nonalcoholic fatty liver disease...
TRANSCRIPT
NONALCOHOLIC NONALCOHOLIC FATTY LIVER FATTY LIVER
DISEASE (NAFLD)DISEASE (NAFLD)
Joel M. Andres, M.D.Joel M. Andres, M.D.University of FloridaUniversity of Florida
OBJECTIVESOBJECTIVES
To understand the To understand the pathophysiologypathophysiology of of nonalcoholic fatty liver disease (NAFLD)nonalcoholic fatty liver disease (NAFLD)-- The link between NAFLD and insulin RThe link between NAFLD and insulin R-- The relationship of insulin R to The relationship of insulin R to steatosissteatosis-- The The ““second hitsecond hit”” theory of theory of steatosissteatosis to NASHto NASH
To learn about To learn about adipocytokinesadipocytokines and and HSCsHSCs,,implicated in the devimplicated in the dev--mentment of hepatic of hepatic inflaminflam and and fibrosis in patients with NAFLDfibrosis in patients with NAFLD
To understand the key items for diagnosis andTo understand the key items for diagnosis andmanagement of NAFLD in childrenmanagement of NAFLD in children
OBESITYOBESITY
BASIC FACTSBASIC FACTS DEFINITIONDEFINITION
Epidemic of obesity, probably Epidemic of obesity, probably the most common health issue the most common health issue of childrenof children
Because BMI norms for children Because BMI norms for children vary with age and gender, BMI vary with age and gender, BMI %tiles rather than absolute %tiles rather than absolute BMIBMI’’s are determineds are determined
% of children 6% of children 6--11 yrs of age 11 yrs of age with BMI >95with BMI >95thth more than more than doubled from 6.5 to 15.3 % doubled from 6.5 to 15.3 % betwbetwlate 70late 70’’s and 2000s and 2000
Cut off values to define the Cut off values to define the heaviest children are the 85heaviest children are the 85thth and and 9595thth %tiles (BMI%tiles (BMI’’s of 25 and 30, s of 25 and 30, respectively, as maturity is respectively, as maturity is approached in adolescence)approached in adolescence)
Above #Above #’’s double if one includes s double if one includes children with BMI > 85children with BMI > 85thth %tile%tile
National Center for Health Stats, 2003
Strauss RS. JAMA 2001;286:2845
Medical Conditions Medical Conditions AssocAssoc’’eded WithWithCHILDHOOD OBESITYCHILDHOOD OBESITY
HypertensionHypertensionHyperlipidemiaHyperlipidemiaImpaired Glucose Tolerance/ DiabetesImpaired Glucose Tolerance/ DiabetesGallbladder Disease/ GallstonesGallbladder Disease/ GallstonesNonalcoholic Fatty Liver Disease (NAFLD)Nonalcoholic Fatty Liver Disease (NAFLD)-- Elevated Liver Elevated Liver TransaminasesTransaminases CommonCommon-- Severe Fibrosis and Cirrhosis Also OccurSevere Fibrosis and Cirrhosis Also Occur
Rashid M, et al. JPGHAN2000;30:48
Tomuinaga K, et al.Dig Dis Sci 1995;40:’02
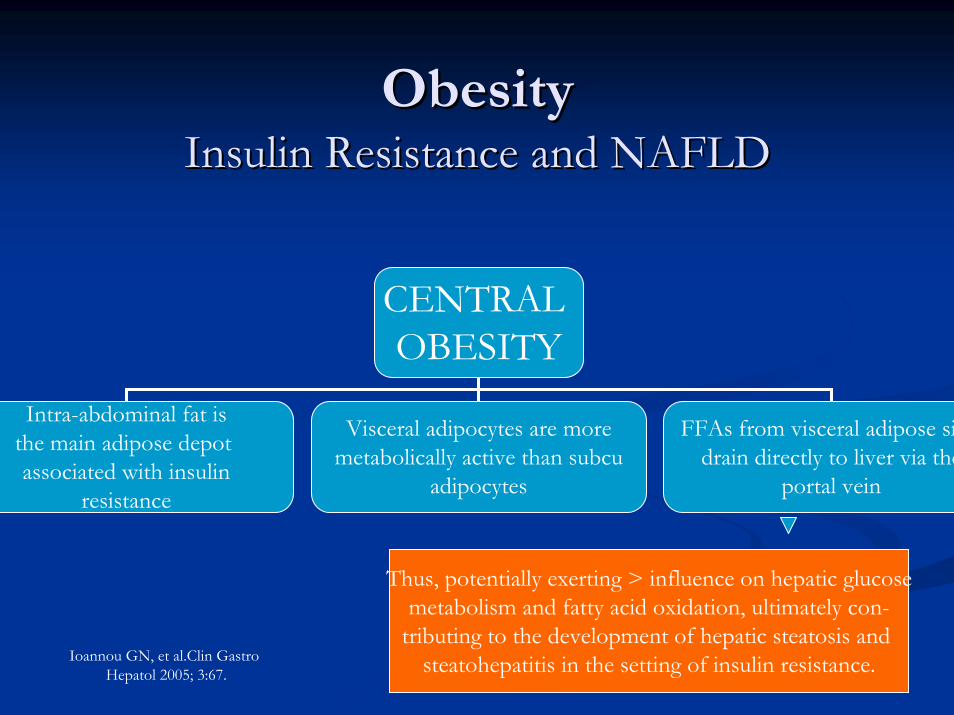
ObesityObesityInsulin Resistance and NAFLDInsulin Resistance and NAFLD
CENTRAL OBESITY
Intra-abdominal fat isthe main adipose depot associated with insulin
resistance
Visceral adipocytes are moremetabolically active than subcu
adipocytes
FFAs from visceral adipose sidrain directly to liver via the
portal vein
Ioannou GN, et al.Clin Gastro Hepatol 2005; 3:67.
Thus, potentially exerting > influence on hepatic glucosemetabolism and fatty acid oxidation, ultimately con-
tributing to the development of hepatic steatosis and steatohepatitis in the setting of insulin resistance.
NAFLDNAFLDHistorical FactsHistorical Facts
KlatskinKlatskin: In 1979, he presented findings of a : In 1979, he presented findings of a landmark landmark histologichistologic study about nonalcoholic study about nonalcoholic liver disease which mimicked alcohol induced liver disease which mimicked alcohol induced hepatitis and cirrhosishepatitis and cirrhosisLudwig: In 1980, he coined the term Ludwig: In 1980, he coined the term ““nonnon--alcoholic alcoholic steatohepatitissteatohepatitis”” in patients whose liver in patients whose liver histology mimicked alcoholic hepatitishistology mimicked alcoholic hepatitis
Ludwig J, et al. Mayo Clin Proc 1980; 55: 434
Spectrum of NAFLDSpectrum of NAFLDBASIC FACTSBASIC FACTS
NAFLD is a broad term NAFLD is a broad term ---- Encompasses Encompasses steatosissteatosis, , steatosissteatosis w w inflammation, NASH, and cirrhosis. NAFLD is now inflammation, NASH, and cirrhosis. NAFLD is now recognrecogn’’ as as the most common cause of liver disease in pediatricsthe most common cause of liver disease in pediatrics
The terms NAFLD and NASH are not interchangeableThe terms NAFLD and NASH are not interchangeable
NASH may be the most common cause of cryptogenic cirrhosis; NASH may be the most common cause of cryptogenic cirrhosis; it may lead to end stage liver disease and is a serious it may lead to end stage liver disease and is a serious complication of childhood obesitycomplication of childhood obesity
The link between NAFLD, insulin resistance and metabolic The link between NAFLD, insulin resistance and metabolic syndrome is not completely understoodsyndrome is not completely understood
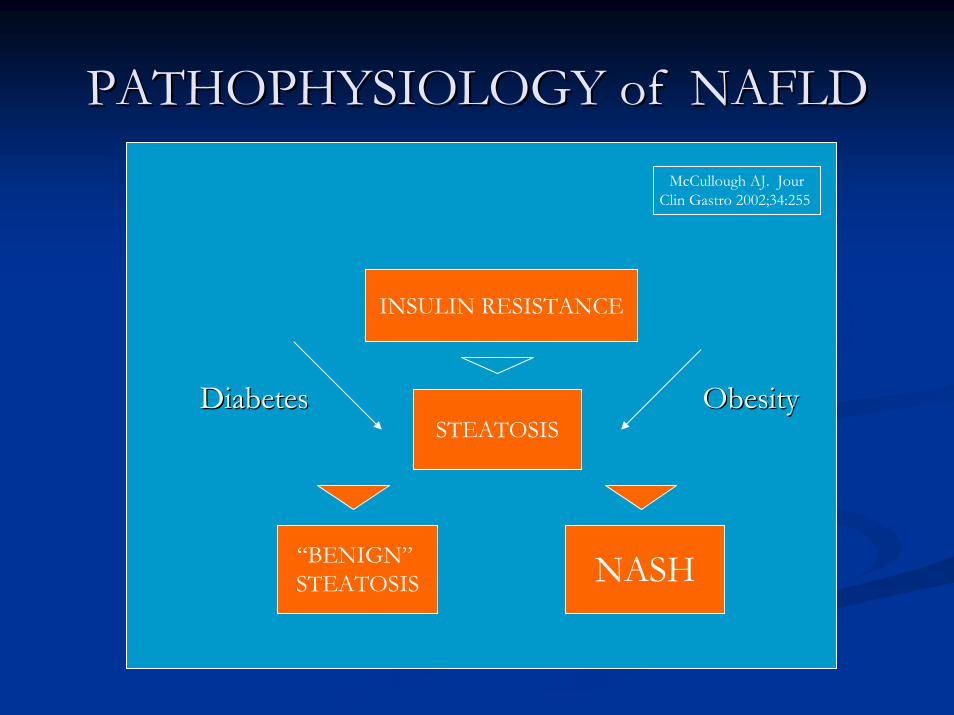
PATHOPHYSIOLOGY of NAFLDPATHOPHYSIOLOGY of NAFLD
INSULIN RESISTANCE
STEATOSIS
“BENIGN”STEATOSIS NASH
DiabetesDiabetes ObesityObesity
McCullough AJ. JourClin Gastro 2002;34:255
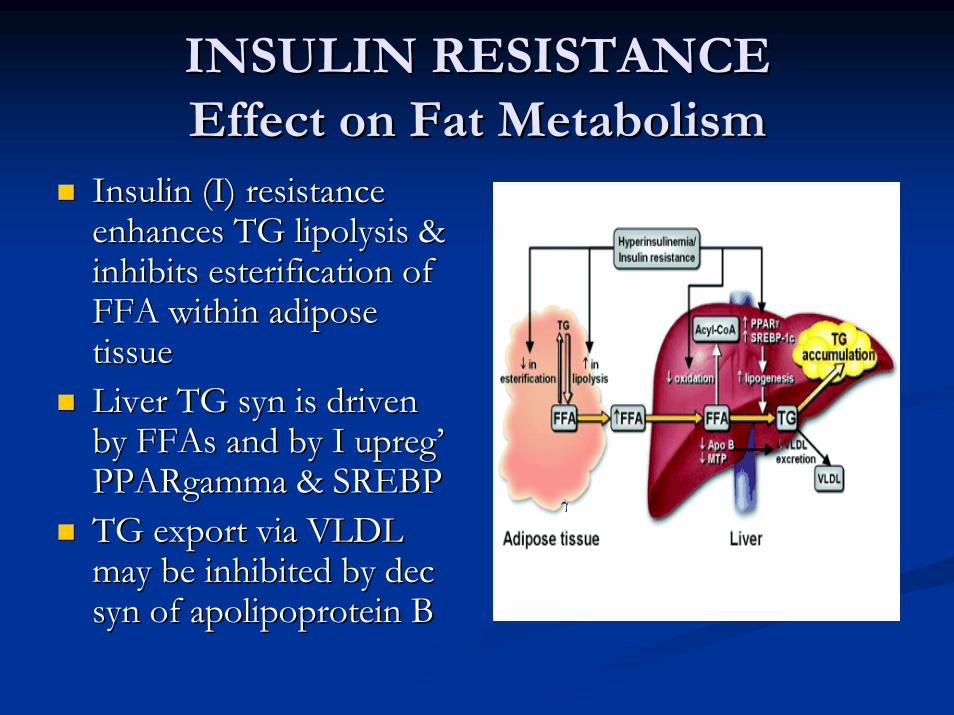
INSULIN RESISTANCEINSULIN RESISTANCEEffect on Fat MetabolismEffect on Fat Metabolism
Insulin (I) resistance Insulin (I) resistance enhances TG enhances TG lipolysislipolysis & & inhibits inhibits esterificationesterification of of FFA within adipose FFA within adipose tissuetissueLiver TG Liver TG synsyn is driven is driven by by FFAsFFAs and by I and by I upregupreg’’PPARgammaPPARgamma & SREBP& SREBPTG export via VLDL TG export via VLDL may be inhibited by may be inhibited by decdecsynsyn of of apolipoproteinapolipoprotein BB
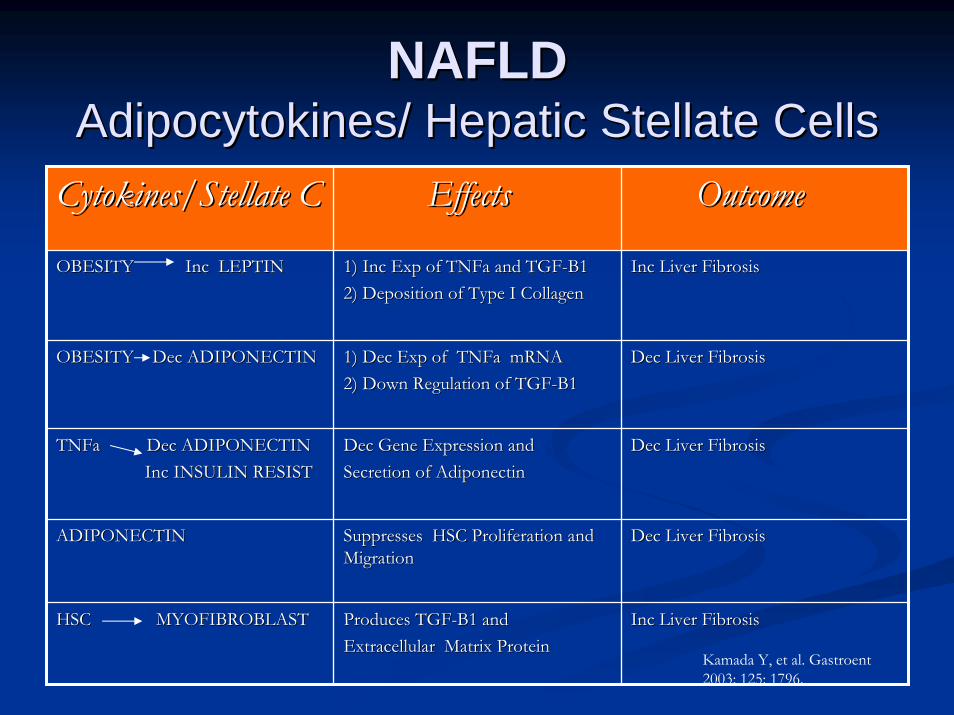
NAFLDNAFLDAdipocytokinesAdipocytokines/ Hepatic / Hepatic StellateStellate CellsCellsCytokines/Cytokines/StellateStellate CC EffectsEffects OutcomeOutcome
OBESITY Inc LEPTIN OBESITY Inc LEPTIN 1) Inc Exp of 1) Inc Exp of TNFaTNFa and TGFand TGF--B1B12) Deposition of Type I Collagen2) Deposition of Type I Collagen
Inc Liver FibrosisInc Liver Fibrosis
OBESITY Dec ADIPONECTINOBESITY Dec ADIPONECTIN 1) Dec Exp of 1) Dec Exp of TNFaTNFa mRNAmRNA2) Down Regulation of TGF2) Down Regulation of TGF--B1B1
Dec Liver FibrosisDec Liver Fibrosis
TNFaTNFa Dec ADIPONECTINDec ADIPONECTINInc INSULIN RESISTInc INSULIN RESIST
Dec Gene Expression and Dec Gene Expression and Secretion of Secretion of AdiponectinAdiponectin
Dec Liver FibrosisDec Liver Fibrosis
ADIPONECTINADIPONECTIN Suppresses HSC Proliferation and Suppresses HSC Proliferation and Migration Migration
Dec Liver FibrosisDec Liver Fibrosis
HSC MYOFIBROBLASTHSC MYOFIBROBLAST Produces TGFProduces TGF--B1 and B1 and ExtracellularExtracellular Matrix ProteinMatrix Protein
Inc Liver FibrosisInc Liver Fibrosis
Kamada Y, et al. Gastroent2003; 125: 1796.
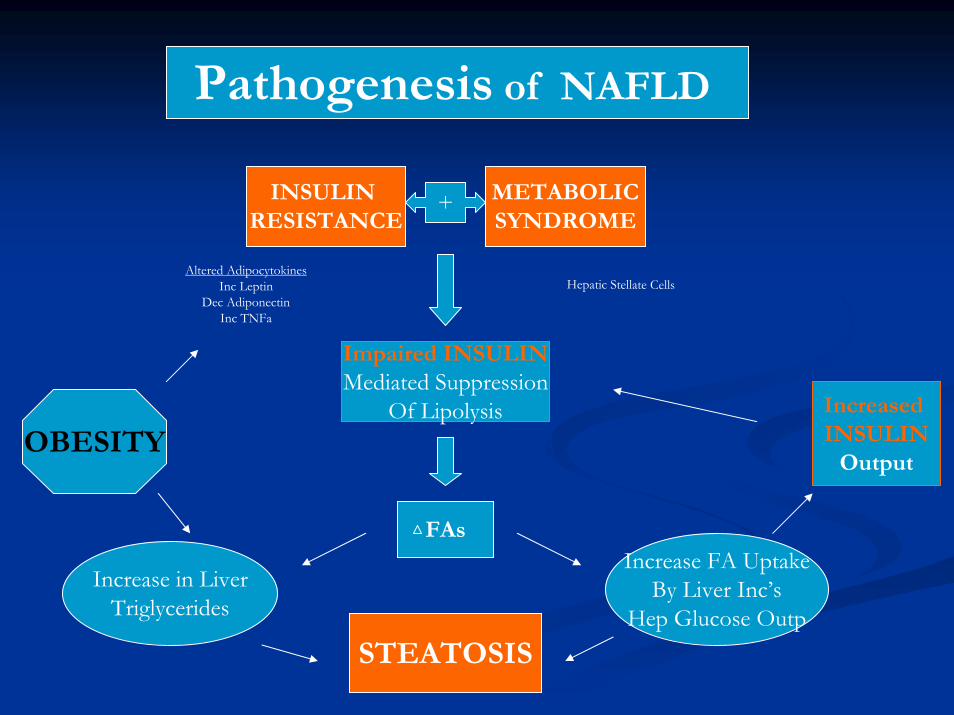
Pathogenesis of NAFLD
INSULIN RESISTANCE
+ METABOLICSYNDROME
Altered AdipocytokinesInc Leptin
Dec AdiponectinInc TNFa
Hepatic Stellate Cells
Impaired INSULINMediated Suppression
Of Lipolysis
FAs
STEATOSIS
Increase in LiverTriglycerides
Increase FA UptakeBy Liver Inc’s
Hep Glucose Outp
Increased INSULIN
OutputOBESITY
STEATOSIS to NASH: STEATOSIS to NASH: ““22ndnd HitHit””
Mitochondrial and Mitochondrial and peroxisomalperoxisomal oxidation of oxidation of FFAsFFAs in liverin liverFree radicals (Reactive O2 species) Free radicals (Reactive O2 species) Lipid Lipid peroxidationperoxidation of membranesof membranesHepatocyteHepatocyte membrane damagemembrane damageInflammationInflammationFibrosisFibrosis
Day CP, et al. NASH. Gastroenterology 1998;114: 842.
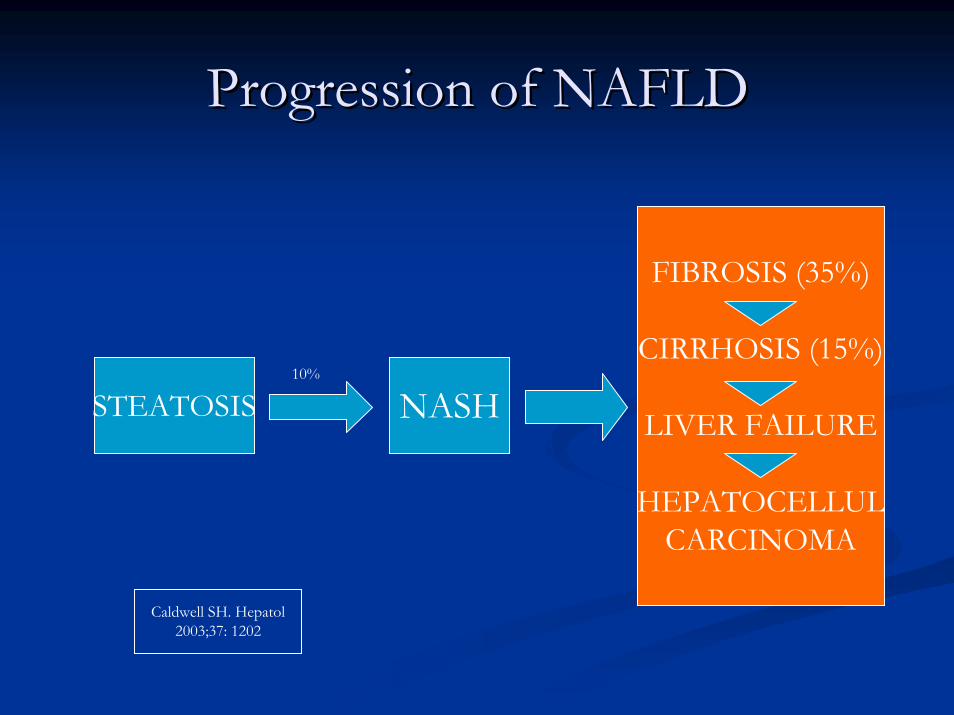
Progression of NAFLDProgression of NAFLD
STEATOSIS NASH
FIBROSIS (35%)
CIRRHOSIS (15%)
LIVER FAILURE
HEPATOCELLULCARCINOMA
10%
Caldwell SH. Hepatol2003;37: 1202
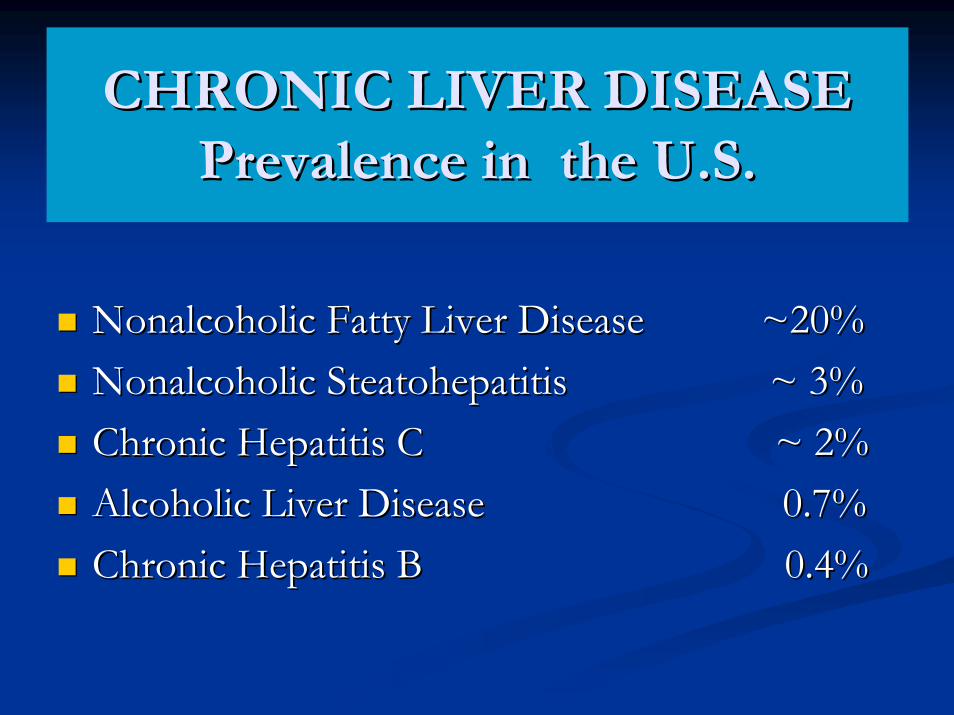
CHRONIC LIVER DISEASECHRONIC LIVER DISEASEPrevalence in the U.S.Prevalence in the U.S.
Nonalcoholic Fatty Liver Disease ~20%Nonalcoholic Fatty Liver Disease ~20%Nonalcoholic Nonalcoholic SteatohepatitisSteatohepatitis ~ 3%~ 3%Chronic Hepatitis C ~ 2%Chronic Hepatitis C ~ 2%Alcoholic Liver Disease 0.7%Alcoholic Liver Disease 0.7%Chronic Hepatitis B 0.4%Chronic Hepatitis B 0.4%
NAFLD: EpidemiologyNAFLD: Epidemiology
Overlooked or underestimated in the past, and not well Overlooked or underestimated in the past, and not well known at presentknown at presentHighest prevalence is in adults aged 40Highest prevalence is in adults aged 40--60 yrs, but 60 yrs, but NAFLD occurs in children & adolescentsNAFLD occurs in children & adolescentsHigh prevalence in industrialized countriesHigh prevalence in industrialized countriesFemales > Males, but controversialFemales > Males, but controversialNASH appears to be overtaking chronic hepatitis C as NASH appears to be overtaking chronic hepatitis C as the next the next ““epidemicepidemic”” in liver diseasein liver disease
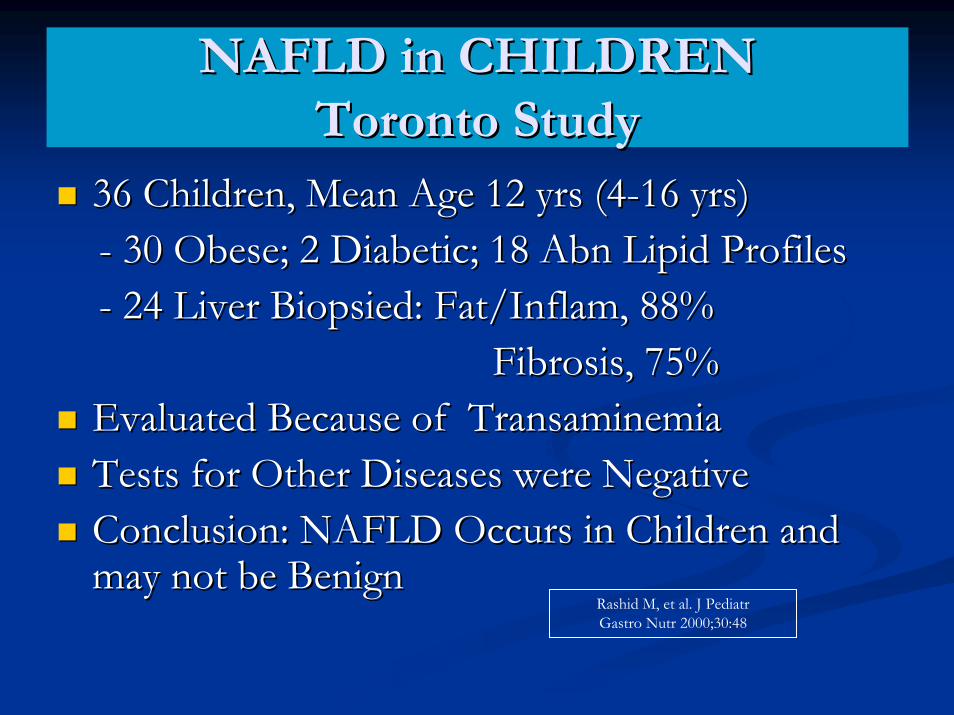
NAFLD in CHILDRENNAFLD in CHILDRENToronto StudyToronto Study
36 Children, Mean Age 12 yrs (436 Children, Mean Age 12 yrs (4--16 yrs)16 yrs)-- 30 Obese; 2 Diabetic; 18 30 Obese; 2 Diabetic; 18 AbnAbn Lipid ProfilesLipid Profiles-- 24 Liver 24 Liver BiopsiedBiopsied: Fat/: Fat/InflamInflam, 88%, 88%
Fibrosis, 75%Fibrosis, 75%Evaluated Because of Evaluated Because of TransaminemiaTransaminemiaTests for Other Diseases were NegativeTests for Other Diseases were NegativeConclusion: NAFLD Occurs in Children and Conclusion: NAFLD Occurs in Children and may not be Benignmay not be Benign
Rashid M, et al. J PediatrGastro Nutr 2000;30:48
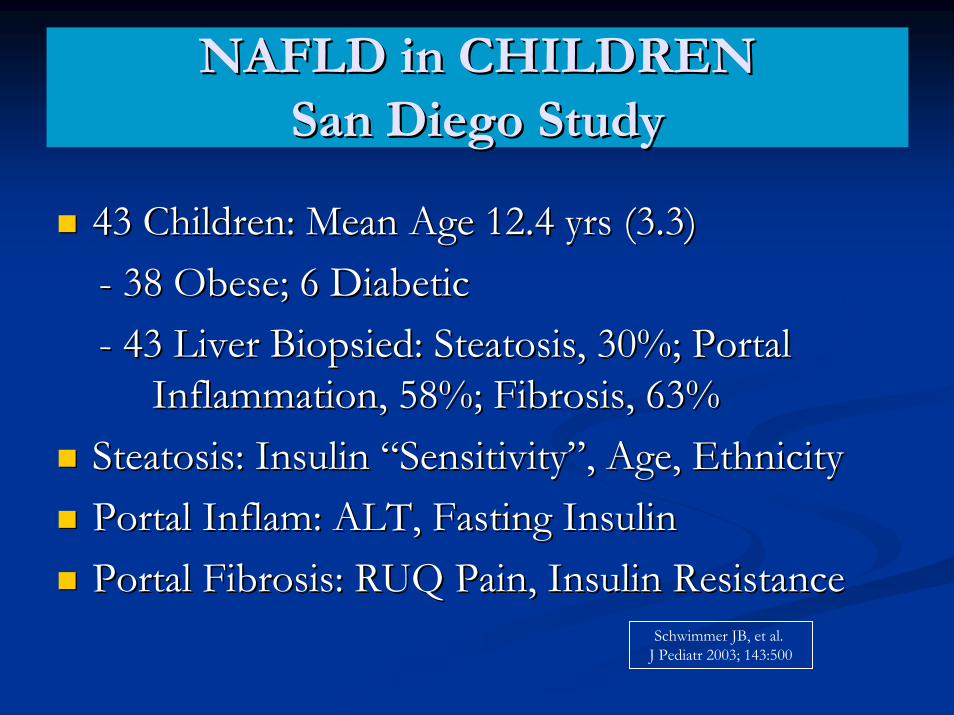
NAFLD in CHILDRENNAFLD in CHILDRENSan Diego StudySan Diego Study
43 Children: Mean Age 12.4 yrs (3.3)43 Children: Mean Age 12.4 yrs (3.3)-- 38 Obese; 6 Diabetic38 Obese; 6 Diabetic-- 43 Liver 43 Liver BiopsiedBiopsied: : SteatosisSteatosis, 30%; Portal , 30%; Portal
Inflammation, 58%; Fibrosis, 63%Inflammation, 58%; Fibrosis, 63%SteatosisSteatosis: Insulin : Insulin ““SensitivitySensitivity””, Age, Ethnicity, Age, EthnicityPortal Portal InflamInflam: ALT, Fasting Insulin: ALT, Fasting InsulinPortal Fibrosis: RUQ Pain, Insulin Resistance Portal Fibrosis: RUQ Pain, Insulin Resistance
Schwimmer JB, et al. J Pediatr 2003; 143:500
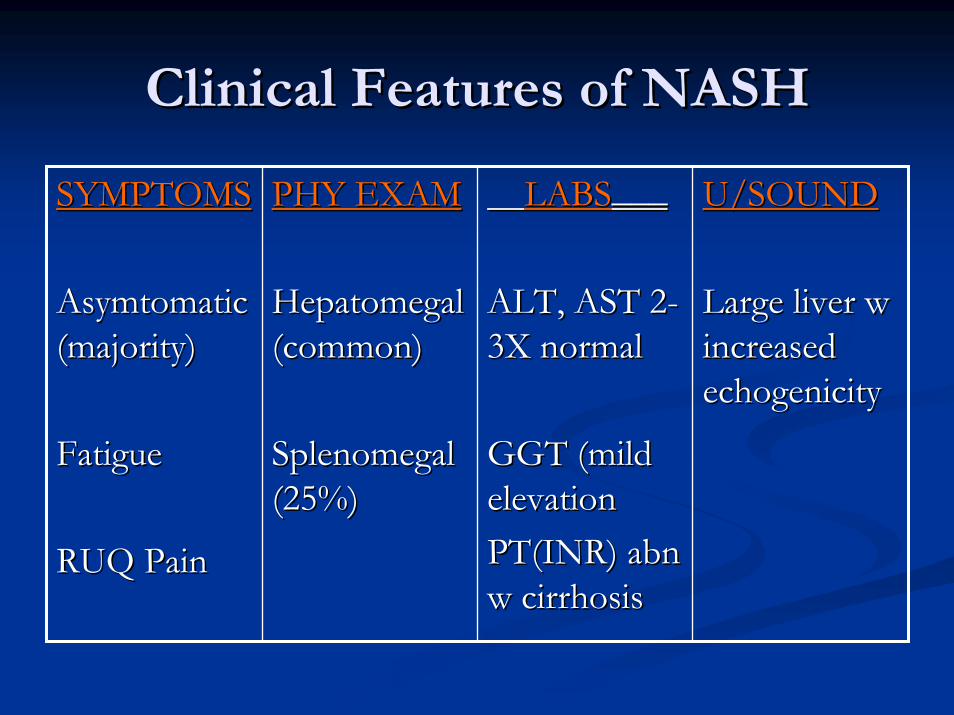
Clinical Features of NASHClinical Features of NASH
SYMPTOMSSYMPTOMS
AsymtomaticAsymtomatic(majority)(majority)
FatigueFatigue
RUQ PainRUQ Pain
PHY EXAMPHY EXAM
HepatomegalHepatomegal(common)(common)
SplenomegalSplenomegal(25%)(25%)
LABSLABS___ ___
ALT, AST 2ALT, AST 2--3X normal3X normal
GGT (mild GGT (mild elevationelevationPT(INR) PT(INR) abnabnw cirrhosisw cirrhosis
U/SOUNDU/SOUND
Large liver w Large liver w increased increased echogenicityechogenicity
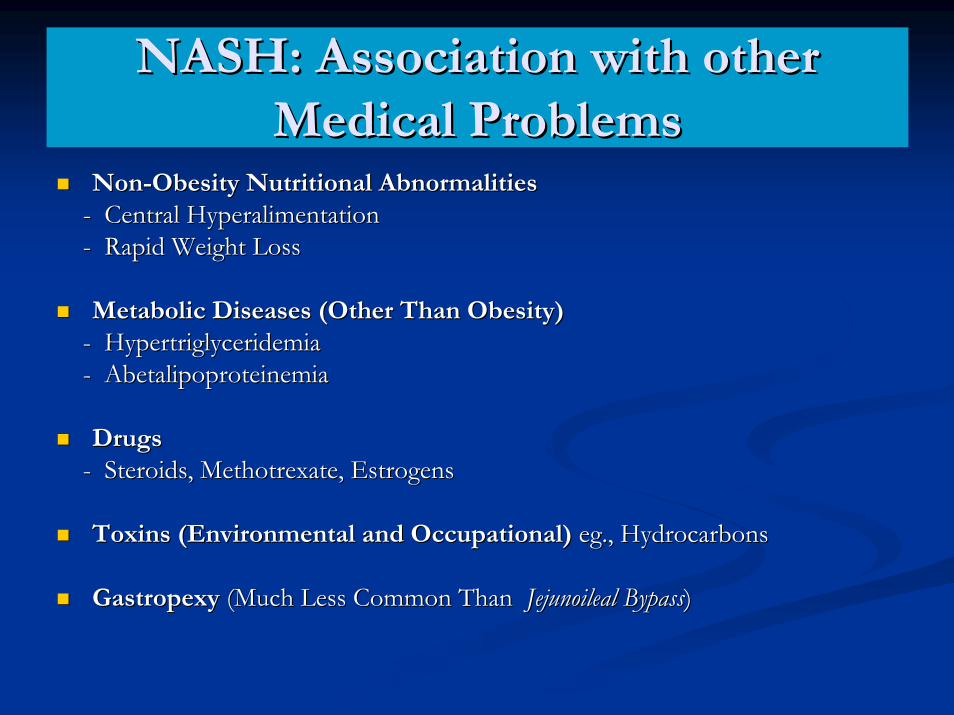
NASH: Association with otherNASH: Association with otherMedical ProblemsMedical Problems
NonNon--Obesity Nutritional AbnormalitiesObesity Nutritional Abnormalities-- Central Central HyperalimentationHyperalimentation-- Rapid Weight LossRapid Weight Loss
Metabolic Diseases (Other Than Obesity)Metabolic Diseases (Other Than Obesity)-- HypertriglyceridemiaHypertriglyceridemia-- AbetalipoproteinemiaAbetalipoproteinemia
DrugsDrugs-- Steroids, Steroids, MethotrexateMethotrexate, Estrogens, Estrogens
Toxins (Environmental and Occupational)Toxins (Environmental and Occupational) egeg., Hydrocarbons., Hydrocarbons
GastropexyGastropexy (Much Less Common Than (Much Less Common Than JejunoilealJejunoileal BypassBypass) )
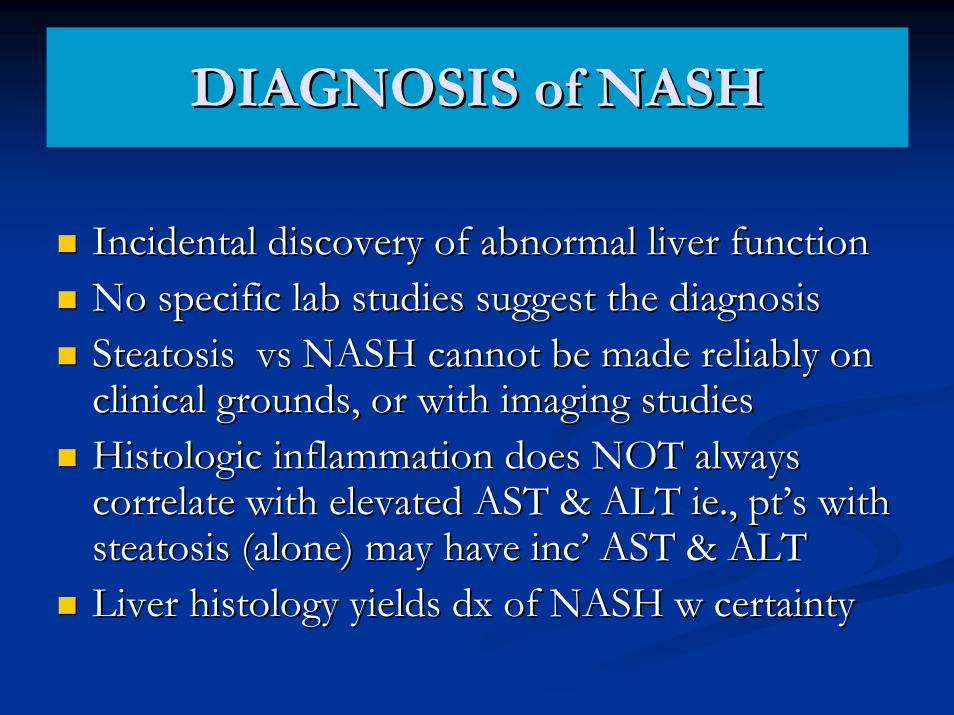
DIAGNOSIS of NASHDIAGNOSIS of NASH
Incidental discovery of abnormal liver functionIncidental discovery of abnormal liver functionNo specific lab studies suggest the diagnosisNo specific lab studies suggest the diagnosisSteatosisSteatosis vsvs NASH cannot be made reliably on NASH cannot be made reliably on clinical grounds, or with imaging studiesclinical grounds, or with imaging studiesHistologicHistologic inflammation does NOT always inflammation does NOT always correlate with elevated AST & ALT correlate with elevated AST & ALT ieie., pt., pt’’s with s with steatosissteatosis (alone) may have inc(alone) may have inc’’ AST & ALTAST & ALTLiver histology yields Liver histology yields dxdx of NASH w certaintyof NASH w certainty
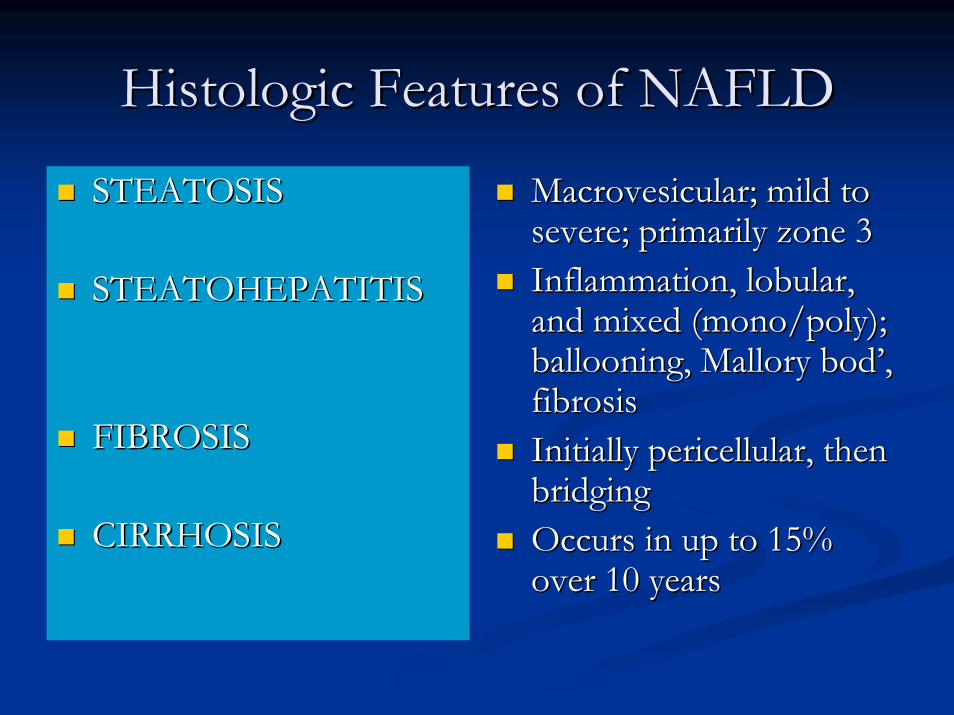
HistologicHistologic Features of NAFLDFeatures of NAFLD
STEATOSISSTEATOSIS
STEATOHEPATITISSTEATOHEPATITIS
FIBROSISFIBROSIS
CIRRHOSISCIRRHOSIS
MacrovesicularMacrovesicular; mild to ; mild to severe; primarily zone 3severe; primarily zone 3Inflammation, lobular, Inflammation, lobular, and mixed (mono/poly); and mixed (mono/poly); ballooning, Mallory ballooning, Mallory bodbod’’, , fibrosisfibrosisInitially Initially pericellularpericellular, then , then bridgingbridgingOccurs in up to 15% Occurs in up to 15% over 10 yearsover 10 years
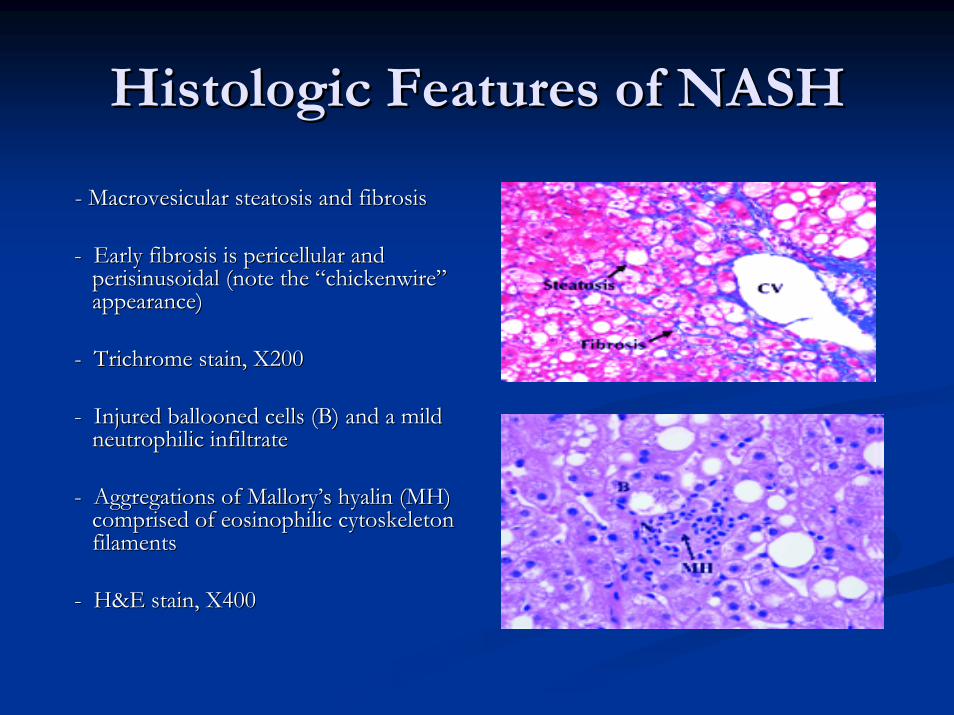
HistologicHistologic Features of NASHFeatures of NASH
-- MacrovesicularMacrovesicular steatosissteatosis and fibrosisand fibrosis
-- Early fibrosis is Early fibrosis is pericellularpericellular and and perisinusoidalperisinusoidal (note the (note the ““chickenwirechickenwire””appearance)appearance)
-- TrichromeTrichrome stain, X200stain, X200
-- Injured ballooned cells (B) and a mild Injured ballooned cells (B) and a mild neutrophilicneutrophilic infiltrateinfiltrate
-- Aggregations of MalloryAggregations of Mallory’’s s hyalinhyalin (MH) (MH) comprised of comprised of eosinophiliceosinophilic cytoskeleton cytoskeleton filamentsfilaments
-- H&E stain, X400H&E stain, X400
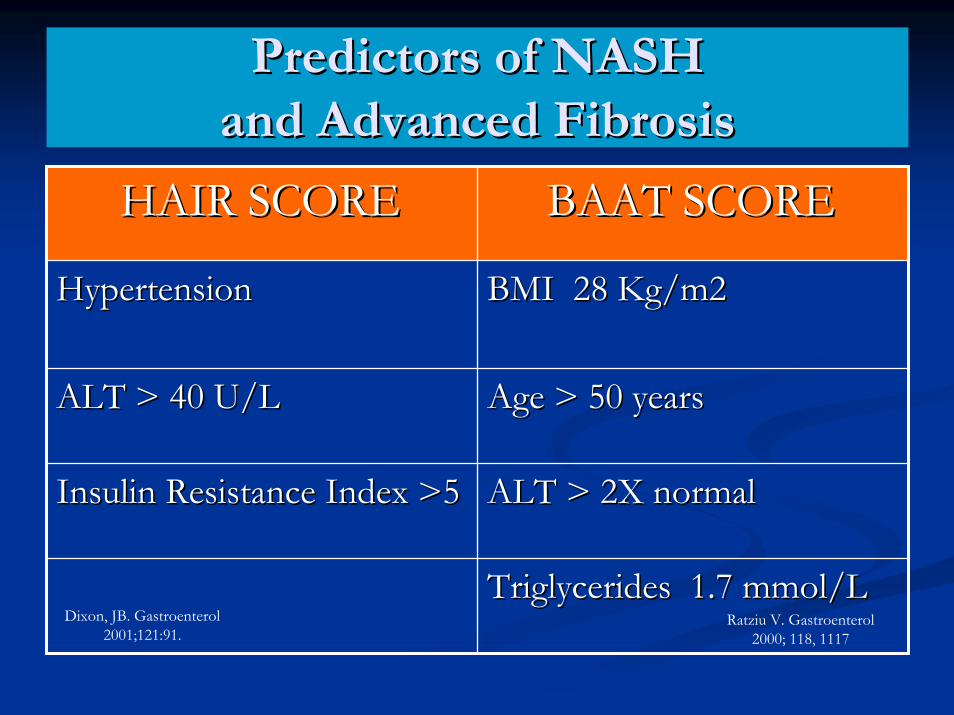
Predictors of NASHPredictors of NASHand Advanced Fibrosisand Advanced Fibrosis
HAIR SCOREHAIR SCORE BAAT SCOREBAAT SCORE
HypertensionHypertension BMI 28 Kg/m2BMI 28 Kg/m2
ALT > 40 U/LALT > 40 U/L Age > 50 yearsAge > 50 years
Insulin Resistance Index >5Insulin Resistance Index >5 ALT > 2X normalALT > 2X normal
Triglycerides 1.7 Triglycerides 1.7 mmolmmol/L/LDixon, JB. Gastroenterol
2001;121:91.Ratziu V. Gastroenterol
2000; 118, 1117
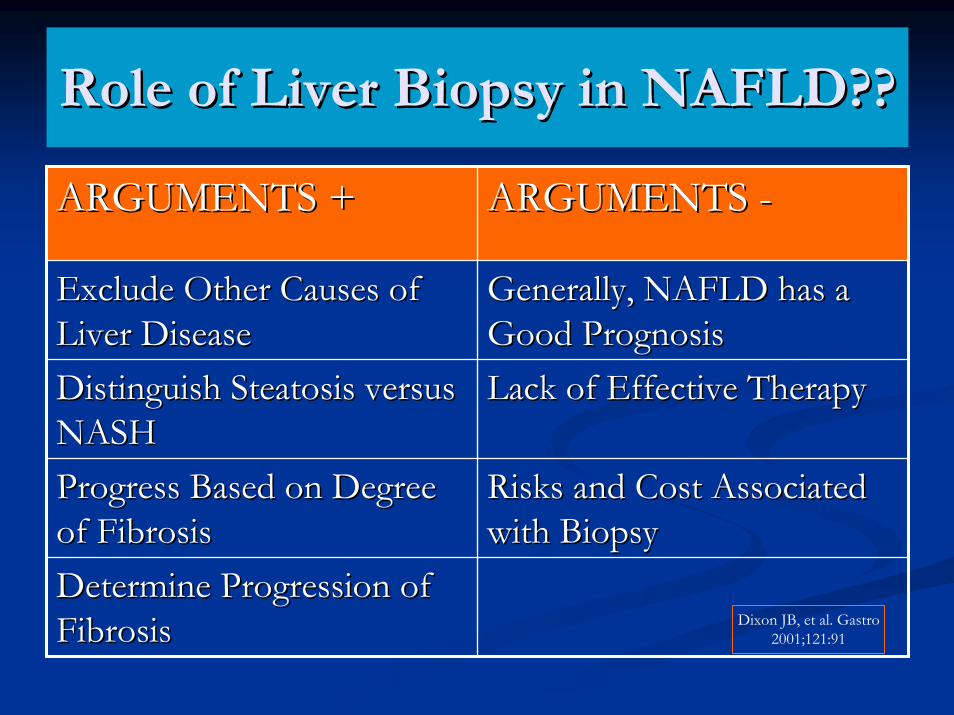
Role of Liver Biopsy in NAFLD??Role of Liver Biopsy in NAFLD??
ARGUMENTS +ARGUMENTS + ARGUMENTS ARGUMENTS --
Exclude Other Causes of Exclude Other Causes of Liver DiseaseLiver Disease
Generally, NAFLD has a Generally, NAFLD has a Good PrognosisGood Prognosis
Distinguish Distinguish SteatosisSteatosis versus versus NASHNASH
Lack of Effective TherapyLack of Effective Therapy
Progress Based on Degree Progress Based on Degree of Fibrosisof Fibrosis
Risks and Cost Associated Risks and Cost Associated with Biopsywith Biopsy
Determine Progression of Determine Progression of FibrosisFibrosis Dixon JB, et al. Gastro
2001;121:91
Treatment of NAFLD/NASHTreatment of NAFLD/NASHCurrent ApproachCurrent Approach
Gradual, Sustained Weight LossGradual, Sustained Weight Loss-- ReRe--establish the establish the ““Family TableFamily Table””-- Promote Better Nutrition in SchoolsPromote Better Nutrition in SchoolsExercise ProgramExercise Program-- Put High Priority on Family FitnessPut High Priority on Family Fitness-- Expand Green Spaces for ExerciseExpand Green Spaces for ExerciseTreat Diabetes Treat Diabetes Treat Lipid Disorder Treat Lipid Disorder Treat HypertensionTreat Hypertension
Treatment of NAFLD/NASHTreatment of NAFLD/NASHExperimental TherapiesExperimental Therapies
Insulin Sensitizing Drugs: Insulin Sensitizing Drugs: ThioglitazonesThioglitazones-- TroglitazoneTroglitazone-- PioglitazonePioglitazone-- RosiglitazoneRosiglitazoneAntioxidants: Vitamin EAntioxidants: Vitamin EUrsodiolUrsodiolBetaineBetaineMetformin
Charlton M. Clin GastroHepatol 2004;2: 1048
Adams LA, et al. Clin GastroHepatol 2004; 2: 1059
Metformin Abdelnalek MF, et al. Am JGastro 2001;96: 2711
““Leave Leave gourmandisinggourmandising……..”” KingKingHenry V advises Falstaff,Henry V advises Falstaff,…”…”know know the grave doth gape for thee thricethe grave doth gape for thee thrice
wider than for other menwider than for other men””
Shakespeare, 1564Shakespeare, 1564--16161616