myelodysplastic/myeloproliferative neoplasms · myelodysplastic/myeloproliferative neoplasms ......
TRANSCRIPT

Am J Clin Pathol 2009;132:281-289 281281 DOI: 10.1309/AJCPJ71PTVIKGEVT 281
© American Society for Clinical Pathology
AJCP / SHP/EAHP WorkSHoP
Myelodysplastic/Myeloproliferative Neoplasms
Kathryn Foucar, MD
Key Words: Myelodysplasia; Myeloproliferative; Myeloid neoplasm, WHO classification
DOI: 10.1309/AJCPJ71PTVIKGEVT
A b s t r a c t
Myelodysplastic/myeloproliferative neoplasms (MDS/MPNs) are rare de novo myeloid neoplasms that exhibit hybrid dysplastic and proliferative features at presentation. This SHP/EAHP Workshop session was uniquely problematic owing to the overlap between MDS/MPNs and both chronic myeloproliferative neoplasms and myelodysplasia. The borderline between MDS/MPNs and overt acute myeloid leukemias was also an issue, mainly related to the accurate and consistent delineation of blast equivalents such as promonocytes. Aside from juvenile myelomonocytic leukemia, genetic features defining specific MDS/MPN subtypes have not been identified. Consequently, there is little change in the 2008 World Health Organization classification of MDS/MPNs compared with the 2001 version.
Myelodysplastic/myeloproliferative neoplasms (MDS/MPNs) are rare de novo myeloid neoplasms that exhibit dys-plastic and proliferative features at presentation. By definition, the CBC shows a variable combination of cytopenias and cytoses with dysplasia of at least 1 lineage. The bone marrow of patients with MDS/MPNs is characteristically hypercellular and shows dysplastic and proliferative features as predicted from the peripheral blood. By definition, the percentage of blasts in the blood and the bone marrow must be less than 20%. Four subtypes of MDS/MPNs have been identified, including chronic myelomonocytic leukemia (CMML), juvenile myelomonocytic leukemia (JMML), atypical chronic myeloid leukemia, BCR-ABL1– (aCML), MDS/MPNs unclassifiable (MDS/MPN-U), along with a provisional category, refractory anemia with ringed sideroblasts and thrombocytosis (RARS-T). The 2008 World Health Organization (WHO) classification system criteria for these subtypes of MDS/MPN are delineated in ❚Table 1❚.1-17
Although abnormalities in the regulation of the RAS path-way are common in various types of MDS/MPN, aside from JMML, distinctive genetic features vital to the subclassifica-tion of MDS/MPNs have not yet been delineated.9,18 Indeed, the newly proposed 2008 WHO classification of MDS/MPNs shows little change from the 2001 classification, reflecting the general lack of new biologic and genetic insights into this distinctive hybrid group of disorders. Cases of CMML with eosinophilia and PDGFRB rearrangement have been removed from the MDS/MPN category and placed in a new genetically defined category.1
Chronic Myelomonocytic Leukemia
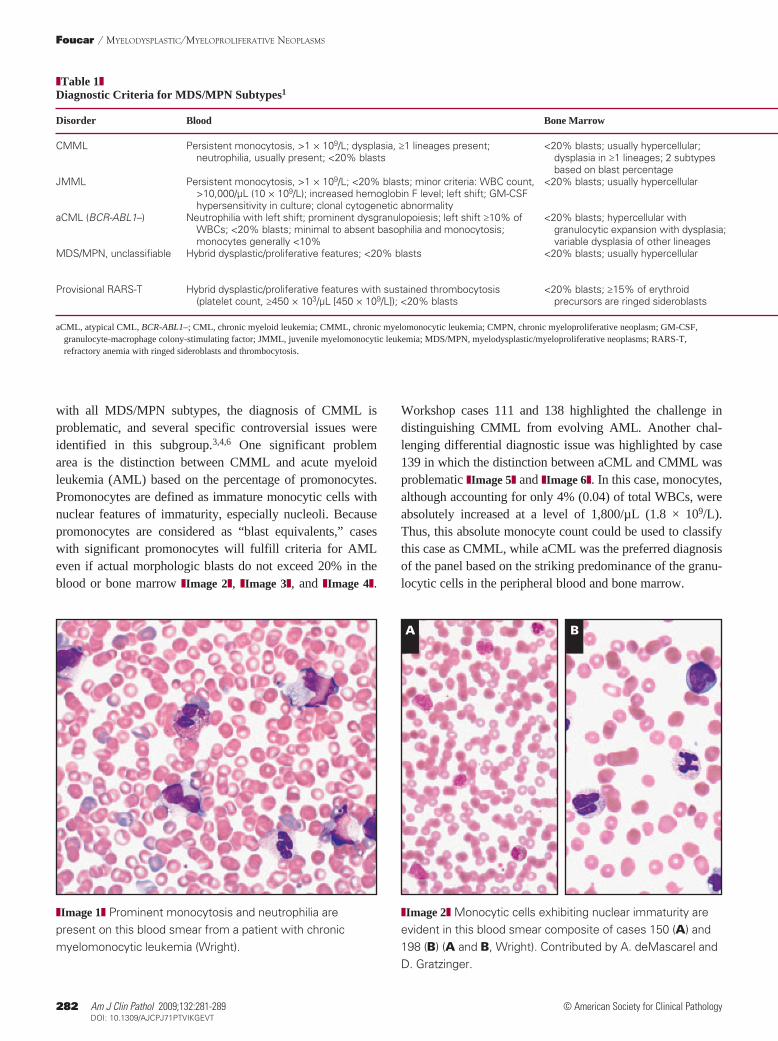
Five workshop cases were ultimately concluded to fulfill the diagnostic criteria for prototypic CMML ❚Image 1❚. As
282 Am J Clin Pathol 2009;132:281-289282 DOI: 10.1309/AJCPJ71PTVIKGEVT
© American Society for Clinical Pathology
Foucar / MyElodySPlAStic/MyEloProlifErAtivE NEoPlASMS
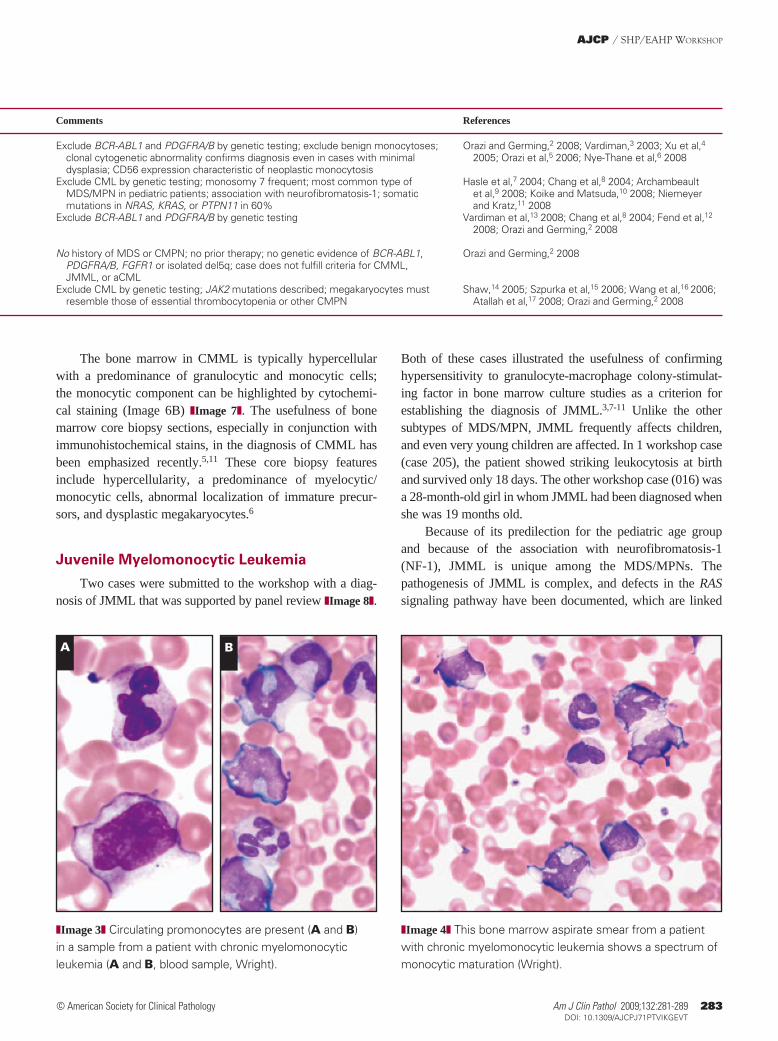
❚Image 2❚ Monocytic cells exhibiting nuclear immaturity are evident in this blood smear composite of cases 150 (A) and 198 (B) (A and B, Wright). Contributed by A. deMascarel and D. Gratzinger.
with all MDS/MPN subtypes, the diagnosis of CMML is problematic, and several specific controversial issues were identified in this subgroup.3,4,6 One significant problem area is the distinction between CMML and acute myeloid leukemia (AML) based on the percentage of promonocytes. Promonocytes are defined as immature monocytic cells with nuclear features of immaturity, especially nucleoli. Because promonocytes are considered as “blast equivalents,” cases with significant promonocytes will fulfill criteria for AML even if actual morphologic blasts do not exceed 20% in the blood or bone marrow ❚Image 2❚, ❚Image 3❚, and ❚Image 4❚.
Workshop cases 111 and 138 highlighted the challenge in distinguishing CMML from evolving AML. Another chal-lenging differential diagnostic issue was highlighted by case 139 in which the distinction between aCML and CMML was problematic ❚Image 5❚ and ❚Image 6❚. In this case, monocytes, although accounting for only 4% (0.04) of total WBCs, were absolutely increased at a level of 1,800/µL (1.8 × 109/L). Thus, this absolute monocyte count could be used to classify this case as CMML, while aCML was the preferred diagnosis of the panel based on the striking predominance of the granu-locytic cells in the peripheral blood and bone marrow.
A B
❚Image 1❚ Prominent monocytosis and neutrophilia are present on this blood smear from a patient with chronic myelomonocytic leukemia (Wright).
❚Table 1❚Diagnostic Criteria for MDS/MPN Subtypes1
Disorder Blood Bone Marrow Comments References
CMML Persistent monocytosis, >1 × 109/L; dysplasia, ≥1 lineages present; <20% blasts; usually hypercellular; Exclude BCR-ABL1 and PDGFRA/B by genetic testing; exclude benign monocytoses; Orazi and Germing,2 2008; Vardiman,3 2003; Xu et al,4 neutrophilia, usually present; <20% blasts dysplasia in ≥1 lineages; 2 subtypes clonal cytogenetic abnormality confirms diagnosis even in cases with minimal 2005; Orazi et al,5 2006; Nye-Thane et al,6 2008 based on blast percentage dysplasia; CD56 expression characteristic of neoplastic monocytosis JMML Persistent monocytosis, >1 × 109/L; <20% blasts; minor criteria: WBC count, <20% blasts; usually hypercellular Exclude CML by genetic testing; monosomy 7 frequent; most common type of Hasle et al,7 2004; Chang et al,8 2004; Archambeault >10,000/µL (10 × 109/L); increased hemoglobin F level; left shift; GM-CSF MDS/MPN in pediatric patients; association with neurofibromatosis-1; somatic et al,9 2008; Koike and Matsuda,10 2008; Niemeyer hypersensitivity in culture; clonal cytogenetic abnormality mutations in NRAS, KRAS, or PTPN11 in 60% and Kratz,11 2008 aCML (BCR-ABL1–) Neutrophilia with left shift; prominent dysgranulopoiesis; left shift ≥10% of <20% blasts; hypercellular with Exclude BCR-ABL1 and PDGFRA/B by genetic testing Vardiman et al,13 2008; Chang et al,8 2004; Fend et al,12 WBCs; <20% blasts; minimal to absent basophilia and monocytosis; granulocytic expansion with dysplasia; 2008; Orazi and Germing,2 2008 monocytes generally <10% variable dysplasia of other lineages MDS/MPN, unclassifiable Hybrid dysplastic/proliferative features; <20% blasts <20% blasts; usually hypercellular No history of MDS or CMPN; no prior therapy; no genetic evidence of BCR-ABL1, Orazi and Germing,2 2008 PDGFRA/B, FGFR1 or isolated del5q; case does not fulfill criteria for CMML, JMML, or aCML Provisional RARS-T Hybrid dysplastic/proliferative features with sustained thrombocytosis <20% blasts; ≥15% of erythroid Exclude CML by genetic testing; JAK2 mutations described; megakaryocytes must Shaw,14 2005; Szpurka et al,15 2006; Wang et al,16 2006; (platelet count, ≥450 × 103/µL [450 × 109/L]); <20% blasts precursors are ringed sideroblasts resemble those of essential thrombocytopenia or other CMPN Atallah et al,17 2008; Orazi and Germing,2 2008
aCML, atypical CML, BCR-ABL1–; CML, chronic myeloid leukemia; CMML, chronic myelomonocytic leukemia; CMPN, chronic myeloproliferative neoplasm; GM-CSF, granulocyte-macrophage colony-stimulating factor; JMML, juvenile myelomonocytic leukemia; MDS/MPN, myelodysplastic/myeloproliferative neoplasms; RARS-T, refractory anemia with ringed sideroblasts and thrombocytosis.
Am J Clin Pathol 2009;132:281-289 283283 DOI: 10.1309/AJCPJ71PTVIKGEVT 283
© American Society for Clinical Pathology
AJCP / SHP/EAHP WorkSHoP
Both of these cases illustrated the usefulness of confirming hypersensitivity to granulocyte-macrophage colony-stimulat-ing factor in bone marrow culture studies as a criterion for establishing the diagnosis of JMML.3,7-11 Unlike the other subtypes of MDS/MPN, JMML frequently affects children, and even very young children are affected. In 1 workshop case (case 205), the patient showed striking leukocytosis at birth and survived only 18 days. The other workshop case (016) was a 28-month-old girl in whom JMML had been diagnosed when she was 19 months old.
Because of its predilection for the pediatric age group and because of the association with neurofibromatosis-1 (NF-1), JMML is unique among the MDS/MPNs. The pathogenesis of JMML is complex, and defects in the RAS signaling pathway have been documented, which are linked
The bone marrow in CMML is typically hypercellular with a predominance of granulocytic and monocytic cells; the monocytic component can be highlighted by cytochemi-cal staining (Image 6B) ❚Image 7❚. The usefulness of bone marrow core biopsy sections, especially in conjunction with immunohistochemical stains, in the diagnosis of CMML has been emphasized recently.5,11 These core biopsy features include hypercellularity, a predominance of myelocytic/monocytic cells, abnormal localization of immature precur-sors, and dysplastic megakaryocytes.6
Juvenile Myelomonocytic Leukemia
Two cases were submitted to the workshop with a diag-nosis of JMML that was supported by panel review ❚Image 8❚.
A B
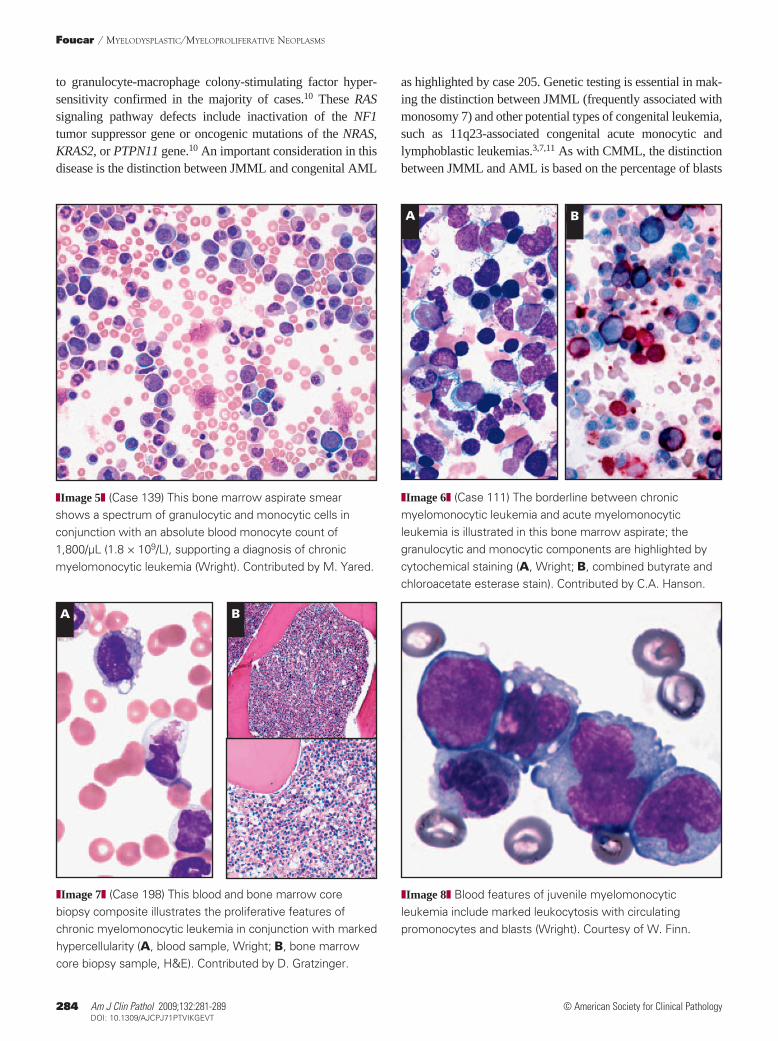
❚Image 3❚ Circulating promonocytes are present (A and B) in a sample from a patient with chronic myelomonocytic leukemia (A and B, blood sample, Wright).
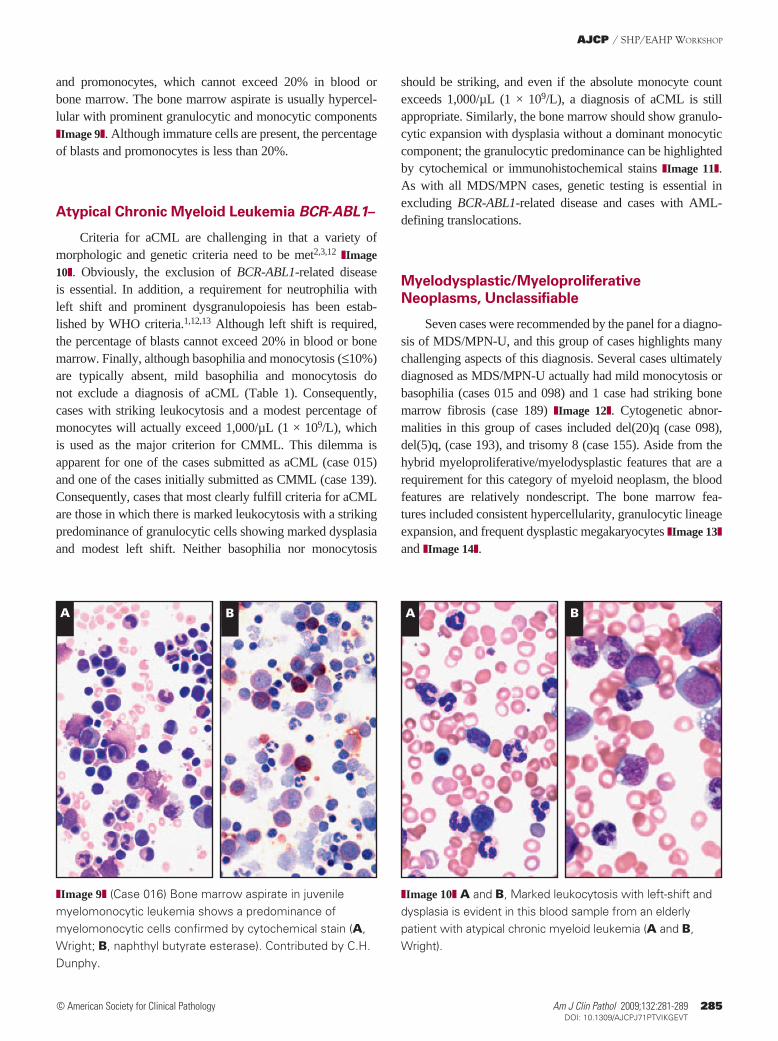
❚Image 4❚ This bone marrow aspirate smear from a patient with chronic myelomonocytic leukemia shows a spectrum of monocytic maturation (Wright).
❚Table 1❚Diagnostic Criteria for MDS/MPN Subtypes1
Disorder Blood Bone Marrow Comments References
CMML Persistent monocytosis, >1 × 109/L; dysplasia, ≥1 lineages present; <20% blasts; usually hypercellular; Exclude BCR-ABL1 and PDGFRA/B by genetic testing; exclude benign monocytoses; Orazi and Germing,2 2008; Vardiman,3 2003; Xu et al,4 neutrophilia, usually present; <20% blasts dysplasia in ≥1 lineages; 2 subtypes clonal cytogenetic abnormality confirms diagnosis even in cases with minimal 2005; Orazi et al,5 2006; Nye-Thane et al,6 2008 based on blast percentage dysplasia; CD56 expression characteristic of neoplastic monocytosis JMML Persistent monocytosis, >1 × 109/L; <20% blasts; minor criteria: WBC count, <20% blasts; usually hypercellular Exclude CML by genetic testing; monosomy 7 frequent; most common type of Hasle et al,7 2004; Chang et al,8 2004; Archambeault >10,000/µL (10 × 109/L); increased hemoglobin F level; left shift; GM-CSF MDS/MPN in pediatric patients; association with neurofibromatosis-1; somatic et al,9 2008; Koike and Matsuda,10 2008; Niemeyer hypersensitivity in culture; clonal cytogenetic abnormality mutations in NRAS, KRAS, or PTPN11 in 60% and Kratz,11 2008 aCML (BCR-ABL1–) Neutrophilia with left shift; prominent dysgranulopoiesis; left shift ≥10% of <20% blasts; hypercellular with Exclude BCR-ABL1 and PDGFRA/B by genetic testing Vardiman et al,13 2008; Chang et al,8 2004; Fend et al,12 WBCs; <20% blasts; minimal to absent basophilia and monocytosis; granulocytic expansion with dysplasia; 2008; Orazi and Germing,2 2008 monocytes generally <10% variable dysplasia of other lineages MDS/MPN, unclassifiable Hybrid dysplastic/proliferative features; <20% blasts <20% blasts; usually hypercellular No history of MDS or CMPN; no prior therapy; no genetic evidence of BCR-ABL1, Orazi and Germing,2 2008 PDGFRA/B, FGFR1 or isolated del5q; case does not fulfill criteria for CMML, JMML, or aCML Provisional RARS-T Hybrid dysplastic/proliferative features with sustained thrombocytosis <20% blasts; ≥15% of erythroid Exclude CML by genetic testing; JAK2 mutations described; megakaryocytes must Shaw,14 2005; Szpurka et al,15 2006; Wang et al,16 2006; (platelet count, ≥450 × 103/µL [450 × 109/L]); <20% blasts precursors are ringed sideroblasts resemble those of essential thrombocytopenia or other CMPN Atallah et al,17 2008; Orazi and Germing,2 2008
aCML, atypical CML, BCR-ABL1–; CML, chronic myeloid leukemia; CMML, chronic myelomonocytic leukemia; CMPN, chronic myeloproliferative neoplasm; GM-CSF, granulocyte-macrophage colony-stimulating factor; JMML, juvenile myelomonocytic leukemia; MDS/MPN, myelodysplastic/myeloproliferative neoplasms; RARS-T, refractory anemia with ringed sideroblasts and thrombocytosis.
284 Am J Clin Pathol 2009;132:281-289284 DOI: 10.1309/AJCPJ71PTVIKGEVT
© American Society for Clinical Pathology
Foucar / MyElodySPlAStic/MyEloProlifErAtivE NEoPlASMS
to granulocyte-macrophage colony-stimulating factor hyper-sensitivity confirmed in the majority of cases.10 These RAS signaling pathway defects include inactivation of the NF1 tumor suppressor gene or oncogenic mutations of the NRAS, KRAS2, or PTPN11 gene.10 An important consideration in this disease is the distinction between JMML and congenital AML
as highlighted by case 205. Genetic testing is essential in mak-ing the distinction between JMML (frequently associated with monosomy 7) and other potential types of congenital leukemia, such as 11q23-associated congenital acute monocytic and lymphoblastic leukemias.3,7,11 As with CMML, the distinction between JMML and AML is based on the percentage of blasts
❚Image 8❚ Blood features of juvenile myelomonocytic leukemia include marked leukocytosis with circulating promonocytes and blasts (Wright). Courtesy of W. Finn.
❚Image 7❚ (Case 198) This blood and bone marrow core biopsy composite illustrates the proliferative features of chronic myelomonocytic leukemia in conjunction with marked hypercellularity (A, blood sample, Wright; B, bone marrow core biopsy sample, H&E). Contributed by D. Gratzinger.
A B
A B
❚Image 5❚ (Case 139) This bone marrow aspirate smear shows a spectrum of granulocytic and monocytic cells in conjunction with an absolute blood monocyte count of 1,800/µL (1.8 × 109/L), supporting a diagnosis of chronic myelomonocytic leukemia (Wright). Contributed by M. Yared.
❚Image 6❚ (Case 111) The borderline between chronic myelomonocytic leukemia and acute myelomonocytic leukemia is illustrated in this bone marrow aspirate; the granulocytic and monocytic components are highlighted by cytochemical staining (A, Wright; B, combined butyrate and chloroacetate esterase stain). Contributed by C.A. Hanson.
Am J Clin Pathol 2009;132:281-289 285285 DOI: 10.1309/AJCPJ71PTVIKGEVT 285
© American Society for Clinical Pathology
AJCP / SHP/EAHP WorkSHoP
and promonocytes, which cannot exceed 20% in blood or bone marrow. The bone marrow aspirate is usually hypercel-lular with prominent granulocytic and monocytic components ❚Image 9❚. Although immature cells are present, the percentage of blasts and promonocytes is less than 20%.
Atypical Chronic Myeloid Leukemia BCR-ABL1–
Criteria for aCML are challenging in that a variety of morphologic and genetic criteria need to be met2,3,12 ❚Image 10❚. Obviously, the exclusion of BCR-ABL1-related disease is essential. In addition, a requirement for neutrophilia with left shift and prominent dysgranulopoiesis has been estab-lished by WHO criteria.1,12,13 Although left shift is required, the percentage of blasts cannot exceed 20% in blood or bone marrow. Finally, although basophilia and monocytosis (≤10%) are typically absent, mild basophilia and monocytosis do not exclude a diagnosis of aCML (Table 1). Consequently, cases with striking leukocytosis and a modest percentage of monocytes will actually exceed 1,000/µL (1 × 109/L), which is used as the major criterion for CMML. This dilemma is apparent for one of the cases submitted as aCML (case 015) and one of the cases initially submitted as CMML (case 139). Consequently, cases that most clearly fulfill criteria for aCML are those in which there is marked leukocytosis with a striking predominance of granulocytic cells showing marked dysplasia and modest left shift. Neither basophilia nor monocytosis
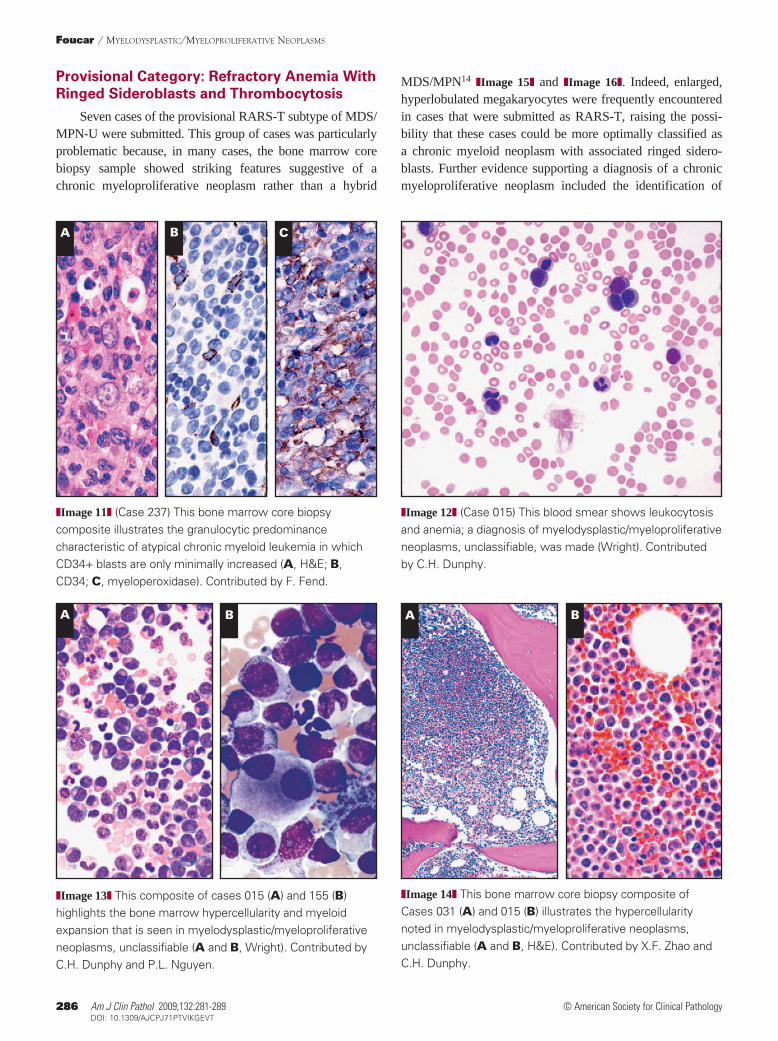
should be striking, and even if the absolute monocyte count exceeds 1,000/µL (1 × 109/L), a diagnosis of aCML is still appropriate. Similarly, the bone marrow should show granulo-cytic expansion with dysplasia without a dominant monocytic component; the granulocytic predominance can be highlighted by cytochemical or immunohistochemical stains ❚Image 11❚. As with all MDS/MPN cases, genetic testing is essential in excluding BCR-ABL1-related disease and cases with AML-defining translocations.
Myelodysplastic/Myeloproliferative Neoplasms, Unclassifiable
Seven cases were recommended by the panel for a diagno-sis of MDS/MPN-U, and this group of cases highlights many challenging aspects of this diagnosis. Several cases ultimately diagnosed as MDS/MPN-U actually had mild monocytosis or basophilia (cases 015 and 098) and 1 case had striking bone marrow fibrosis (case 189) ❚Image 12❚. Cytogenetic abnor-malities in this group of cases included del(20)q (case 098), del(5)q, (case 193), and trisomy 8 (case 155). Aside from the hybrid myeloproliferative/myelodysplastic features that are a requirement for this category of myeloid neoplasm, the blood features are relatively nondescript. The bone marrow fea-tures included consistent hypercellularity, granulocytic lineage expansion, and frequent dysplastic megakaryocytes ❚Image 13❚ and ❚Image 14❚.
A B A B
❚Image 9❚ (Case 016) Bone marrow aspirate in juvenile myelomonocytic leukemia shows a predominance of myelomonocytic cells confirmed by cytochemical stain (A, Wright; B, naphthyl butyrate esterase). Contributed by C.H. Dunphy.
❚Image 10❚ A and B, Marked leukocytosis with left-shift and dysplasia is evident in this blood sample from an elderly patient with atypical chronic myeloid leukemia (A and B, Wright).
286 Am J Clin Pathol 2009;132:281-289286 DOI: 10.1309/AJCPJ71PTVIKGEVT
© American Society for Clinical Pathology
Foucar / MyElodySPlAStic/MyEloProlifErAtivE NEoPlASMS
Provisional Category: Refractory Anemia With Ringed Sideroblasts and Thrombocytosis
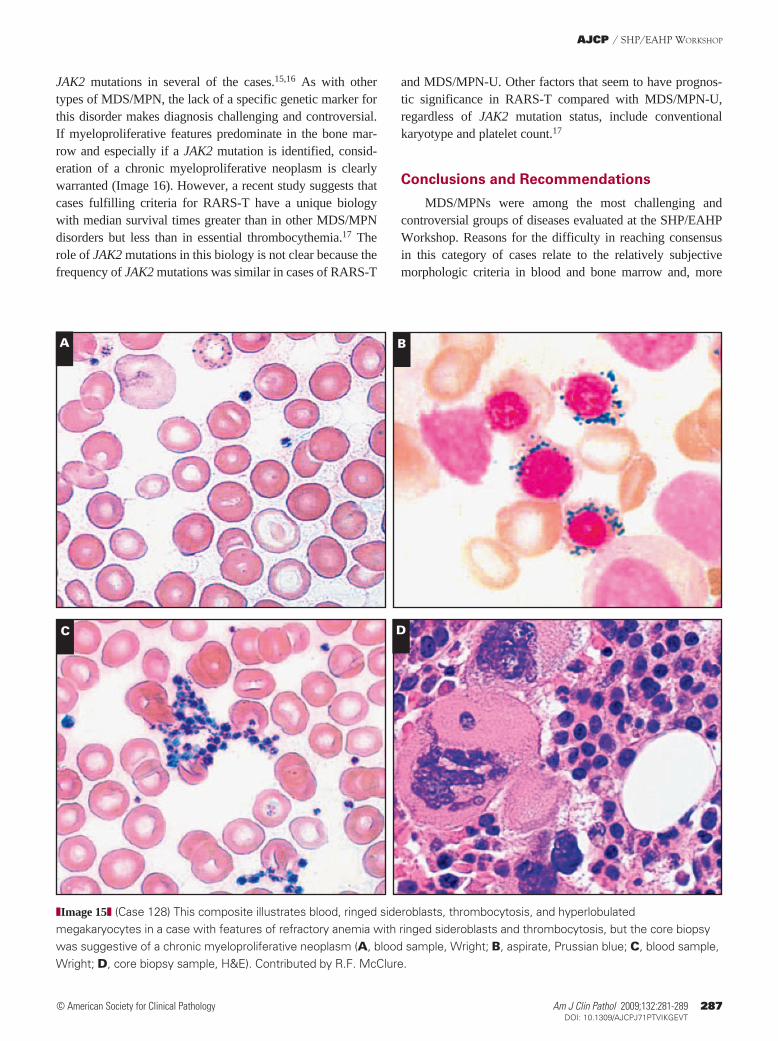
Seven cases of the provisional RARS-T subtype of MDS/MPN-U were submitted. This group of cases was particularly problematic because, in many cases, the bone marrow core biopsy sample showed striking features suggestive of a chronic myeloproliferative neoplasm rather than a hybrid
MDS/MPN14 ❚Image 15❚ and ❚Image 16❚. Indeed, enlarged, hyperlobulated megakaryocytes were frequently encountered in cases that were submitted as RARS-T, raising the possi-bility that these cases could be more optimally classified as a chronic myeloid neoplasm with associated ringed sidero-blasts. Further evidence supporting a diagnosis of a chronic myeloproliferative neoplasm included the identification of
A B C
❚Image 11❚ (Case 237) This bone marrow core biopsy composite illustrates the granulocytic predominance characteristic of atypical chronic myeloid leukemia in which CD34+ blasts are only minimally increased (A, H&E; B, CD34; C, myeloperoxidase). Contributed by F. Fend.
❚Image 12❚ (Case 015) This blood smear shows leukocytosis and anemia; a diagnosis of myelodysplastic/myeloproliferative neoplasms, unclassifiable, was made (Wright). Contributed by C.H. Dunphy.
A B A B
❚Image 13❚ This composite of cases 015 (A) and 155 (B) highlights the bone marrow hypercellularity and myeloid expansion that is seen in myelodysplastic/myeloproliferative neoplasms, unclassifiable (A and B, Wright). Contributed by C.H. Dunphy and P.L. Nguyen.
❚Image 14❚ This bone marrow core biopsy composite of Cases 031 (A) and 015 (B) illustrates the hypercellularity noted in myelodysplastic/myeloproliferative neoplasms, unclassifiable (A and B, H&E). Contributed by X.F. Zhao and C.H. Dunphy.
Am J Clin Pathol 2009;132:281-289 287287 DOI: 10.1309/AJCPJ71PTVIKGEVT 287
© American Society for Clinical Pathology
AJCP / SHP/EAHP WorkSHoP
and MDS/MPN-U. Other factors that seem to have prognos-tic significance in RARS-T compared with MDS/MPN-U, regardless of JAK2 mutation status, include conventional karyotype and platelet count.17
Conclusions and Recommendations
MDS/MPNs were among the most challenging and controversial groups of diseases evaluated at the SHP/EAHP Workshop. Reasons for the difficulty in reaching consensus in this category of cases relate to the relatively subjective morphologic criteria in blood and bone marrow and, more
JAK2 mutations in several of the cases.15,16 As with other types of MDS/MPN, the lack of a specific genetic marker for this disorder makes diagnosis challenging and controversial. If myeloproliferative features predominate in the bone mar-row and especially if a JAK2 mutation is identified, consid-eration of a chronic myeloproliferative neoplasm is clearly warranted (Image 16). However, a recent study suggests that cases fulfilling criteria for RARS-T have a unique biology with median survival times greater than in other MDS/MPN disorders but less than in essential thrombocythemia.17 The role of JAK2 mutations in this biology is not clear because the frequency of JAK2 mutations was similar in cases of RARS-T
A B
C D
❚Image 15❚ (Case 128) This composite illustrates blood, ringed sideroblasts, thrombocytosis, and hyperlobulated megakaryocytes in a case with features of refractory anemia with ringed sideroblasts and thrombocytosis, but the core biopsy was suggestive of a chronic myeloproliferative neoplasm (A, blood sample, Wright; B, aspirate, Prussian blue; C, blood sample, Wright; D, core biopsy sample, H&E). Contributed by R.F. McClure.
288 Am J Clin Pathol 2009;132:281-289288 DOI: 10.1309/AJCPJ71PTVIKGEVT
© American Society for Clinical Pathology
Foucar / MyElodySPlAStic/MyEloProlifErAtivE NEoPlASMS
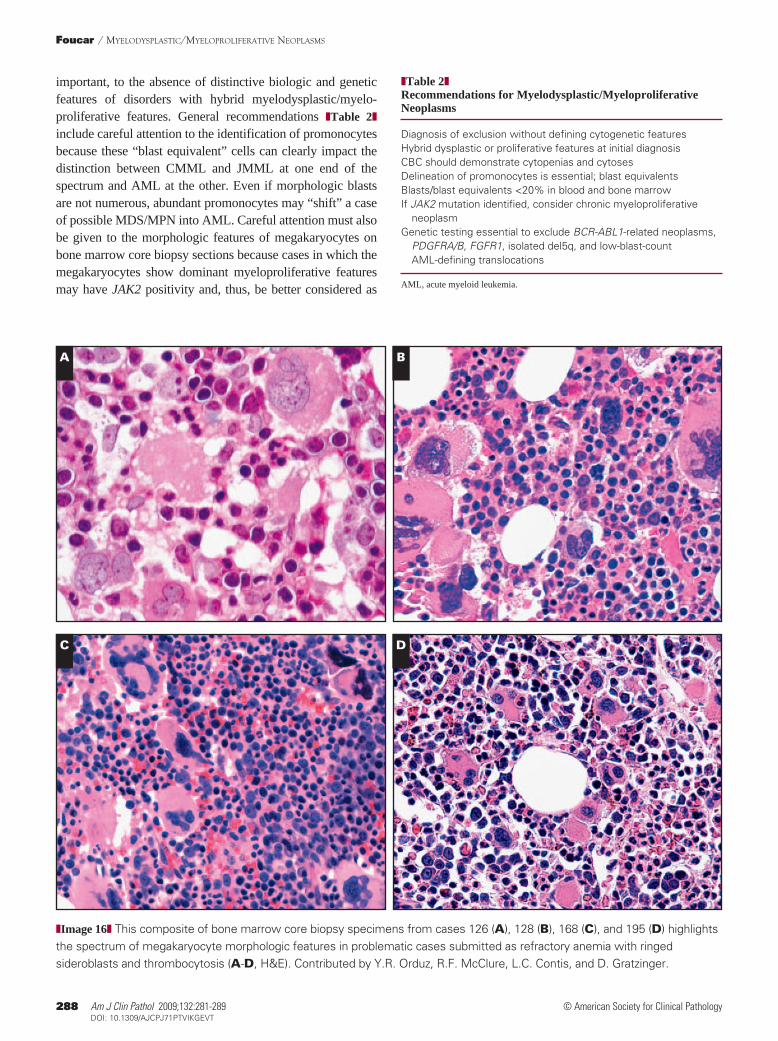
important, to the absence of distinctive biologic and genetic features of disorders with hybrid myelodysplastic/myelo-proliferative features. General recommendations ❚Table 2❚ include careful attention to the identification of promonocytes because these “blast equivalent” cells can clearly impact the distinction between CMML and JMML at one end of the spectrum and AML at the other. Even if morphologic blasts are not numerous, abundant promonocytes may “shift” a case of possible MDS/MPN into AML. Careful attention must also be given to the morphologic features of megakaryocytes on bone marrow core biopsy sections because cases in which the megakaryocytes show dominant myeloproliferative features may have JAK2 positivity and, thus, be better considered as
❚Table 2❚Recommendations for Myelodysplastic/Myeloproliferative Neoplasms
Diagnosis of exclusion without defining cytogenetic featuresHybrid dysplastic or proliferative features at initial diagnosisCBC should demonstrate cytopenias and cytosesDelineation of promonocytes is essential; blast equivalentsBlasts/blast equivalents <20% in blood and bone marrowIf JAK2 mutation identified, consider chronic myeloproliferative neoplasmGenetic testing essential to exclude BCR-ABL1-related neoplasms, PDGFRA/B, FGFR1, isolated del5q, and low-blast-count AML-defining translocations
AML, acute myeloid leukemia.
❚Image 16❚ This composite of bone marrow core biopsy specimens from cases 126 (A), 128 (B), 168 (C), and 195 (D) highlights the spectrum of megakaryocyte morphologic features in problematic cases submitted as refractory anemia with ringed sideroblasts and thrombocytosis (A-D, H&E). Contributed by Y.R. Orduz, R.F. McClure, L.C. Contis, and D. Gratzinger.
A B
C D

Am J Clin Pathol 2009;132:281-289 289289 DOI: 10.1309/AJCPJ71PTVIKGEVT 289
© American Society for Clinical Pathology
AJCP / SHP/EAHP WorkSHoP
8. Chang Y, Jou S, Lin D, et al. Differentiating juvenile myelomonocytic leukemia from chronic myeloid leukemia in childhood. J Pediatr Hematol Oncol. 2004;26:236-242.
9. Archambeault S, Flores N, Yoshimi A, et al. Development of an allele-specific minimal residual disease assay for patients with juvenile myelomonocytic leukemia. Blood. 2008;111:1124-1127.
10. Koike K, Matsuda K. Recent advances in the pathogenesis and management of juvenile myelomonocytic leukaemia. Br J Haematol. 2008;141:567-575.
11. Niemeyer C, Kratz C. Paediatric myelodysplastic syndromes and juvenile myelomonocytic leukaemia: molecular classification and treatment options. Br J Haematol. 2008;140:610-624.
12. Fend F, Horn T, Koch I, et al. Atypical chronic myeloid leukemia as defined in the WHO classification is a JAK2 V617 negative neoplasm. Leuk Res. 2008;32:1931-1935.
13. Vardiman JW, Bennett JM, Bain BJ, et al. Atypical chronic myeloid leukemia, BCR-ABL1 negative. In: Swerdlow SH, Campo E, Harris NL, et al, eds. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed. Lyon, France: IARC Press; 2008:80-81. WHO Classification of Tumours; vol 2.
14. Shaw G. Ringed sideroblasts with thrombocytosis: an uncommon mixed myelodysplastic/myeloproliferative disease of older adults. Br J Haematol. 2005;131:180-184.
15. Szpurka H, Tiu R, Murugesan G, et al. Refractory anemia with ringed sideroblasts associated with marked thrombocytosis (RARS-T), another myeloproliferative condition characterized by JAK2 V617F mutation. Blood. 2006;108:2173-2181.
16. Wang S, Hasserjian RP, Loew JM, et al. Refractory anemia with ringed sideroblasts associated with marked thrombocytosis harbors JAK2 mutation and shows overlapping myeloproliferative and myelodysplastic features. Leukemia. 2006;20:1641-1644.
17. Atallah E, Nussenzveig R, Yin CC, et al. Prognostic interaction between thrombocytosis and JAK2 V617F mutation in the WHO subcategories of myelodysplastic/myeloproliferative disease-unclassifiable and refractory anemia with ringed sideroblasts and marked thrombocytosis. Leukemia. 2008;22:1295-1298.
18. Matsuda K, Shimada A, Yoshida N, et al. Spontaneous improvement of hematologic abnormalities in patients having juvenile myelomonocytic leukemia with specific RAS mutations. Blood. 2007;109:5477-5480.
a type of chronic myeloproliferative neoplasm. Even though a distinctive genetic “marker” for MDS/MPNs has not yet been identified, genetic testing must always be performed on these cases to exclude the possibility of a BCR-ABL1-related disorder or some other translocation such as t(8;21) that would favor a diagnosis of low-blast-count AML.
From the Department of Pathology, University of New Mexico, Health Sciences Center, Albuquerque.
Address reprint requests to Dr Foucar: TriCore Reference Laboratory, 1001 Woodward Pl NE, Albuquerque, NM 87102.
Acknowledgments: The workshop panel acknowledges all pathologists who submitted cases to the MDS/MPN session: B. Alobeid, A. Bagg, G. Bhagat, F.J. Bot, L.C. Contis, A. deMascarel, C.H. Dunphy (2 cases), F. Fend, T. George, D. Gratzinger, C.A. Hanson, R.F. McClure, T.J. Molina, P.L. Nguyen, A. Orazi, Y.R. Orduz, D.S. Rao, A. Schmitt-Graeff, K.S. Theil, X. Wang, M. Yared, and X.F. Zhao.
References 1. Vardiman JW, Brunning RD, Arber DA, et al. Introduction
and overview of the classification of the myeloid neoplasms. In: Swerdlow SH, Campo E, Harris NL, et al, eds. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed. Lyon, France: IARC Press; 2008:18-30. WHO Classification of Tumours; vol 2.
2. Orazi A, Germing U. The myelodysplastic/myeloproliferative neoplasms: myeloproliferative diseases with dysplastic features. Leukemia. 2008;22:1308-1319.
3. Vardiman JW. Myelodysplastic syndromes, chronic myeloproliferative diseases, and myelodysplastic/myeloproliferative diseases. Semin Diagn Pathol. 2003;20:154-179.
4. Xu Y, McKenna R, Karandikar N, et al. Flow cytometric analysis of monocytes as a tool for distinguishing chronic myelomonocytic leukemia from reactive monocytosis. Am J Clin Pathol. 2005;124:799-806.
5. Orazi A, Chiu R, O’Malley DP, et al. Chronic myelomonocytic leukemia: the role of bone marrow biopsy immunohistology. Mod Pathol. 2006;19:1536-1545.
6. Nye-Thane N, Lampert I, Naresh K. Bone marrow trephine morphology and immunohistochemical findings in chronic myelomonocytic leukaemia. Br J Haematol. 2008;141:771-781.
7. Hasle H, Baumann I, Bergsträsser E, et al. The International Prognostic Scoring System (IPSS) for childhood myelodysplastic syndrome (MDS) and juvenile myelomonocytic leukemia (JMML). Leukemia. 2004;18:2008-2014.