multidisciplinary management of prostate malignancy
TRANSCRIPT
Multidisciplinary Management of Prostate Malignancy
Joseph W. Basler, PhD, MD*, Carol Jenkins, RN, and Gregory Swanson, MD
Address*Departments of Urology and Radiation Oncology, University of Texas Health Sciences Center, MC7845, 7703 Floyd Curl Drive, San Antonio, TX 78229-3900, USA.E-mail: [email protected]
Current Prostate Reports 2005, 3:51–57Current Science Inc. ISSN 1544-1865Copyright © 2005 by Current Science Inc.
IntroductionThe most commonly diagnosed urologic malignanciesinclude prostate cancer, urothelial malignancies, renalcancer, and testicular cancer. The diagnosis of each ismade through a thorough evaluation of signs and symp-toms related to the affected organ systems. Initial stag-ing evaluation and treatment of localized disease alsofalls exclusively in the hands of the urologist, except inthe case of prostate cancer. In this case, patients occa-sionally are diagnosed by interventional radiologists inconjunction with primary care and initial treatment mayinvolve only consultation with radiation oncologists.However, these patients may need the care of a urologistbecause of treatment-related side effects (eg, hematuria,irritative voiding) or disease progression. Clinical asso-ciations among specialty physicians have come aboutthrough a realization that multimodal therapies aremore effective for renal, advanced urothelial, and testic-ular cancer. Furthermore, the lack of effective curativetherapy for prostate cancer in advanced stages and lackof consensus on optimal treatment for localized disease
have spawned clinical trials that have become ubiqui-tous among cancer treatment centers.
Multidisciplinary clinics (MDC) for cancer patientshave been the subject of several recent reports. Strasser etal. [1] reported retrospectively on their experience with apalliative care MDC for advanced cancer patients. Theirquestionnaire-driven study indicated an improved level ofpatient satisfaction with the clinic and an increasednumber of constructive recommendations in the MDCsetting. Ko and Chaudhry [2] reported their experiencewith cancer patients in the multidisciplinary setting,emphasizing the need for continued vigilance with respectto existing comorbid variables. A report by Gabel et al. [3]in 1997 demonstrated improved patient satisfaction and ashortened interval to initiation of treatment in the MDCsetting. Along the same lines, Chang et al. [4] reported thatthe MDC for breast cancer often provided patients withtreatment options not otherwise offered.
Valicenti et al. [5] reported on the experience withnewly diagnosed prostate cancer patients at Thomas Jeffer-son University. Their experience was based on a modelsystem in which each new prostate cancer patient was seenand examined by a urologist (100%), radiation oncologist(41%), and medical oncologist (5%) during the initialvisit. Most patients (87%) had clinically localized prostatecancer. After the consultations, the clinical team, whichalso would include a pathologist and radiologist (whennecessary), presented each patient for discussion andgeneration of a recommendation of treatment options forthe patient. Relevant clinical trials also were considered inthe recommendations. Although most patients came forsecond opinions, a significant number (67%) ultimatelychose to have treatment through the center. The organiza-tional structure and commitment of the participants wereconsidered key to effective functioning of the MDC.
The design and function of their MDC seems ideo-logically and functionally sound. However, from a prac-tical perspective, having three specialists in waiting fornew prostate cancer patients will not always be econom-ically feasible. This is especially true considering that theurologist and radiation oncologist may be the only onescalled upon for the initial treatment of most patients.Another approach, in the face of more limited resources,is to only schedule combined visits for those most likelyto benefit from them. The mechanism for this involvesthe development of guidelines for scheduling based on
Most urologic malignancies are diagnosed initially and managed by urologists. However, better outcomes may be attained by integrating the surgical, medical, and radiologic disciplines. The primary care physician remains an impor-tant cornerstone whose talents should not be underesti-mated in the overall patient management scheme. Additional services such as endocrinology, physical therapy, pain control, hospice, nutrition, biofeedback, and hyperbar-ics, among others, should be considered in the overall health care team. The organization of the team, including definition of the duties of key personnel and even the physical framework of the clinic, contribute to its success in treating patients with prostate cancer. Pitfalls of the process also are discussed in this article.
52 Prostate Cancer
the likelihood of needing a particular specialist and theknowledge of the usual recommendations for similarpatients’ conditions.
Rather than describe treatment-specific diagnosis andtreatment regimens for prostate cancer, this article focuseson the organizational structure and responsibilities ofvarious services in a functional multidisciplinary prostatecancer management clinic. It will draw on the experiencesgained over the past 5 years at the South Texas VeteransAdministration Health Care System (STVAHCS) andUniversity of Texas Health Sciences Center at San AntonioDepartment of Urology. The STVAHCS GU Tumor Clinicis a tertiary center that handles all of the referrals fromSan Antonio through the lower Rio Grande Valley and thesouthern Texas Gulf Coast. Approximately 4500 prostatecancer-related visits are scheduled annually. This multi-disciplinary clinic system is similar in many respects tothe Thomas Jefferson MDC structure, but it involves theused of generally agreed upon algorithms for patientcounseling, thus eliminating extraneous re-evaluationswhile still providing a high level of counseling and care.Flexibility is important to allow unanticipated visits withspecialists as needed. Some pitfalls of the system areaddressed because experience has shown that even themost sophisticated systems have occasional oversightsthat may compromise effectiveness.
The Organizational Strata of a Successfully Integrated Multidisciplinary ClinicMissionThe plan described assumes an active role for the MDCthat spans the timeframe starting before the prostate cancerdiagnosis, through treatment, and throughout the patient’snatural lifetime. The key focus of the clinic is to provideeducation, with diagnosis and treatment following as indi-cated. For the at-risk patient, diagnosis is offered whenappropriate and desired. After diagnosis, if curative inter-vention is possible and likely to decrease morbidity ormortality, it is offered. However, for advanced disease,cancer management, rather than cure, usually is the strat-egy. The latter often requires the most cooperative effort
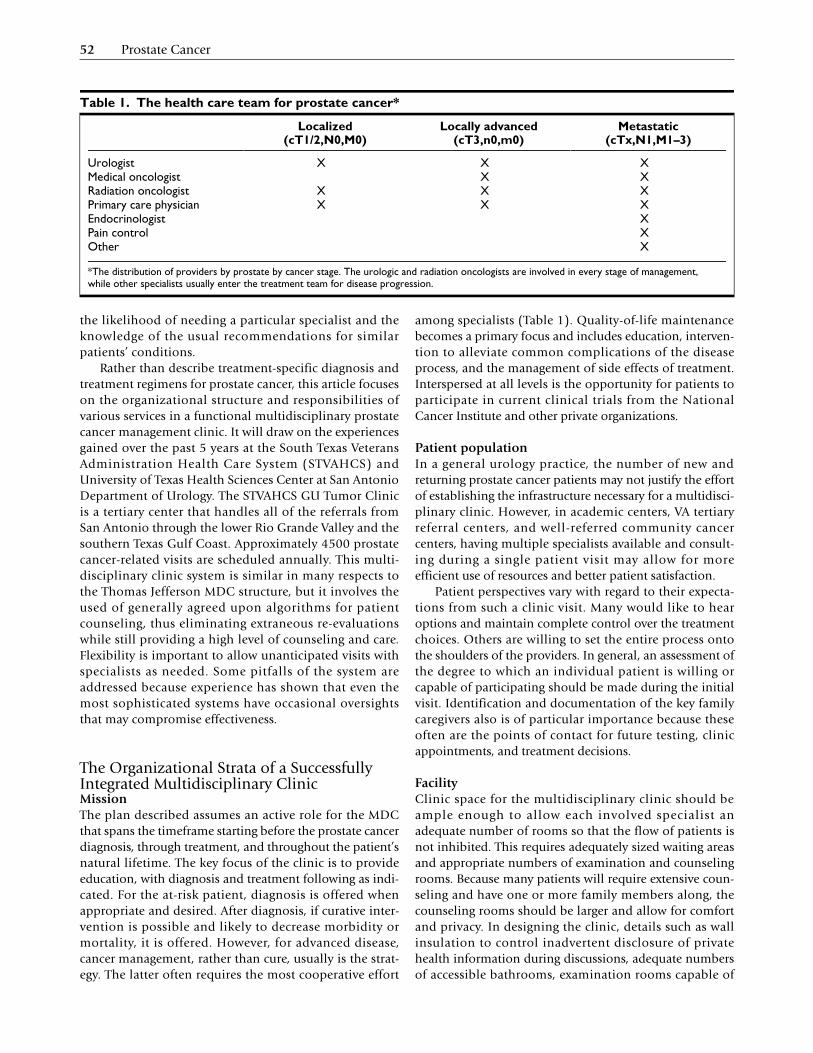
among specialists (Table 1). Quality-of-life maintenancebecomes a primary focus and includes education, interven-tion to alleviate common complications of the diseaseprocess, and the management of side effects of treatment.Interspersed at all levels is the opportunity for patients toparticipate in current clinical trials from the NationalCancer Institute and other private organizations.
Patient populationIn a general urology practice, the number of new andreturning prostate cancer patients may not justify the effortof establishing the infrastructure necessary for a multidisci-plinary clinic. However, in academic centers, VA tertiaryreferral centers, and well-referred community cancercenters, having multiple specialists available and consult-ing during a single patient visit may allow for moreefficient use of resources and better patient satisfaction.
Patient perspectives vary with regard to their expecta-tions from such a clinic visit. Many would like to hearoptions and maintain complete control over the treatmentchoices. Others are willing to set the entire process ontothe shoulders of the providers. In general, an assessment ofthe degree to which an individual patient is willing orcapable of participating should be made during the initialvisit. Identification and documentation of the key familycaregivers also is of particular importance because theseoften are the points of contact for future testing, clinicappointments, and treatment decisions.
FacilityClinic space for the multidisciplinary clinic should beample enough to allow each involved specialist anadequate number of rooms so that the flow of patients isnot inhibited. This requires adequately sized waiting areasand appropriate numbers of examination and counselingrooms. Because many patients will require extensive coun-seling and have one or more family members along, thecounseling rooms should be larger and allow for comfortand privacy. In designing the clinic, details such as wallinsulation to control inadvertent disclosure of privatehealth information during discussions, adequate numbersof accessible bathrooms, examination rooms capable of
Table 1. The health care team for prostate cancer*
Localized (cT1/2,N0,M0)
Locally advanced (cT3,n0,m0)
Metastatic (cTx,N1,M1–3)
Urologist X X XMedical oncologist X XRadiation oncologist X X XPrimary care physician X X XEndocrinologist XPain control XOther X
*The distribution of providers by prostate by cancer stage. The urologic and radiation oncologists are involved in every stage of management, while other specialists usually enter the treatment team for disease progression.

Multidisciplinary Management of Prostate Malignancy • Basler et al. 53
handling wheelchairs and stretchers, and the ergonomicsof the examination rooms should be considered. The flowof patients within the clinic should be designed to mini-mize possible patient embarrassment and maintain confi-dentiality. This is particularly important when patientshaving catheters or wheelchairs or those on stretchers arebrought in for consultation. A successful design will nothave patients crossing paths as they move through thefacility. Examination room design also is important toallow the patient and physician to function within theirown space. Too often, patients are forced to look at theback of the physician’s head as he documents the visit. Asimple change in room design allowing the physician toalways be facing the patient adds the invaluable eye contactthat nurtures the physician-patient relationship. Becauseprostate examination is inherently messy, an easily accessi-ble sink, soap, and towels for patient use are importantand convey a sense of respect in the overall process.
In addition, especially for patients with more advanceddisease or recurrences after initial treatment attempts,ancillary capabilities such as laboratory, radiology(computed tomography, magnetic resonance, generalX-ray, ultrasonography, interventional), nuclear medicine,
and cystoscopy should be available on site, or close by, tospeed diagnosis and treatment recommendations. If theclinic is part of a larger facility, attempts also should bemade to allow these patients priority in the ancillarydepartments on the day of their visits.
Record keepingThe clinic records ideally should be shared and immedi-ately available to the treating team and ancillary services.An integrated electronic medical record such as the VAcomputerized patient record system allows every aspect ofthe patients’ care to be reviewed without delays caused bypoor handwriting or dictation/transcription processing. Alist of current providers, including the primary care physi-cian (PCP) and any other specialists with whom thepatient may be involved, should be maintained with chartcopies sent to each after the clinic visits. This will allow fora smooth integration of care should the patient requireadmission, further work-up, or medical clearance prior toprocedures (Table 2).
In the private sector, sources of frustration and delaythat must be addressed include insurance restrictions onproviders and facilities and precertification require-ments for laboratory, radiography, and invasive proce-dures. Preclinic review of the patients’ records andprevious studies and phone interviews by an experi-enced clinical nurse, physician assistant, or other desig-nated provider may be able to anticipate testing andprocedures so that the precertifications can be in processor completed by the time of the visit. Depending on thethird-party insurer, it may be necessary to have theprimary care provider prepare referrals for consultationsby each of the physicians in the clinic in order for thevisit to occur as designed. Intraclinic referrals (specialistto specialist; specialist to facility) may be appropriateand acceptable, but care must be taken to avoid short-circuiting the referral documentation required by third-party insurers. Patient satisfaction may plummet if thevisit leads to unexpected additional expenses for lack ofattention to detail.
Tumor registryMost hospitals operate a tumor registry in an ongoingeffort to maintain their cancer program’s approval by theAmerican College of Surgeons Commission on Cancer. Formany reasons, the registry should be an integral part of thedesign of documentation in the multidisciplinary clinic.Anticipating the entry of these data by accurate clinicaland, when appropriate, pathologic staging in the medicalrecord will allow rapid entry into the Tumor Registry data-base and more efficient queries for quality assurance (QA)and research purposes (eg, screening for clinical trials,research papers). In many institutions, the Tumor Registrymay be cumbersome because of data entry methodologyand restrictions, but it remains a readily available resourcefrom which to begin QA and research databases.
Table 2. Documentation recommendations for the multidisciplinary clinic chart*
Patient contact informationFamily or other significant person's contact informationIdentify decision-maker within the familyPatient's decision-making abilities, delegationsAdvanced directives, power-of-attorney documentsPhysician list and contact informationPrimary care physician, other specialists and providersProblem listMedical, surgical diagnoses/histories with datesMedication listInclude start and stop dates of genitourinary-related
medicationsInclude outpatient administration logLaboratory and radiology reports (with summary sheets as
necessary)Prostate-specific antigen and date list annotated with
treatmentsUp-to-date notes and consultation reportsFormat notes for easy summation, coding, and database
entryClinical and pathologic staging information as indicatedConcise summary of any conferences regarding the patient
(including dates and providers)Future
Upcoming testing, clinic visit schedulesReminders of necessary less frequent periodic testing (eg,
bone mineral density testing)
*Documentation recommendations that allow efficient evaluation, re-evaluation, and treatment. In paper charts, a separate section for "pending review" helps to alert the physician to new laboratory and radiology reports. These generally are not filed until reviewed and signed. Electronic records often will have an alert mechanism for review of the new results.

54 Prostate Cancer
Quality assurance databaseThis database is important to assure that all patients aregiven equal access to available resources, to identifypatients with incomplete evaluation and treatment, and toavoid the occasional patient who becomes lost to follow-up. The QADB may be as simple as a spread sheet thattracks the patient’s progress in appointments, laboratorytests, and imaging. More sophisticated endeavors willallow outcomes measures, such as patient satisfactionsurveys, quality of life, voiding dysfunction, and sexualdysfunction instruments, and objective assessments (eg,prostate-specific antigen [PSA]) to be assessed with regardto treatments administered over time.
Research databaseThis database, which may be derived from the QADB,provides the basis for participation in clinical trials andnew research efforts. Research databases in general willrequire approval and oversight by an institutional reviewboard with appropriate measures instituted for patientconfidentiality and consent.
Educational materialsA multitude of educational materials from pamphlets,books, and web sites are available to allow the patient a hardcopy of the information necessary to become informed andallow appropriate decision-making. The delineation of all ofthese goes beyond the scope of this article. However, eachclinic should investigate the available resources for theirpopulation of patients or create their own materials. Themain standards should be to present an honest andbalanced approach to the topic of prostate cancer treatment.In centers that offer treatment, a general assessment of theirlocal success rates and potential complication rates will be ahelpful tool for the patient in preparation for treatment.When appropriate, document translations to the patient’snative language should be provided. Standardized readingmaterial also is a valuable asset to define and document theinformed consent process. The latter point should not betaken lightly because an underinformed patient or one whojumps to treatment without considering options may laterclaim physician culpability for poor results or complica-tions. Careful documentation of the consultations, treat-ment planning conferences, and recommendations withdetailed reasoning can protect the physician, the clinic, andits reputation.
Support groupsAlthough many physicians view prostate cancer supportgroups as fringe activity, they provide an important sourceof comfort and sharing of ideas. They also provide awindow into the current thoughts of the general publicregarding the diagnosis and treatment of prostate cancerand the complications of treatment that may go unre-ported in the office. Involvement by the MDC personnel asspeakers, consultants, or advisors will help to fulfill the
primary educational goal and provide an opportunity todispel myths and misconceptions that may circulate in thelay community.
Key personnelThe success of the multidisciplinary effort depends on thedevelopment of a personnel infrastructure that includesthe clinical nurse (CN) or case manager (CM), the physi-cians, nurse practitioners, physician assistants, and ancil-lary personnel from scheduling clerks, billing/insurancespecialists, technicians, and patient advocates. Althoughnot all clinics will have each of these positions, the func-tions of each serve to speed progress through the systemand hopefully improve patient satisfaction and improveclinical outcomes. Data supporting the latter two objec-tives are sparse, but are anticipated to justify the effort.
In the scheme of things, the CN or CM serves as themain coordinator of activities and maintains patientcontact information and scheduling. As the CN/CMgains experience with patients and the physician team,he or she will begin to anticipate the need for testing andallow smooth flow by initiating precertifications andpaperwork as needed. A close interaction of this personwith the clinic scheduling manager is essential. Anotherfunction of the CN/CM is to serve as a point of contactand monitor a patient’s progress through the system.Significant other noncancerous genitourinary problemsalso are monitored so that the patient does not becomelost to follow-up with regard to other diagnoses withinthe clinic structure. Maintenance of an accurate problemlist also will help to prevent such errors. Maintenance ofmedication administration logs also are an importantaspect of the CN/CM, especially for patients undergoinghormone therapy (HT) or those receiving zolendronicacid infusions. The former can become unduly compli-cated for patients on an intermittent HT protocol with-out accurate documentation.
The CN/CM also should carefully monitor the no-showlist, reviewing each case and rescheduling visits and testingas indicated. The no-show rate at STVAHCH approaches15% for the tumor clinic. Reasons for the missed visits arevaried and include other illnesses, lost appointmentreminders, and lack of transportation. Maintaining a focuson the patients’ disease process rather than their punctual-ity and adding flexibility to scheduling brings most backinto the fold for appropriate follow-up. In some cases,close follow-up by the patient’s PCP with phone consulta-tions and less frequent visits to the clinic are acceptable.
The PCP usually is responsible for the initial contactwith the clinic prior to the diagnosis of prostate cancer. Insome centers, this consultation may be separate from themultidisciplinary clinic, although identification of the at-risk population allows possible participation in preventionstrategies. PCPs are an invaluable asset for their expertise inmanaging the general medical problems and preanestheticevaluation, should a procedure requiring anesthesia be

Multidisciplinary Management of Prostate Malignancy • Basler et al. 55
necessary. In some instances, routine care and follow-up ofthe prostate cancer falls back to the PCP if long-distancetravel makes clinic visits impractical for the patient.Continued monitoring of such patients and regular phoneconsultations are encouraged. In addition, pain control,nursing home, and terminal care issues are within the prac-tice scope of many PCPs.
A urologic oncologist or experienced urologistprovides the backbone of the clinic structure becauseevery aspect of care, from the initial referral by the PCP(or self referral in many cases) for suspicion of prostatecancer, through biopsies, treatment planning, andmanagement of advanced disease, fall under his or herpurview. As such, the urologic oncologist functions as thedistributor of consultations to other services and must bewell versed in the controversies, standards of care, andtreatment (or non-treatment) options available. Caremust be taken to avoid shunting patients to one treat-ment or service over others based on economic consider-ations, personal biases, or anecdotal experiences. In thisregard, it is wise to set up standard operating proceduresand algorithms, which define testing, timing of consulta-tions to other specialists, and treatment options. Theseshould be agreed on by the entire treatment team.
The patient and family often will bring their ownconception or misconception of the situation based onprior knowledge, readings, or experiences with the situa-tions of friends and family. Therefore, an important part ofthe discussion is to seek out the patient’s perspective andpreconceptions to provide a basis for the ensuing discus-sion. This will allow the physician to function in theprimary role as educator, setting the stage for the patientsand their family to be an integral part of the decision-mak-ing process. As mentioned previously, it often is necessaryto assess the degree to which the patient is able or wants tobe involved with the decision-making process. The familycaregiver and PCP often are invaluable resources in assess-ing the appropriateness of recommendations based on thepatient’s abilities or disabilities.
In academic centers, integration of the urologic oncol-ogy fellows and urology residents should be a primaryeducational goal and will allow the urologic oncologist tosupervise and better serve a larger group of patients. Nursepractitioners and physician assistants often are extremelyhelpful when fellows and residents are not involved or are inlimited supply. In either case, algorithm-based managementprotocols, which keep less experienced providers on track,are helpful [6•,7••]. Treatment algorithms serve as a basisfrom which to start and should not be seen as inviolatebecause each patient has a unique set of circumstances.
Radiation oncologists play an important role in treat-ment at every clinical stage. Specifically, after diagnosis ofprostate cancer and initial counseling, the radiationoncologist provides an overview of radiotherapy optionsincluding potentially curative treatment (for localizeddisease) and palliative efforts for more advanced stages.
Historically, almost all patients with prostate cancer wereseen first by a urologist; therefore, many radiation oncol-ogists perceived that the role of radiation was gettingshort-changed in the discussion of options. This hasresulted in some efforts to bypass the traditional referralpatterns to make sure that patients are informed of everyoption. However, this circumvention may leave thepatient with more limited options because surgical treat-ments generally are not presented and any other noncan-cerous urologic issues may remain unaddressed. Forexample, irritative voiding issues could be addressed bythe urologist before radiation treatment with an expectedimprovement in post-treatment functional outcomes.
Other specialty providersMedical oncologists experienced in the management ofprostate cancer who are familiar with the nuances of HTusually become involved when the patients have failedother forms of treatment or have presented with advanceddisease. Clinical trials of chemotherapy agents in earlier-stage disease (eg, pre-prostatectomy studies) are in devel-opment and may help to involve the medical oncologistsearlier. Endocrinologists have become involved in the careof advanced cancer patients who are undergoing HT for themanagement of the bone-related side effects. Occasionalinvolvement by orthopedists and neurosurgeons are neces-sary for dealing with advanced cancer- or osteoporosis-related compressions and fractures. Pre-emptive treatmentsand procedures often may prevent devastating complica-tions related to fractures. One of the goals of the MDC is toproactively identify potential complications such as theseand deal with them through radiotherapy or medicationbefore they get to the point where stabilization proceduresare necessary. Biofeedback may be helpful in treating thecomplications of surgery (incontinence) or radiation(urgency). Hyperbarics have been helpful in the patientwith irradiation cystitis. Physical therapists, nutritionists,and palliative care specialists (hospice) may become aregular part of the clinic for patients with advanced cancer.
Integration of providersThe combined clinic attempts to get beyond the self-serv-ing turf issues and provides a forum where a balancedapproach and presentation can be provided to patientsregarding their options in dealing with their cancer. Thisnecessitates an open and honest dialog among the differ-ent specialists and with the patients. There are multipleissues to consider. For example, the radiation oncologistsmust acknowledge that from the perspective of cancercontrol alone, surgery indeed is the gold standard for cT1and cT2 disease. For disease that is truly confined to thegland, radiation cannot improve on surgical removal. Thehope of radiotherapy is to approach the surgical results,while avoiding the potential morbidity of a major surgery.At the same time, the urologic oncologists have recognizedthat surgery is not in the best interest of every patient. For

56 Prostate Cancer
patients with cT3 disease and higher or cT2 with a high riskof extracapsular extension, radiation alone or combinedwith surgery may be better able to encompass the disease.An honest dialogue also would point out that nerve-spar-ing prostatectomy and brachytherapy implant haveapproximately the same rate of long-term impotence;therefore, if that concern is the patient’s sole motivationfor seeking brachytherapy, they may be misguided. In addi-tion, high-grade cancers (Gleason score ≥ 7) do not alwaysrespond well to radiation, especially if those cancers arebulky. Such patients may be better served with a surgicalapproach including node dissection and planned postop-erative radiation, depending on the final pathologic find-ings. Integration of services rather than competitionshould drive the clinic.
Localized DiseaseTo facilitate discussions, appropriate new patients shouldbe seen by a urologic oncologist and a radiation oncolo-gists during the same visit. The potentially curative optionsare presented in as balanced a manner as possible andtailored appropriately for individual patients. The radia-tion oncologist gives a detailed discussion regarding exter-nal beam radiation therapy and brachytherapy and offers aperspective on other options. The urologic oncologist doesthe same for the surgical option. A specific discussion ofrisks and benefits for each modality also is presented.Taking the patient’s overall health into account, the physi-cians then can collectively make a recommendation. Theunification of all of these considerations leaves the patientswith treatment options tailored to their specific situation.In most cases, the initial visit ends at this point because theamount of information to be digested by the patient can bestaggering. Patients may be encouraged to go home, readtheir information, check out recommended web sites,attend a support group meeting (eg, Us Too or other pros-tate cancer support group), and return for additionaldiscussions and formulation of a treatment plan. Provisionof patients with educational material and a statementregarding their particular cancer (clinical stage, Gleasonscore, PSA) is important. If desired, this will give thepatient adequate documentation for second opinions ordiscussions with the PCP.
At a minimum, the MDC patient should leave the visitwith a feeling that there was a team approach to the prob-lem, without the conflicting recommendations of a dispar-ate group of physicians. This empowers patients to maketreatment choices with which they can be satisfied. Oncethe patient’s desires are known and an informed decisionis made, the appropriate specialists make arrangements fortreatment and follow-up. A physician or clinic that makesthe same recommendation to every patient, regardless ofhealth status or tumor factors, likely is not functioning intheir patients’ best interest. On the other hand, if thepatient is presented with strongly opposing views, the
process may lead to more confusion than help in the deci-sion-making process.
Advanced DiseaseA combined approach using the skills of the urologiconcologist, radiation oncologist, and medical oncologistis crucial to managing the disease successfully. The goal ofthis approach is to control disease progression by mini-mizing the problems associated with local growth (eg,bladder outlet obstruction, hematuria, ureteral obstruc-tion) and distant spread (eg, fractures, cord compres-sion). However, disease progression is only part of theproblem with these patients. The urologic oncologist usu-ally assumes a primary role in coordinating the groupeffort and handling the HT that has become an inevitablepart of the treatment plan. The latter requires an under-standing of the issues regarding timing, duration, andexpected outcomes of HT. Managing the sequelae of HTrequires expertise in bone metabolism, hot flushes,fatigue, muscle wasting, anemia, and sexual dysfunction.In many cases, the advice of an endocrinologist, physicaltherapist, dietician, and others must be sought and coor-dinated as well. Advanced disease patients make up anincreasing percentage of the population of the MDC asthe clinic matures. They also are the patients most likelyto benefit from inclusion in clinical trials.
Follow-up ResponsibilitiesIt is important to build a follow-up program that incorpo-rates the input of the urologic oncologist and radiationoncologist. In the straightforward patient who is biochem-ically free of disease after treatment of localized diseaseand is suffering from no adverse sequelae, follow-up even-tually may fall to the PCP with periodic reports back to theclinic regarding PSA levels and re-referral for additionalconsultation if other issues arise. For those at high risk ofrecurrence or those suffering from adverse sequelae oftreatment, combined follow-up visits should be the ruleuntil every issue is settled. Patients who suffer a local fail-ure after radiotherapy are evaluated by the urologic oncol-ogist to assess candidacy for salvage surgery or othermodality (eg, HT). Any additional radiotherapy is coordi-nated with the radiation oncologist and chemotherapywith the medical oncologist. In most cases of failed localtherapy, the urologic oncologist assumes a primary role infollow-up and further treatment planning. As such, thesepatients usually remain under the care of the urologiconcologist in the MDC for life.
ConferencesIn addition to the immediate discussion of individualpatients, Tumor Board conferences, during which challeng-ing cases are presented and openly discussed among the

Multidisciplinary Management of Prostate Malignancy • Basler et al. 57
physician specialists and other providers, provide aneducational enhancement to the overall MDC process.Such conferences should be scheduled at an intervalappropriate to the patient population, usually biweekly ormonthly. Management strategies and new modalities fortreatment often come from such discussions. The results ofsuch discussions should be recorded in the patient’s recordby the case manager for later discussion with the patient.Short literature reviews and presentations regarding keyissues by the residents and fellows also may be a keycomponent of the conference.
Potential Pitfalls of the Multidisciplinary ClinicTable 3 describes problems we have seen that may berelated to the structure of the MDC for prostate cancermanagement. The first two issues occur when providersbecome too focused on their specific area of treatment ofthe prostate cancer. Patients also may decline or fail tokeep follow-up visits with their PCP while being treated inthe MDC. An adequate periodically reviewed problem listand encouragement regarding continued involvement ofthe PCP will minimize this issue.
The next three issues relate partly to scheduling diffi-culties or inflexibility. A busy clinic may adopt policies thatrestrict return visits for no-shows or those not seekingactive treatment. In no case should patients who declineclinical trials be excluded from follow-up. Our clinicattempts direct contact with a no-show patient, but manytimes works through the PCPs to arrange appropriatefollow-up and testing. If distance or transportation is anissue, arrangements with a urologist or clinic closer tohome can be made. If patients decline further recom-mended visits, careful documentation of their reasonsshould be entered in the record. Patients declining treat-ment are placed on observation protocol and scheduledfor periodic testing and visits for re-discussion of issues asindicated. The CN or CM should maintain the QADB,
which should allow identification of “lost to follow-up”patients. Reasons for these include death, moving toanother location, change in third-party insurance, and oth-ers. Careful documentation of attempts to contact thesepatients including certified return letters should be madein the patient’s clinic record.
The latter three problems require attention to docu-mentation, clear communication with the patient regard-ing the plans, and provision of the current algorithms fortesting and management as new providers come on service.Periodic re-discussion of the algorithms in light of newclinical data is important as a measure to continuallyupdate treatment options.
ConclusionsThe MDC can function well as an educational resource forpatients and provide state-of-the-art-care for patients withprostate cancer of all stages. Integrated activities of provid-ers and an appropriate physical and personnel infrastruc-ture are keys to success. Clear and concise documentationof treatment strategies along with a functioning qualityassurance infrastructure are important to keep physicianson track and patients satisfied with their treatment.
References and Recommended ReadingPapers of particular interest, published recently, have been highlighted as:• Of importance•• Of major importance
1. Strasser F, Sweeney C, Willey J, et al.: Impact of a half-day multi-disciplinary symptom control and palliative care outpatient clinic in a comprehensive cancer center on recommendations, symptom intensity, and patient satisfaction: retrospective descriptive study. J Pain Symptom Manage 2004, 27:481–491.
2. Ko C, Chaudhry S: The need for a multidisciplinary approach to cancer care. J Surg Res 2002, 105:53–57.
3. Gabel M, Hilton N, Nathanson S: Multidisciplinary breast cancer clinics: Do they work? Cancer 1997, 79:2380–2384.
4. Chang JH, Vines E, Bertsch H, et al.: The impact of a multidis-ciplinary breast cancer center on recommendations for patient management: the University of Pennsylvania experience. Cancer 2001, 91:1231–1237.
5. Valicenti RK, Gomella LG, El-Gabry EA, et al.: The multidisci-plinary clinic approach to prostate cancer counseling and treatment. Semin Urol Oncol 2000, 18:188–191.
6.• Hamdy FC, Basler JW, Neal DE, Catalona WJ: Management of Urologic Malignancies. London: Churchill Livingstone; 2002.
Outline an algorithm-based approach to the management of every aspect of prostate cancer.
7.•• Theodorescu D, Rabbani F, Donat S: Follow-up of genitouri-nary malignancies for the office urologist: a practical approach. Part 1: prostate and bladder cancers. AUA Update Series 2004, 23:297–307.
This referenced outline of follow-up protocols provides an excellent starting point for clinics.
Table 3. Potential problems within the multidisciplinary clinic
Inattention to other significant genitourinary or medical problems
Lack of care coordinationNo-show consternationNo treatment; no follow-up mentalityLost to follow-up patientsInadequate documentation of the treatment planInexperienced provider derails treatment planNew specialist with nonconforming ideas for treatment