neonatal early onset sepsis - frann.org · • 10 to 100-fold drop in early onset sepsis rate:...
TRANSCRIPT
2/15/2018
1
Neonatal Early Onset SepsisRisk based approach to management
Anette Kunig, MD
February 6, 2018
Neonatal Early Onset Sepsis (EOS)
• Definition
• Invasive bacterial infection of the blood and/or CSF within the first week after birth
• Pathogenesis
• Normal GI and GU flora
• Ascending colonization maternal genital tract and uterus
• Colonization and infection of the fetus/newborn
• Presentation
• Sick infant requiring respiratory and/or hemodynamic support
• Nonspecific signs also associated with normal transition to extrauterine life
2/15/2018
2
Neonatal SepsisMajor Advances Over Last 30 Years
Primarily Driven OB/GYN Innovations
• Advances
• Prenatal
• CDC: Universal GBS carrier ID
• CDC: Aggressive intrapartum antibiotic prophylaxis and chorioamnionitistreatment
• Postnatal
• Improved management of sick neonates
• Effects
• 10 to 100-fold drop in early onset sepsis rate: currently 3/10,000
• 2 to 20-fold drop in sepsis mortality: currently as low as 2% in term babies
February 15, 2018 3
Benitz 2015, Schrag 2000, Bromberger 2000, Escobar 2014, Braun 2015
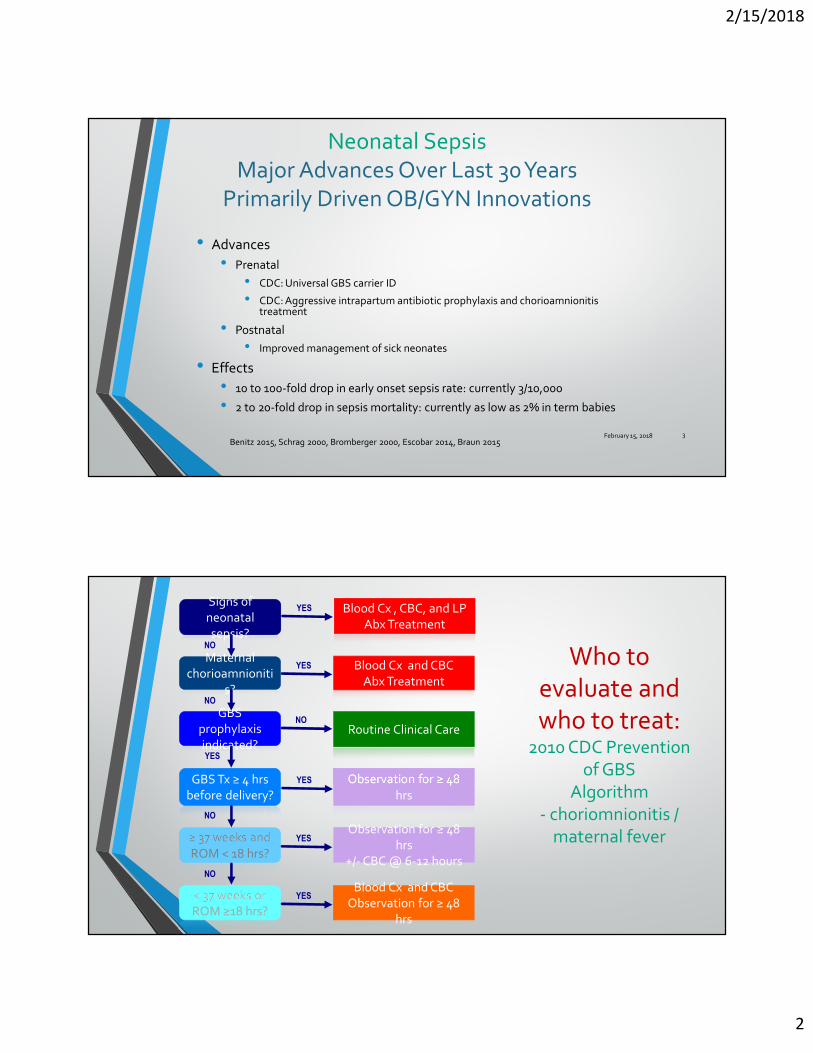
Signs of neonatal sepsis?
Blood Cx , CBC, and LPAbx Treatment
Maternal chorioamnioniti
s?
Blood Cx and CBCAbx Treatment
Observation for ≥ 48 hrs
Observation for ≥ 48 hrs
+/- CBC @ 6-12 hours
Blood Cx and CBCObservation for ≥ 48
hrs
< 37 weeks orROM ≥18 hrs?
Routine Clinical Care
≥ 37 weeks andROM < 18 hrs?
GBS prophylaxis indicated?
GBS Tx ≥ 4 hrsbefore delivery?
YES
YES
YES
NO
YES
YES
NO
NO
NO
YES
NO
Who to evaluate and who to treat:
2010 CDC Prevention of GBS
Algorithm- choriomnionitis /
maternal fever
2/15/2018
3
Critique of CDC recommendations
• Good:
• Prenatal management
• Large reduction in incidence of EOS
• Not so good:
• Expert opinion, not efficacy studies
• Based on prevention of neonatal group B strep sepsis only
• Identification of carriers
• Intrapartum antibiotic prophylaxis
5
Critique of CDC recommendations
• Not so good
• Based on data prior to 2002
• No change between 2002 and 2010 in CDC recommendation
• Before widespread use of intrapartum antibiotic prophylaxis
• EOS risk 5-10 fold higher
• Decreased incidence of sepsis
• More data on poor positive predictive value of CBC
• Large number infants being evaluated for sepsis, 15-20%
• Large number infants receiving empiric antibiotics, 5-8%

2/15/2018
4
Critique of CDC recommendations
• Don’t account for newborns clinical presentation
• Newer algorithms developed for evaluation and treatment of at-risk infants
• Well, equivocal, and clinically ill
• Reduction in evaluation and treatment
• Persistent high rates of treatment in a setting where the incidence of EOS is decreased
Imbalance between Infection and Sepsis Evaluation / Antibiotic Treatment
EOS incidence
0.3/1000 Live Births
Blood Cultures 14.4%
Antibiotics 5%
Data from KPNC
2010-2012
Disturbed maternal bonding
Disturbed microbiome
2/15/2018
5
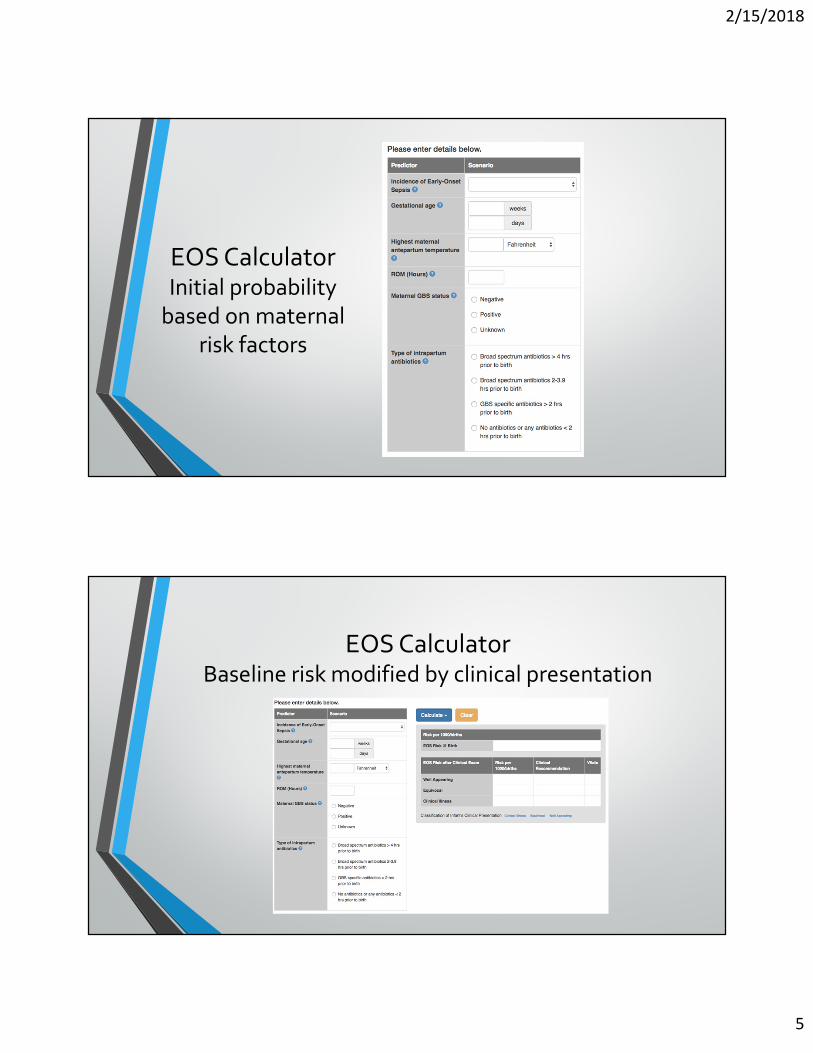
EOS CalculatorInitial probability
based on maternal risk factors
EOS CalculatorBaseline risk modified by clinical presentation
2/15/2018
6
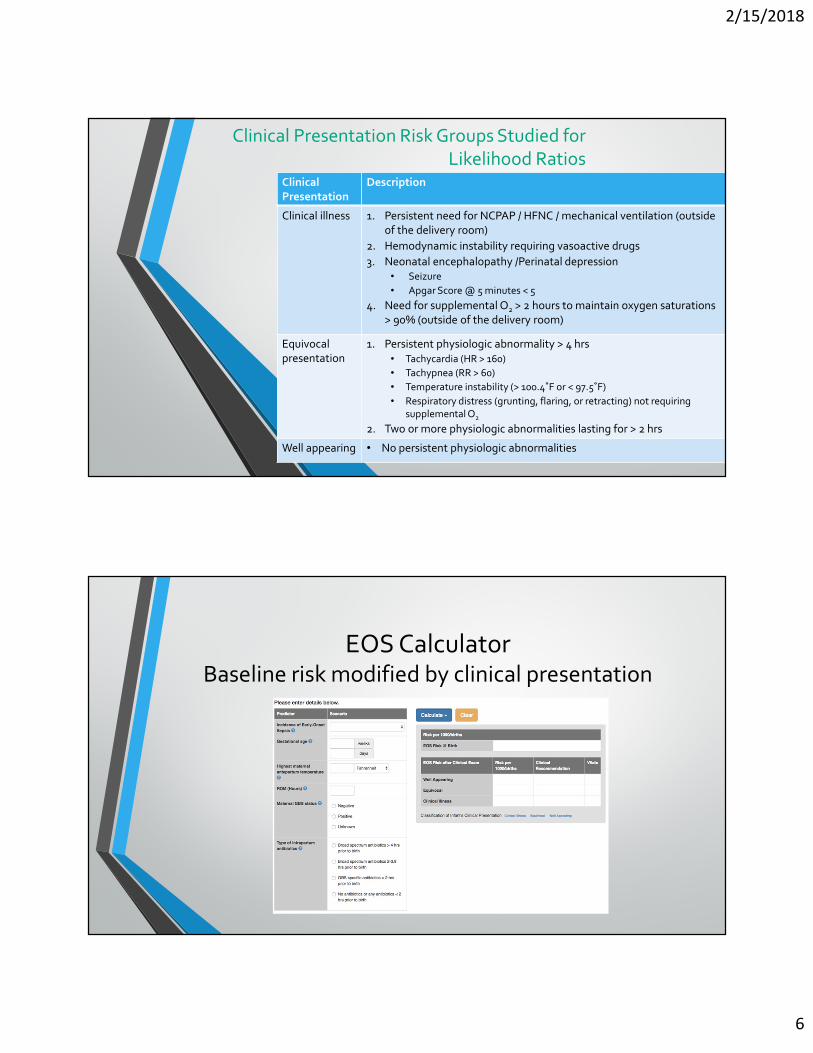
Clinical Presentation Risk Groups Studied for Likelihood Ratios
Clinical
Presentation
Description
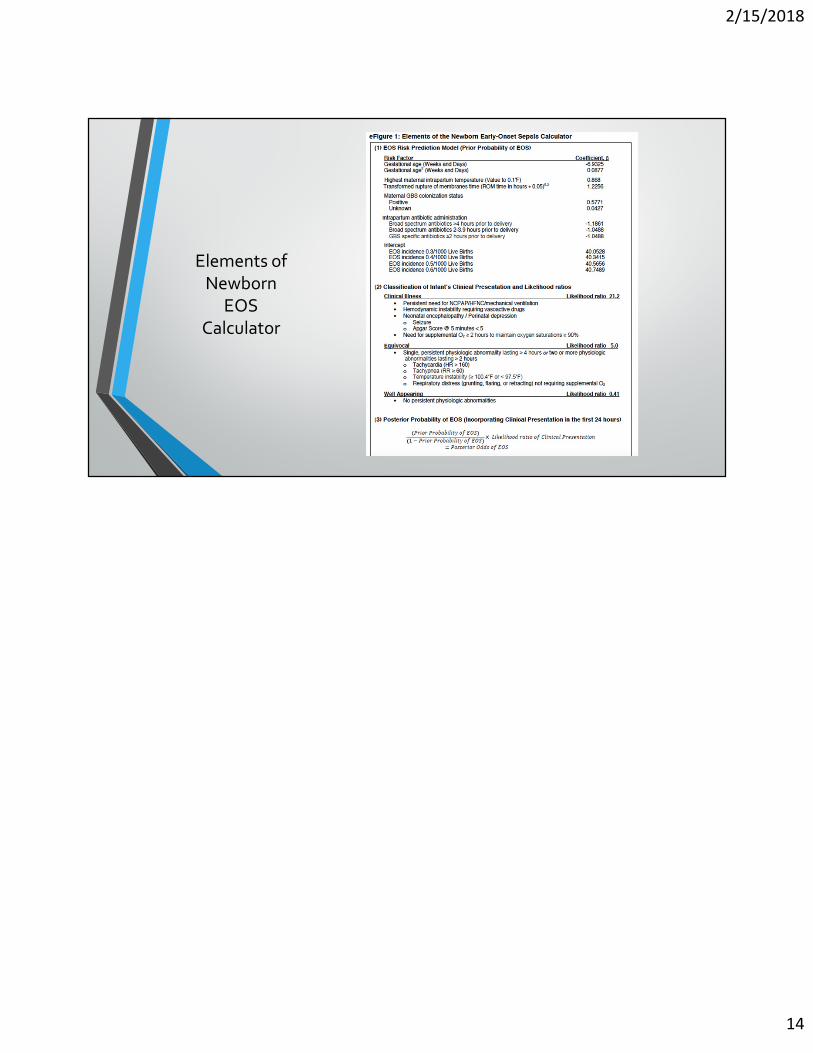
Clinical illness 1. Persistent need for NCPAP / HFNC / mechanical ventilation (outside of the delivery room)
2. Hemodynamic instability requiring vasoactive drugs
3. Neonatal encephalopathy /Perinatal depression• Seizure
• Apgar Score @ 5 minutes < 5
4. Need for supplemental O2 > 2 hours to maintain oxygen saturations > 90% (outside of the delivery room)
Equivocalpresentation
1. Persistent physiologic abnormality > 4 hrs
• Tachycardia (HR > 160)
• Tachypnea (RR > 60)
• Temperature instability (> 100.4˚F or < 97.5˚F)
• Respiratory distress (grunting, flaring, or retracting) not requiring supplemental O2
2. Two or more physiologic abnormalities lasting for > 2 hrs
Well appearing • No persistent physiologic abnormalities
EOS CalculatorBaseline risk modified by clinical presentation
2/15/2018
7
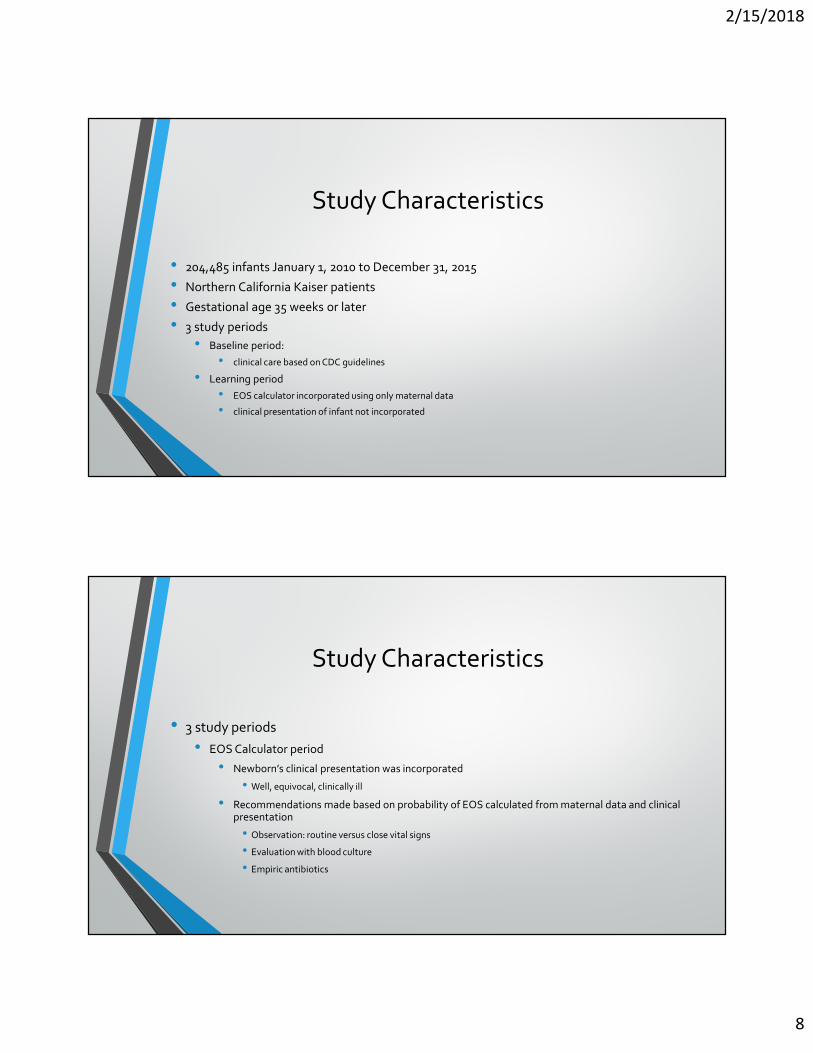
Implementing the EOS Calculator and applying recommendations based on risk
EOS risk
(per 1000)
Intervention Observation Location
<0.4 none routine FCC
0.4-0.9 none Q4h x 24h FCC
1-3 Blood culture Q4h x 24h FCC
>3 Antibiotics and Blood culture
Per NICU NICU
SET TREATMENT THRESHOLDS
Clinical recommendations for evaluation and treatment
2/15/2018
8
Study Characteristics
• 204,485 infants January 1, 2010 to December 31, 2015
• Northern California Kaiser patients
• Gestational age 35 weeks or later
• 3 study periods
• Baseline period:
• clinical care based on CDC guidelines
• Learning period
• EOS calculator incorporated using only maternal data
• clinical presentation of infant not incorporated
Study Characteristics
• 3 study periods
• EOS Calculator period
• Newborn’s clinical presentation was incorporated
• Well, equivocal, clinically ill
• Recommendations made based on probability of EOS calculated from maternal data and clinical presentation
• Observation: routine versus close vital signs
• Evaluation with blood culture
• Empiric antibiotics
2/15/2018
9
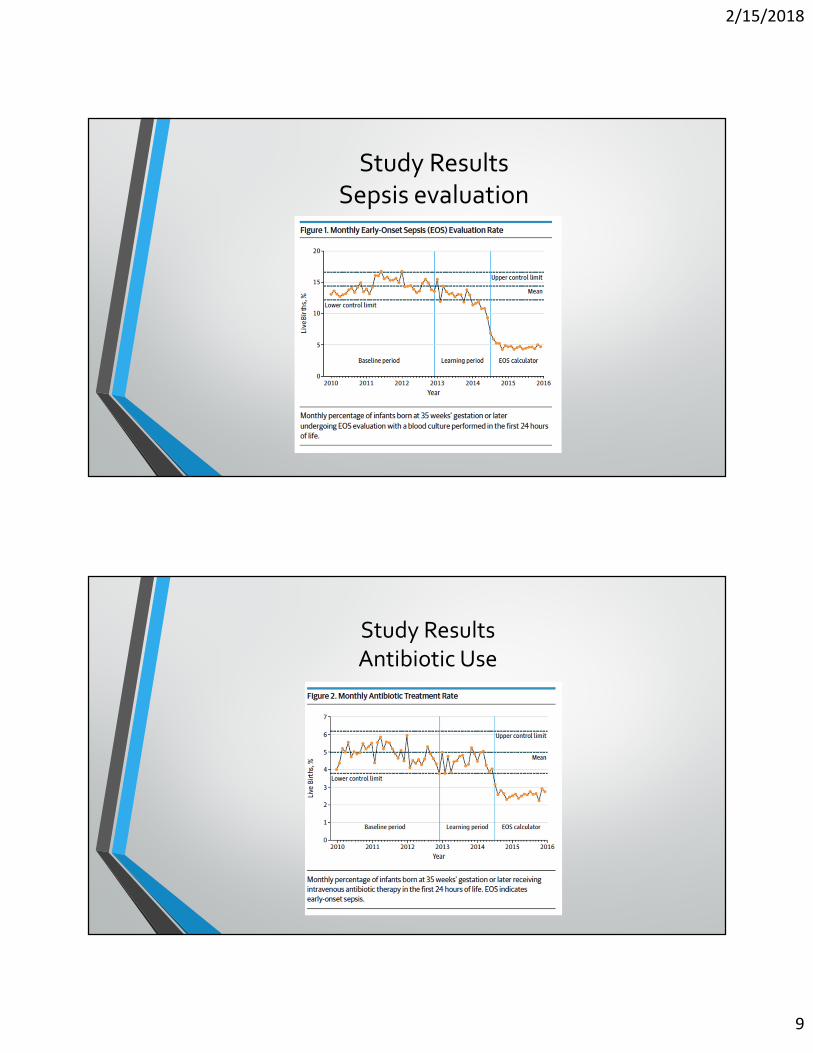
Study ResultsSepsis evaluation
Study ResultsAntibiotic Use
2/15/2018
10
Study Results
• No increase in EOS between the baseline period and the EOS calculator period
• Infants with sepsis are not being missed by decreasing rates evaluation and treatment
• No increase in antibiotic usage over 24-72 hour across all study periods
• Antibiotics weren’t being delayed until infants showed signs of illness
Conclusions
• CDC guidelines have greatly reduced the incidence of EOS
• Developed prior to widespread use of intrapartum antibiotics
• Empiric antibiotics for all newborns with maternal chorio ( temperature >38C) regardless of clinical condition
• imbalance between the incidence of EOS and percentage of infants having sepsis evaluations or receiving antibiotics
• EOS calculator uses clinical appearance of infant to stratify maternal risk factors
• Decreases sepsis evaluations
2/15/2018
11
Conclusions
• Decreases empiric antibiotic use
• Asthma, autoimmune disorders, obesity
• No difference in antibiotics use at 24-72 hours
• No increase in early onset sepsis (positive cultures within first 7 days)
Limitations
• Larger studies needed to evaluate safety of delaying antibiotic treatment until infant becomes symptomatic
• no adverse events seen in study
• Scenario is uncommon
• Risk of delaying treatment weighed against treating large number infants unnecessarily
• Prior probability EOS in various insitutions may differ from what was used in this study
• Risk threshold for clinical interventions can be adjusted based on center characteristics
• Lower risk threshold in centers with poor prenatal care, low rates of GBS screening, lack of peds follow up, etc
2/15/2018
12
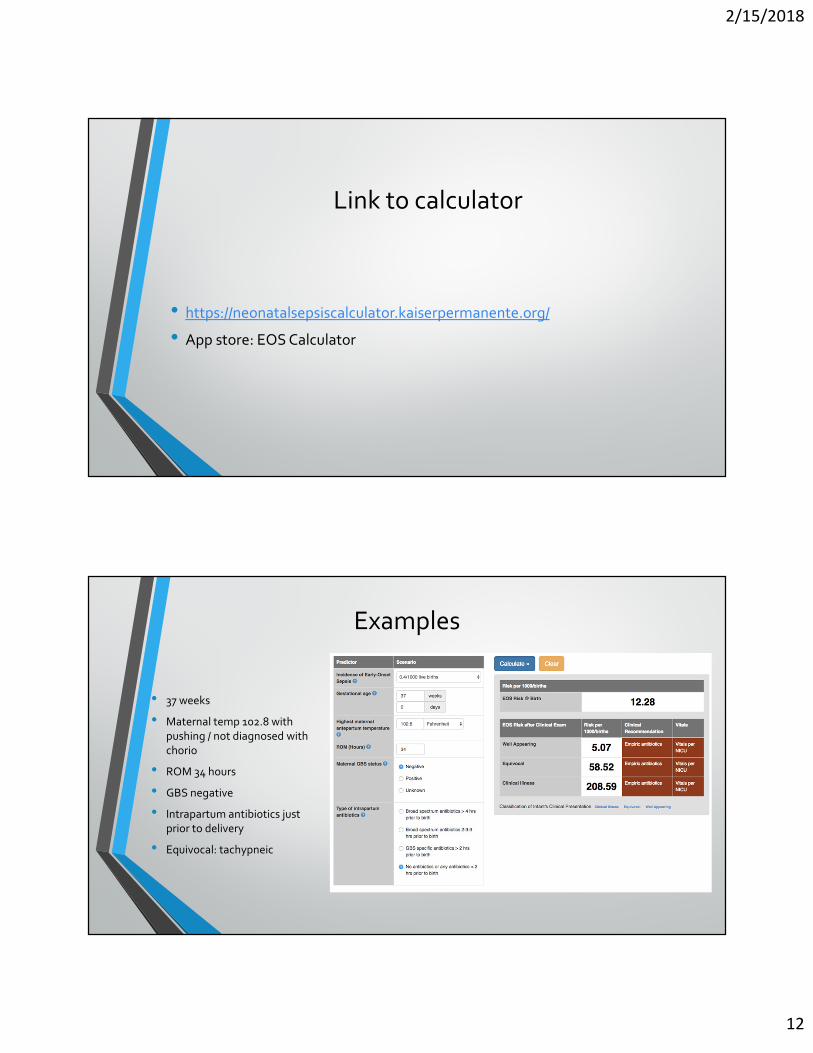
Link to calculator
• https://neonatalsepsiscalculator.kaiserpermanente.org/
• App store: EOS Calculator
Examples
• 37 weeks
• Maternal temp 102.8 with pushing / not diagnosed with chorio
• ROM 34 hours
• GBS negative
• Intrapartum antibiotics just prior to delivery
• Equivocal: tachypneic
2/15/2018
13
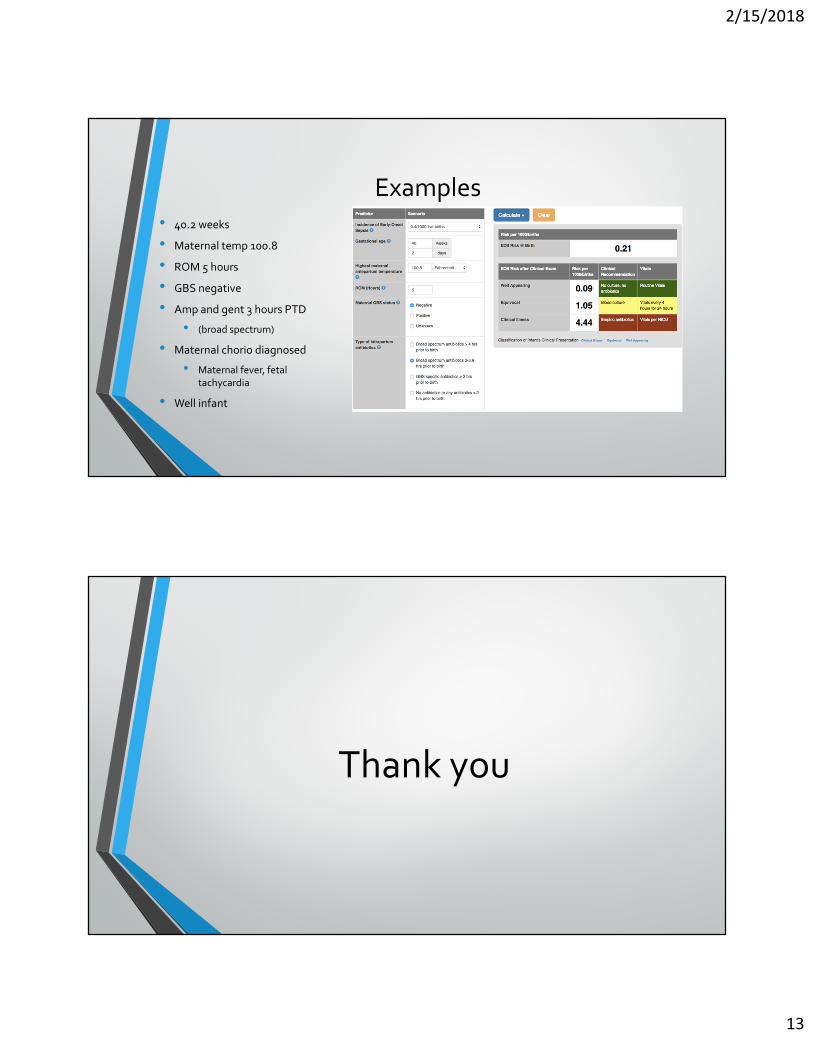
Examples
• 40.2 weeks
• Maternal temp 100.8
• ROM 5 hours
• GBS negative
• Amp and gent 3 hours PTD
• (broad spectrum)
• Maternal chorio diagnosed
• Maternal fever, fetal tachycardia
• Well infant
Thank you
2/15/2018
14
Elements of Newborn
EOS Calculator