multidisciplinary head and neck cancer clinic and adherence with speech pathology
TRANSCRIPT

The LaryngoscopeVC 2011 The American Laryngological,Rhinological and Otological Society, Inc.
Multidisciplinary Head and Neck Cancer Clinic and Adherence withSpeech Pathology
Heather Starmer, MA, CCC-SLP; Giuseppe Sanguineti, MD; Shanthi Marur, MD; Christine G. Gourin, MD
Objectives: To determine the effect of referral patterns on compliance with speech–language pathology (SLP) treatmentof voice and swallowing difficulties in patients with head and neck cancer (HNCA).
Study Design: Retrospective cohort study.Methods: Patients with newly diagnosed oropharyngeal HNCA referred for pretreatment SLP evaluation comprised the
study population. Compliance was measured by participation in SLP therapy during and after head and neck treatment, aswell as by the number of missed and completed visits. Outcomes were compared between patients who were initially eval-uated through the multidisciplinary clinic and those evaluated outside of the multidisciplinary clinic format.
Results: The final study sample included 118 individuals with oropharyngeal tumors. All patients were treated with pri-mary radiotherapy with or without chemotherapy. Patients evaluated initially through the multidisciplinary clinic had moreSLP visits than those who did not participate in the multidisciplinary clinic (mean ¼ 1.8 vs. 0.2, P <.0001). Participation inSLP treatment was significantly greater for patients �60 years of age (odds ratio [OR] ¼ 2.4, P ¼.032) and for patients whoparticipated in the multidisciplinary clinic (OR ¼ 19.3, P <.0001). Tumor stage, sex, race, marital status, and insurance statuswere not associated with patient compliance. Multivariate analysis revealed that participation in a multidisciplinary clinic wasthe only significant variable associated with SLP treatment compliance (OR ¼ 12.9, P <.0001), after controlling for all othervariables.
Conclusions: Patients evaluated in a multidisciplinary clinic are more likely to comply with SLP treatmentrecommendations.
Key Words: Multidisciplinary care, head and neck cancer, patient compliance.Level of evidence: 4.
Laryngoscope, 121:2131–2135, 2011
INTRODUCTIONHead and neck cancer (HNCA) and its treatments
can have grave consequences for both communicationand swallowing functions. The use of radiation andchemotherapy have been beneficial in sparing removal oforgans; however, organ preservation does not necessarilyequate to preservation of function. Acute toxicities suchas xerostomia, mucositis, and dysgeusia may negativelyimpact desire to eat during, and in the weeks followingtreatment.1 This may predispose patients to overrelianceon tube feedings for nutrition and hydration and prolongtheir dependence on these devices. Patients at elevatedrisk for feeding tube dependence include those withlarger primary tumors, hypopharyngeal, and oropharyn-geal primaries, flap reconstruction, tracheostomy,chemotherapy, and increased age.2
Mounting evidence suggests that therapeutic inter-vention initiated prior to treatment may help topreserve long-term function and improve quality of life.3
Pretreatment evaluation of swallowing and communica-tion status assists in early identification of dysfunction.Additionally, during the pretreatment consultation, thespeech–language pathologist has the opportunity to pro-vide education regarding potential treatment side effectsimpacting communication and swallowing, and provideexercises and strategies to minimize their impact. Suchvisits may occur in a number of settings including theoutpatient speech–language pathology (SLP) clinic, dur-ing an inpatient admission, or as part of amultidisciplinary team evaluation.
Patient compliance with treatment recommenda-tions is a widely acknowledged issue in modernmedicine. Factors that have been associated with non-compliance include insurance issues, logistic barriers(distance, transportation, time, and need for interpreterservices), patient apathy, and resolution or lack of symp-toms.4,5 Noncompliance has been shown in some realmsto contribute to suboptimal patient outcomes.6 Addition-ally, missed visits have a negative economic impact onthe medical system leading to lost revenue and wastedclinician time. Determining ways to improve compliancehas the potential to optimize both patient outcomes andefficiency of care. We sought to evaluate the impact on amultidisciplinary care model on patient compliance withSLP treatment recommendations.
From the Department of Otolaryngology—Head and Neck Surgery(H.S., C.G.), Department of Radiation Oncology and Molecular RadiationSciences (G.S.), Department of Medical Oncology (S.M.), Johns HopkinsMedical Institutions, Baltimore, Maryland, U.S.A.
Editor’s Note: This Manuscript was accepted for publication Janu-ary 8, 2011.
The authors have no financial disclosures for this article.The authors have no conflicts of interest to declare.
Send correspondence to Dr. Heather Starmer, Department of Oto-laryngology—Head and Neck Surgery, Johns Hopkins Medical Institu-tions, 601 N. Caroline Street, Suite 6260, Baltimore, MD 21287. E-mail:[email protected]
DOI: 10.1002/lary.21746
Laryngoscope 121: October 2011 Starmer et al.: Multidisciplinary Care and Patient Compliance
2131

MATERIALS AND METHODSPatients with newly diagnosed oropharyngeal HNCA
referred for pretreatment SLP evaluation comprised the studypopulation. Medical records of individuals diagnosed with oro-pharyngeal cancers between 2006 and 2010 were reviewed incompliance with the Health Insurance Portability and Account-ability Act and in accord with previous approval by the JohnsHopkins institutional review board. All patients received theironcologic treatment at Johns Hopkins. Compliance was meas-ured by participation in SLP therapy during and after head andneck treatment, as well as by the number of missed and com-pleted visits. Outcomes were compared between patients whowere initially evaluated through the multidisciplinary head andneck clinic and those evaluated outside of the multidisciplinaryclinic format. During the study time period, standard of careincluded SLP referral for all patients undergoing radiation ther-apy for HNCA.
For those individuals seen in the multidisciplinary clinic,thorough swallowing and speech/voice assessments were con-ducted, and the patient was educated regarding the role of theSLP on the team. Assessment included subjective analysis ofspeech and voice, measurement of maximal interincisal opening,and a fiberoptic endoscopic evaluation of swallowing (FEES). Forthose patients not seen in the multidisciplinary setting, the oncolo-gist (medical, surgical, or radiation) informed the patient of theneed to meet with the SLP prior to treatment, and office staff con-tacted patients to schedule appointments prior to initiation ofradiation. Referring physicians all participate in the Johns Hop-kins multidisciplinary clinic on a rotating basis. The standard SLPtreatment protocol included pretreatment assessment, follow upduring treatment, and posttreatment evaluations and intervention.Whenever possible, appointments were coordinated with other pro-vider appointments to minimize travel requirements and facilitatecompliance. Patient demographic factors (age, sex, race, maritalstatus, insurance status, and T stage) and clinical outcomes wereanalyzed. Participation was measured in regard to whether thepatient was ever seen by the SLP, the number of completed visits(as documented by notes in the medical record), and the numberof missed visits (determined through review of outpatient schedul-ing program data). Appointments were made by the SLP officecoordinator, and patients were notified by telephone as well as byreminder mailings.
Data were analyzed using Stata 10 (StataCorp, CollegeStation, TX). Standard statistical analysis, including theunpaired t-test for continuous data, and chi-square tests for cat-egoric data were used to evaluate factors associated withreferral and SLP participation categories. The Mann-Whitneytest was used to evaluate associations with the number of SLPvisits, which were not normally distributed. Age categorieswere created based on the results of Lowess smoothed regres-sion analysis. Multiple logistic regression analysis was used toidentify factors associated with SLP treatment compliance withcompliance as the outcome variable. Odds ratios (OR) areexpressed relative to a reference baseline category.
RESULTSThe final study sample included 118 individuals
with oropharyngeal primary tumors. There were 25 indi-viduals initially seen by the SLP in the multidisciplinaryclinic, whereas 93 were referred for SLP evaluations out-side of the multidisciplinary format. Patients werepredominantly young (79% with age <60), male (85%),White (86%), and married (75%). The majority ofpatients were insured (90%). There were no significantdifferences between the groups in regards to age, sex,
race, marital status, or insurance status (Table I). Allpatients were treated with primary radiotherapy with orwithout chemotherapy.
Adherence to SLP treatment protocols variedaccording to primary referral pattern (Table II). Patientsevaluated initially through the multidisciplinary clinichad more SLP visits than those who did not participatein the multidisciplinary clinic (mean ¼ 1.8 vs. 0.2,P <.0001). Compliance with follow-up was 80% for thoseseen initially through the multidisciplinary clinic,whereas only 17% for those who were not (as measuredby 6 participation in SLP intervention at any point).There was no significant difference in number of missedvisits according to referral pattern. On univariate analy-sis, participation in SLP treatment was significantlygreater for patients �60 years of age (OR ¼ 2.4 95% con-fidence interval [CI] ¼ 1.08–5.52, P ¼ .032) and for
TABLE I.Characteristics of Patients Evaluated in a Multidisciplinary ClinicFormat and Those Seen Outside of the Multidisciplinary Clinic.
Seen in Multi-dClinic (n ¼ 25)
OutsideReferrals(n ¼ 93) P Value
Age
<60 years 11 (44%) 68 (73.12%) .06
�60 years 14 (56%) 25 (26.88%)
Sex
Male 21 (84%) 79 (84.95%) .907
Female 4 (16%) 14 (15.05%)
Race
Caucasian 22 (88%) 80 (86.02%) .214
African American 0 (0%) 9 (9.68%)
Hispanic 1 (4%) 1 (1.08%)
Other 2 (8%) 3 (3.23%)
Marital status
Married 19 (76%) 70 (75.27%) .337
Single 4 (16%) 12 (12.90%)
Divorced 0 (0%) 8 (8.60%)
Widowed/other 2 (8%) 3 (3.23%)
Insurance status
Private insurance 15 (60%) 63 (67.74%) .518
Medicare 7 (28%) 17 (18.28%)
Medical Assistance 0 (0%) 4 (4.30%)
No insurance/self pay 3 (12%) 9 (9.68%)
T stage
T1 9 (36%) 32 (34.41%) .127
T2 12 (48%) 34 (36.56%)
T3 0 (0%) 17 (18.28%)
T4 4 (16%) 10 (10.75%)
Participation in SLP services
Yes 20 (80%) 16 (17.20%) <.0001
No 5 (20%) 77 (82.80%)
Mean number ofmissed SLP visits
0.92 1.09 .607
Mean number ofcompleted SLP visits
1.8 0.22 <.0001
SLP ¼ speech–language pathology.
Laryngoscope 121: October 2011 Starmer et al.: Multidisciplinary Care and Patient Compliance
2132
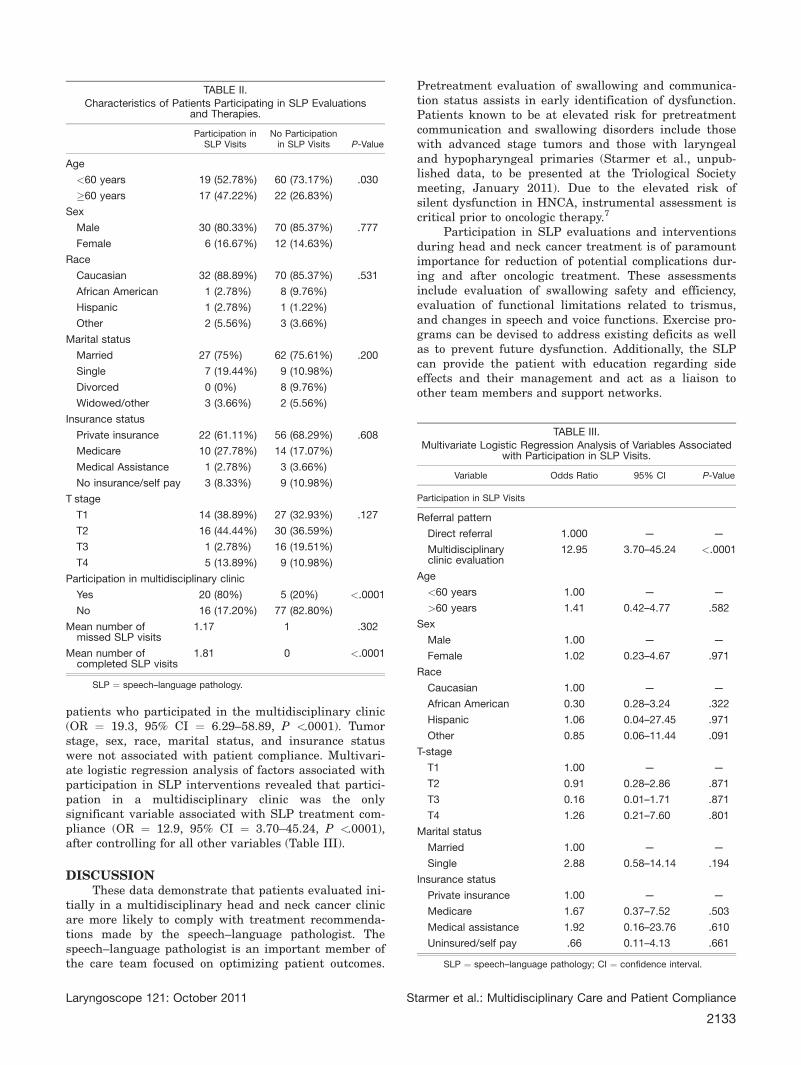
patients who participated in the multidisciplinary clinic(OR ¼ 19.3, 95% CI ¼ 6.29–58.89, P <.0001). Tumorstage, sex, race, marital status, and insurance statuswere not associated with patient compliance. Multivari-ate logistic regression analysis of factors associated withparticipation in SLP interventions revealed that partici-pation in a multidisciplinary clinic was the onlysignificant variable associated with SLP treatment com-pliance (OR ¼ 12.9, 95% CI ¼ 3.70–45.24, P <.0001),after controlling for all other variables (Table III).
DISCUSSIONThese data demonstrate that patients evaluated ini-
tially in a multidisciplinary head and neck cancer clinicare more likely to comply with treatment recommenda-tions made by the speech–language pathologist. Thespeech–language pathologist is an important member ofthe care team focused on optimizing patient outcomes.
Pretreatment evaluation of swallowing and communica-tion status assists in early identification of dysfunction.Patients known to be at elevated risk for pretreatmentcommunication and swallowing disorders include thosewith advanced stage tumors and those with laryngealand hypopharyngeal primaries (Starmer et al., unpub-lished data, to be presented at the Triological Societymeeting, January 2011). Due to the elevated risk ofsilent dysfunction in HNCA, instrumental assessment iscritical prior to oncologic therapy.7
Participation in SLP evaluations and interventionsduring head and neck cancer treatment is of paramountimportance for reduction of potential complications dur-ing and after oncologic treatment. These assessmentsinclude evaluation of swallowing safety and efficiency,evaluation of functional limitations related to trismus,and changes in speech and voice functions. Exercise pro-grams can be devised to address existing deficits as wellas to prevent future dysfunction. Additionally, the SLPcan provide the patient with education regarding sideeffects and their management and act as a liaison toother team members and support networks.
TABLE II.Characteristics of Patients Participating in SLP Evaluations
and Therapies.
Participation inSLP Visits
No Participationin SLP Visits P-Value
Age
<60 years 19 (52.78%) 60 (73.17%) .030
�60 years 17 (47.22%) 22 (26.83%)
Sex
Male 30 (80.33%) 70 (85.37%) .777
Female 6 (16.67%) 12 (14.63%)
Race
Caucasian 32 (88.89%) 70 (85.37%) .531
African American 1 (2.78%) 8 (9.76%)
Hispanic 1 (2.78%) 1 (1.22%)
Other 2 (5.56%) 3 (3.66%)
Marital status
Married 27 (75%) 62 (75.61%) .200
Single 7 (19.44%) 9 (10.98%)
Divorced 0 (0%) 8 (9.76%)
Widowed/other 3 (3.66%) 2 (5.56%)
Insurance status
Private insurance 22 (61.11%) 56 (68.29%) .608
Medicare 10 (27.78%) 14 (17.07%)
Medical Assistance 1 (2.78%) 3 (3.66%)
No insurance/self pay 3 (8.33%) 9 (10.98%)
T stage
T1 14 (38.89%) 27 (32.93%) .127
T2 16 (44.44%) 30 (36.59%)
T3 1 (2.78%) 16 (19.51%)
T4 5 (13.89%) 9 (10.98%)
Participation in multidisciplinary clinic
Yes 20 (80%) 5 (20%) <.0001
No 16 (17.20%) 77 (82.80%)
Mean number ofmissed SLP visits
1.17 1 .302
Mean number ofcompleted SLP visits
1.81 0 <.0001
SLP ¼ speech–language pathology.
TABLE III.
Multivariate Logistic Regression Analysis of Variables Associatedwith Participation in SLP Visits.
Variable Odds Ratio 95% CI P-Value
Participation in SLP Visits
Referral pattern
Direct referral 1.000 — —
Multidisciplinaryclinic evaluation
12.95 3.70–45.24 <.0001
Age
<60 years 1.00 — —
>60 years 1.41 0.42–4.77 .582
Sex
Male 1.00 — —
Female 1.02 0.23–4.67 .971
Race
Caucasian 1.00 — —
African American 0.30 0.28–3.24 .322
Hispanic 1.06 0.04–27.45 .971
Other 0.85 0.06–11.44 .091
T-stage
T1 1.00 — —
T2 0.91 0.28–2.86 .871
T3 0.16 0.01–1.71 .871
T4 1.26 0.21–7.60 .801
Marital status
Married 1.00 — —
Single 2.88 0.58–14.14 .194
Insurance status
Private insurance 1.00 — —
Medicare 1.67 0.37–7.52 .503
Medical assistance 1.92 0.16–23.76 .610
Uninsured/self pay .66 0.11–4.13 .661
SLP ¼ speech–language pathology; CI ¼ confidence interval.
Laryngoscope 121: October 2011 Starmer et al.: Multidisciplinary Care and Patient Compliance
2133

Communication challenges may arise during and af-ter organ preservation treatments. Laryngeal edema maydevelop during radiation therapy leading to hoarseness orvoice loss. Nearly half of patients undergoing radiation forlaryngeal cancer will report some voice related handicapafter treatment.8 These difficulties may include symptomssuch as reduced pitch range, reduced loudness, andreduced phrase length.9 There appears to be some relation-ship between the severity of xerostomia and voicedifficulties following radiotherapy.10 The SLP can help toprepare patients for such problems and help to maintaincommunication in the most efficient manner possible.
Functional swallowing outcomes following organ pres-ervation therapies are dependent upon patient managementprior to and during HNCA treatment. There is evidence thatcompletion of prophylactic swallowing and trismus exercisesduring the course of treatment can be protective against tis-sue fibrosis and functional restrictions.3,11 Oropharyngealdeficits including reduced epiglottic tilt, pharyngeal constric-tor function, laryngeal elevation, tongue base retraction,airway protection, pharyngeal clearance, and cricopharyng-eal opening have been cited in the literature as commonfindings after organ preservation therapies for HNCA.12
These problems may lead to aspiration, long-term feedingtube dependence, and pulmonary complications.13 Trismusmay also develop leading to difficulty with accomplishingdesired oral intake.14 Maintaining an oral diet throughouttreatment and engaging the pharyngeal musculature isbelieved to have a positive impact on long-term function,although this has not been systematically evaluated to date.
There is evidence that speech, voice, and swallowinginterventions prior to radiotherapy improve long termfunction3,11 and it is suspected that patient quality of lifeand satisfaction improve as a result of these interventions.Clearly then, patient participation in SLP services shouldbe optimized in the most efficient way possible. Our datademonstrate that evaluation through a multidisciplinarysetting may help to optimize this efficiency thus maximiz-ing the potential for compliance and positive outcomes.
This series included only individuals with oropharyn-geal primary tumors due to the frequency at which we seethis population in our multidisciplinary clinic. Subjects werepredominantly young, White, married males. With the ris-ing incidence of HPV associated oropharyngeal cancers, thisis a fair representation of patients evaluated for oropharyn-geal primaries at our institution; however, this series maynot be representative of a broader sample of head and neckcancer patients. Although HPV status was not directlyaddressed in our analysis, it may be an interesting variableto consider when evaluating compliance in a broader sampleof HNCA patients. Patients with HPV-related head andneck cancers tend to be younger than traditional head andneck patients with lower exposure to risk factors such astobacco and alcohol.15 Differences in demographics betweenthe HPV-related HNCAs and malignancies not associatedwith HPVmay influence patient compliance as well. The rel-ative heterogeneity of this population may fail to identifythe impact of other demographic variables on patientcompliance.
We did not find a relationship between the numberof missed visits and referral patterns. It is likely that
this reflects that those patients seen outside of a multi-disciplinary setting are less likely to make anyappointments, and therefore, there are no appointmentsto miss. We suspect that the emphasis on the importanceof the SLP in the care team during the multidisciplinaryclinic is more salient to patients than a brief mentionduring an appointment that reviews all of the potentialside effects of radiation therapy. Further, the ability toestablish a clinical relationship between the patient andthe SLP from the time of diagnosis assists in thepatient’s familiarity and comfort with that individual.
One factor that may impact patient compliancewith treatments of any type is distance to the treatmentfacility. In this series, we did not analyze distance fromplace of residence to the treatment facility. Due to ourpatient referral pattern (regional, national, and interna-tional), we found it difficult to ascertain in aretrospective manner where patients resided duringtheir treatment. As all patients in this series weretreated onsite with daily radiotherapy and posttreat-ment follow-up appointments were coordinated, we feltthat distance was not an important variable for this pop-ulation. We do recognize that in other instances distancewould be a very important variable for consideration.
An important future direction would be to analyzefunctional outcomes and quality of life of patients seenthrough the multidisciplinary clinic as opposed to thoseseen through physician referral. Although we suspectimproved participation should lead to improved outcomes,this is not directly addressed in this article. One barrier togathering this data is how to account for patient outcomeswhen they are never seen by the SLP. Quality-of-lifeinstruments administered by the oncologists as well asproxy measures such as retention of feeding tube and per-formance status may give us an approximation of patientstatus, but certainly cannot be equated with quantitativeevaluative measures. This conundrum of how to captureand describe the outcomes of the noncompliant patient willcontinue to require consideration.
CONCLUSIONSPatients seen initially by a SLP in a multidiscipli-
nary HNCA clinic are more likely to participate inevaluations and treatments pertinent to optimization ofswallowing and communication outcomes. We believesuch participation can minimize patient anxiety regard-ing treatment effects, provide for early identification ofdifficulties, and employ early intervention to addressand prevent dysfunction. It is our hope that such inter-ventions will not only contribute to optimal function, butalso optimal quality of life in patients treated for HNCA.
BIBLIOGRAPHY
1. Jham BC, Freire ARS. Oral complications of radiotherapy in the head andneck. Rev Bras Otorrinolaringol 2006;72:704–708.
2. Cheng S, Terrell J, Bradford C, et al. Variables associated with feedingtube placement in patients with head and neck cancer. Arch OtolaryngolHead Neck Surg 2006;132:655–661.
3. Kulbersh BD, Rosenthal EL, McGrew BM, et al. Pretreatment, preopera-tive swallowing exercises may improve dysphagia quality of life. Laryn-goscope 2006;116:883–886.
4. Portone C, Johns M, Hapner E. A review of patient adherence to the rec-ommendation for voice therapy. J Voice 2008;22:192–196.
Laryngoscope 121: October 2011 Starmer et al.: Multidisciplinary Care and Patient Compliance
2134

5. Kosmider S, Shedda S, Jones I, et al. Predictors of clinic non-attend-ance—opportunities to improve patient outcomes in colorectal cancer.Intern Med J 2010;40:757–763.
6. Patel U, Patadia M, Holloway M, Rosen F. Poor radiotherapy compliancepredicts persistent regional disease in advanced head/neck Cancer. La-ryngoscope 2009;119:528–533.
7. Simental A, Carrau R. Assessment of swallowing function in patients withhead and neck cancer. Curr Oncol Rep 2004;6:162–165.
8. Van Gogh CD, Verdonck-de Leeuw IM, Boon-Kamma BA, et al. The effi-cacy of voice therapy in patients after treatment for early glottic carci-noma. Cancer 2006;106:95–105.
9. Orlikoff RF, Kraus DH, Budnick AS, et al. Vocal function following suc-cessful chemoradiation treatment for advanced laryngeal cancer: prelim-inary results. Phonoscope 1999;2:67–77.
10. Roh JL, Kim AY, Cho MJ. Xerostomia following radiotherapy of the headand neck affects vocal function. J Clin Oncol 2005;23:3016–3023.
11. van der Molen L, van Rossum MA, Burkhead L, et al. A randomized pre-ventive rehabilitation trial in advanced head and neck cancer patientstreated with chemoradiotherapy: feasibility, compliance, and short-termeffects. Dysphagia 2010 [Epub ahead of print].
12. Kotz T, Costello R, Li Y, et al. Swallowing dysfunction after chemoradia-tion for advanced squamous cell carcinoma of the head and neck. HeadNeck 2004;26:365–372.
13. Nguyen NP, Frank C, Moltz CC, et al. Aspiration rate following chemora-diation for head and neck cancer: an underreported occurrence. Radio-ther Oncol 2006;80:302–306.
14. Teguh D, Levendag P, Voet P, et al. Trismus in patients with oropharyn-geal cancer: relationship with dose in structures of mastication appara-tus. Head Neck 2008;30:622–630.
15. D’Souza G, Kreimer AR, Viscidi R, et al. Case control study of humanpapillomavirus and oropharyngeal cancer. N Engl J Med 2007;356:1944–1956.
Laryngoscope 121: October 2011 Starmer et al.: Multidisciplinary Care and Patient Compliance
2135