national association of school psychologists annual ... · national association of school...
TRANSCRIPT

Cognitive Behavioral Interventions for Students
with Obsessive‐Compulsive Disorder
National Association of School Psychologists Annual Conference, 2011
San Francisco, CADouglas T. Jones, Michael L. Sulkowski, & Robert J. Wingfield
Introduction• Overview
– Etiology – Associated Issues
• Cognitive Behavioral Therapy– Conceptualization– SUDs and Hierarchy
• Exposure and Response Prevention (ERP)– Treatment Practice– Treatment in schools

Overview

Obsessive Compulsive Disorder (OCD)
•OCD is characterized by obsessions and/or compulsions that are significantly impairing and distressing
• Functional impairment for more than 1 hr per day
American Psychiatric Association. (2000).

OCD Prevalence• 1-3% of U.S. Youth (McKay &
Storch, 2009)o Child OCD – more than 1 in 100
o 4th most common psychiatric disorder in the United States (Leahy & Holland, 2000).

OCD Onset / Treatment• Usual onset in late teens or
early twenties (Kessler, 2005 & Wewetzer et al., 2001).o 6-15 for maleso 20-29 for females
• 80% of adults with OCD have childhood onset (Kessler, 2005).
• Average total of 17 yrsbetween onset of symptoms (age 14.5) and appropriate treatment (age 31.5)

OCD Etiology• Biological Model
o Neurobiological abnormalities• PANDAS
• Cognitive Behavioral Modelo Obsessive-Compulsive cycle
• Behavioral conditioning• Cognitive distortions
7

Obsessive Compulsive Disorder (OCD)
• Obsessions:o Recurrent or persistent thoughts, impulses, or images seen as
intrusive or inappropriate that cause marked anxiety/distress
o Not simply excessive worries
o Attempts are made to suppress or neutralize obsessions
American Psychiatric Association. (2000).

Obsessive Compulsive Disorder (OCD)
• Compulsions:o Repetitive behaviors or mental acts driven to perform in
response to obsession, or according to rules rigidly applied
o Behaviors or mental acts are aimed at preventing or reducing distress or preventing dreaded event or situation
American Psychiatric Association. (2000).

Obsessions
Compulsions
Fear/Anxiety
Reduction in Distress
The Obsessive-Compulsive Cycle
Negative Reinforcement
(Piacentini et al, 2006)10
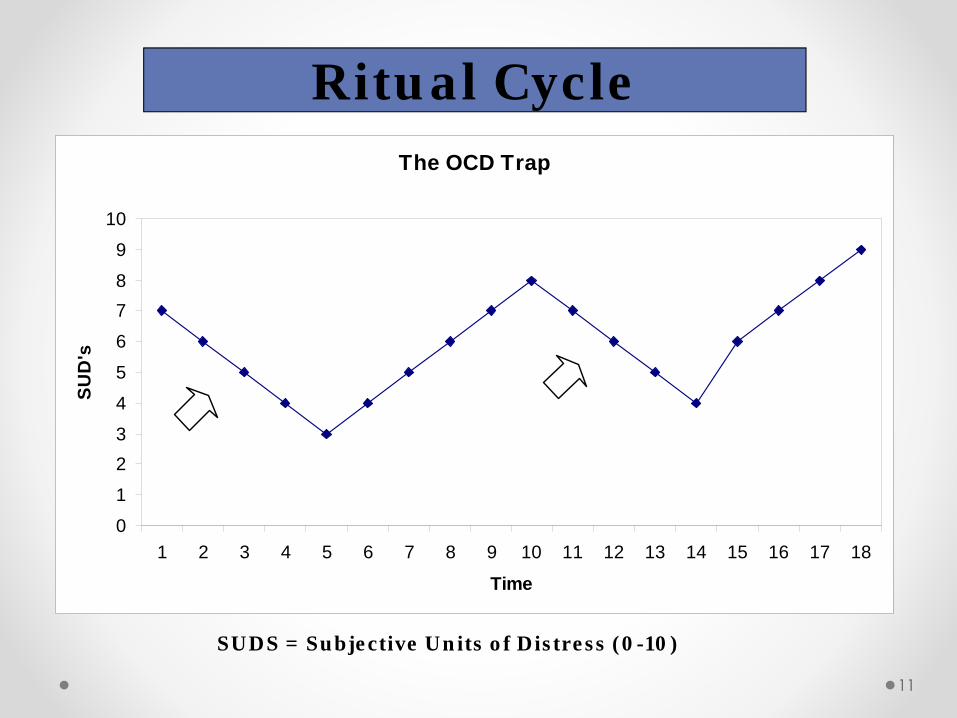
Ritual Cycle
SUDS = Subjective Units of Distress (0-10)
11
The OCD Trap
0
1
23
4
5
6
78
9
10
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Time
SUD
's

Common OCD Symptom Patterns
• Contamination and cleaning (hand washing)
• Self doubt and checking, re-writing, repeating, hoarding
• Organizing / need for symmetry
• Scrupulosity (religious obsessions)
• Aggressive obsessions (fear of harming others)

Signs of OCD in Children
• Contamination Behaviorso Frequent cleaning/hand washing (red, chapped hands)o Long frequent trips to the bathroom.o Avoidance of the playground, art supplies, sticky substances.o Untied shoe laces (may be contaminated)
• Checking and redoing activities/behaviorso Compulsively going over letters and numbers with pencil.o Taking excessive time to perform tasks.o Rereading and rewriting, and frequent erasing.

Signs of OCD in Children (Cont.)
• Reassurance Seekingo Am I okay, is this right?o Asking frequent questions when the answer is already evident.
• Anxiety and Avoidanceo Withdrawal from usual activities or friends.o Excessive fear of bad things happening to self or others.o Excessive fears of making mistakes.o Persistent lateness.
• Counting and Organizing

Associated Issues
o Academic Difficulties• Work completion issues
o Disruptive Disorders• ADHD• ODD
o Depression and Anxiety Disorders• Generalized Anxiety• Trichotillomania

Vignettes• Mary
o Obsessions – Perfectionistic, Not-good-enough worrieso Compulsions – Checking, Studying, Re-writing
• Joeyo Obsessions – Just right feelingo Compulsions – Touching others, Pulling threads
• Johno Obsessions – Contamination, sexualityo Compulsions – Cleaning, avoidance

COGNITIVE BEHAVIORAL
THERAPY

Early Psychological Treatments: The “T” in CBT
• OCD once was thought to be resistant to psychological treatmento Traditional treatments even could worsen symptoms
(Christensen, Hadzi-Pavlovic, Andrews, & Mattick, 1987)• Can increase doubting symptoms and accommodate rituals
o Traditional behavioral treatments also proved ineffective (e.g., thought stopping, relaxation training; McKay, Storch, Nelson, Morales, & Moretz, 2009).

The “B” in CBT• E/RP breaks the association between specific stimuli,
situations, or anxiety-provoking thoughts and reliance on anxiety reducing rituals (Foa, Abramowitz, Franklin, & Kozak, 1999)
• The therapy has a biological basiso Facilitates habituation and may affect action in basolateral
amygdala, hippocampus, and the medial prefrontal cortex (Quirk & Mueller, 2007)

The “C” in CBT• Highlight the role of dysfunctional beliefs and
interpretations that sustain ritualso More appropriate and applicable to treating adults
• Cognitive therapy must be done carefullyo Can reinforce rituals or engender new ones
• Use CT to externalize OCD symptoms or motivate children
o The OCD monstero Let’s try an experiment

Dysfunctional cognitions• Black and white/all or nothing thinking
o “If it is not perfect, then it’s garbage.”• Magical thinking
o “If I think a bad thought, then something bad will happen.”
• Overestimation of risko “If I even take the slightest chance,
something bad will happen.”• Hypermoraity
o “Ill go to hell if . . .”

Dysfunctional cognitions• Thought/action fusion (similar to magical thinking)
o “If I have the bad thought, it will happen.”• Overimportance of thought
o “I cannot have bad thoughts—I must have a pure mind.”• “What if” thinking
o “In the future, what if I . . . Make a mistake? Get AIDS? Hurt someone?
• Intolerance of uncertaintyo “I cannot relax unless I am 100% certain that I will be okay,
safe, certain.• The martyr complex
o “I choose to . . . To prevent . . . “

CBT For Pediatric OCD• Pioneered by Dr. John March (March &
Mulle, 1998)o Must consider developmental and cognitive levelo Should include family members/caregivers
• Collaborative efforts between the child, caregivers, and child
o Should appeal to children and be fun• Incorporate elements of play into therapy

Efficacy of CBT for Pediatric OCD
• Generally large effects sizes across studies of randomized and non-randomized trials of CBT in youth (Watson & Rees, 2008)
o Effect sizes range from 0.95 to 2.56
• These results are similar to those found in adult OCD treatment studies (Abramowitz, 1998)

CBT for Pediatric OCD• Assessment• Psychoeducation• Socialization to treatment
o For child and family
• Development of an OCD symptoms hierarchy• Engage in exposures and active treatment• Conclude treatment• Offer booster sessions as needed

Assessment• Omnibus behavior screeners
o BASC-2, CBCL
• Single construct measureso BAI, RCMAS-2,
• Structured/semi-structured interviews• OCD specific measures
o OIC-R, FOCIo CY-BOCS (the “gold standard”)

Psychoeducation• Provide information on OCD to children
and caregiverso Prevalenceo Course of the disordero Impact on familieso Nature of symptoms
• Describe CBTo Treatment componentso Efficacy of the treatment, especially for OCDo Typical number of sessions, length of sessions

Socialization to Treatment• Emphasize that exposures will be gradual• May need to motivate some youth
o Be dispassionate and firmo Motivational interviewing techniques
• Exposure intensity corresponds with positive treatment outcomes
• The therapist should establish rapport o Convey warmth, optimism, confidence, and even a playful attitude
• Get parents/caregivers on board

Development of a Symptoms Hierarchy
• Day 1 or 2 (the easiest part of treatment)• Work with child to develop a list of feared
stimuli or situations• Write down everything and ask clarifying
questions• Rank order items on a scale (1 – 10; 1 – 100)• “Everything is a 10!”• “Nothing scares me”• Use of anchor points and contrasts

30
OCD Hierarchy
SUDS Level
99 Touching an unknown sticky substance, without washing95 Holding loose hair90 Touching known sticky substances (e.g. egg), without washing85 Touching unknown trash articles60 Using a public restroom 60 Witnessing a political argument60 Witnessing other sensitive-subject arguments (i.e. religion)60 Seeing parents spend a lot of money at one time60 Touching loose hair with finger55 Touching known sticky substance (e.g. syrup),without washing
50 Touching a known sticky substance (e.g. soda), without washing
30 Touching a dirty railing30 Walking into a public bathroom

Ranking Your Own Fears• Work with a partner to rank order your
fears
• List fears and corresponding thoughtso (e.g., spiders, death, heights, elevators)
• Come up with a list of ways to engender these fears (exposures)o (e.g., licking a doorknob, leaving the house unlocked when
nobody is home)
Exposure and Response
Prevention

Exposure and Response Prevention
CBT with exposure and response prevention (ERP) is the best established psychological treatment for OCD.
Gold standard (DeRubeis & Crits-Christoph, 1998).63% to 83% of participants obtained some benefit, many long term after ERP (Abramowitz, 1997; Foa & Kozak, 1996; Stanley & Turner, 1995).
33

Exposure and Response Prevention
How does it work?E/RP breaks the association between specific stimuli, situations, or anxiety-provoking thoughts and reliance on anxiety reducing rituals (Foa, Abramowitz, Franklin, & Kozak, 1999)The therapy has a biological basis.
Facilitates habituation and may affect action in basolateral amygdala, hippocampus, and the medial prefrontal cortex (Quirk & Mueller, 2007)
34

Informal progress monitoring strategies
• Subjective units of distress (SUDs)o Thumbnail judgments of distresso Can be taken any time during
therapyo Children can monitor and
document their own SUDs

ERPExposure (in vivo)
Children are gradually exposed to anxiety-provoking stimuli…
PreventionWhile refraining (or prevented) from engaging in anxiety-reductive compulsive behaviors.
Exposure (imaginal)Children expose themselves to feared thoughts through scripting.Scripting: written in the first person containing sufficient detail to evoke an anxiety response; usually 3to5 minutes longVerbalizing: repeatedly read the script aloud until the anxiety decreases or record the scenario on an audiotape and repeatedly listen to the tape.Focus is getting used to one’s thoughts

ERPExposure Practice
Predictability and Control: combination of allowing client as much control and predictability as possible while continuing to push and challenge is the best strategy.Distraction: Encourage as much focus on the feared stimulus during exposure as possible.
Length of Exposures: Outcomes studies indicate exposure sessions generally range from 30 to 120 minutes.Longer sessions were correlated with larger effect sizes on measures of OCD symptoms Thus, 90 to 120 minute sessions may be the most useful length of session.
ERPTroubleshooting:
Motivational Issues: level of readiness to change significantly predict treatment attrition (Wilson, Bell-Dolan, & Beitman, 1997)
Encourage child to voice reasons for change, explore future costs and benefits of change
Reassurance Seeking: Therapist and family must refrain from answering questions during exposures if the answer may provide reassurance. Reassurance seeking is another form of a compulsion.

0102030405060708090
100
Onset
5min
10min
15min
20min
25min
30min
35min
40min
1st Trial2nd Trial3rd Trial4th Trial5th Trial
How ERP Works
SUDS
Storch, 2006

School Psychologists’ Reports on OCD
• Sloman et al. (2007)o 89.8% of respondents had experience with at least one OCD
case.
o 82.4% reported that they were “much or very much” influenced by evidence based treatments AND
o 89.5% of participants adhered to a cognitive behavioral theoretical orientation AND
o 81% reported that they were “much or very much” inclined to implement CBT as a choice of treatment.
• Resultso Only 7.1% reported using exposure based elements “much or
very much” in the treatment of OCD.
o Nearly half (46%) stated that there was “minimal to no change” in outcome.
(Storch , 2006)

What can school psychologists do in the school setting?
• Help school personnel recognize that OCD is a neurobehavioral disorder that reflects abnormal information processing in the CNS and not “oppositional behavior.”
• Help personnel view the child with OCD the same as child with diabetes or asthma
• Refrain from punishing the student for situations or behaviors he or she has no control over (e.g., being tardy, absent, no attending to work)
• Record changes in a child’s behavior (both negative and positive) that may be a result of medication and/or behavioral interventions.

What can school psychologists do in the
school setting?
• Allow breaks during testing
• Extended time for homework and projects (only until child overcomes being “bossed around by OCD”) If misapplied this could reinforce OCD.
• Monitor child to ensure he or she isn’t using OCD as an excuse to avoid academic demands
• Students with OCD are generally eligible for 504 Plans
(Marche and Mulle, 1998)

Exposure and Response Prevention Activity
• Part One - Imaginal Scripting– Using your hierarchy formed in the previous activity create an
imaginal script or exposure for a distressing item (SUDS around 7 or 8).
– Examples– Funeral of a loved one– Skydiving

Exposure and Response Prevention Activity
• Part Two - En Vivo ERP o Form into groups of three – be the therapist / student– Take turns leading one another through your exposure– Monitor SUDs level!– Do not flood
– Do not go above a 5 or 6…– Proceed until SUDS level drops by half


References• American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington,
DC: Author.
• Abramowitz, J. S. (1998). Does cognitive-behavioral therapy cure obsessive-compulsive disorder? A meta-analytic evaluation of clinical significance. Behavior Therapy, 29, 339-335
• Abramowitz, J. S., Whiteside, S. P., & Deacon, B. J. (2005). The effectiveness of treatment for pediatric obsessive-compulsive disorder: A meta-analysis. Behavior Therapy, 36, 55-63.
• Arnold, L. M., Auchenbach, M. B., & McElroy, S. L. (2001). Psychogenic excoriation. clinical features, proposed diagnostic criteria, epidemiology and approaches to treatment. CNS Drugs, 15, 351-359.
• Azrin, N. H. & Nunn, R. G. (1973). Habit reversal: a method of eliminating nervous habits and tics. Behaviour Research and Therapy, 11, 619-628.
• Barkley, R. A., & Mash, E. J. (2003). Child psychopathology (2nd ed.). New York: Gilford Press.
• Barsky, A. J., & Ahern, D. K. (2004). Cognitive behavior therapy for hypochondriasis: A randomized controlled trial. Journal of the American Medical Association, 291, 1464-1470.
• Chambless, D. L., Baker, M. J., Baucom, D. H., Beutler, L. E., Calhoun, K. S., Crits-Christoph, P., et al. (1998). Update on empirically validated therapies, II. The Clinical Psychologist, 51, 3-16.
• Christensen H., Hadzi-Pavlovic D., Andrews G., & Mattick R. (1987). Behavior therapy and tricyclic medication in the treatment of obsessive-compulsive disorder: A quantitative review. Journal of Consulting and Clinical Psychology, 55, 701-711.
• Cororve, M. B., & Gleaves, D. H. (2001). Body dysmorphic disorder: A review of conceptualizations, assessment, and treatment strategies. Clinical Psychology Review, 21, 949-970.
• Deckersbach, T., Wilhelm, S., & Keuthen, N. (2003). Self-injurious skin picking: Clinical characteristics, assessment methods, and treatment modalities. Brief Treatment and Crisis Intervention, 3, 249-260.
• DeRubeis, R. J., & Crits-Christoph, P. (1998). Empirically supported individual and group psychological treatments for adult mental disorders. Journal of Consulting and Clinical Psychology, 66, 37-52.
•• Foa, E. B., Huppert, J. D., Leiberg, S., Langner, R. Kichic, R. Hajcak, G., et al., (2002). The Obsessive–Compulsive Inventory:
development and validation of a short version. Psychological Assessment, 14, 485–496.
• Foa, E. B., & Kozak, M. J. (1996). Psychological treatment for obsessivecompulsive disorder. In M. R. Mavissakalian & R. F. Prien(Eds.), Long-term treatments of anxiety disorders (pp. 285–309). Washington, DC: American Psychiatric Press.

References• Hyman, B. M., & Pedrick, C. (1999). The OCD workbook: Your guide to breaking free from obsessive-compulsive disorder. Oakland,
CA, US: New Harbinger Publications.
• Kessler, R. C., Berglund, P., Demler, O., Jin, R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Archives of General Psychiatry, 62, 593-602.
• Leahy, R. L., & Holland, S. J. (2000). Treatment plans and interventions for depression and anxiety disorders. New York: Guilford.
• Foa, E. B., Abramowitz, J. S., Franklin, M. E., & Kozak, M. J. (1999). Feared consequences, fixity of belief, and treatment outcome in patients with obsessive–compulsive disorder. Behavior Therapy, 30, 717–724.
• March, J. S., & Mulle, K. (1998). OCD in Children and Adolescents. New York: Guilford.
• McKay, D. (1999). Two-year follow-up of behavioral treatment and maintenance for body dysmorphic disorder. Behavior Modification, 23, 620-632.
• McKay, D. & Storch, E.A. Eds. (2009). Cognitive-behavior therapy for children: treating complex and refractory cases. Springer, New York.
• McKay, D., Storch, E. A., Nelson, B., Morales, M., & Moretz, M. W. (2009). Obsessive-compulsive disorder in children and adolescents: Treating difficult cases. In D. McKay & E. A. Storch (Eds.), Cognitive-behavior therapy for children and adolescents: Treating difficult cases (pp. 81–114). New York: Springer.
• Neziroglu, F., McKay, D., Todaro, J., & Yaryura-Tobias, J. A. (1996). Effect of cognitive behavior therapy on persons with body dysmorphic disorder and comorbid axis II diagnoses. Behavior Therapy, 27, 67-77.
• Pence, S. L., Jr., Sulkowski, M. L., Jordan, C., & Storch, E. A. (2010). When exposures go wrong: trouble-shooting guidelines for managing difficult scenarios that arise in exposure-based treatment for obsessive–compulsive disorder. American Journal of Psychotherapy.
• Piacentini, J., March, J., & Franklin, M. (2006). Cognitive–behavioral therapy for youth with obsessive−compulsive disorder. In P. C. Kendall (Ed.), Child and adolescent therapy: Cognitive–behavioral procedures (3rd ed., (pp. 297–321). New York: Guilford Press.
• Quirk, G. J., & Mueller, D. (2007). Neural Mechanisms of Extinction Learning and Retrieval. Neuropsychopharmacology, 33, 56-72.•••
References• Scahill L, Riddle MA, Hardin MT, Ort SI, King RA, Goodman WK, & Leckman J F. (1997). Children's Yale Brown Obsessive Compulsive
Scale: Reliability and validity. J Am Acad Child Adolesc Psychiatry 36:844—852.
• Sloman, G. M., Gallant, J., & Storch, E. A. (2007). A School-Based Treatment Model for Pediatric Obsessive-Compulsive Disorder. Child Psychiatry and Human Development, 38, 303-319.
• Stanley, M. A. & Turner, S. M. (1995). Current status of pharmacological and behavioral treatment of obsessive—compulsive disorder. Behavior Therapy, 26, 163-186.
• Storch, E. A., Stigge-Kaufman, D., Bagner, D., Merlo, L. J., Shapira, N. A., Geffken, G. R., Murphy, T. K., & Goodman, W. K. (2007). Florida Obsessive-Compulsive Scale: Development, reliability, and validity. Journal of Clinical Psychology.
• Storch, E. A.(2006). Treatment of a patient with Obsessive-Compulsive Disorder. Journal of Family Practice, 55, 329-333.
• Visser, S., and Bouman, T. K. (2001). The treatment of hypochondriasis: Exposure plus response prevention vs cognitive therapy. Behaviour Research and Therapy, 39, 423-442.
• Watson, H. J., & Rees, C. S. (2008). Meta-analysis of randomized, controlled treatment trials for pediatric obsessive-compulsivedisorder. Journal of Child Psychology and Psychiatry, 49, 489–498.
• Wilhelm, S., Deckersbach, T., Coffey, B.J., Bohne, A., Peterson, A.L., & Baer, L. (2003). Habit reversal versus supportive psychotherapy for Tourette disorder: A randomized controlled trial. American Journal of Psychiatry, 160, 1175–1177.
• Wilhelm & Steketee. (2006). Cognitive Therapy for Obsessive-Compulsive Disorder: A Guide for Professionals. New Harbinger Publications: Oakland, CA.
• Wilson, M., Bell-Dolan, D., & Beitman, B. (1997). Application of the stages of change scale in a clinical drug trial. Journal of Anxiety Disorders, 11, 395 – 408.
• Wewetzer, C., Jans, T., Müller, B., Neudörfl, A., Bücherl, U., Remschmidt, H., et al. (2001). Long-term outcome and prognosis of obsessive-compulsive disorder with onset in childhood or adolescence. European child & adolescent psychiatry, 10, 37-46.
• Woods, D. W., Wetterneck, C. T., & Flessner, C. A. (2006). A controlled evaluation of acceptance and commitment therapy plus habit reversal for trichotillomania. Behaviour Research and Therapy, 44, 639-656.