neurological emergencies - kyena.org · neurological emergencies ... spinal shock vs neurogenic...
TRANSCRIPT
NeurologicalEmergencies
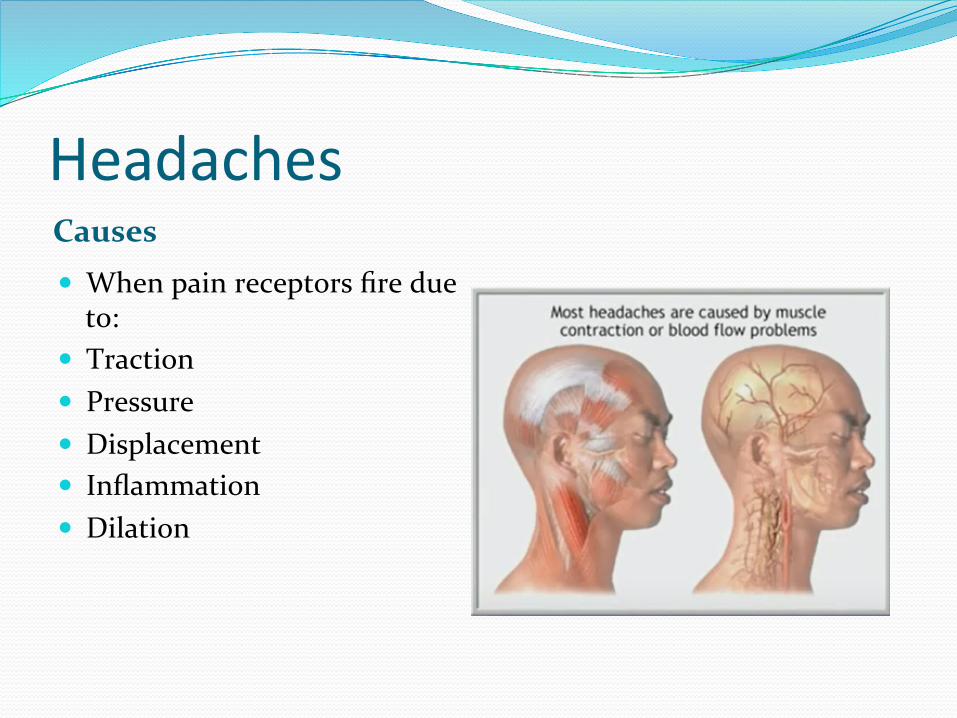
Headaches Causes � Whenpainreceptorsfiredueto:
� Traction� Pressure� Displacement� Inflammation� Dilation
Headachescont.PrimaryHA SecondaryHA� Noorganiccause� Includes:migraines,tension,cluster
� 50%oftheseareMigraines
� Associationw/anOrganiccause� Tumor� Aneurysm� Meningitis� TemporalArteritis
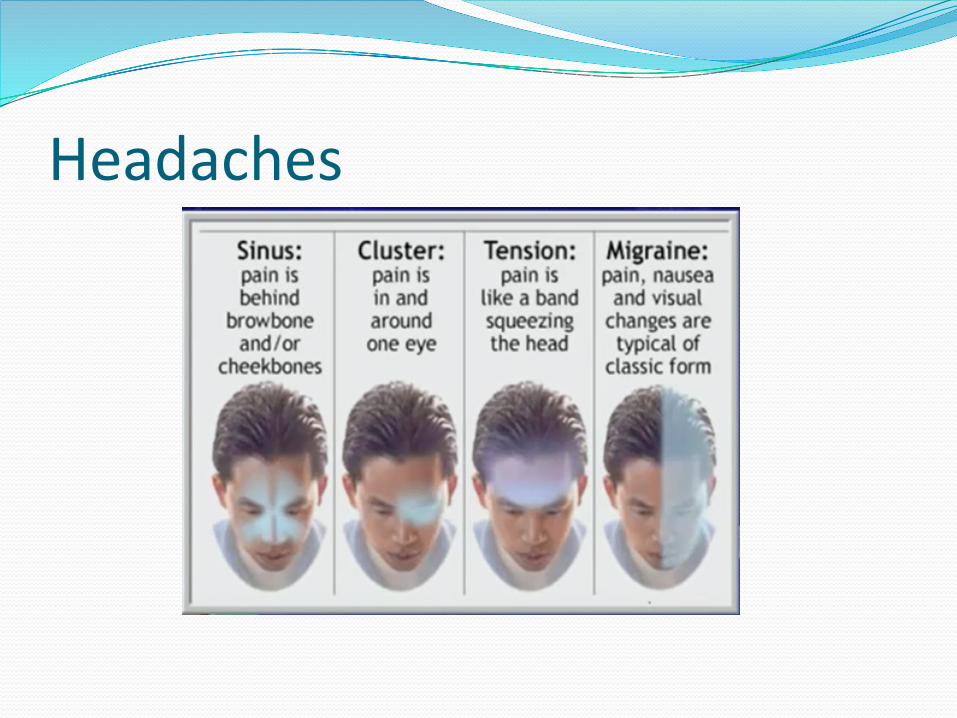
Headaches
Headaches RedFlags� SuddenOnset(Peaking<1min.)� ChangefrompriorHA� Concurrentevidenceofinfection� AlteredMentalStatus� Age>50(regardlessofpriorHA’s)� Immunosuppression� FocalNeurologicalDeficits� StiffNeck� ToxicAppearance
Migraines
� CanbewithorwithoutAura� Unilateral� Pulsating� AssociatedwithN&V� Photo/Phonophobia
TemporalArteri6sAKA“GiantCellArteritis”� InflammatoryProcess� Freq.assoc.w/lupus,RA,orInfections
� Unilateral,severepain,constant
� ClassicFinding:Tenderovertemporalartery
� Mayleadtoblindnessd/tbloodsupplytotheopticnerve
� Diagnostics:SedRate,Biopsyforconfirmation
� Tx:Highdosesteroids,analgesics,needvascular/neurologistconsultandadmit.
Headachescont.CTindications: LumbarPuncture� SuddenOnset� Onsetwithexertion/cough� FocalNeurologicalDeficits� StiffNeck� NewOnset� Immunocompromised� Changein“Usual”HApattern
� IfsuspectbleeddespitenormalCT
� Meningitis:cellcountelevated,decreaseinglucose
� Intra-cranialHTN:Cellcountnormal,proteinnormal
� SAH:Bloodinsubarachnoidspace
HeadachesInterventions Medications� Environmental
� Decreaselights/sounds� IVAccess
� FluidBolus� MedicationAdministration
� Ergots:(Imitrex)� MostUsefulwithinhoursofonset.Caution
withknownCAD.� Compazine
� Indicatedformigraine.� Givewithantihistaminetoreducedystonias
� Toradol� Cautioninrenalimpairment
� Zofran� Reglan
� PossDystonia,Sedation� Phenegran
� Movingawayfromit’suse.ConcernsaboutIVuse.Possiblyaddicting.
� Euphoriapossible� OpiateNarcotics
� Maskconditions.Freq.Narcoticuse.Causeshypotension,depressedLOC
StrokeInterruptioninvascularsupply
� Ischemic&HemorrhagicTypes� 50%ofallstrokesfatal� 50%ofsurvivorshavepermanentdeficits� ThirdleadingCauseofDeath
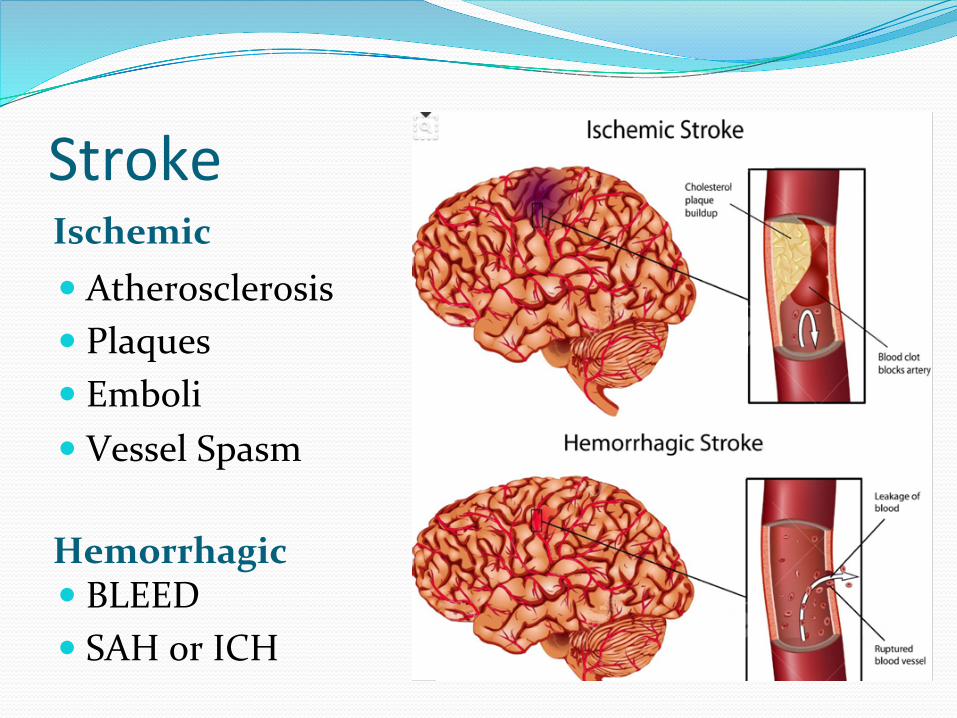
StrokeIschemic
Hemorrhagic
� Atherosclerosis� Plaques� Emboli� VesselSpasm
� BLEED� SAHorICH
CVAVS.TIAStroke/CVA
TIA
� NoO2� ClotintheBrainstoppingtheoxygen
� PERMANENT
� LowO2� Narrowbloodvessels
� Vasoconstriction� PlaqueSELF-LIMITING
Acutestrokeinyoungerpa6ents� Arterial
� Dissection(spontaneous,traumatic)� Fibromusculardysplasia,Marfan’s,vasculitis� Vasoactivedrugs:cocaine,amphetamines
� Paradoxicalcardiacembolus(PFO)� Hypercoagulablestates
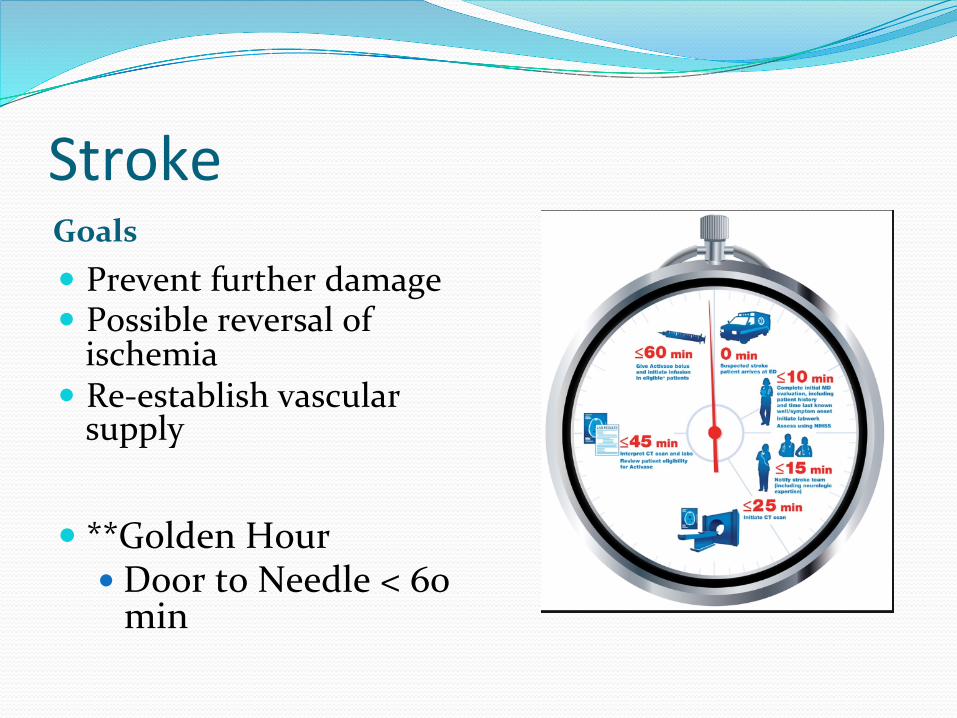
StrokeGoals� Preventfurtherdamage� Possiblereversalofischemia
� Re-establishvascularsupply
� **GoldenHour� DoortoNeedle<60min
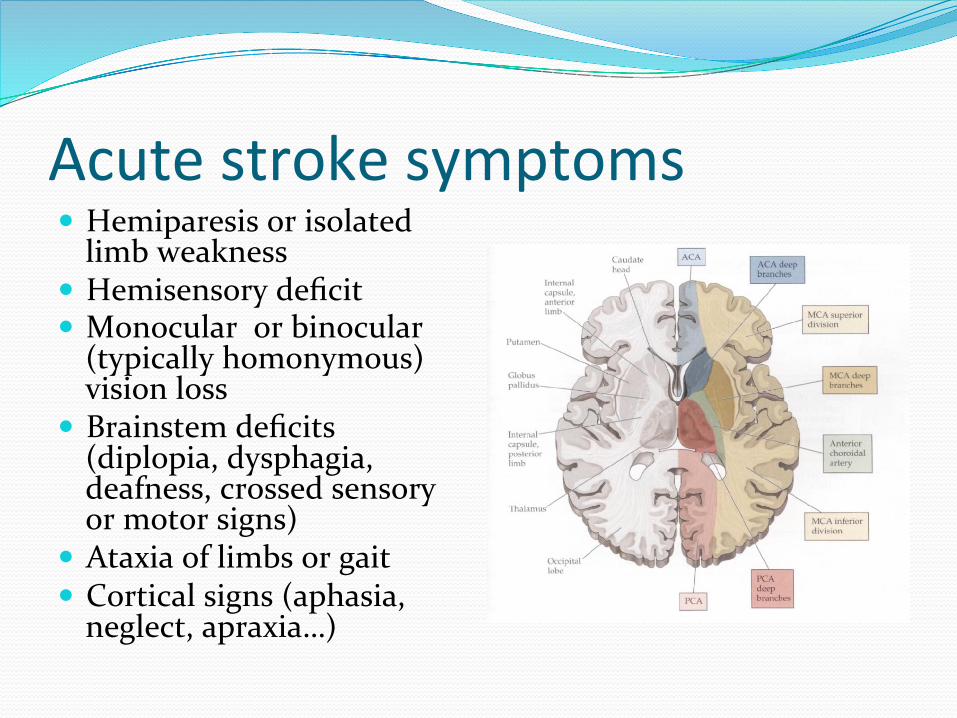
Acutestrokesymptoms� Hemiparesisorisolatedlimbweakness
� Hemisensorydeficit� Monocularorbinocular(typicallyhomonymous)visionloss
� Brainstemdeficits(diplopia,dysphagia,deafness,crossedsensoryormotorsigns)
� Ataxiaoflimbsorgait� Corticalsigns(aphasia,neglect,apraxia…)
StrokeInterventions
� GCS<8=intubate� Hi-flowO2� RapidIVaccess� Cautiousfluidadministration
� Position:HOBElev30-40degreesifnotcontra-indicated
StrokeMedications� RSI� Anti-hypertensives
� MaintainSBP<185� MaintainDBP<110
� Fibrinolytics� TPA,Alteplase� Ideallywithin3hrsofonset.Possiblyconsideredupto4-6hours.
� Givenasarapidbolus,therestover60min
� Mustmeetqualifyingcriteria� Considerrisk/benefitandfamilyconsultation.
Demen6a� OrganicDisorder� Decreasedcognitivefunction
� LOCremainsunchanged� Memorymostcommonlyaffected
Demen6aDisposition/Education
� Ifacutechangeornewonset:Admit.� Ifd/chome:Considerptsafetyinnormalenvironment.� Primarycarefollowupimportant.� Considerfamily’sabilitytocareforpt.
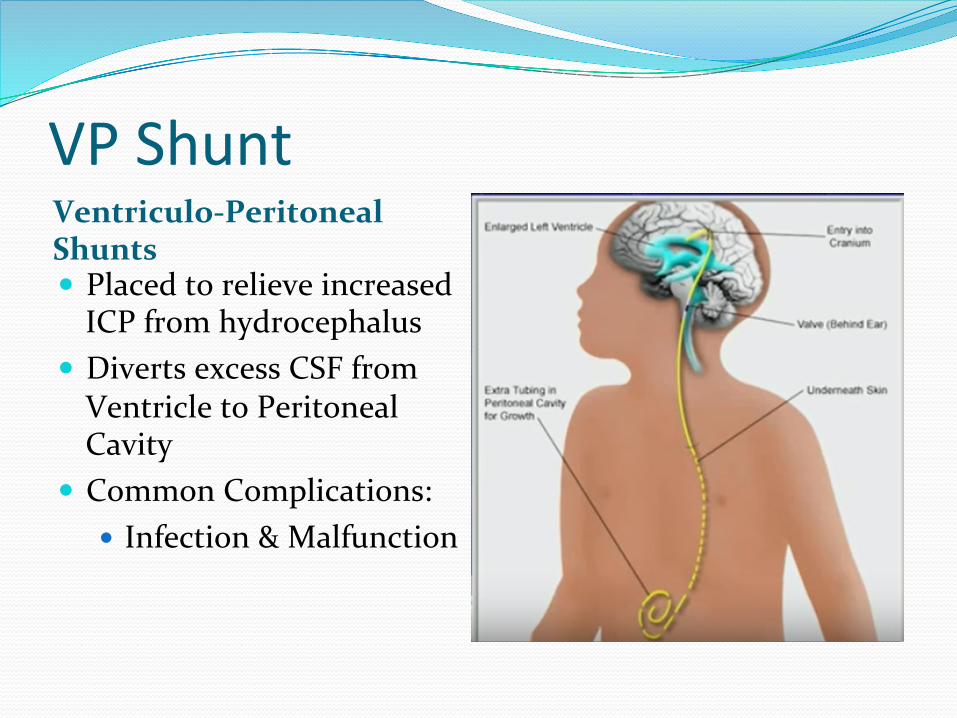
VPShuntVentriculo-PeritonealShunts� PlacedtorelieveincreasedICPfromhydrocephalus
� DivertsexcessCSFfromVentricletoPeritonealCavity
� CommonComplications:� Infection&Malfunction
VPShuntAssessment EXAM� Typeofshunt� Whenwasitplaced� Priorproblems� Reasonitwasplaced� Neurochanges� Fever� N&V
� LOC,Behavior,Lethargy,Inconsolable?
� Fever?� AbdomenDistended?� Fontanelles:TenseorBulging?
� Abdomen:Tender(Infection?)
VPShuntDiagnostics Interventions
� CBC(Infection)� Chemistries/Glucose� Xrays:ShuntSeries-Skull,CXR,KUB
� CTofHead,Abdomen� LP:Ifinfectionquestionable
� Carefulwithfluids� Antbiotics:Infection� Anti-emetics:N&V
SeizuresSuddenDischargeofNeuronalImpulses� Temporarilyimpairsmovement,sensation,orcognition
� WithorWithoutALossofConsciousness
SeizuresCauses AtRiskGroups
� Electrolyteimbalances� Metabolic(Fever,Hyperglycemia,Stress,Fatigue)
� NerveCellStructureChanges� Hypoxia� Tumors� Trauma
� HxofHeadInjury� Stroke� CNSInfection� DegenerativeCNSConditions
SeizuresSTATUSEPILEPTICUS� Aseriesofseizuresunrelenting� Diaphragm/Intercostalscan’t
relax� Emergencyduetoriskfor
Hypoxia� NeuronalDischargewill
continueaftertxbutbeMASKED
� NeuronalCellularChanges/DestructionwillContinue
� HighDosesofBenzosandNeuroleptics!!
� **NOPARALYTICS!
SeizuresPSEUDOSEIZURES
� Canbeinterruptedbyvocal/tactilestimuli� Characterizedbyabruptreturnofconsciousnesspossiblyfollowedby“LossofConsciousness”
� SuddenlossofTone� ButprotectiveMechanismsremainintact
SeizuresInterventions� SupportABC’s� SupplementalO2� PROTECTPATIENT
� STATUSEPILEPTICUS� SUCTIONPRN� RISKFORASPIRATION� RSIIFRESPIRATORYCOMPROMISE� IVACCESS� CARDIAC,PULSEOXMONITORING
29
Guillain-Barre Syndrome � An autoimmune attack of the peripheral nerve myelin. The
result is acute, rapid segmental demyelination of peripheral nerves and some cranial nerves, producing: � ascending weakness with dyskinesia (inability to execute
voluntary movements) � hyporeflexia (subnormal or absent reflexes) � paresthesias (numbness).
� Myelin is a complex substance that covers nerves, providing insulation and speeding the conduction of impulses from the cell body to the dendrites. It is produced by Schwann cells that are spared, allowing for remyelination in the recovery phase of the disease
30
Guillian Barre Syndrome � Causes
� Respiratory or gastrointestinal infection (Campylobacter jejuni) � Vaccination � Pregnancy � Surgery The antecedent event usually occurs 2 weeks before symptoms begin. Weakness usually begins in the legs and progresses upward for about 1 month.
Treatment� Telemetry� Respiratoryparameters� ICUmonitoring� Corticosteroidshavenotbeenshowntobebeneficial
� ExtremitySplinting
31
Intra-CranialPressure
� ManagingsecondaryproblemsrelatedtoincreasingICPisparamount
� ThegoalistomaintainaphysiologicalCerebralPerfusionPressure
� ManyheadinjuriescanleadtoIncreasingICP
Intra-CranialPressureCPP CPPCompensation� Pressureexertedtoperfusecerebraltissues
� Normal70-100MMHG� Calculated=MAP–ICP� IE:TheaverageSBPminustheresistance(ICP)
� CompensatoryMechanismsstrivetokeepCPPatPhysiologicallevels
� Initially,afairamountofchangeiscompensatedandtolerated
� Ascompensatoryresourcesaredepletedarapiddeclineoccurs
� InlateincreasingICP:smallchangesinpressurecancausebigchangesinvolume
KeepingICPDown� IncreasetheMAP
� Fluids� Blood� Pressors
� DecreasetheIntracranialVolume� Diuretics� ElevateHOB
� DecreaseVasodilation� CerebralIschemiacausesPHchanges
� IncreasingConcentrationsofCO2causesvasodialtion(BAD)
ICP&Hyperven6la6on???
� ItisnotHYPEROXYGENATION
� ItisanincreaseintheMINUTEVENTILATION
� ConsiderHyperventilationIfnoclinicalimprovementwith� Sedation� Diuretics� CSFDrainage� Positioning� MaintainNormothermia� Prevention/TxSeizures
ICPHerniationSyndrome� Whenvolumecan’tbecompensatedforanymore,riskofherniationoccurs.
� Herniationdirectlyaffectsbrainstem&Vitallifefunctions� Cranialnervefunctionsaffected
� LOC� Pupillary� Motor� VitalSignChanges
Cushing’sResponse/TriadIndicatesImpendingHerniationThreeclinicalCriteria
1. Hypertension2. Bradycardia
Somesaythethirdoneis….3.Irregularrespirations
Or3.WideningPulsePressure
Or3.PupillaryChanges
IncreasingICPEarlyFindings LateFindings� LOC,Behavior,Anxiety,Restlessness,Agitation
� Decreasingresponsiveness� SluggishPupillaryresponsetolight
� Motor:Pronatordrift,decreasingstrength
� Vitals:Occasionaltachycardia,someHTNseen
� Fixedordilatedpupils� Hemiparesis� Posturing
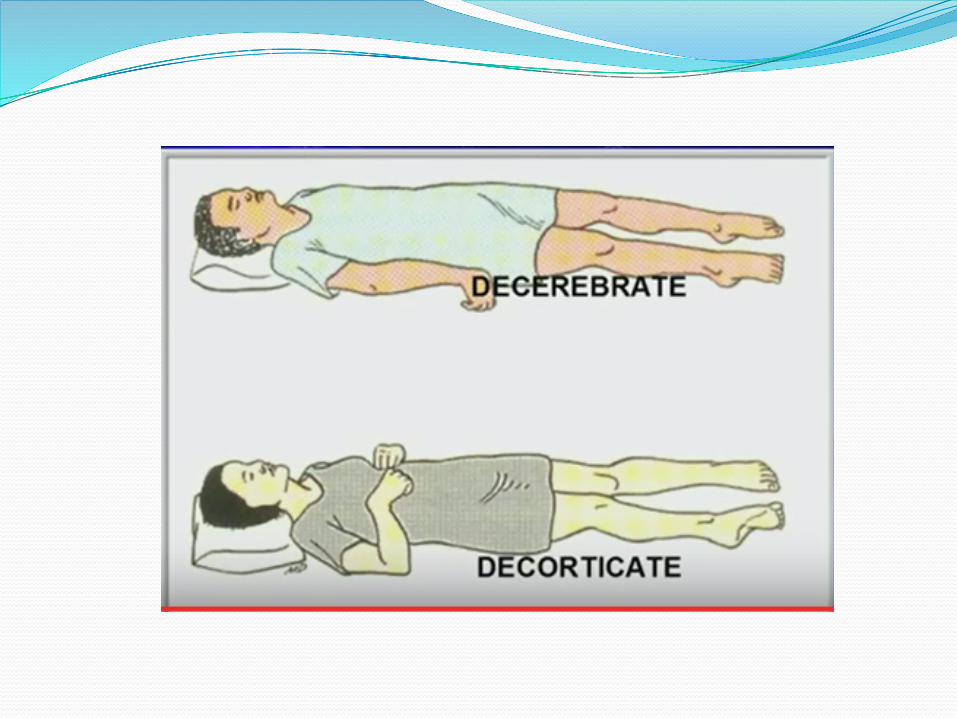
� Decerebrete� Decorticate
� Cushing’sresponse
SpinalCordInjuriesInsulttospinalcordresultinginachange,inthenormalmotor,sensoryorautonomicfunction.Thischangeiseithertemporaryorpermanent.
Mechanisms:i) Directtraumaii) Compressionbybonefragments/haematoma/
discmaterialiii) Ischemiafromdamage/impingementonthe
spinalarteries
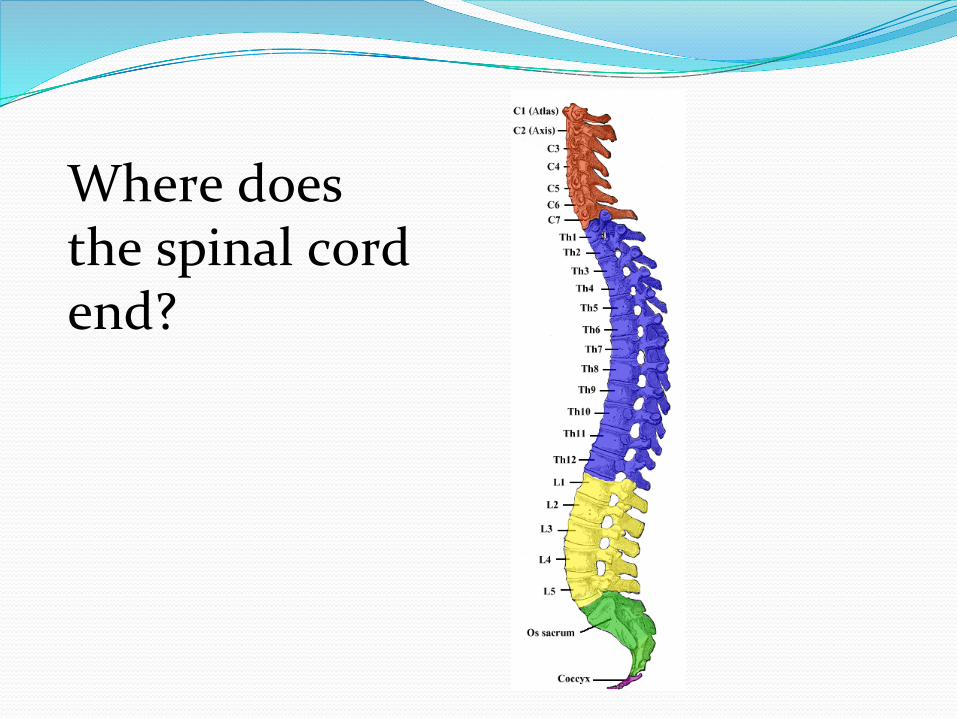
Wheredoesthespinalcordend?
31pairsofspinalnerves: 8cervical 12thoracic 5lumbar 5sacral 1coccygeal
SpinalCord
SpinalCordInjuryClassifica6onInjuryeither:1) Complete
2) Incomplete
Complete:i) Lossofvoluntarymovementofpartsinnervatedby
segment,thisisirreversibleii) Lossofsensationiii) Spinalshock
Incomplete:i) Somefunctionispresentbelowsiteofinjuryii) Morefavourableprognosisoveralliii) Arerecognisablepatternsofinjury,althoughthey
arerarelypureandvariationsoccur
InjurydefinedbyASIAImpairmentScaleASIA–AmericanSpinalInjuryAssociation:A–Complete:nosensoryormotorfunctionpreservedinsacralsegmentsS4–S5
B–Incomplete:sensory,butnomotorfunctioninsacralsegments
C–Incomplete:motorfunctionpreservedbelowlevelandpowergraded<3
D–Incomplete:motorfunctionpreservedbelowlevelandpowergraded3ormore
E–Normal:sensoryandmotorfunctionnormal
MuscleStrengthGrading:� 5–Normalstrength� 4–Fullrangeofmotion,butlessthan
normalstrengthagainstresistance� 3–Fullrangeofmotionagainstgravity� 2–Movementwithgravityeliminated� 1–Flickerofmovement� 0–Totalparalysis
SpinalShockvsNeurogenicShockSpinalShock:� Transientreflexdepressionofcordfunctionbelowlevelofinjury
� Initiallyhypertensionduetoreleaseofcatecholamines� Followedbyhypotension� Flaccidparalysis� Bowelandbladderinvolved� Sometimespriaprismdevelops� Symptomslastseveralhourstodays
Neurogenicshock:� Triadofi)hypotension ii)bradycardia iii)hypothermia
� MorecommonlyininjuriesaboveT6� SecondarytodisruptionofsympatheticoutflowfromT1–L2
� Lossofvasomotortone–poolingofblood� Lossofcardiacsympathetictone–bradycardia� Bloodpressurewillnotberestoredbyfluidinfusionalone
� Massivefluidadministrationmayleadtooverloadandpulmonaryedema
� Vasopressorsmaybeindicated� Atropineusedtotreatbradycardia
Typesofincompleteinjuriesi) CentralCordSyndrome
ii) AnteriorCordSyndrome
iii) PosteriorCordSyndrome
iv) Brown–SequardSyndrome
v) CaudaEquinaSyndrome
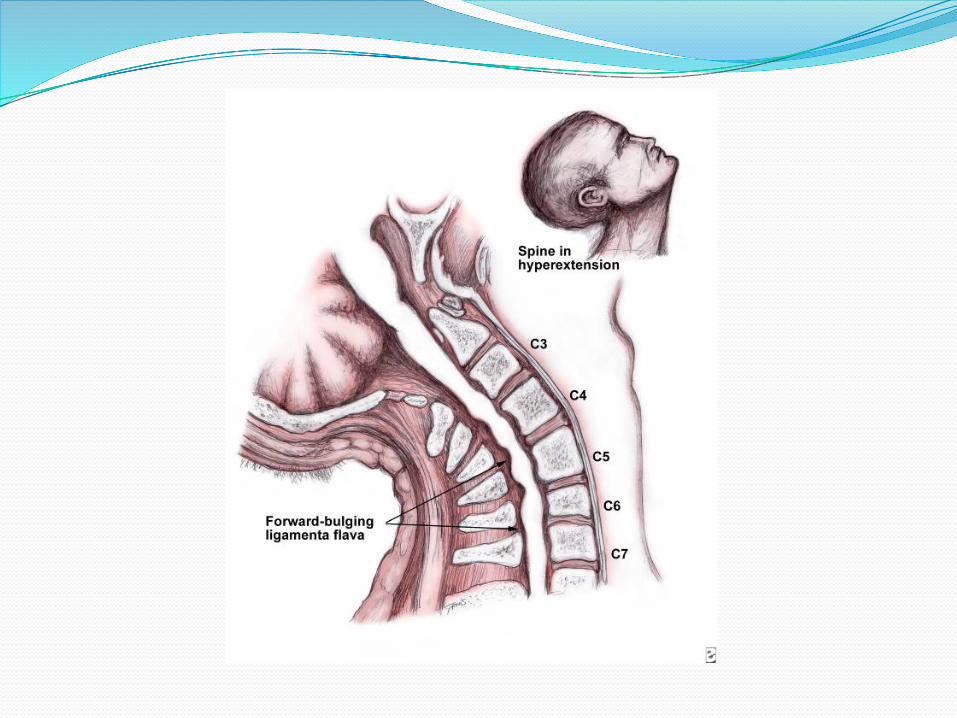
i) CentralCordSyndrome:� Typicallyinolderpatients� Hyperextensioninjury� Compressionofthecordanteriorlybyosteophytesand
posteriorlybyligamentumflavum
� Alsoassociatedwithfracturedislocationandcompressionfractures
� Morecentrallysituatedcervicaltractstendtobemoreinvolvedhenceflaccidweaknessofarms>legs
� Perianalsensation&somelowerextremitymovementandsensationmaybepreserved
ii)AnteriorCordSyndrome:� Duetoflexion/rotation� Anteriordislocation/compressionfractureofavertebralbodyencroachingtheventralcanal
� Corticospinalandspinothalamictractsaredamagedeitherbydirecttraumaorischemiaofbloodsupply(anteriorspinalarteries)
Clinically:� Lossofpower� Decreaseinpainandsensationbelowlesion� Dorsalcolumnsremainintact
ii)PosteriorCordSyndrome:Hyperextensioninjurieswithfracturesoftheposteriorelementsofthevertebrae Clinically:
� Proprioceptionaffected–ataxiaandfalteringgait� Usuallygoodpowerandsensation
iv)Brown–SequardSyndrome:� Hemi-sectionofthecord� Eitherduetopenetratinginjuries:i)stabwoundsii)gunshotwounds
� FracturesoflateralmassofvertebraeClinically:� Paralysisonaffectedside(corticospinal)� Lossofproprioceptionandfinediscrimination(dorsalcolumns)
� Painandtemperaturelossontheoppositesidebelowthelesion(spinothalamic)
v)CaudaEquinaSyndrome:� Duetobonycompressionordiscprotrusions
inlumbarorsacralregionClinically� Nonspecificsymptoms–backpain -bowelandbladderdysfunction -legnumbnessandweakness -saddleparesthesia
REVIEW
� Whichofthefollowingisanearlysignofincreasingintracranialpressureinapatientwithaheadinjury?
1. Bradycardiaandprematureventricularescapebeats2. Unilateralfixedanddilatedpupil3. Nausea&Vomiting4. Extensionofupperextremitieswithstimuli
Answer
� Whichofthefollowingisanearlysignofincreasingintracranialpressureinapatientwithaheadinjury?
1. Bradycardiaandprematureventricularescapebeats2. Unilateralfixedanddilatedpupil3. Nausea&Vomiting4. Extensionofupperextremitieswithstimuli
REVIEW
� Whichtypeofheadacheisassociatedwithhavinganaura,signalingthestartofaheadache?
1. Cluster2. Migraine3. Tension4. Temporalarteritis
Answer
� Whichtypeofheadacheisassociatedwithhavinganaura,signalingthestartofaheadache?
1. Cluster2. Migraine3. Tension4. Temporalarteritis
REVIEW
� Whencaringforapatientduringaclonic-tonicseizure,whichnursingactionhasthefirstpriority?
1. Establishandmaintainapatentairway2. Insertapaddedtonguebladebetweenthepatient’steeth3. Padthesiderails4. Administeroxygen
Answer
� Whencaringforapatientduringaclonic-tonicseizure,whichnursingactionhasthefirstpriority?
1. Establishandmaintainapatentairway2. Insertapaddedtonguebladebetweenthepatient’steeth3. Padthesiderails4. Administeroxygen
REVIEW
� Autonomicdysreflexiainspinalcordinjury(SCI)ischaracterizedbywhichofthefollowingsymptoms?
1. Pupillaryconstriction2. Tachycardia3. Hypertension4. Sweatingbelowthelevelofthelesion
Answer
� Autonomicdysreflexiainspinalcordinjury(SCI)ischaracterizedbywhichofthefollowingsymptoms?
1. Pupillaryconstriction2. Tachycardia3. Hypertension4. Sweatingbelowthelevelofthelesion
REVIEW
Anelderlypatienthasahistoryoffallingathomeandadeclineinmentationoverthelast2weeks.Thepatientisconfusedtotimeandlocation.Bloodglucoseis104mg/dL.Thenursewouldsuspecta(n):1. Diffuseaxonalinjury2. Subarachnoidhemorrhage3. Epiduralhematoma4. Subduralhematoma
Answer
Anelderlypatienthasahistoryoffallingathomeandadeclineinmentationoverthelast2weeks.Thepatientisconfusedtotimeandlocation.Bloodglucoseis104mg/dL.Thenursewouldsuspecta(n):1. Diffuseaxonalinjury2. Subarachnoidhemorrhage3. Epiduralhematoma4. Subduralhematoma
REVIEW
Apatientwithagunshotwoundtothebackisawakeandreportsthathehasfeelingtotherightsideofhisbody,butnottheleft,andcanmovehisleftside,butnottheright.Hisconditioniscalled:1. Anteriorcordsyndrome2. Brown-Sequardsyndrome3. Centralcordsyndrome4. Autonomicdysreflexia
Answer
Apatientwithagunshotwoundtothebackisawakeandreportsthathehasfeelingtotherightsideofhisbody,butnottheleft,andcanmovehisleftside,butnottheright.Hisconditioniscalled:1. Anteriorcordsyndrome2. Brown-Sequardsyndrome3. Centralcordsyndrome4. Autonomicdysreflexia