nancy pares, rn, msn metro community college. identify pathophysiology and nursing process of...
TRANSCRIPT

NURS 2410 Unit 6 and 7
Nancy Pares, RN, MSNMetro Community College

Identify pathophysiology and nursing process of selected sensory/neurological system alterations inclusive of:◦ Visual, hearing, retinoblastoma (covered in onco
unit), hydrocephalus, cerebral palsy, spina bifida, muscular dystrophies, spinal cord injuries and systemic lupus
Objective 1

Visual disorders◦ Myopia◦ Astigmatism◦ Strabismus◦ Amblyopia
Disorders of Eye

Visual disorders◦ Cataracts◦ Glaucoma◦ Retinoblastoma◦ Color blindness◦ Retinopathy of prematurity (ROP)
Disorders of Eye

Otitis media Otitis externa Hearing impairment
Disorders of Ear

Figure 24-2 Of the three anatomic differences in the eustachian tube between adults and small children (shorter, wider, more horizontal), which do you think could cause more problems for the child and why? Answer: More horizontal. Small children who are bottle fed in a supine position have a greater probability of developing otitis media because the eustachian tube opens when the child sucks and the horizontal angle provides easy access to the middle ear. In older children the greater angle helps keep foreign substances and germs away from the middle ear.
Epistaxis Nasopharyngitis Sinusitis Pharyngitis Tonsillitis
Disorders of Nose and Throat

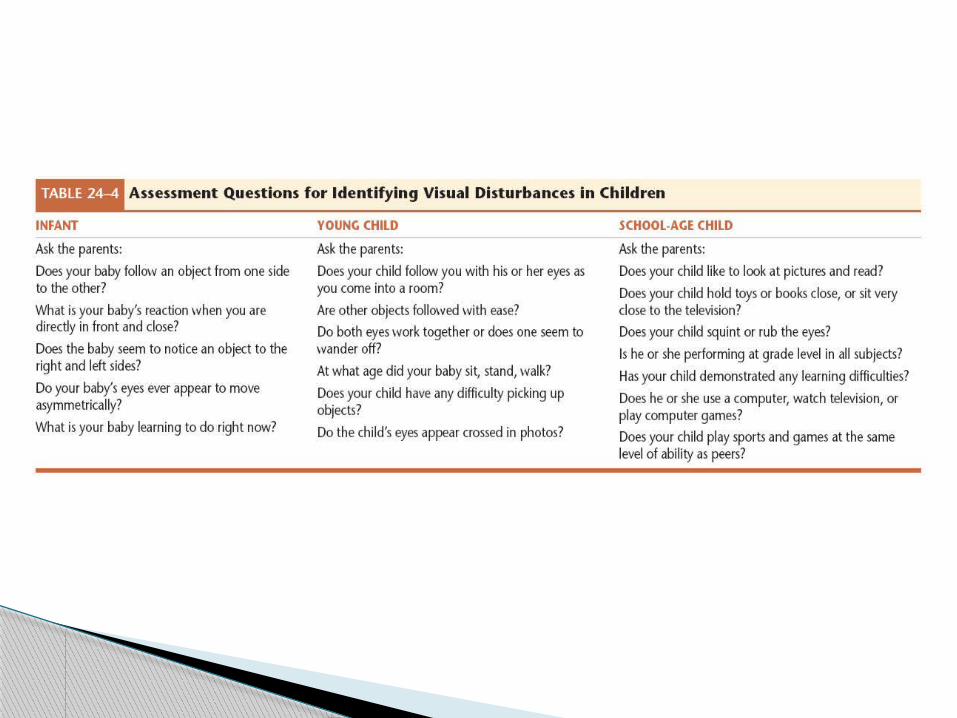
20/20 by age 6 or 7 (visual acuity) Screening starts at well-child exams when
cooperative (screening timing and frequency)
Vision Screening
Infant in hospital◦ Screening timing and frequency◦ Many states mandate
Observation for cues to hearing Clinical manifestations
Hearing Screening

Chronic ear infections Chronic fluid/effusion Follow-up needed for hearing deficit
Risk Factors

Conjunctivitis◦ Bacterial
Antibiotic eye drops◦ Viral and allergic
Supportive care Periorbital cellulitis
◦ Oral or intravenous antibiotics
Abnormalities of Eyes

Other disorders◦ Multiple types of treatments based on etiology
Occlusion therapy Compensatory lenses Surgery Vision therapy
◦ Refer to eye specialist
Abnormalities of Eyes

Otitis media◦ Antibiotic usage◦ Supportive care
Abnormalities of Ears
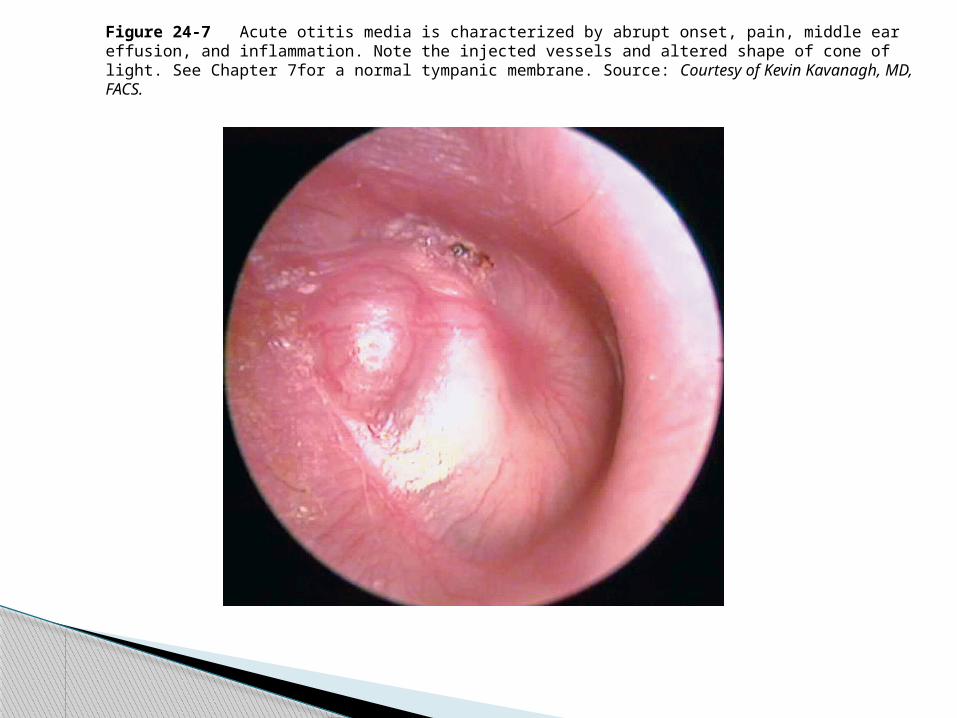
Figure 24-7 Acute otitis media is characterized by abrupt onset, pain, middle ear effusion, and inflammation. Note the injected vessels and altered shape of cone of light. See Chapter 7for a normal tympanic membrane. Source: Courtesy of Kevin Kavanagh, MD, FACS.

Figure 24-8 Otitis media with effusion is noted on otoscopy by fluid line or air bubbles. Pneumatic otoscopy or tympanometry shows a nonmobile tympanic membrane. Note that the light reflex is not in the expected position due to a change in tympanic membrane shape from air bubbles. Where would you expect to see the light reflex? (See Chapter 7 for a description of normal findings.) Source: Courtesy of Kevin Kavanagh, MD, FACS.

Recurrent otitis media or effusion◦ ENT referral for possible tympanostomy tube
placement Otitis externa
◦ Antibiotic ear drops
Abnormalities of Ears

Hearing loss◦ Sensorineural
Cochlear implant
Abnormalities of Ears


Box 24-7 (continued) Cochlear Implants


Collaborative care includes antibiotics if bacterial in etiology◦ Nasopharyngitis◦ Pharyngitis◦ Tonsillitis
Tonsillectomy Criteria for surgery
◦ Sinusitis
Abnormalities of Nose and Throat

Primary intervention is prevention◦ ROP interventions and prevention strategies
Protective eyewear
Eye Abnormalities

Prevention focus◦ Decrease otitis media◦ Increase access to care◦ Increase frequency of hearing screens◦ Reduce noise-induced hearing loss
Ear Abnormalities

Prevention measures Education to prevent communicable
diseases Home care for common communicable
diseases Injury prevention Dental emergencies
◦ Tooth avulsion
Nose, Throat, and Mouth Abnormalities
Avoid triggers Long-term planning for chronic illness Maintain fluid balance Promote adequate and appropriate nutrition
Nursing Management of Systemic Lupus Erythematosus

Promote skin integrity Promote rest and comfort Emotional support Community activities and support groups
Nursing Management of Systemic Lupus Erythematosus

Plan care◦ Age and developmentally appropriate
Medication regimen◦ Education on importance of regimen◦ Education on side effects
Promotion of general health◦ Avoid infectious individuals
Collaborate with Family of a Child with Human Immunodeficiency Virus (HIV)

Promotion of growth and development◦ Proper food◦ Proper atmosphere, toys, friends
Emotional support◦ Caregiver◦ Child
Support groups
Collaborate with Family of a Child with Human Immunodeficiency Virus (HIV)

Increasingly common Children at risk for allergy Testing for latex allergy Latex allergy questionnaire
Latex Allergy


Alternative products Medical-alert ID bracelet Epinephrine kit at home and school Education of caregivers related to
hypersensitivity reactions◦ Preparation to provide care
Nursing Care for Child with Latex Allergy

Type I◦ Definition
Type II◦ Definition
Type III◦ Definition
Type IV◦ Definition
Hypersensitivity Reactions in Children


History Assessment
◦ Type I and Type II carry EpiPen
Nursing Management
Cranial bones are not completely ossified◦ Allows for brain growth
The posterior fontanel closes at 3-4 months The anterior fontanel closes at 18 months Increases risk for brain and spinal cord
injury
Neurological Anatomic Differences in Children

Figure 33-2 The skull and brain grow and develop rapidly during early childhood. Infants and young children are at higher risk for injury to the brain and spinal cord because of developing anatomic structures.

Levels of consciousness—most important indicator of neurological dysfunction
Consciousness—receptiveness to stimuli Alertness—arousal, ability to react Cognitive power—ability to process data
and respond Altered levels of consciousness
◦ Causes
Nursing Assessment of Altered Levels of Consciousness and Other Neurological Conditions

Levels of consciousness assessment◦ Categories: confusion, delirium, lethargy,
obtunded, stupor, and coma◦ Decorticate and decerebrate posturing
Nursing Assessment of Altered Levels of Consciousness and Other Neurological Conditions
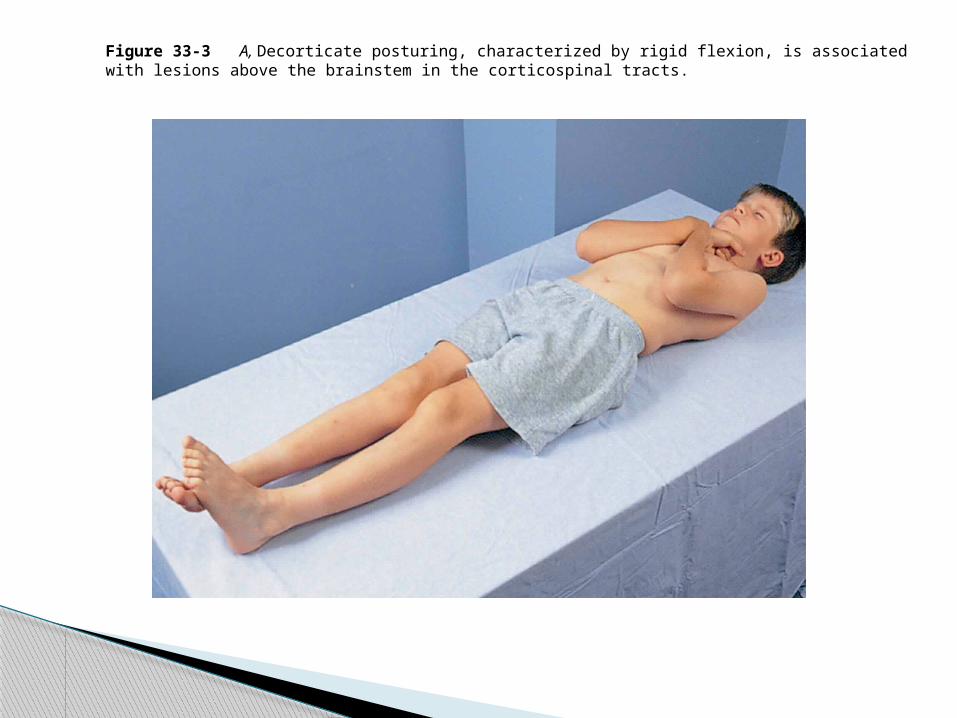
Figure 33-3 A, Decorticate posturing, characterized by rigid flexion, is associated with lesions above the brainstem in the corticospinal tracts.
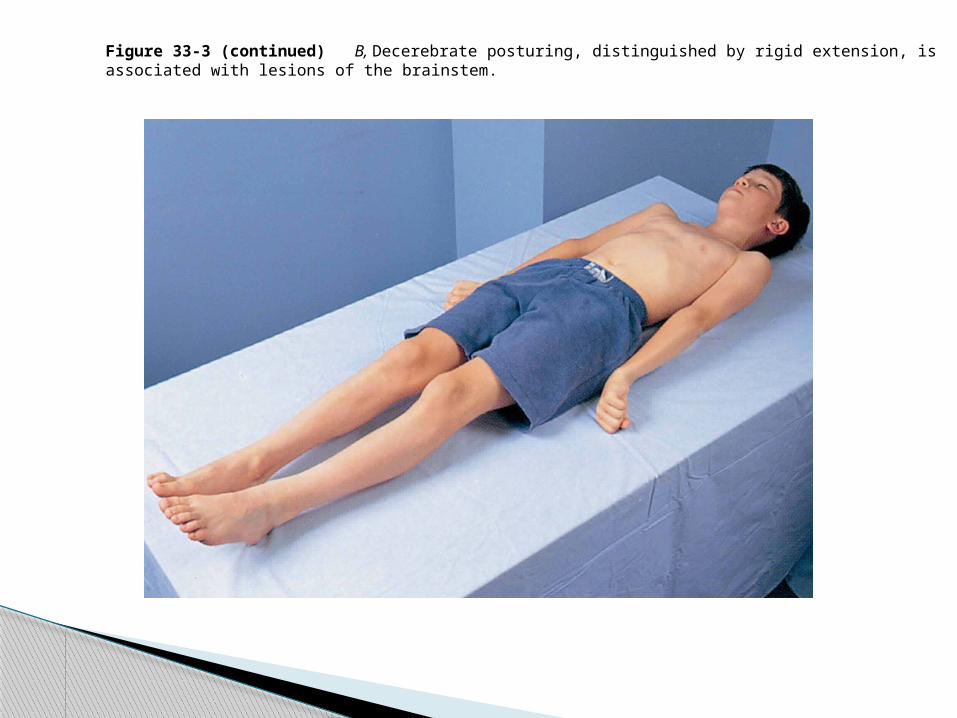
Figure 33-3 (continued) B, Decerebrate posturing, distinguished by rigid extension, is associated with lesions of the brainstem.

Increased intracranial pressure ◦ Scales for responsiveness
Nursing Assessment of Altered Levels of Consciousness and Other Neurological Conditions
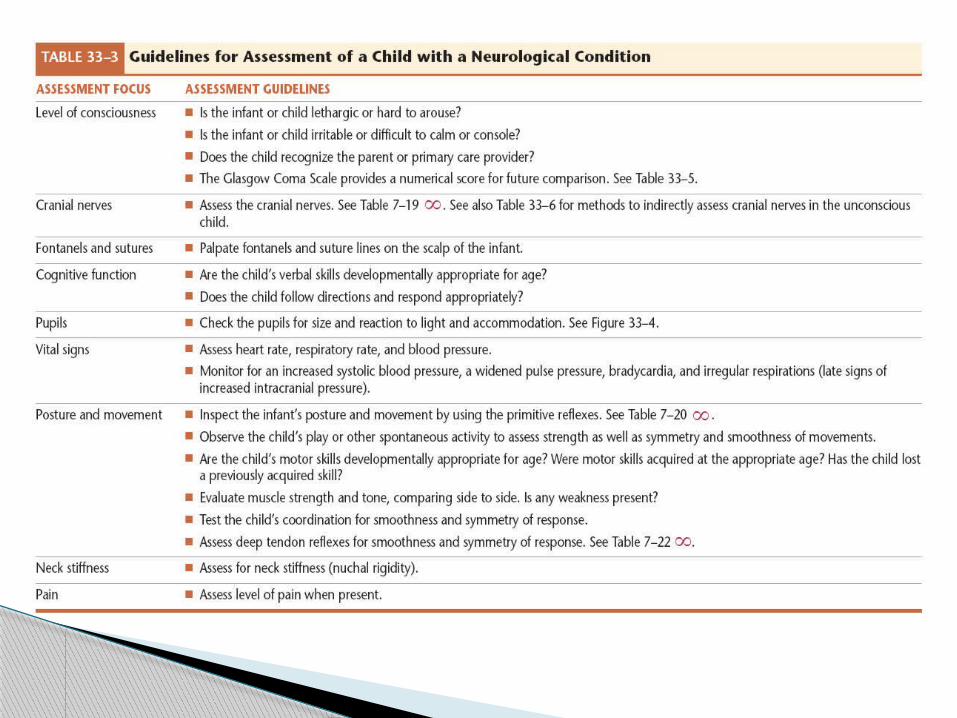


Increased intracranial pressure ◦ Glasgow coma scale
Nursing Assessment of Altered Levels of Consciousness and Other Neurological Conditions

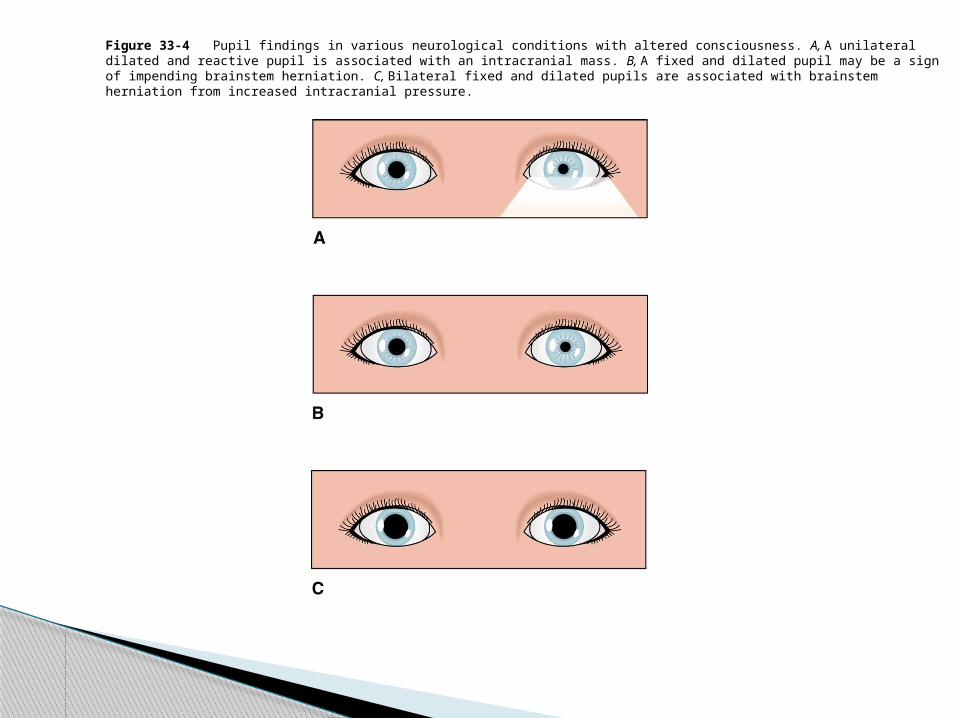
Figure 33-4 Pupil findings in various neurological conditions with altered consciousness. A, A unilateral dilated and reactive pupil is associated with an intracranial mass. B, A fixed and dilated pupil may be a sign of impending brainstem herniation. C, Bilateral fixed and dilated pupils are associated with brainstem herniation from increased intracranial pressure.

An acute seizure that lasts over 30 minutes Electrolytes, glucose, blood gases,
temperature, and blood pressure need monitoring if a seizure occurs for longer than 10 minutes
Status Epilepticus

Maintain airway Ensure safety Administer medications Provide emotional support Provide education
Nursing Management for Seizures

Malformation of the spinal cord and canal Impaired physical mobility related to
neuromuscular impairment Impaired urinary elimination related to
sensory impairment Risk for latex allergy response related to
multiple surgical procedures
Myelodysplasia

Imbalance between production and absorption of CSF
Leads to increased CSF volume in brain Commonly associated with
myelomeningocele (spinal-fluid-filled sac protruding through vertebrae)
Treatment may include placement of a shunt
Hydrocephalus

Risk for infection related to the presence of shunt
Risk for caregiver role strain related to care of a child with a chronic condition
Risk for delayed development related to compression of brain tissue with excess cerebral spinal fluid
Nursing Diagnosis for Myelodysplasia and Hydrocephalus

Group of permanent disorders of movement and posture
Causes activity limitations Nonprogressive in nature May have additional sensory, cognition,
communication and behavior problems
Cerebral Palsy

Community care◦ Case manager◦ Early intervention◦ Financial needs◦ School assistance and IEP needed
Children with Cerebral Palsy

Figure 33-19 A child with cerebral palsy has abnormal muscle tone and lack of physical coordination.

Multidiscipline care◦ Orthopedic surgeon care◦ Speech therapy◦ Regular eye exams◦ Pediatric nurse practitioner or pediatrician◦ Support groups
Children with Cerebral Palsy
Traumatic brain injuries◦ Falls are a major cause◦ Primary vs. secondary◦ Cushing’s triad
Nursing management of mild vs. severe brain injury◦ Emergency care◦ Long-term care
Mild, Moderate, and Severe Brain Injury


Figure 33-20 Child having baclofen pump filled.

Explain the pathophysiology and nursing process of congenital defects of the musculoskeletal system inclusive of:◦ Cranial malformations, club foot,
kyphosis/scoliosis, hip dysplasia, Bone tumors covered in oncology (unit 7)
Objective 2

Child’s bones◦ More porous and pliable◦ Less dense
Infant skull◦ Fontanel closure: 18 months◦ Overall growth completion: 2 years
Child bone growth from epiphyseal plate
Musculoskeletal Differences

Muscles◦ Number same as adult◦ Only length and circumference grow
Ligaments and tendons◦ Stronger than bone until puberty
Musculoskeletal Differences

Figure 35-3 Skeletal and muscle development throughout childhood.

Figure 35-3 (continued) Skeletal and muscle development throughout childhood.

Figure 35-3 (continued) Skeletal and muscle development throughout childhood.

Feet and legs◦ Metatarsus adductus (intoeing)
Structural Deformities

Figure 35-4 Metatarsus adductus is characterized by convexity (curvature) of the lateral border of the foot. The child’s right foot demonstrates the disorder. Note that the forefoot turns inward and appears out of alignment with the remainder of the foot.

Feet and legs◦ Talipes equinovarus (clubfoot)
Structural Deformities

Figure 35-5 Parents of a child with clubfoot will have many questions. Can the condition be treated? Will the child be able to walk normally after surgery? Will they need help caring for the infant? How much will surgery and other care cost? Will any subsequent children have a clubfoot? Source: Modified from Staheli, L. T. (1992). Fundamentals of pediatric orthopedics (p. 5.10). New York: Raven Press.
Feet and legs◦ Genu valgum (knock-knees)◦ Genu varum (bowlegs)
Structural Deformities

Figure 35-8 A, Genu valgum, or knock-knees. Note that the ankles are far apart when the knees are together. B, Genu varum, or bowlegs. The legs are bowed so that the knees are far apart as the child stands.
Hip◦ Dysplasia◦ Legg-Calvé-Perthes◦ Slipped capital femoral epiphysis (SCFE)
Structural Deformities

Figure 35-9 The asymmetry of the gluteal and thigh fat folds is easy to see in this child with developmental dysplasia of the hip.

Figure 35-10 The most common treatment for DDH in a child under 3 months of age is a Pavlik harness. A shirt should be worn under the harness to prevent skin irritation (it was omitted for clarity in this photograph).

Figure 35-13 In slipped capital femoral epiphysis, the femoral head is displaced from the femoral neck at the proximal epiphyseal plate.

Spine◦ Scoliosis, kyphosis, lordosis◦ Torticollis
Structural Deformities

Figure 35-14 A child may have varying degrees of scoliosis. For mild forms, treatment will focus on strengthening and stretching. Moderate forms will require bracing. Severe forms may necessitate surgery and fusion. Clothes that fit at an angle, such as this teenage girl’s shorts, and anatomic asymmetry of the back provide clues for early detection.

Prevent complications of immobility Assist coping with treatment
◦ Support long-term adaptation Facilitate pain control
Deformities: Nursing Care

Bone infection Etiology: idiopathic or nosocomial
◦ Due to trauma, pins Symptoms
◦ Bone pain◦ Edema◦ Joint pain◦ Fever
Osteomyelitis
Skeletal tuberculosis◦ Pain, spasms, muscle atrophy◦ “Doughy” swelling over joints, limited mobility
Septic arthritis◦ Pain, fever, local inflammation, joint tenderness,
loss of spontaneous movement
Rarer Bone Infections
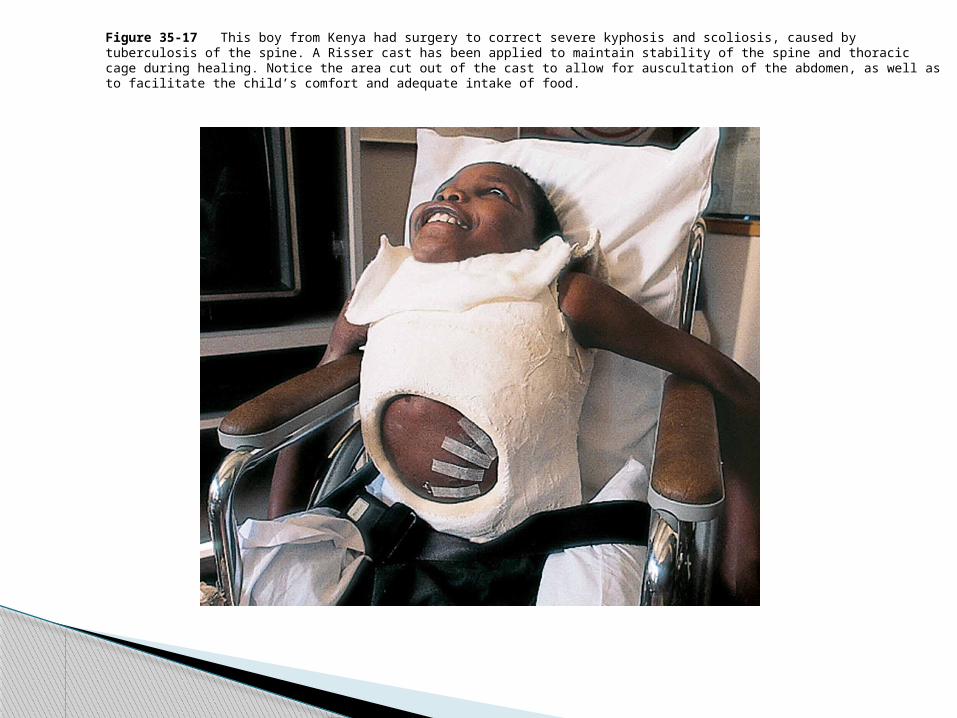
Figure 35-17 This boy from Kenya had surgery to correct severe kyphosis and scoliosis, caused by tuberculosis of the spine. A Risser cast has been applied to maintain stability of the spine and thoracic cage during healing. Notice the area cut out of the cast to allow for auscultation of the abdomen, as well as to facilitate the child’s comfort and adequate intake of food.

Pain relief Maintain joint mobility Prevent deformities Promote self-care Well-balanced diet Hydration Medication management
Nursing Management of Juvenile Arthritis

Achondroplasia◦ Short stature, prominent forehead
Marfan syndrome◦ Connective tissue disorder◦ Skeletal changes◦ Cardiac, respiratory, vision changes
Chronic Conditions

Osteogenesis imperfecta◦ Brittle-bone disease, collagen defect◦ Thin, soft skin; increased flexibility; short
stature;weak muscles; hearing loss
Chronic Conditions

Muscular dystrophies◦ Muscle degeneration and wasting◦ Early signs:weakness and hypotonia◦ Life-threatening
Chronic Conditions

Figure 35-18 Because the leg muscles of children with muscular dystrophy are weak, they must perform the Gowers maneuver to raise to a standing position. A and B, The child first maneuvers to a position supported by arms and legs.

Figure 35-18 (continued) Because the leg muscles of children with muscular dystrophy are weak, they must perform the Gowers maneuver to raise to a standing position. A and B, The child first maneuvers to a position supported by arms and legs.

Figure 35-18 (continued) Because the leg muscles of children with muscular dystrophy are weak, they must perform the Gowers maneuver to raise to a standing position. C, The child next pushes off the floor and rests one hand on the knee.

Figure 35-18 (continued) Because the leg muscles of children with muscular dystrophy are weak, they must perform the Gowers maneuver to raise to a standing position. D and E, The child then pushes himself upright.

Figure 35-18 (continued) Because the leg muscles of children with muscular dystrophy are weak, they must perform the Gowers maneuver to raise to a standing position. D and E, The child then pushes himself upright.

Figure 35-19 This young boy with muscular dystrophy needs to receive tube feedings and home nursing care. He attends school when possible and is able to use an adapted computer.

Limit movement◦ Snug but do not impair circulation◦ No direct contact with skin◦ Assess neurovascular and skin status
Braces
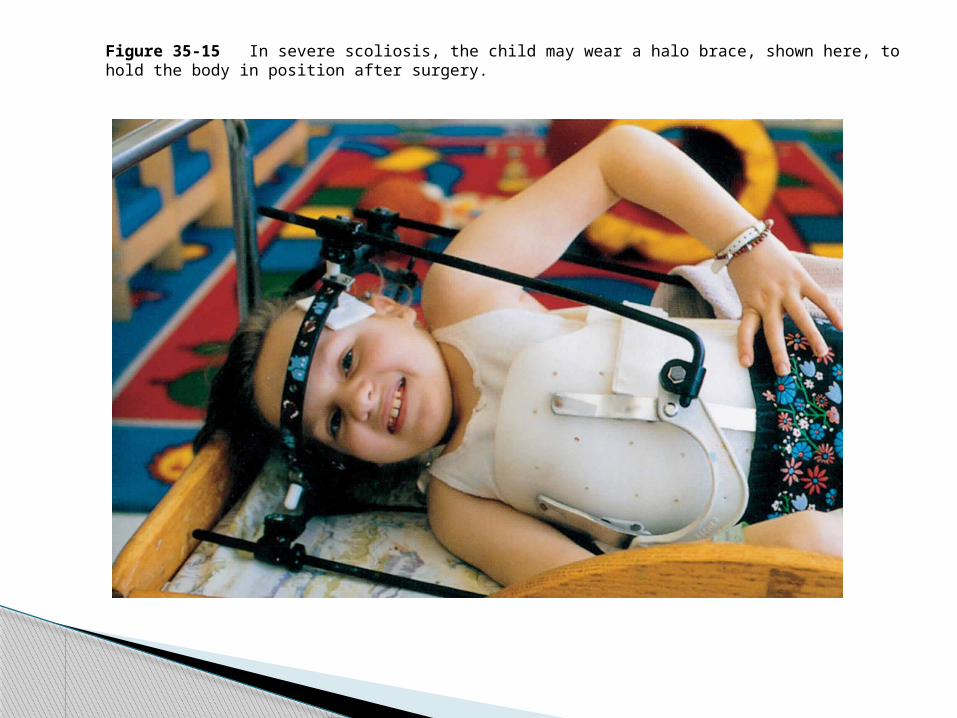
Figure 35-15 In severe scoliosis, the child may wear a halo brace, shown here, to hold the body in position after surgery.

Figure 35-12 Although the Toronto brace used for treatment of Legg-Calvé-Perthes disease may seem formidable for a child to wear, you can see by this photograph that, as usual, children adapt quite well to it.

Prevention◦ Greater risk for children◦ Teach use of protective equipment, safe play
Types◦ Closed
Casting◦ Open
Surgery and casting
Fractures (review)

Describe pathophysiology and nursing process of inflammatory diseases of childhood◦ Meningitis, Reyes syndrome, tetanus, Kawasaki
disease
Objective 3

An inflammation of the meninges covering the brain and spinal cord
Caused by either viral or bacterial agents
Meningitis

Acute inflammation of the brain Symptoms include nuchal rigidity or
positive Kernig or Brudzinski Symptoms depend on the causative
organism
Encephalitis

Discuss the psychopathology and nursing process of alterations in the psycho-social functions of the childrearing period◦ Learning disabilities◦ ADHD◦ Mental health
Objective 4

Developmental and behavioral disorders◦ Pervasive developmental disorders◦ Nursing management
Stabilize environmental stimuli Provide supportive care Enhance communication Maintain a safe environment Provide anticipatory guidance
Nursing Management of Children and Adolescents with Mental Health Disorders
Attention deficit disorder (ADD) and attention deficit hyperactivity disorder (ADHD)◦ Nursing management
Administer medication Minimize environmental distractions Implement behavior management plans Provide emotional support Promote self-esteem
Nursing Management of Children and Adolescents with Mental Health Disorders

Attention deficit disorder (ADD) and attention deficit hyperactivity disorder (ADHD)◦ School issues
Nursing Management of Children and Adolescents with Mental Health Disorders

Suicide◦ Nursing management:
Safety 24-hour monitoring Medication Care in community
Nursing Management of Children and Adolescents with Mental Health Disorders

Effects up to 5 of school children Children do not process information
correctly
Learning Disabilities

Individual education plan (IEP)◦ Developed through an interdisciplinary approach◦ Specific goals are included
Learning Disabilities



Limitations in adaptive and intellectual functioning
Conditions associated:◦ Down syndrome◦ Fragile X syndrome◦ Fetal alcohol syndrome
Mental Retardation

Nursing management◦ Maintain safe environment◦ Provide assistance with adaptive functioning
Mental Retardation

Evaluation depends on needs and developmental level
First evaluation needs to assess the family’s understanding of the disorder
Mental Retardation

Discuss pathophysiology and nursing process associated with blood dyscrasias inclusive of:◦ Sickle cell anemia, iron deficiency anemia, von
willenbrand disease, thalassemias Objective 2
◦ Describe nursing process and procedure for pediatric blood transfusions (covered in NURS 2520)
Unit 7- Objective 1
Iron deficiency anemia◦ Lack of iron◦ Anemia of prematurity◦ Affects production of RBCs◦ RBCs appear hypochromic, decreased hemoglobin
synthesis
Anemia

Iron deficiency anemia◦ Manifestations based on severity
Pallor Fatigue Irritability Pica
Anemia

Normocytic anemia◦ Decreased number of RBCs◦ Normal size with pale center◦ Associated with multiple causes◦ Manifestations similar to iron deficiency anemia
Anemia

Sickle-cell anemia◦ Genetic mutation◦ Hemoglobin S replaces normal hemoglobin◦ RBCs lose doughnut shape, become sickleshaped
Anemia

Figure 28-4 Many of these red blood cells show an elongated crescent shape characteristic of sickle cell anemia.Source: Courtesy of Dr. Ed Wong, Laboratory Medicine, Children’s National Medical Center, Washington, DC.

Sickle-cell anemia◦ Manifestations appear in multiple body systems◦ Severity based on pathologic changes
Anemia

Figure 28-5 The etiology, pathophysiology, and disease process of sickle cell anemia.

Thalassemias◦ Groups of hereditary disorders◦ Hemoglobin synthesis abnormal◦ Range from mild to severe◦ Three types
Anemia

Thalassemias◦ Clinical manifestations based on type and severity
Pallor Fatigue Failure to thrive
◦ Severe anemia leads to chronic hypoxia
Anemia

Hereditary spherocytosis◦ Congenital hemolytic anemia◦ No abnormality of hemoglobin◦ Cells have unusual structure◦ Manifestations appear in neonatal period or
infancy◦ Severity varies
Anemia

Goals of Care◦ Adequate nutrition◦ Hydration and fluid balance◦ Promotion of adequate tissue perfusion◦ Promotion of growth and development◦ Family and patient education
Anemia

Failure of bone marrow to produce blood cells
Disorder is idiopathic or acquired Clinical presentation varies depending on
degree Most common is bleeding secondary to
thrombocytopenia
Aplastic Anemia

Hereditary bleeding disorder X-linked—expressed in males, females have
carrier status
Hemophilia

Manifestations range from mild to moderate to severe◦ Spontaneous bleeding◦ Hemarthrosis◦ Deep tissue hemorrhage◦ Nosebleeds◦ Hematuria◦ Easy bruising
Hemophilia

Autosomal dominant trait Equal expressivity in males and females Manifestations
◦ Easy bruising◦ Epistaxis
von Willebrand Disease

Disseminated intravascular coagulation (DIC)◦ Complication from another illness◦ Most common following infection in children◦ Manifestation range
Minor oozing Frank hemorrhage
Bleeding Disorders: Clotting Disorders

Idiopathic thrombocytopenic purpura (ITP)◦ Autoimmune disorder◦ After a viral illness
Bleeding Disorders: Clotting Disorders

Idiopathic thrombocytopenic purpura (ITP)◦ Manifestations
Ecchymoses Petechiae Purpura Bleeding from gums Nosebleeds Blood in urine Blood in stools
Bleeding Disorders: Clotting Disorders

HSP◦ Vasculitis
Raised purpuric lesions Joint pain Colicky abdominal pain GI bleeding Renal involvement
Bleeding Disorders: Clotting Disorders

RBCs◦ Oxygenation◦ Circulation◦ Fluid◦ Nutrition◦ Pain management
Nursing Care of a Child with a Hematologic Disorder Is Based on the Disorder

WBCs◦ Infection◦ Oxygenation◦ Nutrition
Nursing Care of a Child with a Hematologic Disorder Is Based on the Disorder

Platelets and bleeding disorders◦ Bleeding◦ Oxygenation◦ Circulation◦ Injury prevention
Nursing Care of a Child with a Hematologic Disorder Is Based on the Disorder

Team approach Family involved
◦ Decisions with family and child
Collaborative Care Approach for a Child with a Hematologic Disorder

Discuss the pathophysiology and nursing process of pediatric oncology◦ Leukemia, Hodgkins disease, Wilm’s tumor
Objective 3

Therapy may be singular or combination of treatments◦ Surgery◦ Chemotherapy◦ Radiation◦ Biotherapy◦ HSCT◦ Complementary therapies◦ Palliative care
Clinical Therapy

Based on type of cancer and therapy◦ Infection control◦ Pain◦ Nutrition◦ Growth and development◦ Emotional needs◦ Spiritual needs
Nursing Care Plan

Metabolic◦ Tumor lysis syndrome◦ Septic shock◦ Hypercalcemia
Hematologic◦ Caused by bone marrow suppression◦ Require transfusion and careful RBC and WBC
assessment
Three Types of Oncological Emergencies

Space-occupying lesions: tumors with extensive growth◦ Spinal cord compression◦ Increased ICP◦ Brain herniation◦ Seizures
Three Types of Oncological Emergencies

Space-occupying lesions: tumors with extensive growth◦ Hepatomegaly◦ Gastrointestinal obstruction◦ Cardiac and respiratory complications◦ SVC syndrome
Three Types of Oncological Emergencies

Brain and central nervous system◦ Most common malignancy in children, next to
leukemia◦ Treatment depends on type and location of tumor◦ Surgery◦ Radiation◦ Chemotherapy
Solid Tumors

Figure 29-13 Approximately 1,700 children under the age of 14 years are diagnosed annually as having tumors of the brain and central nervous system. The four most common brain tumors in children are medulloblastoma, cerebral astrocytoma, ependymoma, and brainstem glioma.
Neuroblastoma◦ Definition◦ Treatment based on protocol
Surgical Chemotherapy Radiation HSCT
Solid Tumors


Wilms’ tumor◦ Define◦ Treatment based on stage
Requires surgical removal Radiation Chemotherapy
Solid Tumors


Table 29-8 (continued) National Wilms Tumor Study Staging System
Bone tumors (osteosarcomas)◦ Definition◦ Treatment
Surgery required Chemotherapy Radiation
Ewing’s sarcoma◦ Similar to osteosarcoma
Solid Tumors

Most commonly diagnosed malignancy in children under 14
Definition
Leukemia

Difficult due to multisystem effect Long period of treatment required Assessment complete and thorough
◦ Observe for signs of bleeding◦ Observe for signs of infection
Nursing Management

Monitor for toxic side effects of chemotherapy or tumor cell lysis◦ Renal function◦ Special attention for children on
cyclophosphamide
Nursing Management

Nutrition CNS infiltration Pain Bone marrow suppression
◦ Isolation and transmission precautions
Nursing Management

Education of family and child◦ Careful handwashing◦ Prevention of spread of infection◦ Oral care
Nursing Management

Hodgkin’s disease◦ Definition◦ Treatment based on staging
Outpatient setting Chemotherapy
Soft Tissue Tumors

Figure 29-16 Lymph nodes and organs affected in Hodgkin disease in children.
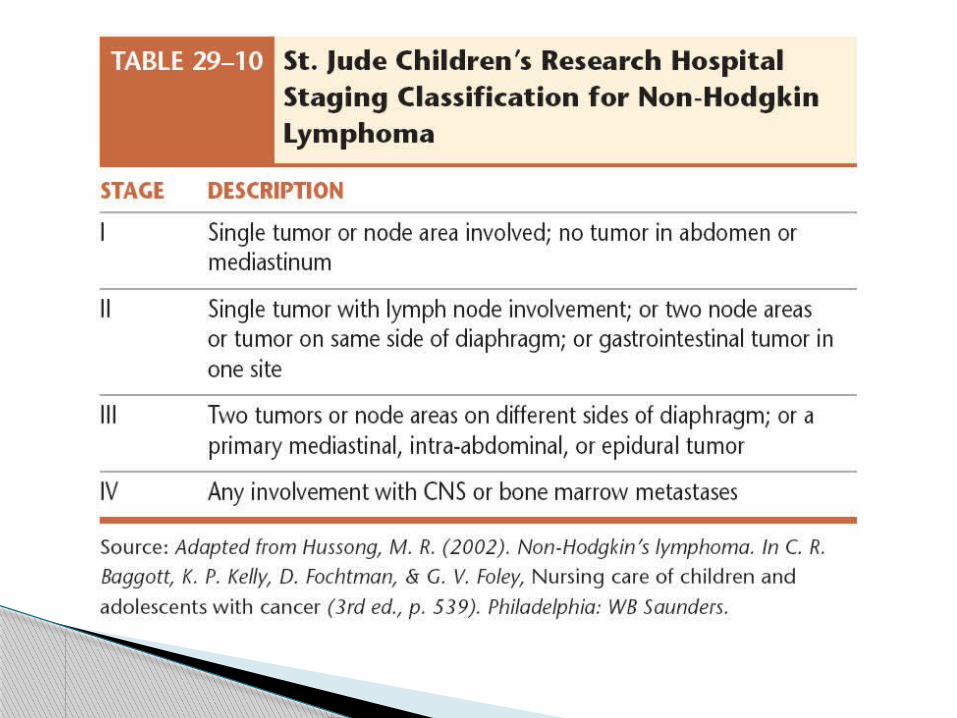
Non-Hodgkin lymphoma◦ Definition◦ Three types◦ Treatment tailored to stage
Stages I and II treat with drugs Stages III and IV treat with additional drugs and
longer period
Soft Tissue Tumors
Rhabdomyosarcoma◦ Definition◦ Locations◦ Treatment
Surgical when possible Widefield radiation Chemotherapy
Soft Tissue Tumors

Figure 29-17 Rhabdomyosarcoma is characterized by ptosis and swelling. Source: From Vaughn, D., Asbury, T., & Riordan-Eva, P. (1995). General opthalmology (14th ed.). Norwalk, CT: Appleton & Lange.
Retinoblastoma◦ Definition◦ Treatment
Radiation almost always used Chemotherapy sometimes used, but often ineffective Removal of eye if other treatment fails
Soft Tissue Tumors
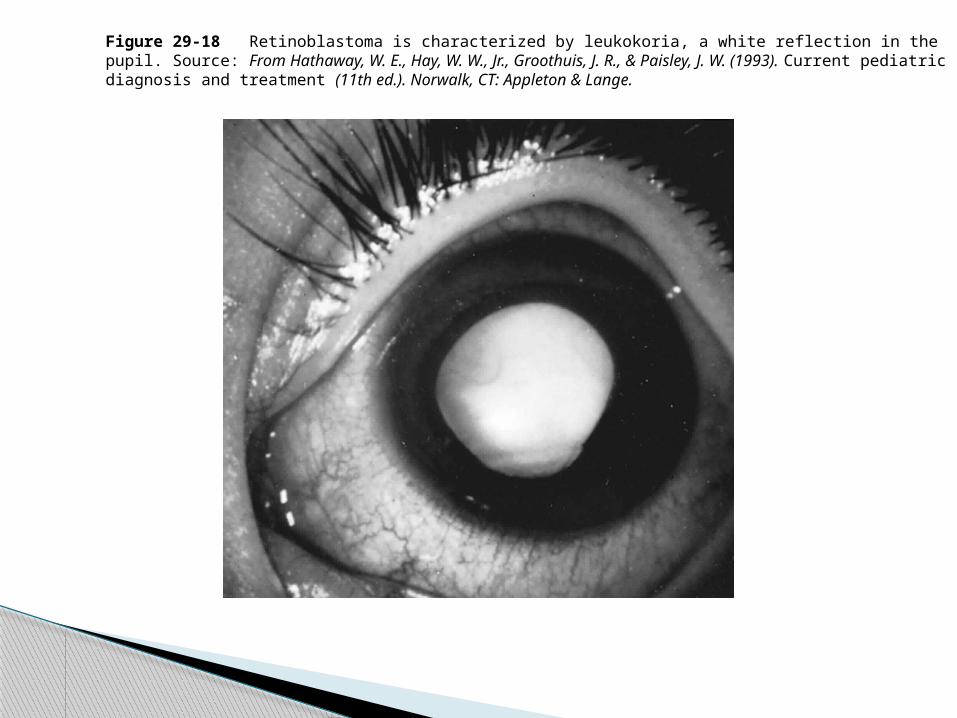
Figure 29-18 Retinoblastoma is characterized by leukokoria, a white reflection in the pupil. Source: From Hathaway, W. E., Hay, W. W., Jr., Groothuis, J. R., & Paisley, J. W. (1993). Current pediatric diagnosis and treatment (11th ed.). Norwalk, CT: Appleton & Lange.

Similar to other cancers Physiologic assessment Psychosocial assessment Collaboration with family Collaboration with medical team Intervention based on assessment and side
effects of therapy
Nursing Management

Cancer affects all areas of function Effects of therapy
◦ Surgery External and internal body changes
◦ Radiation Long-term effects Growth Secondary cancers
Psychological and Physiological Problems of Cancer Survival

Effects of therapy◦ Chemotherapy
Effects immediate May present years later
Psychological and Physiological Problems of Cancer Survival

Long-term planning◦ Family stressors
Questions regarding outcomes Financial concerns
◦ Frequent follow-up Physical Physiological Developmental Cognitive Interventions started as soon as deficit noted
Psychological and Physiological Problems of Cancer Survival

Team members◦ Nurses◦ Primary and specialty care providers◦ Social workers◦ Case managers◦ Child life therapist◦ Psychologist
Collaboration to Provide Family-Centered Care

For the school-age child◦ Encourage maintenance of learning◦ Involvement of school appropriate with
permission Spiritual and emotional needs
◦ Encourage participation in support groups
Collaboration to Provide Family-Centered Care

Treatment for disorders unresponsive to other therapy
Pretransplant phase◦ Total body irradiation◦ Strict isolation
Transplant phase◦ Intravenous transfusion of donor stem cells◦ Transplant starts to grow in 2 to 4 weeks
Hematopoietic Stem Cell Transplant (HSCT)

Posttransplant phase◦ Lasts several weeks◦ Major risk is infection◦ Immunosuppressive agents prevent graftversus-
host disease
Hematopoietic Stem Cell Transplant (HSCT)

Nursing care◦ Prevent infections◦ Injury prevention◦ Growth and development◦ Nutrition◦ Physical activity limits◦ Oral health◦ Mental and spiritual health◦ Family and social relationships
Hematopoietic Stem Cell Transplant (HSCT)