myths in emergency medicine. aim mythology common myths evidence based practice
TRANSCRIPT

MYTHS IN EMERGENCY MEDICINE

AIM
• Mythology
• Common myths
• Evidence based practice

Mythology
• Shared stories that arise and last for generations– Oral initially, then written down
• Respond to profound communal needs– Power relations (gods – men, father – son)
• Plato and others deployed mythos to support their abstract logos
• First physician (Asklepios) mythological son of Apollo

Medical Myths
• Same communal need based– Specialist - generalist
• Based on authoritarian dictates– In the absence of, or contrary to, evidence

Selected EM Myths
1. Analgesia should be withheld in acute abdominal pain, pending assessment
2. A digital rectal exam should be used in assessment of suspected appendicitis
3. The Trendelenberg position improves circulation in shocked patients
4. Atropine should be used before scoline in paediatric intubations

Analgesia should be withheld in acute abdominal pain, pending assessment
JUSTIFICATION
• In order to diagnose acute abdomen successfully, all clinical signs must be present in their unaltered state
• From early 20th century
• Cope’s Early Diagnosis of the Acute Abdomen claimed administration of analgesia would delay diagnosis and result in increased morbidity / mortality

The evidence• 2 of 17 papers since 1997• Wolfe, J.M., et al, Am J Emerg Med 22(4):280, July 2004
– DB crossover RCT.
– Morphine / NS, or NS / Morphine.
– Before and after evaluated by a surgeon & EP, each documenting the presence or absence of six physical signs.
– Morphine median decrease in pain 20mm, 0mm with placebo.
– No change in six physical findings (rebound, right lower quadrant tenderness, guarding, referred pain, cough pain or position pain)
– Overall physical examination changed in 3 of 21 patients after morphine, and 3 of 23 after placebo.
• Green, R., et al, Pediatrics 116(4):978. DB,PC,RCT. – Administration of morphine did not reduce the diagnostic confidence of either EPs
or surgeons. – EP diagnosis 69% morphine group, 66% controls prior to administration, 70% vs.
71% post-administration. – Surgeon expressed confidence in the diagnosis for 74% of patients in both groups.

Bottom Line
• There is good evidence that the early ED use of IV morphine reduces acute abdominal pain, without obscuring the diagnosis or changing the treatment.

A digital rectal exam should be used in assessment of suspected appendicitis
JUSTIFICATION
• Rectal examination will be tender in the presence of an inflamed appendix, allowing diagnosis to be made
The evidence• Over 20 papers since 1979• Bonello, J.C., et al, Dis Col & Rect 22(2):97
– DRE in patients subsequently undergoing surgery for presumed appx. n= 495 patients, DRE positive 46% of proven appx. Not appx, 53% positive rectal exams.
– Results of rectal exam do not confirm or rule out the diagnosis of acute appendicitis • Dixon, J.M., et al, Br Med J 302(6773):386, 1991
– 1,204 patients main complaint RLQ pain. DRE in 85%. – Nonspecific abdominal pain (38%) acute appendicitis (37%). – All of the patients with appendicitis with rectal tenderness also had positive findings on
abdominal examination– DRE did not provide additional diagnostic information if rebound tenderness was evaluated. – DRE made no difference to management plan for any patient.
• Manimaran, N., et al, Ann Roy Coll Surg Engl 86:292, July 2004 – Routine DRE has largely been abandoned in the pediatric population but continues to be
commonly performed in adults. – Contribution of the DRE to the management of 100 patients with acute abdominal pain. Also
assessed patients' perceptions concerning the DRE. – 67% lower abdominal pain. DRE pelvic tenderness in 3, unremarkable in 97. In no case did
DRE results prompt a change in the initial diagnosis or management. 78% examination was uncomfortable 19% painful.
– Do not support routine performance of a DRE for all adults presenting with acute abdominal pain

Bottom line
• PR should not form part of the routine examination of RLQ pain: it is uncomfortable, and poorly tolerated.
• It has a place when alternative diagnoses are likely.
• Should be considered an investigation, not examination

The Trendelenberg position improves circulation in shocked patients
JUSTIFICATION
• Feet up, head down.
• WWI, Walter Cannon suggested use of this for shock treatment.
• Increase VR to heart, CO and organ perfusion.
• 10 years later, Cannon retracted his support, but no one noticed….

The evidence• Taylor Surg Gynae Obstec 1967;124:1005-10
– Shocked vs controls. In 88%, SBP, DBP, MAP all reduced. Lung volumes reduced.
• Bivins, H.G., et al, Ann Emerg Med 14(7):641 – RBC radionuclide scanning to determine the effect of the
Trendelenburg position on blood volume distribution in ten healthy adult males.
– At baseline, 46% of total blood volume was located in the upper body compartment
– Blood volume in the upper compartment increased by a median of only 1.8% (range, -1.3% to +/- 4.7%)
• Sibbald, W.J., et al, Critical Care Med 7(5):218– Swan-Ganz measurements in 76 critically ill patients.– Failed to document any consistent beneficial or detrimental
effect of the Trendelenburg position

Bottom line
• Trendlenberg position does not help improve outcome of treatment of shock
• May be detrimental on lung volumes and BP
Atropine should be used before scoline in paediatric intubations
JUSTIFICATION
• Atropine will reduce the risk of bradycardia and asystole induced by laryngoscopy or scoline.
• Studies in the OR with multiple doses of scoline suggest bradycardia common.
The evidence• Mcauliffe Can J Anaes 1995;42:724-9
– Halothane and succinylcholine anesthesia. No atropine more bradycardia, but episodes resolved spontaneously and without sequelae.
• Mirakhur Anaesthesia 1978;33:906-12– 23 of 25 atropine-treated children experienced persistent
tachycardia. • Parnis Anaesth intensive care 1994;22:61-5
– Surveys of anaesthetists in Australia. Most do not routinely premedicate children with atropine but reserve its use for repeated doses of succinylcholine.
• Fleming CJEM 2005;7:114-8– Bradycardia induced by hiccups and defecation resolves
spontaneously and is not routinely treated with atropine.

Bottom line
• There is no evidence to support the use of atropine before emergency intubation of children, using single dose scoline.
• It may be harmful: ventricular arrhythmias, loss of protective reflexes and masking of hypoxia related bradycardia.

Why do myths persist?
• Lack of time to keep up to date with evidence– In EM alone, 800 new English articles a
month
• Textbooks– How to update?
• Teaching styles

ABM

EBM
• Evidence-based medicine is the conscientious, explicit and judicious use of current best evidence in making decisions about the care of individual patients." – CEBM

How can we use EBM?
• Reading journals• Medline searches
– Both time consuming, not real time
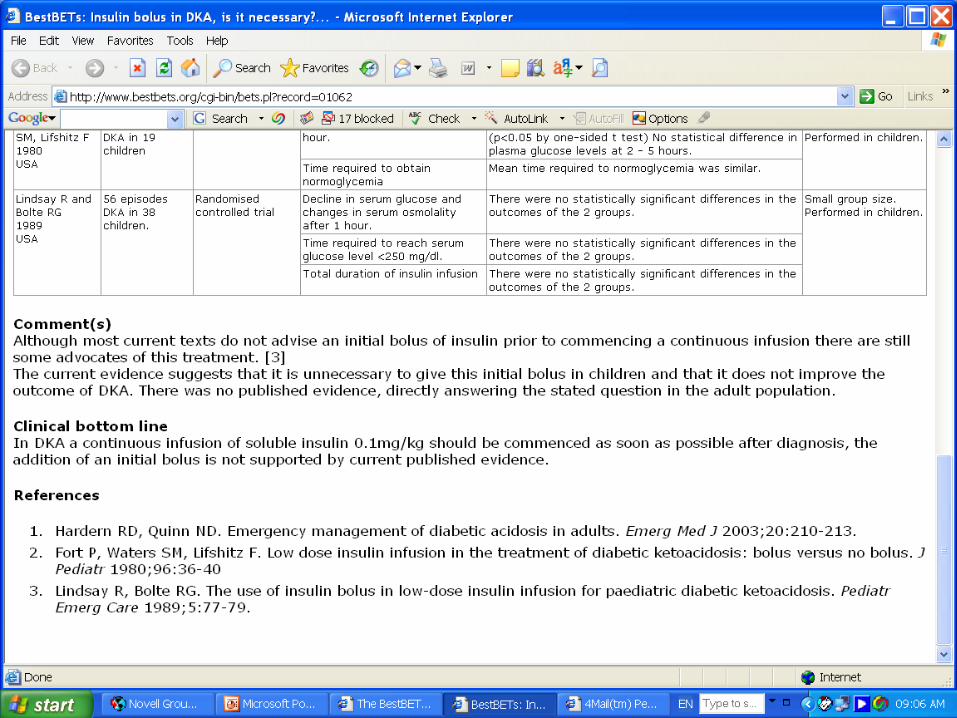
• Look up other people’s work– Critical appraisal topics (CATS)– Best evidence reviews (BETS)– Websites
• ebm.bmjjournals.com• www.acpjc.org• www.cebm.net• www.ccme.org• www.bestbets.org













Decision making in EM

• The likelihood that something will happen can be plausibly estimated by how often it has happened in the past

Applying Bayesian thinking
• What is the likelihood that your patient has the disease in question?– Scores
• e.g. Wells’ score for DVT• Low (2%), intermediate (15%), high (35%)
• Apply a test appropriately– e.g. D Dimer
• Won’t help intermediate group
• What is the new likelihood?– Low with negative test – almost 0
– High with positive test – very likely
What does this mean?
• In EM, we gamble– Make assumptions about the likelihood of the
presence of a condition– Apply a test– Increase or decrease that likelihood
• Can never say for 100%
• Be comfortable with your degree of uncertainty…