nash: beyond the acronym, certainties and clinical dilemmas
TRANSCRIPT

NASH: BEYOND THE ACRONYM, CERTAINTIES AND CLINICAL DILEMMAS12-14 MAY 2016 RIGA, LATVIA
Scientific Organising CommitteeJean-François Dufour, Bern, SwitzerlandManuel Romero-Gomez, Sevilla, SpainVlad Ratziu, Paris, France
www.easl.eu

Follow the colour codes and pictogrammes throughout this book to find the sessions of interest to you!
What’s your colour?
Cholestatic and autoimmune
Viral hepatitis
Liver tumoursCirrhosis and complications
General hepatology
Metabolic, alcohol and toxicity
Specialties
FieldsLiver transplant and surgery
Public health
Basic and translational science
Imaging and interventional
C
M
J
CM
MJ
CJ
CMJ
N
2. What's your colour.pdf 1 18.03.16 14:08

3EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016Follow the colour codes and pictogrammes throughout this book to find the sessions of interest to you!
What’s your colour?
Cholestatic and autoimmune
Viral hepatitis
Liver tumoursCirrhosis and complications
General hepatology
Metabolic, alcohol and toxicity
Specialties
FieldsLiver transplant and surgery
Public health
Basic and translational science
Imaging and interventional
C
M
J
CM
MJ
CJ
CMJ
N
2. What's your colour.pdf 1 18.03.16 14:08
CONTENTS
Welcome message..........................................................................................................................................................................................................................5
Committees ............................................................................................................................................................................................................................................6
Acknowledgements .......................................................................................................................................................................................................................7
General information .....................................................................................................................................................................................................................9
Scientific programme ...............................................................................................................................................................................................................13
ePoster sessions ............................................................................................................................................................................................................................19
Invited speakers’ abstracts .............................................................................................................................................................................................30
ePoster abstracts ..........................................................................................................................................................................................................................71

APPLY FOR AN EASLFELLOWSHIP PROGRAMME!
THE LEADING LIVER ASSOCIATION IN EUROPE
EASL Physician Scientist FellowshipApplications open from 30 April - 30 June 2016
APPLICATION CONDITIONS• No restrictions on applicant’s nationality• Leading European hosting institutions• Open to all registered EASL members
As a continuation of the Dame Sheila Sherlock EASL Fellowship Programs, this initia-tive aims at enabling physician-scientists to take a leave from their clinical duties and to spend 6 or 12 months in a research laboratory.
Physician Scientist Fellowship Program is open to all registered EASL members and applicants can apply for either:
• 6-month research fellowship of €20,000• 12-month research fellowship of €40,000
One 6-month and one 12-month fellowship will be awarded each year.
i For more information on application conditions, deadlines and details visit www.easl.eu
www.easl.eu

5EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
We are delighted to invite you to attend the EASL Monothematic Conference “NASH: Beyond the acronym: certainties and clinical dilemmas” in Riga, Latvia.
COVERED TOPICSNASHEpidemiologyDisease History and PrognosticDiagnosis ProgressDisease Management
TARGETED AUDIENCEHepatologistsPhysicians with interest in HepatologyResearchers in the field of NASHHealth professionalsYoung researchers and trainees
WHY ATTEND?The latest on NASH diagnosis and managementCutting edge clinical research on NASHNetwork with renowned specialists and leading experts
Prof. Jean-François DufourBern, Switzerland
Prof. Manuel Romero-GómezSevilla, Spain
Prof. Vlad RatziuParis, France
WELCOME MESSAGE

6 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Prof. Jean-François Dufour, Bern, SwitzerlandProf. Manuel Romero-Gómez, Sevilla, SpainProf. Vlad Ratziu, Paris, France
EASL GOVERNING BOARD SECRETARY GENERALLaurent Castera, Paris, France
VICE-SECRETARYTom Hemming Karlsen, Oslo, Norway
TREASURERMauro Bernardi, Bologna, Italy
SCIENTIFIC COMMITTEE MEMBERSAnnalisa Berzigotti, Bern, SwitzerlandAlejandro Forner, Barcelona, SpainMarco Marzioni, Ancona, ItalyPhilip N. Newsome, Birmingham, United KingdomFrank Tacke, Aachen, Germany
EDUCATIONAL COUNCILLORSMassimo Pinzani, London, United KingdomFrancesco Negro, Geneva, Switzerland
EU POLICY COUNCILLORSHelena Cortez-Pinto, Lisbon, Portugal
EXECUTIVE DIRECTORGregoire Pavillon, Aclens, Switzerland
SCIENTIFIC ORGANISING COMMITTEE

7EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
ACKNOWLEDGEMENTS
PREMIUM SPONSORS
EASL thanks its Premium Sponsors for their generous contributions and support of the EASL Monothematic Conference: "NASH: Beyond the acronym, certainties and clinical dilemmas" with an unrestricted educational grant.

LIVER FIBROSIS: THE NEXT GOAL OF TARGETED THERAPY? 17-18 JUNE 2016 PORTO, PORTUGAL
www.easl.eu/_events
Scientific Organising CommitteeSophie Lotersztajn, Creteil, France Massimo Pinzani, London, UKChristian Trautwein, Aachen, Germany
www.easl.eu
JOIN US IN PORTOREGISTER TODAY!

GENERAL INFORMATION

GE
NE
RA
L IN
FOR
MA
TIO
N
10 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
GENERAL INFORMATION
CONFERENCE VENUERadisson Blu Hotel Latvija, Elizabetes 55 LV-1010,Riga, Latvia
DISCOVER RIGACity website: http://www.latvia.travel/en/city/riga-8
Riga, the capital of Latvia, is the pearl both of Latvia and the whole of the Baltics. Riga is included in the UNESCO World Cultural and Natural Heritage list. It is located in the central part of the country, on the South coast of the Gulf of Riga, at the mouth of the largest river, the Daugava. Riga is home for more than 700,000 inhabitants and is the largest city in the Baltic States.
As Riga has developed at the crossroads of trade, the metropolis has become a multicultural city in which one can always find a large number of things that are of interest. Each century has left its mark in the city’s features. They can be seen in the architecture of the Old Town and the City Centre. This cultural heritage coexists harmoniously with the quick pace of modern living.
LANGUAGEThe official language of the conference is English.
CLIMATERiga has a humid continental climate with warm summers and no dry season. The month of May is characterized by rising daily high temperatures, with daily highs increasing from 16°C to 20°C over the course of the month, exceeding 25°C or dropping below 9°C only one day in ten.
NAME BADGESAll participants are kindly requested to wear their name badges throughout the EASL Monothematic Conference in order to be admitted to the lecture halls and other scheduled activities.
REGISTRATION AND ACCOMMODATIONAll participants are invited to register online in order to save time upon their arrival at the conference.
Hotel accommodation for the EASL Monothematic Conference will be offered to participants during the online registration process. Detailed information, as well as access to the online registration is available on the website. Registered participants are entitled to reduced rates in the conference hotel.
REGISTRATION DESKThe on-site registration desk at the conference venue will be open at the following times:Thursday 12 May 2016 12:00 – 19:30Friday 13 May 2016 08:30 – 18:00Saturday 14 May 2016 08:30 – 11:30

GE
NE
RA
L IN
FOR
MA
TIO
N
11EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
CME ACCREDITATIONThe European Association for the Study of the Liver (EASL) is accredited by the European Accreditation Council for Continuing Medical Education (EACCME) to provide the following CME activity for medical specialists. The EACCME is an institution of the European Union of Medical Specialists (UEMS), www.uems.net. The EASL Monothematic Conference Conference: “NASH: Beyond the acronym, certainties and clinical dilemmas” is designated for a maximum of (or ‘for up to’) 12 hours of European external CME credits. Each medical specialist should claim only those hours of credit that he/she actually spent in the educational activity. Through an agreement between the European Union of Medical Specialists and the American Medical Association, physicians may convert EACCME credits
to an equivalent number of AMA PRA Category 1 Credits™. Information on the process to convert EACCME credit to AMA credit can be found at http://www.ama-assn.org/go/internationalcme Live educational activities, occurring outside of Canada, recognized by the UEMS-EACCME for ECMEC credits are deemed to be Accredited Group Learning Activities (Section 1) as defined by the Maintenance of Certification Program of The Royal College of Physicians and Surgeons of Canada. EACCME credits. Each medical specialist should claim only those hours of credit that he/she actually spent in the educational activity. The EACCME credit system is based on 1 ECMEC per hour with a maximum of 3 ECMECs for half a day and 6 ECMECs for a full-day event.
ACCESS RIGADirect flights are available from the European airports listed below to the Riga International Airport (RIX):
AUSTRIA BELGIUM FRANCE GERMANY IRELAND
Vienna BrusselsCharleroi
Paris BerlinBremenCologneDusseldorfFrankfurt
Dublin
ITALY NETHERLANDS NORWAY SWITZERLAND UNITED KINGDOM
Milan Amsterdam Oslo BaselZurichGeneva
DoncasterEast MidlandsGlasgowLeeds London

GE
NE
RA
L IN
FOR
MA
TIO
N
12 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
GENERAL INFORMATION
TRANSPORT TO THE VENUEThe conference venue, Radisson Blu Hotel Latvija, is 20 minutes by taxi from Riga International Airport (RIX).
By public transportTake the bus 22 from Abrenes iela to Melnsila iela. Then, take the bus 53 to Esplan de. Walk 200 meters to Elizabetes iela, the Radisson Blu Latvija is across the street.
By carTake along the P133 motorway, then take the A10 in direction of the centre. Turn left on Lielirbes iela, then keep on for 1 Km and then turn right on Elizabetes iela, the Radisson Blu Hotel Latvija is on your right-hand side.
DRESS CODE AND SMOKING POLICYDress code is informal for all occasions. This will be a non-smoking event.
BANKING, SAFETY AND SECURITYThe currency used in Latvia is the EURO. Foreign currency can be exchanged at banks, bureau de change and automatic currency exchange machines.
Please do not leave bags or suitcases unattended at any time, whether inside or outside the session halls. Hotels strongly recommend that you use their safety deposit boxes for your valuables.
LIABILITY AND INSURANCEThe EASL Office cannot accept liability for personal accidents or loss of or damage to private property of participants. Participants are advised to take out their own personal travel and health insurance for their trip.

SCIENTIFICPROGRAMME

SC
IEN
TIF
IC P
RO
GR
AM
ME
14 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
SCIENTIFIC PROGRAMME
DAY 1 – THURSDAY 12 MAY 2016
12:00 – 14:00 Registration
13:00 – 14:00 ePoster presentations 1
1. EPIDEMIOLOGY
Chair: Vlad Ratziu, France
14:00 – 14:30 CURRENT EPIDEMIOLOGICAL TRENDS IN THE WEST, EAST AND DEVELOPING COUNTRIES Jorn Schattenberg, Germany
14:30 – 15:00 ePoster presentations 2
2. ASSESSING INDIVIDUAL RISK
Chair: Fabio Marra, Italy
15:00 – 15:30 ALCOHOL CONSUMPTION: BETWEEN HARM AND BENEFIT. HOW MUCH, IF ANY, ALCOHOL ARE PATIENTS ALLOWED TO DRINK? Ramón Bataller, United States
15:30 – 16:00 NASH AFTER NAP: COFFEE AND CANNABIS Rodolphe Anty, France
16:00 – 16:30 CLINICAL CASE 1. DIFFERENTIAL DIAGNOSIS NASH – DILI Raúl Andrade, Spain
16:30 – 17:00 GENES AND miRNAs: BIOLOGY AND CLINICAL ASSOCIATIONS Quentin Anstee, United Kingdom

SC
IEN
TIF
IC P
RO
GR
AM
ME
15EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
17:00 – 17:30 ePoster presentations 3 and coffee break
3. NATURAL HISTORY AND PROGNOSTIC STUDIES
Chair: Jean-François Dufour, Switzerland
17:30 – 18:00 RISK OF PROGRESSION IN EARLY DISEASE Raluca Pais, France
18:00 – 18:30 NATURAL HISTORY OF NASH Leon Adams, Australia
18:30 – 19:00 CIRRHOSIS AND LIVER RELATED MORTALITY IN NASH Matias Ekstedt, Sweden
19:00 – 19:30 HEPATOCELLULAR CARCINOMA: CURRENT TRENDS IN NAFLD Helen Reeves, United Kingdom
19:30 ePoster presentations 4 and cocktail reception
DAY 2 – FRIDAY 13 MAY 2016
08:30 – 09:00 ePoster presentations 5
4. ASSOCIATED PATHOGENIC CONDITIONS IN NAFLD
Chair: Ramón Bataller, United States
09:00 – 09:30 DIAGNOSIS AND NATURAL HISTORY: WHAT SHOULD THE HEPATOLOGIST KNOW ABOUT DIABETES? Amalia Gastaldelli, Italy
09:30 – 10:00 GUT MICROBIOTA & NASH Herbert Tilg, Austria
10:00 – 10:30 METABOLICALLY HEALTHY OBESE INDIVIDUALS: FACT OR FICTION? Konstantinos Kantartzis, Germany

SC
IEN
TIF
IC P
RO
GR
AM
ME
16 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
10:30 – 11:00 ePoster presentations 6 and coffee break
11:00 – 11:30 OBSTRUCTIVE SLEEP APNEA - AN OVERLOOKED DIAGNOSIS THAT CAN WORSEN NASH Judith Aron-Wisnewski, France
11:30 – 12:00 ASSOCIATION OF NAFLD WITH CHRONIC KIDNEY DISEASE Sven Francque, Belgium
12:00 – 12:30 NASH & CARDIOVASCULAR DISEASE Javier Ampuero, Spain
12:30 – 13:00 CLINICAL CASE 2: PREDICTING OUTCOMES IN NASH Jean-François Dufour, Switzerland
13:00 – 14:00 Lunch
13:30 – 14:00 ePoster presentations 7
5. PROGRESS IN DIAGNOSIS
Chair: Elisabetta Bugianesi, Italy
HISTOLOGY
14:00 – 14:30 CURRENT CLASSIFICATIONS AND THEIR LIMITATIONS Dina Tiniakos, United Kingdom
14:30 – 15:00 NASH WITH ADVANCED FIBROSIS AND HCV AND WILSON’S DISEASE MASQUERADING NASH Carolin Lackner, Austria
NON-INVASIVE ASSESSMENT OF STEATOSIS, NASH AND FIBROSIS
15:00 – 15:30 SERUM MARKERS Emmanuel Tsochatzis, United Kingdom
15:30 – 16:00 ELASTOMETRY Salvatore Petta, Italy

SC
IEN
TIF
IC P
RO
GR
AM
ME
17EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
16:00 – 16:30 ePoster presentations 8 and coffee break
16:30 – 17:00 NEW IMAGING TECHNIQUES Rohit Loomba, United States
17:00 – 17:30 METABOLOMIC Malu Martínez-Chantar, Spain
17:30 – 18:00 THE SEARCH FOR INNOVATIVE MARKERS: FROM IMAGING TO EPIGENETIC BIOMARKERS Manuel Romero-Gómez, Spain
DAY 3 – SATURDAY 14 MAY 2016
08:30 – 09:00 ePoster presentations 9
6. MECHANISMS OF NASH PROGRESSION
Chair: Manuel Romero-Gomez, Spain
09:00 – 09:30 CARCINOGENESIS IN NAFLD: MECHANISMS Mathias Heikenwälder, Germany
09:30 – 10:00 FIBROGENESIS IN NAFLD: MECHANISM Fabio Marra, Italy
10:00 – 10:30 CHEMOKINES, MYOKINES AND ADIPOKINES IN NASH Carmelo García-Monzón, Spain
10:30 – 11:00 CLINICAL CASE 3: THE CHALLENGES OF MONITORING NAFLD Helena Cortez-Pinto, Portugal
11:00 – 11:30 ePoster presentations 10 and coffee break

SC
IEN
TIF
IC P
RO
GR
AM
ME
18 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
7. MANAGEMENT OF NAFLD
Chair: Manuel Romero-Gomez, Spain
11:30 – 12:00 INTRODUCTION TO BARIATRIC SURGERY: TECHNIQUES, SHORT TERM AND LONG-TERM RESULTS AND COMPLICATIONS Salvador Morales, Spain
12:00 – 12:30 MACRO AND MICRONUTRIENTS IN NASH Shira Zelber-Sagi, Israel
12:30 – 13:00 THE BENEFITS OF EXERCISE: HOW TO PRESCRIBE? Mike Trenell, United Kingdom
13:00 – 13:30 WEIGHT LOSS IN NASH: MANAGEMENT AND BENEFICIAL ASPECTS Eduardo Vilar, Spain
13:30 – 14:00 CURRENT INSULIN SENSITIZING AGENTS IN NASH Philip Newsome, United Kingdom
14:00 – 14:30 THE PROMISE OF FUTURE DRUGS IN NASH Vlad Ratziu, France
14:30 CONCLUDING REMARKS Jean-Francois Dufour, SwitzerlandManuel Romero-Gómez, SpainVlad Ratziu, France

ePosterSESSIONS

ePO
ST
ER
SE
SS
ION
S
20 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
THURSDAY 12 MAY 2016ePoster presentations 1: 13:30 – 14:00
Screen Title Abstract Presenter
1 DYSMETABOLIC IRON OVERLOAD SYNDROME IN NON-ALCOHOLIC FATTY LIVER DISEASE PATIENTS
MR-146 Claudia Oliveira
2 EVALUATION OF HEPATOCELLULAR CARCINOMA (HCC) BY 18 FDG MICROPET-CT ON EXPERIMENTAL MIXED RODENT MODEL OF NONALCOHOLIC STEATOHEPATITIS (NASH)-RELATED HCC
MR-102 Leila Mouelhi
3 PNPLA3 AND TNF-α G238A GENETIC POLYMORPHISMS IN EGYPTIAN PATIENTS WITH DIFFERENT GRADES OF SEVERITY OF NAFLD.
MR-163 Mona Hegazy
4 THE CONTROLLED ATTENUATION PARAMETER (CAP) IN NAFLD AND OTHER NON-ALCOHOLIC CHRONIC LIVER DISEASES: SHOULD IT BE CONSIDERED A DIAGNOSTIC CRITERIA FOR METABOLIC SYNDROME?
MR-117 Rosa Coelho
5 REFRACTORY SUBACUTE STEATOHEPATITIS AFTER BILIOPANCREATIC DIVERSION: A CASE REPORT
MR-124 Sander Lefere
6 CONTROLLED ATTENUATION PARAMETER AND LIVER STIFFNESS MEASUREMENTS BY FIBROSCAN FOR THE DETECTION OF NON-ALCOHOLIC FATTY LIVER DISEASE IN PATIENTS WITH TYPE 2 DIABETES: RESULTS FROM A PILOT STUDY
MR-106 Yusuf Yilmaz

ePO
ST
ER
SE
SS
ION
S
21EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
ePoster presentations 2: 14:30 – 15:00
Screen Title Abstract Presenter
1 CORONARY ARTERY CALCIUM SCORE (CACS) AND FRAMINGHAM SCORE (FS) IN EVALUATION OF CARDIOVASCULAR RISK AFTER LIVER TRANSPLANTATION.
MR-103 Claudia Oliveira
2 PREVALENCE AND CHARACTERISTICS OF PATIENTS WITH OBESE VERSUS NON-OBESE NON-ALCOHOLIC FATTY LIVER DISEASE (NAFLD) IN THAILAND
MR-133 Chalermrat Bunchorntavakul
3 CHANGES OF THE GUT MICROBIOTA IN PATIENTS WITH OBESITY, METABOLIC SYNDROME AND NONALCOHOLIC FATTY LIVER DISEASE (NAFLD) VERSUS HEALTHY CONTROLS
MR-160 María Teresa Arias Loste
4 INTERVENTION WITH THE CCR2 INHIBITOR PROPAGERMANIUM ATTENUATES INSULIN RESISTANCE, ADIPOSE TISSUE INFLAMMATION AND DEVELOPMENT OF NASH
MR-161 Petra Mulder
5 NORUDCA IMPROVES LIVER INJURY AND GLUCOSE SENSITIVITY IN MOUSE MODELS OF OBESITY AND STEATOSIS
MR-164 Daniel Steinacher
6 ASSOCIATION BETWEEN LEFT VENTRICULAR MASS AND HEPATIC FAT CONTENT IN PATIENTS WITH NON-ALCOHOLIC FATTY LIVER DISEASE
MR-178 Daniele Pastori

ePO
ST
ER
SE
SS
ION
S
22 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
ePoster presentations 3: 17:00 – 17:30
Screen Title Abstract Presenter
1 EVALUATION OF HEPATOCELLULAR CARCINOMA (HCC) BY 18 FDG MICROPET-CT ON EXPERIMENTAL MIXED RODENT MODEL OF NONALCOHOLIC STEATOHEPATITIS (NASH)-RELATED HCC
MR-102 Claudia Oliveira
2 HIGH INCIDENCE OF NON-ALCOHOLIC FATTY LIVER DISEASE IN FIRST EPISODE SCHIZOPHRENIA SPECTRUM PATIENTS: A 3 YEARS PROSPECTIVE STUDY
MR-162 María Teresa Arias Loste
3 OBETICHOLIC ACID ATTENUATES FIBROSIS DEVELOPMENT IN A HIGH-FAT DIET INDUCED NASH MODEL (LDLR-/-.LEIDEN MICE)
MR-167 Petra Mulder
4 EXERCISE THERAPY IN PATIENTS CONSUMING MODERATE ALCOHOL: A RANDOMISED CONTROL TRIAL
MR-105 David Houghton
5 FATTY LIVER INDEX (FLI) AS A MULTIDISCIPLINARY SCORE NOT ONLY FOR A CORRECT DIAGNOSIS OF NONALCOHOLIC FATTY LIVER DISEASE (NAFLD) BUT ALSO TO IMPROVE ACCURACY IN CARDIOVASCULAR DISEASE IN DIABETIC TYPE 2 PATIENTS
MR-130 Diego Caroli
6 TM6SF2 KO AND PNPLA3 I148M KNOCKIN MICE AS NAFLD ANIMAL MODELS: SIMILAR BUT NOT THE SAME.
MR-109 Eriks Smagris

ePO
ST
ER
SE
SS
ION
S
23EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
ePoster presentations 4: 19:30 – 20:00
Screen Title Abstract Presenter
1 IMPACT OF AEROBIC EXERCISE IN POSTMENOPAUSAL WOMEN WITH NONALCOHOLIC FATTY LIVER DISEASE: A 24 - WEEK RANDOMIZED CLINICAL TRIAL
MR-108 Claudia Oliveira
2 THE FTO RS1421085 T>C POLYMORPHISM IS ASSOCIATED WITH THE SEVERITY OF NON-ALCOHOLIC FATTY LIVER
MR-168 María Teresa Arias Loste
3 SILIBININ EXERTS BENEFICIAL EFFECTS ON GUT-LIVER AXIS IN MURINE AND HUMAN NON-ALCOHOLIC FATTY LIVER DISEASE
MR-192 Federico Salomone
4 MOLECULAR CHARACTERIZATION OF THE FECAL MICROBIOME IN BRAZILIAN NASH OBESE AND OBESE WITHOUT NASH PATIENTS COMPARED TO LEAN HEALTHY CONTROLS
MR-115 Hugo Brito
5 SMOKING IS ASSOCIATED WITH FIBROSIS BUT NOT WITH NAFLD ACTIVITY
MR-134 Isabelle Munsterman
6 CIRCULATING MICRORNAS IN PATIENTS WITH NON-ALCOHOLIC FATTY LIVER DISEASE IN TAIWAN
MR-143 Jee-Fu Huang

ePO
ST
ER
SE
SS
ION
S
24 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
FRIDAY 13 MAY 2016ePoster presentations 5: 08:30 – 09:00
Screen Title Abstract Presenter
1 HYPOLACTASIA (LCT-13910CC GENOTYPE) IS ASSOCIATED WITH INSULIN RESISTANCE IN BRAZILIAN PATIENTS WITH NONALCOHOLIC STEATOHEPATITIS (NASH)
MR-110 Claudia Oliveira
2 POSSIBILITY OF GHRELIN AS NON-INVASIVE MARKER FOR NAFLD/NASH DIAGNOSIS
MR-126 Nazarii Kobyliak
3 SECRETOME PROFILES OF HUMAN MESENCHYMAL STEM CELLS BEFORE AND AFTER HEPATOCYTIC DIFFERENTIATION – IDENTIFICATION OF PATHWAYS IMPACTING ON POTENTIAL TREATMENT OF NASH
MR-129 Sandra Winkler
4 MELANIN PRODUCED BY YEAST NADSONIELLA NIGRA AS NOVEL THERAPEUTICS AGENTS IN NAFLD/NASH MANAGEMENT
MR-181 Savytska Maryana
5 THE BERLIN QUESTIONNAIRE SCREENS AND EPWORTH SLEEPINESS SCALE FOR OBSTRUCTIVE SLEEP APNEA IN NON-ALCOHOLIC FATTY LIVER DISEASE.
MR-195 Bochra Bouchabou
6 AN OPEN LABEL RANDOMIZED CONTROLLED TRIAL OF VITAMIN D VS PENTOXIFYLLINE IN NON-DIABETIC PATIENTS OF NAFLD
MR-149 Sanchit Budhiraja

ePO
ST
ER
SE
SS
ION
S
25EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
ePoster presentations 6: 10:30 – 11:00
Screen Title Abstract Presenter
1 MOLECULAR CHARACTERIZATION OF THE FECAL MICROBIOME IN BRAZILIAN NASH OBESE AND OBESE WITHOUT NASH PATIENTS COMPARED TO LEAN HEALTHY CONTROLS
MR-115 Claudia Oliveira
2 SYNERGISTIC EFFECT OF ALIVE PROBIOTIC AND ABSORBENT SMECTITE GEL FOR NAFLD/NASH PREVENTION: EXPERIMENTAL STUDY
MR-171 Nazarii Kobyliak
3 LIVER AND SYSTEMIC IRON LOADING CHARACTERISE INITIAL DISEASE PROGRESSION IN NAFLD
MR-184 John Ryan
4 DIAGNOSTIC ACCURACY OF SHEAR WAVE ELASTOGRAPHY FOR THE ASSESSMENT OF LIVER STIFFNESS IN CHILDREN WITH FATTY LIVER DISEASE
MR-174 Matteo Garcovich
5 ADIPOSE TISSUE INSULIN RESISTANCE IS ASSOCIATED WITH MACROPHAGE ACTIVATION IN NON-DIABETIC PATIENTS WITH NON ALCOHOLIC FATTY LIVER DISEASE
MR-150 Milena Marietti
6 PATATIN-LIKE PHOSPHOLIPASE DOMAIN-CONTAINING PROTEIN 3 POLYMORPHISM AND THE RISK OF HEPATOCELLULAR CARCINOMA DEVELOPMENT IN RELATION TO UNDERLYING LIVER DISEASES
MR-152 Pisit Tangkijvanich

ePO
ST
ER
SE
SS
ION
S
26 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
ePoster presentations 7: 13:30 – 14:00
Screen Title Abstract Presenter
1 COMPARATIVE ANALYSIS OF ONLINE PATIENT EDUCATION RESOURCES PERTAINING TO NASH OR NAFLD
MR-172 Rishabh Gulati
2 IMPACT OF GWAS-IDENTIFIED COMMON VARIANTS ON HISTOPATHOLOGICAL FEATURES OF NAFLD PATIENTS
MR-159 Rocío Gallego-Durán
3 NASH: AN UNDERECOGNIZED CAUSE OF CRYPTOGENIC CIRRHOSIS
MR-182 Rym Ennaifer
4 HIGH RISK POPULATIONS: ATTITUDES TO NAFLD AMONG DIABETOLOGISTS
MR-136 Thomas Marjot
5 THE RECOGNITION OF OXIDIZED LIPIDS BY IGM ANTIBODIES IS AN EARLY EVENT IN THE PATHOGENESIS OF HUMAN NON-ALCOHOLIC FATTY LIVER DISEASE
MR-154 Tim Hendrikx
6 ASSOCIATION OF PRO12ALA POLYMORPHISM OF PPAR-γ GENE WITH BIOCHEMICAL MARKERS OF LIVER INJURY IN NONALCOHOLIC FATTY LIVER DISEASE PATIENTS
MR-104 Vasyl Prysyazhnyuk

ePO
ST
ER
SE
SS
ION
S
27EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen Title Abstract Presenter
1 ELAFIBRANOR, A LIVER TARGETED PPARα/δ AGONIST FOR GLOBAL MANAGEMENT OF NASH
MR-210 Dean Hum
2 VALIDATION OF NON-INVASIVE METHODS FOR ADVANCED FIBROSIS DETECTION IN NAFLD PATIENTS
MR-169 Rocío Gallego-Durán
3 ARE FEMALES REALLY MORE PROTECTED THAN MALES IN THE PROGRESSION FROM NAFLD TO NASH?
MR-144 Veronica Marin
4 REGENERATE: A PHASE 3, DOUBLE-BLIND, RANDOMIZED, PLACEBO-CONTROLLED MULTICENTER STUDY OF OBETICHOLIC ACID THERAPY FOR NONALCOHOLIC STEATOHEPATITIS
MR-147 Vlad Ratziu
5 SARCOPENIA IS AN INDEPENDENT RISK FACTOR FOR BIOPSY-PROVEN NON-ALCOHOLIC STEATOHEPATITIS IN A KOREAN POPULATION
MR-180 Won Kim
6 LEAN VERSUS OVERWEIGHT/OBESE NONDIABETIC NONALCOHOLIC FATTY LIVER DISEASE (NAFLD) – A CLINICOPATHOLOGICAL COMPARATIVE STUDY
MR-120 Sanchit Budhiraja
ePoster presentations 8: 16:00 – 16:30

ePO
ST
ER
SE
SS
ION
S
28 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
SATURDAY 14 MAY 2016ePoster presentations 08:30 – 09:00
Screen Title Abstract Presenter
1 HEPATOCELLULAR CARCINOMA IN NON-ALCOHOLIC STEATOHEPATITIS (NASH) – HISTOPATHOLOGICAL ASPECTS
MR-125 Claudia Oliveira
2 LIVER STIFFNESS VALUES MEASURED BY SHEAR WAVE ELASTOGRAPHY DEPENDING ON TRANSAMINASE ACTIVITY IN PATIENTS WITH NONALCOHOLIC FATTY LIVER DISEASE
MR-121 Nazarii Kobyliak
3 LYSOSOMAL ACID LIPASE ACTIVITY IS ASSOCIATED WITH AST TO PLATELET RATIO INDEX IN PATIENTS WITH NON-ALCOHOLIC FATTY LIVER DISEASE
MR-173 Francesco Baratta
4 NON-ALCOHOLIC FATTY LIVER DISEASE PATIENT’S PROFILE IN LATVIA
MR-137 Jekaterina Kucina
5 RESVERATROL IMPROVES HEPATIC NITRIC OXIDE SYNTHESIS AND ATTENUATING ENDOTHELIAL DYSFUNCTION IN NON-ALCOHOLIC FATTY LIVER DISEASE
MR-128 Balasubramaniyan Vairappan
6 SPLEEN DIMENSIONS EVALUATED BY ULTRASOUND ARE INVERSELY ASSOCIATED WITH LYSOSOMAL ACID LIPASE ACTIVITY IN PATIENTS WITH NON-ALCOHOLIC FATTY LIVER DISEASE
MR-179 Licia Polimeni

ePO
ST
ER
SE
SS
ION
S
29EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
ePoster presentations 10: 11:00 – 11:30
Screen Title Abstract Presenter
1 CYTOKERATIN 18 FRAGMENT LEVEL IS A USEFUL BIOMARKER IN PREDICTING STEATOSIS AND NASH BUT NOT FIBROSIS
MR-148 Sanchit Budhiraja
2 NATURAL EXTRACTS ABOLISH LIPID ACCUMULATION IN CELLS HARBOURING NON-FAVOURABLE PNPLA3 GENOTYPE
MR-165 Ángela Rojas
3 PRIMARY CARE SEQUENTIAL USE OF FIB-4 AND THE ENHANCED LIVER FIBROSIS TEST TO STRATIFY PATIENTS WITH NAFLD DOUBLES CIRRHOSIS DETECTION AND REDUCES REFERRALS OF PATIENTS WITH MILD DISEASE
MR-132 Ankur Srivastava
4 TOWARDS A NON-INVASIVE DIAGNOSIS OF NON-ALCOHOLIC STEATO HEPATITIS (NASH)
MR-145 Carla M. Chackelevicius
5 ANGIOPOIETIN-LIKE4 IS ASSOCIATED WITH LIPID METABOLISM AND SEVERE FIBROSIS IN NON-DIABETIC PATIENTS WITH NON ALCOHOLIC FATTY LIVER DISEASE
MR-151 Chiara Rosso
6 ASSOCIATION BETWEEN SEVERITY OF NONALCOHOLIC FATTY LIVER DISEASE AND THE RATIOS OF CHOLESTEROL AND TRIGLYCERIDES
MR-135 Chia-Yen Dai

INVITED SPEAKERS’ ABSTRACTS

SP
EA
KE
RS
’ AB
ST
RA
CT
S
31EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
NASH AFTER NAP: COFFEE AND CANNABIS
Rodolphe Anty* 1
1Hepatology unit, Digestive department, University Hospital of Nice, INSERM U1065, Nice, France
Corresponding author’s email: [email protected]
The impact of coffee and cannabis on Non-alcoholic fatty liver diseases (NAFLD) differ.In the case of coffee consumption-a legal substance- numerous epidemiological studies have studied the impact of various coffee preparations on NAFLD, NASH and liver fibrosis. In the case of cannabis –an illegal substance in most countries (at least for recreational purpose)- very few epidemiological studies assessing cannabis consumption on liver diseases are available.Coffee consumption seems to be protective for liver fibrosis during NAFLD [1-3]. While cannabis consumption seems to be deleterious in chronic hepatitis C and may be deleterious during NAFLD, however little epidemiological data are available [4].A substantial number of compounds are contained in coffee and cannabis and the number of studies in the literature concerning these two products is very different [5, 6]. In the case of coffee consumption, potential beneficial compounds and mechanisms for fatty liver protection remain speculative [7]. In contrast, the discovery of the endocannabinoid system has lead to a lot of research into many organs (from the brain to the adipose tissue) due to the fact that it is implicated in many physiological pathways [8]. The discovery of the cannabinoid receptors 1 (CB1) and 2 (CB2), which have opposite effects in many organs, came as a breakthrough in the understanding of this system. In the liver, stimulation of CB1 may impair liver fibrosis while stimulation of CB2 may improve inflammation and fibrosis [9]. While the first patented drug rimonabant –an inverse agonist of CB1- given to lose weight and improve the metabolic profile has been removed from the market due to adverse effects on the central nervous system, the modulation of the endocannabinoid system by organ specific drugs could be a new way of treatment for patients with NAFLD [9].In summary, cannabis users are exposed to potential beneficial or deleterious substances. New research into agonists/inverse agonists of endocannabinoid receptors is promising. Identification of the beneficial compounds and a better the understanding of their signaling pathways could be helpful in the field of the NAFLD/NASH. In the meantime, patients should be advised to drink regularly coffee without sweetener and to restrain from smoking cannabis (or tobacco).

SP
EA
KE
RS
’ AB
ST
RA
CT
S
32 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
References[1] Molloy JW, Calcagno CJ, Williams CD, Jones FJ, Torres DM, Harrison SA. Association of coffee and caffeine
consumption with fatty liver disease, nonalcoholic steatohepatitis, and degree of hepatic fibrosis. Hepatology 2011;10:24731.
[2] Anty R, Marjoux S, Iannelli A, Patouraux S, Schneck AS, Bonnafous S, et al. Regular coffee but not espresso drinking is protective against fibrosis in a cohort mainly composed of morbidly obese European women with NAFLD undergoing bariatric surgery. J Hepatol 2012;57:1090-1096.
[3] Shen H, Rodriguez AC, Shiani A, Lipka S, Shahzad G, Kumar A, et al. Association between caffeine consumption and nonalcoholic fatty liver disease: a systemic review and meta-analysis. Therap Adv Gastroenterol 2016;9:113-120.
[4] Hezode C, Roudot-Thoraval F, Nguyen S, Grenard P, Julien B, Zafrani ES, et al. Daily cannabis smoking as a risk factor for progression of fibrosis in chronic hepatitis C. Hepatology 2005;42:63-71.
[5] Muriel P, Arauz J. Coffee and liver diseases. Fitoterapia 2010;81:297-305.[6] Andre CM, Hausman JF, Guerriero G. Cannabis sativa: The Plant of the Thousand and One Molecules. Front
Plant Sci 2016;7:19.[7] Saab S, Mallam D, Cox GA, 2nd, Tong MJ. Impact of coffee on liver diseases: a systematic review. Liver
international : official journal of the International Association for the Study of the Liver 2014;34:495-504.[8] Mouslech Z, Valla V. Endocannabinoid system: An overview of its potential in current medical practice. Neuro
Endocrinol Lett 2009;30:153-179.[9] Mallat A, Teixeira-Clerc F, Lotersztajn S. Cannabinoid signaling and liver therapeutics. J Hepatol 2013;59:891-
896.
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
33EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
CLINICAL CASE 1.DIFFERENTIAL DIAGNOSIS NASH – DILI
Raul J. Andrade* 1, 2, 3 on behalf of Spanish DILI Registry and Spanish DILI Registry1Medicine, UNIVERSITY OF MÁLAGA, 2IBIMA, Virgen de la Victoria University Hospital, 3CIBERehd, Málaga, Spain
Corresponding author’s email: [email protected]
A 44-year-old-woman started tamoxifen on January 2003 after breast cancer surgery. Her baseline liver biochemistry showed, AST 68 U/L (normal < 35), ALT 86 U/L (normal<43), and GGT 280 U/L (normal < 35), whereas TB (0.47 mg/dL) and ALP (80 U/L) where within normal range. She had no other underlying diseases or was taking concomitant treatments, except for lorazepam for insomnia during several years. On July 2003 she noticed jaundice and her liver profile was TB 1.85 mg/dL, AST 186 U/L, ALT 112 U/L, and GGT 446 U/L, with normal within ALP values. The liver enzymes improved except for TB that reached 3.68 mg/dL after five months and the treatment was discontinued in December 2003. The patient voluntary decided to reintroduce tamoxifen treatment three months later and on April 2004 was admitted to hospital with jaundice. The analytical values were TB 10.83 mg/dL, AST 154 U/L, ALT 47 U/L, ALP 132 U/L (normal < 100) and GGT 351 U/L. Serology ruled out viral causes and screening for autoantibodies was negative. Abdominal ultrasound showed a heterogeneous liver and hepatomegaly. A liver biopsy showed chronic liver disease with regenerative liver nodules and fibrosis, as well as mild steatosis.Idiosyncratic drug-induced liver injury (DILI) is a complex and multi-layered disorder that affects susceptible subjects exposed to therapeutic doses of drugs whose diagnosis remains largely of exclusion. While DILI is uncommonly diagnosed, non-alcoholic fatty liver disease (NAFLD) is highly prevalent due to the widespread occurrence of obesity and the metabolic syndrome in western countries. Because of this, distinguishing DILI from non-alcoholic fatty liver disease (NAFLD) and NASH is often a difficult task in the evaluation of suspected cases of hepatotoxicity. Actually, the growing prevalence of NAFLD recently led to a consensus group to raise the cut-off point of transaminases from > 2 X upper limit of normal (ULN) to 5 X ULN for consider a case as possible DILI in order to avoid the inclusion of many false positive cases of minor increases in transaminases of uncertain meaning. On the other hand, yet rarely, drugs can cause fat accumulation in the liver. Approximately 2% of NAFLD instances are believed to be caused by drugs. In contrast, some degree of liver steatosis is frequently encountered in liver biopsy specimens of DILI cases. Thus, a recent review of 249 of biopsies from the Drug Induced Liver Injury Network DILIN) indicated that although this is rarely described as the dominant pattern, 26% of cases showed some degree of steatosis, with macrovesicular steatosis as the dominant pattern in over 70% of the cases. However, it is difficult to ascertain the extent

SP
EA
KE
RS
’ AB
ST
RA
CT
S
34 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
to which fat accumulation in many of these cases is a hepatotoxic effect of the drug or it is simply a pre-existing liver lesion. Indeed, an interaction between DILI and NAFLD probably occurs in many instances, is complex and bidirectional. Although, whether NAFLD/NASH are risk factors for DILI is yet unproven, hepatotoxicity produced by drugs such as tamoxifen or methotrexate can aggravate underlying NAFLD and vice versa. Several components of the metabolic syndrome can influence DILI outcome. For example, diabetes mellitus was a risk factor for DILI severity in the DILIN experience, as was also for chronic outcome in the Spanish DILI Registry survey along with hypertension and hyperlipidemia. In contrast, hyperlipidemia was protective for the development of acute liver failure in Spanish DILI patients this effect probably being mediated by the use of statins. In the causality assessment of suspected DILI cases with known NAFLD, or risk factor for it such as obesity or metabolic syndrome the adjudication would be particularly difficult if the resulting pattern is hepatocellular because there is no specific biomarker to distinguish true DILI from a flare of transaminases typical of the natural course of NAFLD. The height of transaminase values along a rapid improvement after dechallenge with the suspected drug can be an important clue. For other phenotypes such as cholestasis or mixed injury the diagnosis of DILI can be more evident.
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
35EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
NAFLD NATURAL HISTORY: RISK OF PROGRESSION IN EARLY DISEASE
Raluca Pais* 1
1Hepatogastroenterology, Assistance Publique Hôpitaux de Paris, Hôpital Pitié-Salpétrière – Université Pierre et Marie Curie, UMR_S 938, INSERM – CDR Saint Antoine, Institute of Cardiometabolism and Nutrition (ICAN), Paris, France
Corresponding author’s email: [email protected]
The spectrum of NAFLD (non alcoholic fatty liver disease) encompasses two entities with distinct histological features: isolated steatosis (NAFL) with no/minimal inflammation and steatohepatitis (NASH). While lipid droplet accumulation within hepatocyte is the defining histological feature for NAFLD, the long-term outcomes seem to be determined by other histological lesions (lobular/portal inflammation, hepatocyte ballooning and fibrosis), which accompany steatosis in various degrees1.The current concept is that triglyceride (TG) storage as lipid droplets in the liver is an adaptive response to adipose tissue insulin resistance and has no harmful effect. Instead non-TG metabolites of fatty acids are responsible for lipotoxic liver injury and disease progression2. Blocking DGAT2 (diacylglycerol acyltransferase 2), the final enzyme catalyzing TG formation, results in less steatosis but more inflammation and fibrosis. These data suggests that there should be little or no transition from steatosis to NASH.Earlier studies failed to demonstrate any significant histological changes in patients with bland steatosis. Later studies confirmed that patients with bland steatosis have similar survival with general population while patients with NASH have increased overall, liver-related and CV mortality (Figure). However isolated cases of progression from steatosis to advanced fibrosis have been previously described. In the study of Ekstedt et al., among 36 patients with bland steatosis, 47% had fibrosis progression with 3 patients (8%) developing bridging fibrosis over 13 years of follow-up3.Recently, two studies with paired liver biopsies specifically analysed the evolution of patients with NAFL. Progression to bridging fibrosis occurred in almost one quarter of patients (24% over 3.7 years of follow-up in the French study and 22% over a median of 8 years of follow-up in the British study)4, 5. Although sampling error and interobserver variability are possible confounders, the striking reproducibility of the results of these two studies, most probably reflect unambiguous disease progression. Remarkably, fibrosis progression occurred together with the development of ballooning and transition to NASH. This highlights the prognostic significance of the histological lesions on the baseline biopsy, especially steatosis and inflammation. Fibrosis progression was associated with the persistence/aggravation of metabolic risk factors. In a recent meta-analysis, among 133 patients with NAFL, fibrosis progression occurred in 39% of patients at a mean rate of 1

SP
EA
KE
RS
’ AB
ST
RA
CT
S
36 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
stage over 14 years. Rapid fibrosis progression (from none to bridging fibrosis of cirrhosis) occurred in 17% of patients with NAFL over a short follow-up period of 6 years. When only patients with stage 0 or 1 fibrosis were analysed, fibrosis progression rate was similar between patients with NAFL and NASH6. This suggests that additional physiopathologic pathways might drive fibrosis progression in the “fast progressors” group.In conclusion, NAFL is not such a benign condition as initially believed and some patients are at risk for disease progression. Patients with NAFL might justify of similar surveillance rate as patients with NASH, at least in case of aggravation of metabolic risk factors. We should also keep in mind that if fibrosis is associated with long-term clinical outcomes, inflammation and ultimately NASH are the main drivers that precedes and play a key role in fibrosis progression. This justifies the current focus of clinical trials on the resolution of NASH. It also raises the question if pharmacological treatment should not be considered in earlier stages of the disease.
References 1. Angulo P, Kleiner DE, Dam-Larsen S, et al. Liver Fibrosis, but no Other Histologic Features, Associates with
Long-term Outcomes of Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2015;149:389-97.2. Neuschwander-Tetri BA. Nontriglyceride hepatic lipotoxicity: the new paradigm for the pathogenesis of
NASH. Curr Gastroenterol Rep 2010;12:49-56.3. Ekstedt M, Franzen LE, Mathiesen UL, et al. Long-term follow-up of patients with NAFLD and elevated liver
enzymes. Hepatology 2006;44:865-73.4. Pais R, Pascale A, Fedchuck L, et al. Progression from isolated steatosis to steatohepatitis and fibrosis in
nonalcoholic fatty liver disease. Gastroenterol Clin Biol 2010.5. McPherson S, Hardy T, Henderson E, et al. Evidence of NAFLD progression from steatosis to fibrosing-
steatohepatitis using paired biopsies: Implications for prognosis and clinical management. J Hepatol 2015;62:1148-55.
6. Singh S, Allen AM, Wang Z, et al. Fibrosis Progression in Nonalcoholic Fatty Liver vs Nonalcoholic Steatohepatitis: A Systematic Review and Meta-analysis of Paired-Biopsy Studies. Clin Gastroenterol Hepatol 2015;13:643-654.e9.
Figure:
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
37EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
NATURAL HISTORY OF NASH
Leon Adams* 1
1The University of Western Australia, Crawley, Australia
Corresponding author’s email: [email protected]
Non-alcoholic fatty liver disease (NAFLD) encompasses a histological spectrum from non-alcoholic fatty liver (NAFL), which is characterized by steatosis without significant liver injury, to nonalcoholic steatohepatitis (NASH) where inflammation and ballooning is present, with or without fibrosis. The natural history of NASH parallels its more aggressive histological picture, with prospective cohort studies demonstrating a higher rate of morbidity and mortality compared to NAFL, particularly when fibrosis is present. The additional morbidity associated with NASH is not limited to liver disease, with an increase in cardio-vascular events also described.Longitudinal studies of NAFLD patients with paired liver biopsies, suggest that one third of patients with NAFL and NASH have progressive fibrosis over an average follow-up between 2.2-13.8 years, however the rate of progression is twice as high in NASH subjects. Although fibrosis progression in NASH patients is characteristically indolent, some patients may progress rapidly from no fibrosis to advanced fibrosis over an average 6 year period, however this has been observed in both NASH and NAFL patients. In contrast to fibrosis progression over time, features of steatosis, inflammation and ballooning tend to reduce which is paralleled by reduction in amino-transaminase levels. Factors which influence the histological progression of NASH are outlined below.
Predictors of progressive fibrosis in NASHSexNo consistent relationship between sex and fibrosis has been found in NASH, with cross-sectional and longitudinal studies reporting conflicting findings. The relationship between sex and fibrosis may be complicated by menopausal status, with one cross-sectional study finding both men and post-menopausal women having a higher risk of fibrosis compared with pre-menopausal women.Race and EthnicityAlthough Hispanic patients have an increased prevalence of NAFLD compared to Caucasians, there appears to be no difference in susceptibility to NASH or fibrosis. Cohorts of patients undergoing bariatric surgery suggest Asian patients may be prone to more severe histological changes, although potential confounding environmental factors such as diet have not been assessed.

SP
EA
KE
RS
’ AB
ST
RA
CT
S
38 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Genetic PolymorphismsPolymorphisms in the PNPLA3 and TM6SF2 genes are associated with an increased risk of NAFLD as well NASH and fibrosis. A polymorphism in the IFNL4 gene, which is associated with response to interferon based treatment in chronic hepatitis C, has also been associated with fibrosis in NAFLD and has been amalgamated into a predictive score in conjunction with other clinical factors.AgeCross-sectional studies have demonstrated increasing age to be consistently associated with more severe fibrosis in NASH patients, however this may simply be a marker of the cumulative exposure to other pathogenic factors. Longitudinal studies have not consistently demonstrated age to impact the rate of fibrosis progression.Metabolic FeaturesDiabetes, measures of insulin resistance (eg QUICKI) and obesity are risk factors for liver fibrosis in cross-sectional cohorts of NASH patients. However, not all longitudinal studies, have demonstrated these metabolic factors to be predictive of a higher rate of fibrosis progression. An increase or decrease in body mass index over time, has been associated with progression or resolution of liver fibrosis respectively in NAFLD patients and the emergence of diabetes also appears to parallel fibrosis progression. One meta-analysis examining the full spectrum of NAFLD found hypertension to be a risk factor for fibrosis progression, however an earlier meta-analysis limited to NASH patients did not.Histological FactorsThe degree of hepatic steatosis does not appear to predict disease progression in NASH. The degree of inflammation however, has been associated with progression to advanced fibrosis in a meta-analysis, but not in any single cohort study. Two large studies published in abstract form, have suggested that other histological features of NASH including ballooning, portal inflammation and Mallory Denk bodies predict progression to advanced fibrosis.Molecular FactorsActivation of hepatic stellate cells (HSC) and deposition of fibronectin are early indicators of a fibrogenic response to liver injury. Consequently, histological staining for HSC activation using alpha-smooth muscle actin and fibronectin staining, has been shown to accurately predict fibrosis progression in NAFLD patients.ConclusionA minority of NASH patients will develop progressive fibrosis over a 10 year period, however the prediction of those patients who will progress remains difficult. Control of metabolic risk factors is likely to be important to alter the natural history and genetic and molecular markers may assist prognostication in the future.
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
39EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
GUT MICROBIOTA AND NASH
Herbert Tilg* 1
1Medical University Innsbruck, Innsbruck, Austria
Corresponding author’s email: [email protected]
Gut microbiota and NASHThe human intestinal tract contains an enormous number of microorganisms i.e. the microbiota consisting of more than 1014 bacteria, archaea and viruses. Importantly, the microbiome exceeds the human genome more than 100-fold (1). Recent studies suggest that the microbiota might regulate many metabolic and inflammatory pathways in very diverse diseases including NAFLD.
Experimental studiesAn association of an altered intestinal microbiota with NAFLD has been increasingly described. An age-related increase in breath ethanol content had been demonstrated in ob/ob mice and this effect was eliminated by antibiotic treatment with neomycin proving a role for intestinal bacteria (2). Treatment with the probiotic VSL#3 improved liver histology, reduced hepatic total fatty acid content, and decreased serum alanine aminotransferase (ALT) levels (3). VSL’3 affected liver fibrosis but did not protect from inflammation and steatosis in NASH. In ApoE-/- mice low grade intestinal inflammation drives development of steatohepatitis and worsens the severity of atherosclerosis. Prebiotics also show efficacy as mice treated with fructo-oligo-saccharides show less hepatic steatosis and a decrease in fatty oxidation. Overall, animal studies support the concept for a role of the gut´s microbiota in experimental NAFLD and interference with antibiotics, pre- and probiotics may affect disease phenotype.
Clinical studiesSubstantial evidence has evolved in the last years suggesting that the intestinal microbiota is involved in human NAFLD. NASH patients exhibit small intestinal bacterial overgrowth (SIBO), an impaired intestinal permeability, and increased circulating endotoxin and TNFa levels (4). Two recent clinical studies investigated the gut microbiome in NASH patients. In these studies, differences were abundant at phylum, family, and genus levels between healthy subjects and NASH patients. Importantly, fewer differences were observed between obese and NASH microbiomes. Proteobacteria, Enterobacteriaceae, and Escherichia were the only phylum, family and genus types exhibiting significant difference between obese and NASH microbiomes (5). Another study showed that patients with NASH had a lower percentage of Bacteroidetes compared to both simple steatosis and healthy controls (6).

SP
EA
KE
RS
’ AB
ST
RA
CT
S
40 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Overall, evidence is evolving that there exists similar to obesity and type 2 diabetes a “gut microbiotal signature” which has the potential in the future to differentiate between patients with simply fatty liver and NASH and might furthermore allow to elucidate underlying pathomechanisms in the development of NASH. NAFLD severity in humans has been recently associated with gut dysbiosis and a shift of metabolic functions of the gut microbiota (7). Gut microbiota analysis in humans therefore might be used in the future to classify NAFLD and predict disease severity. Studies identifying how manipulation of gut microbiota in NASH might prove beneficial are eagerly needed.
References1. Moschen AR, Kaser S, Tilg H. Non-alcoholic steatohepatitis: a microbiota-driven disease. Trends Endocrinol
Metab 2013;24:537-545.2. Cope K, Risby T, Diehl AM. Increased gastrointestinal ethanol production in obese mice: implications for
fatty liver disease pathogenesis. Gastroenterology 2000;119:1340-1347.3. Li Z, Yang S, Lin H, Huang J, Watkins PA, Moser AB, et al. Probiotics and antibodies to TNF inhibit
inflammatory activity and improve nonalcoholic fatty liver disease. Hepatology 2003;37:343-350.4. Wigg AJ, Roberts-Thomson IC, Dymock RB, McCarthy PJ, Grose RH, Cummins AG. The role of small
intestinal bacterial overgrowth, intestinal permeability, endotoxaemia, and tumour necrosis factor alpha in the pathogenesis of non-alcoholic steatohepatitis. Gut 2001;48:206-211.
5. Zhu L, Baker SS, Gill C, Liu W, Alkhouri R, Baker RD, et al. Characterization of gut microbiomes in nonalcoholic steatohepatitis (NASH) patients: a connection between endogenous alcohol and NASH. Hepatology 2013;57:601-609.
6. Mouzaki M, Comelli EM, Arendt BM, Bonengel J, Fung SK, Fischer SE, et al. Intestinal microbiota in patients with nonalcoholic fatty liver disease. Hepatology 2013;58:120-127.
7. Boursier J, Mueller O, Barret M, Machado M, Fizanne L, Araujo-Perez F, et al. The severity of nonalcoholic fatty liver disease is associated with gut dysbiosis and shift in the metabolic function of the gut microbiota. Hepatology 2016;63:764-775.
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
41EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
OBSTRUCTIVE SLEEP APNEA – AN OVERLOOKED DIAGNOSIS THAT CAN WORSEN NASH
Judith Aron-Wisnewsky* 1
1IHU ICAN, Pitié-Salpêtrière Hospital, Paris, France
Corresponding author’s email: [email protected]
Obstructive sleep apnea (OSA) and its hallmark chronic intermittent hypoxia (CIH) are established factors involved in NAFLD pathogenesis and exacerbation. This has now been demonstrated in rodents models exposed to intermittent hypoxia, both in paediatric and adults populations. OSA and CIH induce insulin-resistance and dyslipidemia which are involved in NAFLD physiopathogenesis. CIH is increasing HIF1α gene expression and that of downstream genes involved in lipogenesis, therefore increasing β-oxydation and subsequently exacerbating liver oxidative stress. OSA also disrupts the gut liver axis, thus increasing intestinal permeability with a possible role of gut microbiota in the link between OSA and NAFLD. OSA patients should be screened for NAFLD and conversely those with NAFLD for OSA. To date there is no evidence that treating OSA with CPAP will improve NAFLD exacerbation but might at least stabilize and slow its progression. Anyhow, these multimorbid patients should be efficiently treated for all their metabolic co-morbidities and involved in weight stabilization or weight loss programs and physical activity life style interventions.
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
42 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
NAFLD AND CHRONIC KIDNEY DISEASE
Sven M. Francque* 1
1Gastroenterology Hepatology, University Hospital Antwerp, Edegem, Belgium
Corresponding author’s email: [email protected]
The prevalence of chronic kidney disease (CKD) is increasing in the Western adult population, in relation to its riks factors ageing, smoking, arterial hypertension, overweight/obesity and diabetes. As such, CKD shares several risk factors with non-alcoholic fatty liver disease (NAFLD). It is hence not surprising to find an association between the two conditions. Evidence is increasing, however, that points towards a cause-effect relationship that goes beyond a simple association based on shared risk factors. Because of the large overlap in risk factors and co-morbidities in NAFLD, CDK, metabolic syndrome and cardiovascular disease, it is extremely difficult to analyse unilateral and unidirectional cause-effect relationships based on clinical data, even if prospectively collected follow-up data are available. Methodological issues, amongst others related to the mode of diagnosis of NAFLD (for which liver biopsy is still the gold standard to accurately diagnose different disease features) and CDK hamper the interpretation of the data. Nevertheless, there is mounting evidence of an increased pervalence and incidence of CKD in patients with NAFLD, with higher figures in patients with non-alcoholic steatohepatitis (NASH) and in patients with significant fibrosis compared to patients with non-alcoholic fatty liver (NAFL) and without fibrosis respectively. The potential mechanisms linking the 2 conditions are poorly understood, Production by the inflamed and steatotic liver in NASH patients of pro-inflammatory mediators, prothrombotic factors, pro-fibrogenic and pro-atherogenic molecules have been postulated as potential factors involved. Impact of the liver on endothelial function in several vascular beds may be a crucial factor in the complex relationship between metabolic syndrome, NAFLD, cardiovascular disease and CKD. The relation between NAFLD and CKD is probably not unidirectional, as, amongst others, experimental data in nephrectomized animals also show an impact on the liver. The association also has potential clinical implications, both for diagnosis (should we screen for CKD in NAFLD?) and for treatment (e.g. the potential benefit of the use of sartans on both NAFLD (sartans have been reported to impact on fibrogenesis in animal models) and CKD, but also CVD; or the implications for management of renal problems in liver transplantation for NASH-related end-stage liver disease or hepatocellular carcinoma).
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
43EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
NASH AND CARDIOVASCULAR RISK
Javier Ampuero* 1, 2
1Unit For Clinical Management Of Digestive Diseases, VIRGEN DEL ROCIO UNIVERSITY HOSPITAL, 2Instituto de Biomedicina de Sevilla, Sevilla, Spain
Corresponding author’s email: [email protected]
Non-alcoholic fatty liver disease (NAFLD) encompasses a spectrum ranging from simple steatosis to steatohepatitis (NASH) without excess alcohol intake and is considered to be the hepatic manifestation of metabolic syndrome. Prevalence rates are rising because of overweight and obesity. In fact, NAFLD is the most common cause of chronic liver disease in Western countries with a prevalence of 20%>30%, which is increased up to 70% in obese and diabetic subjects.NAFLD is closely associated with abdominal obesity, atherogenic dyslipidemia, hypertension, insulin resistance and impaired glucose tolerance, which are all features of the metabolic syndrome. Recent studies indicate that NAFLD is closely related to cardiovascular disease, especially to thickening of the intima-media layer of the carotid artery (as the morphostructural manifestation of the presence of subclinical atheromatosis). In addition, the presence of impaired carotid-femoral pulse wave velocity or left ventricular dysfunction are frequently found in patients showing NAFLD. We should be alert about an increased risk of coronary artery disease in subjects with NAFLD and to be more aggressive in the searching of primary prevention with the performance of tests of detection of subclinical atherosclerosis. The right management of this kind of patients will enable to modify the natural history both liver and cardiovascular disease.
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
44 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
NAFLD: CURRENT CLASSIFICATIONS AND THEIR LIMITATIONS
Dina G. Tiniakos* 1, 2
1Institute of Cellular Medicine, Newcastle University, UK, Newcastle upon Tyne, United Kingdom, 2Laboratory of Histology-Embryology, Medical School, National & Kapodistrian University of Athens, Athens, Greece
Corresponding author’s email: [email protected]
Steatosis, steatosis with inflammation, non-alcoholic steatohepatitis (NASH) and cirrhotic nonalcoholic fatty liver disease (NAFLD) are generally considered components of a continuous spectrum. Most experts agree that the minimal requirements for the morphological diagnosis of NASH include hepatocyte ballooning in addition to steatosis and inflammation. These key lesions are typically accentuated in zone 3 of the hepatic acinus. Fibrosis is not required for the diagnosis of NASH as it is not required for the diagnosis of chronic hepatitis of other etiology.1 Liver biopsy interpretation is still regarded as the “gold” standard for making accurate diagnoses in NAFLD although sampling limitations are recognized. Clear definitions for some of the key histopathological components, such as ballooning, are lacking partly reflecting inter-observer variation in making a diagnosis of steatohepatitis. Even the definition of steatosis itself, according which presence of fat in >5% of hepatocytes is regarded as the cut-off for making a diagnosis of NAFLD, is somewhat arbitrary since this is based on early biochemical studies that indicated that normal liver contained 5% lipid by weight. Evaluation of morphological features of NAFLD by semi-quantitative scoring is frequently performed to provide standardized assessment of disease activity grade and fibrosis stage to support clinical decision making and for use in clinical trials. One of the most widely used scores for grading activity, the NAFLD activity score (NAS) developed by the NIH-sponsored NASH Clinical Research Network, derives from the sum of semi-quantitative numerical scores for steatosis, hepatocyte and acinar inflammation.2 This has been erroneously used in the past to classify NAFLD as “NASH” or “not-NASH”. However, NAS was never intended to and should not replace the histopathological classification of NAFLD types.3 Recently, a simple histological algorithm was developed to standardize and limit inter-observer-related variation in the histological diagnosis of NASH.4 The European Fatty Liver Inhibition of Progression (FLIP) algorithm informed by the scores for steatosis, hepatocellular ballooning and inflammation allows for NAFLD stratification into two main diagnostic categories: steatosis versus NASH. The FLIP algorithm can significantly reduce the inter-observer bias of the diagnosis of NASH among expert hepatopathologists as well as between general pathologists.4 The FLIP algorithm is accompanied by semi-quantitative scoring of the key features of NASH, steatosis (S,0-3), activity (A, 0-4), and
SP
EA
KE
RS
’ AB
ST
RA
CT
S
45EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
fibrosis (F, 0-4), known as the SAF score. The main difference from previous histological scoring systems, like the NAS, is that in SAF the severity of NAFLD activity is reflected by the sum of scores for hepatocyte ballooning (0-2) and acinar inflammation (0-2) only and steatosis is graded separately.5 Using the SAF score, NAFLD may be categorized as mild disease (A<2 and/or F<2) or significant disease (A≥2 and/or F≥2) defined by hepatocyte ballooning, acinar inflammation and fibrosis, parameters of known prognostic significance in NAFLD, and not by steatosis that has no prognostic value. The prognostic relevance of the dichotomous classification of mild and significant NAFLD remains to be evaluated in further studies.
References1. Burt AD, Lackner C, Tiniakos D. Diagnosis and assessment of NAFLD: definitions and histopathological
classification. Semin Liver Dis. 2015;35(3):207-20.2. Kleiner DE, Brunt EM, Van Natta M, et al. Design and validation of a histological scoring system for
nonalcoholic fatty liver disease. Hepatology 2005;41:1313–21.3. Brunt EM, Kleiner DE, Wilson LA, et al. Nonalcoholic fatty liver disease (NAFLD) activity score and the
histopathologic diagnosis in NAFLD: distinct clinico-pathologic meanings. Hepatology 2011;53(3):810-20.4. Bedossa P, Poitou C, Veyrie N, et al. Histopathological algorithm and scoring system for evaluation of liver
lesions in morbidly obese patients. Hepatology 2012;56:1751-9.5. Bedossa P & FLIP Pathology Consortium. Utility and appropriateness of the fatty liver inhibition of
progression (FLIP) algorithm and steatosis, activity, and fibrosis (SAF) score in the evaluation of biopsies of nonalcoholic fatty liver disease. Hepatology 2014;60:565-75.
Disclosure of Interest: None Declared
SP
EA
KE
RS
’ AB
ST
RA
CT
S
46 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
NASH WITH ADVANCED FIBROSIS AND HCV AND WILSONS DISEASE MASQUERADING NASH
Carolin Lackner* 1
1Medical University of Graz, Institute of Pathology, Graz, Austria
Corresponding author’s email: [email protected]
Metabolic syndrome (MS)-associated NAFLD and chronic hepatitis C are among the most prevalent liver diseases and thus the co-existence of both conditions is not an infrequent setting in clinical practice. NAFLD comprises a spectrum of liver diseases including non-alcoholic fatty liver (NAFL), non-alcoholic steatohepatitis (NASH) and NAFLD-associated cirrhosis. Among the NAFLD types, NASH is considered a progressive lesion associated with the development of fibrosis, cirrhosis and eventually hepatocellular carcinoma (HCC) in a subset of patients. The co-occurrence of both diseases is clinically important owing to an apparently synergistical effect on the severity of liver disease associated with higher fibrosis stage, and the development of cirrhosis and HCC. While the clinical diagnosis of HCV infection and respective fibrosis stage can be achieved by non-invasive molecular and radiological methods, the diagnosis of NASH is dependent on a liver biopsy and histological evaluation. The histological changes of NASH, in particular centrilobular accentuation of liver injury with steatosis, inflammation, hepatocellular ballooning, Mallory Denk bodies (MDBs) and pericellular fibrosis, are distinct from portal and periportal based inflammation and fibrosis in chronic hepatitis C. However, some of the morphological hallmarks of NASH, especially hepatocelllular ballooning and MDBs can be discrete changes and may even be missing in H&E stained sections in advanced fibrosis or cirrhosis stages. The reliable and objective detection of ballooned hepatocytes and/or MDBs can be facilitated by several recently described immunohistochemical markers. The definition of advanced fibrosis stage by non-invasive methods has not been evaluated in detail in a setting of combined NASH/HCV. Both, histological stage and detection of pericellular fibrosis as a footprint of prior episodes of NASH may have important implications for patient management.Wilson´s disease (WD) is a hereditary disorder of copper metabolism due to mutations in the copper-transporting P-type ATPase, ATP7B. The ATP7B protein mediates the transport of copper from intracellular chaperone proteins for excretion into the bile and incorporation of copper into apo-ceruloplasmin. Mutations in the ATP7B gene lead to copper accumulation and liver injury due to impaired secretion of copper. Eventually copper is released into the blood and is deposited in other organs like the brain, kidneys and cornea. Most patients present between the ages 5 and 35 with either liver disease or as a progressive neurological or psychiatric disorder. Without treatment WD is a fatal. Most patients die from complications of liver disease and less frequently from progressive

SP
EA
KE
RS
’ AB
ST
RA
CT
S
47EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
neurological disease. The development of cirrhosis is associated with increased risk of death. However, provided an early diagnosis, WD is a treatable and even preventable condition. Patients who are diagnosed in a precirrhotic stage and receive adequate care seem to enjoy good long-term prognosis and less frequent need for a liver transplant.The clinical diagnosis of WD can be challenging. Therefore diagnostic algorithms based on clinical symptoms and biochemical variables have been published by international expert committees. Liver biopsy is required for the quantification of liver copper for diagnostic purposes in patients in whom clinical signs and non-invasive tests do not allow a definitive diagnosis or if additional causes for liver disease are suspected. On histology any type of liver pathology may be encountered in WD. However, one of the manifestations is with features of steatosis and steatohepatitis with morphological overlap with MS-associated fatty liver disease or resembling autoimmune hepatitis. Some of the features of steatohepatitis may differ between WD and classical MS-associated NASH in adults or type 1 NASH in children. In WD portal and periportal based liver injury with portal inflammation and fibrosis, interphase activity, and ballooned hepatocytes with MDBs prevail which is in contrast to the centrilobular accentuation of morphological changes in MS-associated NASH. However, distinction of WD from type 2 paediatric NAFLD may be impossible on morphological grounds. WD may be the underlying cause of liver disease in an individual with biochemical abnormalities and/or metabolic risk factors for NAFLD/NASH. Therefore, a high level of suspicion is important in order to meet the diagnosis in a patient who has been biopsied for other reasons than WD. In particular, WD should be suspected in the young or middle aged individuals who have unexplained chronic liver disease, or no classical risk factors for MS-associated NASH and/or liver disease and neurological or psychiatric symptoms. In some patients also the co-occurrence of NAFLD/NASH and WD cannot be excluded.
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
48 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
NON-INVASIVE ASSESSMENT OF STEATOSIS, NASH AND FIBROSIS: SERUM MARKERS
Emmanuel Tsochatzis* 1
1Royal Free Hospital NHS Trust, London, United Kingdom
Corresponding author’s email: [email protected]
NAFLD is a disease of high prevalence and relatively low severity in the majority of patients. Although liver biopsy is the gold standard for diagnosing steatohepatitis and assessing disease severity, it would be inappropriate to biopsy every patient diagnosed with NAFLD, as it is a costly and invasive procedure, which is associated with patient discomfort and potential side effects. In order to address this rising need, non-invasive tests and strategies have been developed that attempt to diagnose NAFLD, NASH and stage the disease. In this talk, I will review and critically appraise the evidence on the use of non-invasive blood tests for diagnosing steatosis, NASH and staging fibrosis.
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
49EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
SARCOPENIA IS ASSOCIATED WITH SEVERE LIVER FIBROSIS IN PATIENTS WITH NON-ALCOHOLIC FATTY LIVER DISEASE
Salvatore Petta* 1, Stefania Ciminnisi, Vito Di Marco, Daniela Cabibi, Calogero Cammà, Giulio Marchesini, Antonio Craxì1Section of Gastroenterology, DI.BI.MI.S University of Palermo, Palermo, Italy
Corresponding author’s email: [email protected]
We tested whether sarcopenia is associated with the severity of liver fibrosis(main outcome) and with the entire spectrum of liver damage in patients with NAFLD.We considered 225 consecutive patients with a histological diagnosis of NAFLD(Kleiner score). The skeletal muscle index(SMI)[SMI(%)=total appendicular skeletal muscle mass(kg)/weight(kg)×100] was measured by electrical bioimpedentiometry.The lower SMI tertile was independently associated with male gender(p<0.001), visceral obesity(p<0.001) and higher HOMA(p=0.002). The prevalence of severe fibrosis progressively increased from 18.6% in patients in the upper, to 26.5% in those in the middle and to 49.3% in those in the lower SMI tertile(p<0.001). This association was maintained(OR 2.03,CI 1.21-3.39,p=0.007), together with older age(OR 1.11,CI 1.07-1.16, p<0.001), higher HOMA values(OR 1.33,CI 1.11-1.58, p=0.002) and NASH(OR 11.2,CI 1.33-94.6, p=0.02), after adjusting for these factors and for hypertension and visceral obesity. Similarly, a significant association was found between lower SMI tertile and NASH(p=0.005), the severity of steatosis(p=0.004), presence of ballooning(p=0.001) and grade 2-3 lobular inflammation(p=0.07). After adjusting for metabolic and liver confounders, the association was only maintained with the severity of steatosis(OR 1.53,CI 1.07-2.18, p=0.01) and ballooning(OR 2.19,CI 1.17-4.11, p=0.01).In a cohort of patients with NAFLD, sarcopenia is a marker/risk factor for the entire spectrum of liver damage, independently of well known liver and metabolic risk factors. Studies are needed to assess the impact of sarcopenia correction on hepatic and metabolic complications in NAFLD patients.
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
50 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
NEW IMAGING TECHNIQUES FOR THE NON-INVASIVE ASSESSMENT IN NAFLD
Rohit Loomba* 1
1Division of Gastroenterology, Department of MedicineDivision of Epidemiology, Department of Family Medicine and Public Health, University of California at San Diego, San Diego, CA, United States
Corresponding author’s email: [email protected]
Non-alcoholic fatty liver disease (NAFLD) is the most common cause of chronic liver disease in the United States (US).(1-4) NAFLD is characterized by presence of hepatic steatosis in the absence of excessive alcohol use or other identifiable liver disease. It is commonly classified into two main subtypes: non-alcoholic fatty liver (NAFL) and non-alcoholic steatohepatitis (NASH).(5) Although these were previously considered to be distinct entities with separate disease courses and prognoses, more recent literature has demonstrated that NAFL and NASH actually represent points across a disease continuum that ultimately culminates in progression to hepatic fibrosis and cirrhosis if not intervened upon.(6-8) Approximately 20% of NAFLD patients may rapidly progress to advanced fibrosis,(3, 9) and the development of advanced fibrosis is associated with an increased risk for morbidity and mortality through hepatic (cirrhosis, hepatocellular carcinoma) and non-hepatic (cardiovascular disease) complications.(7, 10-12) Thus, prompt diagnosis and timely referrals for at risk patients is needed to off-set the natural progression of this disease through the use of effective interventions. In order to accurately detect presence of NAFLD, and to identify advanced fibrosis, the points at which the maximal benefit may be achieved for interventions, providers must rely heavily on liver biopsies and histologic assessment. Liver biopsies are, however, not without cost or risk (bleeding and perforation), and the inter-provider variability in sampling along with the inter-observer variability in scoring, creates a great deal of uncertainty when attempting to use this diagnostic method for disease assessment.(13, 14) Furthermore, serial liver biopsies for monitoring response to interventions is impractical and unlikely to be well received by patients or providers alike. This growing appreciation for the limitations of liver biopsy, coupled with the increase in potentially effective therapeutic interventions for at risk patients,(6) has led to the development of several non-invasive techniques that can be used to assess for the presence of NAFLD and help to differentiate between disease activity states (NAFL, NASH, fibrosis and advanced fibrosis). Although these non-invasive biomarkers and imaging techniques are appealing for the detection of hepatic fibrosis, differentiation of NAFL from NASH, and for the monitoring of response to interventions, they remain unable to obviate the need for liver biopsies given their limited sensitivity and specificity with accompany false positive and false negative results.(14, 15) A need,

SP
EA
KE
RS
’ AB
ST
RA
CT
S
51EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
therefore, remains for a non-invasive approach to assessing hepatic steatosis and fibrosis in patients at risk for NALFD or those who have already developed NALFD where response to interventions need to be monitored to optimize disease outcomes.Magnetic resonance imaging including MRI-proton density fat fraction (MRI-PDFF) has recently been demonstrated to be a highly accurate diagnostic tool for the detection and quantification of hepatic steatosis and, MR elastography (both 2D and 3 D MRE) for the detection and quantification of hepatic fibrosis, and for differentiating between disease states among NALFD patients.(16-22) It may, therefore, potentially be used in place of liver biopsy for diagnosing NAFLD and for assessing response to certain types of therapies as newer interventions become available. MRI-PDFF is an accurate, robust and quantitative biomarker for the detection of hepatic steatosis as well as quantification of the amount of fat in the liver. It has emerged as a key adjunct endpoint for assessment of treatment response in early phase trials in which the therapies have a proposed mechanism of action that lowers liver fat. MRE is the most accurate, reproducible and quantitative biomarker for the diagnosis of advanced fibrosis in NAFLD(22). It is not affected by obesity, ascites or advanced stage of disease. The results are comparable across various platforms. However, generalizability is limited compared to VCTE or other ultrasound based methods. Following issues would be discussed in details during the presentation.
MRI based assessment of hepatic steatosis and quantitative changes in hepatic fat– What is MRI-PDFF? – Diagnostic accuracy and comparison to other non-invasive imaging techniques– When to use MRI-PDFF? – Why to use MRI-PDFF ? – Advantages of MRI-PDFF over MRS or other ultrasound-based tests such as CAP or
novel QUS methods– Protocol for assessment for treatment response (Examples colesevelam trial and
MOZART Trial) o Importance of co-localization for assessing treatment response in NASH (figure 1)
MRE based assessment of hepatic fibrosis– What is MRE? – Diagnostic accuracy and comparison to other non-invasive imaging techniques– When to use MRE? – Why to use MRE? – Advantages of MRE over VCTE or other ultrasound-based methods– Utility of liver multiscan– Protocol for assessment for treatment response? (How to assess treatment response in
NASH E.g. MOZART Trial) o Importance of co-localization for assessing disease progression (see figure 1)

SP
EA
KE
RS
’ AB
ST
RA
CT
S
52 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Figure 1. Co-localization protocol for assessment of treatment response by MRI-PDFF and MRE in NASH trials
Future studies and considerationsIn this presentation, we will summarize the currently available evidence regarding the use of advanced imaging methods and their utility among patients with NAFLD. The advantages each imaging technique over other non-invasive assessment techniques, and how it may be used for the assessment of disease activity and response to therapy in both clinical trials and clinical practice will be discussed with special emphasis on MRI-PDFF for steatosis quantification and MRE for liver stiffness quantification. This will have considerable implications on the evolving clinical trial atmosphere in NALFD and on clinical practice where the growing burden of NAFLD in the community will need to be met with an enhanced monitoring protocol geared towards early diagnosis and intervention among at risk individuals.
1. Loomba R, Sanyal AJ. The global NAFLD epidemic. Nat Rev Gastroenterol Hepatol 2013;10:686-690. 2. Vernon G, Baranova A, Younossi ZM. Systematic review: the epidemiology and natural history of non-alcoholic
fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment Pharmacol Ther 2011;34:274-285. 3. Williams CD, Stengel J, Asike MI, Torres DM, Shaw J, Contreras M, Landt CL, et al. Prevalence of
nonalcoholic fatty liver disease and nonalcoholic steatohepatitis among a largely middle-aged population utilizing ultrasound and liver biopsy: a prospective study. Gastroenterology 2011;140:124-131.
4. Rinella ME. Nonalcoholic fatty liver disease: a systematic review. Jama 2015;313:2263-2273. 5. Chalasani N, Younossi Z, Lavine JE, Diehl AM, Brunt EM, Cusi K, Charlton M, et al. The diagnosis and
management of non-alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology 2012;142:1592-1609.
6. Spengler EK, Loomba R. Recommendations for Diagnosis, Referral for Liver Biopsy, and Treatment of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis. Mayo Clin Proc 2015;90:1233-1246.

SP
EA
KE
RS
’ AB
ST
RA
CT
S
53EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
7. Singh S, Allen AM, Wang Z, Prokop LJ, Murad MH, Loomba R. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clin Gastroenterol Hepatol 2015;13:643-654 e641-649; quiz e639-640.
8. Matteoni CA, Younossi ZM, Gramlich T, Boparai N, Liu YC, McCullough AJ. Nonalcoholic fatty liver disease: a spectrum of clinical and pathological severity. Gastroenterology 1999;116:1413-1419.
9. Wong VW, Wong GL, Choi PC, Chan AW, Li MK, Chan HY, Chim AM, et al. Disease progression of non-alcoholic fatty liver disease: a prospective study with paired liver biopsies at 3 years. Gut 2010;59:969-974.
10. Bhala N, Angulo P, van der Poorten D, Lee E, Hui JM, Saracco G, Adams LA, et al. The natural history of nonalcoholic fatty liver disease with advanced fibrosis or cirrhosis: an international collaborative study. Hepatology 2011;54:1208-1216.
11. Adams LA, Lymp JF, St Sauver J, Sanderson SO, Lindor KD, Feldstein A, Angulo P. The natural history of nonalcoholic fatty liver disease: a population-based cohort study. Gastroenterology 2005;129:113-121.
12. Arulanandan A, Ang B, Bettencourt R, Hooker J, Behling C, Lin GY, Valasek MA, et al. Association Between Quantity of Liver Fat and Cardiovascular Risk in Patients With Nonalcoholic Fatty Liver Disease Independent of Nonalcoholic Steatohepatitis. Clin Gastroenterol Hepatol 2015;13:1513-1520 e1511.
13. Rockey DC, Caldwell SH, Goodman ZD, Nelson RC, Smith AD, American Association for the Study of Liver D. Liver biopsy. Hepatology 2009;49:1017-1044.
14. Asrani SK. Incorporation of Noninvasive Measures of Liver Fibrosis Into Clinical Practice: Diagnosis and Prognosis. Clin Gastroenterol Hepatol 2015.
15. Papagianni M, Sofogianni A, Tziomalos K. Non-invasive methods for the diagnosis of nonalcoholic fatty liver disease. World J Hepatol 2015;7:638-648.
16. Cui J, Ang B, Haufe W, Hernandez C, Verna EC, Sirlin CB, Loomba R. Comparative diagnostic accuracy of magnetic resonance elastography vs. eight clinical prediction rules for non-invasive diagnosis of advanced fibrosis in biopsy-proven non-alcoholic fatty liver disease: a prospective study. Aliment Pharmacol Ther 2015;41:1271-1280.
17. Singh S, Venkatesh SK, Wang Z, Miller FH, Motosugi U, Low RN, Hassanein T, et al. Diagnostic performance of magnetic resonance elastography in staging liver fibrosis: a systematic review and meta-analysis of individual participant data. Clin Gastroenterol Hepatol 2015;13:440-451.e446.
18. Idilman IS, Keskin O, Celik A, Savas B, Halil Elhan A, Idilman R, Karcaaltincaba M. A comparison of liver fat content as determined by magnetic resonance imaging-proton density fat fraction and MRS versus liver histology in non-alcoholic fatty liver disease. Acta Radiol 2015.
19. Tang A, Desai A, Hamilton G, Wolfson T, Gamst A, Lam J, Clark L, et al. Accuracy of MR imaging-estimated proton density fat fraction for classification of dichotomized histologic steatosis grades in nonalcoholic fatty liver disease. Radiology 2015;274:416-425.
20. Permutt Z, Le TA, Peterson MR, Seki E, Brenner DA, Sirlin C, Loomba R. Correlation between liver histology and novel magnetic resonance imaging in adult patients with non-alcoholic fatty liver disease – MRI accurately quantifies hepatic steatosis in NAFLD. Aliment Pharmacol Ther 2012;36:22-29.
21. Loomba R, Wolfson T, Ang B, Hooker J, Behling C, Peterson M, Valasek M, et al. Magnetic resonance elastography predicts advanced fibrosis in patients with nonalcoholic fatty liver disease: a prospective study. Hepatology 2014;60:1920-1928.
22. Loomba R, Cui J, Wolfson T, Haufe W, Hooker J, Szeverenyi N, Ang B, et al. Novel 3D Magnetic Resonance Elastography for the Noninvasive Diagnosis of Advanced Fibrosis in NAFLD: A Prospective Study. Am J Gastroenterol 2016.
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
54 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
THE SEARCH FOR INNOVATIVE MARKERS: FROM IMAGING TO EPIGENETIC BIOMARKERS
Manuel Romero-Gómez* 1
1Digestive Diseases, Virgen Macarena-Virgen del Rocío University Hospital, Seville, Spain
Corresponding author’s email: [email protected]
Liver biopsy remains as the gold standard for the diagnosis of NAFLD. Steatosis, steatohepatitis and fibrosis stage have to be described as histological features of this disease. Limitations of liver biopsy include: morbimortality associated with the procedure and cost together with sample error . Distribution of lesions in the liver is heterogeneous and concordance between two liver biopsies done at the same time is suboptimal. Besides, longitudinal studies demonstrated that simple steatosis is not a benign and non-progressive disease . Non-invasive methods spectrum ranged from serum to imaging, genes and epigenetic biomarkers. From an etiological point of view, a combination of biochemical parameters and anthropometric data (fatty liver index, hepatic steatosis index, lipid accumulation product) together with ultrasonography are able to confirm steatosis in the majority of patients. Magnetic Resonance spectroscopy could be included as gold standard for steatosis diagnosis in patients with previous controversial results . Histological features related to prognosis are presence of steatohepatitis and fibrosis stage. In general, no imaging examinations have been found to accurately diagnose steatohepatitis using ultrasonography, computed tomography or magnetic resonance. Steatohepatitis is defined by lobular inflammation and ballooning. Optical analysis of MR images of the liver (DeMILI®) generates an output (NASH-MRi) able to predict steatohepatitis with high accuracy (AUROC: 0.83) . Owl-liver® a metabolomic approach corrected by body mass index could also accurately predict steatohepatitis (AUROC: 0.85) . Serum-based method (mainly FGF21 (AUROC: 0.62), CK-18 (0.70), AFABP (AUROC: 0.69) and NASH-test (AUROC: 0.77) did not reach strong validation in external studies and have not been incorporated in clinical practice.Fibrosis is the last histological feature that has to be diagnosed for therapeutic decision making together with prognosis impact. Non-invasive methods like NAFLD-Fibrosis score and FIB-4, a non-invasive method developed in Hepatitis C sitting but has demonstrated to be useful for fibrosis prediction on NAFLD. Both methods accurately confirmed advanced fibrosis and excluded fibrosis, but the main limitation is the wide gray zone for intermediate results. Fibrotest® and Enhanced Liver Fibrosis panel® seems not add value to free-of-charge serum-based methods. In patients with inconclusive results imaging-biomarkers could be useful: transient elastography, Fibro-MRI and Magnetic Resonance Elastography have demonstrated high accuracy for the diagnosis of fibrosis stage1,4. PNPLA3 and TM6SF2 are two key genes in the pathogenesis of NAFLD. Both genes predict risk of developing NAFLD and disease progression to liver-related complication

SP
EA
KE
RS
’ AB
ST
RA
CT
S
55EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
and cardiovascular disease. A strong interaction between miRNA (small, noncoding RNA molecules that regulate gene expression) involved in NAFLD and these two genes remained elusive in the last years. Some miRNAs play a key role in disease progression from healthy liver to steatosis, steatohepatitis, and fibrosis progression to cirrhosis and liver cancer. Indeed, the relatively stable and multicellular nature of circulating miRNA, combined with the noninvasive manner in which they can be measured, has positioned miRNAs as potential biomarkers for NAFLD. Validation process has been unsuccessful for many of the previously identified miRNAs. A few studies have reported that some miRNAs appear to be associated with different histopathological stages of NAFLD. In mice, plasma miRNAs (miR-34a, miR-122, miR-181a, miR-192 and miR-200b) are sensitive indicators of inter-strain differences in the severity of liver injury induced by a choline- and folate-deficient diet, with the strongest correlation occurring with miR-34a. Serum concentrations of miR-21, miR-34a, miR-122, miR-16 and miR-451 are higher in patients with NAFLD than in healthy controls. Moreover, serum levels of miR-122, miR-34a and miR-200b correlate with disease severity from steatosis to NASH, supporting the potential value of these miRNAs to serve as noninvasive biomarkers for NAFLD progression. In the future, the identification of serum panels of miRNAs that can predict the transition across different stages of NAFLD with a high degree of accuracy is clearly needed, however, their potential utility could be limited by a number of factors relevant to NAFLD, including the lack of cell-type specificity and the complexity of contributions from co-morbid conditions as obesity, type 2 diabetes and dyslipidemia with which a significant number of miRNAs have been associated.
Figure:
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
56 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
ON THE ROLE OF IMMUNE CELLS IN THE DEVELOPMENT OF NAFLD, NASH AND SUBSEQUENT HEPATOCELLULAR CANCER
Mathias Heikenwälder* 1
1Institute of Virology, TU Munich, Munich, Germany
Corresponding author’s email: [email protected]
Overweight and metabolic syndrome are reaching pandemic dimensions in industrialized countries and are rising in developed countries. Non-alcoholic fatty liver disease (NAFLD), the most frequent liver disease world-wide, is a clinical manifestation of overweight and metabolic syndrome. A significant number of NAFLD patients develop non-alcoholic steatohepatitis (NASH), fibrosis and subsequent hepatocellular carcinoma (HCC), thus contributing that HCC currently is the most rapidly increasing cancer in the USA and Europe.Although HCC is the second most common cause of cancer related mortality, the exact mechanisms triggering NASH and subsequent HCC are poorly understood and efficacious therapies are lacking. Our group has longstanding expertise in inflammation-driven HCC. Recently, we have established a mouse model of NASH-driven HCC fully recapitulating human pathophyisology in the context of metabolic syndrome. We demonstrated that CD8+ and NKT cells become activated during metabolic syndrome, interact with hepatocytes through cytokines and alter hepatic lipid metabolism causing NASH and HCC. An identical profile of CD8+ and NKT cell activation was found in human NASH livers underlining the clinical relevance of our model.Based on this but other model systems we further tried to elucidate the exact cellular and molecular mechanisms that drive NASH and NASH driven liver cancer, which I will report on.
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
57EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
HYPOXIA ACCELERATES FATTY ACID UPTAKE LEADING TO INCREASED FAT ACCUMULATION AND INFLAMMATION IN MICE AND IN CULTURED HUMAN HEPATOCYTE-DERIVED CELLS
Carmelo Garcia-Monzon* 1, Águeda González-Rodríguez1, Gloria Mateo1, Ines Soro-Arnáiz1, Mar Torres-Capelli1, Julian Aragonés1
1Liver Research Unit, Santa Cristina University Hospital, Madrid, Spain
Corresponding author’s email: [email protected]
Nonalcoholic fatty liver disease (NAFLD) is the most common cause of chronic liver disease in Western countries. NAFLD is strongly associated with overweight/obesity, insulin resistance, type 2 diabetes (T2DM) and cardiovascular complications; therefore, it is considered the hepatic component of the metabolic syndrome. NAFLD is characterized by the progression from a benign steatosis to more severe liver injuries directly associated with lipotoxicity such as nonalcoholic steatohepatitis (NASH), cirrhosis and hepatocellular carcinoma in 10% of NAFLD patients. Recent evidence indicates that NAFLD severity is affected by obstructive sleep apnoea syndrome (OSAS), a recurrent upper-airway obstruction during sleep, leading to periods of chronic intermittent hypoxia (CIH). In this regard, dysregulation of the normal oxygen gradient in the liver that promotes the stabilization of the hypoxia-inducible factors (HIFs) can induce liver steatosis and inflammation. However, the pathogenic mechanisms underlying the progression of NAFLD to NASH in the context of CIH featuring OSAS are not fully understood. As working hypothesis, the more pronounced the CIH is, the more pronounced the progression to NASH and fibrosis. AIM: The purpose of this study was focused on the molecular mechanisms linking hypoxia to NAFLD/NASH setup. METHODS: HIF system, CD36 content and liver damage markers were analyzed in livers from conditional Von Hippel-Lindau knockout (VHL-KO) mice, which display an overexpression of HIFs after VHL gene deletion induced by tamoxifen, and in HepG2 human hepatocytes loaded with palmitic acid submitted to an hypoxic environment (1% O2). RESULTS: As expected, HIF1 and HIF2 were overexpressed in livers from VHL-KO mice compared to control mice. Remarkably, hepatic features of NAFLD and NASH were found in livers from VHL-KO mice together with increased lipid content. Accordingly, CD36 levels were upregulated in these mice after VHL deletion. In human hepatic cells, HIFs were stabilized under hypoxic conditions. Interestingly, hypoxia itself enhanced fatty acid uptake monitored by Nile Red staining due to the increase of CD36 translocation to the plasma membrane. This event was parallel to an increase of inflammatory markers. Noteworthy, palmitic-induced lipotoxicity was more pronounced under hypoxic conditions. CONCLUSIONS:

SP
EA
KE
RS
’ AB
ST
RA
CT
S
58 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Hypoxia accelerates fatty acid uptake, largely due to CD36 translocation to the plasma membrane of hepatocytes, leading to increased fat accumulation and inflammation in mice and in cultured human hepatocyte-derived cells. These results suggest that hypoxia could have a key pathogenic role in the progression of NAFLD to NASH.
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
59EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
CLINICAL CASE 3.THE CHALLENGES OF MONITORING NAFLD
Helena Cortez-Pinto* 1
1Gastroenterology, Faculdade de Medicina de Lisboa, Hospital De Santa Maria, Lisbon, Portugal
Corresponding author’s email: [email protected]
NAFLD is a chronic disease for which there is no approved treatment, thus often needing long-term follow-up.It is very frequent, and not all NAFLD patients need to be followed on a Hepatology specialized clinic. Decision regarding who should be followed on a specialist consultation, depend on several factors. Since the degree of fibrosis is the most important prognostic factor in NAFLD, correlating with liver-related outcomes and mortality (1, 2), if there is evidence of significant fibrosis, more deep investigation is needed, that may include liver biopsy. Patients with evidence of fibrosis should be followed in a specialist consultation, and periodic evaluation of fibrosis should be done. The best timing of follow-up is still not defined, since the risk and speed of progression are unclear. In the majority of cases routine biochemistry, assessment of co-morbidities and non-invasive monitoring of fibrosis should be done in a yearly or 6 months basis, depending on the severity. Regarding what is the best non-invasive method for monitoring fibrosis, it will probably depend on local availabilities and expertise. Transient elastometry if available, should be performed, although it has several shortcomings, mostly related to high BMI. Numerous serum markers as well as combinations of them, such as the NAFLD fibrosis score, FIB-4, and BARD, as well as commercially panels such as FibroTest, FibroMeter and the ELF test can also be used, with acceptable diagnostic accuracy.On the opposite, the absence of fibrosis is rather reassuring, and after counseling on lifestyle changes, it is possible to discharge the patient from specialized care. The patient should then be reevaluated in a 5-year time.For those patients remaining on follow-up, a very important point is the need of a multidisciplinary team (3). In fact, since NAFLD is usually associated with obesity as well as other aspects of the metabolic syndrome, there is need to implement and survey weight loss and exercise. Several recent studies were able to demonstrate that intensive lifestyle interventions (4, 5), such as the 12-month program reported by Vilar-Gomez et al, resulted in a significant percentage of resolution of NASH, reduction of the NAFLD Activity Score, and regression of fibrosis, (5). However, weight regain is very common. In 2008, Bellentani et al., advocated that NAFLD patients should be preferentially referred to multidisciplinary teams, including physicians, dietitians, psychologists, and physical activity supervisors (6). However, even in very good programs, such as the Diabetes Prevention Program, only 38% maintained weight loss after about 3 year follow-up (7).

SP
EA
KE
RS
’ AB
ST
RA
CT
S
60 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Also, in relation with the increased risk of cardiovascular disease, monitoring of the associated risk factors, such as lipid profile, blood pressure, and cardiovascular status is mandatory and in the absence of fibrosis, focus should be on these factors.One very controversial issue is the need to screen for hepatocellular carcinoma (HCC). There is strong evidence of an increased risk of HCC in NAFLD and NASH, even in the absence of cirrhosis (8). However, the systemic surveillance for HCC in unfeasible due to the large number of NAFLD cases at risk, unless it will be possible to define a high-risk group. It is of course mandatory to screen for HCC, in the presence of cirrhosis, and 6-month scheduled surveillance with ultrasound is recommended.
References1. Angulo P, Kleiner DE, Dam-Larsen S, et al. Liver Fibrosis, but No Other Histologic Features, Is Associated
With Long-term Outcomes of Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2015;149:389-397 e310.
2. Ekstedt M, Hagstrom H, Nasr P et al. Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology 2015;61:1547-1554.
3. Centis E, Moscatiello S, Bugianesi E, et al. Stage of change and motivation to healthier lifestyle in non-alcoholic fatty liver disease. J Hepatol 2013;58:771-777.
4. Lassailly G, Caiazzo R, Buob D, et al. Bariatric Surgery Reduces Features of Nonalcoholic Steatohepatitis in Morbidly Obese Patients. Gastroenterology 2015;149:379-388
5. Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, et al. Weight Loss Through Lifestyle Modification Significantly Reduces Features of Nonalcoholic Steatohepatitis. Gastroenterology 2015;149:367-378 e365
6. Bellentani S, Dalle Grave R, Suppini A et al. Behavior therapy for nonalcoholic fatty liver disease: The need for a multidisciplinary approach. Hepatology 2008;47
7. Marchesini G, Mazzella N, Forlani G. Weight Loss for a Healthy Liver. Gastroenterology 2015;149:274-2788. Dyson J, Jaques B, Chattopadyhay D, et al. Hepatocellular cancer: the impact of obesity, type 2 diabetes and a
multidisciplinary team. J Hepatol 2014;60:110-117
Disclosure of Interest: H. Cortez-Pinto: Consultant/ Advisor: Conflict with: Intercept, Sponsored Lectures: National or International: Conflict with: Intercept

SP
EA
KE
RS
’ AB
ST
RA
CT
S
61EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
INTRODUCTION TO BARIATRIC SURGERY: TECHNIQUES, SHORT-TERM AND LONG-TERM RESULTS AND COMPLICATIONS
Salvador Morales* 1
1Sevilla, Spain
Corresponding author’s email: [email protected]
OVERVIEWBariatric surgery appears in the 50s as a promising treatment in cases where the classical approach is not effective and allows, by reducing intake, with or without malabsorption, gets a negative energy balance that facilitates weight loss and long-term maintenance. Currently, he has not only proved this weight loss, but a reduction in comorbidities associated with obesity and reduction in overall mortality in patients undergoing bariatric surgery compared with traditional nonsurgical approach.
SURGICAL TECHNIQUE FOR OBESITYBariatric surgery techniques achieve weight loss through restrictive, malabsorptive or a combination of both procedures. Each type of technique has its inherent advantages and disadvantages, although there is not enough scientific evidence to recommend one procedure over another in a particular patient. To choose the technique is usually consider the eating habit, BMI, age, comorbidities and surgical risk, among other factors. Pure restrictive techniques reduced the gastric capacity, with the aim of achieving a feeling of fullness and satiety, which decreases energy intake. The techniques of this type most commonly performed today are:
– Vertical banded gastroplasty (GVA) : This technique began in 1982, after publishing his experience Mason. Using this technique the stomach is surgically modified in a vertical way compiling a proximal pouch parallel to the lesser curvature, divided from the remainder of the gastric cavity by mechanical sutures.
– Adjustable Gastric Banding (AGB) : In 1985, Kuzmak placed first an adjustable band. This author modified the orinal technique with a new silicone ring provided with an expandable interior cavity connected to a subcutaneous reservoir, allowing regulating the internal passage.
– Sleeve Gastrectomy: This technique is described in the late 80s as the restrictive part of the duodenal switch, being subsequently carried out as a single procedure, as a first time part of the duodenal switch, or as a one step technique. It represents a special case, since not only produces a significant restriction (with new volumes of the stomach of 60-100 cc), since it has been also demonstrated changes in the levels of intestinal

SP
EA
KE
RS
’ AB
ST
RA
CT
S
62 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
hormones after performing this technique, which may be related to more effectively against other pure restrictive techniques.
In the combined technique there is a restrictive component and a malabsorptive component, performing an intestinal bypass. Depending on the extent of the gastrectomy and common loop length predominates restriction or malabsorption. Combined techniques most commonly performed are: - Roux-en-Y Gastric Bypass: the type of bariatric surgery most commonly used
worldwide. This technique consist in creating a small gastric pouch (20-50 cc) to limit food intake, associated with a Roux-Y gastrojejunal anastomosis with a jejunal loop of variable length, which causes the malabsorptive component.
- Biliopancreatic diversion: the malabsorptive component is larger and involves a gastrectomy, with larger capacity than in previous technique, with a Roux-Y gastrojejunal anastomosis and a biliodigestive diversi�n creating a common limb 50- 75 cm from the ileocecal valve.
- Duodenal Switch: it is a technique similar to that described by Scopinaro but transverse gastrectomy is replaced for a vertical one, maintaining full gastric pyloric innervation and function, with the same distances of the alimentary limb and increasing the common limb.
Currently most of procedures that are being performed worldwide are Sleeve gastrectomy and Roux-en-Y Gastric Bypass, both laparoscopically, and in some centers the adjustable gastric band. The biggest obstacle of gastric banding is that it requires a high fulfillment by the patient and a very close control, reducing the acceptance of the technique. But, the Sleeve gastrectomy is booming, because of its simplicity and effectiveness.
SAFETY AND COMPLICATIONS OF BARIATRIC SURGERYRegarding the mortality associated with surgery, a decade ago early mortality (perioperative and up to 30 days) in the US was up to 2%, and a year was up to 5%. With the advancement of technology and the experience of surgeons, this risk has been greatly reduced in recent years, and today you can do the surgery as safely as cholecystectomy, with Intraoperative mortality of 0.1%. Nutritional complications depend on the type of surgery, diet and fulfillment, thereby being necessary the existence of a multidisciplinary team. The same mechanisms that produce weight loss can lead to its development. The most common are excessive weight loss, protein malnutrition and micronutrient deficiency. One of the most common deficiencies after bariatric surgery is the vitamin B12. Also iron deficiency and anemia are very prevalent, particularly if the duodenum is excluded.
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
63EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
MACRO AND MICRONUTRIENTS IN NASH
Shira Zelber-Sagi* 1
1Liver Unit, Department of Gastroenterology, Tel-Aviv Sourasky Medical Center, Tel-Aviv, Israel
Corresponding author’s email: [email protected]
Lifestyle change, including dietary habits, is a modifiable risk factor and thus represents a main target for the primary prevention and treatment of NAFLD and NASH. Although weight reduction is the most established treatment for both NAFLD and NASH (1), it is hard to achieve and maintain in the long term. Therefore, changing dietary composition without reducing caloric intake, may offer a more feasible alternative to treat NAFLD patients. Furthermore, an increasing number of NAFLD patients have normal body mass index (2-5), the so called “lean NAFLD” (6). Several epidemiological studies (7-9) indicate that normal weight NAFLD patients in particularly consume an unhealthy diet as compared to controls, and therefore reveals the importance of dietary composition regardless of obesity.Similarly to cardiovascular disease, different types of dietary fat have different effects in NAFLD and NASH. Omega-3 fatty acids and their subtypes seem to be a potential promising treatment due to their favorable effect on lipid metabolism and anti-inflammatory effect. Recent RCTs, assessed their effect on NASH and fibrosis, yielding conflicting results with regard to liver fat reduction and disappointing results with regard to NASH or fibrosis (10-12).Monounsaturated-fat (MUFA), which characterizes the Mediterranean diet, was demonstrated to have a favorable effect on lipid profile (13,14). It has been suggested that adherence to the Mediterranean diet pattern leads to a significant decrease in liver fat (15). This was supported by two randomized short term trials in NAFLD patients with or without type-2 diabetes assigned to either low fat (30% of calories as fat) or high-MUFA diet/Mediterranean diet (40% of calories as fat) for a 6-8-week period. Liver fat content decreased more in the MUFA/Mediterranean diet despite stable weight in both groups (16, 17). It should be noted that the Mediterranean diet is also characterized by reduced carbohydrates intake (40% of the calories vs. 50-60% in a typical low fat diet), especially reduced sugars and refined carbohydrates, which may account, at least partially, for its success.There is overwhelming evidence with regard to the association between added sugars and NAFLD. The association is more prominent with sugar-sweetened beverages (SSBs) (7, 18-20), but not with diet beverages (21). In addition, cola beverages contain caramel coloring, which is rich in advanced glycation end products (AGEs) that may increase insulin resistance and inflammation (22, 23). These findings are supported by a 6 month RCT in which only regular cola but not isocaloric semi skim milk or aspartame-

SP
EA
KE
RS
’ AB
ST
RA
CT
S
64 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
sweetened diet cola led to increased liver fat (24). Fructose-containing beverages were also demonstrated to be associated with a more severe fibrosis in NAFLD patients if consumed on a daily basis (25), perhaps since fructose increases uric acid levels which is related to oxidative stress and insulin resistance (26). Therefore, like alcohol, questions regarding SSBs consumption should routinely be include as part of the patient’s history.After the elimination of SSBs from the diet, patients may be encouraged to drink coffee. Studies in NAFLD patients repeatedly suggested an inverse association between coffee consumption and liver fibrosis (27-30) and HCC (31). However, with regard to steatosis the results are conflicting (27, 28, 30, 32, 33). The hepatoprotective effects of coffee may be linked not only to caffeine but also to its polyphenolic fraction (34, 35).In spite of the evidence supporting the association of oxidative stress with NASH and the efficacy of antioxidants in animal models, the efficacy of antioxidant therapy in humans has not been demonstrated or properly tested (36), with the exception of vitamin E (37).Choline is an essential component of cell membranes and is required for the synthesis of phospholipids. In a cross-sectional analysis, postmenopausal women with deficient choline intake had worse fibrosis and a similar trend was noted in both premenopausal women and men (38). Choline is particularly abundant in egg yolks and animal sources of protein.Emerging evidence suggests that vitamin D may play a role in the pathogenesis of NAFLD. In support of that, a meta-analysis of observational studies demonstrated that compared to controls, NAFLD patients were more likely to be vitamin D deficient (39). However, a study carefully adjusting for adiposity, suggests that there is no relationship between vitamin D levels and insulin resistance, the amount of liver fat, or the severity of NASH (40).Shifting the focus of goal setting from just weight reduction to dietary change goals may help in our patient’s empowerment and enhancement of self-efficacy. The diet of choice should be the one which individuals are able to adhere for years rather than weeks, with the help of educational and behavioral strategies.
References1. Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, Torres-Gonzalez A, Gra-Oramas B, Gonzalez-
Fabian L, et al. Weight Loss Through Lifestyle Modification Significantly Reduces Features of Nonalcoholic Steatohepatitis. Gastroenterology. 2015;149(2):367-78 e5; quiz e14-5.
2. Chitturi S, Abeygunasekera S, Farrell GC, Holmes-Walker J, Hui JM, Fung C, et al. NASH and insulin resistance: Insulin hypersecretion and specific association with the insulin resistance syndrome. Hepatology. 2002;35:373-9.
3. Pagano G, Pacini G, Musso G, Gambino R, Mecca F, Depetris N, et al. Nonalcoholic steatohepatitis, insulin resistance, and metabolic syndrome: further evidence for an etiologic association. Hepatology. 2002;35:367-72.
4. Lee JH, Rhee PL, Lee JK, Lee KT, Kim JJ, Koh KC, et al. Role of hyperinsulinemia and glucose intolerance in the pathogenesis of nonalcoholic fatty liver in patients with normal body weight. Korean J Intern Med. 1998;13:12-4.
5. Banerji MA, Faridi N, Atluri R, Chaiken RL, Lebovitz HE. Body composition, visceral fat, leptin, and insulin resistance in Asian Indian men. J Clin Endocrinol Metab. 1999;84:137-44.6. Younossi ZM, Stepanova M, Negro F, Hallaji S, Younossi Y, Lam B, et al. Nonalcoholic fatty liver disease in lean individuals in the United States. Medicine. 2012;91(6):319-27.
7. Assy N, Nasser G, Kamayse I, Nseir W, Beniashvili Z, Djibre A, et al. Soft drink consumption linked with fatty liver in the absence of traditional risk factors. Can J Gastroenterol. 2008;22(10):811-8. Musso G, Gambino R, De Michieli F, Cassader M, Rizzetto M, Durazzo M, et al. Dietary habits and their relations to insulin

SP
EA
KE
RS
’ AB
ST
RA
CT
S
65EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
resistance and postprandial lipemia in nonalcoholic steatohepatitis. Hepatology. 2003;37(4):909-16. 9. Yasutake K, Nakamuta M, Shima Y, Ohyama A, Masuda K, Haruta N, et al. Nutritional investigation of
non-obese patients with non-alcoholic fatty liver disease: the significance of dietary cholesterol. Scandinavian journal of gastroenterology. 2009;44(4):471-7.
10. Scorletti E, Bhatia L, McCormick KG, Clough GF, Nash K, Hodson L, et al. Effects of purified eicosapentaenoic and docosahexaenoic acids in non-alcoholic fatty liver disease: Results from the *WELCOME study. Hepatology. 2014.
11. Sanyal AJ, Abdelmalek MF, Suzuki A, Cummings OW, Chojkier M. No significant effects of ethyl-eicosapentanoic acid on histologic features of nonalcoholic steatohepatitis in a phase 2 trial. Gastroenterology. 2014;147(2):377-84 e1.
12. Argo CK, Patrie JT, Lackner C, Henry TD, de Lange EE, Weltman AL, et al. Effects of n-3 fish oil on metabolic and histological parameters in NASH: a double-blind, randomized, placebo-controlled trial. Journal of hepatology. 2015;62(1):190-7. 13. Mensink RP, Zock PL, Kester AD, Katan MB. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a meta-analysis of 60 controlled trials. The American journal of clinical nutrition. 2003;77(5):1146-55.
14. Garg A. High-monounsaturated-fat diets for patients with diabetes mellitus: a meta-analysis. The American journal of clinical nutrition. 1998;67(3 Suppl):577S-82S.
15. Trovato FM, Catalano D, Martines GF, Pace P, Trovato GM. Mediterranean diet and non-alcoholic fatty liver disease.: The need of extended and comprehensive interventions. Clin Nutr. 2014.
16. Bozzetto L, Prinster A, Annuzzi G, Costagliola L, Mangione A, Vitelli A, et al. Liver fat is reduced by an isoenergetic MUFA diet in a controlled randomized study in type 2 diabetic patients. Diabetes care. 2012;35(7):1429-35.
17. Ryan MC, Itsiopoulos C, Thodis T, Ward G, Trost N, Hofferberth S, et al. The Mediterranean Diet Improves Hepatic Steatosis and Insulin Sensitivity in Individuals with Nonalcoholic Fatty Liver Disease. Journal of hepatology. 2013.
18. Zelber-Sagi S, Nitzan-Kaluski D, Goldsmith R, Webb M, Blendis L, Halpern Z, et al. Long term nutritional intake and the risk for non-alcoholic fatty liver disease (NAFLD): a population based study. Journal of hepatology. 2007;47(5):711-7.
19. Ouyang X, Cirillo P, Sautin Y, McCall S, Bruchette JL, Diehl AM, et al. Fructose consumption as a risk factor for non-alcoholic fatty liver disease. Journal of hepatology. 2008;48(6):993-9.
20. Abid A, Taha O, Nseir W, Farah R, Grosovski M, Assy N. Soft drink consumption is associated with fatty liver disease independent of metabolic syndrome. Journal of hepatology. 2009;51(5):918-24.
21. Ma J, Fox CS, Jacques PF, Speliotes EK, Hoffmann U, Smith CE, et al. Sugar-sweetened beverage, diet soda, and fatty liver disease in the Framingham Heart Study cohorts. Journal of hepatology. 2015;63(2):462-9.
22. Gaby AR. Adverse effects of dietary fructose. Alternative medicine review : a journal of clinical therapeutic. 2005;10(4):294-306. 23. Koschinsky T, He CJ, Mitsuhashi T, Bucala R, Liu C, Buenting C, et al. Orally absorbed reactive glycation products (glycotoxins): an environmental risk factor in diabetic nephropathy. Proceedings of the National Academy of Sciences of the United States of America. 1997;94(12):6474-9.
24. Maersk M, Belza A, Stodkilde-Jorgensen H, Ringgaard S, Chabanova E, Thomsen H, et al. Sucrose-sweetened beverages increase fat storage in the liver, muscle, and visceral fat depot: a 6-mo randomized intervention study. The American journal of clinical nutrition. 2012;95(2):283-9.
25. Abdelmalek MF, Suzuki A, Guy C, Unalp-Arida A, Colvin R, Johnson RJ, et al. Increased fructose consumption is associated with fibrosis severity in patients with nonalcoholic fatty liver disease. Hepatology.51(6):1961-71.
26. Choi JW, Ford ES, Gao X, Choi HK. Sugar-sweetened soft drinks, diet soft drinks, and serum uric acid level: the Third National Health and Nutrition Examination Survey. Arthritis and rheumatism. 2008;59(1):109-16.
27. Molloy JW, Calcagno CJ, Williams CD, Jones FJ, Torres DM, Harrison SA. Association of coffee and caffeine consumption with fatty liver disease, nonalcoholic steatohepatitis, and degree of hepatic fibrosis. Hepatology. 2012;55(2):429-36. 28. Zelber-Sagi S, Salomone F, Webb M, Lotan R, Yeshua H, Halpern Z, et al. Coffee consumption and nonalcoholic fatty liver onset: a prospective study in the general population. Translational research : the journal of laboratory and clinical medicine. 2015;165(3):428-36.
29. Anty R, Marjoux S, Iannelli A, Patouraux S, Schneck AS, Bonnafous S, et al. Regular coffee but not espresso drinking is protective against fibrosis in a cohort mainly composed of morbidly obese European women with NAFLD undergoing bariatric surgery. Journal of hepatology. 2012;57(5):1090-6.

SP
EA
KE
RS
’ AB
ST
RA
CT
S
66 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
30. Bambha K, Wilson LA, Unalp A, Loomba R, Neuschwander-Tetri BA, Brunt EM, et al. Coffee consumption in NAFLD patients with lower insulin resistance is associated with lower risk of severe fibrosis. Liver international : official journal of the International Association for the Study of the Liver. 2014;34(8):1250-8.
31. Setiawan VW, Wilkens LR, Lu SC, Hernandez BY, Le Marchand L, Henderson BE. Association of coffee intake with reduced incidence of liver cancer and death from chronic liver disease in the US multiethnic cohort. Gastroenterology. 2015;148(1):118-25; quiz e15.
32. Catalano D, Martines GF, Tonzuso A, Pirri C, Trovato FM, Trovato GM. Protective role of coffee in non-alcoholic fatty liver disease (NAFLD). Dig Dis Sci. 2010;55(11):3200-6.
33. Birerdinc A, Stepanova M, Pawloski L, Younossi ZM. Caffeine is protective in patients with non-alcoholic fatty liver disease. Aliment Pharmacol Ther. 2012;35(1):76-82.
34. Vitaglione P, Morisco F, Mazzone G, Amoruso DC, Ribecco MT, Romano A, et al. Coffee reduces liver damage in a rat model of steatohepatitis: the underlying mechanisms and the role of polyphenols and melanoidins. Hepatology. 2010;52(5):1652-61. 35. Salomone F, Li Volti G, Vitaglione P, Morisco F, Fogliano V, Zappala A, et al. Coffee enhances the expression of chaperones and antioxidant proteins in rats with nonalcoholic fatty liver disease. Translational research : the journal of laboratory and clinical medicine. 2013.
36. Lirussi F, Azzalini L, Orando S, Orlando R, Angelico F. Antioxidant supplements for non-alcoholic fatty liver disease and/or steatohepatitis. Cochrane Database Syst Rev. 2007(1):CD004996.
37. Sanyal AJ, Chalasani N, Kowdley KV, McCullough A, Diehl AM, Bass NM, et al. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. The New England journal of medicine. 2010;362(18):1675-85.
38. Guerrerio AL, Colvin RM, Schwartz AK, Molleston JP, Murray KF, Diehl A, et al. Choline intake in a large cohort of patients with nonalcoholic fatty liver disease. The American journal of clinical nutrition. 2012;95(4):892-900.
39. Eliades M, Spyrou E, Agrawal N, Lazo M, Brancati FL, Potter JJ, et al. Meta-analysis: vitamin D and non-alcoholic fatty liver disease. Aliment Pharmacol Ther. 2013;38(3):246-54.
40. Bril F, Maximos M, Portillo-Sanchez P, Biernacki D, Lomonaco R, Subbarayan S, et al. Relationship of vitamin D with insulin resistance and disease severity in non-alcoholic steatohepatitis. Journal of hepatology. 2015;62(2):405-11.
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
67EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
NASH AND WEIGHT LOSS: MANAGEMENT AND BENEFICIAL ASPECTS
Eduardo Vilar-Gomez* 1
1Unit for the Clinical Management of Digestive Disease, Virgen del Rocio and Virgen de Macarena University Hospitals, Seville, Spain
Corresponding author’s email: [email protected]
Nonalcoholic fatty liver disease (NAFLD), the hepatic manifestation of the metabolic syndrome, has emerged as a leading cause of chronic liver disease worldwide and has been associated with an increased risk of diabetes and ischemic heart disease. Its overall incidence is growing rapidly associated with the parallel epidemics of obesity and type 2 diabetes. NAFLD encompasses a clinicopathologic spectrum ranging from simple steatosis to steatohepatitis (NASH), the more aggressive form of NAFLD which may progress to cirrhosis and its associated complications. Thus, an effective treatment of NASH is needed to halt disease progression. Whereas several drugs have been evaluated in clinical trials, there are currently no approved therapies for NASH. Thus, lifestyle changes focusing on weight loss remain the cornerstone of NASH treatment. Several studies have reported that degree of weight reduction appears to be positively correlated to histological improvements, and most of them concluded that at least 7-10% of WL is required to induce improvement in NAFLD activity score (NAS) and their components (steatosis, lobular inflammation and ballooning), however, weight losses ≥ 10% are required to induce highest rates of steatohepatitis resolution and 1-point of fibrosis reversal. Unfortunately, less than 50% of patients achieve the necessary weight loss goal of more than 7-10% in the trial setting, and many have questioned the sustainability of this kind of intervention. Regarding to specific macronutrient distribution for dietary interventions, benefits of low-fat vs. low-carb diets in overweight/obese patients suffering NASH are lacking, and only losing weight is a priority, reaffirming the importance of calories from any source. Adherence is likely the most important determinant of body weight reduction. More research is needed to inform future guidelines about dietary interventions for weight loss in patients with NAFLD. Thus, in the real world, an intensive lifestyle counseling must be offered to all NASH patients, however, the applicability of these interventions depends largely on their availability and real world adherence to these programs.
Disclosure of Interest: None Declared

SP
EA
KE
RS
’ AB
ST
RA
CT
S
68 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
CURRENT INSULIN SENSITISING AGENTS IN NASH
Philip N. Newsome* 1
1University of Birmingham, Birmingham, United Kingdom
Corresponding author’s email: [email protected]
Insulin resistance is a major component in the pathogenesis of NASH, and indeed many patients with NASH have concomitant type 2 diabetes mellitus. This has driven the development of therapies targeting insulin resistance as well as the use of approved diabetic therapies for patients with NASH. This talk will examine the evolution of insulin sensitising therapies in patients with NASH and speculate on their future position in the management of NASH.
Disclosure of Interest: P. N. Newsome: Grant/Research Support: Conflict with: Pharmaxis, Consultant/ Advisor: Conflict with: Boehringer Ingelheim, Pfizer, Dignity Sciences, Intercept, Johnson&Johnson, Novo Nordisk and Shire

SP
EA
KE
RS
’ AB
ST
RA
CT
S
69EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
NOVEL PHARMACOLOGICAL THERAPIES FOR NAFLD
Vlad Ratziu* 1
1Hopital Pitié Salpétrière, Paris, France
Corresponding author’s email: [email protected]
Despite the burden of disease associated with NASH, the treatment of NASH remains a significant unmet need. While simple to recommend, diet and lifestyle measures as a first-line therapy for non-alcoholic steatohepatitis (NASH) are hardly a model of successful therapy, as most clinicians can testify. They can be complex to implement, hard to sustain and of limited efficacy in advanced stages of the disease. The need for specific pharmacotherapy is now acknowledged by practitioners, the pharmaceutical industry and regulators and is largely expected by patients. The result is a clear move away from products developed second-hand for NASH (such as pioglitazone or metformin) or from generic, non-specific hepatoprotectors (such as pentoxifillin, ursodeoxycholic acid or antioxidants) towards molecules developed and tested specifically for NASH that aim to correct one or several of the pathways of liver injury in this disease. The complex pathogenesis of NASH, however, presents multiple potential therapeutic targets for which compounds are progressing in clinical development. Several compounds have already received either breakthrough status (obeticholic acid) or fast-track status (aramchol, cenicriviroc, elafibranor, GR-MD-02) from the FDA. The two most advanced molecules, obeticholic acid and elafibranor, have shown encouraging data on improving hepatic histology. Both compounds appear to clear NASH, with obeticholic acid improving liver fibrosis and elafibranor improving the glycemic and lipid profile. Much larger trials, currently ongoing, will need to confirm these preliminary data and better characterize the safety and tolerability profile. Meanwhile, other compounds are being tested, a few in phase 2b studies (cenicriviroc, aramchol for NASH, simtuzumab for NASH fibrosis) and many more in earlier, smaller trials. Most of these drug candidates target different pathways, which speaks to the diversity and dynamism of the NASH pipeline. Obeticholic acid, a farnesoid X receptor (FXR) agonist, has completed phase IIb testing. Results from the FLINT trial, demonstrated histologic improvement in patients with NASH compared with placebo: the drug improved steatosis, liver-cell injury and inflammation resulting in a significant reversal of steatohepatitis. Morevover there was also an improvement of fibrosis regardless of the baseline fibrosis stage. Findings from a subgroup analysis showed histologic improvement even in a subset of high-risk NASH patients. Adverse effects were mild to moderate and similar to those observed in the placebo group, with the exception of pruritus, which was more common and more intense compared with placebo and an increase in LDL. Recently published data with elafibranor, a dual PPAR alpha/delta agonist also have shown its ability to reverse NASH without

SP
EA
KE
RS
’ AB
ST
RA
CT
S
70 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
fibrosis worsening, particularly in a subpopulation of patients with moderate/advanced disease. This compound also improved the glycemic and lipid profile.Aramchol, a fatty acid and bile acid modifier, also has published phase II data. Patients who received aramchol 300 mg for 3 months showed a significant reduction in liver fat content compared with patients who received placebo. There was no difference in safety profiles between the treatment and control groups, and no adverse effects were attributed to therapy. A number of other compounds are currently in phase IIb testing, with no data yet available. Simtuzumab is an anti-LOXL2 monoclonal antibody with two 240-week, phase IIb trials under way in patients with NASH, with and without cirrhosis. A 2-year, placebo-controlled, phase IIb trial of cenicriviroc, a dual inhibitor of CCR2 and CCR5, is ongoing in noncirrhotic patients with NASH. Substantial progress has been made in recent years in the care of patients with NASH, including recognition of medical need, acceptance of NASH as an indication of therapy, agreement on an operational definition of NASH, and an improved understanding of targeted compounds and the path of clinical development. As additional phase IIb and phase III data accrue, and as clinicians are educated about the opportunities for reduced disease burden with targeted therapies, progress toward meeting the unmet needs of NASH is expected to move forward in strides.
Suggested ReadingsNeuschwander-Tetri BA, Loomba R, Sanyal AJ, et al. Farnesoid X nuclear receptor ligand obeticholic acid for non-cirrhotic, non-alcoholic steatohepatitis (FLINT): a multicentre, randomised, placebo-controlled trial. Lancet. 2015;385:956-965. Armstrong MG, Gaunt P, Aithal GP et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN) a multicentre double-blind randomized, placebo-controlled phase 2 study. Lancet 2016;387:679-690. Ratziu V, Harrison S, Francque S et al. Elafibranor an agonist of the PPAR alpha and delta induces resolution of NASH without fibrosis worsening. Gastroenterology 2016 in press. Barry-Hamilton V, Spangler R, Marshall D, et al. Allosteric inhibition of lysyl oxidase-like-2 impedes the development of a pathologic microenvironment. Nat Med. 2010;16:1009-1017. Marra F, Tacke F. Roles for chemokines in liver disease. Gastroenterology. 2014;147:577-594. Sanyal A . use of FXR agonists to treat non alcoholic fatty liver disease. Dig Dis 2015;33:426-32Safadi R, Konikoff FM, Mahamid M, et al. The fatty acid-bile acid conjugate aramchol reduces liver fat content in patients with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol. 2014;12:2085-2091. Ratziu V. Novel pharmacological options for NASH. Dig Dis Sci 2016 in press
Disclosure of Interest: None Declared

ePOSTERABSTRACTS

ePO
ST
ER
AB
ST
RA
CT
S
72 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Thursday 12 May 2016ePoster Session 1: 13:30 – 14:00
Screen 1: MR-146
DYSMETABOLIC IRON OVERLOAD SYNDROME IN NON-ALCOHOLIC FATTY LIVER DISEASE PATIENTS
Paula Fabrega1, Claudia P. Oliveira* 2, Hilton M. Leão-Filho3, Jose Tadeu Stefano2, Cintia Cercato1
1ENDOCRINOLOGY, 2GASTROENTEROLOGY, 3RADIOLOGY, University of São Paulo School of Medicine, SAO PAULO, Brazil
Corresponding author’s email: [email protected]
Introduction: Dysmetabolic iron overload syndrome (DIOS) is characterized by hyperferritinemia with normal transferrin saturation, metabolic disorders and mild liver iron overload. DIOS occurs in non-alcoholic fatty liver disease (NAFLD) mainly in steatohepatitis (NASH).
Aims: This study aimed at assessing the DIOS characteristics of our NAFLD patients.
Material and Methods: We conducted a retrospective analysis of 202 patients that underwent liver biopsy due to NAFLD histologic evaluation. The period of analysis was January 2007 to December 2014. Patients were discriminate by gender, age, ferritin serum levels, liver transaminases levels, presence of comorbidities (hypertension, diabetes and dyslipidemia) and histological features of liver biopsy (inflammation, ballooning, fibrosis and steatosis).
Results: The prevalence of DIOS in our NAFLD sample was 7.7% (IC 95% 4.3 – 12.6%). The median ferritin in patients with liver iron overload was 444 ug/L (290 – 536) and in patients without was 152 ug/L (74 – 269). The difference between ferritin level in patients with and without liver iron overload was statistically significant. The cut off level of ferritin to identify liver iron overload was 329.9 ug/L (ROC curve – IC 95% = 0.72 – 0.92), sensibility of 75% and specificity of 82%. The comparison of ferritin levels and biopsy characteristic showed that higher ferritin levels is related with a more severe ballooning degree, the others features were not statistically significant.

ePO
ST
ER
AB
ST
RA
CT
S
73EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Conclusions: The ferritin serum level is an important evaluation tool for NAFLD patients, level above 329.9 ug/L may suggest liver iron overload and higher ferritin is related to a worst histological features (ballooning).
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
74 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Screen 2: MR-185
NAFLD IN CHRONIC HEPATITIS B: A COMMON FINDING WITHOUT IMPACT ON THE LIVER DISEASE PROGRESSION
Leila Mouelhi* 1, Moufida Mahmoudi1, Shema ayadi1, Fatma Houissa1, Kaouther Jery1, Yosra Said1, Radhouene Debbech1, Taoufik Najjar1
1Gastroenterology, Charles Nicolle Hospital, Tunis, Tunisia
Corresponding author’s email: [email protected]
Introduction: Nonalcoholic fatty liver disease (NAFLD) and chronic infection with hepatitis B virus (CHB) are two common causes of chronic liver disease in Tunisia. Approximately one third of patients with CHB have been reported to have NAFLD. Recent studies suggested that NAFLD is associated with antiviral therapy failure; others report suppression of viral replication in NAFLD.
Aims: We aimed to investigate the prevalence of histological evidence of hepatic steatosis, a common hepatocyte change in NAFLD, in a group of patients with chronic HBV infection undergoing liver biopsy and compared clinical data, laboratory features, severity of hepatic fibrosis, viral kinetics and virologic response to entecavir treatment, between patients both with and without steatosis.
Material and Methods: This study was designed as a retrospective monocenter cohort study. All patients with CHB, who underwent liver biopsy for diagnostic purposes over a 5-year period were enrolled in this study. Clinical, biological, and histological factors were evaluated. The impact of hepatic steatosis on pre-treatment serum HBV DNA levels and also on the virologic response to entecavir at 6 and 12 months of therapy was investigated.
Results: A total of 127 cases were involved in the study [median age 43 (19–68) years, 79 (62.2%) males, 26 received an entecavir therapy for at least 48 weeks. Steatosis was present in 28 (19.3%) of the patients.Our data showed that LS is not associated with age, sex, body mass index, HBeAg status, viral load, severity of fibrosis, amount of activity, aspartate aminotransferase, alanine aminotransferase, γ-glutamyl transpeptidase and alkaline phosphatase. However, patients with liver steatosis had higher serum triglyceride, fasting blood glucose, and serum cholesterol level (p=0.04 and 0.01 respectively).

ePO
ST
ER
AB
ST
RA
CT
S
75EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Liver steatosis had no effect on virologic response to entecavir at 6 and 12 months of treatment.Conclusions: Steatosis is a relatively common finding in CHB associated with metabolic host factors. NAFLD had no impact on either the disease progression or the virologic response to entecavir treatment.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
76 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Screen 3: MR-163
PNPLA3 AND TNF-α G238A GENETIC POLYMORPHISMS IN EGYPTIAN PATIENTS WITH DIFFERENT GRADES OF SEVERITY OF NAFLD
Mona A.-E. Hegazy* 1, Ahmed Ezzat1, Laila Rashed2, Abeer Mostafa3
1Internal Medicine, 2Medical Biochemistry, Faculty of Medicine. Cairo University, 3Pathology, National Cancer Institute. Cairo University, Cairo, Egypt
Corresponding author’s email: [email protected]
Introduction: Background: There is growing evidence that genetic as well as environmental factors play an important role in the development and progression of NAFLD. In recent years, the genetic determinants of steatosis are being identified using genome-wide association studies. We investigated the association of the SNP rs738409 in the PNPLA3 gene and the TNF-α G238A polymorphism with the development and severity of NAFLD in an overweight and obese Egyptian population.
Methods: 100 overweight and obese patients with NAFLD and 30 age- and sex- matched controls attending the Gastroenterology and Hepatology outpatient clinic of Kasr Al Ainy Hospital, Cairo University were enrolled in the study. All patients with NAFLD underwent a confirmatory biopsy after a written consent. Fasting plasma glucose, kidney and liver function tests, ALT, AST, GGT, lipid profile, HCV antibodies and HBsAg were measured in all subjects. Abdominal ultrasound was performed and all subjects were genotyped for (rs738409) PNPLA3 and (rs361525) TNF-α gene polymorphisms using PCR-RFLP.
Results: As regard the PNPLA3 gene SNP, the homozygous GG genotype was most frequent among patients with NASH (26%) when compared to those with borderline NASH (20.5%) and simple steatosis (20%). Higher serum levels of ALT and AST were observed in NAFLD patients and control subjects who were carriers of the G allele of rs738409, but this did not reach statistical significance. As regards the TNF-α G238A SNP; the frequency of the A allele was higher in NAFLD patients (20%) compared to the controls (5%) with p value=0.006. The highest TNF G allele frequency was observed in the NASH group (88%) and this was statistically significant with a p value=0.009.
Conclusion: Our study confirmed the association of the PNPLA3 (rs738409) and TNF-α promoter region G238A polymorphisms with susceptibility to NAFLD and its progression.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
77EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 4: YI-MR-117
THE CONTROLLED ATTENUATION PARAMETER (CAP) IN NAFLD AND OTHER NON-ALCOHOLIC CHRONIC LIVER DISEASES: SHOULD IT BE CONSIDERED A DIAGNOSTIC CRITERIA FOR METABOLIC SYNDROME?
Rosa Coelho* 1, Gonçalo Marinho2, Luís Ferreira-Pinto 3, Ana Maria Horta-Vale1, Guilherme Macedo1
1Gastrenterology Department, Centro Hospitalar São João, 2Faculty of Medicine, University of Porto, Porto, Portugal, 3Department of Health and Decision Sciences – CIDES, Faculty of Medicine, University of Porto, Porto, Portugal
Corresponding author’s email: [email protected]
Introduction: The prevalence of metabolic syndrome (MS) has been increasing around the world and non- alcoholic fatty liver disease (NAFLD) seems to be its liver manifestation. Fibroscan® is considered a validated alternative to liver biopsy for assessing liver stiffness. It allows the simultaneous measurement of hepatic steatosis through the controlled attenuation parameter (CAP).
Aims: The aims of this study were: i) to evaluate the CAP’s utility in chronic liver diseases (CLD), specifically in NAFLD patients, and its association with demographic, anthropometric and biochemical parameters classically evaluated in clinical practice; and ii) to establish the association between the CAP value and the MS parameters.
Material and Methods: This prospective cohort study included 94 patients with CLD: chronic hepatitis B (CHB) and C (HCV), NAFLD and autoimmune hepatitis (AIH). Anthropometric measurements, Fibroscan® values, cardiovascular risk factors, alcohol intake, medications and biochemical data were obtained.
Results: In our study, 53% of the patients were male and the mean age was 56.3±12.5 years. Disease etiology was evenly distributed: 25 patients had NAFLD (27%), 25 CHB (27%), 25 CHC (27%) and 19 AIH (20%). Considering cardiovascular risk factors, 16% of patients had type 2 diabetes and 32% hypertension. Obesity (body mass index (BMI) >30 kg/m2) was present in 16% of the patients and 23% of the patients fulfilled the MS criteria. Patients with NAFLD had higher BMI and a higher proportion of hypertension. NAFLD patients presented the highest values for γ-GT (p<0.001) and ferritin (p=0.0017). Median CAP value was higher in NAFLD patients than AIH (p=0.002) and HCV patients

ePO
ST
ER
AB
ST
RA
CT
S
78 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
(p=0.004). In NAFLD patients, median CAP value was correlated to HbA1c (p=0.019), AST (p=0.036) and γ-GT (p=0.040); it was also strongly correlated to the number of MS variables (correlation coeficient ρ=0.669, p=0.001). Considering individually the variables that define the MS, only hypertension showed a significantly higher median CAP value (p=0.038).
Conclusions: CAP is a simple, operator-independent and non-invasive tool for hepatic steatosis detection, strongly correlated to the number of MS parameters in NAFLD patients. In the future it could be added to the MS diagnostic criteria.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
79EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 5: YI-MR-124
REFRACTORY SUBACUTE STEATOHEPATITIS AFTER BILIOPANCREATIC DIVERSION: A CASE REPORT
Sander Lefere* 1, Xavier Verhelst2, Sarah Raevens1, Roberto Troisi3, Hans Van Vlierberghe1, Anja Geerts1
1Department of Gastroenterology and Hepatology, Ghent University Hospital, 2Department of Gastroenterology and Hepatology, hent University Hospital, 3Department of General, Hepatobiliary and Liver Transplantation Surgery, Ghent University Hospital, Ghent, Belgium
Corresponding author’s email: [email protected]
Introduction: As the prevalence of obesity has risen dramatically over the last decades, non-alcoholic steatohepatitis (NASH) has become a major cause of chronic liver disease. Bariatric surgery is an important therapeutic option in NASH if more conservative options fail. Nevertheless, hepatic complications following bariatric surgery, especially jejunoileal bypass surgery, occur in some patients. Severe steatohepatitis necessitating liver transplantation has also been reported following biliopancreatic diversion (BPD, or Scopinaro operation). The pathogenesis of NASH progression after bariatric surgery is poorly understood, yet small intestinal bacterial overgrowth in the surgical blind loop is a known risk factor.
Material and Methods: We present the case of a female patient who underwent BPD surgery at 19 years of age and presented with decompensated NASH cirrhosis five years later.
Results: Her condition deteriorated rapidly and she was listed for transplantation. Partial dismantling of the intestinal bypass, to prevent relapse of liver failure, was postponed until eight weeks after transplantation due to her bad general condition. Bacterial overgrowth was persistently present despite adequate antibiotic treatment. Liver biopsy at the time of dismantling already showed signs of recurrent severe steatohepatitis with hepatocellular necrosis. Because of progression to cirrhosis and clinical decompensation, she underwent retransplantation and a full restoration of intestinal anatomy. Unfortunately, refractory bacterial overgrowth remained present and the patient again developed cirrhosis. After three failed transplantations, we decided in deliberation with the patient not to pursue further therapy. The patient died shortly after.

ePO
ST
ER
AB
ST
RA
CT
S
80 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Conclusions: BPD surgery may result in severe NASH. Therapy consists of liver transplantation and timely dismantling of BPD, yet these measures were unsuccessful in our patient. Although the pathogenesis of NASH development post-bariatric surgery is complex and poorly understood, our case highlights bacterial overgrowth as a major risk factor in disease progression.
Disclosure of Interest: S. Lefere: Grant: Conflict with: Fund for Scientific Research (FWO Flanders, FWO15/ASP/146)), X. Verhelst: Grant: Conflict with: Fund for Scientific Research (FWO Flanders,1700214N), S. Raevens: Grant: Conflict with: Fund for Scientific Research (FWO Flanders, 11W5715N), R. Troisi: : None Declared, H. Van Vlierberghe: : None Declared, A. Geerts: : None Declared

ePO
ST
ER
AB
ST
RA
CT
S
81EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 6: MR-106
CONTROLLED ATTENUATION PARAMETER AND LIVER STIFFNESS MEASUREMENTS BY FIBROSCAN FOR THE DETECTION OF NON-ALCOHOLIC FATTY LIVER DISEASE IN PATIENTS WITH TYPE 2 DIABETES: RESULTS FROM A PILOT STUDY
Meryem Durgay1, 2, Oguzhan Deyneli1, Yusuf Yilmaz* 3
1Department of Endocrinology, 2Department of Internal Medicine, 3Department of Gastroenterology, Marmara University, School of Medicine, Istanbul, Turkey
Corresponding author’s email: [email protected]
Introduction: Type 2 diabetes mellitus (T2DM) is a paramount risk factor for non-alcoholic fatty liver disease (NAFLD). However, the optimal diagnostic modality for the detection of NAFLD in patients with T2DM remains controversial. In addition, current guidelines do not recommend screening for NAFLD in diabetic patients. Successful FibroScan measurements were obtained in 52 (96.2%) study patients. Hepatic steatosis, moderate fibrosis (≥F2), severe fibrosis (≥F3), and cirrhosis (F4) were detected in 90.3%, 36.6%, 19.2%, and 11.5% of the participants. Surprisingly, normal values of alanine aminotransferase (ALT) and platelet count were observed in 74.0% and 98.1% of the cirrhotic patients, respectively.
Aims: Here, we investigated the potential usefulness of FibroScan for the detection of NAFLD and severe liver fibrosis in patients with T2DM.
Material and Methods: A total of 54 patients were prospectively enrolled from the Internal Medicine Clinic of the Marmara University Medical School. Hepatic steatosis ratios were obtained with the Controlled Attenuation Parameter (CAP), whereas the fibrosis stage was investigated using Liver Stiffness Measurment (LSM) values. At least 10 valid measurements with ≤ 30% interquartile range/median (IQR/M) ratios were required to consider the tests reliable. The LSM score was calculated as the median of 10 valid measurements. In line with previous studies, the following cut-offs were used: ≥222dB/m for hepatic steatosis, ≥7.0 kPa for ≥F2 fibrosis, ≥9.6 kPa for ≥F3 fibrosis, and ≥11.5 kPa for F4 fibrosis.

ePO
ST
ER
AB
ST
RA
CT
S
82 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Results: Successful FibroScan measurements were obtained in 52 (96.2%) study patients. Hepatic steatosis, moderate fibrosis (≥F2), severe fibrosis (≥F3), and cirrhosis (F4) were detected in 90.3%, 36.6%, 19.2%, and 11.5% of the participants. Surprisingly, normal values of alanine aminotransferase (ALT) and platelet count were observed in 74.0% and 98.1% of the cirrhotic patients, respectively.
Conclusions: Patients with T2DM have a high prevalence of NAFLD and severe fibrosis that can be efficiently detected with FibroScan. Further studies on the potential clinical usefulness of this screening methodology are warranted.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
83EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Thursday 12 May 2016ePoster Session 2: 14:30 – 15:00
Screen 1: MR-103
CORONARY ARTERY CALCIUM SCORE (CACS) AND FRAMINGHAM SCORE (FS) IN EVALUATION OF CARDIOVASCULAR RISK AFTER LIVER TRANSPLANTATION
Lívia M. C. Linhares1, Claudia P. Oliveira* 1, Mario R. Alvares-da-Silva2, Jose Tadeu Stefano1, Debora R. B. Terrabuio1, Edson Abdala1, Flair Jose Carrilho1, Alberto Q. Farias1, Luiz Augusto C. D ‘ Albuquerque1
1Gastroenterology (LIM 07/ 37), University of São Paulo School of Medicine, SAO PAULO, 2Gastroenterology, Hospital de Clínicas de Porto Alegre, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil
Corresponding author’s email: [email protected]
Introduction: Cardiovascular (CV) disease is a common complication following orthotopic liver transplantation (OLT). Coronary artery calcium score (CACS) is considered a robust tool to assess cardiovascular risk (CVR). We hypothesized that liver transplantation aggravates MS and CVR along time.
Aims: The aim of the present study is to register the prevalence of MS and related diseases among OLT recipients and to know how that impacts on their CVR stratification, using FRS and CACS. Also, we want to determine whether CACS has additive value to FRS in CVR classification.
Material and Methods: Forty consecutive adult patients who underwent OLT were evaluated during outpatient clinic visits in the following four years. Anthropometric and clinical data, Framingham score (FS) and blood biomarkers of atherosclerosis after one and four years of OLT were analysed. CACS was performed at the end of the follow-up.
Results: There were 25 (62.5%) male patients, mean age of 53.8 years and mean body mass index (BMI) of 26.9 kg/m2 at the final evaluation. Prevalence of hypertension, dyslipidemia and metabolic syndrome (MS) significantly increased over time, from 37.5% to 65%, 30% to 60% and 22.5% to 47.5%, respectively. The median FS increased from
ePO
ST
ER
AB
ST
RA
CT
S
84 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
7.5% to 21% (p=0.0354), demonstrating that the 10-year CVR changed from low to high. According to CACS, 27.5% of patients had moderate/severe calcification. Five patients (12.5%) presented at least one CV event after OLT. Patients with previous CV event had higher values of CACS when compared with patients who did not have a history of CV morbidity (median 140.0 x 0; P = 0.001). A significant correlation between CACS and FS, age, alcohol, glucose, glycosylated hemoglobin and triglycerides was found. Levels of blood biomarkers of atherosclerosis did not correlated with MS, FS or CACS.
Conclusions: We concluded that the prevalence of MS and the CVR have a great increase four years after OLT, which is known to impact on late survival. CACS is a useful tool in evaluating liver transplant recipients, and probably can enhance CVR stratification and help prevent CV events in the future.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
85EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 2: MR-133
PREVALENCE AND CHARACTERISTICS OF PATIENTS WITH OBESE VERSUS NON-OBESE NON-ALCOHOLIC FATTY LIVER DISEASE (NAFLD) IN THAILAND
Chalermrat Bunchorntavakul1, Thanaya Techasirioangkun1, Tawesak Tanwandee* 2
1Internal Medicine, Rajavithi Hospital, 2Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Corresponding author’s email: [email protected]
Introduction: Non-alcoholic fatty liver disease (NAFLD) is the most common chronic liver disease worldwide that is highly associated with obesity and metabolic syndrome. The occurrence of NAFLD in non-obese population has been increasingly seen, especially in Asia. However, the characteristics and long-term prognosis of this group of NAFLD remain unclear.
Aims: To evaluate the prevalence and clinical characteristics of non-obese NAFLD.
Material and Methods: Data of > 200 consecutive patients underwent controlled attenuation parameter (CAP) and transient elastography (TE) between October 2015 and December 2015 at a tertiary center in Bangkok were analyzed. NAFLD was defined as CAP >250 without history of alcohol consumption >14 drinks per week. Obesity and overweight was defined as body mass index (BMI) ≥25 kg/m2 and ≥23 kg/m2, respectively. Metabolic comorbidities, including diabetes, dyslipidemia and hypertension, were recored.
Results: Overall, 81 patients have NAFLD: 58% were men, median age 50 (20-74) years, BMI 26.9 (18.1-40.5) kg/m2, ALT 44 (8-314) U/L and 25% have metabolic comorbidities. Among patients with NAFLD, 68% (55/81) were obese and 16% (13/81) were overweight. Transient elastography (TE) results were <7.5 kPa in 53% (43/81), 7.5-8.9 kPa in 5% (4/81), 9-11.9 kPa in 16% (13/81) and ≥12 kPa in 26% (21/81) of patients. There was no significant difference in demographic data, aminotransferase levels, degree of liver fibrosis, and comorbidities between patients with non-obese and obese NAFLD. Though, there was a trend in higher rates of advanced fibrosis among obese patients, compared to non-obese patients with NAFLD. After an exclusion of patients with HCV positive (n=31), the prevalence of non-obese NAFLD remained unchanged (32% of all NAFLD), and still there was no significant difference in clinical characteristics between patients with non-obese and obese NAFLD.

ePO
ST
ER
AB
ST
RA
CT
S
86 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Conclusions: Non-obese NAFLD is common in Thailand, with an overall prevalence of 32% among all patients with NAFLD. There was significant difference in clinical characteristics between patients with non-obese and obese NAFLD.
Figure:
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
87EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 3: YI-MR-160
CHANGES OF THE GUT MICROBIOTA IN PATIENTS WITH OBESITY, METABOLIC SYNDROME AND NONALCOHOLIC FATTY LIVER DISEASE (NAFLD) VERSUS HEALTHY CONTROLS
María Teresa Arias Loste* 1, Esther Nistal2, Carmen Alonso-Martin1, María Ballesteros Pomar3, Paula Iruzubieta1, Marta Aparicio Cabezudo4, Marcos Jimenez4, Patricia Ruiz1, Monica Molina-Edesa5, Emilio Fábrega1, Juan María García-Lobo6, Jose Luis Olcoz2, Javier Crespo1
1Hepatology Unit, Digestive Service, Hospital Universitario Marqués de Valdecilla, Research Institute Valdecilla (IDIVAL), Santander, 2Department of Gastroenterology, University Hospital of León, Institute of Biomedicine (IBIOMED) University of León,, 3Department of Endocrinology and Nutrition, University Hospital of León, 4Department of Gastroenterology, University Hospital of León, Leon, 5Department of Applied Mathematics and Computer Science., University of Cantabria. Institute of Biomedicine and Biotechnology of Cantabria (IBBITEC), 6Department of Molecular Biology., Faculty of Medicine. University of Cantabria. Institute of Biomedicine and Biotechnology of Cantabria (IBBITEC), Santander, Spain
Corresponding author’s email: [email protected]
Introduction: Several studies suggest a role for the gut microbiota in the development of obesity, metabolic syndrome and NAFLD in patients and experimental models. In addition, microbial profiling techniques developed in the past few years enabled major advances in our understanding of the role of gut bacteria and raised possible new therapeutic approximations based on the modification of the intestinal microbioma.
Aims: The aim of this study was to characterize the composition of the gut microbiota in obesity-related to NAFLD.
Material and Methods: Gut bacterial communities were identified by pyrosequencing of the 16S rDNA extracted from faecal samples of 53 obese patients and 20 healthy controls. According to clinical, analytical and ultrasonographic data, patients were classified as NAFLD or non- NAFLD.
Results: Statistical analysis showed that the number of reads of the phylum Proteobacteria was higher in obese patients than in healthy controls (p<0.05). There were also significant changes in the phylum Firmicutes (p<0.05). Obese patients with NAFLD had a higher

ePO
ST
ER
AB
ST
RA
CT
S
88 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
number of reads of this phylum than obese patients without NAFLD. In total, 617 different genera were identified. Most of the sequences were classified within six genera: Bacteroides, Prevotella, Blautia,Faecalibacterium, Clostridium and Oscillospira. The number of Blautia, Oscillospira, Flavobacterium, Alkaliphilus and Eubacterium sequences was lower in obese patients than in controls. The Mann-Whitney U-test indicated that these differences were significant (p<0.05) according to the diagnosis. While, the number of Prevotella, Megasphaera, Lactobacillus, Megamonas and Acidaminococcus sequences revealed an increase in obese patients. These changes were also significant (p<0.05). Obese patients with NAFLD showed similar changes in the same genera in comparison with healthy controls. However, there were not significant differences associated to metabolic syndrome.
Conclusions: Besides differences in phylum, we have observed differences in the proportion of bacterial genera within gut microbiota of obesity-related NAFLD. Obese patients display a higher bacterial richness, and these differences are distinct between NAFLD and non-NAFLD patients. Taken together, our data support the role of dysbiosis in NAFLD development, pointing to the potential role of microbiota modification as a target in obesity-related NAFLD management.Supported by BFU2013-48141-R and BIO/LE02/15. CIBERehd funded by ISCIII.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
89EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 4: YI-MR-161
INTERVENTION WITH THE CCR2 INHIBITOR PROPAGERMANIUM ATTENUATES INSULIN RESISTANCE, ADIPOSE TISSUE INFLAMMATION AND DEVELOPMENT OF NASH
Petra Mulder* 1, Anita M. van den Hoek1, Robert Kleemann1
1Metabolic Health Research, Netherlands Organization for Applied Scientific Research (TNO), Leiden, Netherlands
Corresponding author’s email: [email protected]
Introduction: Obese patients with insulin resistance (IR) and chronic inflammation in white adipose tissue (WAT) have a high risk of developing non-alcoholic steatohepatitis (NASH). The C-C chemokine receptor-2 (CCR2) has a crucial role in the recruitment of immune cells to WAT and liver thereby promoting the inflammatory component of the disease.
Aims: Herein, we examined whether intervention with propagermanium, an inhibitor of CCR2, would attenuate tissue inflammation and NASH development. To mimic the situation in patients, mice with established obesity, IR and WAT inflammation were subjected to treatment.
Material and Methods: Male C57BL/6J mice received a high-fat diet (HFD) for 0,6,12 and 24 weeks to characterize IR development and WAT inflammation (by hyperinsulinemic-euglycemic clamp and histology, respectively) and to define the optimal time point for intervention. In a separate study, mice were pretreated with HFD and then treated with propagermanium (0.05% w/w) after 6 weeks (early intervention) or 12 weeks (late intervention). NASH was analyzed after a total of 24 weeks.
Results: IR developed in WAT after 6 weeks of HFD, which was paralleled by modest WAT inflammation. IR and inflammation in WAT intensified after 12 weeks of HFD, and preceded the development of NASH (24 weeks). The subsequent CCR2 intervention experiment showed that early, but not late, propagermanium treatment attenuated IR. Only the early treatment significantly decreased Mcp-1 and Cd11c gene expression in WAT indicating reduced WAT inflammation. Histopathological analysis of liver demonstrated that propagermanium treatment decreased macrovesicular steatosis and tended to reduce lobular inflammation, with more pronounced effects in the early intervention

ePO
ST
ER
AB
ST
RA
CT
S
90 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
group. Propagermanium improved the ratio between pro-inflammatory (M1) and anti-inflammatory (M2) macrophages, quantified by Cd11c and Arginase-1 gene expression in both intervention groups.
Conclusions: Early therapeutic intervention with the CCR2 inhibitor propagermanium improves IR, reduces WAT inflammation and attenuates NASH development.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
91EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 5: YI-MR-164
NorUDCA IMPROVES LIVER INJURY AND GLUCOSE SENSITIVITY IN MOUSE MODELS OF OBESITY AND STEATOSIS
Daniel Steinacher* 1, Thierry Claudel1, Tatjana Stojakovic2, Elisa Einwallner3, Michael Trauner1 and Prof. Dr. Michael Trauner1Internal Medicine 3, Medical University of Vienna, Vienna, 2Clinical Institute of Medical and Chemical Laboratory Diagnostics, Medical University of Graz, Graz, 3Clinical Institute of Medical and Chemical Laboratory Diagnostics, Medical University of Vienna, Vienna, Austria
Corresponding author’s email: [email protected]
Introduction: Bile acids (BA) have signaling functions and regulate a variety of metabolic and inflammatory pathways. Ursodeoxycholic acid (UDCA) is the only BA used as therapeutic in humans, but showed only limited efficacy in NASH. NorUDCA is a side-chained shortened derivative of UDCA improving liver injury in mouse models of cholestatic liver and bile duct injury.
Aims: We aim to explore whether NorUDCA improves hepatic steatosis and insulin resistance in mouse models of obesity and steatosis.
Material and Methods: ob/ob mice received either a diet supplemented with 0.5% NorUDCA(n=7) or chow diet(n=7) for 6weeks. Intraperitoneal glucose and insulin tolerance tests (IPGTT,IPITT) were performed at week 5&6. wt/wt mice received either high-fat-diet (HFD 61% fat) supplemented with 0.5% NorUDCA (n=6) as prevention arm for 28 weeks or HFD alone for 28 weeks (n=7) or HFD for 22weeks following 6 weeks of HFD supplemented with 0.5% NorUDCA (n=6) as treatment arm. Metabolic characterizations was done by metabolic cages, IPGTT and IPITT. Food and water intake as well as bodyweight were recorded weekly. Serum biochemistry, liver histology, mRNA and protein expression of key markers of inflammation, ER-stress, lipid and glucose metabolism were analyzed.
Results: ob/ob mice treated with NorUDCA showed a reduction in serum AST, ALT and AP levels. mRNA expression of inflammatory markers (F4/80, MCP1 and tnfalpha) were reduced in liver and F4/80 was reduced in white adipose tissue. Furthermore, ER stress markers GRP78, CHOP, sXPB1, ErDj4 were lowered in liver. WAT/bodyweight ratio was increased 1.4 times in NorUDCA group, non-esterified fatty acids decreased

ePO
ST
ER
AB
ST
RA
CT
S
92 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
as well as markers for improved lipid storage function PPARG2, MPGES1 and FABP4 were induced. IPGTT uncovered a significantly faster glucose clearance at 60&90min. TG content in liver did not differ, but TG in serum was increased. The prevention arm with NorUDCA in DIO setting shows a clear reduction in body weight (37% less). The treatment arm shows already within 4 weeks a weight reduction of 13% despite pair feeding to its control group. The analysis of this experimental arm is still ongoing and will be available at the time of the meeting.
Conclusions: NorUDCA treatment improves liver cell injury via reducing NASH features such as inflammation and ER stress. We observed similar beneficial effects on WAT, resulting in an overall improved metabolic situation. NorUDCA may open a new avenue of pharmacological treatment for fatty liver disease and clinical studies are warranted.
Disclosure of Interest: D. Steinacher: : None Declared, T. Claudel: : None Declared, T. Stojakovic: : None Declared, E. Einwallner: : None Declared, M. Trauner: Grant: Conflict with: Albireo, Falk, Intercept, MSD, Consultant: Conflict with: Phenex, Albireo, Falk, Genfit, Gilead, Intercept, MSD, Novatis, Other: Conflict with: norUDCA Co-Inventor Patent Held

ePO
ST
ER
AB
ST
RA
CT
S
93EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 6: YI-MR-178
ASSOCIATION BETWEEN LEFT VENTRICULAR MASS AND HEPATIC FAT CONTENT IN PATIENTS WITH NON-ALCOHOLIC FATTY LIVER DISEASE
Daniele Pastori* 1, Roberto Cangemi1, Licia Polimeni1, Francesco Baratta1, Francesco Violi1, Maria Del Ben1, Francesco Angelico2
1Internal Medicine and Medical Specialties, 2Public Health and Infectious Diseases, Sapienza University of Rome, Rome, Italy
Corresponding author’s email: [email protected]
Introduction: Cardiac abnormalities have been described in patients with non-alcoholic fatty liver disease (NAFLD) compared to those without. Transthoracic echocardiography (TTE) is a simple and accurate method to evaluate cardiac function and structure. The relationship between cardiac structure and hepatic fat content is still undefined.Aims: To investigate the association between cardiac structure and function, and non invasive markers of fatty liver.
Material and Methods: NAFLD was diagnosed by ultrasonography in 247 subjects, and classified according to Hamaguchi criteria. Fatty liver index (FLI) and Lipid Accumulation Product (LAP) were used as markers of hepatic fat content. CK-18 M30 (mIU/ml) was measured. Resting TTE was performed (GE Vivid S6). Left ventricular mass (LVM, g) was calculated by the Devereux formula. Diastolic function was assessed by pulse-wave Doppler of the mitral inflow, for peak velocity of early (E) and late (A) diastolic filling, and its ratio (E/A). The TDI of the diastolic velocities was obtained from the apical 4-chamber view at septal corner of mitral annulus for early (E’). The ratio of E/E’ was also calculated. Systolic left ventricular function was assessed by ejection fraction (EF, %).
Results: Mean age was 58.3±11.0 years; 36.8% were female and 31.2% were diabetic patients. Mean LAP was 89.9±59.8: mean FLI was 73.1±23.3. Mean CK18 was 152.7±46.0 mIU/ml. In women, LVM was correlated to FLI (r=0.388, p<0.001), LAP (r=0.317, p=0.002), CK18 (r=0.276, p=0.019) and BMI (r=0.338, p=0.001). LVM was correlated with FLI (r=0.198, p=0.019), BMI (r=0.361, p<0.001) and HOMA-IR (r=0.265, p=0.002) in men. Diastolic function and EF were not correlated with hepatic indexes. A multivariable linear regression analysis, showed that LAP (B: 0.227, p=0.048) was independently associated with LVM in women but not in men. Similar results were

ePO
ST
ER
AB
ST
RA
CT
S
94 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
obtained in a second model, in which FLI was associated with LVM in women but not in men (B: 0.375, p=0.033). Conclusions: We found that LVM, assessed by TTE is associated with fat liver content in women but not in men. Mechanisms underlying this gender difference deserve more investigation.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
95EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Thursday 12 May 2016ePoster Session 3: 17:00 – 17:30
Screen 1: MR-102
EVALUATION OF HEPATOCELLULAR CARCINOMA (HCC) BY 18 FDG MICROPET-CT ON EXPERIMENTAL MIXED RODENT MODEL OF NONALCOHOLIC STEATOHEPATITIS (NASH)-RELATED HCC
Fernando G. Costa1, Jose Tadeu Stefano1, Caio S. Levy1, Mariana M. Torres1, Camila Maria L. Machado2, Camila G. Carneiro2, Daniele P. Faria2, Carlos Alberto Buchpiguel2, Bruno Cogliati3, Flair Jose Carrilho1, Claudia P. Oliveira* 1
1Gastroenterology (LIM-07), 2Radiology and Oncology (LIM-24), University of São Paulo School of Medicine, 3Pathology, School of Veterinary Medicine and Animal Science, University of São Paulo, SAO PAULO, Brazil
Corresponding author’s email: [email protected]
Introduction: Our group have been showed a mixed rodent model that develops NASH, cirrhosis and hepatocellular carcinoma (HCC). Positron emission tomography (PET)/computed tomography (CT) with 18F-FDG (18-fluoro-2-deoxyglucose) may be applied to evaluate HCC development, quantify the tumor load, identify metastatic spread and quantify the treatment response to a testing drug.
Aims: Our aim is to evaluate advanced HCC using 18-FDG PET/CT on experimental mixed rodent model of HCC NASH-related.
Material and Methods: Male Sprague-Dawley rats with 8 weeks were used and NASH-related HCC was induced by hyperlipidic choline-deficient diet and diethylnitrosamine (100 mg/L) in the drinking water during 19 weeks. After this period, the animals were anesthetized using isoflurane (5% for induction, 2.0%–3.0% for maintenance) in 100% oxygen, injected intravenously with 37 MBq of 18F-FDG and submitted to 18FDG microPET/CT. CT images were acquired immediately before PET imaging for helping anatomical information for fusion with PET images. The PET image is acquired using 1536 ring detectors, detectors LYSO and LGSO. PET and CT) were fused using PMOD™ software. On the day after the last PET/CT, they were anesthetized and sacrificed. Liver samples were collected for histological analysis.

ePO
ST
ER
AB
ST
RA
CT
S
96 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Results: We studied by PET scan nine animals that survived until 19 weeks. The mortality of all the animals was 22% in this animal model. CT showed low-attenuation lesions with early contrast enhancement. Besides, PET scan analyses, some of these lesions have increased 18FDG uptake, suggesting a high glycolytic metabolic rate according grade of differentiation. The mean number of nodules was 5.12 ± 6.36. Of these nodules, 53.7% were HCC in PET scan, 14.6% and 31.7% high grade and low grade dysplastic lesion respectively. Using Edmondson & Steiner classification for HCC lesion we had: 22.7% grade 1, 22.7% grade 2, 36.4% grade 3 and 18.2% grade 4. 18-FDG PET/CT had 62.5% of sensitivity and 100% specificity for diagnosing HCC. Also, PET/CT identified metastases in this model.
Conclusions: 1) Our mixed rodent model is suitable to study early and advanced NASH-related HCC, as well high and low grade dysplasia; 2) PET-CT scan can be used in this HCC rodent model for diagnosis, however primarily, evaluates the aggressive behavior of HCC demonstrated by high glycolytic metabolic rate according grade of differentiation. This approach can have utility to follow new therapeutic drugs, and identify metastatic spread.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
97EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 2: YI-MR-162
HIGH INCIDENCE OF NON-ALCOHOLIC FATTY LIVER DISEASE IN FIRST EPISODE SCHIZOPHRENIA SPECTRUM PATIENTS: A 3 YEARS PROSPECTIVE STUDY
María Teresa Arias Loste* 1, María José Morlan-Coarasa2, Carmen Alonso-Martin1, Paula Iruzubieta1, Silvia Alvarez1, Obdulia Martínez-García2, Angel Estebanez1, Victor Ortiz-García de la Foz2, Emilio Fábrega1, Benedicto Crespo-Facorro2, Javier Crespo1
1Hepatology Unit, Digestive Service, Hospital Universitario Marqués de Valdecilla, Research Institute Valdecilla (IDIVAL), 2Psychiatric Unit, Hospital Universitario Marqués de Valdecilla, Research Institute Valdecilla (IDIVAL) , Santander, Spain, Santander, Spain
Corresponding author’s email: [email protected]
Introduction: Patients with schizophrenia spectrum disorders have increased morbidity and mortalitylargely due to cardiovascular (CV) disease, which is associated with weight gain and metabolic side effects from antipsychotic medications. In this scenario, it is reasonable to expect an increase in the incidence of nonalcoholic fatty liver disease (NAFLD).
Aims: Therefore, the aim of our study is to investigate the development of NAFLD during the first 3 years of antipsychotic treatment in drug-naïve patients with first episode non-affective psychosis.
Material and Methods: Subjects included in this study were drawn from a prospective, randomized, open-label clinical trial. 205 subjects were included in the analysis. The NAFLD fibrosis score, FIB-4 score and the Fatty Liver Index (FLI), were calculated at baseline, 3 months, and then yearly for 3 years.
Results: Based on the FLI, 14 patients (6.83%; 14/205) had a basal score that predicted hepatic steatosis (HS) and, therefore, were excluded. Thus, 191 subjects were included in the final analysis and showed either an indeterminate score (34/191; 17.8%) or were ruled out for HS (157/191; 82.2%). At the end of the follow-up, 25.1% (48/191) of the individuals showed a FLI score ≥60, which is a predictor of HS. Of the individuals considered indeterminate at baseline, 64.7% developed HS, most within the first 2 years. In contrast, only 16.6% of the individuals who had a FLI score <30 at baseline, developed HS during the follow-up. HS development was significantly associated with an increase

ePO
ST
ER
AB
ST
RA
CT
S
98 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
>7% of the BMI (HS 91.7%; non-HS 55.9%; p<0.001), an increase in the triglyceride levels >150 mg/dl (HS 54.2%; non-HS 5.6%; p< 0.001), a decrease in the HDL levels <40 mg/dl in men and 50 mg/dl in women (HS 41.7%; non-HS 17.5%; p=0.001), hypertension (HS 19.5 %; non-HS 4.5%; p=0.002) and a waistcircumference >102 cm in men and >88 cm in women (HS 68.8 %; non-HS 14.0%; p<0.001) at the end of the follow up. None of the patients showed significant liver fibrosis according to the NAFLD fibrosis or FIB-4 scores.
Conclusions: A significant proportion of patients develop NAFLD in a short period of time after the first episode of their illness. Although further studies, including imaging techniques, liver stiffness and/or biopsy, are needed to confirm our data, our results support the importance of monitoring NAFLD development in these patients. The early detection of features of NAFLD may lead to a more careful and accurate cardiovascular surveillance and management in this subset of patients.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
99EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 3: YI-MR-167
OBETICHOLIC ACID ATTENUATES FIBROSIS DEVELOPMENT IN A HIGH-FAT DIET INDUCED NASH MODEL (LDLR-/-.LEIDEN MICE)
Martine C. Morrison1, Petra Mulder* 1, Roeland Hanemaaijer1, Reinout Stoop1, Claire Emson2, Kelvin Li2, Martin Decaris2, Scott Turner2, Robert Kleemann1, Peter Y. Wielinga1
1Metabolic Health Research, Netherlands Organization for Applied Scientific Research (TNO), Leiden, Netherlands, 2KineMed Inc., Emeryville, CA, United States
Corresponding author’s email: [email protected]
Introduction: The LDLr-/-.Leiden mouse is a translational, diet-inducible model for non-alcoholic steatohepatitis (NASH) with associated fibrosis, displaying many clinically relevant features of NASH.
Aims: Here, we aimed to study whether the progression of fibrosis in this model can be retarded or reverted by dietary or pharmaceutical intervention.
Material and Methods: LDLr-/-.Leiden mice were fed a high-fat diet (HFD) for 24w, after which mice were randomized into 4 groups: one group was sacrificed, one continued on HFD, one was switched to chow (dietary intervention) and one received HFD + 10 mg/kg obeticholic acid (OCA) for the remainder of the study (up to 34w). Development of NASH and hepatic fibrosis was assessed blindly by a pathologist, as well as by direct measuring collagen synthesis rates (assessed as the incorporation of deuterium from heavy water into the stable C-H bonds of hydroxyproline (OHP) in the newly synthesized protein).
Results: Both, dietary and OCA intervention improved hepatic steatosis and inflammation, which were manifest after 24w and continued to progress in the 34w HFD group. After 24 weeks of HFD feeding, mice displayed mild fibrosis (5.6±1.4% of perisinusoidal area) which progressed to 25.3±4.9% after 34w of HFD. Mice that were switched to chow diet or treated with OCA showed reduced fibrosis development (9.8±2.8% and 14.5±3.4% at t=34w resp., both p<0.05 vs HFD at t=34w). In line with this, analysis of de novo collagen synthesis showed that both the dietary and the OCA intervention reduced the rate of fibrogenesis relative to HFD control (10.8±1.0% new OHP in 14 days in HFD; 7.5±1.0% in chow and 8.3±0.6% in OCA; both p<0.05 vs HFD).

ePO
ST
ER
AB
ST
RA
CT
S
100 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Conclusions: These data show that LDLr-/-.Leiden mice develop NASH with progressive fibrosis when fed a HFD, which is modifiable by dietary and pharmaceutical interventions.
Disclosure of Interest: M. Morrison: : None Declared, P. Mulder: : None Declared, R. Hanemaaijer: : None Declared, R. Stoop: : None Declared, C. Emson: Employee: Conflict with: KineMed Inc., K. Li: Employee: Conflict with: KineMed Inc., M. Decaris: Employee: Conflict with: KineMed Inc., S. Turner: Employee: Conflict with: KineMed Inc., R. Kleemann: : None Declared, P. Wielinga: : None Declared
ePO
ST
ER
AB
ST
RA
CT
S
101EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 4: YI-MR-105
EXERCISE THERAPY IN PATIENTS CONSUMING MODERATE ALCOHOL: A RANDOMISED CONTROL TRIAL
David Houghton* 1, Kate Hallsworth2, Christian Thoma3, Sophie Cassidy3, Timothy Hardy3, Kieren G. Hollingsworth4, Roy Taylor4, Christopher P. Day3, Steve Masson3, Stuart McPherson3, Quentin M. Anstee3, Micahel I. Trenell3 and MoveLab, Newcastle University1Institute of Cellular Medicine, Newcastle University, Newcastle UpinTyne, 2Institute of Cellular Medicine, Newcastle University, Newcastle Upon Tyne, 3Institute of Cellular Medicine, 4Newcastle Magnetic Resonance Centre, MoveLab, Newcastle University, Newcastle UpinTyne, United Kingdom
Corresponding author’s email: [email protected]
Introduction: Lifestyle change remains the cornerstone of non-alcoholic fatty liver disease (NAFLD) management. Given the interaction between alcohol consumption and obesity-related liver injury, it is important to determine the impact of increased exercise in people that drink moderate amounts of alcohol.
Aims: This study aimed to define the effect of a 12-week exercise intervention on liver steatosis and its mediators in patients with metabolic syndrome associated fatty liver disease that also consume moderate amounts of alcohol.
Material and Methods: 27 patients (mean age 54 ± 11 years, BMI 31 ± 4kg/m2) who were drinking moderate amounts of alcohol (mean 221 ± 75 g/week) were randomised to either 12-weeks exercise (n = 14) or continued standard care (n = 13). Patients were instructed to maintain baseline weight and alcohol consumption. Hepatic triglyceride content (HTGC), subcutaneous and visceral adiposity, body composition, metabolic control, and non-invasive scores for fibrosis were measured at baseline and 12-weeks.
Results: 12-weeks of exercise produced beneficial effects on subcutaneous fat (-23 ± 28 vs. 12 ±19 cm2, P<0.01), whole body fat (-2.1 ± 1.1 vs. 0.2 ± 2.1 kg, P<0.01) and lean body mass (+1.9 ± 1.4 vs. +0.7 ± 1.5 kg, P<0.01) without any change in body weight. There was a significant exercise-induced reduction in cytokeratin-18 (CK-18) (-49 ± 82 vs. 17 ± 38 U/L, P<0.05). No change in HTGC (-0.2 ± 1.2 vs. +0.5 ± 2.1%, P>0.05), HOMA IR (-0.1 ± 0.5 vs. +0.1 ± 0.7, P>0.05), ALT (-6.8 ± 21.3 vs. +3.8 ± 40.0, P>0.05) or NAFLD fibrosis score were observed.

ePO
ST
ER
AB
ST
RA
CT
S
102 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Conclusions: This is the first randomised controlled trial reporting the effects of exercise on liver steatosis and its mediators in patients consuming moderate amounts of alcohol. Exercise significantly improved body composition and markers of hepatocyte apoptosis (CK-18) but, in contrast to reports in strictly defined NAFLD, there was no benefit on HTGC or metabolic control. This suggests that exercise on its own, without a concomitant reduction in alcohol intake may be insufficient to alter steatosis. However, may still ameliorate steatohepatitic liver injury in ‘real-world’ alcohol consuming dual-aetiology fatty liver patients. These pilot data warrant further investigation with histological endpoints.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
103EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 5: MR-130
FATTY LIVER INDEX (FLI) AS A MULTIDISCIPLINARY SCORE NOT ONLY FOR A CORRECT DIAGNOSIS OF NONALCOHOLIC FATTY LIVER DISEASE (NAFLD) BUT ALSO TO IMPROVE ACCURACY IN CARDIOVASCULAR DISEASE IN DIABETIC TYPE 2 PATIENTS
Diego Caroli* 1, Andrea Nogara1, Erik Rosa Rizzotto2, Gianni Ballarin1, Angelo Boscolo Bariga1, Silvia Zanoni1, Stefano De Boni1, Giorgio Cavallarin1, Cinzia Marafin1, Margherita Inglese1, Mario Della Loggia1, Marina Bortolotti1, Roberto Valle1, Laura Peraro2, Salvatore Lobello2, Franca De Lazzari2 and A.Nogara1, E.Rosa-Rizzotto2, G.Ballarin1, A.Boscolo Bariga1, S.Zanoni1, S.De Boni1, G.Cavallarin1, C.Marafin1, M.Inglese1, M.Della Loggia1, M.Bortolotti3, R.Valle3, L.Peraro2, S.Lobello2, F. De Lazzari2 1Hospital, Chioggia-Venice, 2Gastroenterology, Hospital, Sant Antonio Padova, Italy
Corresponding author’s email: [email protected]
Introduction: NAFLD is an increasingly cause of liver damage in western countries and it is characterized by increased serum triglyceride and LDL,reduction of HDL,insulin resistance,glucose intolerance;all of those are crucial risk factors for the development of atherogenesis. The United Kingdom Prospective Diabetes Study(UKPDS risk engine v 2.0) and Fatty liver index(FLI) are validated prognostic scores for cardiovascular (CV) risk in diabetics patients and NAFLD respectively.
Aims: to compare FLI and UKPDS scores to predict CV risk in a cohort of diabetic type 2 patients regularly followed up and undergone to cardiological screening according to a high risk value of UKPDS.
Material and Methods: We retrospectively analyzed 1902 patients regularly followed in our Diabetes Ambulatory in 2012-2013. Data concerning UKPDS risk engine,FLI and the successive CV screening were collected for each patient. 99/1902(19.2%) patients resulted at high CV risk after UKPDS evaluation and undergone to CV screening (ergometric/ecostress test (EET), coronarography (CORO)). Statistical analysis Two tailed t-test,Person’s Chi square test and Analysis of variance(ANOVA) were used.

ePO
ST
ER
AB
ST
RA
CT
S
104 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Results: 66(59 M,mean age 68.1y,mean duration disease 16.1 y, HbA1c>7 prevalent) pts presented UKPDS positive/FLI >60, 8/66 CORO+ (5 PTCA,3 CABG,1PTA AAII) and 5 (4M,mean age 68.6y, mean duration disease 18.4 y,HbA1c >7 prevalent) pts presented UKPDS positive/FLI<20,1/5 CORO+ (1 PTCA;1 CABG;0 PTA AII). We were able to assess a FLI cutoff to better identify,compared to UKPDS, patients that will be positive at CORO(FLI > 52 detected 9/14 pts positive at CORO with p<0.05). 99 pts UKPDS positive(EET negative 69.6%>69/99) (100%>14/14 CORO+) vs 81 pts FLI >52 (EET negative 92.5%>75/81) (64.2%>9/14 CORO+). As expected we found a significative association between CORO+ and FLI+ patients for microalbuminuria (p<0.048); Cholesterol (p<0.020); triglyceride (p<0.001); LDL (p<0.005). The only drug associated to CV risk was the cardioaspirn(p< 0.003).
Conclusions: . FLI could be used to attribute the correct CV risk in patient with FLI>52 in these way we can reduce the number of patients that undergo to CV screening with low percentage of positivity.An early and aggressive program of follow up and treatment could be established in diabetic type 2 patients with FLI>52 and with reasonable suspicion of NAFLD because this population has higher risk to develop CVevents in comparison to FLI<20.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
105EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 6: MR-109
TM6SF2 KO AND PNPLA3 I148M KNOCKIN MICE AS NAFLD ANIMAL MODELS: SIMILAR BUT NOT THE SAME
Eriks Smagris* 1 on behalf of Helen Hobbs /Jonathan Cohen Lab and Helen Hobbs / Jonathan Cohen Lab1Molecular Genetics, The University of Texas Southwestern Medical Center at Dallas, Dallas, United States
Corresponding author’s email: [email protected]
Introduction: Uncertainty regarding the molecular basis of nonalcoholic fatty liver disease (NAFLD) has been a significant obstacle toward development of effective therapies. To overcome this problem in recent years our lab generated several animal models for nonalcoholic fatty liver disease using 2 most common mutation (PNPLA3 I148M and TM6SF2 E167K) associated with human fatty liver diseases.
Aims: To compare two mice NAFLD models – Pnpla3 I148M knock in and Tm6sf2 knock out mice, trying to understand pathophysiological differences between them.
Material and Methods: Homozygous Pnpla3 I148M KI and Tm6sf2 E167K KO mice were generated by homologous recombination, heterozygous mice breeding and were compared with wild type littermates, to see differences in response on different diets (chow, high sucrose diet and high fat diet), changes in liver and plasma, changes in glucose homeostasis.
Results: For Pnpla3 I148M KI only feeding with high sucrose diet (HSD) cause excess fat accumulation in liver, without any evidence of dyslipidemia, liver inflammation or disturbances in glucose metabolism. Instead Tm6sf2 KO mice shows fatty liver accumulation on any of tried diets, accumulates in liver not only triglycerides but also cholesterol esters, have lover levels of plasma cholesterol, shows mild transaminitis and impairment of fat absorption from small intestine. Similar to Pnpla3 I148M KI, Tm6sf2 KO mice shows no changes in glucose homeostasis and no hepatic inflammation. For Pnpla3 I148M KI mice shows 40 X accumulation of mutant protein on lipid droplets, but absence of Tm6sf2 cause also reduced expression of hepatic Pnpla3.
Conclusions: Even Pnpla3 I148M KI and Tm6sf2 E167K KO mice have histologically similar NAFLD, mechanism of fat accumulation in liver is quite different. In case of

ePO
ST
ER
AB
ST
RA
CT
S
106 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Pnpla3 mutation, Pnpla3 protein accumulates on lipid droplets disrupting normal lipid droplet architecture. Instead absence of Tm6sf2 impairs lipidation of interahepatic and small intestine lipoproteins. In both cases NAFLD don’t change glucose homeostasis.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
107EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Thursday 12 May 2016ePoster Session 4: 19:00 – 19:30
Screen 1: MR-108
IMPACT OF AEROBIC EXERCISE IN POSTMENOPAUSAL WOMEN WITH NONALCOHOLIC FATTY LIVER DISEASE: A 24 – WEEK RANDOMIZED CLINICAL TRIAL
Rosamar E. Rezende 1, Sebastião M. Duarte 1, Jose Tadeu Stefano1, Hamilton Roschel2, Bruno Gualano2, Ana Lucia Sa-Pinto2, Denise C. Vezozzo1, Flair Jose Carrilho1, Claudia P. Oliveira* 1
1GASTROENTEROLOGY – LIM 07, 2DIVISION OF RHEUMATOLOGY, UNIVERSITY OF SAO PAULO SCHOOL OF MEDICINE, SAO PAULO, Brazil
Corresponding author’s email: [email protected]
Introduction: Nonalcoholic fatty liver disease (NAFLD) is common in postmenopausal women and it is associated with an increased prevalence of cardiovascular disease.
Aims: We evaluated the effectiveness of aerobic physical activity in reducing hepatic steatosis, metabolic and cardiovascular risks in postmenopausal women with NAFLD.
Material and Methods: Forty sedentary postmenopausal women (mean age 55.3 ± 8.0 years), biopsy-proven NAFLD were randomly divided into two parallel groups: an exercising group (19 patients) and a control group (non-exercising, 21 patients). The exercise group underwent a supervised aerobic physical activity program of 120min/week for 24 weeks. The anthropometric parameters, body composition, hepatic, lipid, and glycemic profiles, homeostasis model assessment-insulin resistance index, cytokines, transient elastography – FibroScan [liver stiffness/controlled attenuation parameter (CAP)], cardiopulmonary exercise test were evaluated at baseline and after 24 weeks of protocol.
Results: At baseline there were no significant differences in anthropometric, metabolic, inflammatory parameters; stiffness and liver fat content by FibroScan between the groups. After 24 weeks, we observed a decrease of waist circumference (WC), an increase of high-density lipoprotein cholesterol (HDL) levels (p<0.05) and improved cardiopulmonary functional capacity in the exercise group. Besides, the CAP analysis showed no significant

ePO
ST
ER
AB
ST
RA
CT
S
108 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
decrease of hepatic steatosis in the exercise group. However, in regards the systemic inflammation there were no significant differences in the cytokines between the groups.
Conclusions: An aerobic physical activity program of 24 weeks in NAFLD postmenopausal women showed improvement in some variables such as WC, HDL, cardiopulmonary performance that may be beneficial in improving cardiovascular risk factors in this population.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
109EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 2: YI-MR-168
THE FTO rs1421085 T>C POLYMORPHISM IS ASSOCIATED WITH THE SEVERITY OF NON-ALCOHOLIC FATTY LIVER
María Teresa Arias Loste* 1, Rocío Gallego-Durán2, Carmen Alonso-Martin1, Paula Iruzubieta1, Susana Llerena1, Javier Ampuero2, Antonio Gil-Gómez2, Javier Abad3, Jose Luis Calleja3, Raúl Jesús Andrade4, Carmelo García-Monzón5, Manuel Romero-Gómez2, Javier Crespo1
1Hepatology Unit, Digestive Service, Hospital Universitario Marqués de Valdecilla, Research Institute Valdecilla (IDIVAL), Santander, 2Inter-Centre Unit of Digestive Diseases & CIBERehd, Virgen Macarena – Virgen del Rocío University Hospitals, University of Sevilla. Instituto de Biomedicina de Sevilla (IBiS), Sevilla, 3Gastroenterology Department, Hospital Puerta de Hierro, Madrid, Madrid, 4Inter-Centre Unit of Digestive Diseases & CIBERehd., Virgen de la Victoria University Hospital. Instituto de Investigación Biomédica de Málaga (IBIMA), Malaga, 5Liver Research Unit, University Hospital Santa Cristina and CIBERehd. Instituto de Investigación Sanitaria Princesa, Madrid, Spain
Corresponding author’s email: [email protected]
Introduction: It has been recently described the role of FTO rs1421085 T>C polymorphism in the downregulation of adipocyte thermogenesis and its association with obesity development
Aims: The aim of our study was to evaluate the role of FTO rs1421085 variant in NAFLD severity in a cohort of Spanish patients
Material and Methods: Cross-sectional multicentre study including a cohort of consecutive NAFLD patients. Patients from a single centre as well as a subset of healthy controls composed estimation cohort. Diagnosis of NAFLD was established according to clinical, ultrasonography, and transient elastometry criteria, and also histological evaluation when available. FTO rs1421085 SNP was determined by allelic discrimination using Taqman probe. A set of biopsy-proven multicentre NAFLD patients was used as validation cohort.
Results: 393 subjects were genotyped: 185 NAFLD patients and 208 healthy volunteers. Genotype frequency was similar between both groups. Rs1421085 genotype distribution in NAFLD patients was: CC 22.2% (41/185), CT 49.2% (91/185) and TT 28.6% (53/185).

ePO
ST
ER
AB
ST
RA
CT
S
110 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
In 88/185 cases (47.6%) liver biopsy was performed. Of them, 60% (53/88) of patients confirmed NASH diagnosis according to Brunt´s classification. Additionally, in absence of histological data, the diagnosis of NASH was established in 5/97(5.2%) cirrhotic patients according to transient elastometry, biochemistry and clinical criteria. A statistically significant higher proportion of CC genotype was found among NASH compared to steatosis simple patients (32.8% (19/58) vs 17.3%(22/127); [O.R. 2.33 [95%CI 1.14-4.76]; p = 0.03). In the subset of patients with BMI<40 kg/m2 40.54%(75/185), these differences were remarkable ( 40%(10/25) vs 14%(7/50); [O.R. 4.10 [95%CI 1.32-12.69]; p =0.02). In the validation set, 216 patients were included. Fibrosis distribution was F0: 58.8% (127/216), F1: 19.0%(41/216), F2: 11.6% (25/216), F3: 9.7%(21/216) and cirrhosis 1% (2/216). 12% (26/216) of patients showed a NAS score higher than 5. Rs1421085 genotype distribution was: CC 14.4% (31/216), CT 43.5% (94/216) and TT 42.1% (91/216). Genotype CC was found associated with NAS Score >5 [O.R. 2.55 (95% CI 0.97-6.69); p=0.05] and lobular inflammation [O.R. 2.32 (95%CI 1.03-5.19); p=0.04].
Conclusions: To our knowledge, this is the first study showing an association between FTO rs1421085 and NAFLD severity. The reduction in adipocyte mitochondrial thermogenesis of this polymorphism could be associated, with the severity of liver injury in non-morbid obese NAFLD
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
111EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 3: MR-192
SILIBININ EXERTS BENEFICIAL EFFECTS ON GUT-LIVER AXIS IN MURINE AND HUMAN NON-ALCOHOLIC FATTY LIVER DISEASE
Federico Salomone* 1, Justyna Godos2, Maurizio Catania3, Giovanni Magrì1, Fabio Galvano2
1Division of Gastroenterology, Ospedale di Acireale, Azienda Sanitaria Provinciale di Catania, 2Department of Biomedical Sciences and Biotechnologies, University of Catania, 3Division of Laboratory Medicine, Ospedale di Acireale, Azienda Sanitaria Provinciale di Catania, Catania, Italy
Corresponding author’s email: [email protected]
Introduction: Clinical and experimental studies have highlighted the importance of gut-liver axis in the onset and progression of non-alcoholic fatty liver disease (NAFLD). Silibinin, a natural phenolic antioxidant, has been demonstrated to improve liver injury in human and experimental NAFLD, although it is unknown whether its hepato-protective effects may depend on modulation of gut-liver crosstalk.
Aims: In this study we aimed to identify whether silibinin may favorably impact on gut-liver axis in murine and human NAFLD.
Material and Methods: We examined the effects of silibinin in mice fed a high fat and high fructose (HFF) diet for 3 months. Expression of occludin and ZO-1 was assessed by real time PCR and western blot on jejunum samples. Portal LPS was assessed by ELISA. Liver TLR4 expression was determined by real time PCR. In a pilot study of thirty patients with NAFLD, we assessed intestinal permeability by the lactulose-mannitol test at baseline and after three months of treatment with Realsil, a nutraceutical containing silibinin.
Results: Treatment of mice with silibinin improved liver steatosis and inflammation. HFF diet was associated with reduced intestinal expression of occludin and ZO-1, indicating disruption of gut epithelial barrier. As a consequence, mice fed HFF diet displayed increased levels of portal LPS and increased liver TLR4 expression. In silibinin-treated animals, intestinal expression of occludin and ZO-1 was restored to control levels; similarly, silibinin administration reduced portal LPS and liver TLR4 levels. Interestingly, in patients with NAFLD a three month-treatment with Realsil not only decreased liver

ePO
ST
ER
AB
ST
RA
CT
S
112 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
enzymes and insulin resistance but also preserved intestinal permeability as showed by values of the lactulose-mannitol ratio.
Conclusions: In this study, we demonstrated for the first time that silibinin exerts beneficial effects on gut-liver axis both in murine and human NAFLD.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
113EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 4: YI-MR-188
SELECTIVE TARGETING OF FXR ISOFORMS α1-4 BY NOVEL BILE ACID DERIVATIVES AND INHIBITION OF LIPOTOXICITY IN HEPG2 CELLS
Hugo Brito* 1, Salete Batista2, Jorge A. Salvador2, Rui E. Castro1, Cecília M. Rodrigues1
1Research Institute for Medicines (iMed.ULisboa), Faculty of Pharmacy, Universidade de Lisboa, Lisbon, 2Faculty of Pharmacy, University of Coimbra, Coimbra, Portugal
Corresponding author’s email: [email protected]
Introduction: Farnesoid X receptor (FXR), a bile acid (BA)-activated nuclear receptor, plays a critical role in maintaining lipid, glucose and BA homeostasis. FXR expression is significantly decreased in livers of non-alcoholic fatty liver disease (NAFLD) patients and genetic ablation leads to hepatic steatosis and hyperlipidaemia. The FXR gene expresses four biologically active variants (FXRα1-4), regulating hepatic and lipid metabolism in an isoform-dependent manner. Activation of FXR variants α1 and α2 significantly reduces hepatic lipid accumulation.
Aims: Our aim was to screen potential BA-derived FXR agonists for their ability to selectively activate different FXR isoforms and protect HepG2 cells against palmitate toxicity.
Material and Methods: Twenty novel BA derivatives, synthesized based on the cholic (CA), deoxycholic (DCA), chenodeoxycholic (CDCA) and ursodeoxycolic (UDCA) acid scaffolds were incubated in HepG2 cells transfected with a dual-luciferase reporter construct and overexpression vector plasmids for FXRα1-4 isoforms. In parallel, BA-derivatives were co-incubated in HepG2 cells treated with 250-500 μM palmitate-BSA, for cell viability assays.
Results: As a result of the different structural modifications, BA derivatives showed differential activation of the FXRα1-4 isoforms, when compared to their precursor BAs. From the precursor BAs, only CDCA, a natural FXR ligand, significantly activated FXRα1 and α2 isoforms, with CA and UDCA displaying a modest activation of FXRα1 isoform only. Interestingly, 2 novel CA-, 1 DCA- and 4 UDCA-derivatives were stronger activators of both FXRα1 and α2, comparing with their corresponding precursors. Further, 3 novel CA-, 2 DCA-, 3 CDCA- and 4 UDCA-derivatives specifically and significantly activated

ePO
ST
ER
AB
ST
RA
CT
S
114 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
FXRα3 and α4. Finally, incubation of HepG2 cells with palmitate-BSA led to up to 35% reduction in cell viability. Co-incubation of cells with BA-derivatives targeting the FXRα1 and α2 isoforms reverted most of the palmitate-BSA-induced lipotoxicity.
Conclusions: In conclusion, herein we provide a novel strategy to screen for selective agonists of FXRα1-4 isoforms and have identified new selective BA-derived FXRα1 through 4 agonists. In addition, specific derivatives appear to afford cytoprotection against lipotoxicity. The differential functional effect of these new molecules will undoubtedly contribute for a better understanding of pharmacological targeting and therapeutic efficacy of FXR agonists in liver diseases such as NAFLD.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
115EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 5: YI-MR-134
SMOKING IS ASSOCIATED WITH FIBROSIS BUT NOT WITH NAFLD ACTIVITY
Isabelle Munsterman* 1, Mark Smits2, Rene Andriessen3, Karin van Nieuwkerk2, Elisabeth Bloemena4, Chris Mulder2, Eric Tjwa3, Erwin van Geenen3
1Gastroenterology and Hepatology, Radboud university medical center, Nijmegen, 2Gastroenterology & hepatology, Vu university medical center, Amsterdam, 3Gastroenterology & Hepatology , Radboud university medical center, Nijmegen , 4Pathology, Vu university medical center, Amsterdam, Netherlands
Corresponding author’s email: [email protected]
Introduction: Smoking is considered to be a modifying factor in the progression from non-alcoholic fatty liver disease (NAFLD) to steatohepatitis. Smoking is also associated with the onset of fibrosis in various diseases, such as NAFLD. The link with NAFLD disease activity is still unclear.
Aims: We aim to investigate the associations between smoking and NAFLD activity and fibrosis.
Material and Methods: Patients with liver biopsies performed between 2008 and 2013 in two Dutch tertiary referral university centres were identified. Characteristics such as smoking status, number of pack-years, alcohol use, diabetes and BMI were collected. A pathologist, blinded for clinical information, revised biopsies and determined the BRUNT and NAFLD activity score (NAS, ranging 0-8). Patients with a high NAS (≥ 5) were compared to patients with a low NAS (<5) and with advanced fibrosis (stage 3-4) to patients with early fibrosis (stage 0-2). We used Spearman’s Rho to assess correlation and multivariate logistic regression to identify predictors for severity of NAFLD activity and fibrosis.
Results: Sixty-five patients were included (mean age 49 ± 14.3, mean BMI of 30.3 ± 5.9, 32% female and 39% with a history of smoking). The number of pack-years was significantly higher in patients with advanced compared to early fibrosis (p = 0.011). Patients with advanced fibrosis were also older (p<0.001). For all characteristics see table 1. Additionally, there was a significant correlation between the severity of fibrosis and number of pack-years (Spearman’s rho=0.376, p=0.010).Patients with a high NAS had a median number of pack-years of 10,3 (IQR 0-24) and

ePO
ST
ER
AB
ST
RA
CT
S
116 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
patients with a low NAS a median of 0 (IQR 0-9). This was not significantly different between groups (p=0,127). No correlation was detected between smoking and NAS (Spearman’s Rho=0,224, p=0,097). Furthermore other patient characteristics such as age, diabetes, BMI or alcohol-use were similar between NAS groups. In multivariate analysis the number of pack-years was independently of diabetes associated with severity of fibrosis (OR 1,080, 95% CI 1,0180-1,146, p=0,011).
Conclusions: Smoking is associated with advanced fibrosis, but not with severity of disease activity in this cohort of patients with NAFLD. A moderate correlation was identified between the number of pack-years and increasing severity of fibrosis. These results support the advice to cease smoking in NAFLD patients.
Figure:
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
117EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 6: MR-143
CIRCULATING MICRORNAS IN PATIENTS WITH NON-ALCOHOLIC FATTY LIVER DISEASE IN TAIWAN
Jee-Fu Huang* 1, Ming-Lung Yu1, Chi-Ming Tai2, Chia-Yen Dai1, Wan-Long Chuang1
1Hepatobiliary Division, Department of Internal Medicine, KAOHSIUNG MEDICAL UNIVERSITY HOSPITAL, 2Institute of Clinical Medicine, College of Medicine, KAOHSIUNG MEDICAL UNIVERSITY, Kaohsiung City, Taiwan
Corresponding author’s email: [email protected]
Introduction: Nonalcoholic steatohepatitis (NASH) is the extreme form of non-alcoholic fatty liver disease (NAFLD) and may progress to advanced liver disease and liver cancer.
Aims: This study aimed to assess the difference of serum miRNAs levels between patients with simple steatosis and those with NASH in Taiwanese patients.
Material and Methods: We prospectively recruited 25 NAFLD patients with elevated alanine aminotransferase (ALT) levels (>1.5 upper limit of normal) after at least 3 months of life style modification. Liver biopsy was performed to evaluate the presence of NASH. The serum miRNAs was extracted using the Complete DNA and RNA Purification Kit (Epicentre, Illumina Corp, USA). MiRNA arrays were performed to obtain miRNA profiles using the TaqMan Array Human MicroRNA Panel v3.0 (Applied Biosystems, Foster City, USA). Each array includes Cards A and B, together containing 768 TaqMan MicroRNA Assays enabling a simultaneous quantification of 754 human miRNAs and 3 endogenous controls. The experiments were performed on an Applied Biosystems 7900 Real-time PCR System (Applied Biosystems). The data were collected and processed using SDS 2.3 (Applied Biosystems) and analyzed using RealTime StatMiner software (Integromics, Armilla, Spain).
Results: A total of 10 NASH patients (5 males, age= 38.9 ± 13.6 years) and other 15 simple steatosis patients (6 males, age= 41.3 ± 16.4 years) were enrolled. The body mass index (BMI) were 29.0 ± 5.1 kg/m2 of NASH group, and 31.8 ± 6.8 kg/m2 of simple steatosis group, respectively. There were significantly increases of mi-423-5p, mi-637 and mi-211 with the fold changes of 2.53 (P= 0.005), 2.33 (P= 0.006), and 2.23 (P= 0.007), respectively. Other metabolic and demographic profiles were comparable between groups.

ePO
ST
ER
AB
ST
RA
CT
S
118 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Conclusions: The serum expressions of microRNAs were different between Taiwanese patients with simple steatosis and NASH. Further validation of tissue expression for potential biomarker exploration will be warranted.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
119EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Friday 13 May 2016ePoster Session 5: 8:30 – 9:00
Screen 1: MR-110
HYPOLACTASIA (LCT-13910CC GENOTYPE) IS ASSOCIATED WITH INSULIN RESISTANCE IN BRAZILIAN PATIENTS WITH NONALCOHOLIC STEATOHEPATITIS (NASH)
Daniel F. C. Mazo1, Rejane Mattar1, Jose Tadeu Stefano1, Joyce M. K. Silva-Etto1, Márcio A. Diniz1, Sebastião M. B. Duarte1, Fabíola Rabelo1, Rodrigo V. C. Lima1, Priscila B. Campos1, Flair Jose Carrilho1, Claudia P. Oliveira* 1
1Gastroenterology (LIM-07), University of São Paulo School of Medicine, SAO PAULO, Brazil
Corresponding author’s email: [email protected]
Introduction: Nonalcoholic fatty liver disease (NAFLD) has a close relationship with metabolic syndrome. The association of LCT-13910CT and LCT-13910TT genotypes with metabolic syndrome components is controversial.
Aims: We assessed hypolactasia (LCT-13910CC) and lactase persistence genotypes in Brazilian NAFLD patients compared to healthy controls and analyzed in nonalcoholic steatohepatitis (NASH) patients its association with biochemical tests, metabolic syndrome and severity of liver histology.
Material and Methods: LCT-13910C>T polymorphism was performed by PCR-restriction fragment length polymorphism in 102 biopsy-proven NAFLD patients (steatosis in 9 and NASH in 93) and compared to that of 501 unrelated healthy volunteers. Anthropometric, clinical, biochemical and liver histology data were analyzed.
Results: No difference in LCT-13910 genotypes profile was noted between NAFLD patients and healthy controls (p=0.941) and also between steatosis and NASH. There were no associations between LCT genotypes with diabetes (p=0.651), dyslipidemia (p=0.328), hypertension (p=0.507) or liver histology in NASH patients. In NASH, hypolactasia was an independent risk factor of insulin resistance, even after adjusting for gender and age (OR=5.0 [95%CI=1.35-20; p=0.017]).
Conclusions: LCT-13910 genotypes distribution in NAFLD patients was the same of general population, but hypolactasia was an independent risk factor of insulin resistance in NASH patients. Further studies including alimentary report are needed.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
120 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Screen 2: YI-MR-126
POSSIBILITY OF GHRELIN AS NON-INVASIVE MARKER FOR NAFLD/NASH DIAGNOSIS
Nazarii Kobyliak* 1, Tetyana Falalyeyeva2, Galyna Mykhalchyshyn1, Petro Bodnar1
1Endocrinology, Bogomolets National Medical University, 2Taras Shevchenko National University of Kyiv, Kyiv, Ukraine
Corresponding author’s email: [email protected]
Introduction: Ghrelin is a hormone produced mainly by the cells lining the fundus of the stomach, which is involved in regulation of lipid and glucose metabolism. Two major forms of ghrelin can be found in circulation: an acylated form, and non-acylated form. Serum acyl-ghrelin (AG) concentration is significantly increased in patients with visceral obesity and insulin resistance.
Aims: This study was conducted to evaluate changes in serum AG levels, its diagnostic accuracy and association with NAFLD in patients with type two diabetes (T2D).
Material and Methods: In this cross-sectional study, 91 T2D patients, age of 40–80 years, were included. All patients were divided into 3 groups. The control group included 28 T2D patients without NAFLD. The main group included 63 T2D patients with NAFLD, which was divided in 2 subgroups depending on transaminase levels: normal (n = 37) and elevated (n = 26) transaminases group. To assess the diagnostic accuracy of AG for NAFLD we used ROC-analysis
Results: We observed 1.5 (p = 0.016) and 2.5 (p < 0.001) fold increasing of serum AG levels in patients with NAFLD and normal or elevated transaminases compared to control groups. In multivariate logistic regression analysis high AG level was an independent, from transaminases activity, triglycerides (OR 1.791; 95%CI 1.162-2.759; p = 0.008) and degree of IR (OR 1.599; 95%CI 1.019-2.508; p = 0.044) predictor that associated with NAFLD. When serum AG used as non-invasive marker for NAFLD detection AUROC was 0.835 (95 % CI 0.752-0.918, p < 0.001). The cut-off value was >0.52 ng/ ml, with sensitivity, specificity, PPV and NPV – 60.3 %, 92.8 %, 95.0 %, 50.9 % respectively. For distinguishing patients with NAFLD and elevated transaminases from patients with NAFLD and normal values AG was less effective. The cut-off value was >0.84 ng/ml. Sensitivity, specificity, PPV and NPV were 50.0 %, 91.8 %, 81.2 %, 72.3 % respectively.

ePO
ST
ER
AB
ST
RA
CT
S
121EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Conclusions: Our study has demonstrated that elevated AG level were associated with NAFLD. Patients with elevated transaminases had significantly higher AG levels. An increase of AG over 0.52 ng/ml can be used as a diagnostic marker for NAFLD detection in patients with T2D.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
122 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Screen 3: YI-MR-129
SECRETOME PROFILES OF HUMAN MESENCHYMAL STEM CELLS BEFORE AND AFTER HEPATOCYTIC DIFFERENTIATION – IDENTIFICATION OF PATHWAYS IMPACTING ON POTENTIAL TREATMENT OF NASH
Sandra Winkler* 1, Madlen Hempel1, Sandra Brückner2, Bruno Christ1
1Applied Molecular Hepatology Lab, Department of Visceral, Transplantation, Thoracic and Vascular Surgery, 2’Applied Molecular Hepatology Lab, Department of Visceral, Transplantation, Thoracic and Vascular Surgery, UNIVERSITY OF LEIPZIG, Leipzig, Germany
Corresponding author’s email: [email protected]
Introduction: Cell therapy is a very promising option to treat acute and chronic liver diseases like e.g. after liver resection or NASH. Because of their known pleiotropic mode of action, mesenchymal stem cells (MSC) seem to be appropriate candidates. Yet, so far, the underlying molecular mechanisms are poorly understood.
Aims: This work aimed to identify and highlight potential factors, mechanisms of action and differences between undifferentiated and hepatocytic differentiated MSC derived from human adipose tissue and bone marrow
Material and Methods: Human MSC were isolated from subcutaneous adipose tissue and bone marrow. Both were differentiated into hepatocyte-like cells for 16 days. The Proteome Profiler Antibody Array (R&D Systems) was applied to identify cytokine profiles of native and hepatocytic differentiated MSC. The data analyses were done using String, David and Pathcards databases.
Results: As markers of hepatocytic differentiation, cell surface antigens CD54 increased and CD166 decreased. Cytokine profiles differed between between MSC from the different tissue sources and changed after differentiation. Using David, cytokine-cytokine receptor interactions, chemokine signaling pathways, the complement and coagulation cascades as well as the JAK-STAT and NOD-like receptor signaling pathways were identified as relevant networks and associated pathways in KEGG. A new online tool, Pathcards, allowed identifying even more relationships like the involvement of the TGF-beta pathway. Also HIF1-alpha signaling pathway might be important.
ePO
ST
ER
AB
ST
RA
CT
S
123EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Conclusions: In summary, MSC from various tissues secrete a basic protein profile, which differs depending on the cell source and the degree of differentiation. Factors involved mainly address inflammatory and growth factor pathways as well as chemo-attraction and innate immunity. Since these are relevant in the pathogenesis of most liver diseases, the elucidation of the molecular mode of actions of MSC might facilitate their clinical translation.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
124 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Screen 4: YI-MR-181
MELANIN PRODUCED BY YEAST NADSONIELLA NIGRA AS NOVEL THERAPEUTICS AGENTS IN NAFLD/NASH MANAGEMENT
Savytska Maryana* 1, Nazarii Kobyliak2, Tetyana Falalyeyeva3, Petro Bodnar2, Tetyana Beregova3, Lyudmyla Ostapchenko3
1Danylo Halytsky Lviv National Medical University, Lviv, 2Endocrinology, Bogomolets National Medical University, 3Taras Shevchenko National University of Kyiv, Kyiv, Ukraine
Corresponding author’s email: [email protected]
Introduction: One of the pathogenic mechanisms of the progression NAFLD to NASH is the accumulation of reactive oxygen species. So, antioxidant therapy is necessary for successful treatment of the liver injury. We have paid attention to melanin produced by yeast Nadsoniella nigra strain X-1 as novel antioxidant and anti-inflammatory agents with low toxicity.
Aims: In current study we aimed to investigate the preventive effect of melanin on the monosodium glutamate (MSG) induced NAFLD model in rats.
Material and Methods: The study was carried out on 45 Wistar rats, that were divided into 3 groups: intact, MSG- and MSG+melanin groups (n=15 in each group). Newborn rats of MSG- and MSG+melanin groups were administered with MSG (4 mg/g, 8 μl/g, subcutaneously) at 2nd -10th days of life. Since the age of 1 month, rats of MSG-group were treated with water (0.25 ml/100 g), rats of MSG+melanin groups with melanin (1 mg/kg) dissolved in water (0.25 ml/100 g). Introduction had been performed intermittently (two-week courses alternated with two-week breaks) for 3 months. In 4-month rats anthropometrical parameters and VAT mass were estimated. To assess morphological changes in liver we used NAS (NAFLD activity score). Lipid extraction from liver was performed according to Folch. The content of proinflammatory cytokines (IL-1β, IL-12Bp40, INF-γ) and anti-inflammatory cytokines (IL-4, IL-10, TGF-β) were measured by ELISA.
Results: We found significantly lower total score (1.0±0.19 vs 3.33±0.36, p<0.001), degree of steatosis (0.73±0.18 vs 1.80±0.17, p<0.001) and manifestation of lobular inflammation (0.27±0.11 vs 1.20±0.17, p<0.001) due to NAFLD activity score in MSG+melanin group compared to MSG-obesity. NASH we confirmed only in 33.3 % of rats with MSG-

ePO
ST
ER
AB
ST
RA
CT
S
125EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
obesity that was significantly higher than after melanin (6.7 %) administration (p=0.033). Melanin administration reduce total lipids and triglycerids content in liver approximately by 22-25% (p<0.001) and amount of visceral fat on 40% (p<0.001) as compared to MSG-obesity group. Melanin reduced the content of IL-1β in rat serum and restored the level of anti-inflammatory cytokines (IL-10, TGF-β) to the control values.
Conclusions: Thus, the administration of melanin can prevent development of NAFLD/NASH in rats with MSG-induced obesity and can be considered as possible novel therapeutic agents but further studies to confirm its action needed.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
126 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Screen 5: MR-195
THE BERLIN QUESTIONNAIRE SCREENS AND EPWORTH SLEEPINESS SCALE FOR OBSTRUCTIVE SLEEP APNEA IN NON-ALCOHOLIC FATTY LIVER DISEASE
Haifa Romdhane1, Bochra Bouchabou* 1, Hend Ayadi1, Myriem Cheikh1, Najet Belhadj1
1Department of gastroenterology, Mongi Slim Universitary Hospital, Tunis, Tunisia
Corresponding author’s email: [email protected]
Introduction: Obstructive sleep apnea (OSA) is associated with non-alcoholic fatty liver disease (NAFLD), a disorder most commonly occurring in patients with obesity and/or metabolic syndrome. Because polysomnography, the standard test for diagnosing OSA, is expensive and time consuming, questionnaires have been developed to identify persons with OSA. The Berlin questionnaire (BQ) reliably and Epworth Sleepiness Scale (ESS) identify middle-aged and older persons in the community who are at high-risk for OSA.
Aims: We aimed to validate the BQ and ESS as a screening tool for OSA in NAFLD patients.
Material and Methods: Patients with ultrasound-diagnosed NAFLD completed the BQ and ESS. Then, we underwent diagnostic polysomnography. The BQ and ESS were scored as high or low risk for OSA, and the diagnosis of OSA was based on polysomnography findings. OSA was defined as an apnea-hypopnea index of ≥ 5 on polysomnography.
Results: Thirty eight patients were evaluated. There were 11 men and 27 women with a mean age of 50 years old [19-79]. Body mass index was on average of 32, 4 kg/m2 [21,4-43]. Twenty three patients (60.5%) had a high-risk BQ score and six patients (15, 7%) had a high-risk ESS. Fifteen of 23 (65, 2%) with a high-risk BQ score had OSA, while 3 of 15 (20%) with a low-risk score had OSA (Fisher test, P = 0.025). Five of 6 (83, 33%) patients with high-risk ESS had OSA, while 4 of 32 (12,5%) with a low-risk score had OSA (Fisher test, P = 0,04). The sensitivity and specificity of the BQ for OSA in NAFLD patients were 82% and 57%, respectively while the sensitivity and specificity of the ESS for OSA were 74% and 43%.
Conclusions: A low-risk BQ score and ESS identify NAFLD patients who are unlikely to have OSA. Polysomnography should be considered in those with a high-risk score.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
127EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 6: YI-MR-149
AN OPEN LABEL RANDOMIZED CONTROLLED TRIAL OF VITAMIN D VS PENTOXIFYLLINE IN NON-DIABETIC PATIENTS OF NAFLD
Sanchit Budhiraja* 1, Ashok K. Jain1, Vinod K. Dixit1, Sunit K. Shukla1, Ravika Budhiraja2, Ashutosh Jain3
1Gastroenterology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, 2Dermatology, SGRDIMSR, Amritsar, 3Internal Medicine, Institute of Medical Sciences, Banaras Hindu University, Varanasi, India
Corresponding author’s email: [email protected]
Introduction: Nonalcoholic fatty liver disease (NAFLD) encompasses a histological spectrum ranging from simple steatosis to nonalcoholic steatohepatitis (NASH). Diet and lifestyle changes are a rational first-line therapy in NAFLD. Pharmacologic therapy is important when lifestyle measures fail.
Aims: The aim of this study was to compare the response to two different treatments i.e. Vitamin E and Pentoxifylline (PTX) in non-diabetic patients of NAFLD in terms of clinical and biochemical outcomes.
Material and Methods: In this open label study, in addition to lifestyle modification advice, non-diabetic patients with biopsy proven NAFLD were randomized to receive either Vitamin E (800 mg in 2 divided doses) or PTX (1200 mg in 3 divided doses).
Results: A total of 48 patients (26 in Vitamin E group and 22 in the PTX group) with a mean follow up of 166.8 days completed the study. At follow up, FBS was less in Vitamin E group (94.69±6.72 mg/dl vs 100.45±9.82 mg/dl; p 0.020). The level of VLDL was lower (p 0.015) in the PTX group (33.15±7.51mg/dl). There was no difference in any other parameter between the two groups.In the Vitamin E group, there was a decrease in systolic blood pressure (SBP) and diastolic blood pressure (p <0.0001), weight (67.96±8.2 kg vs 67.00±7.28 kg; p 0.003), BMI (from 24.14±2.93 kg/m2 to 23.75±2.66 kg/m2; p 0.008), waist and hip circumference. There was a decrease in ALT to 55.38±29.90 at follow up from 67.54±34.50 U/L at baseline (p 0.016). Median triglyceride level decreased from 251.5 mg/dl to 194.5 mg/dl (p 0.002) and HDL increased from 38.08 at baseline to 41.15 at follow up (p 0.0001). FBS decreased

ePO
ST
ER
AB
ST
RA
CT
S
128 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
from 97.88mg/dl at baseline to 94.69 mg/dl at follow up (p 0.018). There was a decrease in the CK18-F level from 348.95 U/L to 319.79 U/L (p 0.0001). In the PTX group, there was a decrease in weight (70.77±7.32 kg to 70.00±6.91 kg; p 0.009) and waist circumference (92.14±11.88 cm to 91.27±11.91cm; p 0.007). ALT decreased from 83.55±38.96 U/L to 64.51±26.54 U/L (p 0.008) and HDL increased from 37.64 mg/dl to 40.5 mg/dl (p 0.0001). There was also a decrease in CK18-F from 344.01 U/L to 303.78 U/L (p 0.022).
Conclusions: Vitamin E therapy was effective in reducing weight, BMI, systolic blood pressure and ALT, improving dyslipidemia as well as blood sugars and CK18-F. PTX therapy improved weight, ALT, HDL and CK18-F. Overall, even though both the treatments decreased ALT and CK18-F, Vitamin E appears to offer distinct advantage over PTX in terms of improvement in dyslipidemia and blood sugars.
Figure:
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
129EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Friday 13 May 2016ePoster Session 6: 10:30 – 11:00
Screen 1: MR-115
MOLECULAR CHARACTERIZATION OF THE FECAL MICROBIOME IN BRAZILIAN NASH OBESE AND OBESE WITHOUT NASH PATIENTS COMPARED TO LEAN HEALTHY CONTROLS
Claudia P. Oliveira* 1, Sebastião M. Duarte 1, Jose Tadeu Stefano1, Marcela Souza2, Livia Rodrigues1, Priscila B. Campos1, Fernando G. Costa1, Daniel F. Mazo1, Flair Jose Carrilho1, Ester C. Sabino2
1GASTROENTEROLOGY (LIM-07), 2Infectious Disease and Institute of Tropical Medicine, University of São Paulo School of Medicine, SAO PAULO, Brazil
Corresponding author’s email: [email protected]
Introduction: Evidence for the role of the gut microbiota in energy storage and the development of NAFLD (Non-alcoholic fatty liver disease) has provided new insight to the pathophysiology of this disease and may help explain the observed phenotypic differences.Aims: The aim of the study was to compare the gut microbiome from Brazilian obese patients with or without NASH versus Brazilian healthy controls.
Material and Methods: We performed a cross sectional study comprising patients biopsied-proven NASH obese (NO; n=11]; obese without NASH (OWN; n=4) and lean healthy controls (HC; n=6). Stool samples were prospectively collected, mixed with RNAlater and stored at -20°C. DNA was extracted from stool samples and PCR amplification was performed using primers for the V4 region of the 16S rRNA gene. The amplicons were sequenced using Ion PGM Torrent platform and data analyzed using QIIME software.
Results: NO or OWN patients had higher percentages of Firmicutes compared to HC (p<0.04) according Phylum. Furthermore, according Class obese in both groups with (NO) or without NASH (OWN) had a tendency a greater percentage of Clostridia than HC (p=0.062). As regards the Family obese patients with or without NASH had higher percentages of Enterobacteriaceae than HC (p<0.037). Curiously, NO patients had some interesting microbioma aspects that are different from obese OWN and HC. There was a

ePO
ST
ER
AB
ST
RA
CT
S
130 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
tendency to have higher percentage of Tenericutes compared to OWN and HC (p=0.063) according Phylum. Analyzing the Class, NO patients had higher percentages of Mollicutes that OWN and HC (p<0.039) and in the other hand, there is a tendency that NO patients have a greater percentage of some types of bacteria Rikenellaceae families, Odoribacteraceae and Mogibacteriaceae that OWN and HC. Finally, according Genero, NO patients had higher percentages of Anaerostipes compared to OWN and HC (p<0.046).These aspects suggest that NASH obese patients could have different microbioma than obese without NASH and healthy controls.
Conclusions: Our data suggest that Brazilian NASH obese and obese without NASH patients have fecal dysbiosis compared with Brazilian lean healthy controls. In the other hand, NASH obese patients in Brazil also have a different microbioma than obese without NASH and healthy controls. Further studies are required to investigate the mechanism underlying the interaction between gut microbes and NASH in obese and lean subjects across the world.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
131EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 2: YI-MR-171
SYNERGISTIC EFFECT OF ALIVE PROBIOTIC AND ABSORBENT SMECTITE GEL FOR NAFLD/NASH PREVENTION: EXPERIMENTAL STUDY
Nazarii Kobyliak* 1, Tetyana Falalyeyeva2, Galyna Mykhalchyshyn1, Tetyana Beregova2, Petro Bodnar1
1Endocrinology, Bogomolets National Medical University, 2Taras Shevchenko National University of Kyiv, Kyiv, Ukraine
Corresponding author’s email: [email protected]
Introduction: Today probiotics have been suggested as a treatment for the prevention of NAFLD. Smectite is a natural silicate that binds to digestive mucous and has the ability to bind endo- and exotoxins, increased water and electrolyte absorption and restored the barrier properties of human intestinal cell monolayers.
Aims: The present study was designed to determine whether probiotics plus smectite is superior to probiotic alone on the monosodium glutamate (MSG) induced NAFLD model in rats.
Material and Methods: We included 60 rats divided into 4 groups 15 animals in each. Rats of group I were intact. Newborns rats of groups II-IV were injected with MSG (4.0 mg/g body weight) subcutaneously at postnatal days 2, 4, 6, 8 and 10. The III (Symbiter) group received 2.5 ml/kg of multiprobiotic “Symbiter” containing concentrated biomass of 14 probiotic bacteria genera Bifidobacterium, Lactobacillus, Lactococcus, Propionibacterium. The III (Symbiter+Smectite) groups received “Symbiter Forte” combination of probiotic biomass with smectite gel (250 mg). Administration was started at 4 weeks after birth and continued intermittently two-week course in 2 weeks intervals. To assess morphological changes in liver we used NAS (NAFLD activity score). Lipid extraction from liver was performed according to Folch. The content of proinflammatory cytokines (IL)-1β, IL-12Bp40, INF-γ) and anti-inflammatory cytokines (IL-4, IL-10, TGF-β) were measured by ELISA.
Results: In both interventional groups reduction of total NAS score as compared to MSG-obesity was observed. However only for Symbiter+Smectite group we don’t find significant changes as compared to intact rats (1.0±0.21 vs 0.20±0.13, p=0.223). Indeed similar values of steatosis score (0.93±0.22 vs 0.87±0.16) in both treatment groups,

ePO
ST
ER
AB
ST
RA
CT
S
132 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
we observed that lower total score for Symbiter+Smectite are associated with more pronounced reduction of lobular inflammation (0.13±0.09 vs 0.33±0.15) as compared to administration of probiotic alone. This data accompanied with significant reduction of IL-1β and restoration of IL-10 between these 2 groups.
Conclusions: Additional to alive probiotic administration of smectite gel due to his absorbent activity and stabilization mucus layer properties can impact on synergistic enhancement of single effect which manifested with reduction of lobular inflammation and at list partly NASH prevention.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
133EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 3: YI-MR-184
LIVER AND SYSTEMIC IRON LOADING CHARACTERISE INITIAL DISEASE PROGRESSION IN NAFLD
John D. Ryan* 1, Andrew Armitage2, Jeremy F. Cobbold1, Rajarshi Banerjee3, Stefan Neubauer3, Lai Mun Wang1, Sant-Rayn Pasricha2, Jane Collier1, Alexander Drakesmith2, Eleanor Barnes1, Michael Pavlides3
1Translational Gastroenterology Unit, 2MRC Human Immunology Unit, Weatherall Institute of Molecular Medicine, 3Oxford Centre for Clinical Magnetic Resonance Research, University of Oxford, Oxford, United Kingdom
Corresponding author’s email: [email protected]
Introduction: Non-alcoholic fatty liver disease (NAFLD) often presents with raised serum ferritin levels. Both raised ferritin and hepatic iron levels have been associated with more advanced NAFLD, although ferritin levels may relate to inflammation rather than iron. Excess iron causes oxidative stress, and may worsen insulin resistance (IR) through the modulation of adipokines such as adiponectin.
Aims: As both oxidative stress and IR are key features of the pathogenesis and progression of NAFLD, deciphering the role of iron in this process is important.
Material and Methods: In this study we examined the iron status of individuals across the clinical spectrum of NAFLD (n=51), using blood, tissue and magnetic resonance (MR) imaging markers. We compared them with chronic viral hepatitis patients (n=30) and healthy controls (n=20).
Results: NAFLD patients were significantly heavier, with significantly higher liver fat and iron measured by MR (proton spectroscopy and T2* respectively), higher insulin and CRP, and lower total adiponectin than viral hepatitis or controls (all p<0.005). Examining NAFLD subgroups by Brunt fibrosis stage revealed a progressive increase in liver fat and iron from early (F0-1, n=17) to moderate fibrosis (F2, n=16) which declined in advanced disease (F3-4, n=18), (p=0.002 for iron). This was mirrored by elevated serum ferritin and hepcidin during the progression from F0-1 to F2, followed by a significant decline in advanced fibrosis (p=0.002 and p=0.0004, respectively). Furthermore, serum ferritin or hepcidin were significant independent predictors of progression from F0-1 to F2 stage by multiple logistic regression. Serum ferritin correlated closely with serum hepcidin, MR liver fat and iron in NAFLD (r=0.73, r=0.56 and r=-0.76 respectively, all p<0.0001)

ePO
ST
ER
AB
ST
RA
CT
S
134 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
but not with CRP or inflammation on biopsy. Total adiponectin correlated inversely with serum ferritin, hepcidin and liver iron levels (r=-0.27, p=0.05; r=-0.28, p=0.049 and r=0.38, p=0.005, respectively), and declined significantly from F0-1 to F2 (p=0.02).
Conclusions: Raised serum ferritin in NAFLD patients reflects increased hepcidin and liver iron, which is associated with insulin resistance markers. Moreover, an increase in iron appears to mark the progression through early fibrosis stages, supporting a causal relationship with the metabolic changes that drive the pathogenesis and progression of the disease, warranting further interventional studies to exploit this important therapeutic target.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
135EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 4: YI-MR-174
DIAGNOSTIC ACCURACY OF SHEAR WAVE ELASTOGRAPHY FOR THE ASSESSMENT OF LIVER STIFFNESS IN CHILDREN WITH FATTY LIVER DISEASE
Matteo Garcovich* 1, Silvio Veraldi2, Enrico Di Stasio3, Maria A. Zocco1, Lidia Monti4, Paolo Tomà4, Maurizio Pompili1, Antonio Gasbarrini1, Valerio Nobili2
1Internal Medicine, Gastroenterology and Liver Diseases Unit, CATHOLIC UNIVERSITY OF SACRED HEARTH, 2Hepatometabolic Unit, Bambino Gesù Children’s Hospital, 3Institute of Biochemistry and Clinical Biochemistry, CATHOLIC UNIVERSITY OF SACRED HEARTH, 4Radiology Unit, Bambino Gesù Children’s Hospital, Rome, Italy
Corresponding author’s email: [email protected]
Introduction: Non-invasive assessment of liver fibrosis by ultrasound elastography techniques has received increasing attention as a means to evaluate disease progression in chronic liver disease patients.
Aims: In this study, we assessed the value of shear wave elastography with Supersonic Shear Imaging (SSI) for the prediction of fibrosis stage in a cohort of pediatric patients with nonalcoholic steatohepatitis.
Material and Methods: Consecutive patients scheduled for liver biopsy were studied by using SSI ultrasound system, a non-invasive method of assessing tissue stiffness. The correlations between laboratory findings, liver stiffness and the fibrosis score were analyzed using logistic regression and receiver operating characteristic curve analyses were performed to calculate area under the receiver operating characteristics curves for the presence of “any” (F≥1) or significant (F≥2) fibrosis.
Results: SSI was performed in 69 consecutive biopsy-proven nonalcoholic steatohepatitis patients (38 males, 31 females, age 12.7±2.65 years). In univariate analysis, SSI showed a very high correlation with liver fibrosis (P< 10-5), a high correlation for degree of portal inflammation (P=0.001), lobular inflammation (P=0.001) and a moderate correlation for degree of histologic steatosis (P=0.032) and histological hepatocyte ballooning (P=0.025). SSI values showed a moderate correlation with ALT and AST, but no correlation was found with other variables. Multivariate analysis confirmed the strong correlation of SSI with fibrosis stage (P< 10-5). Overall, SSI correctly classified 57 of 69 patients (83%). In particular, the ROC curve drawn to differentiate “any” fibrosis (F≥1) from absence

ePO
ST
ER
AB
ST
RA
CT
S
136 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
of fibrosis (F0) yielded an AUROC of 0.92 (95% CI:0.86-0.98), with an optimal cut-off of 5.1 kPa (sensitivity 84%; specificity 95%). The AUROC values for differentiating significant fibrosis (F ≥2) from fibrosis degree of less than F2 was 0.97 (95% CI:0.95-0.99), with an optimal cut-off value of 6.7 kPa.
Conclusions: To date this is the largest case series evaluating the accuracy of SSI in children with fatty liver disease. SSI is an accurate and reproducible non invasive technique detecting efficiently the presence of any degree of fibrosis or significant fibrosis in this population. Larger clinical prospective studies are warranted to confirm SSI accuracy and establish threshold values for fibrosis grading in comparison or in combination with other non-invasive methodologies.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
137EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 5: YI-MR-150
ADIPOSE TISSUE INSULIN RESISTANCE IS ASSOCIATED WITH MACROPHAGE ACTIVATION IN NON-DIABETIC PATIENTS WITH NON ALCOHOLIC FATTY LIVER DISEASE
Milena Marietti* 1, Chiara Rosso1, Konstantin Kazankov2, Melania Gaggini3, Holger Jon Moller4, Chiara Saponaro3, Gian Paolo Caviglia1, Emma Buzzigoli3, Rami I. K. Jouness1, Maria Lorena Abate1, Antonina Smedile1, Giorgio Maria Saracco5, Hendrik Vilstrup2, Jacob George6, Amalia Gastaldelli3, Henning Gronbaek2, Elisabetta Bugianesi1
1Medical Sciences, UNIVERSITY OF TURIN, Torino, Italy, 2Department of Hepatology and Gastroenterology, Aarhus University Hospital, Aarhus, Denmark, 3Cardiometabolic Risk Unit, CNR-Institute of Clinical Physiology, Pisa, Italy, 4Department of Clinical Biochemistry, Aarhus University Hospital, Aarhus, Denmark, 5Department of Oncology, UNIVERSITY OF TURIN, Torino, Italy, 6The Storr Liver Centre, University of Sydney and Westmead Hospital, Westmead, Australia
Corresponding author’s email: [email protected]
Introduction: Non-alcoholic fatty liver disease (NAFLD) has a bidirectional relationship with insulin resistance (IR): the liver is the target of an increased flux of Free Fatty Acids (FFAs) and adipokines stemming from a dysfunctional adipose tissue (AT) but a fatty liver actively contributes to the dyslipidemic profile and to the chronic low grade inflammation. Soluble CD163 (sCD163), a marker of hepatic macrophages activation, has been associated with fibrosis in NAFLD.
Aims: Our aim is to elucidate the link between IR in the liver and in the AT, hepatic macrophages activation and liver damage in 40 non-diabetic patients with NAFLD.
Material and Methods: All study subjects underwent tracers studies with [2H5]glycerol and [2H2]glucose in fasting conditions. AT-IR was calculated as FFAs x insulin (AT-IR1) and as Glycerol Ra x insulin (AT-IR2). Hepatic-IR was derived from endogenous glucose production x insulin. sCD163 levels were measured by an enzyme-linked immunosorbent assay. Hepatic fat was assessed by liver biopsy while visceral fat (VF) and subcutaneous fat (SF) were measured with standard magnetic resonance imaging (MRI). Histology was scored according to Kleiner.

ePO
ST
ER
AB
ST
RA
CT
S
138 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Results: AT-IR showed a significant association with hepatic fat (AT-IR1: r=0.50, p=0.001; AT-IR2: r=0.44, p=0.004), with NAS score (p=0.006 and 0.05 respectively) and with fibrosis (p=0.001 for both) at liver biopsy. Plasma levels of sCD163 were significantly associated with fasting plasma levels of FFAs and with lipolysis (r=0.35, p=0.026; r =0.35, p=0.028, respectively). sCD163 levels were also directly related to AT-IR (AT-IR1 r=0.38, p=0.016 and AT-IR2 r=0.31, p=0.005) and with liver fat (r=0.53; p=0.005), while no correlation was found with Hepatic-IR (r=0.22, p=0.170), VF (r=0.15, p=0.407) or SF (r=0.08, p=0.655). Among histological features, sCD163 plasma levels increased in proportion to the NAS score (r=0.54; p=0.003) and to the degree of fibrosis (p<0.001). At logistic regression analysis, sCD163 plasma levels better predicted moderate/severe (≥F2) fibrosis than AT-IR (OR 5.2, CI:1.1-24.6).
Conclusions: We hypothesize that in NAFLD AT-IR can stimulate hepatic macrophage activation via an increased flux of FFAs thus concurring to liver damage.
Funded by FP7/2007-2013under grant agreement no.HEALTH-F2-2009-241762 for the project FLIP;PRIN2009ARYX4T. Horizon2020 under grant agreement no.634413 for the project EPoS
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
139EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 6: MR-152
PATATIN-LIKE PHOSPHOLIPASE DOMAIN-CONTAINING PROTEIN 3 POLYMORPHISM AND THE RISK OF HEPATOCELLULAR CARCINOMA DEVELOPMENT IN RELATION TO UNDERLYING LIVER DISEASES
Pisit Tangkijvanich* 1, Maneerat Raksayot1 on behalf of Research Unit of Viral Hepatitis and Liver Cancer, Apichaya Khlaiphuengsin1 and Research Unit of Hepatitis and Liver Cancer1Biochemistry, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
Corresponding author’s email: [email protected]
Introduction: A single nucleotide polymorphism (SNP) of patatin-like phospholipase domain containing protein 3 (PNPLA3) (rs738409, C>G) has been associated with disease progression in fatty liver diseases. However, the role of the SNP in patients with hepatocellular carcinoma (HCC) in relation to underlying chronic liver diseases is less clear.
Aims: This study was aimed at evaluating the association between rs738409 and the development of HCC in Thai patients.
Material and Methods: PNPLA3 rs738409 genotypes was determined by allelic discrimination in blood samples of 200 heathy controls and 574 HCC cases [303 with viral hepatitis B, 154 with viral hepatitis C, 46 with alcoholic steatohepatitis (ASH) and 71 with non-alcoholic steatohepatitis (NASH)].
Results: The prevalence of rs738409 genotypes CC, CG and GG in controls was 91 (45.5%), 88 (44.0%), and 21 (10.5%), respectively, while the corresponding figures in all patients with HCC was 243 (42.34%), 259 (45.12%), and 72 (12.54%). The GG genotype had significantly higher distribution in patients with ASH/NASH-related HCC compared with controls (OR=2.09, 95% CI=1.10- 3.96, P=0.025), and viral-related HCC (OR=2.04, 95% CI=1.18- 3.51, P= 0.010). However, the frequency of the GG genotype was similar between controls and patients with viral-related HCC.
Conclusions: These data suggested an association of the PNPLA3 polymorphism with HCC development in patients with ASH/NASH but not among those with chronic viral hepatitis.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
140 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Friday 13 May 2016ePoster Session 7: 13:30 – 14:00
Screen 1: MR-172
COMPARATIVE ANALYSIS OF ONLINE PATIENT EDUCATION RESOURCES PERTAINING TO NASH OR NAFLD
Rishabh Gulati* 1, Mohammad Nawaz2, Nikolaos Pyrsopoulos1
1Rutgers NJMS, Newark, 2Rutgers NJMS, Bloomfield, United States
Corresponding author’s email: [email protected]
Introduction: Role of the Internet is ever increasing in the present era as the first source of medical information. Imprecise, partial comprehension of textual information limits its efficacy in communicating the disease process to the patient. Here, we report a comparative analysis of readability of patient-centered text pertaining to Non-Alcoholic Fatty Liver Disease (NAFLD) and/or Non-alcoholic Steatohepatitis (NASH) available online.
Aims: To determine the readability of online patient centered health information pertaining to NASH or NAFLD
Material and Methods: From September to November 2015, patient-centered information from websites of American College of Gastroenterology (ACG), Mayo Clinic, Medicinenet.com, National Institutes of Health (NIH), Patient.info, Uptodate & WebMD were downloaded & processed in Microsoft Word. All data were formatted & categorized into subsections. Copyright, propriety information & certain medical terms were omitted to limit bias. Text was then analyzed for their specific level of readability using 6 quantitative scales: Flesch–Kincaid level, Gunning fog index, SMOG, Coleman-Liau, FRY & New Dale–Chall.
Results: Modified documents had a mean grade level that was 1 less than their original counterparts. ACG had the highest mean grade level of readability of it’s content (14±0.56), with the lowest being for WebMD (7.1±0.61). When compared with all subsets, the treatment subsection had the highest mean grade level (11.9±0.61). ANOVA analysis showed that there were significant differences in the grade level depending on the source website (p < 0.05), and subsection when compared with all readability tests.

ePO
ST
ER
AB
ST
RA
CT
S
141EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Forest plot analysis depicts significant higher readability grade level of various subsections and websites. The treatment section was usually the most difficult section written when compared with other subsections (p < 0.05).
Conclusions: Patient material is above the recommended 6th grade level across all websites. Treatment section is often the most difficult section to comprehend. Greater emphasis on clear & simple language is warranted to increase quality & comprehension of online patient education resources.
Figure:
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
142 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Screen 2: YI-MR-159
IMPACT OF GWAS-IDENTIFIED COMMON VARIANTS ON HISTOPATHOLOGICAL FEATURES OF NAFLD PATIENTS
Rocío Gallego-Durán* 1, 2, Javier Ampuero2, 3, Jose Antonio Del Campo2, 4, Helena Pastor-Ramírez2, 3, Eduardo Vilar-Gómez2, 3, Antonio Gil-Gómez2, 3, María Teresa Arias-Loste5, 6, María Jesús Pareja-Megía7, Javier Abad8, María Carmen Rico2, 3, Marta García-Valdecasas2, 3, Inmaculada Moreno9, 10, Jose Luis Calleja11, Raúl Jesús Andrade9, 10, Javier Crespo5, 12, Carmelo García-Monzón13, 14, Manuel Romero-Gómez2, 3
1 Inter-Centre Unit of Digestive Diseases & CIBERehd, Virgen Macarena – Virgen del Rocío University Hospitals, University of Sevilla, 2Instituto de Biomedicina de Sevilla (IBiS), 3Inter-Centre Unit of Digestive Diseases & CIBERehd, Virgen Macarena – Virgen del Rocío University Hospitals, University of Sevilla, 4Digestive Diseases Unit, Valme University Hospital, Sevilla, 5Gastroenterology and Hepatology Department, Marqués de Valdecilla University Hospital, 6Infection, Immunity and Digestive Pathology Group, Research Institute Marqués de Valdecilla (IDIVAL), Santander, 7Pathology Unit, Valme University Hospital, Sevilla, 8Gastroenterology Department, Hospital Puerta de Hierro, Madrid, 9Inter-Centre Unit of Digestive Diseases & CIBERehd, Virgen de la Victoria University Hospital, 10Instituto de Investigación Biomédica de Málaga (IBIMA), Málaga, 11Gastroenterology and Hepatology Department, Hospital Puerta de Hierro, Madrid, 12Research Institute Marqués de Valdecilla (IDIVAL), Santander, 13Liver Research Unit and CIBERehd , University Hospital Santa Cristina , 14Instituto de Investigación Sanitaria Princesa, Madrid, Spain
Corresponding author’s email: [email protected]
Introduction: Due to considerable interindividual variation in NAFLD development and progression, in recent years several GWAS studies have been performed to determine genetic influence on this disease.
Aims: The main aim of this study was to evaluate the impact of certain single nucleotide polymorphisms (SNPs) on histopathological features in a cohort of Spanish patients.
Material and Methods: Cross-sectional and multicentre study including 225 biopsy-diagnosed NAFLD patients. After literature search, four SNPs from candidate genes were selected from GWAS (rs738409 from PNPLA3, rs58542926 from TM6SF2, rs2645424 from FDFT1 and rs838145 from IZUMO1) with potential clinical relevance on NAFLD. Clinical, epidemiological and analytical data were recorded. These SNPs were genotyped

ePO
ST
ER
AB
ST
RA
CT
S
143EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
by allelic discrimination using Taqman probe (Applied Byosistems, Spain). Histological assessment was performed using Kleiner score, calculating lobular inflammation, ballooning and steatosis degree. Statistical analysis was performed using SPSS 22.0 software.
Results: It was performed univariate analyses by NASH and significant fibrosis (F2-F4) presence. Independent variables with significance p ≤ 0.05 were introduced in the multivariate analysis (backward Wald logistic regression analysis), in order to avoid potential confounding factors, to identify features related to NASH and significant liver fibrosis. Independent predictor variables for NASH were male gender [OR 3.02 (CI95% 1.02-6.79); p=0.006]; diabetes mellitus [OR 5.70 (CI95% 2.14-15.21); p=0.001] and bear GG genotype from IZUMO1 gene [OR 2.62 (CI95% 1.02-6.76; p=0.046] and GG genotype from PNPLA3 gene [OR 4.16 (CI95% 1.68-10.28); p=0.002]. Area under receiver operating curve (AUROC) obtained for NASH prediction was 0.79 [CI95% 0.71-0.86].Likewise, age at liver biopsy [OR 1.07 (CI95% 1.03-1.11); p=0.001], ALT [OR 1.02 (CI95% 1.01-1.03); p=0.006], insulin levels [OR 1.10 (CI95% 1.04-1.17); p=0.001] and being carrier of GG genotype from IZUMO1 gene [OR 3.10 (CI95% 1.07-8.94); p=0.037] were found independently associated to significant fibrosis development. AUROC achieved for significant fibrosis prediction was 0.88 [CI95% 0.83-0.94].
Conclusions: Influence of both genetic variants, located on IZUMO1 and PNPLA3 genes, were closely related to NAFLD severity, and could be useful as an effective tool for screening and detection of patients suffering from advanced disease stages.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
144 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Screen 3: MR-182
NASH: AN UNDERECOGNIZED CAUSE OF CRYPTOGENIC CIRRHOSIS
Rym Ennaifer* 1, Hend Ayadi1, Myriam Cheikh1, Hayfa Romdhane1, Najet BelHadj1
1Mongi Slim Universitary Hospital, Tunis, Tunisia
Corresponding author’s email: [email protected]
Introduction: Nonalcoholic steatohepatitis (NASH) is a major cause of chronic liver disease and its prevalence is rapidly increasing worldwide. At end-stage, steatosis and liver-cell injury can disappear and the cirrhosis can be wrongly classified as cryptogenic.According to the European guidelines, the diagnosis of NASH at stage of cirrhosis can be made when an overweight or diabetes are present together with hypertension, dyslipidemia, or atheromatosis without histological proof.
Aims: The aim of our study was to evaluate the prevalence of risk factor of metabolic syndrome over a cohort of patients followed for cryptogenic cirrhosis and to determine how much can be attributed to burned-out NASH according to the criteria established by the European guidelines.
Material and Methods: Retrospective study including patients followed in our department for cryptogenic cirrhosis between January 2011 and December 2015.
Results: Among 142 cirrhotic patients, 21 patients were considered as having cryptogenic cirrhosis. They were 11 men and 10 women with a mean age of 61.5 years [49-77]. Alcoholic, viral, autoimmune, vascular and other metabolic causes of chronic liver diseases were excluded. 61.9% of patients (n=13) were overweighted with a mean BMI equal to 28.8 kg/m2 [20-39]. A type 2 diabetes mellitus was diagnosed in 57 % of cases (n=12) and a dyslipidemia in 23.8% of cases (n=5). 28.5% of patients had hypertension. One patient had a history of ischemic stroke. A metabolic syndrome was present in 33.3% of cases (n=7).Abdominal ultrasound revealed hepatic increased echogenicity in 2 cases. According to the European guidelines, the diagnosis of NASH was attributed to 52.3% of patients (n=11): 7 patients had 2 criteria, 2 had 3 criteria and 2 had 4 criteria.
Conclusions: In this Tunisian cohort, 52.5% of cryptogenic cirrhosis could be related to burned out NASH. End-stage NASH should be mentioned as a frequent cause of cryptogenic cirrhosis not only in Western countries.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
145EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 4: YI-MR-136
HIGH RISK POPULATIONS: ATTITUDES TO NAFLD AMONG DIABETOLOGISTS
Thomas Marjot* 1, Emilia Sbardella2, Jonathan Hazlehurst3, Ahmad Moolla3, Jeremy Cobbold4, Jeremy Tomlinson3
1Oxford Centre for Diabetes, Endocrinology and Metabolism, 2Oxford Centre for Diabetes, Endocrinology and Metabolism, Churchill Hospital, 3Oxford Centre for Diabetes, Endocrinology and Metabolism, University of Oxford, 4Department of Gastroenterology and Hepatology, Oxford University Hospitals NHS Foundation Trust, Oxford, United Kingdom
Corresponding author’s email: [email protected]
Introduction: Non-alcoholic fatty liver disease (NAFLD) and type 2 diabetes (T2DM) are common conditions that regularly coexist and can act synergistically to drive adverse outcomes. The prevalence of NAFLD in T2DM is 70%, with 16% having evidence of advanced hepatic fibrosis. There is accumulating evidence for a role of screening for NAFLD +/- fibrosis in diabetic populations.
Aims: Our study therefore had 3 aims: Firstly, to define the attitudes and current clinical practice of diabetes specialists towards NAFLD across the UK. Secondly, to implement an evidenced-based pathway for the assessment of NAFLD in patients attending diabetes outpatient clinics and finally, to assess the impact of a multidisciplinary approach (with combined hepatology and diabetes input) to their clinical management.
Material and Methods: An online survey was disseminated to diabetologists across the UK. Based on findings from this survey, all diabetic patients attending outpatient clinics at Oxford University Hospitals were screened for advanced fibrosis using a Fib-4 score. Those with elevated scores may then benefit from referral to the multidisciplinary metabolic hepatology clinic.
Results: 116 diabetes specialists responded to the survey. Only 4.5% of responders correctly judged the prevalence of NAFLD in diabetic patients to be >50%. Even fewer (1.5%) correctly judged the prevalence of advanced fibrotic disease to be >15%. Whilst most diabetologists performed liver function tests, the vast majority (68%) had not used any non-invasive scoring system to assess risk of advanced disease within the last 12 months. For 20% of responders, a diagnosis of NAFLD did not affect their approach to management. In light of these findings, a local ‘think NAFLD’ campaign was launched

ePO
ST
ER
AB
ST
RA
CT
S
146 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
to educate diabetologists on the assessment, risk and impact of NAFLD in patients with diabetes. In the subsequent 3 months 188 patients attending diabetic clinics were screened for advanced fibrosis using Fib-4. 16% of those screened had an elevated Fib-4. Data has been analyzed from >90 patients attending the multidisciplinary clinic. After 6 months follow up weight reduced by 3% (p=0.0003), ALT by 29% (p=0.0008) and HbA1c by 6.5mmol/mol (p=0.0006).
Conclusions: Amongst diabetologists, there remains limited awareness of the prevalence and severity of NAFLD in the patients they treat. Fib-4 score can easily be used in clinical practice to identify patients at risk of advanced fibrosis who are likely to benefit from a dedicated multidisciplinary approach to their management.
Figure:
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
147EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 5: YI-MR-154
THE RECOGNITION OF OXIDIZED LIPIDS BY IgM ANTIBODIES IS AN EARLY EVENT IN THE PATHOGENESIS OF HUMAN NON-ALCOHOLIC FATTY LIVER DISEASE
Tim Hendrikx* 1, 2, 3, Martin L. Watzenböck2, 3, Sofie M. Walenbergh1, Shahzada Amir2, 3, Sabrina Gruber2, 3, Heike I. Grabsch4, Ger Koek5, Marieke Pierik6, Daisy Jonkers6, Satish Kalhan7, Marten Hofker8, Christoph J. Binder2, 3, Ronit Shiri-Sverdlov1
1Molecular Genetics, MAASTRICHT UNIVERSITY, Maastricht, Netherlands, 2Laboratory Medicine, Medical University of Vienna, 3CeMM, Vienna, Austria, 4Patholgy, MAASTRICHT UNIVERSITY, 5Division of gastroenterology and hepatology, MUMC, 6Internal Medicine, MAASTRICHT UNIVERSITY, Maastricht, Netherlands, 7Pathobiology, Lerner Research Institute, Cleveland, United States, 8Pathology and Laboratory Medicine, UMC, Groningen, Netherlands
Corresponding author’s email: [email protected]
Introduction: Lipid oxidation of membrane phospholipids is accompanied by the formation of oxidation-specific epitopes (OSE). These epitopes are recognized by specific antibodies and represent danger-associated molecular patterns that are generated during chronic inflammatory processes. In a murine model for hepatic inflammation during non-alcoholic fatty liver disease (NAFLD), increased antibody levels targeting OSE were found to be protective.
Aims: Here, our aim was to determine an association between OSE-specific antibody titers and NAFLD in humans.
Material and Methods: IgM and IgG levels with specificity for various OSE were assessed in plasma of NAFLD patients (n = 71) and healthy controls (n = 68). Antibody titers were comprehensively analyzed in NAFLD patients after classification by histological evaluation of liver biopsies. Statistical analysis was performed to determine significant correlations and odds ratios. To study the specificity for lipid-induced inflammation, plasma antibody titers were measured in inflammatory bowel disease (IBD) patients (n = 62).
Results: IgM titers against OSE are lower in NAFLD patients compared to controls. Further biopsy-based classification of NAFLD patients did not show any difference in IgM levels. Importantly, low IgM titers towards the P1 mimotope demonstrated a high

ePO
ST
ER
AB
ST
RA
CT
S
148 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
predictive value for the presence of NASH, even after adjusting for total IgM level. In contrast, increased disease activity during IBD was not associated with reduced IgM titers.
Conclusions: Our data highlight the importance of immune recognition of oxidation-specific epitopes by IgM antibodies and support a protective role for specific IgM in the pathophysiology of non-alcoholic fatty liver disease.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
149EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 6: YI-MR-104
ASSOCIATION OF Pro12Ala POLYMORPHISM OF PPAR-γ GENE WITH BIOCHEMICAL MARKERS OF LIVER INJURY IN NONALCOHOLIC FATTY LIVER DISEASE PATIENTS
Vasyl Prysyazhnyuk* 1
1Depatment of Propaedeutics of Internal Medicine, Bukovinian State Medical University, Chernivtsi, Ukraine
Corresponding author’s email: [email protected]
Introduction: One of the most important genes that regulate adypo- and fibrogenesis are genes which code the synthesis of peroxisome proliferation activator receptors (PPAR). The physiological expression of PPAR-γ in adipocytes provides balanced adipocytokines (adiponectin and leptin) secretion and thus prevents the development of nonalcoholic fatty liver disease (NAFLD).
Aims: The aim of the study was to investigate a possible association of Pro12Ala polymorphism of PPAR-γ gene with biochemical markers of liver injury in NAFLD patients.
Material and Methods: Pro12Ala polymorphism of PPAR-γ gene was studied in 64 NAFLD patients and 20 healthy individuals (control group). All patients and healthy volunteers gave written informed agreement to participate in research. Biochemical blood parameters were investigated at the biochemical analyzer “Accent-200” (“Cormay SA”, Poland) using standard reagents and techniques. To determine the polymorphic variants of genes PPARγ (Pro12Ala) rs 1801282 modified protocols with oligonucleotide primers were used.
Results: Among patients with NAFLD Ala/Ala genotype was diagnosed in 1 person (1,6%), Pro/Ala – 12 (18,7%), Pro/Pro – 51 (79 7%); Ala allele of PPAR-γ gene was observed in 14 cases (10,9%) among 128 selected alleles, Pro-allele – in 114 cases (89,1%) respectively. In the group of healthy volunteers homozygous carriers of Ala-allele were not found, 3 persons (15,0%) from this group were heterozygotes, 85,0% – homozygous carriers of Pro-allele, which did not differ significantly from the genotypes distribution among NAFLD patients.Aspartataminotransferase activity in NAFLD patients Ala-allele carriers was significantly higher at 55,5% (p = 0,007) than in patients with Pro/Pro-genotype.

ePO
ST
ER
AB
ST
RA
CT
S
150 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Alaninaminotransferase activity in Ala-allele cariers was significantly higher by 80,0% (p = 0,03) compared with patients with Pro/Pro genotype. Patients with minor Ala-allele diagnosed higher γ-glutamiltransferase activity, which in 2,1 times (p = 0,04) prevailed appropriate indicator in patients with Pro/Pro-genotype.
Conclusions: Frequency of minor Ala-allele of PPAR-γ gene in patients with nonalcoholic fatty liver disease was not significantly different from that in healthy individuals. The Ala-allele of PPAR-γ gene in patients with nonalcoholic fatty liver disease was associated with significantly higher activity of biochemical markers of cytolytic and cholestatic syndromes compared with those in Pro/Pro-genotype carriers.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
151EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Friday 13 May 2016ePoster Session 8: 16:00 – 16:30
Screen 1: MR-210
ELAFIBRANOR, A LIVER TARGETED PPARα/δ AGONIST FOR GLOBAL MANAGEMENT OF NASH
Dean Hum* 1, Arun Sanyal2, Stephen A. Harrison3, Sophie Megnien1, Pierre Bedossa4, Alice Roudot1, Robert Walczak1, Remy Hanf1, Bart Staels5, 6, Vlad Ratziu7,
8
1Genfit SA, Loos, France, 2Virginia Commonwealth University, Richmond, 3Department of Medicine, Gastroenterology & Hepatology Service, Brooke Army Medical Center, Fort Sam Houston, Texas, United States, 4Department of Pathology, Hôpital Beaujon, University Paris-Denis Diderot, Paris, 5Université Lille 2, 6INSERM U1011, European Genomic Institute for Diabetes (EGID), Institute Pasteur de Lille, Lille, 7Université Pierre et Marie Curie, Hopital Pitié Salpétrière, 8Insititute of Cardiometabolism and Nutrition (ICAN), INSERM, UMRS 938, Paris, France
Corresponding author’s email: [email protected]
Introduction: Elafibranor (Ela) is in late stage clinical development for NASH. Through its liver targeting and dual activation of PPARα and PPARδ in parenchymal and non-parenchymal cells, Ela has demonstrated preventive and curative effects in animal models of NASH and fibrosis (Staels et al). Consistent with these preclinical studies, a randomized, placebo controlled trial (GOLDEN-505) has shown efficacy of a 1-year treatment with Ela at 120 mg/d on the primary outcome of resolution of NASH without worsening of fibrosis in non-diabetic and diabetic patients with NAS≥4 at inclusion (Raziu et al). This effect was seen mainly on improvement in hepatocyte ballooning and lobular inflammation, two histopathologic lesions associated with fibrosis evolution in NASH. Accordingly, most patients who resolved NASH under Ela treatment also had a significant reduction of liver fibrosis. Histological improvement was associated with improvement in hepatic markers (ALT, AST, GGT and ALP) and non-invasive scores of NASH and fibrosis. Confirming previous results in patients with metabolic disorders (Cariou et al), GOLDEN505 showed an improvement of the cardiometabolic risk profile with concomitant improvement of plasma lipids (reduction of triglycerides, total-C, LDL-C and increased HDL-C), insulin-sensitivity and glucose homeostasis (notably further decrease in HbA1c in diabetics), and inflammation/fibrosis markers. Post-hoc analyses suggest that a more marked improvement

ePO
ST
ER
AB
ST
RA
CT
S
152 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
in insulin resistance and glucose homeostasis is associated with the histological efficacy in patients with moderate to high NASH severity at baseline (NAS≥6), whereas there was no apparent relationship between changes in plasma lipids, baseline NASH severity and histological changes. In all clinical trials, Ela was safe and well tolerated without causing serious adverse effects. Overall, Ela has an ideal efficacy:safety profile to improve liver histology and outcomes while also providing a benefit on cardiovascular risk. Ela is being assessed in a phase 3 trial, RESOLVE-IT, which will recruit approximately 2000 patients with NASH and fibrosis (NAS≥4 and F2-F3). An interim analysis on the first ~1000 patients after 72 weeks will support approval based on efficacy on a histological primary end-point.
V. Ratziu et al. Gastroenterology (2016), doi: 10.1053/j.gastro.2016.01.038B. Staels et al. Hepatology (2013) 58:1941-52B. Cariou et al. Diab. Care (2011) 34:2008-14B. Cariou et al. Diab. Care (2013) 36:2923-30
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
153EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 2: YI-MR-169
VALIDATION OF NON-INVASIVE METHODS FOR ADVANCED FIBROSIS DETECTION IN NAFLD PATIENTS
Rocío Gallego-Durán* 1, 2, Rocío Aller3, Helena Pastor-Ramírez1, 2, Carmelo García-Monzón4, Jesús Bañales5, María Teresa Arias-Loste6, Eduardo Vilar-Gómez1, 2, Víctor Aguilar-Urbano7, María Luisa García-Torres8, Jose Luis Calleja9, Jose Luis Olcoz10, Javier Salmerón11, Salvador Benlloch12, Javier García-Samaniego13, Moisés Diago14, María Jesús Pareja-Megía15, Javier Ampuero1, 2, Miguel Fernández-Bermejo16, Judith Gómez-Camarero17, Raúl Jesús Andrade18, Pamela Estévez19, Conrado Fernández-Rodríguez20, Lourdes Grande21, Jose María Moreno-Planas22, Marta Maraver23, Agustín Albillos24, Manuel Romero-Gómez1, 2 on behalf of HEPAmet Registry1Inter-Centre Unit of Digestive Diseases & CIBERehd, Virgen Macarena – Virgen del Rocío University Hospitals, 2Instituto de Biomedicina de Sevilla (IBiS), Sevilla, 3Gastroenterology and Hepatology Department, Clínico de Valladolid University Hospital, Valladolid, 4Liver Research Unit and CIBERehd, University Hospital Santa Cristina , Madrid, 5Biodonostia Research Institute, San Sebastián, 6Gastroenterology and Hepatology Department,, Marqués de Valdecilla University Hospital & IDIVAL, Santander, 7Gastroenterology and Hepatology Department, Costa del Sol Hospital, Málaga, 8Gastroenterology and Hepatology Department, Clínico de Valencia University Hospital, Valencia, 9Gastroenterology and Hepatology Department, Puerta de Hierro Hospital, Madrid, 10Gastroenterology and Hepatology Department, León University Hospital, León, 11Gastroenterology and Hepatology Department, San Cecilio University Hospital, Granada, 12Gastroenterology and Hepatology Department , La Fe University Hospital, Valencia, 13Gastroenterology and Hepatology Department , La Paz University Hospital, Madrid, 14Gastroenterology and Hepatology Department , General de Valencia University Hospital, Valencia, 15Pathology Unit, Valme University Hospital, Sevilla, 16Gastroenterology and Hepatology Department , San Pedro de Alcántara Hospital, Cáceres, 17Gastroenterology and Hepatology Department , Burgos University Hospital, Burgos, 18Inter-Centre Unit of Digestive Diseases & CIBERehd , Virgen de la Victoria University Hospital, Málaga, 19Gastroenterology and Hepatology Department, Meixoeiro Hospital, Vigo, 20Gastroenterology and Hepatology Department, Fundación Alcorcón University Hospital, Madrid, 21Gastroenterology and Hepatology Department, Valme University Hospital, Sevilla, 22Gastroenterology and Hepatology Department, Albacete University Hospital, Albacete, 23Gastroenterology and Hepatology Department, , Juan Ramón Jiménez University Hospital, Huelva, 24Gastroenterology and Hepatology Department, Ramón y Cajal University Hospital, Madrid, Spain
Corresponding author’s email: [email protected]

ePO
ST
ER
AB
ST
RA
CT
S
154 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Aims: The main aim of this study was to compare the usefulness of NAFLD fibrosis score (NFS) and FIB-4 methods in predicting advanced fibrosis in a cohort of NAFLD patients.
Material and Methods: HEPAmet Registry, endorsed by Spanish Association for the Study of the Liver (AEEH), is a multicentric monitored patient database, including Spanish biopsy-proven NAFLD patients that fulfilled at least 2/4 inclusion criteria (steatosis defined by ultrasound (US); ALT or AST above upper limits of normality (ULN); HOMA-IR > 4 or Metabolic syndrome (MetS) defined by ATPIII criteria). Demographic, anthropometric, concomitant diseases and medication, US, transient elastography, analytical and anatomopathological data were recorded. Area under receiver operating curve (AUROC) and predictive values of these non-invasive scores were determined for advanced fibrosis (F3-F4) detection according to Kleiner Score. Statistical analysis was performed using SPSS 22.0 software.
Results: This interim analysis included 693 biopsy-diagnosed NAFLD patients, 42.6% (295/693) men, mean age 47.4+12 years. Of them, 53% displayed metabolic syndrome, 71.6% overweight (defined as BMI>25 kg/m2) and 27.2% suffered from type 2 diabetes mellitus. NASH was identified on 54.8% (380/693) of patients, and 11.5% (80/693) showed advanced fibrosis. Correlation coefficient between NFS and FIB4 scores respect to advanced fibrosis was 0.33 (p<0.01) and 0.29 (p<0.01) respectively. Likewise, it was obtained a correlation rate between them of 0.55 (p<0.01). 34.1% (236/693) and 15%(104/693) of patients were classified as indeterminate for NFS and FIB4 respectively. Both methods reached a similar AUROC for advanced fibrosis prediction, NFS: 0.75 [CI95% 0.69-0.81] and FIB-4: 0.74 [CI95% 0.67-0.81]. NPV for FIB4 cut-off ≤1.45 was 93.7% (536/572) and for NFS threshold ≤-1.45 was 95% (363/382). Nevertheless, using highest cutt-offs for both methods (FIB4 ≥ 3.25 and NFS≥ 0.67), PPV were 58.8% (10/80) and 34.6% (27/100) respectively.
Conclusions: Both models showed similar diagnostic efficacies for advanced fibrosis prediction, however NFS classified a higher proportion as indeterminate. PPVs were lower due in part to a low prevalence of advanced fibrosis in our cohort.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
155EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 3: YI-MR-144
ARE FEMALES REALLY MORE PROTECTED THAN MALES IN THE PROGRESSION FROM NAFLD TO NASH?
Veronica Marin* 1, Silvia Gazzin1, Matteo Dal Ben1, Alan Raseni2, Claudio Tiribelli1, 3, Natalia Rosso1
1ITALIAN LIVER FOUNDATION, 2S.C. Laboratorio Analisi Cliniche, IRCCS Burlo Garofalo, 3Department of medical sciences, University of Trieste, Trieste, Italy
Corresponding author’s email: [email protected]
Introduction: It is well accepted that NASH is more common in men than in women.
Aims: The aim of this study is to assess if females are really more protected than males in the pathogenesis of NAFLD and in the progression to NASH.
Material and Methods: Males and females C57BL/6 mice, immediately after weaning were fed ad-libitum with control (CTRL) or High-Fat High-Carbohydrate diet (HFHCD) for 16 weeks. Body-weight, glycaemia, insulinemia, triglycerides, total cholesterol, HDL-C, LDL-C, ALT and liver histology were screened every 4 weeks. Gene expression analysis and oxidative stress (MDA, GSH/GSSG) were also assessed.
Results: Soon after the 1st week, HFHCD induced a significant bodyweight gain in both genders. Males, after 4 weeks presented hyperplasia of epididymal fat-pads and after week 12th, a significant hepatomegaly, with alteration of glycaemia, insulinemia, lipid profile and ALT. Interestingly, comparable body/blood changes were observed in females only at the 16th week. Despite these differences, liver histology showed in both sexes a mixed macro-microvesicular steatosis increasing steadily after 8 weeks. DGAT2 gene expression was enhanced in both genders. Inflammatory foci were observed only in males, confirmed also by an increase in MCP-1 and TNF-α gene expression. Conversely, females had no signs of inflammation but rather presented an enhanced lipid peroxidation (MDA) and a reduction of GSH/GSSG ratio, confirming an oxidative stress (absent in males). Of notice, both sexes developed progressive fibrosis from week 8th, which rose steadily over the time (confirmed by the up-regulation of Col1A1 and αSMA mRNA expression, and the enhanced extracellular collagen deposition -Sirius Red staining).
Conclusions: Our data highlight a strong gender difference in the onset of liver damage in NAFLD/NASH. Even if the outcome (fibrosis) is similar in both sexes, from blood

ePO
ST
ER
AB
ST
RA
CT
S
156 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
parameters analysis females show no evident signs of injury until a late stage. Translating in clinical practice the lack of alteration in liver tests observed in females might be worrisome, increasing the number of potential undiagnosed NASH cases in women. This finding opens a relevant dilemma: are females really less predisposed to develop steatohepatitis during their life or is just a lack of the standard symptoms for the diagnosis?
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
157EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 4: MR-147
REGENERATE: A PHASE 3, DOUBLE-BLIND, RANDOMIZED, PLACEBO-CONTROLLED MULTICENTER STUDY OF OBETICHOLIC ACID THERAPY FOR NONALCOHOLIC STEATOHEPATITIS
Vlad Ratziu* 1, Arun J. Sanyal2, Leigh MacConell3, Reshma Shringarpure3, Tonya Marmon3, David Shapiro3, Zobair M. Younossi4, 5
1Hepatology, Hopital Pitie Salpetriere, Paris, France, 2Virginia Commonwealth University, Richmond, 3Intercept Pharmaceuticals, Inc., San Diego, 4Center for Liver Disease, Inova Fairfax Hospital,, 5Betty and Guy Beatty Center for Integrated Research, Inova Health System, Falls Church, United States
Corresponding author’s email: [email protected]
Introduction: Nonalcoholic Steatohepatitis (NASH) is a slowly progressive chronic liver disease without approved therapies. Patients with NASH and fibrosis are at high risk of increased mortality. Obeticholic Acid (OCA) is a selective and potent farnesoid X receptor (FXR) agonist, that has been shown to improve liver histology, including NAFLD activity score (NAS) and fibrosis, in a Phase 2 clinical trial (FLINT). Furthermore in FLINT, OCA treated patients had significant improvements in select liver biochemistries, markers of inflammation, and select cardiometabolic parameters. The ongoing, randomized, global, Phase 3 study REGENERATE, will further evaluate the effect of OCA on liver histology and clinical outcomes in patients with biopsy-confirmed NASH with stage 2-3 fibrosis.
Material and Methods: 2065 patients will be randomized 1:1:1 to 10 mg OCA, 25 mg OCA or placebo (Figure), each added to standard of care. An interim analysis at 18 months will evaluate the effect of OCA on liver histology. Total study duration is driven by time required to accrue a total of 264 outcome events and is estimated to be ~6 years. Safety assessments will include adverse events (AEs), adjudicated cardiovascular events, and hepatic events as well as laboratory assessments. The effect of OCA on NASH and fibrosis severity will also be assessed by multiple noninvasive methods (FIB-4, APRI, transient elastography, magnetic resonance elastography, etc.).
Results: The co-primary liver histology endpoints at 18 months include: (I) improvement in fibrosis by ≥1 stage with no worsening of NASH and (II) resolution of NASH with no worsening in fibrosis stage. Further, confirmation of clinical benefit of OCA will be assessed at the end of the study by comparing the time to first occurrence of any of the

ePO
ST
ER
AB
ST
RA
CT
S
158 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
following adjudicated events: histological progression to cirrhosis; uncontrolled ascites; hospitalization for: variceal bleed, hepatic encephalopathy or spontaneous bacterial peritonitis; hepatocellular carcinoma; liver transplant or eligibility for liver transplant (defined by model for end stage liver disease (MELD) score ≥15); and death.
Conclusions: REGENERATE is the first pivotal study in NASH, designed in conjunction with FDA and meant to support approval of OCA for NASH with fibrosis. This robust Phase 3 study is designed to evaluate the effect of OCA on liver histology and effects on progression to cirrhosis, liver-related clinical outcomes and mortality.
Figure:
Disclosure of Interest: V. Ratziu: Consultant: Conflict with: Tobira, Intercept, Exalenz, Sanofi-Synthelabo, Boehringer-Ingelheim, Other: Conflict with: GalMed, Abbott, Genfit, Enterome, Gilead, A. Sanyal: Grant: Conflict with: Salix, Genentech, Intercept, Ikaria, Takeda, GalMed, Novartis, Gilead, Tobira, Consultant: Conflict with: Salix, Immuron, Exhalenz, Nimbus, Genentech, Echosens, Takeda, Merck, Enanta, Zafgen, JD Pharma, Islet, Sciences, Other: Conflict with: Bristol Myers, Gilead, Genfit, Abbott, Ikaria, Exhalenz, UpToDate, Elsevier, L. MacConell: Stockholder: Conflict with: Intercept Pharmaceuticals, Inc., Employee: Conflict with: Intercept Pharmaceuticals, Inc., R. Shringarpure: Stockholder: Conflict with: Intercept Pharmaceuticals, Inc., Employee: Conflict with: Intercept Pharmaceuticals, Inc., T. Marmon: Stockholder: Conflict with: Intercept Pharmaceuticals, Inc., Employee: Conflict with: Intercept Pharmaceuticals, Inc., D. Shapiro: Stockholder: Conflict with: Intercept Pharmaceuticals, Inc., Employee: Conflict with: Intercept Pharmaceuticals, Inc., Z. Younossi: Consultant: Conflict with: Gilead, Enterome, Coneatus, Other: Conflict with: Salix, Janssen, Vertex

ePO
ST
ER
AB
ST
RA
CT
S
159EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 5: MR-180
SARCOPENIA IS AN INDEPENDENT RISK FACTOR FOR BIOPSY-PROVEN NON-ALCOHOLIC STEATOHEPATITIS IN A KOREAN POPULATION
Won Kim* 1, Bo Kyung Koo2, Sae Kyung Joo1, Jung Ho Kim3, Dong Hyun Lee1, Yong Jin Jung1, Donghee Kim4
1Division of Gastroenterology and Hepatology, 2Division of Endocrinology, 3Department of Pathology, Seoul Metropolitan Government Boramae Medical Center, Seoul, Korea, South, 4Division of Gastroenterology and Hepatology, Stanford University, Stanford, United States
Corresponding author’s email: [email protected]
Introduction: Non-alcoholic fatty liver disease (NAFLD) has been frequently found in the non-obese as well as the obese. Furthermore, Asians have a relatively higher prevalence of NAFLD despite lower body mass index (BMI).
Aims: We explored whether sarcopenia, independent of total body fat mass, might affect the histological severity of NAFLD including non-alcoholic steatohepatitis (NASH) and significant fibrosis in a histologically confirmed NAFLD registry cohort.
Material and Methods: NAFLD was categorized as non-NASH NAFL and NASH according to the NASH CRN histologic scoring system. To estimate the appendicular skeletal muscle mass (ASM) and total fat mass, impedance for each segment, including the four limbs and trunk, was measured using multi-frequency bioelectrical impedance analysis. Sarcopenia was defined by either sarcopenic index (SI, ASM/height2) or ASM divided by body weight (ASM%, ASM/Bwt).
Results: Among 309 subjects (145 men and 164 women), 39.8%, 37.9%, and 22.3% were classified as NASH, non-NASH NAFL, or non-NAFLD, respectively. Subjects with sarcopenia had a higher BMI (P<0.001), waist circumference (P<0.001), and homeostasis model assessment of insulin resistance (HOMA-IR) (P=0.004) and a lower cholesterol level (P=0.029) and more frequently hypertension (P<0.001) compared to those without sarcopenia. ASM% was inversely correlated with lobular inflammation (r=-0.134, P=0.029), ballooning (r=-0.148, P=0.013), and fibrosis stages (r=-0.198, P=0.001), but not steatosis (r=-0.052, P=0.384). In logistic regression analyses adjusted for age and gender, sarcopenia was an independent risk factor for NAFLD (odds ratio of SI, 2.60; 95% confidence interval, 1.05–6.43; P=0.039 and OR of ASM%, 3.81; 95% CI, 1.57–

ePO
ST
ER
AB
ST
RA
CT
S
160 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
9.25; P=0.033); however, sarcopenia was no more an independent risk factor for NAFLD in multivariate analysis. On the contrary, sarcopenia was an independent risk factor for NASH in multivariate analysis even after adjustment for age, gender, BMI, smoking, hypertension, diabetes, cholesterol, triglycerides, HDL-cholesterol, and HOMA-IR (OR of ASM%, 1.97; 95% CI, 1.01–3.87; P=0.048). Moreover, sarcopenia was an independent risk factor for significant fibrosis in multivariate analysis adjusted for age, gender, BMI, smoking, hypertension, diabetes, triglycerides, platelet, albumin, and HOMA-IR (OR of SI, 2.24; 95% CI, 1.06–4.73; P=0.034 and OR of ASM%, 2.05; 95% CI, 1.01–4.16; P=0.048).
Conclusions: Sarcopenia was significantly associated with the histological severity of NAFLD in a Korean population. Further studies are warranted to validate these findings in other ethnic populations with NAFLD.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
161EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 6: YI-MR-120
LEAN VERSUS OVERWEIGHT/OBESE NONDIABETIC NONALCOHOLIC FATTY LIVER DISEASE (NAFLD) – A CLINICOPATHOLOGICAL COMPARATIVE STUDY
Sanchit Budhiraja* 1, Ashok K. Jain1, Vinod K. Dixit1, Sunit K. Shukla1, Pankaj K. Asati1, Manish K. Tripathi1
1Gastroenterology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, India
Corresponding author’s email: [email protected]
Introduction: Nonalcoholic fatty liver disease (NAFLD) refers to the accumulation of fat (mainly triglycerides) in hepatocytes that arises due to insulin resistance. A fraction of NAFLD patients (especially Asians) do not meet weight criteria of obesity. Most low BMI NAFLD patients have central obesity and are metabolically obese, which includes findings of insulin resistance.
Aims: The aim of this study was to compare the clinicopathological and biochemical profile of lean and overweight/obese NAFLD patients with a special emphasis on insulin resistance.
Material and Methods: This prospective study was conducted in biopsy proven NAFLD patients aged 18 to 75 years in a university hospital in India. On the basis of Asia Pacific criteria, the patients were divided into lean (BMI <22.99 kg/m2) and overweight/obese (BMI ≥23 kg/m2) NAFLD. Histopathological NASH was defined by NAS (NAFLD activity score) ≥5. Patients with other liver diseases (hepatitis B, C or autoimmune liver disease) and diabetes mellitus were excluded.
Results: Among 88 NAFLD patients, 29 (33%) and 59 (67%) were in the lean and overweight/obese group respectively. The mean age was 33.31 years which was similar in both the groups. Metabolic syndrome was present in 60 (68.2 %) patients. In the lean and overweight/obese group, 55.2% and 74.6% patients had metabolic syndrome respectively (p 0.06). In the lean group, the mean weight (62.76kg, p<0.0001), height (1.71m, p<0.0001), waist circumference (83cm, p<0.0001), hip circumference (89.14cm, p 0.003), waist:hip ratio(0.93, p<0.0001) was significantly lower as compared to overweight/obese group (the respective values being 71.25kg, 1.66m, 92.47cm, 94.90cm,0.97). The median triglyceride level (190mg/dl vs 147 mg/dl; p 0.018) and mean VLDL level (50.40mg/dl vs 33.99mg/dl; p<0.0001) was significantly higher in the lean NAFLD group. However, the

ePO
ST
ER
AB
ST
RA
CT
S
162 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
median levels of fasting serum insulin (5.57μU/ml vs 10.83μU/ml; p 0.009) and HOMA-IR (1.37 vs 2.62; p 0.010) were significantly lower in the lean NAFLD group. NASH was present in 59 patients (67%). 75.9% of the lean patients and 62.7% of overweight/obese patients had NASH (p 0.22). There was no difference in the level of ALT, AST: ALT ratio, HDL or total cholesterol in the two groups.
Conclusions: Lean NAFLD patients had lower mean weight, height, waist:hip ratio. Dyslipidemia was more common in the lean NAFLD group whereas insulin resistance was less in lean NAFLD group. Metabolic syndrome and NASH were equally present in both the groups irrespective of BMI.
Figure:
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
163EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Saturday 14 May 2016ePoster Session 9: 08:30 – 09:00
Screen 1: MR-125
HEPATOCELLULAR CARCINOMA IN NON-ALCOHOLIC STEATOHEPATITIS (NASH) – HISTOPATHOLOGICAL ASPECTS
Priscila B. Campos1, Claudia P. Oliveira* 1, Luciana Kikuchi1, Jose Tadeu Stefano1, Aline L. Chagas1, Paulo Herman2, Luiz Augusto C. D’Albuquerque2, Mário R. Alvares-da-Silva3, Flair Jose Carrilho1, Venâncio A. F. Alves4
1Gastroenterology (LIM-07), 2Gastroenterology (LIM-37), University of São Paulo School of Medicine, SAO PAULO, 3Gastroenterology, Hospital de Clinicas de Porto Alegre, Universidade Federal do Rio Grande do Sul, PORTO ALEGRE, 4Pathology (LIM-14), University of São Paulo School of Medicine, SAO PAULO, Brazil
Corresponding author’s email: [email protected]
Introduction: Hepatocellular carcinoma (HCC) is the most common primary malignancy of the liver. The raise in incidence has been ascribed to the increase in obesity, diabetes and non-alcoholic fat liver disease (NAFLD).
Aims: The aim of this study is to evaluate the pathological and clinical aspects in patients with HCC secondary to NAFLD.
Material and Methods: We evaluated 28 HCC specimens from 18 patients diagnosed with NAFLD undergoing liver resection (10 patients) or liver transplantation (8 patients) from 2005 to 2015. We compared histological features, clinical aspects, imaging findings, demographic and biochemical data, as well as their survival.
Results: We analyzed 11 patients with cirrhosis and 7 patients without cirrhosis, and from them, 28 HCC nodules, 8 (28%) were developed in patients without cirrhosis (NASH staging: F2: 5pts, F3=2pts), while 20 (72%) nodules were developed in patients with cirrhosis (8 F4A x 11 F4B, x 1F4C according Laennec Stage). Ages ranged from 58 to 77 years and 13 patients were male (72%). Thirteen patients (72%) had diabetes mellitus, 13 patients (72%) had arterial hypertension, and 14 patients (77%) had BMI above 25. Only 6 patients (33%) had dyslipidemia. HCC occurred in 7 patients Child A, 4 Child

ePO
ST
ER
AB
ST
RA
CT
S
164 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
B and in 7 patients without cirrhosis. As the performance status, 16 patients had a good performance status (PS) with Eastern Cooperative Oncology Group (ECOG) = 0. Alpha-fetoprotein level was normal in 12 patients. The dimensions of the HCC nodules ranged from 0.8 cm (single nodule) to 15cm in diameter and the predominant macroscopic pattern was nodular (93%). The predominant microscopic pattern was trabecular (46%). Major histological features of HCC are depicted at Table 1. Of all the patients, 11 evolved to death, 8 cases in patients who underwent resection and 3 cases that underwent liver transplantation. The causes of death were primary non function, infection, acute rejection and palliative care caused by the evolution of HCC.
Conclusions: HCC secondary to NAFLD can arise in patients without cirrhosis with normal level of alpha-fetoprotein. Histological markers of “steato-hepatitic HCC” and high architectural and nuclear degrees (g.3) were prevalent. The survival rate was low, especially in patients who underwent resection, despite the good performance status.
Figure:
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
165EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 2: YI-MR-121
LIVER STIFFNESS VALUES MEASURED BY SHEAR WAVE ELASTOGRAPHY DEPENDING ON TRANSAMINASE ACTIVITY IN PATIENTS WITH NONALCOHOLIC FATTY LIVER DISEASE
Nazarii Kobyliak* 1, Oleg Dynnyk 2, Galyna Mykhalchyshyn1, Petro Bodnar1
1Endocrinology, Bogomolets National Medical University, 2Bogomolets Institute of physiology of the Ukrainian National Academy of Sciences, Kyiv, Ukraine
Corresponding author’s email: [email protected]
Introduction: Shear Wave Elastography (SWE) is one of the most promising non-invasive methods for diagnosis of chronic diffuse liver disease. Given its widespread introduction into clinical practice, more attention is paid to the group of scientists from around the world, to the study of factors that can affect the measurement and its diagnostic accuracy.
Aims: The aim of our study was to estimate changes of liver stiffness measured by SWE and evaluation of factors that may affect its value depending on transaminase activity in patients with NAFLD.
Material and Methods: We studies 122 patients with T2D who were diagnosed with fatty liver by abdominal ultrasonography. All patients divided by us on 3 groups. The control group (n=27) included 34 patients with TD2 without NAFLD. In the other two groups we identified patients with NAFLD and normal (n=62) or elevated (n=33) level of transaminases. We performed 10 valid liver stiffness measurement (LSM) in every patient, and a median value was calculated, the result being measured in kPa.
Results: LSM were significantly higher on 44.6% in the increased ALT group and on 32.3% in patients with normal ALT as compared with control group (p<0.001). Also we observed significant higher on 10% LSM in patients with NAFLD and elevated transaminase activity compared to normal ALT group (p=0.003). In univariate correlation analysis insulin resistance by HOMA-IR was significantly associated with LSM in all studies groups. In patients with NAFLD independent from transaminase activity LSM were significantly correlated with anthropometric parameters. Maximum strength of correlation in patients of normal ALT group was observed between LSM and BMI (r = 0.651, p<0.001), therefore in elevated transaminase group for waist circumference (r =0.634, p<0.001). LSM were significantly correlated with ALT (r=-0.483, p=0.004)

ePO
ST
ER
AB
ST
RA
CT
S
166 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
and AST (r=0.499, p=0.003) only in patients with it elevation. Step-wise multiple linear regression analyses demonstrated that in NAFLD patients independent predictors of LSM increasing were HOMA-IR, waist circumference, ALT (adjusted R2 0.582) and AST (adjusted R2 0.541) respectively.
Conclusions: Patients with NAFLD and especially with elevated transaminases have significantly higher liver stiffness values measured by SWE as compared with control. Use both univariate correlation and multiple linear regression analysis showed that independent determinants associated with increasing of LSM were degree of insulin resistance, obesity and transaminase activity.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
167EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 3: YI-MR-173
LYSOSOMAL ACID LIPASE ACTIVITY IS ASSOCIATED WITH AST TO PLATELET RATIO INDEX IN PATIENTS WITH NON-ALCOHOLIC FATTY LIVER DISEASE
Francesco Baratta* 1, Daniele Pastori1, Licia Polimeni1, Giulia Tozzi2, Francesco Violi1, Maria Del Ben1, Francesco Angelico1
1SPAIENZA- UNIVERSITÀ DI ROMA, 2Children’s Hospital and Research Institute “Bambino Gesù, roma, Italy
Corresponding author’s email: [email protected]
Introduction: Lysosomal Acid Lipase (LAL) is a key enzyme in lipid metabolism. Recent evidence suggested that a reduced LAL activity may be found in patients with non-alcoholic fatty liver disease (NAFLD).
Aims: To investigate the relationship between LAL activity and non invasive markers of liver fibrosis.
Material and Methods: We included 280 consecutive patients with ultrasonography (us) evidence of NAFLD. Severity of NAFLD was classified according to Hamaguchi’s criteria. As marker of liver fibrosis, the AST to platelet ratio index (APRI) was calculated for each patient. LAL activity was assessed on dried blood spot with Lalistat 2 method.
Results: Mean age was 55,2 ± 12,3 year and 35,6% were women. 24,3% patients had mild, 41% moderate and 35,7% severe US steatosis. Mean HOMA index was 4,5 ± 3,3. Mean LAL activity was 0,93 ± 0,42 nmol/spot/h. Mean APRI was 0.26 ± 0.18. APRI was correlated with LAL activity (r=-0.245, p<0.001), HOMA index (r=0.154, p=0.01), Hamaguchi score (r=0.213, p<0.001). At multivariable linear regression analysis APRI was indipendently correlated with LAL activity (B: – 0,199; p=0.001), Hamaguchi score (B: 0,128; p<0.05), HOMA index (B: 0,164; p=0.01).Mean age was 55,2 ± 12,3 year and 35,6% were women. 24,3% patients had mild, 41% moderate and 35,7% severe steatosis. Mean HOMA index was 4,5 ± 3,3. Mean LAL activity was 0,93 ± 0,42 nmol/spot/h. Mean APRI was 0.26 ± 0.18. APRI was correlated with LAL activity (r=-0.245, p<0.001), HOMA index (r=0.154, p=0.01), Hamaguchi score (r=0.213, p<0.001). At multivariable linear regression analysis APRI was indipendently correlated with LAL activity (B: -0,199; p=0.001), Hamaguchi score (B: 0,128; p<0.05), HOMA index (B: 0,164; p=0.01).

ePO
ST
ER
AB
ST
RA
CT
S
168 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Conclusions: We found that in patients with NAFLD, LAL activity was associated with the severity of liver fibrosis, as assessed by the APRI index. Further study are needed to confirm the association between reduced LAL activity and histological severity of liver fibrosis.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
169EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 4: MR-137
NON-ALCOHOLIC FATTY LIVER DISEASE PATIENT’S PROFILE IN LATVIA
Jekaterina Kucina* 1, Ieva Tolmane2, Ivars Tolmanis3, Baiba Rozentale1
1at Riga East Clinical University hospitals, stationary “Infectology Center of Latvia”, Riga, Latvia, 2Hepatology, at Riga East Clinical University hospitals, stationary “Infectology Center of Latvia”, 3Digestive Diseases Centre ‘’GASTRO’’, Riga, Latvia
Corresponding author’s email: [email protected]
Introduction: Non-alcoholic fatty liver disease is becoming a widespread liver disease in highly developed countries leading to liver insufficiency, which in turn diminishes patients’ quality of life, as well as enhances the development of physical incapacity.
Aims: To identify the profile of patients with non-alcoholic fatty liver disease in Latvia.
Material and Methods: The study was carried out both retrospectively and prospectively at Riga East Clinical University hospitals clinic “Infectology Center of Latvia”. The study included 75 patients with morphologically established non-alcoholic fatty liver disease (NAFLD) or steatohepatitis (NASH). Patients were interviewed by telephone with a specially designed questionnaire, which included information about lifestyle, physical activities and health. Analysis of medical documentation was performed.
Results: Among the 75 patients with NAFLD, 45.3% (n=34) of patients were female and 54.7% (n=41) were male. Average age was 47.6 ± 11.0 years. It was recognized that 46.7% (n=35) of patients with NAFLD were obese (body mass index (BMI) ≥30.0 kg/m2) and 34.7% (n=26) – overweight (BMI 25.0 – 29.9 kg/m2). At the time of diagnosis, patients already had serious morphological changes in liver – 44.0% (n=33) had severe stage steatosis 61.3% (n=46) – mixed type and 58.6% (n=44) had inflammatory cell infiltration. Elevated alanine aminotransferase activity was detected in 86.6% (n=65) of patients, aspartate aminotransferase activity – in 89.3% (n=67) of cases. At least one potentially dangerous comorbidity occurs in 56.0% (n=42) of patients. Respondents mainly had type 2 diabetes mellitus, it occurred in 20.0% (n=15) of patients, hypercholesterolemia – in 48.0% (n=36) of patients, arterial hypertension – in 37.3% (n=28) of patients. Physically active 7 times a week were 32.0% (n=24) of patients, 2 – 3 times a week – 20.0% (n=15) of patients, 1 – 2 times a week – 32.0% (n=24) of patients. Patients were more often engaged in physical activities 1 – 3 times a week.

ePO
ST
ER
AB
ST
RA
CT
S
170 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Conclusions: Patients with non-alcoholic fatty liver disease in Latvia are mostly middle-aged people of both genders with predominantly sedentary lifestyle. Most of them have obesity and diseases associated with non-alcoholic fatty liver disease.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
171EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 5: YI-MR-128
RESVERATROL IMPROVES HEPATIC NITRIC OXIDE SYNTHESIS AND ATTENUATING ENDOTHELIAL DYSFUNCTION IN NON-ALCOHOLIC FATTY LIVER DISEASE
Balasubramaniyan Vairappan* 1, Sundhar Mohandas1
1Biochemistry, Jawaharlal Institute of Postgraduate Medical Education and Research, Pondicherry, India
Corresponding author’s email: [email protected]
Introduction: Endothelial nitric oxide synthase (eNOS) deficient mice have shown to increase early stage of non-alcoholic statohepatitis (NASH) pathogenesis. Resveratrol treatment has been suggested to bear protective effects on liver injury of various aetiologies. Indeed, the role of resveratrol in modulating hepatic nitric oxide (NO) synthesis and related molecular mechanism involved in non-alcoholic fatty liver disease (NAFLD) remains unidentified.
Aims: The purpose of this study was to evaluate the effect of resveratrol on high-fat diet (HFD) induced endothelial dysfunction and associated fatty liver disease in mice.
Material and Methods: CD-1 mice (n=10/group) were studied for 90 days. Three groups were studied. 1) control, 2) HFD (Dyets Inc. USA) and 3) HFD + resveratrol (Sigma, USA; 10mg/kg b.w. daily by gastric lavage, for 7 days)
Results: Compared to naive mice, HFD supplementation significantly (p<0.001) increased serum alanine aminotransferase (ALT), aspartate aminotransferase (AST), interleukin (IL)-1β, tumour necrosis factor (TNF) α and asymmetric dimethylarginine (ADMA). Resveratrol treatment to HFD treated mice shows significantly (p<0.05) reduced the above parameters. Furthermore, HFD fed mice show significantly (p<0.05) increased hepatic protein expression of eNOS, iNOS and neuregulin-1 (NRG-1) when compared to control. Resveratrol treatment to HFD fed mice significantly decreased the expression of eNOS and iNOS but NRG-1 expression was unaltered. Resveratrol treatment significantly (P<0.05) increased hepatic NO levels in HFD fed mice.
Conclusions: Our study is the first indication of evidence that the significant improvement of NO and decreased NOS inhibitor by resveratrol in NAFLD and provide a future therapeutic approach for NAFLD patients with endothelial dysfunction.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
172 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Screen 6: YI-MR-179
SPLEEN DIMENSIONS EVALUATED BY ULTRASOUND ARE INVERSELY ASSOCIATED WITH LYSOSOMAL ACID LIPASE ACTIVITY IN PATIENTS WITH NON-ALCOHOLIC FATTY LIVER DISEASE
Licia Polimeni* 1, Daniele Pastori1, Francesco Baratta1, Giulia Tozzi2, Fiorella Piemonte2, Francesco Violi1, Francesco Angelico3, Maria Del Ben1
1Department of Internal Medicine and Medical Specialties, Sapienza University, 2Unit for Neuromuscular and Neurodegenerative Diseases, Children’s Hospital and Research Institute “Bambino Gesù”, 3Department of Public Health and Infectious Diseases, Sapienza University, Rome, Italy
Corresponding author’s email: [email protected]
Introduction: Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease. Lysosomal Acid Lipase (LAL) is a key enzyme in lipid metabolism and a reduction of its activity may contribute to intracellular lipid accumulation in adult NAFLD. Splenomegaly is a typical feature of both Wolman Syndrome and Cholesterol Ester Storage Disease, the two genetic forms of LAL deficiency. A less severe reduction of LAL activity has been suggested as an under-recognized cause of NAFLD. Ultrasonography (US) determination of spleen dimensions is accurate.
Aims: The aim of this study was to determine if spleen biometry evaluated by US is associated with LAL activity in a population of NAFLD patients.
Material and Methods: The study has been performed in 252 consecutive patients with a liver US positive for NAFLD. Spleen longitudinal diameter and area were measured during US. Splenomegaly was defined as a spleen area >45 cm2 and /or longitudinal diameter >12 cm. LAL activity was measured with dried blood spot method (Lalistat2, nmol/spot/h).
Results: Mean age was 55.1 ± 10.8 years and 38.1% of patients were women. US showed splenomegaly in 33 patients (13,1%). From the lower to the highest quartile of spleen area a significant decrease of LAL activity (0.95 vs 0.87 vs 0.77 vs 0.78 nmol/spot/h; p< 0.05), age (57.9 vs 56.2 vs 55.9 vs 55.1 years; p=0.001) and prevalence of statin users (42.9 vs 41.4 vs 25.9 vs 19.6 %; p< 0.05) were found; on the contrary, BMI (28.3 vs 30.2 vs 31.2 vs 31.3 kg/m2; p< 0.01) and waist circumference (103.0 vs 105.0 vs 109.0 vs
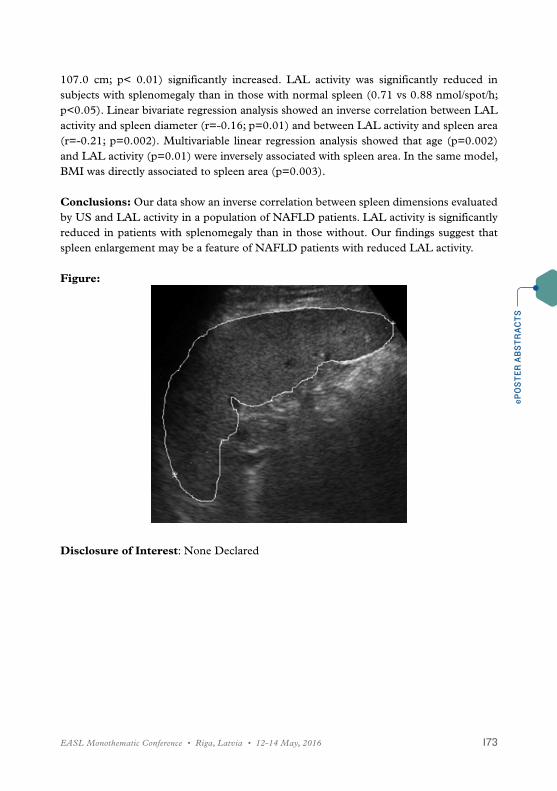
ePO
ST
ER
AB
ST
RA
CT
S
173EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
107.0 cm; p< 0.01) significantly increased. LAL activity was significantly reduced in subjects with splenomegaly than in those with normal spleen (0.71 vs 0.88 nmol/spot/h; p<0.05). Linear bivariate regression analysis showed an inverse correlation between LAL activity and spleen diameter (r=-0.16; p=0.01) and between LAL activity and spleen area (r=-0.21; p=0.002). Multivariable linear regression analysis showed that age (p=0.002) and LAL activity (p=0.01) were inversely associated with spleen area. In the same model, BMI was directly associated to spleen area (p=0.003).
Conclusions: Our data show an inverse correlation between spleen dimensions evaluated by US and LAL activity in a population of NAFLD patients. LAL activity is significantly reduced in patients with splenomegaly than in those without. Our findings suggest that spleen enlargement may be a feature of NAFLD patients with reduced LAL activity.
Figure:
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
174 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Saturday 14 May 2016ePoster Session 10: 11:00 – 11:30
Screen 1: YI-MR-148
CYTOKERATIN 18 FRAGMENT LEVEL IS A USEFUL BIOMARKER IN PREDICTING STEATOSIS AND NASH BUT NOT FIBROSIS
Sanchit Budhiraja* 1, 1, Ashok K. Jain1, Vinod K. Dixit1, Sunit K. Shukla1, Ashutosh Jain2, Pankaj K. Asati1
1Gastroenterology, 2Internal Medicine, Institute of Medical Sciences, Banaras Hindu University, Varanasi, India
Corresponding author’s email: [email protected]
Introduction: Non alcoholic fatty liver disease (NAFLD) is a spectrum of liver disease (from minor steatosis to cirrhosis). Differentiating various stages of the disease is important for therapeutic decision making and prognostic outcomes. The gold standard for the diagnosis and staging of NAFLD is liver biopsy. Cytokeratin 18 fragment (CK18-F) levels are a marker of hepatocyte apoptosis.
Aims: The aim of this study was to evaluate the role of serum cytokeratin 18 fragment level (CK18-F) in predicting steatosis, significant NASH and fibrosis when compared to the gold standard i.e liver biopsy.
Material and Methods: 88 patients with biopsy proven NAFLD were enrolled. Histological findings were classified according to the NAFLD activity score (NAS) proposed by the Nonalcoholic Steatohepatitis Clinical Research Network. In addition to basic serum biochemical profile, serum CK18-F level was measured using M30 Apoptosense ELISA. Patients with diabetes mellitus and significant alcohol consumption were excluded.
Results: Of the 88 patients, 59 (67%) had a NAS score of ≥5 suggesting histopathological NASH and 33% patients had a score of <5. The mean level of CK18-F was significantly (p 0.024) higher (382±138 U/L) when significant steatosis (steatosis grade 2 or 3 on NAS) was present as compared to when there was no/mild steatosis [(320±106.8 U/L) (steatosis grade 0 or 1 on NAS scoring)]. There was a statistically significant difference in the level

ePO
ST
ER
AB
ST
RA
CT
S
175EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
of CK18-F in the group with NASH (NAS ≥5) when compared to the group with no NASH (NAS<5). Even though the CK18-F level was higher in the group with fibrosis grade 1-2 (381.9±139.22 U/L) as compared to the group with no fibrosis (334.6±117.05 U/L), this was not statistically significant (P 0.087). The AUROC for detection of NASH for CK18-F was 0.82. A value of 304 U/L was 83.1 % sensitive and 82.8% specific for the diagnosis of significant NASH. The AUROC for fibrosis detection using CK18-F was 0.62. A value of 325.5 was 62% sensitive and 61% specificity for diagnosis of fibrosis.
Conclusions: Measurement of serum CK18-F was useful in prediction of significant steatosis and NASH but not fibrosis.
Figure:
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
176 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Screen 2: YI-MR-165
NATURAL EXTRACTS ABOLISH LIPID ACCUMULATION IN CELLS HARBOURING NON-FAVOURABLE PNPLA3 GENOTYPE
Ángela Rojas* 1, Jose A Del Campo2, Rosario Maldonado3, Paloma Gallego4, Juan Bautista4, Manuel Romero-Gómez1
1Unit for Clinical Management of Digestive Diseases and CIBERehd, Inter-Centre Unit of Digestive Diseases and CIBERehd, Virgen Macarena – Virgen del Rocío University Hospitals, INSTITUTE OF BIOMEDICINE OF SEVILLE, UNIVERSITY OF SEVILLE, SEVILLA, SPAIN., 2Unit for Clinical Management of Digestive Diseases and CIBERehd, 3Clinical and Experimental Pharmacology Research Unit, , Valme University Hospital, Sevilla, 4Biochemistry and molecular biology, University of Seville, Seville, Spain
Corresponding author’s email: [email protected]
Introduction: Hepatic steatosis is characterized by the excessive triglycerides accumulation as lipid droplets in the cytoplasm of hepatocytes, which result from an imbalance between uptake, synthesis, export, and oxidation of fatty acids. G-allele of PNPLA3 favours the increase of triglycerides accumulation.
Aims: In this study, we examined the effect of quercetin and other natural extracts from mushroom (M) and artichoke (A) on reducing lipid accumulation in hepatic cells.
Material and Methods: Hepatocytes (Huh7.5) were treated with oleic acid 1mM (OA) containing with or without quercetin and soluble extracts to observe the lipid accumulation by Oil Red O stain, the intracelular triglycerides (TG) concentration by Nile Red and the LD size measured by Imaging Software cell^F. Reverse transcription polymerase chain reaction (RT-PCR) was used to measure sterol regulatory element binding proteins-1 (SREBP-1), peroxisome proliferator-activated receptor (PPARα) and γ and cholesterol acyltransferase (ACAT) expression. . PNPLA3 (rs738409) genotype was determined by RT-PCR Taqman probes.
Results: Quercetin prevents stetosis decreasing the intracellular concentration of lipids, the lipids droplets size and the levels of intracellular TG through the down-regulation of SREBP-1c, PPARγ and ACAT1 expression levels however it increases PPARα expression. The natural extracts suppressed OA-induced lipid accumulation (figue 1) and the

ePO
ST
ER
AB
ST
RA
CT
S
177EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
intracellular TG. Also, they tend to decrease the hepatic lipogenesis through SREBP-1c, besides the activation of lipolysis through the increasing the expression of PPARα.
Conclusions: Quercetin has the same ability to the water-soluble extracts suppressing significantly the intracellular lipid accumulation in a steatosis model induced by OA. These components tend to reduce SREBP-1c expression, finally leading to inhibit hepatic lipogenesis. The increased activation of PPAR”” inducing lipolysis and together the reduction of lipogenesis could be postulated to be responsible for decreased hepatic fat content. In this report, we found some component in the natural extracts which has a regulatory effect on lipid accumulation and shown the evidence evaluating the mechanisms of action hepatic lipid metabolism in different experimental setting: in vitro, in vivo, and in human trials.
Figure:
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
178 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Screen 3: YI-MR-132
PRIMARY CARE SEQUENTIAL USE OF FIB-4 AND THE ENHANCED LIVER FIBROSIS TEST TO STRATIFY PATIENTS WITH NAFLD DOUBLES CIRRHOSIS DETECTION AND REDUCES REFERRALS OF PATIENTS WITH MILD DISEASE
Ankur Srivastava* 1, 2, 3, Ruth Gailer4, 5, Shirin Demma1, Sudeep Tanwar1, 6, Alex Warner5, Deepak Suri2, 7, Sarah Morgan5, Karen Sennett8, Douglas Thorburn1, 3, Julie Parkes1, 9, Emmanouil Tsochatzis1, 3, William Rosenberg1, 3 and Camden and Islington Liver Working Group1Department of Hepatology, UCL INSTITUTE OF LIVER AND DIGESTIVE HEALTH, 2Department of Hepatology, University College London Hospital, 3Hepatology and Liver Transplantation, Royal Free London, 4Primary Care and Population Health, University College London, 5Primary Care, Camden Clinical Commissioning Group, 6Department of Gastroenterology, Barts Health, 7Department of Gastroenterology, Whittington Hospital, 8Primary Care, Islington Clinical Commissioning Group, London, 9Public Health Sciences and Medical Statistics, University of Southampton, Southampton, United Kingdom
Corresponding author’s email: [email protected]
Introduction: Identifying patients with NAFLD who may develop cirrhosis in primary care is difficult. Patients with advanced fibrosis remain undiagnosed until presenting with decompensated cirrhosis, whilst many with mild disease are referred to busy specialist clinics. In March 2014, Camden & Islington (C&I) London boroughs commisioned a primary care risk stratification pathway using FIB-4 followed by ELF test for indeterminate cases.
Aims: At 18 months, we evaluated pathway effectiveness data to assess impact on cirrhosis detection.
Material and Methods: Patients with NAFLD & abnormal transaminases were eligible for pathway entry. Patients were stratified to low risk (FIB-4<1.30; or FIB-4 1.30-3.25 & ELF<9.5) or high risk (FIB-4>3.25; or FIB-4 1.30-3.25 & ELF>9.5) indicative of ≥F3 fibrosis. High-risk patients were recommended for referral. For primary care outcomes, the C&I electronic database was interrogated for aggregate data. For secondary care

ePO
ST
ER
AB
ST
RA
CT
S
179EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
outcomes, hospital records were reviewed at Royal Free London, UCLH & Whittington Hospital of all referred patients. The primary endpoint was “consultant’s final fibrosis assessment” – a binary outcome: Advanced fibrosis/Cirrhosis vs. lesser degree/no fibrosis based on composite of liver histology (when available), imaging, fibroscan, bloods & clinical judgement. Diagnostic performance was compared to pre-pathway (2012-2013) & those referred on and off the pathway since March 2014.
Results: At 18 months, 844 patients were managed on the pathway. 245 patients (29.4%) required ELF test (FIB-4 1.30-3.25). Overall, 663 (78.6%) were stratified as <F3 fibrosis, and 181 patients (21.4%) as high risk of ≥F3 fibrosis. To date, hospital data are available for 81 cases. 33 patients are awaiting investigations or have normal LFTs (ineligible). For eligible patients, ≥F3 fibrosis was diagnosed in 24/48 (50%) patients compared to 7/116 (6.0%) non-pathway and 6/85 (7.1%) pre-pathway referrals. For 8/11 (72.7%) cirrhotics detected via the pathway, CLD was not evident from clinical examination, bloods or imaging. To allow direct comparison to pre-pathway, 1 year analysis showed 283% & 250% increases in ≥F3 fibrosis and cirrhosis detection respectively (figure 1).
Conclusions: Early analysis of the C&I NAFLD pathway suggests risk-stratification using FIB-4 & ELF in primary care increases advanced liver disease detection, and reduces referrals of patients with <F3 disease. The pathway displays early promise in addressing an important clinical challenge.
Figure:

ePO
ST
ER
AB
ST
RA
CT
S
180 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Disclosure of Interest: A. Srivastava: : None Declared, R. Gailer: : None Declared, S. Demma: : None Declared, S. Tanwar: : None Declared, A. Warner: : None Declared, D. Suri: : None Declared, S. Morgan: : None Declared, K. Sennett: : None Declared, D. Thorburn: : None Declared, J. Parkes: Sponsored Lectures (National or International): Conflict with: Siemens Healthcare Diagnostics,, E. Tsochatzis: : None Declared, W. Rosenberg: Grant: Conflict with: Siemens Healthcare Diagnostics,, Consultant: Conflict with: Siemens Healthcare Diagnostics,, Sponsored Lectures (National or International): Conflict with: Siemens Healthcare Diagnostics,

ePO
ST
ER
AB
ST
RA
CT
S
181EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 4: YI-MR-145
TOWARDS A NON-INVASIVE DIAGNOSIS OF NON-ALCOHOLIC STEATO HEPATITIS (NASH)
Pablo J. Giraudi1, Sabrina E. Gambaro1, Carla M. Chackelevicius* 1, Michela Giuricin2, Deborah Bonazza3, Fabrizio Zanconati4, Nicolò de Manzini2, Claudio Tiribelli1, 5, Silvia Palmisano2, Natalia Rosso1
1Centro Studi Fegato, Fondazione Italiana Fegato, 2Chirurgia Generale, Università degli Studi di Trieste, Ospedale di Cattinara, 3School of Anatomic Pathology, University of Udine and Trieste; Department of Medical, Surgical and Health Sciences, University of Trieste, 4UCO Anatomia e Istologia Patologica, 5Università degli Studi di Trieste, Clinica Patologie del fegato, Cattinara Teaching Hospital, Trieste, Italy
Corresponding author’s email: [email protected]
Introduction: Nonalcoholic steatohepatitis (NASH) is a common, often “silent”, liver disease. The major feature in NASH is fatty liver, along with inflammation and fibrosis. Liver biopsy, the gold standard for its diagnosis, was established almost a century ago. Surprisingly, reliable non-invasive diagnostic tools have not been developed yet.
Aims: Validate in vivo, proteins identified in silico as biomarkers for NASH diagnosis.
Material and Methods: CD44, SPARC, EGFR and IGF2, were identified by in silico studies as candidate biomarkers for being secreted factors with clinical relevance.A cohort of 45 adult morbid obese consenting patients (BMI> 35 kg/m2; 17 males and 28 females, age range: 19-63) undergoing bariatric surgery was enrolled. Wedge liver biopsy was performed and blood samples were collected. Exclusion criteria were alcohol consumption, viral hepatitis infection, known chronic liver disease. Liver histology was classified by Brunt’s score and patients were divided according to fibrosis stage: F0 (n=3), F1 (n=35), F2 (n=7). Plasmatic concentration of candidate biomarkers was measured by ELISA, at the moment of the surgery (T0) and during the follow-up at 6 and 12 months after bariatric surgery. Lean healthy subjects were used as controls in the follow-up study.
Results: Our cohort of patients showed to have alterations of glucose homeostasis (63.8%); hypercholesterolemia (44%); hypertriglyceridemia (27.6%) and altered transaminases levels (19.1%). As expected, correlation analysis of these parameters with the degree of fibrosis do not provide any predictive value about the hepatic fibrosis stage.Regarding our biomarkers, plasmatic levels of IGF2 correlated inversely with the fibrosis score (p<0.01) while EGFR levels showed a direct correlation with fibrosis stage (p<0.01).

ePO
ST
ER
AB
ST
RA
CT
S
182 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Data at T0, allow to discriminate healthy subjects from subjects with middle stage of fibrosis (scores 1 and 2). During the follow-up, we observed improvement of plasma level of CD44, IGF2 and EGFR, which reached values similar to healthy subjects at 12 months, when; the metabolic pattern also improved.
Conclusions: Our study looks like a promising first step towards the development of future non-invasive diagnostic tools to distinguish even first phases of NASH.
Acknowledgements: U05SPFRA14 – fondi FRA 2014 (CdA dd. 19.12.2014) and FIF. PJG was sponsored by Fondazione Umberto Veronesi (Grants 2015), SEG by Proyecto 297 CTGAS (CUPB91C12000000001) and CMC by MAE
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
183EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 5: YI-MR-151
ANGIOPOIETIN-LIKE4 IS ASSOCIATED WITH LIPID METABOLISM AND SEVERE FIBROSIS IN NON-DIABETIC PATIENTS WITH NON ALCOHOLIC FATTY LIVER DISEASE
Chiara Rosso* 1, Milena Marietti1, Melania Gaggini2, Chiara Saponaro2, Gian Paolo Caviglia1, Fabrizia Carli2, Emma Buzzigoli2, Rami I. K. Jouness1, Maria Lorena Abate1, Antonina Smedile1, Giorgio Maria Saracco3, Amalia Gastaldelli2, Elisabetta Bugianesi1
1Medical Sciences, UNIVERSITY OF TURIN, Torino, 2Cardiometabolic Risk Unit, CNR-Institute of Clinical Physiology, Pisa, 3Department of Oncology, UNIVERSITY OF TURIN, Torino, Italy
Corresponding author’s email: [email protected]
Introduction: Non-alcoholic fatty liver disease (NAFLD) results from an imbalance between lipid deposition and removal, driven by increased lipid flow and de novo lipogenesis (DNL) in insulin resistance (IR). The angiopoietin-like4 (ANGPTL4) is involved in the regulation of lipid metabolism through the inhibition of lipoprotein lipase, leading to systemic hypertriglyceridemia and hepatic steatosis.
Aims: Our aim was to explore the association between ANGPTL4, lipid metabolism, monocyte chemoattractant protein-1 (MCP-1) and liver damage in a well characterized group of non-diabetic NAFLD patients.
Material and Methods: We enrolled 54 subjects, 45 patients with biopsy proven NAFLD and 9 healthy controls (CT). Adipose tissue IR (AT-IR) indices in fasting condition were derived from free fatty acids (FFAs) levels and tracer studies (D2 glycerol): AT-IR1: FFAs x insulin (INS) and AT-IR2: glycerol Ra x INS. Plasma FFAs composition was assessed by GC-MS and the ratio palmitic/linoleic acid (16:0/18:2), which has been associated with DNL, has been calculated. ANGPTL4 and MCP-1 plasma levels were measured by Multiplex Assay based on the Luminex technology. Liver histology was score according to Kleiner.
Results: Plasma levels of ANGPTL4 were similar to CT when NAFLD were analyzed as a whole group, but was 22% higher in obese vs non-obese NAFLD. Overall, ANGPTL4 resulted positively associated with plasma levels of FFAs and triglycerides (r=0.49, p<0.01; r=0.30, p=0.03), liver fat (r=0.40, p<0.01) and lipolysis (r=0.28, p=0.04). Compared to

ePO
ST
ER
AB
ST
RA
CT
S
184 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
CT, NAFLD subjects had increased AT-IR and 16:0/18:2 ratio that were significantly related to ANGPTL4 levels (AT-IR1 r=0.51, p<0.01 and AT-IR2 r=0.37, p=0.04; 16:0/18:2 ratio r=0.32, p=0.02). MCP-1 levels were increased by 40% in NAFLD vs CT and directly related to ANGPTL4 levels (r=0.46, p<0.01). Among histological features, ANGPTL4 was increased by 30% in the presence of inflammation and by 60% in severe fibrosis but was unchanged by degree of ballooning. At regression analysis, ANGPTL4 levels were associated with the degree of fibrosis independent of BMI, ATIR and MCP-1.
Conclusions: ANGPTL4 is significantly associated with alterations in lipid metabolism, AT-IR and severe hepatic fibrosis in non-diabetic subjects with NAFLD.
Funded by:FP7/2007-2013under grant agreement no.HEALTH-F2-2009-241762 for the project FLIP; PRIN2009ARYX4T. Horizon2020under grant agreement no.634413 for the project EPoS.
Disclosure of Interest: None Declared

ePO
ST
ER
AB
ST
RA
CT
S
185EASL Monothematic Conference • Riga, Latvia • 12-14 May, 2016
Screen 6: MR-135
ASSOCIATION BETWEEN SEVERITY OF NONALCOHOLIC FATTY LIVER DISEASE AND THE RATIOS OF CHOLESTEROL AND TRIGLYCERIDES
Chia-Yen Dai* 1, 2, 3, 4, Kuan-Ta Wu1, Jeng-Fu Yang1, Chung-Feng Huang2, Ching-I Huang, 3, Chia-I Lin2, Meng-Hsuan Hsieh1, 4, Jee-Fu Huang3, 4, Wan-Long Chuang3,
4, Ming-Lung Yu2, 3, 4, Hsien-Yi Wang5
1Health Management Center, 2Department of Occupational and Environmental Medicine, 3Hepatobiliary Division, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, 4Faculty of Internal Medicine, College of Medicine, Kaohsiung Medical University , Kaohsiung, 5Department of Nephrology, Chi–Mei Medical Center, Tainan, Taiwan
Corresponding author’s email: [email protected]
Introduction: Nonalcoholic fatty liver disease (NAFLD) is reported to be associated with metabolic parameters. Limited data support the notion that lipid ratios are risk factors for NAFLD.
Aims: The retrospective study aimed to evaluate the association between lipid ratios and NAFLD.
Material and Methods: We have conducted a large population, cross-sectional, retrospective study enrolling 44,767 adults who have received examination in our department for health checkups in our tertiary medical center. The data on blood pressure, fasting glucose, total cholesterol (TC), triglycerides (TG), and high-density lipoprotein cholesterol (HDL-C) levels were obtained. The NAFLD severity (none, mild, moderate and severe) was evaluated by ultrasound examinations done by expert hepatologists. By using multivariate analyses we evaluated the odds between lipid ratios and NAFLD.
Results: Of the enrolled 44,767 subjects (mean age: 43.0±11 years, 28,744 males), the prevalence rate of fatty liver in the present study was 53.76%. The individuals were stratified into four subgroups based on their lipid profiles ratios (TC/HDL-C with a cut-off of 4.0 and TG/HDL-C with a cut-off of 2.0, respectively). In the subgroup with the lowest TC/HDL-C and TG/HDL-C ratios, the prevalence of NAFLD, hypertension, and diabetes was lower than that of the other three subgroups. Patients with higher lipid ratios had a significantly greater risk for advanced NAFLD.

ePO
ST
ER
AB
ST
RA
CT
S
186 Programme & Abstracts • NASH: Beyond the acronym, certainties and clinical dilemmas
Conclusions: The severity of NAFLD was associated with lipid ratios. Adults with high TC/HDL-C or TG/HDL-C ratios, or both, have a greater risk for NAFLD, especially advanced NAFLD
Disclosure of Interest: None Declared

NEW PERSPECTIVES IN HEPATITIS C VIRUS INFECTION - THE ROADMAP FOR CURE23-24 SEPTEMBER 2016 PARIS, FRANCE
Scientific Organising CommitteeThomas Berg, GermanyRaymond Chung, United StatesXavier Forns, SpainNorah Terrault, United States
Co-organised by:
SPONSORSHIP O
PPORTUNITIE
S
specialconfe
rence@
easloffi
ce.eu
REGISTER OR SUBMIT YOUR ABSTRACTS TODAY!
KEY DEADLINE:Abstract submission: 27 June 2016
www.easl.eu
This event has been supported by an unrestricted grant by:
AbbVie Bristol-Myers Squibb Gilead Sciences Europe Ltd.
www.easl.eu/_events
GET NOTIFIED FOR ANY NEWS AND
DEVELOPMENTS
Visit easl.eu for more information
SEE YOU
NEXT YEAR!