myocardium, heartbeat and cardiac output
DESCRIPTION
Myocardium, heartbeat and cardiac output. Chapter 12 pages 361 - 367, 372 - 375. Myocardium (cardiac muscle). Heart is myocardium lined with endothelial cells facing blood Myocardium combines properties of skeletal and smooth muscle - PowerPoint PPT PresentationTRANSCRIPT

Myocardium, heartbeat and cardiac output
Chapter 12
pages 361 - 367, 372 - 375

Myocardium (cardiac muscle)
Heart is myocardium lined with endothelial cells facing blood Myocardium combines properties of skeletal and smooth
muscle Same sarcomere structure as skeletal muscle with light and
dark bands Fibers are shorter and have more branching when compared to
skeletal muscle fibers
Excitation-contraction coupling is regulated by troponin and tropomyosin as in skeletal muscle Smooth muscle myosin needs Ca2+-calmodulin complex to hydrolyze
ATP
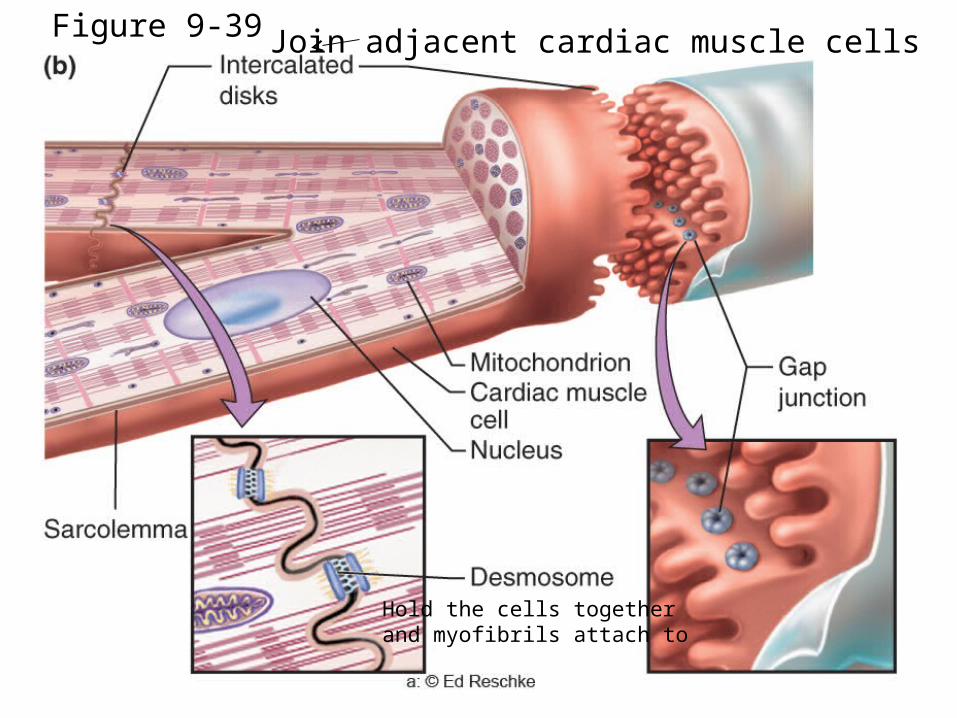
Join adjacent cardiac muscle cells
Hold the cells togetherand myofibrils attach to
Figure 9-39

Myocardium (cardiac muscle)
Electrical conduction is similar to smooth muscle No external innervation, neuromuscular junction, or
ligand-gated AChRs required as in skeletal muscle Some myocardial fibers undergo spontaneous
pacemaker activity without external input Many fibers are connected via gap junctions like
smooth muscle to conduct pacemaker potentials
Myocardium (cardiac muscle)
Spontaneous activity and other contractile machinery modulated by hormones and neurotransmitters to alter cardiac output
Epinephrine/norepinephrine – adrenergic receptors (GPCRs)
Acetylcholine – muscarinic AChRs (GPCRs) Nicotinic AChRs are ligand-gated ion channels in
neuromuscular junction

Which of the following are found in both cardiac and skeletal muscle fibers?
1 2 3 4 5
20% 20% 20%20%20%1. Gap junctions
2. Sarcomeres
3. Nicotinic AChRs
4. Muscarinic AChRs
5. -adrenergic receptors

Electrical conduction in heart
Heart contains non-contractile myocardium for heartbeat coordination Approximately 1% of myocardial fibers are non-contractile
Extensively connected by gap junctions Remember that depolarization of one cell can be rapidly
transmitted to a second cell via ion flow through gap junction channels
Spread wave of electrical excitation and coordinate contraction of contractile myocardium
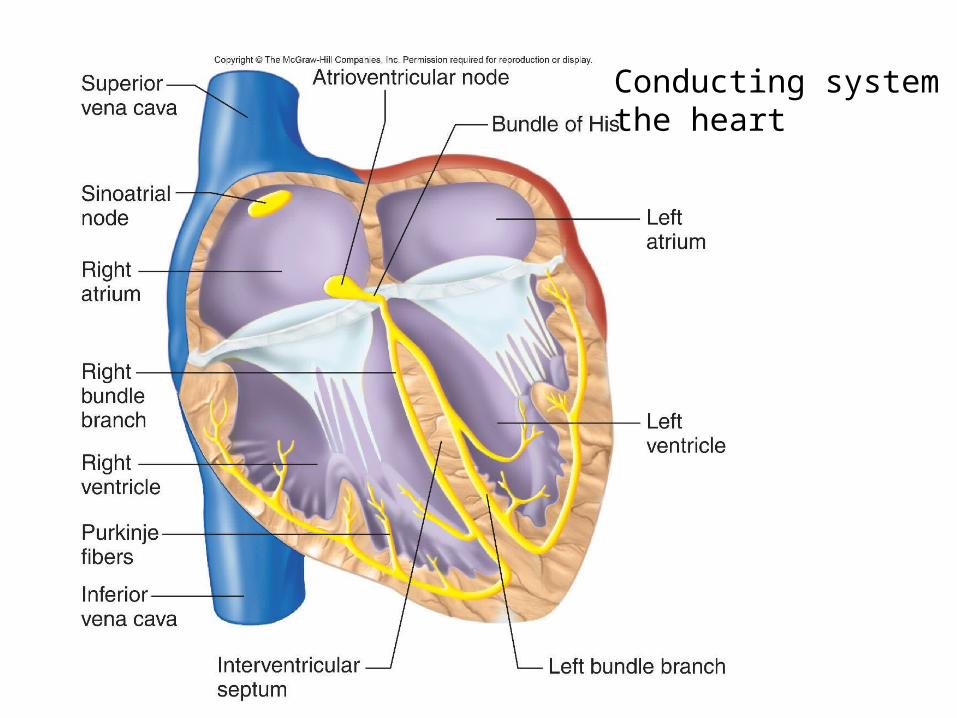
Conducting system ofthe heart

P atria contractQRS ventricles contract
T ventriclesrepolarize
Sequence of cardiac excitation
Pacemaker potentials and myocardial excitability
Spontaneous APs in SA node do not require external depolarization
Peripheral nerves and skeletal muscle require synaptic transmission and EPSPs
SA node will spontaneously depolarize at rest without external excitation
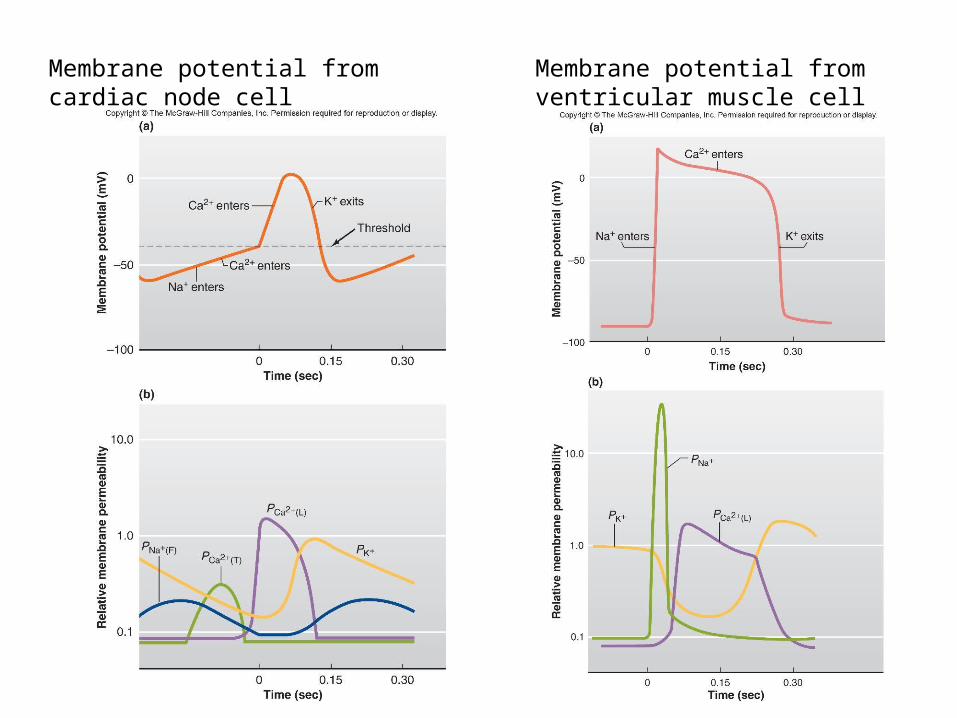
Membrane potential fromcardiac node cell
Membrane potential fromventricular muscle cell

Pacemaker potentials and myocardial excitability
Unlike SA node, APs in contractile myocardium still require external source of depolarization
This external depolarization is provided by gap junctions
APs in contractile myocardium have much longer duration than skeletal muscle and peripheral nerves
Long AP functions to produced sustained contraction instead of a twitch

Excitation-contraction coupling
Some differences between cardiac and skeletal muscle excitation-contraction coupling
External Ca2+ required Larger fraction of cytosolic Ca2+ comes from
VGCCs (voltage gated calcium channels) that remain open during plateau AP

Excitation-contraction coupling
SR does not encircle cardiac A-M filament bundles Not all A-M filaments available for cycling during
cardiac AP Strength of contraction modulated by increasing
Ca2+ not by tetanus or recruiting fibers Longer refractory period of cardiac muscle
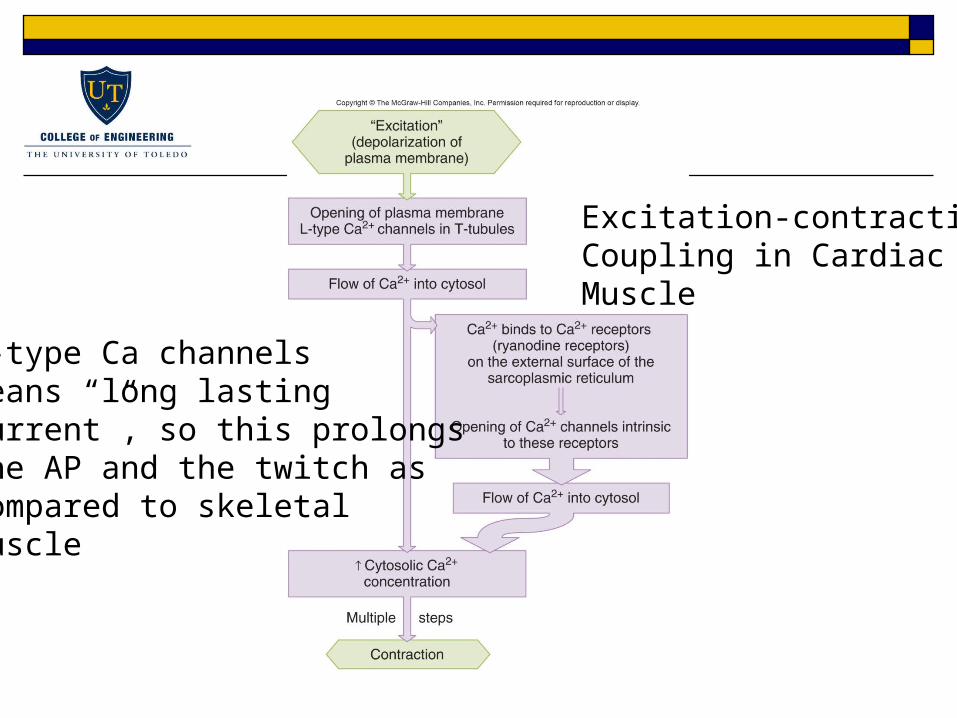
Excitation-contractionCoupling in CardiacMuscle
L-type Ca channelsmeans “long lastingcurrent”, so this prolongsthe AP and the twitch ascompared to skeletalmuscle
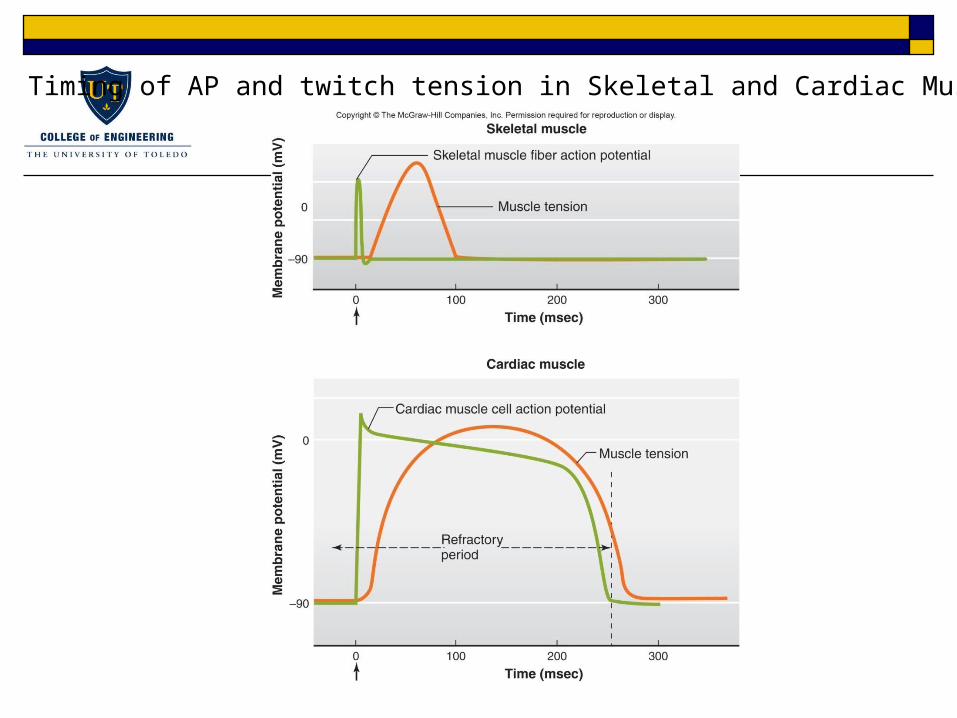
Timing of AP and twitch tension in Skeletal and Cardiac Muscle

Electrocardiogram (ECG or EKG) records electrical signals produced by myocardial tissue due cardiac cycle
Coordinated contraction of heart muscle produces an large electrical signal due to bulk ion flow
Voltage changes due to bulk ion flow can be recorded with surface electrodes
EKG amplitude is proportional to V(t) and dV/dt Characteristic waveform is observed and can be
used to diagnose problems
Electrocardiogram

Typical EKG
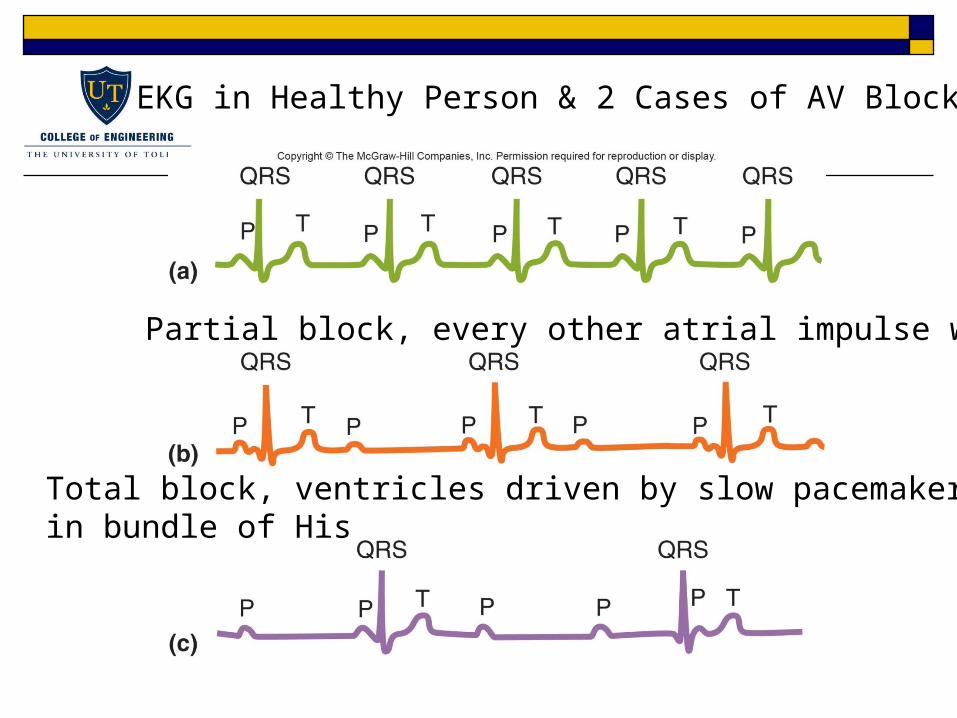
EKG in Healthy Person & 2 Cases of AV Block
Partial block, every other atrial impulse works
Total block, ventricles driven by slow pacemaker cellin bundle of His
Cardiac output
The average flow rate of blood through heart per minute is known as cardiac output (CO)
CO is product of SV (stroke volume) and heart rate (HR) CO = SV x HR Can control heart rate and stroke volume to change
cardiac output during rest or periods of intense activity Heart rate change be modulated by altering
excitability of pacemaker cells
Cardiac output
SV = EDV – ESV, can change SV in two ways Systemic vasculature can control amount of blood
returned to ventricle following diastole (EDV) Ventricular contractility can control amount of blood left in
ventricle following systole (ESV) Control of CO is accomplished via autonomic
nervous system Parasympathetic system decreases CO Sympathetic system increases CO
Control of heart rate
Normal heart will beat around 100 beats/min without any autonomic innervation
Numerous sympathetic and parasympathetic efferents terminate in SA node
At rest, parasympathetic system is more active so resting HR is 70 beats/min, below inherent rate of 100 beats/min
Control of heart rate
Sympathetic system increases HR by increasing inward cation (If) and low-threshold T-type Ca2+ currents in SA node Larger inward current increases rate of spontaneous
depolarization Parasympathetic fibers decrease HR by decreasing
If and T-type Ca2+ currents Parasympathetic fibers also increase K+ channel
activity Smaller inward current reduces rate of spontaneous
depolarization

Effects of sympathetic and parasympathetic nerveson SA nodal cell

Major factors that affect the heart rate

Signal Transduction Review
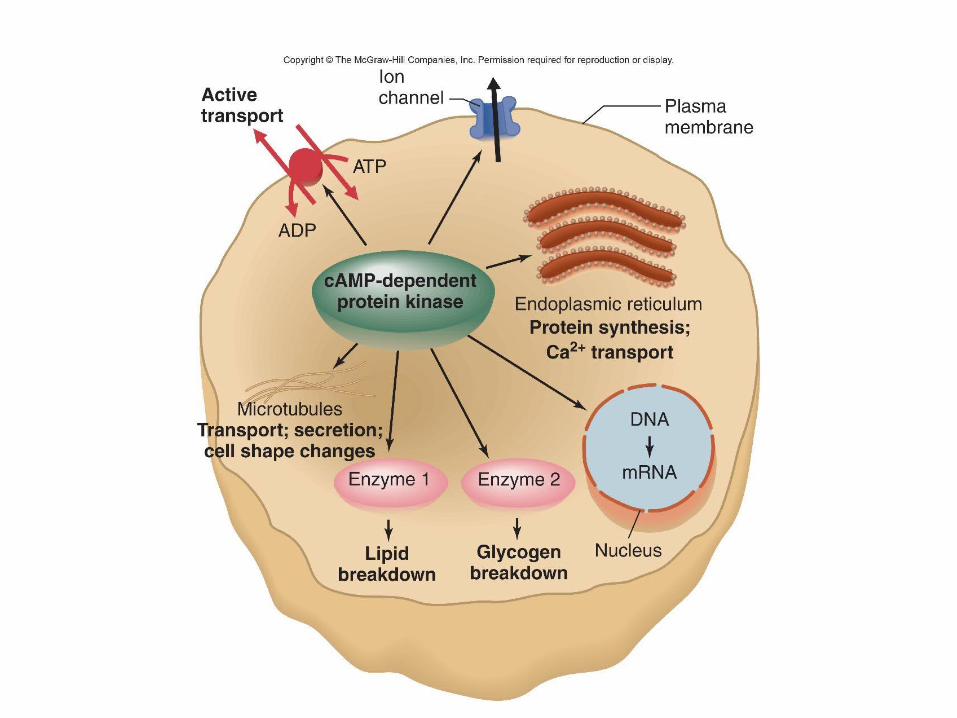

GPCRs and heart rate
Activation of GPCRs will effect contractility and heart rate via modulation of voltage-gated ion channels
Sympathetic increase of heart rate NE → adrenergic GPCR → activates adenylyl cyclase → increases
cAMP → activates PKA → increased phosphorylation of If and T-type channels → more inward current → increased dVm/dt
Phosphorylated channels are more likely to open at “resting” Vm
Parasympathetic decrease of heart rate ACh → mAChR GPCR → inhibits adenylyl cyclase → decreases
cAMP → deactivates PKA → decreased phosphorylation of If and T-type channels → less inward current → decreased dVm/dt
Dephosphorylated channels are less likely to open at “resting” Vm

Control of stroke volume – ventricular filling
Changes in EDV and ESV affect SV Remember SV = EDV – ESV EDV alters ability of ventricles to eject blood Relationship between SV and EDV is called Frank-
Starling mechanism Consequence of relationship between muscle fiber
length and tension Stretched cardiac muscle generates more tension

Ventricular Function Curve, EDV is major determinant ofventricular stretch which yields more forceful contraction

Control of stroke volume – ventricular filling
Therefore filling ventricles more will increase ability of ventricles to eject blood
Direct relationship venous return → atrial volume → ventricular filling → EDV → SV
Main function is to make sure pulmonary and systemic blood flows are equal
Prevents accumulation of blood in pulmonary or systemic vessels

Control of stroke volume - afterload
Increased arterial pressure increases ESV (end
systolic volume) Increased arterial pressure will shorten ventricular
ejection Valve closes when Parterial > Pventricle
Less time to eject blood from ventricle during single cycle, so stroke volume decreases


Control of stroke volume - afterload
If blood pressure is elevated, heart must work harder to eject same amount of fluid
This requires increased ventricular contractility Arteries can control systemic pressures via
constriction and dilation Preload – venous return that fills ventricle to
increase SV Afterload – arterial pressure that heart must work
against or result is decrease in SV Changes in SV due to preload and afterload are
“passive” effects
Control of stroke volume - contractility
EDV is somewhat affected by atrial contractility ESV is controlled by ventricular contractility Contractility changes are “active”, affected by
sympathetic and parasympathetic innervation Reflects increased myocardial activity independent
of length-tension relation
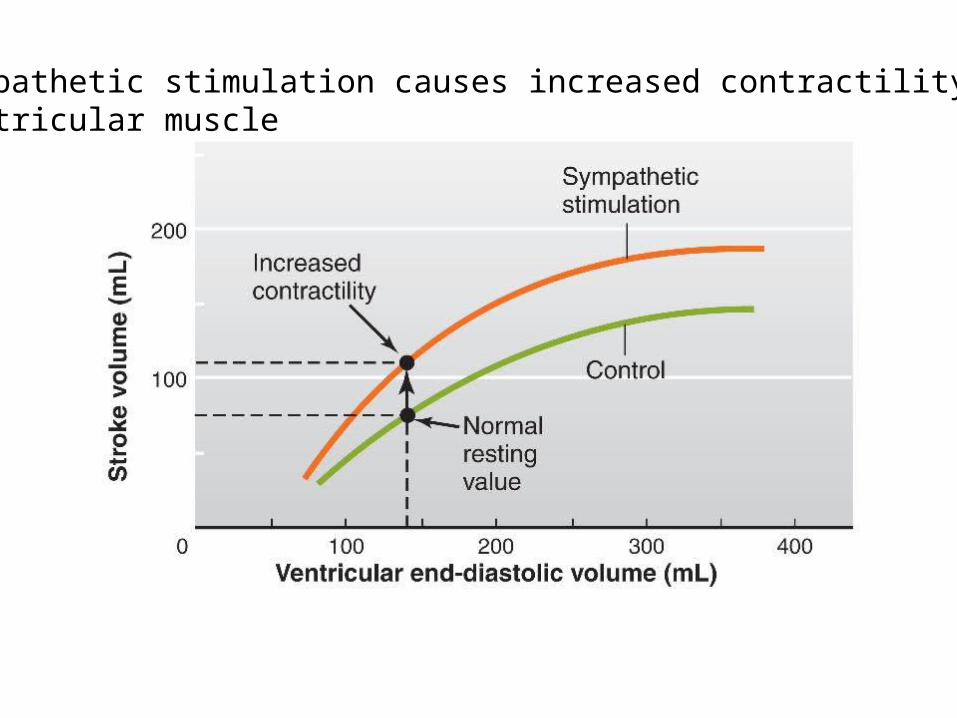
Sympathetic stimulation causes increased contractility ofventricular muscle

Rate of force development andrelaxation increase as well asthe force developed

Control of stroke volume - contractility
Main target is control of Ca2+ influx through VGCCs (voltage gated calcium channels) and CICR (calcium induced calcium release)
Atrial myocardium has sympathetic and parasympathetic innervation mAChRs and adrenergic GPCRs
Ventricular myocardium only has sympathetic innervation adrenergic GPCRs

Mechanisms of sympathetic effects oncardiac muscle contractility

Major factors determining cardiac output. Reversal of arrowsillustrate how cardiac output is decreased