemonstrates the most pertinent observation Ican make: the importance of communicationbetween libraries.
There already is communication in many forms:meetings of patch groups, with University
libraries, of Greater Manchester libraries, ofPCT libraries, for example, as well as theLIHNN email list, and the underused ADITUSvirtual-communities. For longer term changesand developments this is fine, but I think thereshould be more dialogue on everyday issues:how to do user surveys, discussing the best wayto arrange and manage interlibrary loans, howto deal with missing books and users, for exam-ple, not to mention how to get the most out ofthe ever-increasing range of electronicresources - every library service has its ownway of doing these things. The variety of methodsI have seen to deal with these and other issues,
and the duplication of thought, effort and timespent on the same things highlights to me simplechanges which can be made to improve efficiency. Even sharing posters, leaflets, help-sheets and training materials can be hugelybeneficial, can be done instantly by email, andcan help to create a shared identity forlibraries. In Salford and Trafford, for example,we are beginning to promote a single libraryservice, rather than several separate libraries,by using leaflets and posters as well as planningevents to encourage use from particular groups
who do not use the library as much as theyshould.
Now that my year is coming to an end, whatam I doing next? In September I’ll be startingthe MA in Library and InformationManagement at Manchester MetropolitanUniversity and, dependent on money, I shouldbe finished by the end of Summer 2005.Funding for postgraduate students in this fieldcomes mainly from the Arts and HumanitiesResearch Board, but as the name suggests competition is against all the other students inthe arts and humanities (I have applied to thembefore to fund an MA in history without anysuccess, so fingers crossed please.) If the AHRBis unforthcoming again, then I may be able toget a smaller sum of money from the Universityitself, and I’ll also be looking for a part time job.
Now for the question that everyone asks me: doI want to stay in the NHS when I’ve qualified?The diplomatic answer is ‘probably, yes.’Without much experience of any other kind oflibrary though, it’s difficult to be certain. I dothink that the personal service that can beoffered in a smaller library environment canmake it more fun, and a busy student-orientatedlibrary seems to make for an enjoyable workingday, whereas I would be worried about gettingstuck in a rut of shelving books in a hugeUniversity library or similar. But that’s just mypre-conceived opinion, so in fact the trueanswer should be ‘probably, but I’m open topersuasion.’
The good news then, is that my experience hasn’tput me off wanting to work in libraries (anothercommon question!) In fact, the year has beenmore varied and interesting than I expected, soI’m more certain than I was twelve months ago.What attracts me is the mixture of the traditionalaspects of the library profession together withthe rapid development of new, electronic information management techniques, and thepotential to use my a wide range of skills toassist others and promote education and learning.We should all think of the three patron saints ofLibraries: Jerome, Lawrence and particularlyCatharine of Alexandria whose skill, languageand devotion allowed her to spread knowledgeand wisdom to those around her.
Finally, while I have the opportunity, I’d like tosay that this year will hopefully have animmense impact and provide a massive head-start for my future career, so thanks to thosepeople whose idea it was to have a graduatetrainee. And thanks to everyone i have workedwith over the year, at Salford PCT, TraffordHealthcare, Bolton, Salford and TraffordMental Health, Salford Royal Hospitals andMedicines Information at Hope Hospital.
11
SALFORD & TRAFFORD’S GRADUATE TRAINEEJames Allen
Stained glass window in the Chapel of St Catharine’sCollege, Cambridge. From www.caths.cam.ac.uk
John Hutton
LIHNNK*13 spring'04 v2 9/6/04 2:41 pm Page 12