neuro-onc sig meeting venous thromboembolic events care strategies for the neuro-oncology patient
TRANSCRIPT

Neuro-Onc SIG Meeting
Venous Thromboembolic Events
Care Strategies for the Neuro-Oncology Patient
Neuro-Onc SIG Meeting
AgendaI. Introduction & WelcomeII. CEU Presentation:
Venous Thromboembolic EventsCare Strategies for the Neuro-Oncology
PatientIII. SIG Meeting

Venous Thromboembolic Events
Care Strategies for the Neuro-Oncology Patient
A Neu-Onc SIG CEU presentation
Mary Elizabeth Davis, RN, MSN, AOCNSClinical Nurse [email protected]
Venous Thromboembolic EventsVTE stats: • Includes PE and DVT• 3rd most common cardiovascular illness• Approx 1 million/year in US• 2/3 result from hospitalization: approx 300K die• PE - most common preventable cause of hospital
related death • 2nd leading cause of death in patients with active
cancer (possibly 1st)

Stats Specific for Glioma :• Semrad, et.al. (2007) -9489 malignant glioma pts
- 7.5% had VTE within first 6mos dx (55% within 2 months post-op) - Associated with poorer prognosis
- + VTE = 30% ↑ risk death within 2yrs
• Risk-3-60% first 6 wks after sx then 24% over life (Batchelor & Byrne, 2006, Jenkins, et. al, 2010, Marras, Geerts & Perry, 2000)

Specific for Glioma Proposed pathophysiology:
• Higher plasma levels of thrombosis associated biomarkers (D-dimer, lipoprotein A, VEGF, tissue plasminogen factor(tPA), PAI-1)
• Pathologic specimens: intra-lumen thrombosis common (distorted vasculature, increased interstitial pressure)
• Surgical resection make cause release of procoagulant microparticles into circulation & post-op immobility/ paresis may further contribute
Jenkins, et al., 2010, Sartori, et al,2011)

Consequences of VTE • Inpatient hospitalization• Interruption of cancer treatment• Need for pharmacologic management-
- chronic anticoagulation- financial burden- ↑ risk of bleeding
• ↑ risk of recurrent DVT (PTS)• ↓ QOL• ↓ survival
- likelihood of death 2-6x > for patients with cancer who have VTE

Risk of VTE• Active cancer Dx
• 4-7x > risk VTE than no Ca (Aikens, Rivey & Hansen, 2013)
• Hi risk Cas: Pancreatic, gastric, brain, myeloproliferative
• √ Malignant Gliomas
• Histology: Adeno > SCC
• Previous h/o DVT
• Metastatic Dx 2x > local disease
• N/A PBTs- rarely metastasize outside CNS
• ? Patient specific
• N/A, but …GBM 5x> other brain histology (such as AA, AO) (Brandes et al 1997)

Risk of VTE• Cancer treatment
• Surgical procedures• √ brain tumors
• ↑ risk surgery> 4 hours• Subtotal resection > total• Larger tumor size (5cm)
• Chemotherapy • √ high grade Gliomas • esp bevacizumab NCCN
• Glucocorticoids(Johannesdottir, et al, 2013)
• √ brain tumors
Risk Analysis- Chemotherapy Predictive model (Khorana et.al 2008)
5 clinical lab parameters- site of cancer- pre chemo plt ct > 350x109 /L- hgb < 10g/dL (or use ESA)- leukocyte ct > 11 x 109/L- BMI > 35kg/m2

• √ Gliomas –especially leg paresis; DVT more likely in paretic limb (Brandes, et al, 1997)
• Immobility
• ↑ incidence with ↑ age • √ GBM : peak incidence at 45-70 years
Risk of VTE
Other patient specific risks: • Cardiovascular risk factors: htn, DM, cigarette smoking, high cholesterol levels • Genetic risk factors: factor V Leiden, prothrombin gene mutation G20210A, protein C and S deficiency, and anti-thrombin deficiency
• Obesity • ? Patient specific
• CVC line• ESA (erythropoiesis
stimulating agent)
• Not usu applicable for Gliomas

Assessment/ DiagnosisS/S:• DVT “classic” calf pain,
redness, tenderness, swelling
• ** steroids may mask• Acute PE: dyspnea,
tachypnea, and pleuritic chest pain- also apprehension, cough, syncope, and tachycardia.
Dx: US, VQ scan, CXR, CT
Photo by Dr. James Heilman, used with permission
©2000 by Radiological Society of North America teaching slideSchoepf U J et al. Radiology 2000;217:693-700

Peri-Op Prophylaxis
• Ruff & Posner 1983; retrospective chart review-post-op glioma pts: elastic bandages verses external pneumatic compression; Incidence clots 25% vs 3%
• Frim et al, 1992: Neurosurgery regimen: compression boots and low dose heparin: adding heparin sig ↓ VTE
Mechanical compression
Photo by ME Davis, used by permission

• MacDonald, et al 2003: Unfractionated Heparin vs LMWH with pneumatic compression boots in craniotomy patients - No difference in intra-op blood loss, transfusion requirements or post-
op plts counts- No difference in post-op VTE events, hemorrhage or
thrombocytopenia
• Pan, Tsa & Mitchell, 2009 : retrospective review of 294 GBM pts with VTE – 2 % rate ICH: “the benefits of anticoagulation therapy may outweigh
the risk of ICH”
Peri-Op Prophylaxis
Ambulatory Prophylaxis•Vena Cava Filters
• prevention of PE for hi risk pts• Contraindication to anticoag• Filter does NOT prevent DVT
• Anticoagulation• PROTECHT (Prophylaxis of thromboembolism during
chemotherapy) Trial (Agnelli et al, 2009)
• SAVE-ONCO (Agnelli, et al 2011), FRAGEM (Marraveyas, et al 2012)
• PRODIGE (Prophylaxis Using Dalteparin in Glioblastoma Multiforme) Trial (Perry et al, 2010)
• Meta-analysis: Aikens, Rivey & Hansen, 2013

ProphylaxisASCO, 2007
• All hospitalized cancer patients should be considered for prophylaxis in the absence of bleeding or other comps.• Routine prophylaxis of ambulatory cancer pts is NOT recommended except pts on lenalidomide or thalidomide• Pts undergoing major surgery for malignant disease should be considered for pharmacologic prophylaxis

ProphylaxisNCCN Guidelines, 2013
• All surgical oncology pts receive pharmacologic VTE prophylaxis with or without mechanical prophylaxis for duration of hospitalization• if contraindications to anticoag- mechanical prophylaxis should be used;• High risk post op patients- extended duration of prophylaxis up to 4 weeks

Anticoagulation
• Unfractionated heparin (UFH)- converting to warfarin
• Low Molecular weight Heparin (LMWH) : – Dalteparin - Fragmin®– Enoxaparain - Lovenox®– Tinzaparin - Innohep®
• Factor Xa inhibitor: Fondaparinux- Arixtra®

Treatment VTEClot Trial Lee, et al, 2003
676 pts pt with active Ca and acute VTE randomized to either• LMWH (Dalteparin) 200 IU/kg/day x 1mo then ↓ 150 IU x
5months• LMWH (Dalteparin) 200 IU/kg x 5 days with transition to
oral warfarin
Results: LMWH only arm: 50% reduction in recurrent VTE (9 vs 17% p= .002) with no difference in rate of major bleeding (6% vs 4% p=.27)
• Results repeated and confirmed (Cochrane Review)
• NCCN guidelines recommend LMWH FIRST line for Ca pts
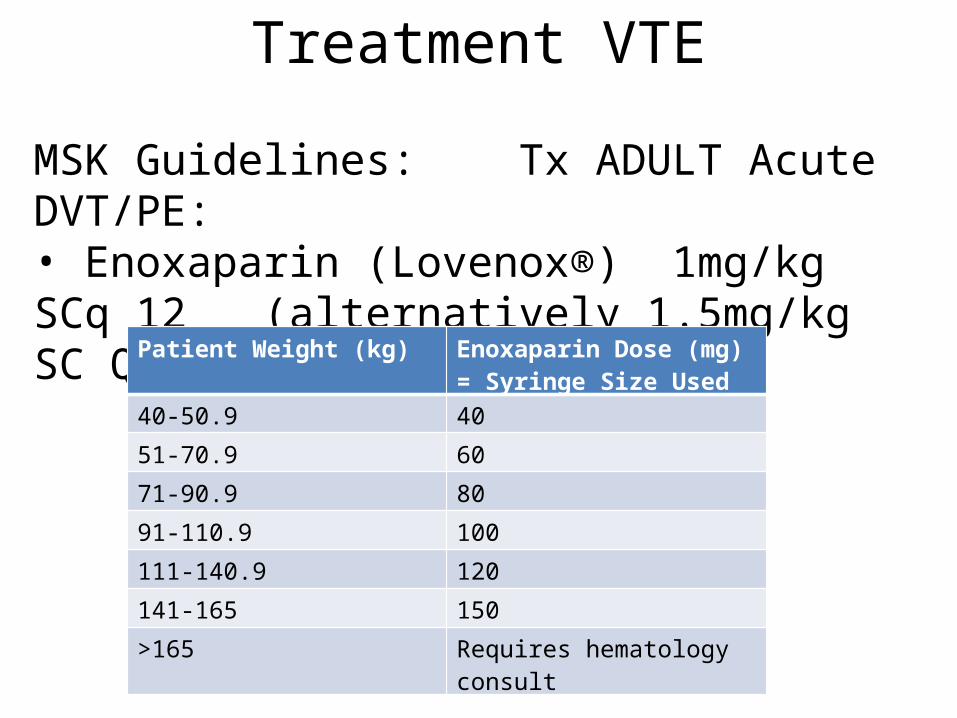
MSK Guidelines: Tx ADULT Acute DVT/PE: • Enoxaparin (Lovenox®) 1mg/kg SCq 12 (alternatively 1.5mg/kg SC QD)
Treatment VTE
Patient Weight (kg) Enoxaparin Dose (mg)= Syringe Size Used
40-50.9 40
51-70.9 60
71-90.9 80
91-110.9 100
111-140.9 120
141-165 150
>165 Requires hematology consult
Nsg Considerations- VTE• Pt/family education:
– Pt risk factors, s/s VTE– Promotion of activity as tolerated/ indicated– Medication indication, dose, schedule, SE, self care– Subcutaneous injection technique, needle disposal– When to call & S/S to report
• Monitor for SE, bleeding;– Special caution LMWH: renal insufficiency, obesity,
LBW/elderly <50kg– Antiangiogenic therapies

Anti-angiogenic therapy and Anticoagulation
Limited data- mainly retrospective reviews
• Nghiemphu, Green, Pope, Lai & Cloughesy, 2007• Norden, Bartolomeo at al, 2011
“Data raises concern about the risks of full anticoagulation in bevacizumab treated pts, however both VTE and bleeding are a known risk… (from gliomas) and whether or not anticoagulation increases this risk to a clinically significant degree has yet to be shown” (Perry, 2010, pg 595)

References• Agnelli, G., George, D.J., Kakkar, A.K. et al (1012) Semuloparin for thromboprophylaxis in
patients receiving chemotherapy for cancer NEJM 366, 601-9.• Agnelli, G., Gussoni, G., Bianchi, C et al, (2009) Nadroparin for the prevention of
thromboembolic events in ambulatory patients with metastatic or locally advanced solid cancer receiving chemotherapy: a randomised placebo-controlled double blind study. Lancet Oncology 10 ,943-949.
• Aikens, G.B., Rivey, M.P. & Hansen C.J. (2013) Primary Venous Thromboembolism Prophylaxis in ambulatory cancer patients The Annals of Pharmocology 47, 198-209
• Batchelor T.T. & Byrne, T.N. (2006) Supportive care of brain tumor patients. Hematol Oncol Clin N Am 20 , 1337-1361.
• Brandes, A.A., Scelzi, E., Salmistraro, G. et al (1997) Incidence of risk of thromboembolism during treatment high-grade gliomas: a prospective study. EurJ cancer33, (10) 1592-96.
• Frim, D.M., Barker, F.G., Poletti, C.E & Hamilton A. (1992) Postoperative low-dose heparin decreases thromboembolic complications in neurosurgical patients Neurosurgery 30 (6) 830-833.
• Jenkins , E.O., Schiff, D., Mackmanm N. & Key, N.S. (2010) Venous thromboembolism in malignant gliomas J Thromb Haemost 8 (2) 221-227.
• Khorana, A.A., Kuderer, NM., Culakova, E., Lyman, G.H.& Francis, C.W. (2007) Development and validation of a predictive model for chemotherapy associated thrombosis

• Lee, A.Y., Levine, M.N., Baker, R.I. et al (2003) Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. NEJM 10;349(2):146-53.• Lyman, G.H.,et.al (2007) American Society of Clinical Oncology Guideline: recommendations for Venous Thromboembolism Prophylaxis and treatment in patients with Cancer. JOC 25( 34) 5490-5505. • Maraveyas, A., Walters, J., Roy, R. et al (2012) Gemcitabine verses gemcitabine plus dalteparin thromboprophylaxis in pancreatic cancer Eur J Canc 48, 1283-92.• Marras, L.C Geerts, W.H, & Perry, J.R (2000) The risk of venous thromboembolism is increased throughout the course of malignant glioma: an evidence based review Cancer 89 (3) 640-6.• Nghiemphu, P.L., Green, R.M., Pope, W.B., Lai, A.,& Cloughesy, T.F (2008) Safety of anticoagulation use and bevacizumab in patients with glioma Neuro-oncology 10: 355-360.• Norden, A.D., Bartolomeo, J., Tanaka, S….& Wen, P.Y (2011) Safety of concurrent bevacizumab and anticoagulation in glioma patients J Neuroonc106; 121-125• Perry, J.R. (2010) Anticoagulation of malignant glioma patients in the era of novel antiangiogenic agents Current Opinions in Neurology 23: 592-596.
References

• Perry, J.R., Julian, J.A., Laperriere, N.J et al.,(2010)PRODIGE: a randomized placebo-controlled trial of dalteparin low molecular weight heparan thromboprophylaxis in patients with newly diagnosed malignant glioma J Thomb Haemost 8, 1959-65.
• Ruff, R. L. & Posner, J.B. (1983) Incidence and treatment of peripheral venous thrombosis in patients with glioma Annals of Neurology 13 (3) 334-336.
• Sartori, M.T. et al (2010) Prothrombotic state in glioblastoma multiforme: an evaluation of the procoagulant activity of circulating microparticles J Neuroncol doi 10.1007/z11060-010-0462-8
• Semrad , T.J., O’Donnell, R., Wun, T., Chew, H., Harvey, D., Zhou, H & White, R. (2007) Epidemiology of venous thromboembolism in 9489 patients with malignant glioma J Neurosurg 106:601–608,
• Streiff, M.B (2011) Anticoagulation in the management of venous thromboembolism in the cancer patient J Thromb Thrombolysis 31; 282-294.
References

Thank you!
Any Questions?

Neuro-Onc SIG MeetingAgenda
I. Introduction & WelcomeII. CEU Presentation: Venous Thromboembolic Events: Care Strategies for the Neuro-Onc PatientIII. Volunteer to take minutes:IV. Call to order:V. Minutes from previous meeting: (Next slide)VI. Approval of Minutes VII. Discuss Sig Goals/Objectives:VIII. SIG Survey Questions:
• Writing, presentations, leadership, mentoring• Virtual CME? • Do you get the newsletter/read it?• Ideas for Newsletter topics??• would like to get involved(leave name/ email)
VIX. Burning Clinical Questions/discussion