natriuretic peptides & troponin - baptist health collegeuserfiles/pdfs/natriuretic peptides...
TRANSCRIPT
3/30/2016
1
Theresa JosephMedical Scientific Liaison
Roche Diagnostics
Natriuretic Peptides & Troponin:Testing Today
1
• Your Name Here is an employee of Roche Diagnostics within the division of Medical Scientific Affairs.
• Data presented is intended for purely educational use to provide the participant with scientific, evidenced-based data in compliance with FDA guidelines.
All Trademarks, trade names, images, or logos mentioned or used herein are the property of their respective owners and are not used for purposes of promotion or as an indication of affiliation with
the provider of any particular good or service.
Disclosures
2
Program Description
• This program is intended to familiarize health professionals and laboratorians with data supporting evidenced-based practice guidelines related to care of the patient with Acute Coronary Syndrome and/or Heart Failure.
• The Focus will be on diagnostic and prognostic value of troponin & natriuretic peptides.
3
• Describe the biochemical and physiological effects of the
cardiac natriuretic peptide and troponin system.
• Identify biological and physiological factors for
consideration in the clinical application of natriuretic
peptide and troponin measurements in acute and chronic
disease settings
• Analyze evidenced-based clinical outcome data related to
the diagnostic and prognostic impact of natriuretic peptide
and troponin use in primary and acute care settings
Objectives
4
Biology of the NP SystemSynthesis and Release
pre-proBNP 1-134
Meprin ABNP7-32
DPP-IVBNP3-32
proBNP 1-108
BNP1-32NT-proBNP 1-76
proBNP 1-108
Signal peptide(26 amino acids)
Kim & Januzzi. 2011. Circulation;123(18), 2015-2019
5
B-Type Natriuretic Peptides
Characteristics BNP NT-proBNP
Size 32 Amino acids (AA) 76 AA
Half-life 20 minutes 60-120 minutes
StabilityUp to 4 hrs at room
temp.
Up to 3 days at room
temp.
ClearanceNP Receptor-C,
Endopeptidases, kidneyUnclear, possibly kidney
EMCREG International Newsletter, Dec. 2005, Vol. 6
Characteristic
6
3/30/2016
2
Natriuretic Peptides: Influences from cardiovascular/renal dysfunction, age, BMI
7
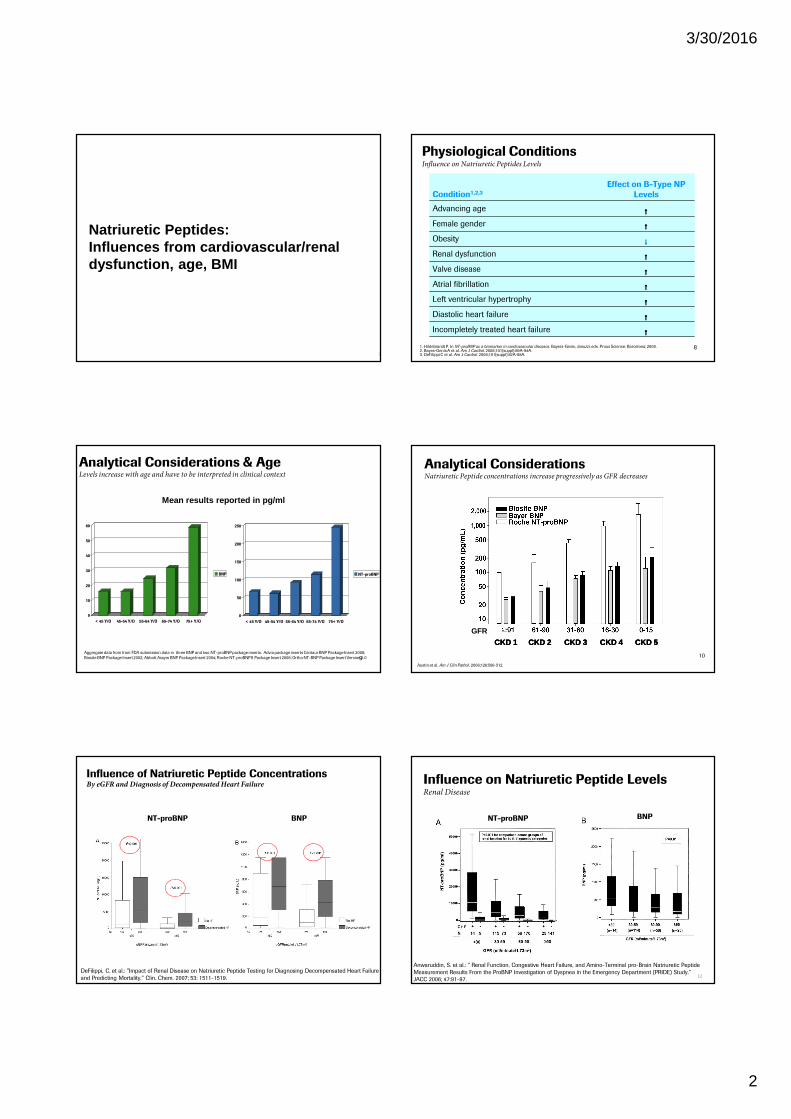
Physiological ConditionsInfluence on Natriuretic Peptides Levels
Condition1,2,3
Effect on B-Type NP
Levels
Advancing age ↑↑↑↑Female gender ↑↑↑↑Obesity ↓↓↓↓Renal dysfunction ↑↑↑↑Valve disease ↑↑↑↑Atrial fibrillation ↑↑↑↑Left ventricular hypertrophy ↑↑↑↑Diastolic heart failure ↑↑↑↑Incompletely treated heart failure ↑↑↑↑
1. Hildebrandt P. In NT-proBNP as a biomarker in cardiovascular diseases. Bayers-Genis, Januzzi, eds. Prous Science: Barcelona; 2008. 2. Bayes-GenisA et al. Am J Cardiol. 2008;101(suppl):89A-94A. 3. DeFilippi C et al. Am J Cardiol. 2008;101(suppl):82A-88A.
8
0
10
20
30
40
50
60
< 45 Y/O 45-54 Y/O 55-64 Y/O 65-74 Y/O 75+ Y/O
BNP
Analytical Considerations & Age Levels increase with age and have to be interpreted in clinical context
0
50
100
150
200
250
< 45 Y/O 45-54 Y/O 55-64 Y/O 65-74 Y/O 75+ Y/O
NT-proBNP
Mean results reported in pg/ml
Aggregate data from from FDA submission data in three BNP and two NT-proBNP package inserts. Advia package inserts Centaur BNP Package Insert 2008;
Biosite BNP Package Insert 2002; Abbott Axsym BNP Package Insert 2004; Roche NT-proBNP II Package Insert 2008; Ortho NT-BNP Package Insert Version 1.0 9
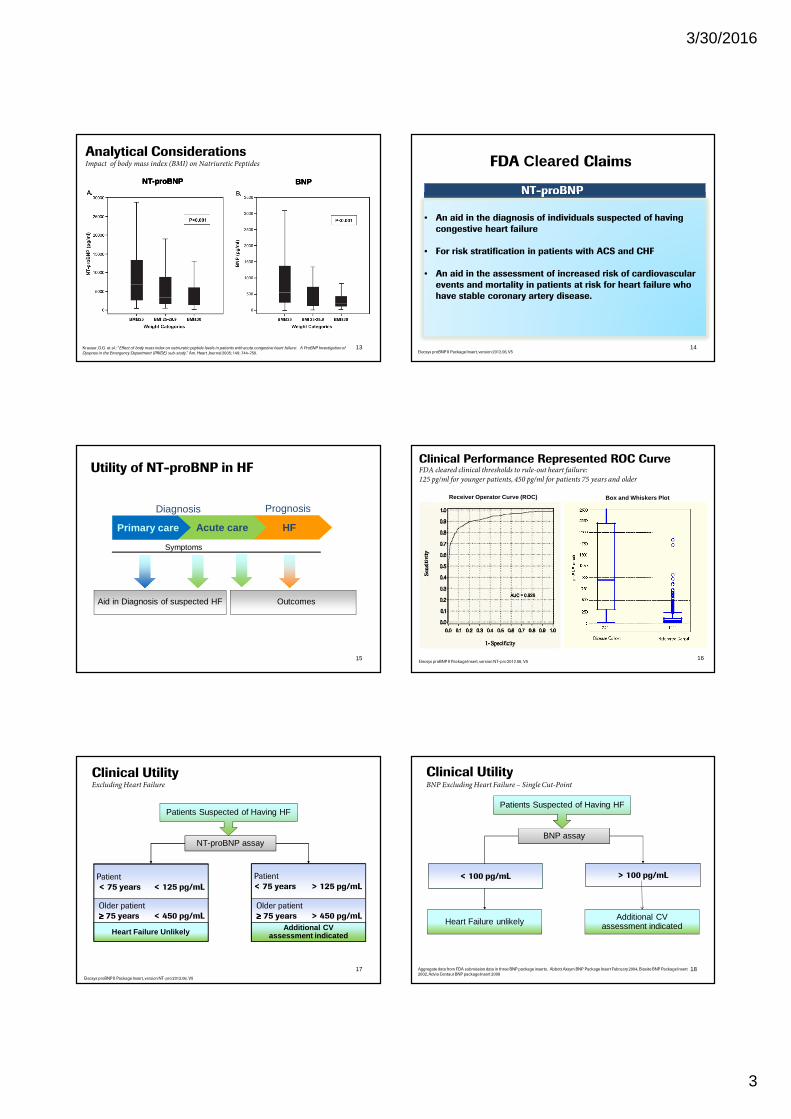
Analytical Considerations Natriuretic Peptide concentrations increase progressively as GFR decreases
10
Austin et al. Am J Clin Pathol. 2006;126:506-512.
GFRGFRCKD 1CKD 1 CKD 2CKD 2 CKD 3CKD 3 CKD 4CKD 4 CKD 5CKD 5
GFRCKD 1 CKD 2 CKD 3 CKD 4 CKD 5
Influence of Natriuretic Peptide Concentrations By eGFR and Diagnosis of Decompensated Heart Failure
DeFilippi, C. et al.: ”Impact of Renal Disease on Natriuretic Peptide Testing for Diagnosing Decompensated Heart Failure
and Predicting Mortality.” Clin. Chem. 2007; 53: 1511-1519.
NT-proBNP BNP
Influence on Natriuretic Peptide LevelsRenal Disease
Anwaruddin, S. et al.: “ Renal Function, Congestive Heart Failure, and Amino-Terminal pro-Brain Natriuretic Peptide
Measurement Results From the ProBNP Investigation of Dyspnea in the Emergency Department (PRIDE) Study.”
JACC 2006; 47:91-97.
NT-proBNP BNP
12
3/30/2016
3
Analytical Considerations Impact of body mass index (BMI) on Natriuretic Peptides
Krauser, D.G. et al.: “Effect of body mass index on natriuretic peptide levels in patients with acute congestive heart failure: A ProBNP Investigation of
Dyspnea in the Emergency Department (PRIDE) sub-study.” Am. Heart Journal 2005; 149: 744-750.
NT-proBNPNT-proBNP BNPBNPNT-proBNP BNP
13
FDA Cleared Claims
Elecsys proBNP II Package Insert, version 2012.06, V5
NT-proBNP
• An aid in the diagnosis of individuals suspected of having
congestive heart failure
• For risk stratification in patients with ACS and CHF
• An aid in the assessment of increased risk of cardiovascular
events and mortality in patients at risk for heart failure who
have stable coronary artery disease.
14
Utility of NT-proBNP in HF
HFAcute carePrimary care
Symptoms
Aid in Diagnosis of suspected HF Outcomes
PrognosisDiagnosis
15
Clinical Performance Represented ROC CurveFDA cleared clinical thresholds to rule-out heart failure:
125 pg/ml for younger patients, 450 pg/ml for patients 75 years and older
16
Receiver Operator Curve (ROC) Box and Whiskers Plot
Elecsys proBNP II Package Insert, version NT-pro 2012.06, V5
Clinical Utility Excluding Heart Failure
Elecsys proBNP II Package Insert, version NT-pro 2012.06, V5
Heart Failure Unlikely Additional CV assessment indicated
Patient
< 75 years > 125 pg/mL
Older patient
≥≥≥≥ 75 years > 450 pg/mL
NT-proBNP assay
Patients Suspected of Having HF
Patient
< 75 years < 125 pg/mL
Older patient
≥≥≥≥ 75 years < 450 pg/mL
17
> 100 pg/mL
BNP assay
Heart Failure unlikely
Patients Suspected of Having HF
Additional CV assessment indicated
< 100 pg/mL
Aggregate data from FDA submission data in three BNP package inserts. Abbott Axsym BNP Package Insert February 2004, Biosite BNP Package Insert
2002, Advia Centaur BNP package Insert 2008
Clinical Utility BNP Excluding Heart Failure – Single Cut-Point
18
3/30/2016
4
• Different modes of degradation• Different half-lives• Different cut-offs
• General recommendations apply to both BNP and NT-proBNP • Individual values are NOT interchangeable
Are BNP and NT-proBNP Values Interchangeable?Basic Differences
Source: 1 Hall, C, Eur J Heart Fail (2004) 6 (3) 257-260, 2 Maisel et al, State of the Art Using NP Levels, Eur J Heart Failur (2008) 10, 824-839
NO!
1
19
Demographics And Clinical Characteristics
Patients classified according to AHA/ACC heart failure classification scheme. Study included 86 health controls and 820 patients with HF in stages A-D. 479 patients had symptomatic heart failure in NYHA classes I-IV.
20Emdin, M. et al: “Comparison of Brain Natriuretic Peptide (BNP) and Amino-Terminal proBNP for Early
Diagnosis of Heart Failure.» Clin. Chem. 2007; 53:1289-1297.
Plasma Concentrations of BNP and NT-proBNP in healthy
controls and patients with heart failure in stages A-DConcentrations levels at 10th, 25th, 50th(median), 75th and 90th percentile, *: differences between groups are statistically significant with p<0.001 for all groups of comparison.
21Emdin, M. et al: “Comparison of Brain Natriuretic Peptide (BNP) and Amino-Terminal proBNP for Early
Diagnosis of Heart Failure.» Clin. Chem. 2007; 53:1289-1297.
A B C D
BNP, (ng/L) 11 (5–19) 20 (10–40) 165 (52–378) 404 (182–1012)
NT-proBNP, (ng/L) 43 (26–85) 88 (43–224) 1136 (379–2824) 4394 (1467–10 184)
Plasma Concentrations of BNP and NT-proBNP in healthy
controls and patients with HF in NYHA stages I-IVConcentrations levels at 10th, 25th, 50th(median), 75th and 90th percentile, *: differences between groups are statistically significant with p<0.001 for all groups of comparison.
22Emdin, M. et al: “Comparison of Brain Natriuretic Peptide (BNP) and Amino-Terminal proBNP for Early
Diagnosis of Heart Failure.» Clin. Chem. 2007; 53:1289-1297.
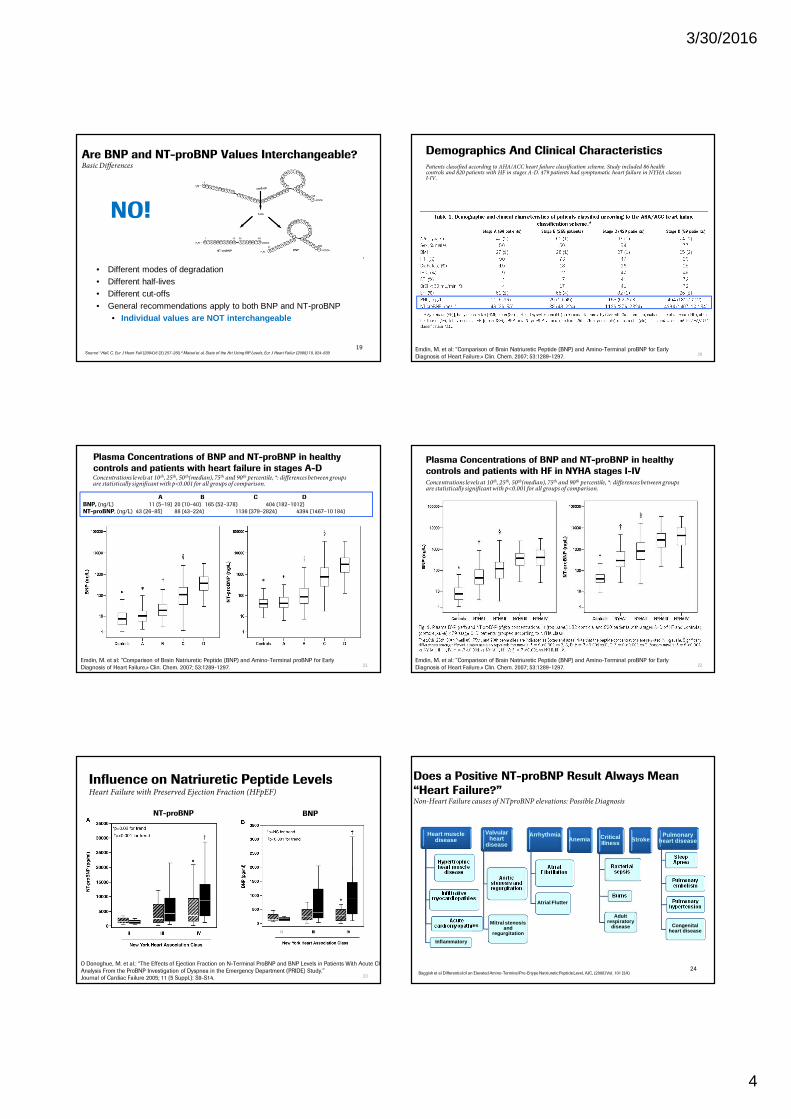
Influence on Natriuretic Peptide LevelsHeart Failure with Preserved Ejection Fraction (HFpEF)
O Donoghue, M. et al.: “The Effects of Ejection Fraction on N-Terminal ProBNP and BNP Levels in Patients With Acute CHF:
Analysis From the ProBNP Investigation of Dyspnea in the Emergency Department (PRIDE) Study.”
Journal of Cardiac Failure 2005; 11 (5 Suppl.): S9-S14.
NT-proBNP BNP
23
Heart muscle disease
Hypertrophic heart muscle
disease
Infiltrative myocardiopathies
Acute cardiomyopathies
Inflammatory
Valvular heart
disease
Aortic stenosis and regurgitation
Mitral stenosis and
regurgitation
Arrhythmia
Atrial Fibrillation
Atrial Flutter
Anemia Critical Illness
Bacterial sepsis
Burns
Adult respiratory
disease
StrokePulmonary
heart disease
Sleep Apnea
Pulmonary embolism
Pulmonary hypertension
Congenital heart disease
Does a Positive NT-proBNP Result Always Mean
“Heart Failure?”Non-Heart Failure causes of NTproBNP elevations: Possible Diagnosis
Baggish et al Differential of an Elevated Amino-Terminal Pro-B type Natriuretic Peptide Level, AJC, (2008) Vol. 101 (3A) 24
3/30/2016
5
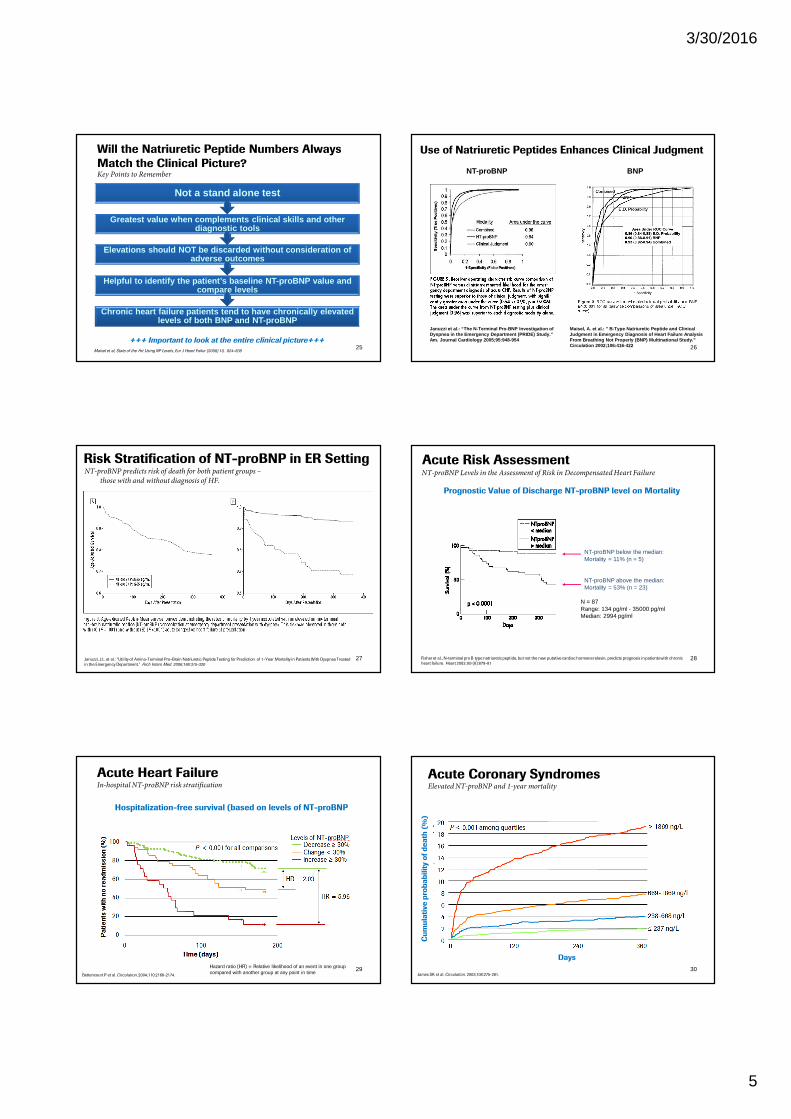
Will the Natriuretic Peptide Numbers Always
Match the Clinical Picture?Key Points to Remember
Maisel et al, State of the Art Using NP Levels, Eur J Heart Failur (2008) 10, 824-839
+++ Important to look at the entire clinical picture+++
Chronic heart failure patients tend to have chronic ally elevated levels of both BNP and NT-proBNP
Helpful to identify the patient’s baseline NT-proBN P value and compare levels
Elevations should NOT be discarded without consider ation of adverse outcomes
Greatest value when complements clinical skills and other diagnostic tools
Not a stand alone test
25
Use of Natriuretic Peptides Enhances Clinical Judgment
NT-proBNP BNP
Maisel, A. et al.: ” B-Type Natriuretic Peptide and Clinical Judgment in Emergency Diagnosis of Heart Failure An alysis From Breathing Not Properly (BNP) Multinational Stu dy.” Circulation 2002;106:416-422
Januzzi et al.: “The N-Terminal Pro-BNP Investigati on of Dyspnea in the Emergency Department (PRIDE) Study.” Am. Journal Cardiology 2005;95:948-954
26
Risk Stratification of NT-proBNP in ER Setting
Januzzi, J.L. et al.: “Utility of Amino-Terminal Pro–Brain Natriuretic Peptide Testing for Prediction of 1-Year Mortality in Patients With Dyspnea Treated
in the Emergency Department.” Arch Intern Med. 2006;166:315-320
NT-proBNP predicts risk of death for both patient groups –
those with and without diagnosis of HF.
27 Fisher et al., N-terminal pro B type natriuretic peptide, but not the new putative cardiac hormone relaxin, predicts prognosis in patients with chronic
heart failure. Heart 2003; 89 (8):879-81
NT-proBNP below the median:Mortality = 11% (n = 5)
NT-proBNP above the median:Mortality = 53% (n = 23)
N = 87Range: 134 pg/ml - 35000 pg/mlMedian: 2994 pg/ml
Prognostic Value of Discharge NT-proBNP level on Mortality
Acute Risk AssessmentNT-proBNP Levels in the Assessment of Risk in Decompensated Heart Failure
28
Acute Heart Failure In-hospital NT-proBNP risk stratification
Hospitalization-free survival (based on levels of NT-proBNP
.Bettencourt P et al. Circulation. 2004;110:2168-2174.
Hazard ratio (HR) = Relative likelihood of an event in one group
compared with another group at any point in time29
Cu
mu
lati
ve
pro
ba
bilit
y o
f d
ea
th (
%)
Days
Acute Coronary SyndromesElevated NT-proBNP and 1-year mortality
James SK et al. Circulation. 2003;108:275-281.30
3/30/2016
6
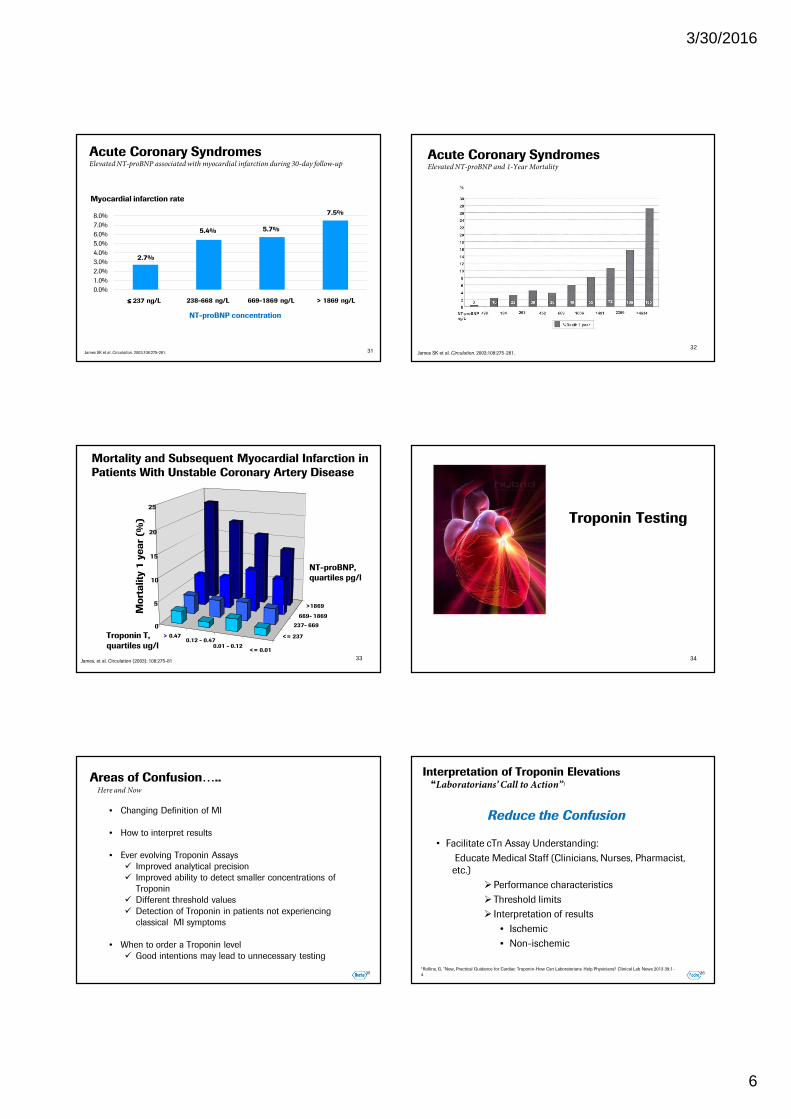
Acute Coronary SyndromesElevated NT-proBNP associated with myocardial infarction during 30-day follow-up
31James SK et al. Circulation. 2003;108:275-281.
2.7%
5.4% 5.7%
7.5%
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
Myocardial infarction rate
NT-proBNP concentration
> 1869 ng/L669-1869 ng/L238-668 ng/L≤≤≤≤ 237 ng/L
James SK et al. Circulation. 2003;108:275-281.
Acute Coronary SyndromesElevated NT-proBNP and 1-Year Mortality
32
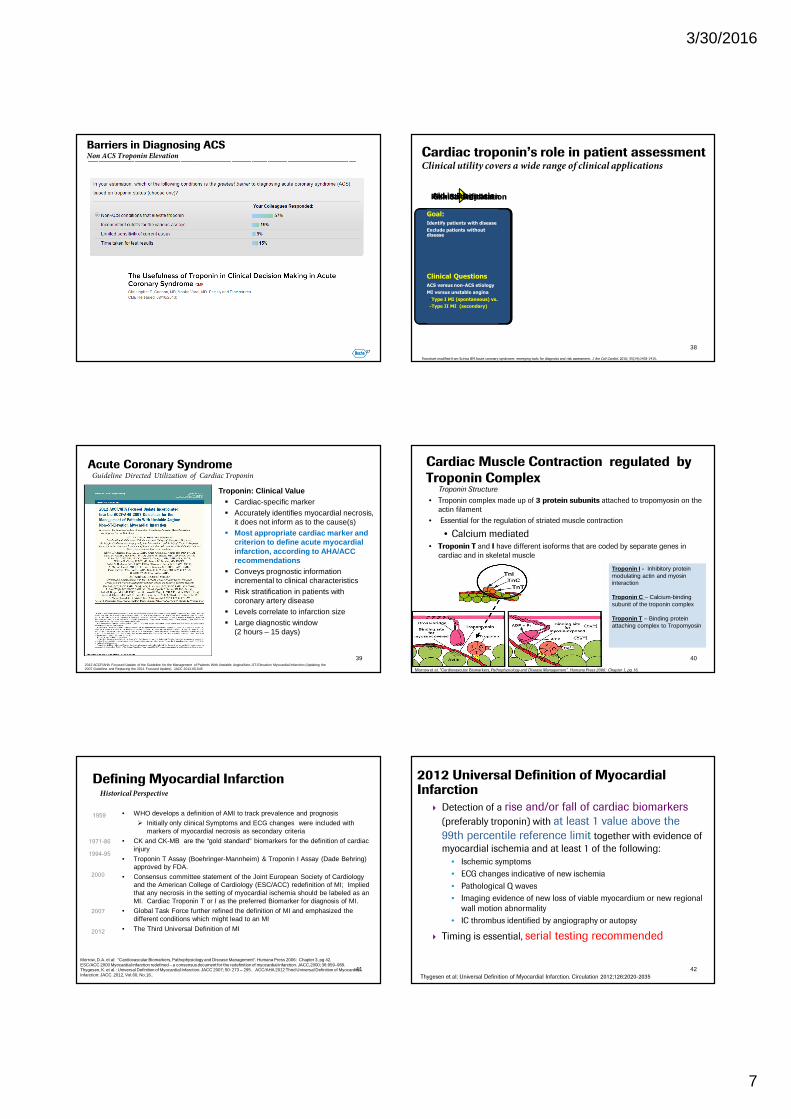
0
5
10
15
20
25
<= 237
237- 669
669- 1869
>1869
NT-proBNP,
quartiles pg/l
> 0.470.12 - 0.47
0.01 - 0.12<= 0.01
Troponin T,
quartiles ug/l
Mo
rta
lity
1 y
ea
r (%
)
Mortality and Subsequent Myocardial Infarction in
Patients With Unstable Coronary Artery Disease
James, et al. Circulation (2003); 108:275-8133 34
Troponin Testing
35
Areas of Confusion…..
• Changing Definition of MI
• How to interpret results
• Ever evolving Troponin Assays
� Improved analytical precision
� Improved ability to detect smaller concentrations of
Troponin
� Different threshold values
� Detection of Troponin in patients not experiencing
classical MI symptoms
• When to order a Troponin level
� Good intentions may lead to unnecessary testing
Here and Now
36
• Facilitate cTn Assay Understanding:
Educate Medical Staff (Clinicians, Nurses, Pharmacist,
etc.)
�Performance characteristics
�Threshold limits
� Interpretation of results
• Ischemic
• Non-ischemic
Interpretation of Troponin Elevations
“Laboratorians’ Call to Action”1
1Rollins, G. “New, Practical Guidance for Cardiac Troponin-How Can Laboratorians Help Physicians? Clinical Lab News 2013 39:1-
4
Reduce the Confusion
3/30/2016
7
37
Barriers in Diagnosing ACSNon ACS Troponin Elevation
Goal:
The test results change treatment decisions
Clinical Questions
Does specific test result change clinical practice (e.g. admission, catheterization, antithrombotic therapy, early discharge, ICD replacement
Goal:
Independent association with outcomes
Improved prognosis / stratification beyond established tools
Clinical Questions
What are risks of CV death, SCD, MI, recurrent ischemia, HF, stent thrombosis
Goal:
Identify patients with disease
Exclude patients without disease
Clinical Questions
ACS versus non-ACS etiology
MI versus unstable angina
-Type I MI (spontaneous) vs.
-Type II MI (secondary)
Cardiac troponin’s role in patient assessmentClinical utility covers a wide range of clinical applications
Flowchart modified from Scirica BM Acute coronary syndrome: emerging tools for diagnosis and risk assessment. J Am Coll Cardiol. 2010; 55(14):1403-1415.
Aid in DiagnosisRisk StratificationClinical Implication
38
Acute Coronary SyndromeGuideline Directed Utilization of Cardiac Troponin
� Troponin: Clinical Value� Cardiac-specific marker� Accurately identifies myocardial necrosis,
it does not inform as to the cause(s)� Most appropriate cardiac marker and
criterion to define acute myocardial infarction, according to AHA/ACC recommendations
� Conveys prognostic information incremental to clinical characteristics
� Risk stratification in patients with coronary artery disease
� Levels correlate to infarction size� Large diagnostic window
(2 hours – 15 days)
2012 ACCF/AHA Focused Update of the Guideline for the Management of Patients With Unstable Angina/Non–ST-Elevation Myocardial Infarction (Updating the2007 Guideline and Replacing the 2011 Focused Update). JACC 2012.60.645
39
Troponin Structure
40
• Troponin complex made up of 3 protein subunits attached to tropomyosin on the
actin filament
• Essential for the regulation of striated muscle contraction
• Calcium mediated • Troponin T and I have different isoforms that are coded by separate genes in
cardiac and in skeletal muscle
Morrow et al. “Cardiovascular Biomarkers, Pathophysiology and Disease Management”. Humana Press 2006: Chapter 1, pg 16.
Cardiac Muscle Contraction regulated by
Troponin Complex
Troponin I - Inhibitory protein modulating actin and myosin interaction
Troponin C – Calcium-binding subunit of the troponin complex
Troponin T – Binding protein attaching complex to Tropomyosin
Defining Myocardial Infarction
1959 • WHO develops a definition of AMI to track prevalence and prognosis
� Initially only clinical Symptoms and ECG changes were included with markers of myocardial necrosis as secondary criteria
• CK and CK-MB are the “gold standard” biomarkers for the definition of cardiac injury
• Troponin T Assay (Boehringer-Mannheim) & Troponin I Assay (Dade Behring) approved by FDA.
• Consensus committee statement of the Joint European Society of Cardiology and the American College of Cardiology (ESC/ACC) redefinition of MI; Implied that any necrosis in the setting of myocardial ischemia should be labeled as an MI. Cardiac Troponin T or I as the preferred Biomarker for diagnosis of MI.
• Global Task Force further refined the definition of MI and emphasized the different conditions which might lead to an MI
• The Third Universal Definition of MI2012
2000
1994-95
2007
Historical Perspective
Morrow, D.A. et al: “Cardiovascular Biomarkers, Pathophysiology and Disease Management”. Humana Press 2006: Chapter 3, pg 42.ESC/ACC 2000 Myocardial infarction redefined – a consensus document for the redefinition of myocardial infarction. JACC,2000; 36:959–969. Thygesen, K. et al.: Universal Definition of Myocardial Infarction. JACC 2007; 50: 273 – 295. ACC/AHA 2012 Third Universal Definition of Myocardial Infarction: JACC. 2012, Vol.60, No.16..
1971-86
41
2012 Universal Definition of Myocardial Infarction
� Detection of a rise and/or fall of cardiac biomarkers
(preferably troponin) with at least 1 value above the
99th percentile reference limit together with evidence of
myocardial ischemia and at least 1 of the following:
• Ischemic symptoms
• ECG changes indicative of new ischemia
• Pathological Q waves
• Imaging evidence of new loss of viable myocardium or new regional
wall motion abnormality
• IC thrombus identified by angiography or autopsy
� Timing is essential, serial testing recommended
Thygesen et al: Universal Definition of Myocardial Infarction. Circulation 2012;126:2020-2035
42
3/30/2016
8
Interpretation of Troponin Elevations Thresholds / Cutoffs
• 97th Percentile
• 99th Percentile
• 10% CV
• 10% or 20% CV
Practical Considerations - Interpretation of Troponin
Elevations Evolving Universal Definition of Myocardial
Infarction: Thresholds
Adapted from Fox, Keith AA, “High Sensitivity Troponin, Strengths and Weaknesses”. Presented @ ESC Congress 26-08-2012.
Diagnosis of
MI“Normal”
Population”
99th centile
(Universal Definition)
4th generation
assay
3rd
generation
assay
WHO
definition
The 99th percentile of a health reference population is…
45
Troponin T Elevations in the General Population
cTnT was undetectable among healthy subjects in the Dallas Heart Study
Wallace T.E. et al: Circ. 2006;113:1958-196546
Interpretation of troponin elevationsImportance of serial troponin sampling
Allows for differentiation of acute versus chronic troponin elevation
No agreement on what the absolute frequency of troponin testing should
be
• AHA Guidelines: baseline, 6 hours, and 12 hours1
• Universal Definition of MI: 0, 3, 6 hours2
Other Factors:
• Biological variation
• Defining criteria for a significant change
• Serial specimen collection improves identification of an acute event
1. Anderson JL, Adams CD, Antman EM, et al. 2012 ACCF/AHA focused update incorporated into the ACCF/AHA 2007 Guidelines for the management of patients with unstable angina/non-ST-
elevation myocardial infarction. J Am Coll Cardiol. 2013;61(23):e179-347.2. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Circulation. 2012;126(16):2020-2035.
Non ACS Troponin
Elevations
White et al., Clinical Implications of 3rd Definition of MI. Heart 2013.
Injury related to supply/demandOf myocardial ischemia
Injury not related to myocardial ischemia
Multifactorial or indeterminatemyocardial injury
48
3/30/2016
9
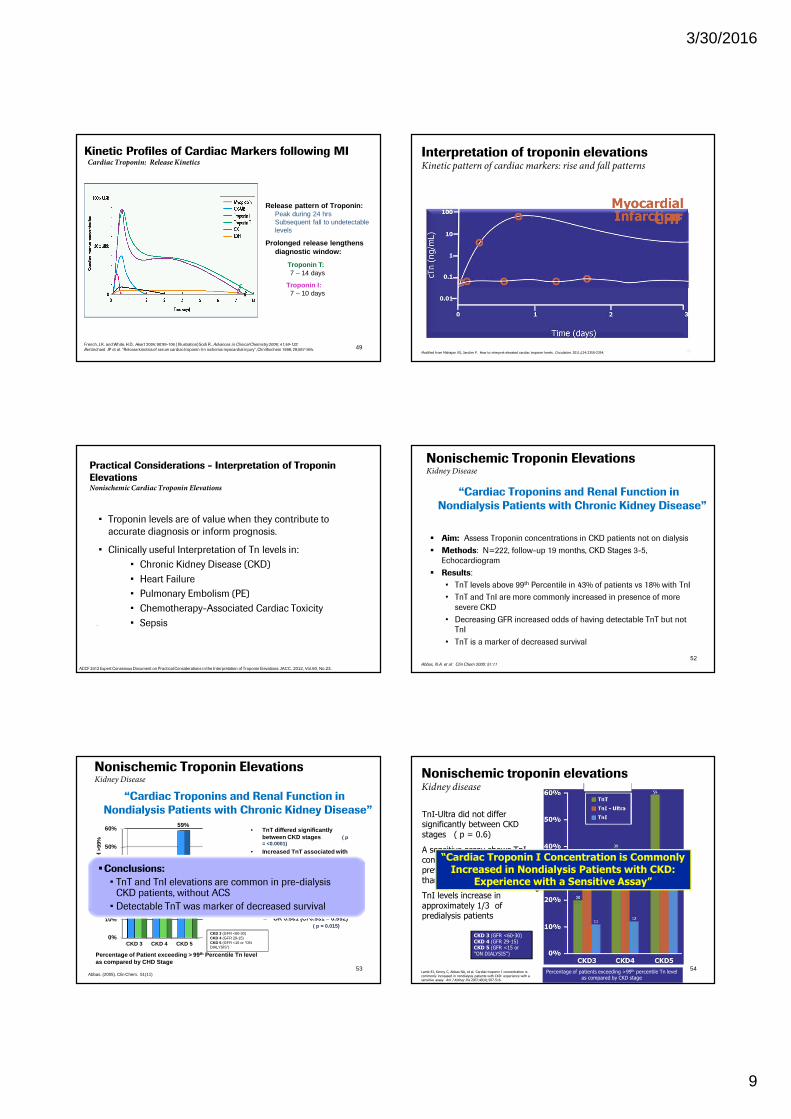
Release pattern of Troponin:Peak during 24 hrs Subsequent fall to undetectable levels
Prolonged release lengthens diagnostic window:
Troponin T:7 – 14 days
Troponin I:7 – 10 days
French, J.K. and White, H.D., Heart 2004; 90:99-106 ( Illustration) Sodi R., Advances in Clinical Chemistry 2006; 41;49-122.
Bertinchant JP et al. “Release kinetics of serum cardiac troponin I in ischemic myocardial injury”, Clin Biochem 1996; 29;587-594.
Kinetic Profiles of Cardiac Markers following MICardiac Troponin: Release Kinetics
49Modified from Mahajan VS, Jarolim P. How to interpret elevated cardiac troponin levels. Circulation. 2011;124:2350-2354.
Interpretation of troponin elevationsKinetic pattern of cardiac markers: rise and fall patterns
• Troponin levels are of value when they contribute to
accurate diagnosis or inform prognosis.
• Clinically useful Interpretation of Tn levels in:
• Chronic Kidney Disease (CKD)
• Heart Failure
• Pulmonary Embolism (PE)
• Chemotherapy-Associated Cardiac Toxicity
• Sepsis
Practical Considerations - Interpretation of Troponin
ElevationsNonischemic Cardiac Troponin Elevations
.
ACCF 2012 Expert Consensus Document on Practical Considerations in the Interpretation of Troponin Elevations: JACC. 2012, Vol.60, No.23.
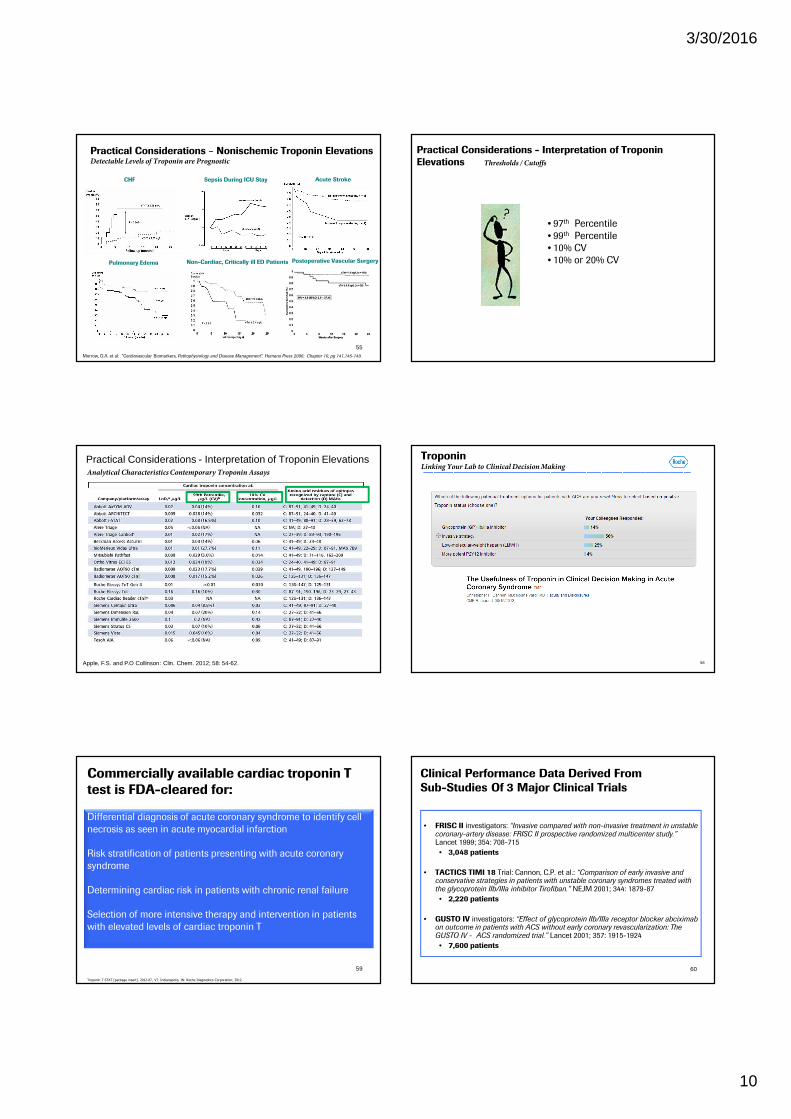
� Aim: Assess Troponin concentrations in CKD patients not on dialysis
� Methods: N=222, follow-up 19 months, CKD Stages 3-5,
Echocardiogram
� Results:
• TnT levels above 99th Percentile in 43% of patients vs 18% with TnI
• TnT and TnI are more commonly increased in presence of more
severe CKD
• Decreasing GFR increased odds of having detectable TnT but not
TnI
• TnT is a marker of decreased survival
Abbas, N.A. et al: Clin Chem 2005: 51:11
Nonischemic Troponin ElevationsKidney Disease
“Cardiac Troponins and Renal Function in
Nondialysis Patients with Chronic Kidney Disease”
52
• TnT differed significantly between CKD stages ( p = <0.0001)
• Increased TnT associated with reduced eGFR
• OR 0.939 (CI 0.916 – 0.963) ( p = <0.001)
% c
Tn
Leve
l>9
9%
0%
10%
20%
30%
40%
50%
60%
CKD 3 CKD 4 CKD 5
TnTTn I
20%
11%
39%
12%
59%
26%
Abbas. (2005). Clin Chem. 51(11)
Percentage of Patient exceeding > 99 th Percentile Tn level as compared by CHD Stage
“Cardiac Troponins and Renal Function in
Nondialysis Patients with Chronic Kidney Disease”
• TnI differed significantly between CKD stages 4 & 5 ( p = 0.0197) But not between CKD stages 3 & 4.
• Increased TnI associated with reduced eGFR
– OR 0.961 (CI 0.931 – 0.992) ( p = 0.015)
CKD 3 (GFR <60-30)CKD 4 (GFR 29-15)CKD 5 (GFR <15 or “ON DIALYSIS”)
�Conclusions:
• TnT and TnI elevations are common in pre-dialysis CKD patients, without ACS
• Detectable TnT was marker of decreased survival
Nonischemic Troponin ElevationsKidney Disease
53
cT
n L
ev
el
>9
9%
TnI-Ultra did not differ significantly between CKD stages ( p = 0.6)
A sensitive assay shows TnI concentrations to be more prevalent in pts with CKD than previously believed
TnI levels increase in approximately 1/3 of predialysis patients
Lamb EJ, Kenny C, Abbas NA, et al. Cardiac troponin I concentration is
commonly increased in nondialysis patients with CKD: experience with a sensitive assay. Am J Kidney Dis 2007;49(4);507-516.
Nonischemic troponin elevationsKidney disease
Percentage of patients exceeding >99th percentile Tn level as compared by CKD stage
CKD 3 (GFR <60-30)CKD 4 (GFR 29-15)CKD 5 (GFR <15 or “ON DIALYSIS”)
“Cardiac Troponin I Concentration is Commonly Increased in Nondialysis Patients with CKD:
Experience with a Sensitive Assay”
54
3/30/2016
10
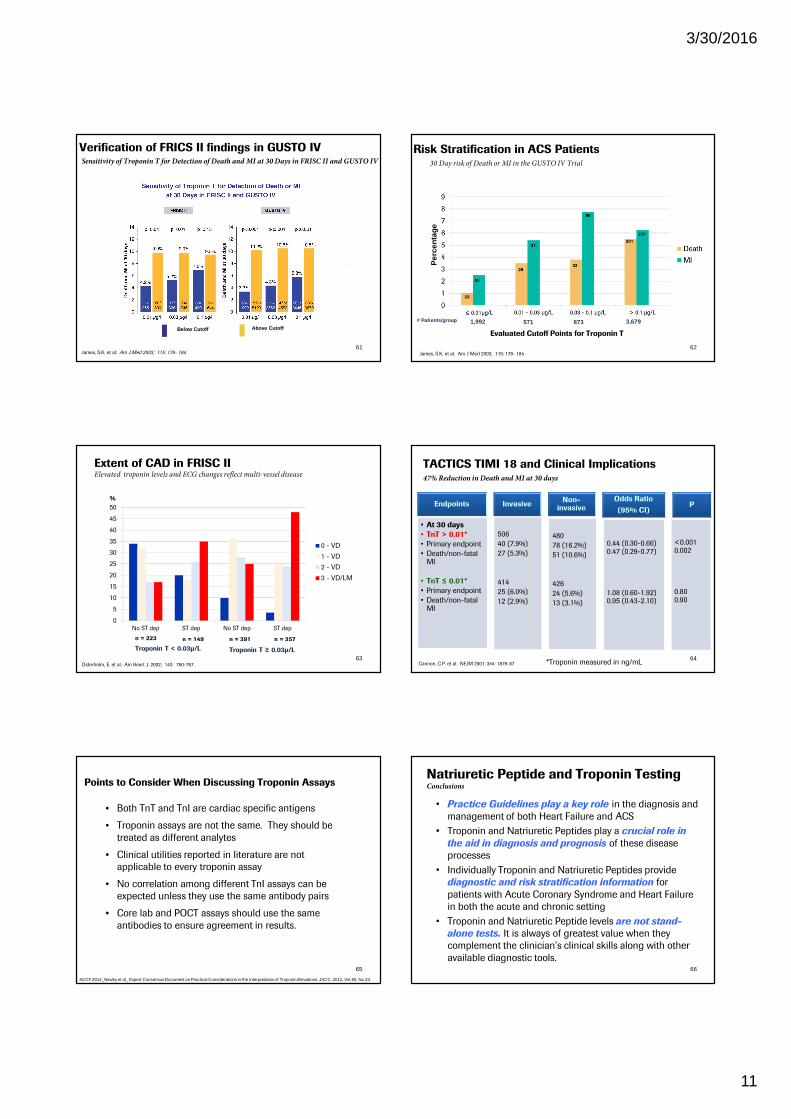
Morrow, D.A. et al: “Cardiovascular Biomarkers, Pathophysiology and Disease Management”. Humana Press 2006: Chapter 10, pg 141,145-149.
Practical Considerations – Nonischemic Troponin ElevationsDetectable Levels of Troponin are Prognostic
CHF
Pulmonary Edema
Sepsis During ICU Stay
Non-Cardiac, Critically ill ED Patients
Acute Stroke
Postoperative Vascular Surgery
55
Practical Considerations - Interpretation of Troponin
Elevations Thresholds / Cutoffs
• 97th Percentile
• 99th Percentile
• 10% CV
• 10% or 20% CV
Apple, F.S. and P.O Collinson: Clin. Chem. 2012; 58: 54-62.
Practical Considerations - Interpretation of Troponin ElevationsAnalytical Characteristics Contemporary Troponin Assays
58
TroponinLinking Your Lab to Clinical Decision Making
Differential diagnosis of acute coronary syndrome to identify cell
necrosis as seen in acute myocardial infarction
Risk stratification of patients presenting with acute coronary
syndrome
Determining cardiac risk in patients with chronic renal failure
Selection of more intensive therapy and intervention in patients
with elevated levels of cardiac troponin T
Commercially available cardiac troponin T
test is FDA-cleared for:
Troponin T STAT [package insert]. 2012-07, V7. Indianapolis, IN: Roche Diagnostics Corporation; 2012.
59
Clinical Performance Data Derived From
Sub-Studies Of 3 Major Clinical Trials
60
• FRISC II investigators: “Invasive compared with non-invasive treatment in unstable coronary-artery disease: FRISC II prospective randomized multicenter study.”Lancet 1999; 354: 708-715
• 3,048 patients
• TACTICS TIMI 18 Trial: Cannon, C.P. et al.: “Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor Tirofiban.” NEJM 2001; 344: 1879-87
• 2,220 patients
• GUSTO IV investigators: “Effect of glycoprotein IIb/IIIa receptor blocker abciximabon outcome in patients with ACS without early coronary revascularization: The GUSTO IV - ACS randomized trial.” Lancet 2001; 357: 1915-1924
• 7,600 patients
3/30/2016
11
Verification of FRICS II findings in GUSTO IV
James, S.K. et al: Am J Med 2003; 115: 178- 184
Sensitivity of Troponin T for Detection of Death and MI at 30 Days in FRISC II and GUSTO IV
Below Cutoff Above Cutoff
61
Risk Stratification in ACS Patients
Per
cent
age
James, S.K. et al: Am J Med 2003; 115: 178- 184
22
# Patients/group 1,992 571 873 3,679
Evaluated Cutoff Points for Troponin T
30 Day risk of Death or MI in the GUSTO IV Trial
62
Extent of CAD in FRISC IIElevated troponin levels and ECG changes reflect multi-vessel disease
0
5
10
15
20
25
30
35
40
45
50
No ST dep ST dep No ST dep ST dep
0 - VD
1 - VD
2 - VD
3 - VD/LM
n = 223 n = 149 n = 391 n = 357
Troponin T < 0.03µ/L Troponin T ≥ 0.03µ/L
Diderholm, E. et al.: Am Heart J. 2002; 143: 760-767.
%
63
TACTICS TIMI 18 and Clinical Implications
Endpoints
• At 30 days
• TnT > 0.01*
• Primary endpoint
• Death/non-fatal MI
• TnT ≤ 0.01*
• Primary endpoint
• Death/non-fatal MI
Invasive
506
40 (7.9%)
27 (5.3%)
414
25 (6.0%)
12 (2.9%)
Non-invasive
480
78 (16.2%)
51 (10.6%)
426
24 (5.6%)
13 (3.1%)
Odds Ratio
(95% CI)
0.44 (0.30-0.66)0.47 (0.29-0.77)
1.08 (0.60-1.92)0.95 (0.43-2.10)
P
<0.0010.002
0.800.90
Cannon, C.P. et al.: NEJM 2001; 344: 1879-87
47% Reduction in Death and MI at 30 days
64*Troponin measured in ng/mL
• Both TnT and TnI are cardiac specific antigens
• Troponin assays are not the same. They should be
treated as different analytes
• Clinical utilities reported in literature are not
applicable to every troponin assay
• No correlation among different TnI assays can be
expected unless they use the same antibody pairs
• Core lab and POCT assays should use the same
antibodies to ensure agreement in results.
65
Points to Consider When Discussing Troponin Assays
ACCF 2012_Newby et al_ Expert Consensus Document on Practical Considerations in the Interpretation of Troponin Elevations: JACC. 2012, Vol.60, No.23.
• Practice Guidelines play a key role in the diagnosis and
management of both Heart Failure and ACS
• Troponin and Natriuretic Peptides play a crucial role in
the aid in diagnosis and prognosis of these disease
processes
• Individually Troponin and Natriuretic Peptides provide
diagnostic and risk stratification information for
patients with Acute Coronary Syndrome and Heart Failure
in both the acute and chronic setting
• Troponin and Natriuretic Peptide levels are not stand-
alone tests. It is always of greatest value when they
complement the clinician’s clinical skills along with other
available diagnostic tools.
Natriuretic Peptide and Troponin TestingConclusions
66