multidisciplinary management of advanced primary and metastatic breast cancer
TRANSCRIPT

416
Multidisciplinary Management of Advanced Primary and Metastatic Breast Cancer Gabriel N. Horfobagyi, M.D.
Combined modality therapy has become the treatment of choice for patients with primary breast cancer, including those with locally advanced breast cancer. Primary or in- duction chemotherapy, followed by surgery or radiation therapy or both, and adjuvant systemic therapy is a gen- erally accepted strategy. Most tumors respond with a more than 50% decrease in tumor size, and approxi- mately 70% of patients experience down-staging through primary chemotherapy. Breast conservation is possible for many patients with locally advanced breast cancer, and almost all patients initially are rendered disease free.
Primary chemotherapy should be the initial choice of treatment for patients with locally advanced tumors, but it is unclear what the optimal sequence of subsequent therapies should be, or whether one or two local treat- ment modalities are necessary.
The most dramatic example of the efficacy of these regi- mens was demonstrated in patients with inflammatory breast cancer. Previously a universally fatal condition, the natural history of this disease has been changed dramati- cally by the introduction of these combined modality thera- pies. Five-year survival rates of 3540% commonly are re- ported, and it is likely that about one third of patients with this highly aggressive form of disease will survive beyond 10 years without recurrence. Combined modality therapy that includes primary chemotherapy provides appropriate local control, the possibility of breast conservation therapy, and, probably, an increased survival rate, at least for some sub- sets of patients with locally advanced breast cancer. The use of similar treatment strategies for early breast cancer is cur- rently under evaluation.
Hormone therapy and combination chemotherapy represent the main treatment approaches to metastatic
Presented at the National Conference on Breast Cancer, Boston, Massachusetts, August 26-28, 1993.
From the Department of Breast and Gynecologic Medical Oncol- ogy, The University of Texas M. D. Anderson Cancer Center, Hous- ton, Texas.
Supported in part by the Nylene Eckles Breast Cancer Research Foundation.
The authors thank Lidia Vogelsang for her secretarial assistance. Address for reprints: Gabriel N. Hortobagyi, M.D., Department
of Breast and Gynecologic Medical Oncology, The University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Boulevard, Houston, TX 77030.
Accepted for publication January 31, 1994.
breast cancer. Radiotherapy is also a useful palliative tool, especially for control of painful bone metastases and central nervous system involvement. Patient and tumor characteristics help in the optimal selection of systemic therapy. Palliative therapy for symptomatic control and prolongation of life also preserves a good quality of life.
Dose-intensive chemotherapy is being evaluated as a treatment to increase complete response rates and cause remission consolidation. Clinical trials on several new and effective cytotoxic agents, as well as new hormonal compounds, are being completed and are showing en- couraging preliminary results. Monoclonal antibodies to specific tumor antigens, growth factors, or their receptors have opened the possibility of more selective and poten- tially more effective treatments. Clinical investigation during the next decade will establish the role of these new modalities in the overall management of patients with breast cancer. Cancer 1994: 74:416-23.
Key words: breast cancer, chemotherapy, hormone therapy.
Locally Advanced Breast Cancer
Despite educational campaigns aimed at the lay public and the medical profession, and despite the availability of mammographic screening programs, locally ad- vanced breast cancer remains an important problem in current practice. While in systematically screened pop- ulations, locally advanced breast cancer should repre- sent less than 5% of those diagnosed, in inner city hos- pitals and underserved areas of the country, Stage I11 and locally advanced breast cancer may represent up to 20-30% of newly diagnosed patients with breast can- cer. The management of these patients has evolved sub- stantially over the last 3 decades, and the various cur- rent options will be summarized below.'
The last 2 decades have established the contribu- tion of adjuvant systemic treatments to the primary management of breast cancer.' Postoperative adjuvant chemotherapy and adjuvant hormone therapy clearly decreased the odds of recurrence and death from breast cancer for patients with both node negative and node positive tumors. Although far fewer studies have been
Treatment of Stage III/IV Breast Cancer/Hortobagyi 41 7
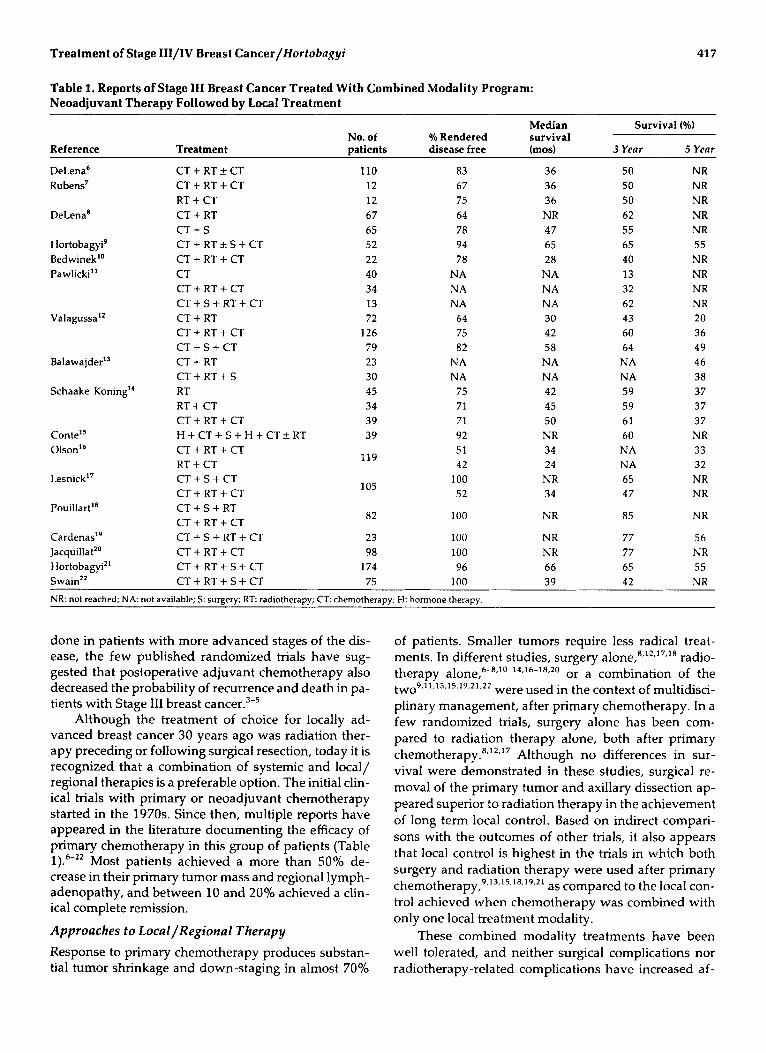
Table 1. Reports of Stage 111 Breast Cancer Treated With Combined Modality Program: Neoadjuvant Therapy Followed by Local Treatment
Median Survival (%) No. of YO Rendered survival
Reference Treatment patients disease free (mod 3 Year 5 Year
DeLena6 Rubens7
DeLena’
Hortobagyi’ Bedwinek” Pawlicki”
Valagussa”
Balawa jder”
Schaake- Koning“
Lesnick”
PouiIIarP
Cardenas” Jacquillat” Hortobagyi” Swain22
CT + RT -+ CT CT + RT + CT RT + CT CT + RT C T + S CT + RT f S + CT CT + RT + CT CT CT + RT + CT CT + S + RT + CT CT + RT CT + RT + CT CT + S + CT CT + RT CT + RT + S RT RT + CT CT + RT + CT H + CT+ S + H + C T a RT CT + RT + CT RT + CT CT + S + CT CT + RT + CT CT + S + RT CT + RT + CT CT + S + RT + CT CT + RT + CT CT + RT + S + CT
110 12 12 67 65 52 22 40 34 13 72
126 79 23 30 45 34 39 39
119
105
82
23 98
174
83 67 75 64 78 94 78
NA NA NA
64 75 82
NA NA
75 71 71 92 51 42
100 52
100
100 100 96
36 36 36 NR 47 65 28
NA NA NA 30 42 58
NA NA 42 45 50 NR 34 24 NR 34
NR
NR NR 66
50 50 50 62 55 65 40 13 32 62 43 60 64 NA NA 59 59 61 60 NA NA 65 47
85
77 77 65
NR NR NR NR NR 55 NR NR NR NR 20 36 49 46 38 37 37 37 NR 33 32 NR NR
NR
56 NR 55
CT + RT + 5 + CT 75 100 39 42 NR NR: not reached; NA: not available; S: surgery; R T radiotherapy; CT: chemotherapy; H: hormone therapy.
done in patients with more advanced stages of the dis- ease, the few published randomized trials have sug- gested that postoperative adjuvant chemotherapy also decreased the probability of recurrence and death in pa- tients with Stage 111 breast ~ a n c e r . ~ - ~
Although the treatment of choice for locally ad- vanced breast cancer 30 years ago was radiation ther- apy preceding or following surgical resection, today it is recognized that a combination of systemic and local/ regional therapies is a preferable option. The initial clin- ical trials with primary or neoadjuvant chemotherapy started in the 1970s. Since then, multiple reports have appeared in the literature documenting the efficacy of primary chemotherapy in this group of patients (Table 1).6-22 Most patients achieved a more than 50% de- crease in their primary tumor mass and regional lymph- adenopathy, and between 10 and 20% achieved a clin- ical complete remission.
Approaches to Local/Regional Therapy Response to primary chemotherapy produces substan- tial tumor shrinkage and down-staging in almost 70%
of patients. Smaller tumors require less radical treat- ments. In different studies, surgery a l ~ n e , ~ , ’ ~ , ’ ~ , ’ ~ radio- therapy alone,6-8,1 0-1 4.16-18.20 or a combination of the
were used in the context of multidisci- plinary management, after primary chemotherapy. In a few randomized trials, surgery alone has been com- pared to radiation therapy alone, both after primary ~hemotherapy.~,’~,’’ Although no differences in sur- vival were demonstrated in these studies, surgical re- moval of the primary tumor and axillary dissection ap- peared superior to radiation therapy in the achievement of long term local control. Based on indirect compari- sons with the outcomes of other trials, it also appears that local control is highest in the trials in which both surgery and radiation therapy were used after primary chemotherapy,9.~3.~5. 18.19.21 as compared to the local con- trol achieved when chemotherapy was combined with only one local treatment modality.
These combined modality treatments have been well tolerated, and neither surgical complications nor radiotherapy-related complications have increased af-
two9,1 1.13.15.19.21.22

418 CANCER Supplement July 1, 2994, Volume 74, No. 1
ter primary chemotherapy, except in those studies in which radiotherapy and chemotherapy have been ad- ministered simultaneously.
Breast Conservation after Primary Chemotherapy
Even 20 years ago, the first clinical trials of primary che- motherapy demonstrated that some (or many) patients with locally advanced breast cancer could be treated with breast con~ervation.~- '~ Our first study at the Uni- versity of Texas M. D. Anderson Cancer Center demon- strated that 15% of patients could be treated with che- motherapy and radiation therapy.' The first protocol for locally advanced breast cancer developed at the Milan Cancer Institute also showed that more than 50% of pa- tients could b2 treated appropriately without having to sacrifice their breasts.6 A review of the multiple publi- cations in this area over the last 20 years suggests that although breast conservation is clearly possible, the percentage of patients who are offered and accept breast conservation varies markedly from center to cen- ter. This suggests that down-staging is only one of the criteria used by different investigators to select patients for breast conservation therapy, and that different ex- pectations of aesthetic outcome might influence these decisions strongly.
The extension of clinical trials with preoperative chemotherapy to Stage I and Stage I1 breast cancer has confirmed the efficacy of these regimens and suggested that down-staging was even more prominent in these early stage^.^^-^^ Consequently, breast conservation is possible for a higher percentage of patients with Stage I and Stage I1 disease (SO-SO%) after primary chemother- apy. It also is evident from these studies of Stage I and Stage I1 breast cancer, however, that the size of the breast is only one of the exclusion criteria for breast con- servation, and that patients with multifocal disease (and other commonly employed criteria for exclusion) are probably not good candidates for breast conservation, regardless of their response to primary chemotherapy.
Inflammatory Breast Cancer
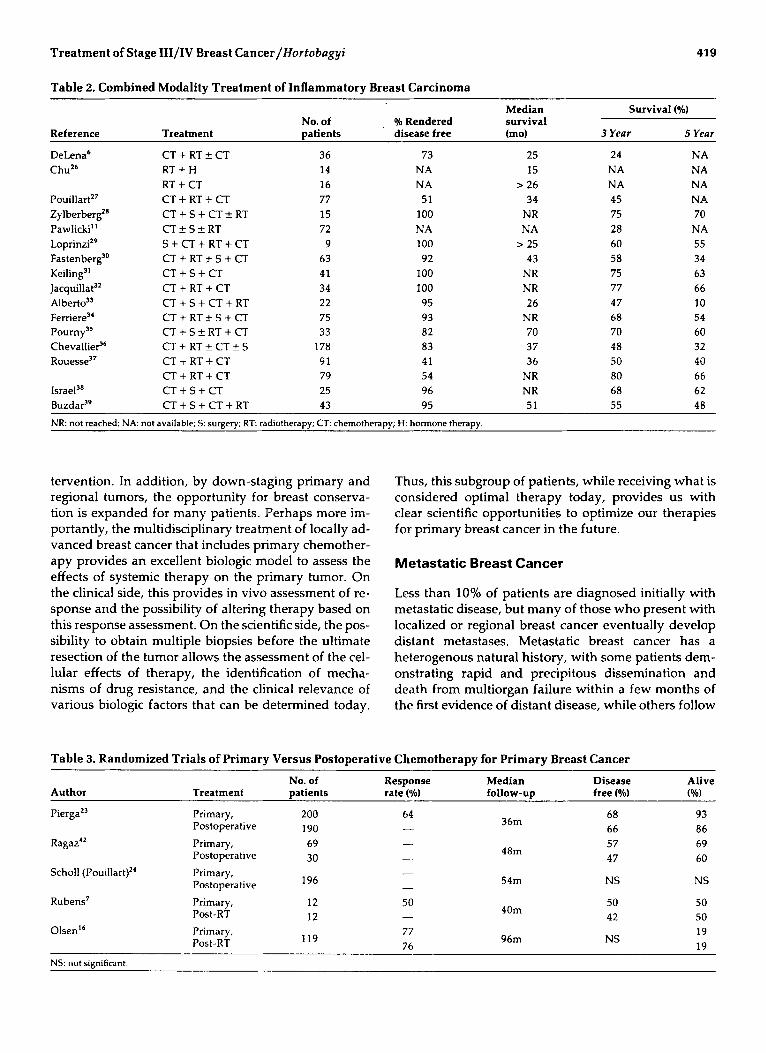
Before the advent of systemic therapy, inflammatory breast cancer was a uniformly lethal disease.' The local recurrence rate was very high, distant metastases devel- oped in the first year, and few if any patients survived beyond 2 years. Therefore, the most dramatic demon- stration of the efficacy of combined modality therapy that includes primary chemotherapy was observed in the group of patients with inflammatory breast cancer (Table 2).6.2h-39 As in the noninflammatory subgroup, primary chemotherapy produced objective response rates of 60-80% in patients with inflammatory breast cancer, and initially, almost all patients could be ren- dered disease free with limited surgery and standard
doses and the fractionation schedules of radiation ther- a~y . ' ,~O In contrast with historic experience, 3-year sur- vival rates in the 40-70% range have been reported consistently, and at 5 years, 30-50% of patients remain alive, most of them free of metastatic breast cancer. In the few clinical trials with longer follow-up, this per- centage (30-50%) of patients remains disease free 10 and 15 years later.4'
Survival Effects
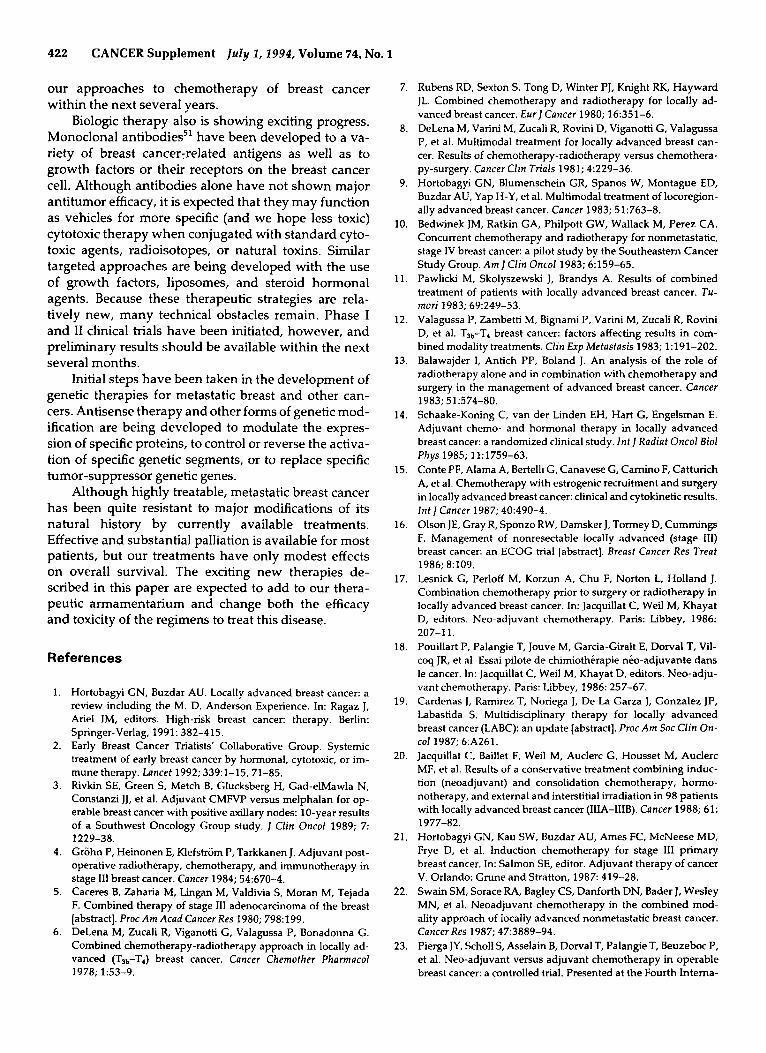
Because most of the reports about multidisciplinary treatment of locally advanced breast cancer derive from open Phase I1 trials, the comments dn the possible sur- vival effects are tentative at best. Only mature pro- spective randomized trials will determine the survival benefit of these regimens. The results of open Phase I1 trials, however, compare favorably to historic controls and literature controls, suggesting a higher survival rate at 5 and 10 years, especially in the worst prognostic sub- groups (patients with inflammatory breast cancer,4o su- praclavicular lymph node involvement,' and T4 pri- mary lesions). It is evident from the earlier discussion that patients with Stage I11 breast cancer treated with local therapy followed by postoperative adjuvant che- motherapy have a survival rate superior to those treated with local therapies alone. The controversy relates to whether preoperative chemotherapy or postoperative chemotherapy offers superior survival when used in multidisciplinary treatment (Table 3).7*'6,23v24,42 From the available evidence, it is clear that the results obtained with primary chemotherapy are certainly equivalent, and possibly superior, to those obtained with postoper- ative chemotherapy in the randomized trials reported to date. In most of these trials, however, trends in favor of primary chemotherapy do not reach statistical sig- nificance. Only better designed trials with adequate power and longer follow-up will define the magnitude of the survival benefit obtained.
Dose Intensification
One of the research directions to improve the survival of patients with locally advanced breast cancer is dose intensification of primary or postoperative (postradio- therapy) chemotherapy. Several reports of open Phase I1 trials have suggested an early benefit in disease free survival.43 No definite survival benefits have been re- ported, however, and comparative trials are necessary to assess the relative value of dose intensification in this group of patients.
Comments
Neoadjuvant chemotherapy permits optimal local con- trol with less radical surgical and radiotherapeutic in-
Treatment of Stage III/IV Breast Cancer/ffottobagyi 41 9
Table 2. Combined Modality Treatment of Inflammatory Breast Carcinoma
Median Survival (%) No. of 016 Rendered survival
Reference Treatment Datients disease free (mol 3 Year 5 Year
DeLena6 CT + RT rf: CT 36 73 25 24 NA ChuZ6 R T + H 14 NA I5 NA NA
RT + CT 16 NA > 26 NA NA P~uiIIart’~ CT + RT + CT 77 51 34 45 NA Zylberberg” CT + S + CT k RT 15 100 NR 75 70 Pawlicki” CT rf: S rf: RT 72 NA NA 28 NA LoprinziZ9 S + CT + RT + CT 9 100 > 25 60 55 Fastenberg” CT + RT f S + CT 63 92 43 58 34 Keiling” CT + S + CT 41 100 NR 75 63 J a ~ q u i l l a t ~ ~ CT + RT + CT 34 100 NR 77 66 Alberto’’ CT + S + CT + RT 22 95 26 47 10 Femere3‘ CT + R T f S + CT 75 93 NR 68 54 P ~ u r n y ~ ~ CT + S rf: RT + CT 33 82 70 70 60 Chevallie? C T + R T * C T + S 178 83 37 48 32 Rouesse3’ CT + RT + CT 91 41 36 50 40
CT + RT + CT 79 54 NR 80 66 Israel3’ CT + S + CT 25 96 NR 68 62 Buzda?’ CT + S + CT + RT 43 95 51 55 48 NR: not reached; NA: not available; 5: surgery; R T radiotherapy; C T chemotherapy; H: hormone therapy.
tervention. In addition, by down-staging primary and regional tumors, the opportunity for breast conserva- tion is expanded for many patients. Perhaps more im- portantly, the multidisciplinary treatment of locally ad- vanced breast cancer that includes primary chemother- apy provides an excellent biologic model to assess the effects of systemic therapy on the primary tumor. On the clinical side, this provides in vivo assessment of re- sponse and the possibility of altering therapy based on this response assessment. On the scientific side, the pos- sibility to obtain multiple biopsies before the ultimate resection of the tumor allows the assessment of the cel- lular effects of therapy, the identification of mecha- nisms of drug resistance, and the clinical relevance of various biologic factors that can be determined today.
Thus, this subgroup of patients, while receiving what is considered optimal therapy today, provides us with clear scientific opportunities to optimize our therapies for primary breast cancer in the future.
Metastatic Breast Cancer
Less than 10% of patients are diagnosed initially with metastatic disease, but many of those who present with localized or regional breast cancer eventually develop distant metastases. Metastatic breast cancer has a heterogenous natural history, with some patients dem- onstrating rapid and precipitous dissemination and death from multiorgan failure within a few months of the first evidence of distant disease, while others follow
Table 3. Randomized Trials of Primary Versus Postoperative Chemotherapy for Primary Breast Cancer
Author Treatment patients rate (46) follow-up free (%) (%I
PiergaZ3 Primary, 200 64 Postoperative 190 -
No. of Response Median Disease Alive
68 93 66 86
36m
Ragaz”
Scholl (Pouillart)”
Rubens7
- Primary, 69 Postoperative 30 - Primary, Postoperative 196
Primary, 12 50 - Post-RT 12
48m
54m
40m
57 47
NS
50 42
69 60
NS
50 50 19 19
96m NS 77 76
119 OlsenI6 Primary,
Post-RT . - ..
NS: not significant.
420 CANCER Supplement July I , 1994, Volume 74, No. 1
Chemotherapy / 'I
No Response Response - HDCT Consolidation
+/- ASCS + GF Continue to Second-Line
Chemotherapy Best Response + 2-6 Cycles
Observation
I
I
1
Low Tumor Burden Good Performance Status
Long DFI, ER (+)
Hormone Therapy 1 - - - - - - - - -
Response ' No Response
Chemotherapy 1 1
Hormone Therapy I I 1 Progression
HDCT +/-
ASCS
GF
Hormone Therapy
+
1
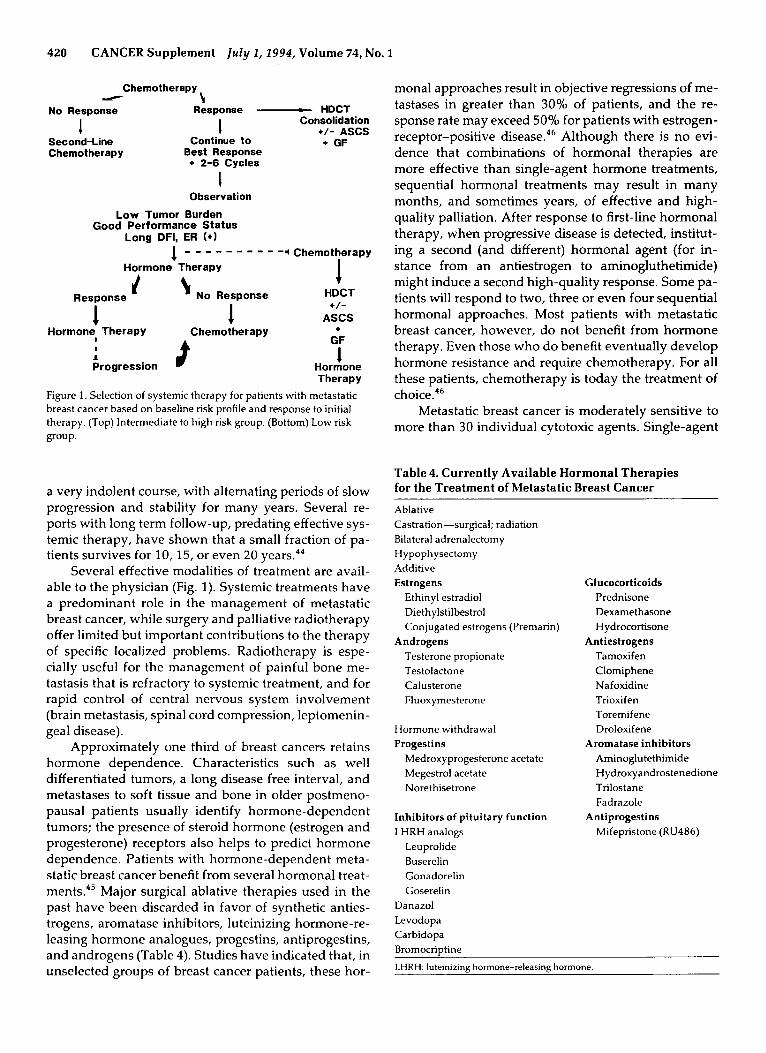
Figure 1 . Selection of systemic therapy for patients with metastatic breast cancer based on baseline risk profile and response to initial therapy. (Top) Intermediate to high risk group. (Bottom) Low risk group.
a very indolent course, with alternating periods of slow progression and stability for many years. Several re- ports with long term follow-up, predating effective sys- temic therapy, have shown that a small fraction of pa- tients survives for 10, 15, or even 20 years.44
Several effective modalities of treatment are avail- able to the physician (Fig. 1). Systemic treatments have a predominant role in the management of metastatic breast cancer, while surgery and palliative radiotherapy offer limited but important contributions to the therapy of specific localized problems. Radiotherapy is espe- cially useful for the management of painful bone me- tastasis that is refractory to systemic treatment, and for rapid control of central nervous system involvement (brain metastasis, spinal cord compression, leptomenin- geal disease).
Approximately one third of breast cancers retains hormone dependence. Characteristics such as well differentiated tumors, a long disease free interval, and metastases to soft tissue and bone in older postmeno- pausal patients usually identify hormone-dependent tumors; the presence of steroid hormone (estrogen and progesterone) receptors also helps to predict hormone dependence. Patients with hormone-dependent meta- static breast cancer benefit from several hormonal treat- m e n t ~ . ~ ~ Major surgical ablative therapies used in the past have been discarded in favor of synthetic anties- trogens, aromatase inhibitors, luteinizing hormone-re- leasing hormone analogues, progestins, antiprogestins, and androgens (Table 4). Studies have indicated that, in unselected groups of breast cancer patients, these hor-
monal approaches result in objective regressions of me- tastases in greater than 30% of patients, and the re- sponse rate may exceed 50% for patients with estrogen- receptor-positive disease.46 Although there is no evi- dence that combinations of hormonal therapies are more effective than single-agent hormone treatments, sequential hormonal treatments may result in many months, and sometimes years, of effective and high- quality palliation. After response to first-line hormonal therapy, when progressive disease is detected, institut- ing a second (and different) hormonal agent (for in- stance from an antiestrogen to aminogluthetimide) might induce a second high-quality response. Some pa- tients will respond to two, three or even four sequential hormonal approaches. Most patients with metastatic breast cancer, however, do not benefit from hormone therapy. Even those who do benefit eventually develop hormone resistance and require chemotherapy. For all these patients, chemotherapy is today the treatment of choice.46
Metastatic breast cancer is moderately sensitive to more than 30 individual cytotoxic agents. Single-agent
Table 4. Currently Available Hormonal Therapies for the Treatment of Metastatic Breast Cancer
Ablative Castration-surgical; radiation Bilateral adrenalectomy Hypoph ysectomy Additive Estrogens
Ethinyl estradiol Diethylstilbestrol Conjugated estrogens (Premarin)
Testerone propionate Testolactone Calusterone Fluoxymesterone
Androgens
Hormone withdrawal Progestins
Medroxyprogesterone acetate Megestrol acetate Norethisetrone
Inhibitors of pituitary function LHRH analogs
Leuprolide Buserelin Gonadorelin Goserelin
Danazol Levodopa Carbidopa Bromocriptine
Glucocorticoids Prednisone Dexamethasone Hydrocortisone
Antiestrogens Tamoxifen Clomiphene Nafoxidine Trioxi fen Toremifene Droloxifene
Aromatase inhibitors Aminoglutethimide H ydroxyandrostenedione Trilostane Fadrazole
Antiprogestins Mifepristone (RU486)
LHRH: luteinizing hormone-releasing hormone.

Treatment of Stage III/IV Breast Cancer/Hortobagyi 421
therapy, however, is effective in only 20-30% of pa- tients, with the notable exception of the anthracyclines and some of the recently introduced cytotoxic agents (vide infra). Responses to single-agent therapy are par- tial and of short duration. Several effective combina- tions have been developed. The most commonly used consist of cyclophosphamide, methotrexate, and fluo- rouracil (CMF), and cyclophosphamide, doxorubicin (or epirubicin), and 5-fluorouracil. Regimens containing anthracycline are most effective in producing objective remissions, including complete remissions, and re- mission durations with this type of therapy last a few months longer than those obtained with other combi- nations. These combinations also produce somewhat increased toxic effects, especially alopecia. Response rates with combination chemotherapy vary from 50- 8070, depending on patient and tumor characteristics, the dose intensity of the regimen, and the criteria for evaluation of response. The average duration of re- sponse for metastatic breast cancer treated with combi- nation chemotherapy varies from 7 to 14 months, being longer for patients who achieve a complete clinical re- mission (12-18 months). The median survival after combination chemotherapy has been reported to be be- tween 15 and 24 months. Complete remissions occur in only 10-25% of patients; while most patients experi- ence a relapse, a small percentage of them (less than 10%) survive with an unmaintained complete re- mission for periods that may exceed 15 years.47
Over the last decade, dose intensity has been iden- tified as a major variable in the efficacy of cytotoxic che- m ~ t h e r a p y . ~ ~ Retrospective analyses, and prospective randomized trials have confirmed the results of preclin- ical experiments and demonstrated that higher dose in- tensity often (but not always) produces higher re- mission rates and, in the case of combination chemo- therapy, a prolonged response duration and survival. More recently, the appearance of effective hematopoi- etic support to counteract the severe myelosuppressive effects of high dose chemotherapy has allowed the ad- ministration of cytotoxic therapy at a significantly in- creased dose intensity. Doses that exceed the standard by 4- to 20-fold have been administered safely to pa- tients with metastatic breast cancer in recent years. Al- though high dose chemotherapy administered to pa- tients with refractory metastatic breast cancer produces higher than expected overall response rates, sometimes approaching 50%, complete responses are rare, re- mission durations are short, and no survival benefit is detected. Furthermore, the morbidity and mortality of these regimens for this group of patients are substantial. When high dose combination chemotherapy is used as front-line therapy for patients with metastatic breast cancer, overall response rates approach 90%, complete remission rates exceed SO%, and remission durations are similar to those achieved with longer duration of
Table 5. New Cytotoxic Agents Under Clinical Evaluation for the Treatment of Metastatic Breast Cancer
Adozelesin (U-73795) Amonafide Anthrapyrazoles Camptothecin
Cemcitabine Miltefosine Rhizoxin Taxanes Vinorelbine
CPT- 1 1
standard dose chemotherapy. Some centers recently have reported that up to 20-25% of patients so treated remain in an unmaintained complete remission 2 and 3 years after the administration of high dose chemother- apy. Several recent reports demonstrated that high dose chemotherapy used as consolidation treatment of ob- jective remissions obtained by standard dose therapy results in somewhat higher complete remission rates, although the survival benefit of this approach remains to be proven. Currently, several prospective random- ized trials are being conducted to evaluate the relative benefits and toxicity of high dose versus standard dose combination chemotherapy for metastatic breast can- cer.
The last 3 years have witnessed the appearance of several new and exciting cytotoxic agents that already are demonstrating antitumor efficacy against metastatic breast cancer (Table 5).49 The taxanes (paclitaxel and docetaxel) have been evaluated more extensively than some of the others. In patients with previously un- treated or minimally treated metastatic breast cancer, paclitaxel produces objective responses in 50-60'30 of patients, including some with clear-cut resistance to an- thracyclines, previously the "gold standard" for the treatment of this tumor.50 Similarly encouraging pre- liminary results have been found with docetaxel, sug- gesting that 60-70% of previously untreated patients achieve an objective response and 40-50% of pre- viously treated patients with metastatic breast cancer also respond favorably to this agent. Currently, these two drugs are being incorporated into combination che- motherapy. Vinorelbine, a new vinca alkaloid, has been shown to produce objective remissions in 40-50% of patients with untreated metastatic breast cancer and 20-30% of those with refractory metastatic disease. Amonafide and several elliptinium derivatives have demonstrated modest activity, in the 20% range. The anthrapyrazoles, derived from the antraquinone moi- ety, have shown highly promising activity in limited Phase I1 trials. It is very probable that the development of these various exciting new cytotoxic agents will affect
422 CANCER Supplement IuZy I , 2994, Volume 74, No. 1
our approaches to chemotherapy of breast cancer within the next several years.
Biologic therapy also is showing exciting progress. Monoclonal antibodies51 have been developed to a va- riety of breast cancer:related antigens as well as to growth factors or their receptors on the breast cancer cell. Although antibodies alone have not shown major antitumor efficacy, it is expected that they may function as vehicles for more specific (and we hope less toxic) cytotoxic therapy when conjugated with standard cyto- toxic agents, radioisotopes, or natural toxins. Similar targeted approaches are being developed with the use of growth factors, liposomes, and steroid hormonal agents. Because these therapeutic strategies are rela- tively new, many technical obstacles remain. Phase I and I1 clinical trials have been initiated, however, and preliminary results should be available within the next several months.
Initial steps have been taken in the development of genetic therapies for metastatic breast and other can- cers. Antisense therapy and other forms of genetic mod- ification are being developed to modulate the expres- sion of specific proteins, to control or reverse the activa- tion of specific genetic segments, or to replace specific tumor-suppressor genetic genes.
Although highly treatable, metastatic breast cancer has been quite resistant to major modifications of its natural history by currently available treatments. Effective and substantial palliation is available for most patients, but our treatments have only modest effects on overall survival. The exciting new therapies de- scribed in this paper are expected to add to our thera- peutic armamentarium and change both the efficacy and toxicity of the regimens to treat this disease.
References
1.
2.
3.
4.
5.
6.
Hortobagyi GN, Buzdar AU. Locally advanced breast cancer: a review including the M. D. Anderson Experience. In: Ragaz J, Ariel IM, editors. High-risk breast cancer: therapy. Berlin: Springer-Verlag, 1991: 382-415. Early Breast Cancer Trialists' Collaborative Group. Systemic treatment of early breast cancer by hormonal, cytotoxic, or im- mune therapy. Lancet 1992; 339:l-15,7145. Rivkin SE, Green S, Metch B, Glucksberg H, Gad-elMawla N, Constanzi JJ, et al. Adjuvant CMFVP versus melphalan for op- erable breast cancer with positive axillary nodes: 10-year results of a Southwest Oncology Group study. J Clin Oncol 1989; 7:
Grohn P, Heinonen E, Klefstrom P, Tarkkanen J. Adjuvant post- operative radiotherapy, chemotherapy, and immunotherapy in stage I11 breast cancer. Cancer 1984; 54:670-4. Caceres B, Zaharia M, Lingan M, Valdivia S, Moran M, Tejada F. Combined therapy of stage 111 adenocarcinoma of the breast [abstract]. Proc Am Acad Cancer Res 1980; 798:199. DeLena M, Zucali R, Viganotti G, Valagussa P, Bonadonna G. Combined chemotherapy-radiotherapy approach in locally ad- vanced (TJb-T4) breast cancer. Cancer Chemother Pharmacol
1229-38.
1978; 1:53-9.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
Rubens RD, Sexton S, Tong D, Winter PJ, Knight RK, Hayward JL. Combined chemotherapy and radiotherapy for locally ad- vanced breast cancer. EurJ Cancer 1980; 16:351-6. DeLena M, Varini M, Zucali R, Rovini D, Viganotti G, Valagussa P, et al. Multimodal treatment for locally advanced breast can- cer. Results of chemotherapy-radiotherapy versus chemothera- py-surgery. Cancer Clin Trials 1981; 429-36. Hortobagyi GN, Blumenschein GR, Spanos W, Montague ED, Buzdar AU, Yap H-Y, et al. Multimodal treatment of locoregion- ally advanced breast cancer. Cancer 1983; 51:763-8. Bedwinek JM, Ratkin GA, Philpott GW, Wallack M, Perez CA. Concurrent chemotherapy and radiotherapy for nonmetastatic, stage IV breast cancer: a pilot study by the Southeastern Cancer Study Group. Am J Clin Oncol 1983; 6:159-65. Pawlicki M, Skolyszewski J, Brandys A. Results of combined treatment of patients with locally advanced breast cancer. Tu- mori 1983; 69249-53. Valagussa P, Zambetti M, Bignami P, Varini M, Zucali R, Rovini D, et al. Tab-T4 breast cancer: factors affecting results in com- bined modality treatments. Clin Exp Metastasis 1983; 1:191-202. Balawajder I, Antich PP, Boland J. An analysis of the role of radiotherapy alone and in combination with chemotherapy and surgery in the management of advanced breast cancer. Cancer
Schaake-Koning C, van der Linden EH, Hart G, Engelsman E. Adjuvant chemo- and hormonal therapy in locally advanced breast cancer: a randomized clinical study. Int J Radiat Oncol B i d
Conte PF, Alama A, Bertelli G, Canavese G, Camino F, Catturich A, et al. Chemotherapy with estrogenic recruitment and surgery in locally advanced breast cancer: clinical and cytokinetic results. Znt ] Cancer 1987; 40:490-4. Olson JE, Gray R, Sponzo RW, Damsker J, Tormey D, Cummings F. Management of nonresectable locally advanced (stage 111) breast cancer: an ECOG trial [abstract]. Breast Cancer Res Treat 1986; 8:109. Lesnick G, Perloff M, Korzun A, Chu F, Norton L, Holland J. Combination chemotherapy prior to surgery or radiotherapy in locally advanced breast cancer. In: Jacquillat C, Weil M, Khayat D, editors. Neo-adjuvant chemotherapy. Paris: Libbey, 1986:
Pouillart P, Palangie T, Jouve M, Garcia-Giralt E, Dorval T, Vil- coq JR, et al. Essai pilote de chimioth6rapie nho-adjuvante dans le cancer. In: Jacquillat C, Weil M, Khayat D, editors. Neo-adju- vant chemotherapy. Paris: Libbey, 1986: 257-67. Cardenas J, Ramirez T, Noriega J, De La Garza J, Gonzalez JP, Labastida S. Multidisciplinary therapy for locally advanced breast cancer (LABC): an update [abstract]. Proc Am Soc Clin On- col 1987; 6:A261. Jacquillat C, Baillet F, Weil M, Auclerc G, Housset M, Auclerc MF, et al. Results of a conservative treatment combining induc- tion (neoadjuvant) and consolidation chemotherapy, hormo- notherapy, and external and interstitial irradiation in 98 patients with locally advanced breast cancer (IIIA-IIIB). Cancer 1988; 61:
Hortobagyi GN, Kau SW, Buzdar AU, Ames FC, McNeese MD, Frye D, et al. Induction chemotherapy for stage Ill primary breast cancer. In: Salmon SE, editor. Adjuvant therapy of cancer V. Orlando: Grune and Stratton, 1987 419-28. Swain SM, Sorace RA, Bagley CS, Danforth DN, Bader J, Wesley MN, et al. Neoadjuvant chemotherapy in the combined mod- ality approach of locally advanced nonmetastatic breast cancer. Cancer Res 1987; 47:3889-94. Pierga JY, Scholl S, Asselain B, Dorval T, Palangie T, Beuzeboc P, et al. Neo-adjuvant versus adjuvant chemotherapy in operable breast cancer: a controlled trial. Presented at the Fourth Intema-
1983; 51:574-80.
Phys 1985; 11:1759-63.
207-1 1.
1977-82.
Treatment of Stage III/IV Breast Cancer/Hortobagyi 423
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
tional Conference on Adjuvant Therapy of Primary Breast Can- cer; 1992 Feb 26-29; St. Gallen: 56. Scholl SM, Asselain B, Beuzeboc P, Dorval T, Garcia-Giralt E, Jouve M, et al. lmproved survival rates following first line che- motherapy in operable breast cancer: 4 year results of a random- ized hial (S6). Presented at the Fourth International Congress on Anti-Cancer Chemotherapy; 1993 Feb 2-5; Paris, France: 65. Bonadonna G, Veronesi U, Brambilla C, Ferrari L, Luini A, Greco M, et al. Primary chemotherapy to avoid mastectomy in tumors with diameters of three centimeters or more. ] Nut1 Cancer Insf
Chu AN, Wood WC, Doucette JA. Inflammatory breast carci- noma treated by radical radiotherapy. Cancer 1980; 452730-7. Pouillart P, Palangie T, Jouve M, Garcia-Giralt E, Vilcoq JR, Ba- taini JP, et al. Cancer inflammatoire du sein trait; par une asso- ciation de chimiothirapie et d‘irradiation: risultats d’un essai randornisi Ctudiant le role d’une immunothirapie par le BCG. Paris: Masson, 1981: 171-86. Zylberberg B, Salat-Baroux J, Ravina JH, Dormont D, Amiel JP, Biebold P, et al. Initial chemoimmunotherapy in inflammatory carcinoma of the breast. Cancer 1982; 49:1537-43. Loprinzi CL, Carbone PP, Tormey DC, Rosenbaum PR, Cald- well W, Kline JC, et al. Aggressive combined modality therapy for advanced local-regional breast carcinoma. J Clin Oncol 1984;
Fastenberg NA, Buzdar AU, Montague ED, Jessup JM, Martin RG, Hortobagyi GN, et al. Management of inflammatory carci- noma of the breast: a combined modality approach. Am J Clin Oncol 1985; 8:134-41. Keiling R, Guiochet N, Calderoli H, Hurteloup P, Krzisch C. Pre- operative chemotherapy in the treatment of inflammatory breast cancer. In: Wagner DJT, Blijham GH, Smeets JBE, Wils JA, editors. Primary chemotherapy in cancer medicine. New York: Liss, 1985:
Jacquillat C, Weil M, Auclerc G, Auclerc MF, Sellami M, Khayat D, et al. Neo-adjuvant chemotherapy in the conservative man- agement of breast cancers: study on 205 patients. In: Jacquillat C, Weil M, Khayat D, editors. Neo-adjuvant chemotherapy. Paris: Libbey, 1986: 197-206. Albert0 P, Schafer P, Mermillod B, Rosset G, Pipard G, Obra- dovic D, et al. Traitement combin; des cancers inflammatoires due sein par chimiothirapie suivie de chirurgie et de radiothhra- pie. In: Jacquillat C, Weil M, Khayat D, editors. Neo-adjuvant chemotherapy. Paris: Libbey, 1986: 237-42. Femere JP, Bignon YJ, Legros M, Dauplat j, Achard JL, Travade A, et al. Rbsultats du traitement des cancers inflammatoires due sein par une association thbrapeutique comportant une chimi- oth&apie initiale. In: Jacquillat C, Weil M, Khayat D, editors. Neo-adjuvant chemotherapy. Pans: Libbey, 1986: 271-7. Pourny C, Nguyen TD, Nzengu B, Cattan A. Traitements par chimiothirapie premiere de cancers du sein MO, localement ad- vances (T3-T4) ou s’accompagnant de signes inflammatoires lo- caux. In: Jacquillat C, Weil M, Khayat D, editors. Neo-adjuvant chemotherapy. Paris: Libbey, 1986: 293-9. Chevallier B, Bastit P, Graic Y, Menard JF, Dauce JP, Julien JP, et al. The Centre H. Becquerel studies in inflammatory non meta-
1990; 82~1539-45.
2: 157-63.
95-104.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
static breast cancer: combined modality approach in 178 patients. B r J Cancer 1993; 67:594-601. Rouesse J, Friedman S, Sarrazin D, Mouriesse H, le Chevalier T, Amagada R, et al. Primary chemotherapy in the treatment of inflammatory breast carcinoma: a study of 230 cases from the lnstitut Gustave-Roussy. ] Clin Oncol 1986; 4:1765-71. Israel L, Breau JL, Morere JF. Two years of high-dose cyclophos- phamide and 5-fluorourad followed by surgery after 3 months for acute inflammatory breast carcinomas: a phase I1 study of 25 cases with a median follow-up of 35 months. Cancer 1986; 57:24-8. Buzdar A, Marcus C, Hortobagyi G, Ames F, Montague E. Com- bined modality approach in inflammatory carcinoma of the breast-preliminary results of a prospective study. Presented at the 15th International Congress of Chemotherapy; 1987 July 19-24; Istanbul, Turkey: 169. Jaiyesimi IA, Buzdar AU, Hortobagyi GN. lnflammatory breast cancer: a review. ] Clin Oncol 1992; 10:1014-24. Koh EH, Buzdar AU, Ames FC, Singletary SE, McNeese MD, Frye D, et al. lnflammatory carcinoma of the breast: results of a combined-modality approach-M. D. Anderson Cancer Center experience. Cancer Chemofher Pharmacol 1990; 27:94-100. Ragaz J, Baird B, Rebbeck P, Coldie J, Coldman A, Basco V. Early results of the British Columbia breast cancer preoperative (neo-adjuvant) chemotherapy trial. In: Banzet P, Holland JF, Khayat D, Weil M, editors. Neo-adjuvant chemotherapy. Paris: Springer-Verlag, 1991: 186-92. Antman KH. Dose-intensive therapy in breast cancer. In: Armi- tage JO, Antman KH, editors. High-dose cancer therapy. Balti- more, MD: Williams & Wilkins, 1992: 701-18. Bloom HJB, Richardson WW, Hames EJ. Natural history of un- treated breast cancer (1805-1933): comparison of untreated and treated cases according to histological grade of malignancy. BM]
Buzdar AU. Current status of endocrine treatment of carcinoma of the breast. Semin Surg Oncol 1990; 6:77-82. Henderson IC. Principles in the management of metastatic dis- ease. In: Hams JR, Helman S, Henderson IC, et al., edi- tors. Breast diseases. 2nd ed. Philadelphia: Lippincott, 1991:
Hortobagyi GN, Frye D, Buzdar AU, Hug V, Fraschini G. Com- plete remissions in metastatic breast cancer: A thirteen year fol- low-up report. Proceedings of the 24th Annual Meeting of the American Society of Clinical Oncology; 1988 May 22-24; New OrIeans:37. Hortobagyi GN. The importance of dose-response in cytotoxic therapy for breast cancer. In: Henderson IC, Borden EC, editors. Advances in breast cancer treatment. London: Mediscript, 1990:
Hortobagyi GN. Overview of new treatments for breast cancer. Breast Cancer Res Treat 1992; 21:3-13. Holmes FA, Walters RS, Theriault RL, Forman AD, Newton LK, Raber MN, et al. Phase 11 trial of taxol, an active drug in the treatment of metastatic breast cancer. ]Nut1 Cancer Inst 1991; 83:
Waldmann TA. Monoclonal antibodies in diagnosis and ther- apy. Science 1991; 252:1657-62.
1962; 2213-21.
547-677.
47-69.
1797-805.