non-mydriatic wide field fundus photography in bilateral serous retinal detachment due to hellp...
TRANSCRIPT
Arch Gynecol Obstet (2012) 286:819–820
DOI 10.1007/s00404-012-2343-1LETTER TO THE EDITOR
Non-mydriatic wide Weld fundus photography in bilateral serous retinal detachment due to HELLP syndrome
Wolfgang J. Mayer · Imad Hakim · Michael W. Ulbig · Marcus Kernt · Christos Haritoglou
Received: 5 March 2012 / Accepted: 16 April 2012 / Published online: 24 April 2012© Springer-Verlag 2012
Dear editor,
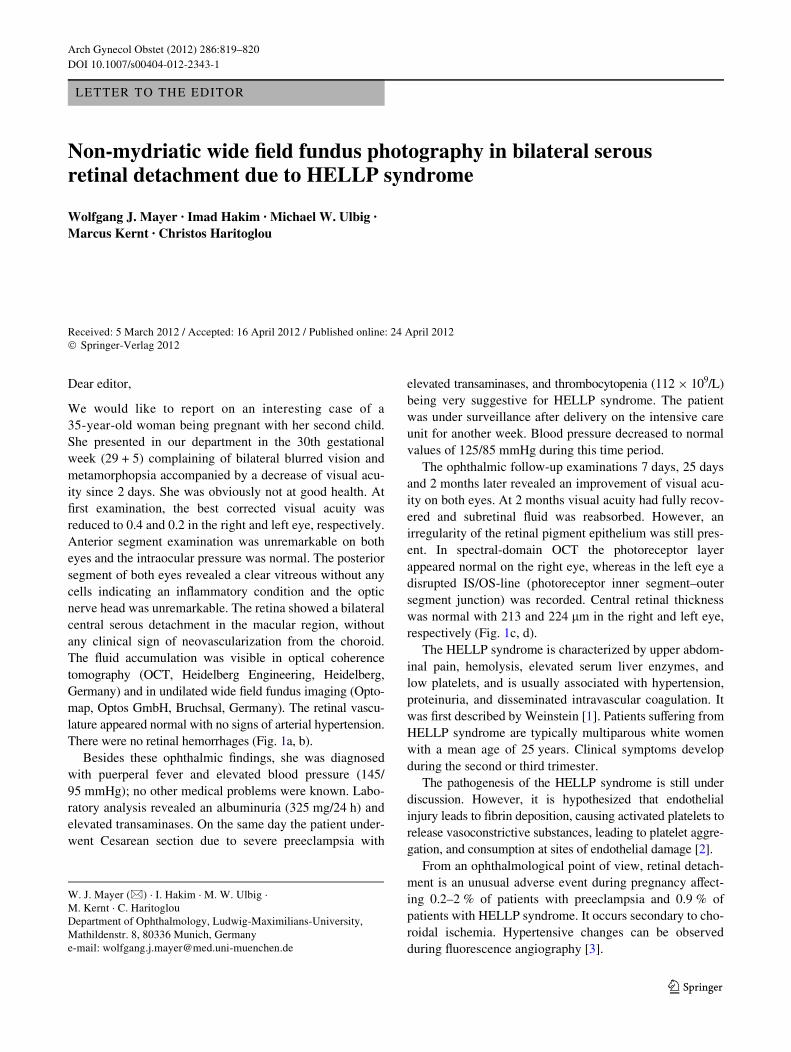
We would like to report on an interesting case of a35-year-old woman being pregnant with her second child.She presented in our department in the 30th gestationalweek (29 + 5) complaining of bilateral blurred vision andmetamorphopsia accompanied by a decrease of visual acu-ity since 2 days. She was obviously not at good health. AtWrst examination, the best corrected visual acuity wasreduced to 0.4 and 0.2 in the right and left eye, respectively.Anterior segment examination was unremarkable on botheyes and the intraocular pressure was normal. The posteriorsegment of both eyes revealed a clear vitreous without anycells indicating an inXammatory condition and the opticnerve head was unremarkable. The retina showed a bilateralcentral serous detachment in the macular region, withoutany clinical sign of neovascularization from the choroid.The Xuid accumulation was visible in optical coherencetomography (OCT, Heidelberg Engineering, Heidelberg,Germany) and in undilated wide Weld fundus imaging (Opto-map, Optos GmbH, Bruchsal, Germany). The retinal vascu-lature appeared normal with no signs of arterial hypertension.There were no retinal hemorrhages (Fig. 1a, b).
Besides these ophthalmic Wndings, she was diagnosedwith puerperal fever and elevated blood pressure (145/95 mmHg); no other medical problems were known. Labo-ratory analysis revealed an albuminuria (325 mg/24 h) andelevated transaminases. On the same day the patient under-went Cesarean section due to severe preeclampsia with
elevated transaminases, and thrombocytopenia (112 £ 109/L)being very suggestive for HELLP syndrome. The patientwas under surveillance after delivery on the intensive careunit for another week. Blood pressure decreased to normalvalues of 125/85 mmHg during this time period.
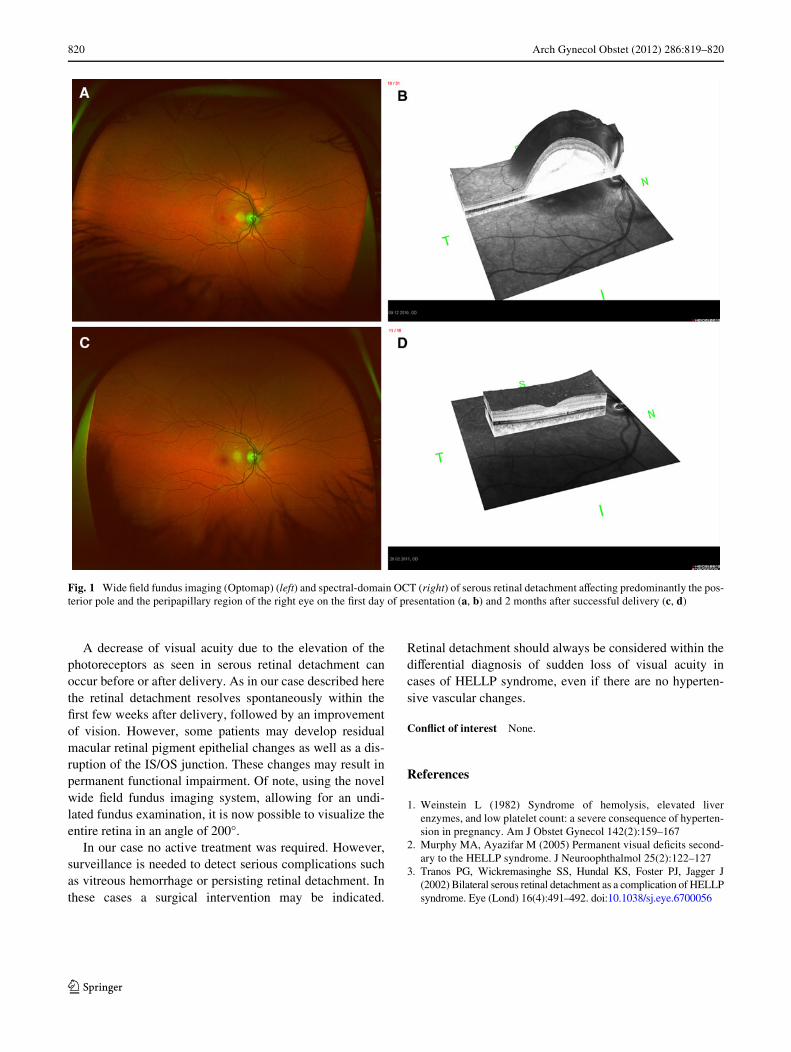
The ophthalmic follow-up examinations 7 days, 25 daysand 2 months later revealed an improvement of visual acu-ity on both eyes. At 2 months visual acuity had fully recov-ered and subretinal Xuid was reabsorbed. However, anirregularity of the retinal pigment epithelium was still pres-ent. In spectral-domain OCT the photoreceptor layerappeared normal on the right eye, whereas in the left eye adisrupted IS/OS-line (photoreceptor inner segment–outersegment junction) was recorded. Central retinal thicknesswas normal with 213 and 224 �m in the right and left eye,respectively (Fig. 1c, d).
The HELLP syndrome is characterized by upper abdom-inal pain, hemolysis, elevated serum liver enzymes, andlow platelets, and is usually associated with hypertension,proteinuria, and disseminated intravascular coagulation. Itwas Wrst described by Weinstein [1]. Patients suVering fromHELLP syndrome are typically multiparous white womenwith a mean age of 25 years. Clinical symptoms developduring the second or third trimester.
The pathogenesis of the HELLP syndrome is still underdiscussion. However, it is hypothesized that endothelialinjury leads to Wbrin deposition, causing activated platelets torelease vasoconstrictive substances, leading to platelet aggre-gation, and consumption at sites of endothelial damage [2].
From an ophthalmological point of view, retinal detach-ment is an unusual adverse event during pregnancy aVect-ing 0.2–2 % of patients with preeclampsia and 0.9 % ofpatients with HELLP syndrome. It occurs secondary to cho-roidal ischemia. Hypertensive changes can be observedduring Xuorescence angiography [3].
W. J. Mayer (&) · I. Hakim · M. W. Ulbig · M. Kernt · C. HaritoglouDepartment of Ophthalmology, Ludwig-Maximilians-University, Mathildenstr. 8, 80336 Munich, Germanye-mail: [email protected]
123
820 Arch Gynecol Obstet (2012) 286:819–820
A decrease of visual acuity due to the elevation of thephotoreceptors as seen in serous retinal detachment canoccur before or after delivery. As in our case described herethe retinal detachment resolves spontaneously within theWrst few weeks after delivery, followed by an improvementof vision. However, some patients may develop residualmacular retinal pigment epithelial changes as well as a dis-ruption of the IS/OS junction. These changes may result inpermanent functional impairment. Of note, using the novelwide Weld fundus imaging system, allowing for an undi-lated fundus examination, it is now possible to visualize theentire retina in an angle of 200°.
In our case no active treatment was required. However,surveillance is needed to detect serious complications suchas vitreous hemorrhage or persisting retinal detachment. Inthese cases a surgical intervention may be indicated.
Retinal detachment should always be considered within thediVerential diagnosis of sudden loss of visual acuity incases of HELLP syndrome, even if there are no hyperten-sive vascular changes.
ConXict of interest None.
References
1. Weinstein L (1982) Syndrome of hemolysis, elevated liverenzymes, and low platelet count: a severe consequence of hyperten-sion in pregnancy. Am J Obstet Gynecol 142(2):159–167
2. Murphy MA, Ayazifar M (2005) Permanent visual deWcits second-ary to the HELLP syndrome. J Neuroophthalmol 25(2):122–127
3. Tranos PG, Wickremasinghe SS, Hundal KS, Foster PJ, Jagger J(2002) Bilateral serous retinal detachment as a complication of HELLPsyndrome. Eye (Lond) 16(4):491–492. doi:10.1038/sj.eye.6700056
Fig. 1 Wide Weld fundus imaging (Optomap) (left) and spectral-domain OCT (right) of serous retinal detachment aVecting predominantly the pos-terior pole and the peripapillary region of the right eye on the Wrst day of presentation (a, b) and 2 months after successful delivery (c, d)
123